
Recent Insights into the Measurement of Carbon Dioxide Concentrations for Clinical Practice in Respiratory Medicine

 , ,
, ,
Abstract
:1. Introduction
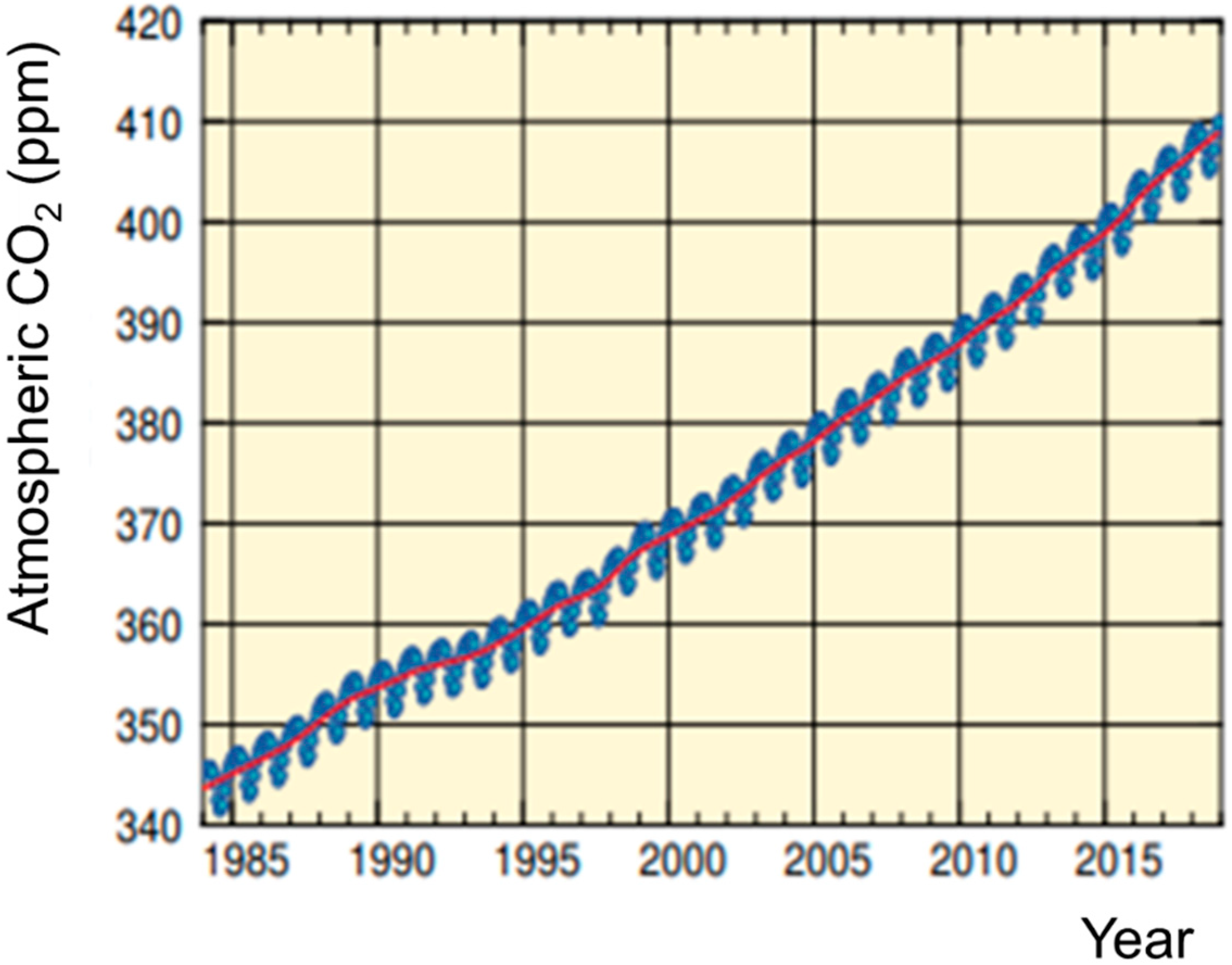
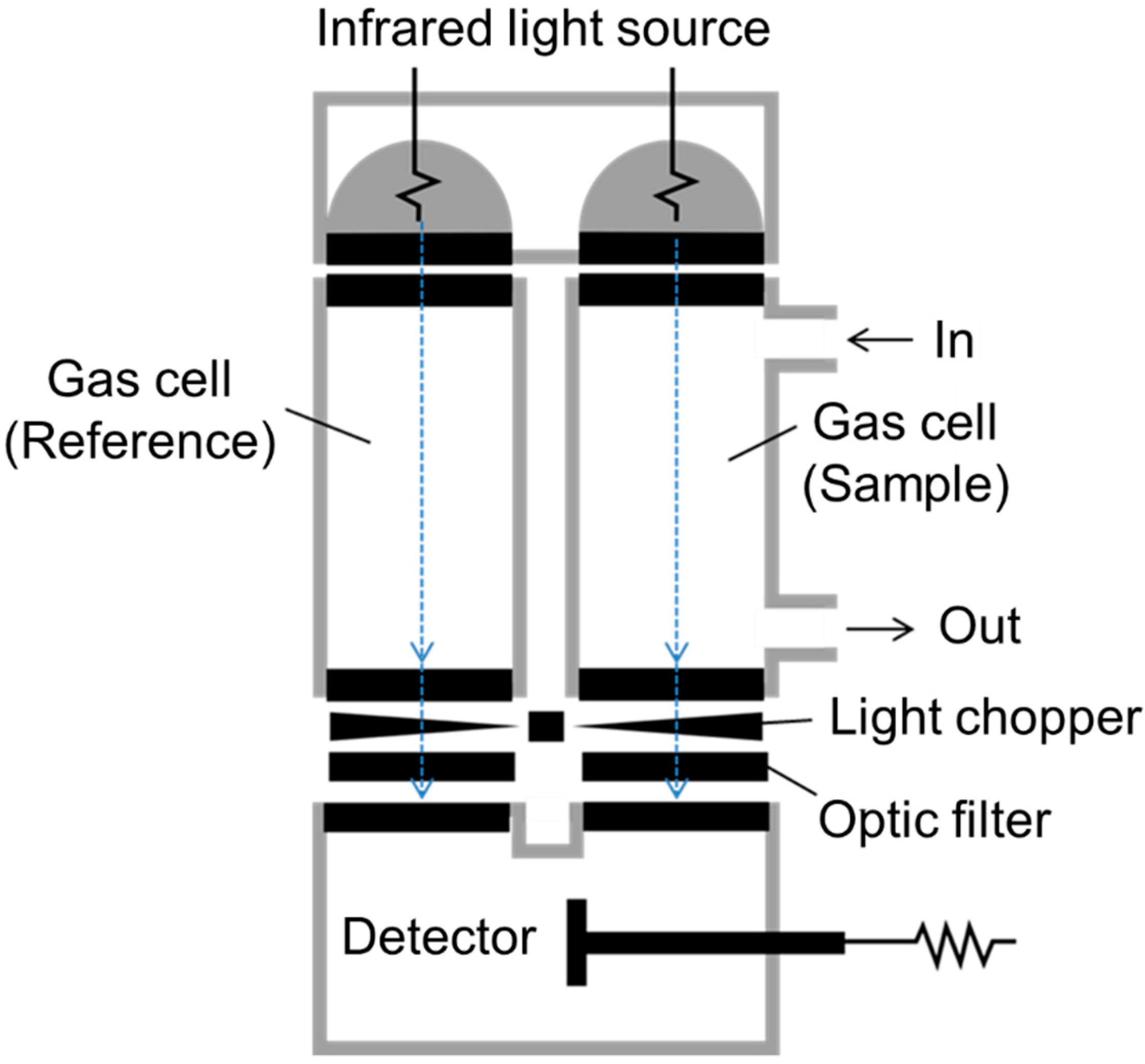
