
Current Strategies to Guide the Antiplatelet Therapy in Acute Coronary Syndromes
 , , , ,
, , , ,
Abstract
:1. Introduction
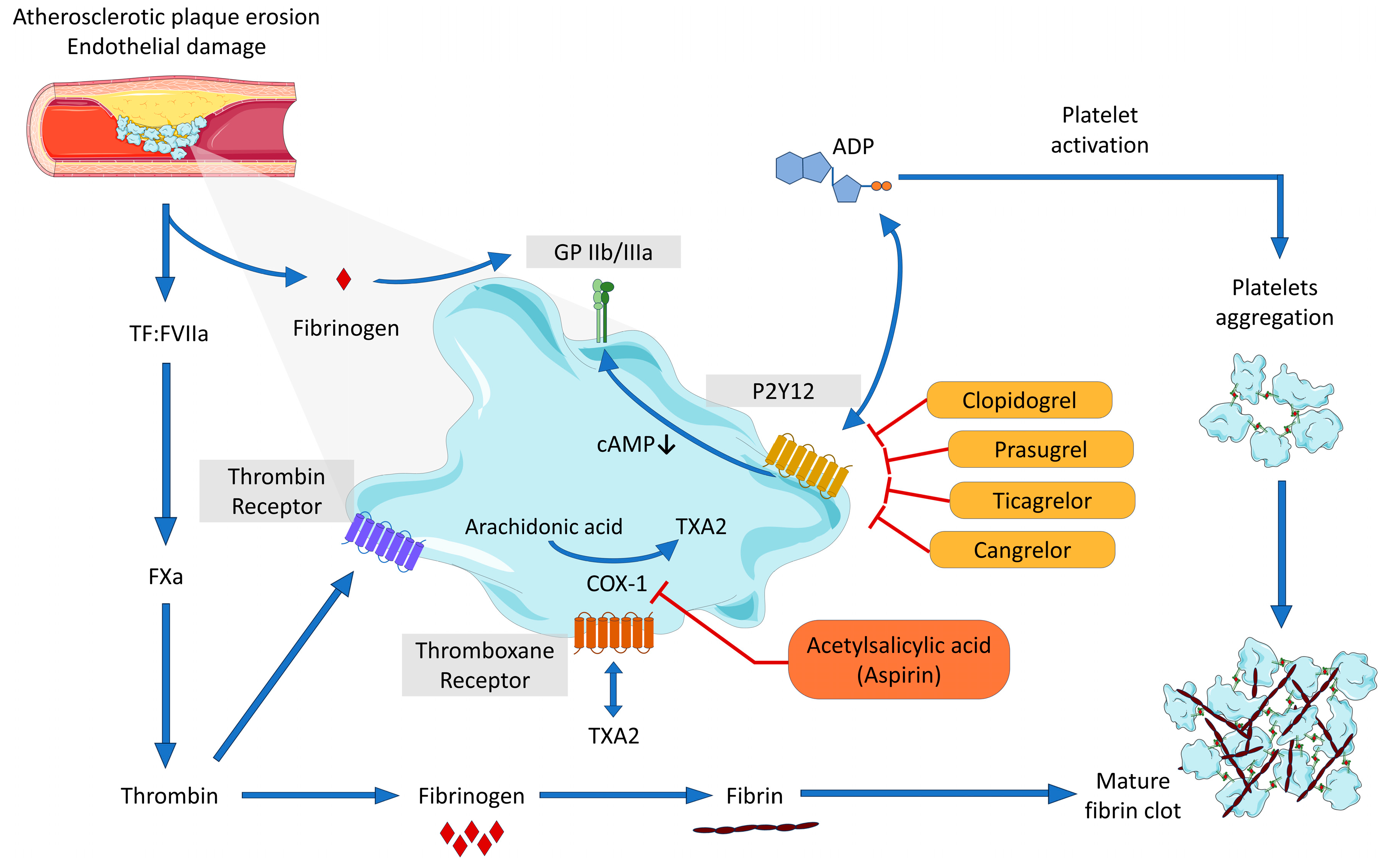
2. Platelet Biology and Function
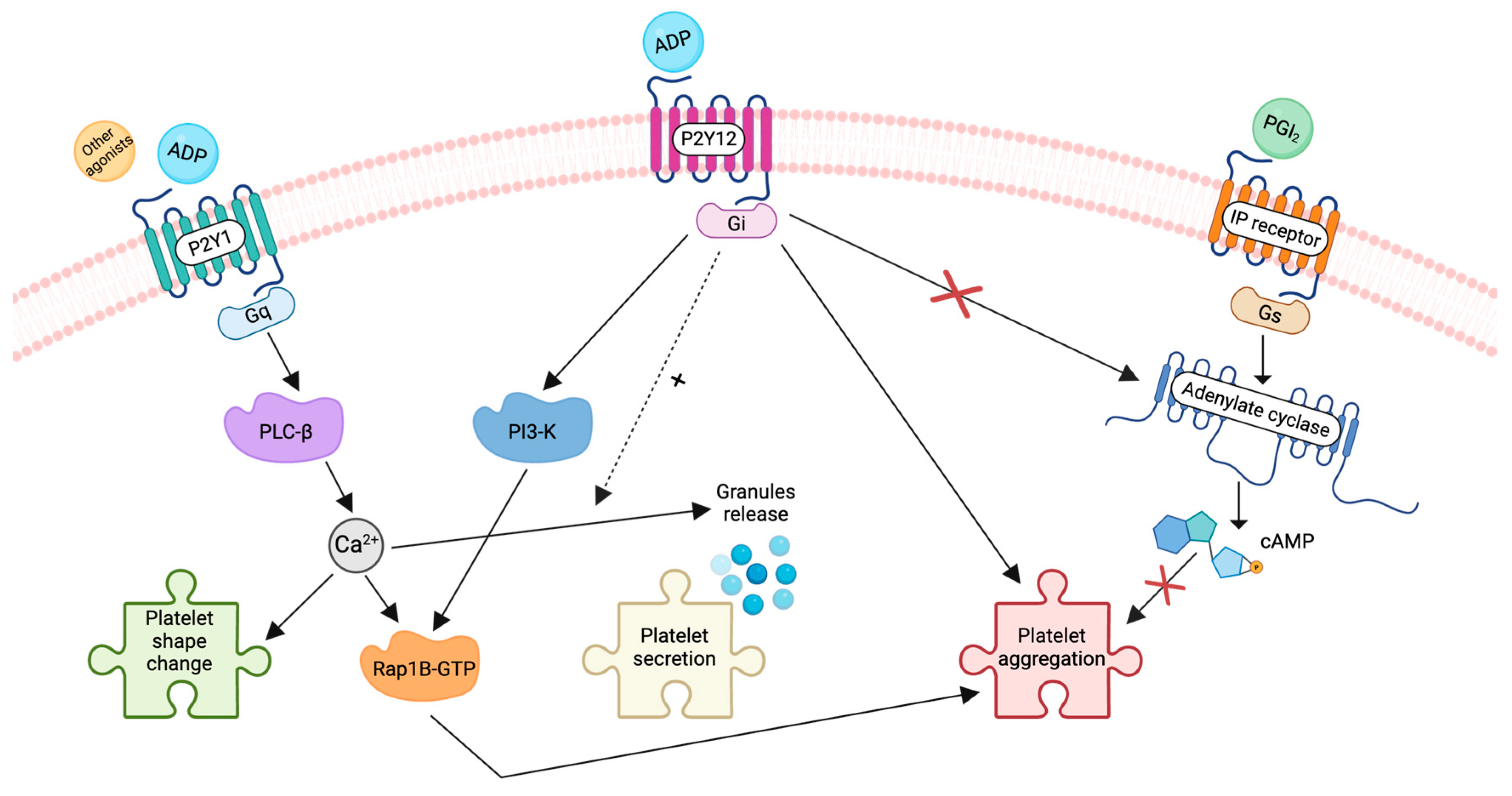
3. Role of P2Y12 and P2Y1 in ADP-Induced Platelet Activation
4. Different Approaches for Testing Platelet Function
4.1. Light Transmission Aggregometry
4.2. Whole Blood Aggregometry
4.3. VerifyNow
4.4. Platelet Function Analyzer-100/200
4.5. Thromboelastography
4.6. VASP Phosphorylation
5. Evidence Regarding Different Antiplatelet Agents
5.1. Aspirin or Acetylsalicylic Acid (ASA)
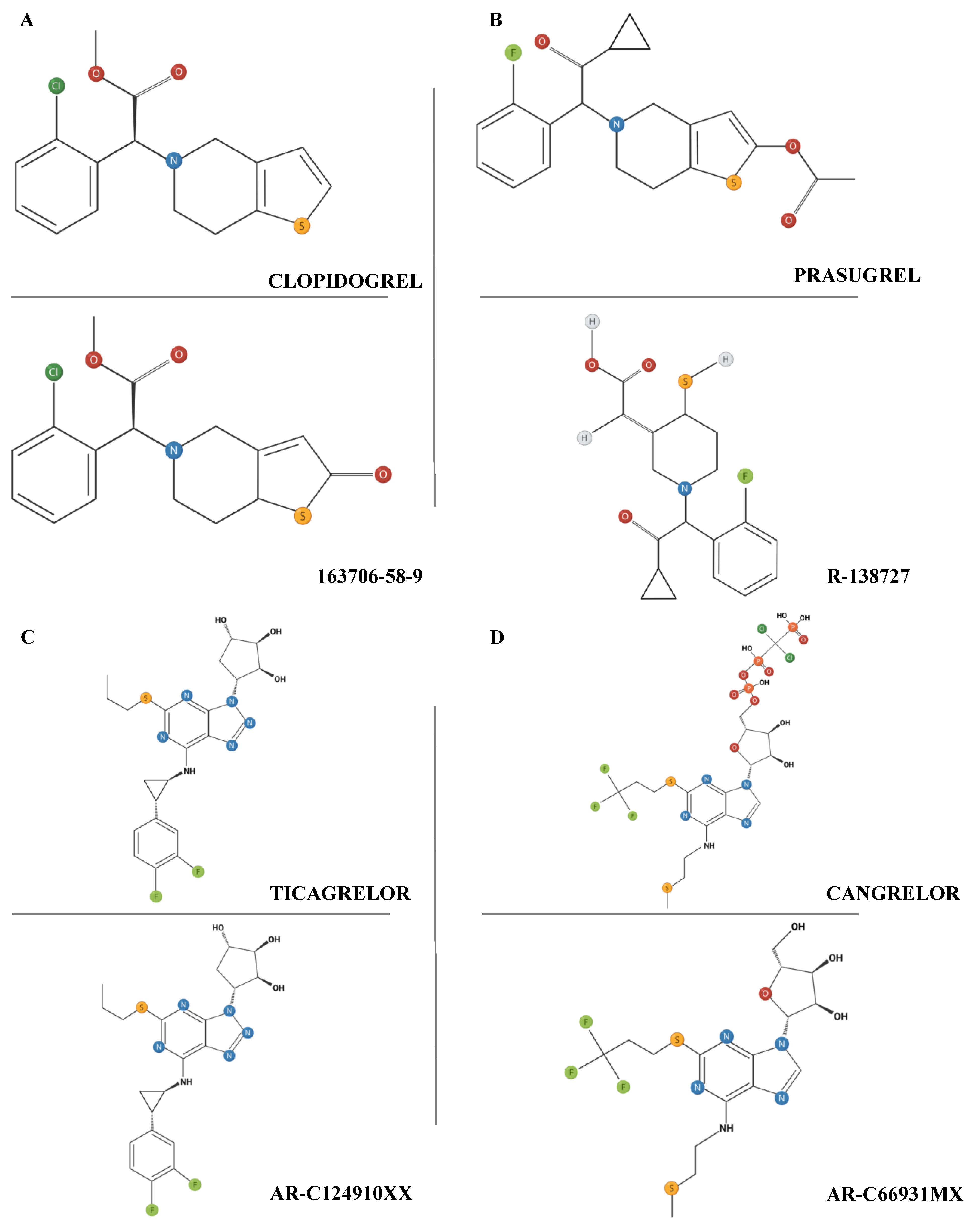
5.2. Clopidogrel
5.3. Prasugrel
5.4. Ticagrelor
5.5. Cangrelor
5.6. Comparing Prasugrel and Ticagrelor
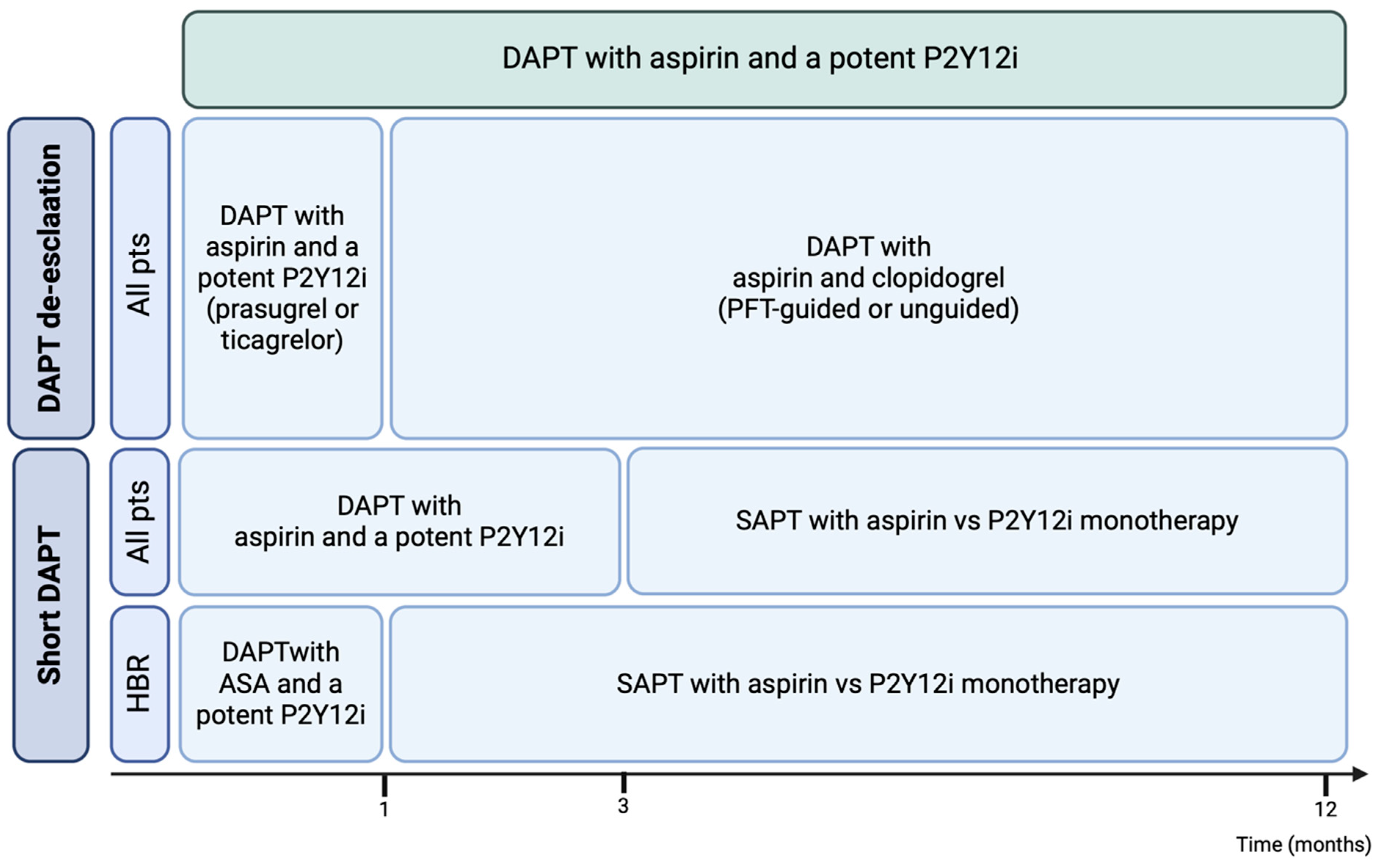
6. Alternative Strategies for Patients with High Bleeding Risk
6.1. P2Y12i Monotherapy
6.2. PFT-Guided Anti-P2Y12 Therapy
6.3. Genotype-Guided Anti-P2Y12 Therapy
6.4. Unguided De-Escalation of P2Y12i
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AC | adenylate cyclase |
| ACC | American College of Cardiology |
| ACS | acute coronary syndromes |
| ADP | adenosine diphosphate |
| AHA | American Heart Association |
| AKT | protein kinase B |
| AMI | acute myocardial infarction |
| APC | activated protein C |
| ARU | aspirin response units |
| ASA | acetylsalicylic acid |
| BARC | bleeding academic research consortium |
| CABG | coronary artery bypass grafting |
| cAMP | cyclic adenosine monophosphate |
| CCS | chronic coronary syndrome |
| cGMP | cyclic guanosine monophosphate |
| CI | confidence interval |
| COX-1 | cyclooxygenase-1 |
| CV | cardiovascular |
| CYP | cytochrome P450 |
| CYP2C9 | cytochrome P450 family 2 subfamily C member 9 |
| DAG | diacylglycerol |
| DAPT | dual antiplatelet therapy |
| DAT | dual antithrombotic therapy |
| DES | drug-eluting stent |
| DOAC | direct oral anticoagulant |
| ESC | European Society of Cardiology |
| FDA | Food and Drug Administration |
| GP | glycoprotein |
| GPCR | G-protein-coupled receptor |
| HBR | high bleeding risk |
| HIR | high ischemic risk |
| HTPR | high on-treatment platelet reactivity |
| IP3 | inositoltriphosphate |
| ITAM | immunoreceptor tyrosine-based activation motif |
| LAMP | lysosome-associated membrane protein |
| LD | load dose |
| LoF | Loss of function |
| LTA | light transmission aggregometry |
| MACCE | major adverse cardiovascular and cerebrovascular events |
| MACEs | major adverse cardiovascular events |
| MD | maintenance dose |
| MEA | multiple electrode aggregometry |
| MI | myocardial infarction |
| NACE | net adverse clinical events |
| NO | nitric oxide |
| NSTE-ACS | non-ST-elevation acute coronary syndromes |
| P2Y12i | P2Y12 inhibitor |
| PAR | protease-activated receptor |
| PAU | platelet aggregation units |
| PCI | percutaneous coronary interventions |
| PFA | platelet function analyzer |
| PFT-GT | PFT-guided therapy |
| PFT | platelet function test |
| PGE1 | prostaglandin E1 |
| PGI2 | prostacyclin |
| PI-3K | phosphatidylinositol 3-kinase |
| PI(4,5)P2 | phosphatidylinositol 4,5-bisphosphate |
| PKA | protein kinase A |
| PKG | protein kinase G |
| PLC | phospholipase C |
| PRP | platelet-rich plasma |
| PRU | P2Y12 response units |
| RCT | randomized clinical trial |
| ROTEM | rotation thromboelastometry |
| RR | rate ratio |
| TAT | triple antithrombotic therapy |
| TEG | thromboelastography |
| TF | tissue factor |
| TIA | transient ischemic attack |
| TIMI | thrombolysis in myocardial infarction |
| TRAP | thrombin receptor-activating peptide |
| TX | thromboxane |
| VASP | vasodilator-stimulated phosphoprotein |
| VKA | vitamin K antagonists |
| vWF | von Willebrand factor |
References
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.-A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the Management of Acute Coronary Syndromes. Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef] [PubMed]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e18–e114. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Jennings, C.L.; Manning, E.; Cameron, S.J. Platelets at the Vessel Wall in Non-Thrombotic Disease. Circ. Res. 2023, 132, 775–790. [Google Scholar] [CrossRef] [PubMed]
- Lefrançais, E.; Ortiz-Muñoz, G.; Caudrillier, A.; Mallavia, B.; Liu, F.; Sayah, D.M.; Thornton, E.E.; Headley, M.B.; David, T.; Coughlin, S.R.; et al. The Lung Is a Site of Platelet Biogenesis and a Reservoir for Haematopoietic Progenitors. Nature 2017, 544, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Tilburg, J.; Becker, I.C.; Italiano, J.E. Don’t You Forget about Me(Gakaryocytes). Blood 2022, 139, 3245–3254. [Google Scholar] [CrossRef] [PubMed]
- Thon, J.N.; Italiano, J.E. Platelets: Production, Morphology and Ultrastructure. In Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 2012; pp. 3–22. [Google Scholar] [CrossRef]
- Gryglewski, R.J.; Botting, R.M.; Vane, J.R. Mediators Produced by the Endothelial Cell. Hypertension 1988, 12, 530–548. [Google Scholar] [CrossRef] [PubMed]
- Anfossi, G.; Russo, I.; Massucco, P.; Mattiello, L.; Balbo, A.; Cavalot, F.; Trovati, M. Studies on Inhibition of Human Platelet Function by Sodium Nitroprusside. Kinetic Evaluation of the Effect on Aggregation and Cyclic Nucleotide Content. Thromb. Res. 2001, 102, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Russo, I.; Barale, C.; Melchionda, E.; Penna, C.; Pagliaro, P. Platelets and Cardioprotection: The Role of Nitric Oxide and Carbon Oxide. Int. J. Mol. Sci. 2023, 24, 6107. [Google Scholar] [CrossRef]
- Gkaliagkousi, E.; Ritter, J.; Ferro, A. Platelet-Derived Nitric Oxide Signaling and Regulation. Circ. Res. 2007, 101, 654–662. [Google Scholar] [CrossRef]
- Pareti, F.I.; Carrera, D.; Mannucci, L.; Mannucci, P.M. Effect on Platelet Functions of Derivatives of Cyclic Nucleotides. Thromb. Haemost. 1978, 39, 404–410. [Google Scholar] [CrossRef]
- Russo, I.; Doronzo, G.; Mattiello, L.; De Salve, A.; Trovati, M.; Anfossi, G. The Activity of Constitutive Nitric Oxide Synthase Is Increased by the Pathway cAMP/cAMP-Activated Protein Kinase in Human Platelets. New Insights into the Antiaggregating Effects of cAMP-Elevating Agents. Thromb. Res. 2004, 114, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Anfossi, G.; Russo, I.; Massucco, P.; Mattiello, L.; Doronzo, G.; De Salve, A.; Trovati, M. Impaired Synthesis and Action of Antiaggregating Cyclic Nucleotides in Platelets from Obese Subjects: Possible Role in Platelet Hyperactivation in Obesity. Eur. J. Clin. Investig. 2004, 34, 482–489. [Google Scholar] [CrossRef]
- Anfossi, G.; Russo, I.; Trovati, M. Platelet Dysfunction in Central Obesity. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Di Giovine, G.; Verdoia, M.; Barbieri, L.; Schaffer, A.; Aimaretti, G.; Bellomo, G.; Marino, P.; Suryapranata, H.; Sinigaglia, F.; De Luca, G.; et al. Impact of Diabetes on Fibrinogen Levels and Its Relationship with Platelet Reactivity and Coronary Artery Disease: A Single-Centre Study. Diabetes Res. Clin. Pract. 2015, 109, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Russo, I.; Penna, C.; Musso, T.; Popara, J.; Alloatti, G.; Cavalot, F.; Pagliaro, P. Platelets, Diabetes and Myocardial Ischemia/Reperfusion Injury. Cardiovasc. Diabetol. 2017, 16, 71. [Google Scholar] [CrossRef]
- Barale, C.; Cavalot, F.; Frascaroli, C.; Bonomo, K.; Morotti, A.; Guerrasio, A.; Russo, I. Association between High On-Aspirin Platelet Reactivity and Reduced Superoxide Dismutase Activity in Patients Affected by Type 2 Diabetes Mellitus or Primary Hypercholesterolemia. Int. J. Mol. Sci. 2020, 21, 4983. [Google Scholar] [CrossRef] [PubMed]
- Barale, C.; Russo, I. Influence of Cardiometabolic Risk Factors on Platelet Function. Int. J. Mol. Sci. 2020, 21, 623. [Google Scholar] [CrossRef] [PubMed]
- Nagy, B.; Jin, J.; Ashby, B.; Reilly, M.P.; Kunapuli, S.P. Contribution of the P2Y12 Receptor-Mediated Pathway to Platelet Hyperreactivity in Hypercholesterolemia. J. Thromb. Haemost. 2011, 9, 810–819. [Google Scholar] [CrossRef] [PubMed]
- Van de Wouwer, M.; Collen, D.; Conway, E.M. Thrombomodulin-Protein C-EPCR System: Integrated to Regulate Coagulation and Inflammation. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 1374–1383. [Google Scholar] [CrossRef]
- Loghmani, H.; Conway, E.M. Exploring Traditional and Nontraditional Roles for Thrombomodulin. Blood 2018, 132, 148–158. [Google Scholar] [CrossRef]
- Warn-Cramer, B.J.; Almus, F.E.; Rapaport, S.I. Studies of the Factor Xa-Dependent Inhibitor of Factor VIIa/Tissue Factor (Extrinsic Pathway Inhibitor) from Cell Supernates of Cultured Human Umbilical Vein Endothelial Cells. Thromb. Haemost. 1989, 61, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Kauskot, A.; Hoylaerts, M.F. Platelet Receptors. In Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 2012; pp. 23–57. [Google Scholar] [CrossRef]
- Ruggeri, Z.M.; Mendolicchio, G.L. Adhesion Mechanisms in Platelet Function. Circ. Res. 2007, 100, 1673–1685. [Google Scholar] [CrossRef] [PubMed]
- Berridge, M.J. Inositol Trisphosphate and Diacylglycerol as Second Messengers. Biochem. J. 1984, 220, 345–360. [Google Scholar] [CrossRef] [PubMed]
- Sage, S.O.; Rink, T.J. The Kinetics of Changes in Intracellular Calcium Concentration in Fura-2-Loaded Human Platelets. J. Biol. Chem. 1987, 262, 16364–16369. [Google Scholar] [CrossRef] [PubMed]
- Watson, S.P.; Gibbins, J. Collagen Receptor Signalling in Platelets: Extending the Role of the ITAM. Immunol. Today 1998, 19, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Rendu, F.; Brohard-Bohn, B. The Platelet Release Reaction: Granules’ Constituents, Secretion and Functions. Platelets 2001, 12, 261–273. [Google Scholar] [CrossRef]
- Smith, C.W. Release of α-Granule Contents during Platelet Activation. Platelets 2022, 33, 491–502. [Google Scholar] [CrossRef]
- Senzel, L.; Gnatenko, D.V.; Bahou, W.F. The Platelet Proteome. Curr. Opin. Hematol. 2009, 16, 329–333. [Google Scholar] [CrossRef]
- Schwertz, H.; Köster, S.; Kahr, W.H.A.; Michetti, N.; Kraemer, B.F.; Weitz, D.A.; Blaylock, R.C.; Kraiss, L.W.; Greinacher, A.; Zimmerman, G.A.; et al. Anucleate Platelets Generate Progeny. Blood 2010, 115, 3801–3809. [Google Scholar] [CrossRef]
- Della Corte, A.; Tamburrelli, C.; Crescente, M.; Giordano, L.; D’Imperio, M.; Di Michele, M.; Donati, M.B.; De Gaetano, G.; Rotilio, D.; Cerletti, C. Platelet Proteome in Healthy Volunteers Who Smoke. Platelets 2012, 23, 91–105. [Google Scholar] [CrossRef]
- Springer, D.L.; Miller, J.H.; Spinelli, S.L.; Pasa-Tolic, L.; Purvine, S.O.; Daly, D.S.; Zangar, R.C.; Jin, S.; Blumberg, N.; Francis, C.W.; et al. Platelet Proteome Changes Associated with Diabetes and during Platelet Storage for Transfusion. J. Proteome Res. 2009, 8, 2261–2272. [Google Scholar] [CrossRef] [PubMed]
- Parguiña, A.F.; Grigorian-Shamajian, L.; Agra, R.M.; Teijeira-Fernández, E.; Rosa, I.; Alonso, J.; Viñuela-Roldán, J.E.; Seoane, A.; González-Juanatey, J.R.; García, A. Proteins Involved in Platelet Signaling Are Differentially Regulated in Acute Coronary Syndrome: A Proteomic Study. PLoS ONE 2010, 5, e13404. [Google Scholar] [CrossRef]
- Sacristán, D.; Marques, M.; Zamorano-León, J.J.; Luque, M.; Armengol, J.; Del Castillo, J.; Martín, J.; Delpón, E.; Ramos-Mozo, P.; de Prada, T.P.; et al. Modifications by Olmesartan Medoxomil Treatment of the Platelet Protein Profile of Moderate Hypertensive Patients. Proteomics Clin. Appl. 2008, 2, 1300–1312. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Ostberg, O.; Wihlborg, A.-K.; Brogren, H.; Jern, S.; Erlinge, D. Quantification of ADP and ATP Receptor Expression in Human Platelets. J. Thromb. Haemost. 2003, 1, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Jantzen, H.M.; Milstone, D.S.; Gousset, L.; Conley, P.B.; Mortensen, R.M. Impaired Activation of Murine Platelets Lacking G Alpha(I2). J. Clin. Investig. 2001, 108, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kunapuli, S.P. P2Y12 Receptor in Platelet Activation. Platelets 2011, 22, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, E.; Bosco, O.; Tropel, P.; Laffargue, M.; Calvez, R.; Altruda, F.; Wymann, M.; Montrucchio, G. Resistance to Thromboembolism in PI3Kgamma-Deficient Mice. FASEB J. 2001, 15, 2019–2021. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, M. The P2 Receptors and Congenital Platelet Function Defects. Semin. Thromb. Hemost. 2005, 31, 168–173. [Google Scholar] [CrossRef]
- Jin, J.; Kunapuli, S.P. Coactivation of Two Different G Protein-Coupled Receptors Is Essential for ADP-Induced Platelet Aggregation. Proc. Natl. Acad. Sci. USA 1998, 95, 8070–8074. [Google Scholar] [CrossRef]
- Garcia, A.; Kim, S.; Bhavaraju, K.; Schoenwaelder, S.M.; Kunapuli, S.P. Role of Phosphoinositide 3-Kinase Beta in Platelet Aggregation and Thromboxane A2 Generation Mediated by Gi Signalling Pathways. Biochem. J. 2010, 429, 369–377. [Google Scholar] [CrossRef]
- Cattaneo, M.; Lecchi, A.; Randi, A.M.; McGregor, J.L.; Mannucci, P.M. Identification of a New Congenital Defect of Platelet Function Characterized by Severe Impairment of Platelet Responses to Adenosine Diphosphate. Blood 1992, 80, 2787–2796. [Google Scholar] [CrossRef]
- Cattaneo, M.; Lecchi, A.; Lombardi, R.; Gachet, C.; Zighetti, M.L. Platelets from a Patient Heterozygous for the Defect of P2CYC Receptors for ADP Have a Secretion Defect despite Normal Thromboxane A2 Production and Normal Granule Stores: Further Evidence That Some Cases of Platelet “primary Secretion Defect” Are Heterozygous for a Defect of P2CYC Receptors. Arterioscler. Thromb. Vasc. Biol. 2000, 20, E101–E106. [Google Scholar] [CrossRef]
- Cattaneo, M.; Lombardi, R.; Zighetti, M.L.; Gachet, C.; Ohlmann, P.; Cazenave, J.P.; Mannucci, P.M. Deficiency of (33P)2MeS-ADP Binding Sites on Platelets with Secretion Defect, Normal Granule Stores and Normal Thromboxane A2 Production. Evidence That ADP Potentiates Platelet Secretion Independently of the Formation of Large Platelet Aggregates and Thromboxane A2 Production. Thromb. Haemost. 1997, 77, 986–990. [Google Scholar] [PubMed]
- Cattaneo, M.; Zighetti, M.L.; Lombardi, R.; Martinez, C.; Lecchi, A.; Conley, P.B.; Ware, J.; Ruggeri, Z.M. Molecular Bases of Defective Signal Transduction in the Platelet P2Y12 Receptor of a Patient with Congenital Bleeding. Proc. Natl. Acad. Sci. USA 2003, 100, 1978–1983. [Google Scholar] [CrossRef] [PubMed]
- Andre, P.; Delaney, S.M.; LaRocca, T.; Vincent, D.; DeGuzman, F.; Jurek, M.; Koller, B.; Phillips, D.R.; Conley, P.B. P2Y12 Regulates Platelet Adhesion/Activation, Thrombus Growth, and Thrombus Stability in Injured Arteries. J. Clin. Investig. 2003, 112, 398–406. [Google Scholar] [CrossRef]
- Nurden, P.; Savi, P.; Heilmann, E.; Bihour, C.; Herbert, J.M.; Maffrand, J.P.; Nurden, A. An Inherited Bleeding Disorder Linked to a Defective Interaction between ADP and Its Receptor on Platelets. Its Influence on Glycoprotein IIb-IIIa Complex Function. J. Clin. Investig. 1995, 95, 1612–1622. [Google Scholar] [CrossRef] [PubMed]
- Turner, N.A.; Moake, J.L.; McIntire, L.V. Blockade of Adenosine Diphosphate Receptors P2Y(12) and P2Y(1) Is Required to Inhibit Platelet Aggregation in Whole Blood under Flow. Blood 2001, 98, 3340–3345. [Google Scholar] [CrossRef]
- Chen, J.; Qu, Y.; Jiang, M.; Li, H.; Cui, C.; Liu, D. Population Pharmacokinetic/Pharmacodynamic Models for P2Y12 Inhibitors: A Systematic Review and Clinical Appraisal Using Exposure Simulation. Clin. Pharmacokinet. 2024, 63, 303–316. [Google Scholar] [CrossRef]
- Born, G.V. Aggregation of Blood Platelets by Adenosine Diphosphate and Its Reversal. Nature 1962, 194, 927–929. [Google Scholar] [CrossRef]
- Pai, M.; Wang, G.; Moffat, K.A.; Liu, Y.; Seecharan, J.; Webert, K.; Heddle, N.; Hayward, C. Diagnostic Usefulness of a Lumi-Aggregometer Adenosine Triphosphate Release Assay for the Assessment of Platelet Function Disorders. Am. J. Clin. Pathol. 2011, 136, 350–358. [Google Scholar] [CrossRef]
- Rand, M.L.; Leung, R.; Packham, M.A. Platelet Function Assays. Transfus. Apher. Sci. 2003, 28, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, N.S.; Panzer-Knodle, S.G.; Haas, N.F.; Taite, B.B.; Szalony, J.A.; Page, J.D.; Feigen, L.P.; Lansky, D.M.; Salyers, A.K. Assessment of Platelet Function Assays. Am. Heart J. 1998, 135, S170–S178. [Google Scholar] [CrossRef] [PubMed]
- Harrison, P. Progress in the Assessment of Platelet Function. Br. J. Haematol. 2000, 111, 733–744. [Google Scholar] [PubMed]
- Michelson, A.D. Platelet Function Testing in Cardiovascular Diseases. Circulation 2004, 110, e489–e493. [Google Scholar] [CrossRef] [PubMed]
- Tóth, O.; Calatzis, A.; Penz, S.; Losonczy, H.; Siess, W. Multiple Electrode Aggregometry: A New Device to Measure Platelet Aggregation in Whole Blood. Thromb. Haemost. 2006, 96, 781–788. [Google Scholar] [PubMed]
- Paniccia, R.; Antonucci, E.; Maggini, N.; Romano, E.; Gori, A.M.; Marcucci, R.; Prisco, D.; Abbate, R. Assessment of Platelet Function on Whole Blood by Multiple Electrode Aggregometry in High-Risk Patients with Coronary Artery Disease Receiving Antiplatelet Therapy. Am. J. Clin. Pathol. 2009, 131, 834–842. [Google Scholar] [CrossRef] [PubMed]
- Valarche, V.; Desconclois, C.; Boutekedjiret, T.; Dreyfus, M.; Proulle, V. Multiplate Whole Blood Impedance Aggregometry: A New Tool for von Willebrand Disease. J. Thromb. Haemost. 2011, 9, 1645–1647. [Google Scholar] [CrossRef] [PubMed]
- van Werkum, J.W.; Harmsze, A.M.; Elsenberg, E.H.; Bouman, H.J.; ten Berg, J.M.; Hackeng, C.M. The Use of the VerifyNow System to Monitor Antiplatelet Therapy: A Review of the Current Evidence. Platelets 2008, 19, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.C.; Aucoin-Barry, D.; Manuelian, D.; Monbouquette, R.; Reisman, M.; Gray, W.; Block, P.C.; Block, E.H.; Ladenheim, M.; Simon, D.I. Incidence of Aspirin Nonresponsiveness Using the Ultegra Rapid Platelet Function Assay-ASA. Am. J. Cardiol. 2003, 92, 1492–1494. [Google Scholar] [CrossRef]
- Koessler, J.; Kobsar, A.L.; Rajkovic, M.S.; Schafer, A.; Flierl, U.; Pfoertsch, S.; Bauersachs, J.; Steigerwald, U.; Rechner, A.R.; Walter, U. The New INNOVANCE® PFA P2Y Cartridge Is Sensitive to the Detection of the P2Y12 Receptor Inhibition. Platelets 2011, 22, 20–27. [Google Scholar] [CrossRef]
- Linnemann, B.; Schwonberg, J.; Rechner, A.R.; Mani, H.; Lindhoff-Last, E. Assessment of Clopidogrel Non-Response by the PFA-100 System Using the New Test Cartridge INNOVANCE PFA P2Y. Ann. Hematol. 2010, 89, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Edwards, A.; Jakubowski, J.A.; Rechner, A.R.; Sugidachi, A.; Harrison, P. Evaluation of the INNOVANCE PFA P2Y Test Cartridge: Sensitivity to P2Y(12) Blockade and Influence of Anticoagulant. Platelets 2012, 23, 106–115. [Google Scholar] [CrossRef]
- Chen, A.; Teruya, J. Global Hemostasis Testing Thromboelastography: Old Technology, New Applications. Clin. Lab. Med. 2009, 29, 391–407. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Johnson, R.I.; Kirmani, B.H. Pre- and Post-Bypass Platelet Function Testing With Multiple Electrode Aggregometry and TEG Platelet Mapping in Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2015, 29, 1272–1276. [Google Scholar] [CrossRef] [PubMed]
- Barragan, P.; Bouvier, J.-L.; Roquebert, P.-O.; Macaluso, G.; Commeau, P.; Comet, B.; Lafont, A.; Camoin, L.; Walter, U.; Eigenthaler, M. Resistance to Thienopyridines: Clinical Detection of Coronary Stent Thrombosis by Monitoring of Vasodilator-Stimulated Phosphoprotein Phosphorylation. Catheter. Cardiovasc. Interv. 2003, 59, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Aleil, B.; Ravanat, C.; Cazenave, J.P.; Rochoux, G.; Heitz, A.; Gachet, C. Flow Cytometric Analysis of Intraplatelet VASP Phosphorylation for the Detection of Clopidogrel Resistance in Patients with Ischemic Cardiovascular Diseases. J. Thromb. Haemost. 2005, 3, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, G.; Rothe, G.; Ruf, A.; Barlage, S.; Tschöpe, D.; Clemetson, K.J.; Goodall, A.H.; Michelson, A.D.; Nurden, A.T.; Shankey, T.V. European Working Group on Clinical Cell Analysis: Consensus Protocol for the Flow Cytometric Characterisation of Platelet Function. Thromb. Haemost. 1998, 79, 885–896. [Google Scholar] [CrossRef] [PubMed]
- Matzdorff, A. Platelet Function Tests and Flow Cytometry to Monitor Antiplatelet Therapy. Semin. Thromb. Hemost. 2005, 31, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Fuster, V.; Sweeny, J.M. Aspirin: A Historical and Contemporary Therapeutic Overview. Circulation 2011, 123, 768–778. [Google Scholar] [CrossRef]
- Baigent, C.; Collins, R.; Appleby, P.; Parish, S.; Sleight, P.; Peto, R. ISIS-2: 10 Year Survival among Patients with Suspected Acute Myocardial Infarction in Randomised Comparison of Intravenous Streptokinase, Oral Aspirin, Both, or Neither. The ISIS-2 (Second International Study of Infarct Survival) Collaborative Group. BMJ 1998, 316, 1337–1343. [Google Scholar] [CrossRef]
- CURRENT-OASIS 7 Investigators; Mehta, S.R.; Bassand, J.-P.; Chrolavicius, S.; Diaz, R.; Eikelboom, J.W.; Fox, K.A.A.; Granger, C.B.; Jolly, S.; Joyner, C.D.; et al. Dose Comparisons of Clopidogrel and Aspirin in Acute Coronary Syndromes. N. Engl. J. Med. 2010, 363, 930–942. [Google Scholar] [CrossRef] [PubMed]
- Gravinese, C.; Bianco, M.; Cerrato, E.; Destefanis, P.; Luciano, A.; Bernardi, A.; Bellucca, S.; Varbella, F.; Gaita, F.; Pozzi, R. Is Aspirin Still the Cornerstone of Antiplatelet Therapy in Patients With Coronary Artery Disease? An Historical and Practical Narrative Review. Hosp. Pract. Res. 2017, 2, 94–101. [Google Scholar] [CrossRef]
- Valgimigli, M.; Ariotti, S.; Costa, F. Duration of Dual Antiplatelet Therapy after Drug-Eluting Stent Implantation: Will We Ever Reach a Consensus? Eur. Heart J. 2015, 36, 1219–1222. [Google Scholar] [CrossRef] [PubMed]
- Feres, F.; Costa, R.A.; Abizaid, A.; Leon, M.B.; Marin-Neto, J.A.; Botelho, R.V.; King, S.B.; Negoita, M.; Liu, M.; de Paula, J.E.T.; et al. Three vs Twelve Months of Dual Antiplatelet Therapy after Zotarolimus-Eluting Stents: The OPTIMIZE Randomized Trial. JAMA 2013, 310, 2510–2522. [Google Scholar] [CrossRef] [PubMed]
- Hahn, J.-Y.; Song, Y.B.; Oh, J.-H.; Cho, D.-K.; Lee, J.B.; Doh, J.-H.; Kim, S.-H.; Jeong, J.-O.; Bae, J.-H.; Kim, B.-O.; et al. 6-Month versus 12-Month or Longer Dual Antiplatelet Therapy after Percutaneous Coronary Intervention in Patients with Acute Coronary Syndrome (SMART-DATE): A Randomised, Open-Label, Non-Inferiority Trial. Lancet 2018, 391, 1274–1284. [Google Scholar] [CrossRef] [PubMed]
- Bianco, M.; Careggio, A.; Destefanis, P.; Luciano, A.; Perrelli, M.G.; Quadri, G.; Rossini, R.; Campo, G.; Vizzari, G.; D’Ascenzo, F.; et al. P2Y12 Inhibitors Monotherapy after Short Course of Dual Antiplatelet Therapy in Patients Undergoing Percutaneous Coronary Intervention: A Meta-Analysis of Randomized Clinical Trials Including 29 089 Patients. Eur. Heart J. Cardiovasc. Pharmacother. 2021, 7, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Frigoli, E.; Heg, D.; Tijssen, J.; Jüni, P.; Vranckx, P.; Ozaki, Y.; Morice, M.-C.; Chevalier, B.; Onuma, Y.; et al. Dual Antiplatelet Therapy after PCI in Patients at High Bleeding Risk. N. Engl. J. Med. 2021, 385, 1643–1655. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.-J.; Kim, J.-S.; Hong, S.J.; Lim, D.-S.; Lee, S.-Y.; Yun, K.H.; Park, J.-K.; Kang, W.C.; Kim, Y.H.; Yoon, H.-J.; et al. 1-Month Dual-Antiplatelet Therapy Followed by Aspirin Monotherapy After Polymer-Free Drug-Coated Stent Implantation: One-Month DAPT Trial. JACC Cardiovasc. Interv. 2021, 14, 1801–1811. [Google Scholar] [CrossRef] [PubMed]
- Madhavan, M.V.; Kirtane, A.J.; Redfors, B.; Généreux, P.; Ben-Yehuda, O.; Palmerini, T.; Benedetto, U.; Biondi-Zoccai, G.; Smits, P.C.; von Birgelen, C.; et al. Stent-Related Adverse Events > 1 Year after Percutaneous Coronary Intervention. J. Am. Coll. Cardiol. 2020, 75, 590–604. [Google Scholar] [CrossRef]
- Valgimigli, M.; Costa, F.; Lokhnygina, Y.; Clare, R.M.; Wallentin, L.; Moliterno, D.J.; Armstrong, P.W.; White, H.D.; Held, C.; Aylward, P.E.; et al. Trade-off of Myocardial Infarction vs. Bleeding Types on Mortality after Acute Coronary Syndrome: Lessons from the Thrombin Receptor Antagonist for Clinical Event Reduction in Acute Coronary Syndrome (TRACER) Randomized Trial. Eur. Heart J. 2017, 38, 804–810. [Google Scholar] [CrossRef]
- Mehran, R.; Baber, U.; Sharma, S.K.; Cohen, D.J.; Angiolillo, D.J.; Briguori, C.; Cha, J.Y.; Collier, T.; Dangas, G.; Dudek, D.; et al. Ticagrelor with or without Aspirin in High-Risk Patients after PCI. N. Engl. J. Med. 2019, 381, 2032–2042. [Google Scholar] [CrossRef] [PubMed]
- Vranckx, P.; Valgimigli, M.; Jüni, P.; Hamm, C.; Steg, P.G.; Heg, D.; van Es, G.A.; McFadden, E.P.; Onuma, Y.; van Meijeren, C.; et al. Ticagrelor plus Aspirin for 1 Month, Followed by Ticagrelor Monotherapy for 23 Months vs Aspirin plus Clopidogrel or Ticagrelor for 12 Months, Followed by Aspirin Monotherapy for 12 Months after Implantation of a Drug-Eluting Stent: A Multicentre, Open-Label, Randomised Superiority Trial. Lancet 2018, 392, 940–949. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.-K.; Hong, S.-J.; Cho, Y.-H.; Yun, K.H.; Kim, Y.H.; Suh, Y.; Cho, J.Y.; Her, A.-Y.; Cho, S.; Jeon, D.W.; et al. Effect of Ticagrelor Monotherapy vs Ticagrelor with Aspirin on Major Bleeding and Cardiovascular Events in Patients with Acute Coronary Syndrome: The TICO Randomized Clinical Trial. JAMA 2020, 323, 2407–2416. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Steinhubl, S.R.; Berger, P.B.; Mann, J.T.; Fry, E.T.A.; DeLago, A.; Wilmer, C.; Topol, E.J.; CREDO Investigators. Clopidogrel for the Reduction of Events During Observation Early and Sustained Dual Oral Antiplatelet Therapy Following Percutaneous Coronary Intervention: A Randomized Controlled Trial. JAMA 2002, 288, 2411–2420. [Google Scholar] [CrossRef] [PubMed]
- Sabatine, M.S.; Cannon, C.P.; Gibson, C.M.; López-Sendón, J.L.; Montalescot, G.; Theroux, P.; Claeys, M.J.; Cools, F.; Hill, K.A.; Skene, A.M.; et al. Addition of Clopidogrel to Aspirin and Fibrinolytic Therapy for Myocardial Infarction with ST-Segment Elevation. N. Engl. J. Med. 2005, 352, 1179–1189. [Google Scholar] [CrossRef] [PubMed]
- CAPRIE Steering Committee. A Randomised, Blinded, Trial of Clopidogrel versus Aspirin in Patients at Risk of Ischaemic Events (CAPRIE). Lancet 1996, 348, 1329–1339. [Google Scholar] [CrossRef] [PubMed]
- Sabatine, M.S.; Cannon, C.P.; Gibson, C.M.; López-Sendón, J.L.; Montalescot, G.; Theroux, P.; Lewis, B.S.; Murphy, S.A.; McCabe, C.H.; Braunwald, E.; et al. Effect of Clopidogrel Pretreatment before Percutaneous Coronary Intervention in Patients with ST-Elevation Myocardial Infarction Treated with Fibrinolytics: The PCI-CLARITY Study. JAMA 2005, 294, 1224–1232. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Zhao, F.; Mehta, S.R.; Chrolavicius, S.; Tognoni, G.; Fox, K.K. Clopidogrel in Unstable Angina to Prevent Recurrent Events Trial Investigators Effects of Clopidogrel in Addition to Aspirin in Patients with Acute Coronary Syndromes without ST-Segment Elevation. N. Engl. J. Med. 2001, 345, 494–502. [Google Scholar] [CrossRef]
- Gibson, C.M.; Mehran, R.; Bode, C.; Halperin, J.; Verheugt, F.W.; Wildgoose, P.; Birmingham, M.; Ianus, J.; Burton, P.; van Eickels, M.; et al. Prevention of Bleeding in Patients with Atrial Fibrillation Undergoing PCI. N. Engl. J. Med. 2016, 375, 2423–2434. [Google Scholar] [CrossRef]
- Lopes, R.D.; Heizer, G.; Aronson, R.; Vora, A.N.; Massaro, T.; Mehran, R.; Goodman, S.G.; Windecker, S.; Darius, H.; Li, J.; et al. Antithrombotic Therapy after Acute Coronary Syndrome or PCI in Atrial Fibrillation. N. Engl. J. Med. 2019, 380, 1509–1524. [Google Scholar] [CrossRef] [PubMed]
- Cannon, C.P.; Bhatt, D.L.; Oldgren, J.; Lip, G.Y.H.; Ellis, S.G.; Kimura, T.; Maeng, M.; Merkely, B.; Zeymer, U.; Gropper, S.; et al. Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation. N. Engl. J. Med. 2017, 377, 1513–1524. [Google Scholar] [CrossRef]
- Vranckx, P.; Valgimigli, M.; Eckardt, L.; Tijssen, J.; Lewalter, T.; Gargiulo, G.; Batushkin, V.; Campo, G.; Lysak, Z.; Vakaliuk, I.; et al. Edoxaban-Based versus Vitamin K Antagonist-Based Antithrombotic Regimen after Successful Coronary Stenting in Patients with Atrial Fibrillation (ENTRUST-AF PCI): A Randomised, Open-Label, Phase 3b Trial. Lancet 2019, 394, 1335–1343. [Google Scholar] [CrossRef] [PubMed]
- Brandt, J.T.; Payne, C.D.; Wiviott, S.D.; Weerakkody, G.; Farid, N.A.; Small, D.S.; Jakubowski, J.A.; Naganuma, H.; Winters, K.J. A Comparison of Prasugrel and Clopidogrel Loading Doses on Platelet Function: Magnitude of Platelet Inhibition Is Related to Active Metabolite Formation. Am. Heart J. 2007, 153, 66.e9–66.e16. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.-J.; Ardissino, D.; De Servi, S.; Murphy, S.A.; et al. Prasugrel versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef] [PubMed]
- Erlinge, D.; Gurbel, P.A.; James, S.; Lindahl, T.L.; Svensson, P.; Ten Berg, J.M.; Foley, D.P.; Wagner, H.; Brown, P.B.; Luo, J.; et al. Prasugrel 5 Mg in the Very Elderly Attenuates Platelet Inhibition but Maintains Noninferiority to Prasugrel 10 Mg in Nonelderly Patients: The GENERATIONS Trial, a Pharmacodynamic and Pharmacokinetic Study in Stable Coronary Artery Disease Patients. J. Am. Coll. Cardiol. 2013, 62, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Erlinge, D.; Ten Berg, J.; Foley, D.; Angiolillo, D.J.; Wagner, H.; Brown, P.B.; Zhou, C.; Luo, J.; Jakubowski, J.A.; Moser, B.; et al. Reduction in Platelet Reactivity with Prasugrel 5 Mg in Low-Body-Weight Patients Is Noninferior to Prasugrel 10 Mg in Higher-Body-Weight Patients: Results from the FEATHER Trial. J. Am. Coll. Cardiol. 2012, 60, 2032–2040. [Google Scholar] [CrossRef] [PubMed]
- Roe, M.T.; Armstrong, P.W.; Fox, K.A.A.; White, H.D.; Prabhakaran, D.; Goodman, S.G.; Cornel, J.H.; Bhatt, D.L.; Clemmensen, P.; Martinez, F.; et al. Prasugrel versus Clopidogrel for Acute Coronary Syndromes without Revascularization. N. Engl. J. Med. 2012, 367, 1297–1309. [Google Scholar] [CrossRef] [PubMed]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef]
- Choi, Y.; Kang, D.-Y.; Lee, J.; Lee, J.; Kim, M.; Kim, H.; Park, J.; Cho, S.; Lee, J.; Cha, S.J.; et al. Ticagrelor Versus Clopidogrel in East Asian Patients with Acute Coronary Syndrome and Diabetes Mellitus. JACC Asia 2022, 2, 666–674. [Google Scholar] [CrossRef]
- Bianco, M.; Careggio, A.; Biolè, C.A.; Quadri, G.; Quiros, A.; Raposeiras-Roubin, S.; Abu-Assi, E.; Kinnaird, T.; Ariza-Solè, A.; Liebetrau, C.; et al. Ticagrelor or Clopidogrel after an Acute Coronary Syndrome in the Elderly: A Propensity Score Matching Analysis from 16,653 Patients Treated with PCI Included in Two Large Multinational Registries. Cardiovasc. Drugs Ther. 2021, 35, 1171–1182. [Google Scholar] [CrossRef] [PubMed]
- Bianco, M.; Mottola, F.F.; Cerrato, E.; Giordana, F.; Cinconze, S.; Baralis, G.; Verra, A.; Musumeci, G.; Rossini, R. Acute Coronary Syndrome in Very Elderly Patients-a Real-World Experience. Heart Vessel. 2023, 38, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Gimbel, M.; Qaderdan, K.; Willemsen, L.; Hermanides, R.; Bergmeijer, T.; de Vrey, E.; Heestermans, T.; Tjon Joe Gin, M.; Waalewijn, R.; Hofma, S.; et al. Clopidogrel versus Ticagrelor or Prasugrel in Patients Aged 70 Years or Older with Non-ST-Elevation Acute Coronary Syndrome (POPular AGE): The Randomised, Open-Label, Non-Inferiority Trial. Lancet 2020, 395, 1374–1381. [Google Scholar] [CrossRef] [PubMed]
- Mauri, L.; Kereiakes, D.J.; Yeh, R.W.; Driscoll-Shempp, P.; Cutlip, D.E.; Steg, P.G.; Normand, S.-L.T.; Braunwald, E.; Wiviott, S.D.; Cohen, D.J.; et al. Twelve or 30 Months of Dual Antiplatelet Therapy after Drug-Eluting Stents. N. Engl. J. Med. 2014, 371, 2155–2166. [Google Scholar] [CrossRef] [PubMed]
- Bonaca, M.P.; Braunwald, E.; Sabatine, M.S. Long-Term Use of Ticagrelor in Patients with Prior Myocardial Infarction. N. Engl. J. Med. 2015, 373, 1274–1275. [Google Scholar] [CrossRef] [PubMed]
- Angiolillo, D.J. Dual Antiplatelet Therapy Guided by Platelet Function Testing. Lancet 2017, 390, 1718–1720. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Lincoff, A.M.; Gibson, C.M.; Stone, G.W.; McNulty, S.; Montalescot, G.; Kleiman, N.S.; Goodman, S.G.; White, H.D.; Mahaffey, K.W.; et al. Intravenous Platelet Blockade with Cangrelor during PCI. N. Engl. J. Med. 2009, 361, 2330–2341. [Google Scholar] [CrossRef]
- Harrington, R.A.; Stone, G.W.; McNulty, S.; White, H.D.; Lincoff, A.M.; Gibson, C.M.; Pollack, C.V.; Montalescot, G.; Mahaffey, K.W.; Kleiman, N.S.; et al. Platelet Inhibition with Cangrelor in Patients Undergoing PCI. N. Engl. J. Med. 2009, 361, 2318–2329. [Google Scholar] [CrossRef] [PubMed]
- Steg, P.G.; Bhatt, D.L.; Hamm, C.W.; Stone, G.W.; Gibson, C.M.; Mahaffey, K.W.; Leonardi, S.; Liu, T.; Skerjanec, S.; Day, J.R.; et al. Effect of Cangrelor on Periprocedural Outcomes in Percutaneous Coronary Interventions: A Pooled Analysis of Patient-Level Data. Lancet 2013, 382, 1981–1992. [Google Scholar] [CrossRef]
- Halvorsen, S.; Mehilli, J.; Cassese, S.; Hall, T.S.; Abdelhamid, M.; Barbato, E.; De Hert, S.; de Laval, I.; Geisler, T.; Hinterbuchner, L.; et al. 2022 ESC Guidelines on Cardiovascular Assessment and Management of Patients Undergoing Non-Cardiac Surgery. Eur. Heart J. 2022, 43, 3826–3924. [Google Scholar] [CrossRef]
- Angiolillo, D.J.; Rollini, F.; Storey, R.F.; Bhatt, D.L.; James, S.; Schneider, D.J.; Sibbing, D.; So, D.Y.F.; Trenk, D.; Alexopoulos, D.; et al. International Expert Consensus on Switching Platelet P2Y12 Receptor-Inhibiting Therapies. Circulation 2017, 136, 1955–1975. [Google Scholar] [CrossRef] [PubMed]
- Schüpke, S.; Neumann, F.-J.; Menichelli, M.; Mayer, K.; Bernlochner, I.; Wöhrle, J.; Richardt, G.; Liebetrau, C.; Witzenbichler, B.; Antoniucci, D.; et al. Ticagrelor or Prasugrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2019, 381, 1524–1534. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D.; Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction; Katus, H.A.; Lindahl, B.; Morrow, D.A.; et al. Third Universal Definition of Myocardial Infarction. Circulation 2012, 126, 2020–2035. [Google Scholar] [CrossRef] [PubMed]
- Navarese, E.P.; Khan, S.U.; Kołodziejczak, M.; Kubica, J.; Buccheri, S.; Cannon, C.P.; Gurbel, P.A.; De Servi, S.; Budaj, A.; Bartorelli, A.; et al. Comparative Efficacy and Safety of Oral P2Y12 Inhibitors in Acute Coronary Syndrome: Network Meta-Analysis of 52,816 Patients from 12 Randomized Trials. Circulation 2020, 142, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Omerovic, E.; Erlinge, D.; Koul, S.; Frobert, O.; Andersson, J.; Ponten, J.; Björklund, F.; Kastberg, R.; Petzold, M.; Ljungman, C.; et al. Rationale and Design of Switch Swedeheart: A Registry-Based, Stepped-Wedge, Cluster-Randomized, Open-Label Multicenter Trial to Compare Prasugrel and Ticagrelor for Treatment of Patients with Acute Coronary Syndrome. Am. Heart J. 2022, 251, 70–77. [Google Scholar] [CrossRef]
- Montalescot, G.; van’t Hof, A.W. Prehospital Ticagrelor in ST-Segment Elevation Myocardial Infarction. N. Engl. J. Med. 2014, 371, 2339. [Google Scholar] [CrossRef] [PubMed]
- Montalescot, G.; Bolognese, L.; Dudek, D.; Goldstein, P.; Hamm, C.; Tanguay, J.-F.; ten Berg, J.M.; Miller, D.L.; Costigan, T.M.; Goedicke, J.; et al. Pretreatment with Prasugrel in Non-ST-Segment Elevation Acute Coronary Syndromes. N. Engl. J. Med. 2013, 369, 999–1010. [Google Scholar] [CrossRef]
- Watanabe, H.; Domei, T.; Morimoto, T.; Natsuaki, M.; Shiomi, H.; Toyota, T.; Ohya, M.; Suwa, S.; Takagi, K.; Nanasato, M.; et al. Effect of 1-Month Dual Antiplatelet Therapy Followed by Clopidogrel vs. 12-Month Dual Antiplatelet Therapy on Cardiovascular and Bleeding Events in Patients Receiving PCI: The STOPDAPT-2 Randomized Clinical Trial. JAMA 2019, 321, 2414–2427. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, H.; Morimoto, T.; Natsuaki, M.; Yamamoto, K.; Obayashi, Y.; Ogita, M.; Suwa, S.; Isawa, T.; Domei, T.; Yamaji, K.; et al. Comparison of Clopidogrel Monotherapy After 1 to 2 Months of Dual Antiplatelet Therapy with 12 Months of Dual Antiplatelet Therapy in Patients with Acute Coronary Syndrome: The STOPDAPT-2 ACS Randomized Clinical Trial. JAMA Cardiol. 2022, 7, 407–417. [Google Scholar] [CrossRef]
- De Luca, L.; D’Ascenzo, F.; Musumeci, G.; Saia, F.; Parodi, G.; Varbella, F.; Marchese, A.; De Servi, S.; Berti, S.; Bolognese, L. Incidence and Outcome of Switching of Oral Platelet P2Y12 Receptor Inhibitors in Patients with Acute Coronary Syndromes Undergoing Percutaneous Coronary Intervention: The SCOPE Registry. EuroIntervention 2017, 13, 459–466. [Google Scholar] [CrossRef]
- Zettler, M.E.; Peterson, E.D.; McCoy, L.A.; Effron, M.B.; Anstrom, K.J.; Henry, T.D.; Baker, B.A.; Messenger, J.C.; Cohen, D.J.; Wang, T.Y.; et al. Switching of Adenosine Diphosphate Receptor Inhibitor after Hospital Discharge among Myocardial Infarction Patients: Insights from the Treatment with Adenosine Diphosphate Receptor Inhibitors: Longitudinal Assessment of Treatment Patterns and Events after Acute Coronary Syndrome (TRANSLATE-ACS) Observational Study. Am. Heart J. 2017, 183, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Sibbing, D.; Aradi, D.; Jacobshagen, C.; Gross, L.; Trenk, D.; Geisler, T.; Orban, M.; Hadamitzky, M.; Merkely, B.; Kiss, R.G.; et al. Guided De-Escalation of Antiplatelet Treatment in Patients with Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention (TROPICAL-ACS): A Randomised, Open-Label, Multicentre Trial. Lancet 2017, 390, 1747–1757. [Google Scholar] [CrossRef] [PubMed]
- Price, M.J.; Berger, P.B.; Teirstein, P.S.; Tanguay, J.-F.; Angiolillo, D.J.; Spriggs, D.; Puri, S.; Robbins, M.; Garratt, K.N.; Bertrand, O.F.; et al. Standard- vs. High-Dose Clopidogrel Based on Platelet Function Testing after Percutaneous Coronary Intervention: The GRAVITAS Randomized Trial. JAMA 2011, 305, 1097–1105. [Google Scholar] [CrossRef] [PubMed]
- Tousek, P.; Osmancik, P.; Paulu, P.; Kocka, V.; Widimsky, P. Clopidogrel Up-Titration versus Standard Dose in Patients with High Residual Platelet Reactivity after Percutaneous Coronary Intervention: A Single-Center Pilot Randomised Study. Int. J. Cardiol. 2011, 150, 231–232. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhang, D.; Zhuang, S.; Lai, Y. Modifying Clopidogrel Maintenance Doses According to Vasodilator-Stimulated Phosphoprotein Phosphorylation Index Improves Clinical Outcome in Patients with Clopidogrel Resistance. Clin. Cardiol. 2011, 34, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.-P.; Cayla, G.; Cuisset, T.; Elhadad, S.; Rangé, G.; Vicaut, E.; Montalescot, G. Randomized Comparison of Platelet Function Monitoring to Adjust Antiplatelet Therapy versus Standard of Care: Rationale and Design of the Assessment with a Double Randomization of (1) a Fixed Dose versus a Monitoring-Guided Dose of Aspirin and Clopidogrel after DES Implantation, and (2) Treatment Interruption versus Continuation, 1 Year after Stenting (ARCTIC) Study. Am. Heart J. 2011, 161, 5–12.e5. [Google Scholar] [CrossRef] [PubMed]
- Trenk, D.; Stone, G.W.; Gawaz, M.; Kastrati, A.; Angiolillo, D.J.; Müller, U.; Richardt, G.; Jakubowski, J.A.; Neumann, F.-J. A Randomized Trial of Prasugrel Versus Clopidogrel in Patients with High Platelet Reactivity on Clopidogrel after Elective Percutaneous Coronary Intervention with Implantation of Drug-Eluting Stents. J. Am. Coll. Cardiol. 2012, 59, 2159–2164. [Google Scholar] [CrossRef] [PubMed]
- Hazarbasanov, D.; Velchev, V.; Finkov, B.; Postadjian, A.; Kostov, E.; Rifai, N.; Aradi, D. Tailoring Clopidogrel Dose According to Multiple Electrode Aggregometry Decreases the Rate of Ischemic Complications after Percutaneous Coronary Intervention. J. Thromb. Thrombolysis 2012, 34, 85–90. [Google Scholar] [CrossRef]
- Aradi, D.; Rideg, O.; Vorobcsuk, A.; Magyarlaki, T.; Magyari, B.; Kónyi, A.; Pintér, T.; Horváth, I.G.; Komócsi, A. Justification of 150 Mg Clopidogrel in Patients with High On-clopidogrel Platelet Reactivity. Eur. J. Clin. Investig. 2012, 42, 384–392. [Google Scholar] [CrossRef]
- Ari, H.; Ozkan, H.; Karacinar, A.; Ari, S.; Koca, V.; Bozat, T. The EFFect of hIgh-Dose ClopIdogrel treatmENT in Patients with Clopidogrel Resistance (The EFFICIENT Trial). Int. J. Cardiol. 2012, 157, 374–380. [Google Scholar] [CrossRef]
- Xu, L.; Wang, L.; Yang, X.; Li, K.; Sun, H.; Zhang, D.; Wang, H.; Li, W.; Ni, Z.; Xia, K.; et al. Platelet Function Monitoring Guided Antiplatelet Therapy in Patients Receiving High-Risk Coronary Interventions. Chin. Med. J. 2014, 127, 3364–3370. [Google Scholar] [PubMed]
- Samardzic, J.; Krpan, M.; Skoric, B.; Pasalic, M.; Petricevic, M.; Milicic, D. Serial Clopidogrel Dose Adjustment after Platelet Function Testing Improves Outcome of Acute Coronary Syndrome Patients Undergoing Percutaneous Coronary Intervention with High On-Treatment Platelet Reactivity. J. Thromb. Thrombolysis 2014, 38, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.-C.; Li, Y.; Guan, S.-Y.; Li, J.; Wang, X.-Z.; Jing, Q.-M.; Wang, Z.-L.; Han, Y.-L. Efficacy and Safety of Individually Tailored Antiplatelet Therapy in Patients with Acute Coronary Syndrome after Coronary Stenting: A Single Center, Randomized, Feasibility Study. J. Geriatr. Cardiol. JGC 2015, 12, 23. [Google Scholar] [PubMed]
- Paarup Dridi, N.; Johansson, P.I.; Lønborg, J.T.; Clemmensen, P.; Radu, M.D.; Qayyum, A.; Pedersen, F.; Kollslid, R.; Helqvist, S.; Saunamäki, K.; et al. Tailored Antiplatelet Therapy to Improve Prognosis in Patients Exhibiting Clopidogrel Low-Response Prior to Percutaneous Coronary Intervention for Stable Angina or Non-ST Elevation Acute Coronary Syndrome. Platelets 2015, 26, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Siller-Matula, J.M.; Gruber, C.; Francesconi, M.; Dechant, C.; Jilma, B.; Delle-Karth, G.; Grohs, K.; Podczeck-Schweighofer, A.; Christ, G. The Net Clinical Benefit of Personalized Antiplatelet Therapy in Patients Undergoing Percutaneous Coronary Intervention. Clin. Sci. 2015, 128, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Cayla, G.; Cuisset, T.; Silvain, J.; Leclercq, F.; Manzo-Silberman, S.; Saint-Etienne, C.; Delarche, N.; Bellemain-Appaix, A.; Range, G.; El Mahmoud, R.; et al. Platelet Function Monitoring to Adjust Antiplatelet Therapy in Elderly Patients Stented for an Acute Coronary Syndrome (ANTARCTIC): An Open-Label, Blinded-Endpoint, Randomised Controlled Superiority Trial. Lancet 2016, 388, 2015–2022. [Google Scholar] [CrossRef]
- Mikkelsson, J.; Paana, T.; Lepantalo, A.; Karjalainen, P.P. Personalized ADP-Receptor Inhibition Strategy and Outcomes Following Primary PCI for STEMI (PASTOR Study). Int. J. Cardiol. 2016, 202, 463–466. [Google Scholar] [CrossRef] [PubMed]
- Bagai, A.; Peterson, E.D.; McCoy, L.A.; Effron, M.B.; Zettler, M.E.; Stone, G.W.; Henry, T.D.; Cohen, D.J.; Schulte, P.J.; Anstrom, K.J.; et al. Association of Measured Platelet Reactivity with Changes in P2Y 12 Receptor Inhibitor Therapy and Outcomes after Myocardial Infarction: Insights into Routine Clinical Practice from the TReatment with ADP Receptor iNhibitorS: Longitudinal Assessment of Treatment Patterns and Events after Acute Coronary Syndrome (TRANSLATE-ACS) Study. Am. Heart J. 2017, 187, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Komócsi, A.; Merkely, B.; Hadamitzky, M.; Massberg, S.; Rizas, K.D.; Hein-Rothweiler, R.; Gross, L.; Trenk, D.; Sibbing, D.; Aradi, D. Impact of Body Mass on P2Y12-Inhibitor de-Escalation in Acute Coronary Syndromes—A Substudy of the TROPICAL-ACS Trial. Eur. Heart J. Cardiovasc. Pharmacother. 2023, 9, 608–616. [Google Scholar] [CrossRef]
- Zheng, Y.-Y.; Wu, T.-T.; Yang, Y.; Hou, X.-G.; Gao, Y.; Chen, Y.; Yang, Y.-N.; Li, X.-M.; Ma, X.; Ma, Y.-T.; et al. Personalized Antiplatelet Therapy Guided by a Novel Detection of Platelet Aggregation Function in Stable Coronary Artery Disease Patients Undergoing Percutaneous Coronary Intervention: A Randomized Controlled Clinical Trial. Eur. Heart J. Cardiovasc. Pharmacother. 2020, 6, 211–221. [Google Scholar] [CrossRef]
- Mshelbwala, F.S.; Hugenberg, D.W.; Kreutz, R.P. Intensified P2Y12 Inhibition for High-on Treatment Platelet Reactivity. J. Thromb. Thrombolysis 2020, 50, 619–627. [Google Scholar] [CrossRef] [PubMed]
- You, J.; Li, H.; Guo, W.; Li, J.; Gao, L.; Wang, Y.; Geng, L.; Wang, X.; Wan, Q.; Zhang, Q. Platelet Function Testing Guided Antiplatelet Therapy Reduces Cardiovascular Events in Chinese Patients with ST-segment Elevation Myocardial Infarction Undergoing Percutaneous Coronary Intervention: The PATROL Study. Catheter. Cardiovasc. Interv. 2020, 95, 598–605. [Google Scholar] [CrossRef]
- Zheng, Y.-Y.; Wu, T.-T.; Yang, Y.; Hou, X.-G.; Chen, Y.; Ma, X.; Ma, Y.-T.; Zhang, J.-Y.; Xie, X. Diabetes and Outcomes Following Personalized Antiplatelet Therapy in Coronary Artery Disease Patients Who Have Undergone PCI. J. Clin. Endocrinol. Metab. 2022, 107, e214–e223. [Google Scholar] [CrossRef] [PubMed]
- Ammirabile, N.; Landolina, D.; Capodanno, D. Navigating the Course of Dual Antiplatelet Therapy after Percutaneous Coronary Intervention: A Review of Guided Approaches. Circ. Cardiovasc. Interv. 2023, 16, e013450. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Wang, Y.; Wu, Y.; Huang, C.; Yan, H.; Zhu, W.; Xu, W.; Zhang, L.; Zhu, J. Individualized Dual Antiplatelet Therapy Based on Platelet Function Testing in Patients Undergoing Percutaneous Coronary Intervention: A Meta-Analysis of Randomized Controlled Trials. BMC Cardiovasc. Disord. 2017, 17, 157. [Google Scholar] [CrossRef] [PubMed]
- Lyu, S.-Q.; Yang, Y.-M.; Zhu, J.; Wang, J.; Wu, S.; Zhang, H.; Shao, X.-H.; Ren, J.-M. The Efficacy and Safety of CYP2C19 Genotype-Guided Antiplatelet Therapy Compared with Conventional Antiplatelet Therapy in Patients with Acute Coronary Syndrome or Undergoing Percutaneous Coronary Intervention: A Meta-Analysis of Randomized Controlled Trials. Platelets 2020, 31, 971–980. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Zhao Li, Y.; Wu, H.; Zhou, G.; Yang, J.; Yang, J.; Ding, J.W.; Fan, Z.X.; Yang, C.J. Efficacy and Safety of Genotype-Guided Antiplatelet Therapy versus Standard Treatment in 4,604 Patients with CAD after PCI: A Meta-Analysis of Randomized Controlled Trials. Pharmazie 2020, 75, 651–655. [Google Scholar] [CrossRef] [PubMed]
- Tang, B.; Wang, X.; Wang, X.; Liu, L.; Ma, Z. Genotype-Guided Antiplatelet Therapy Versus Standard Therapy for Patients with Coronary Artery Disease: An Updated Systematic Review and Meta-Analysis. J. Pharm. Pharm. Sci. 2022, 25, 9–23. [Google Scholar] [CrossRef] [PubMed]
- Galli, M.; Benenati, S.; Capodanno, D.; Franchi, F.; Rollini, F.; D’Amario, D.; Porto, I.; Angiolillo, D.J. Guided versus Standard Antiplatelet Therapy in Patients Undergoing Percutaneous Coronary Intervention: A Systematic Review and Meta-Analysis. Lancet 2021, 397, 1470–1483. [Google Scholar] [CrossRef]
- Galli, M.; Benenati, S.; Franchi, F.; Rollini, F.; Capodanno, D.; Biondi-Zoccai, G.; Vescovo, G.M.; Cavallari, L.H.; Bikdeli, B.; Ten Berg, J.; et al. Comparative Effects of Guided vs. Potent P2Y12 Inhibitor Therapy in Acute Coronary Syndrome: A Network Meta-Analysis of 61,898 Patients from 15 Randomized Trials. Eur. Heart J. 2022, 43, 959–967. [Google Scholar] [CrossRef]
- Tavenier, A.H.; Mehran, R.; Chiarito, M.; Cao, D.; Pivato, C.A.; Nicolas, J.; Beerkens, F.; Nardin, M.; Sartori, S.; Baber, U.; et al. Guided and Unguided De-Escalation from Potent P2Y12 Inhibitors among Patients with Acute Coronary Syndrome: A Meta-Analysis. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 8, 492–502. [Google Scholar] [CrossRef] [PubMed]
- Kuno, T.; Fujisaki, T.; Shoji, S.; Sahashi, Y.; Tsugawa, Y.; Iwagami, M.; Takagi, H.; Briasoulis, A.; Deharo, P.; Cuisset, T.; et al. Comparison of Unguided De-Escalation versus Guided Selection of Dual Antiplatelet Therapy after Acute Coronary Syndrome: A Systematic Review and Network Meta-Analysis. Circ. Cardiovasc. Interv. 2022, 15, e011990. [Google Scholar] [CrossRef] [PubMed]
- Birocchi, S.; Rocchetti, M.; Minardi, A.; Podda, G.M.; Squizzato, A.; Cattaneo, M. Guided Anti-P2Y12 Therapy in Patients Undergoing PCI: Three Systematic Reviews with Meta-Analyses of Randomized Controlled Trials with Homogeneous Design. Thromb. Haemost. 2023. [Google Scholar] [CrossRef] [PubMed]
- Aluvilu, A.; Ferro, A. Role of Platelet Function Testing in Acute Coronary Syndromes: A Meta-Analysis. Open Heart 2022, 9, e002129. [Google Scholar] [CrossRef]
- Sibbing, D.; Aradi, D.; Alexopoulos, D.; Ten Berg, J.; Bhatt, D.L.; Bonello, L.; Collet, J.-P.; Cuisset, T.; Franchi, F.; Gross, L.; et al. Updated Expert Consensus Statement on Platelet Function and Genetic Testing for Guiding P2Y12 Receptor Inhibitor Treatment in Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2019, 12, 1521–1537. [Google Scholar] [CrossRef] [PubMed]
- Claassens, D.M.F.; Vos, G.J.A.; Bergmeijer, T.O.; Hermanides, R.S.; van’t Hof, A.W.J.; van der Harst, P.; Barbato, E.; Morisco, C.; Tjon Joe Gin, R.M.; Asselbergs, F.W.; et al. A Genotype-Guided Strategy for Oral P2Y12 Inhibitors in Primary PCI. N. Engl. J. Med. 2019, 381, 1621–1631. [Google Scholar] [CrossRef] [PubMed]
- Fontana, P.; Cattaneo, M.; Combescure, C.; Reny, J.-L. Tailored Thienopyridine Therapy: No Urgency for CYP2C19 Genotyping. J. Am. Heart Assoc. 2013, 2, e000131. [Google Scholar] [CrossRef] [PubMed]
- Cuisset, T.; Deharo, P.; Quilici, J.; Johnson, T.W.; Deffarges, S.; Bassez, C.; Bonnet, G.; Fourcade, L.; Mouret, J.P.; Lambert, M.; et al. Benefit of Switching Dual Antiplatelet Therapy after Acute Coronary Syndrome: The TOPIC (Timing of Platelet Inhibition after Acute Coronary Syndrome) Randomized Study. Eur. Heart J. 2017, 38, 3070–3078. [Google Scholar] [CrossRef]
- Kim, C.J.; Park, M.-W.; Kim, M.C.; Choo, E.-H.; Hwang, B.-H.; Lee, K.Y.; Choi, Y.S.; Kim, H.-Y.; Yoo, K.-D.; Jeon, D.-S.; et al. Unguided De-Escalation from Ticagrelor to Clopidogrel in Stabilised Patients with Acute Myocardial Infarction Undergoing Percutaneous Coronary Intervention (TALOS-AMI): An Investigator-Initiated, Open-Label, Multicentre, Non-Inferiority, Randomised Trial. Lancet 2021, 398, 1305–1316. [Google Scholar] [CrossRef]
- Kim, H.-S.; Kang, J.; Hwang, D.; Han, J.-K.; Yang, H.-M.; Kang, H.-J.; Koo, B.-K.; Rhew, J.Y.; Chun, K.-J.; Lim, Y.-H.; et al. Prasugrel-Based de-Escalation of Dual Antiplatelet Therapy after Percutaneous Coronary Intervention in Patients with Acute Coronary Syndrome (HOST-REDUCE-POLYTECH-ACS): An Open-Label, Multicentre, Non-Inferiority Randomised Trial. Lancet 2020, 396, 1079–1089. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Acetylsalicylic Acid (ASA) | Clopidogrel | Prasugrel | Ticagrelor | Cangrelor | |
|---|---|---|---|---|---|
| Mechanism of Action | Inhibition of prostaglandin synthesis and TxA2-mediated platelet aggregation | Irreversible inhibition of P2Y12 receptor | Irreversible inhibition of P2Y12 receptor | Reversible inhibition of P2Y12 receptor | Reversible inhibition of P2Y12 receptor |
| Roat of Administration | Oral | Oral | Oral | Oral | Intravenous |
| Recommended Dosage in ACS | 300–325 mg (loading dose) 75–100 mg Once daily | 300–600 mg (loading dose) 75 mg Once daily | 60 mg (loading dose) 10 mg (5 mg) Once daily | 180 mg (loading dose) 90 mg Twice daily | Bolus (30 µg/Kg) followed by Infusion (4 µg/Kg/min) for at least 2 h |
| Half-life | 20 min | ≈6 h | <5 min | 6–12 h | 3–6 min |
| CYP interaction | No | CYP2C19 | No | CYP3A | No |
| Side Effects |
|
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russo, I.; Brookles, C.G.; Barale, C.; Melchionda, E.; Mousavi, A.H.; Biolè, C.; Chinaglia, A.; Bianco, M. Current Strategies to Guide the Antiplatelet Therapy in Acute Coronary Syndromes. Int. J. Mol. Sci. 2024, 25, 3981. https://doi.org/10.3390/ijms25073981
Russo I, Brookles CG, Barale C, Melchionda E, Mousavi AH, Biolè C, Chinaglia A, Bianco M. Current Strategies to Guide the Antiplatelet Therapy in Acute Coronary Syndromes. International Journal of Molecular Sciences. 2024; 25(7):3981. https://doi.org/10.3390/ijms25073981
Chicago/Turabian StyleRusso, Isabella, Carola Griffith Brookles, Cristina Barale, Elena Melchionda, Amir Hassan Mousavi, Carloalberto Biolè, Alessandra Chinaglia, and Matteo Bianco. 2024. "Current Strategies to Guide the Antiplatelet Therapy in Acute Coronary Syndromes" International Journal of Molecular Sciences 25, no. 7: 3981. https://doi.org/10.3390/ijms25073981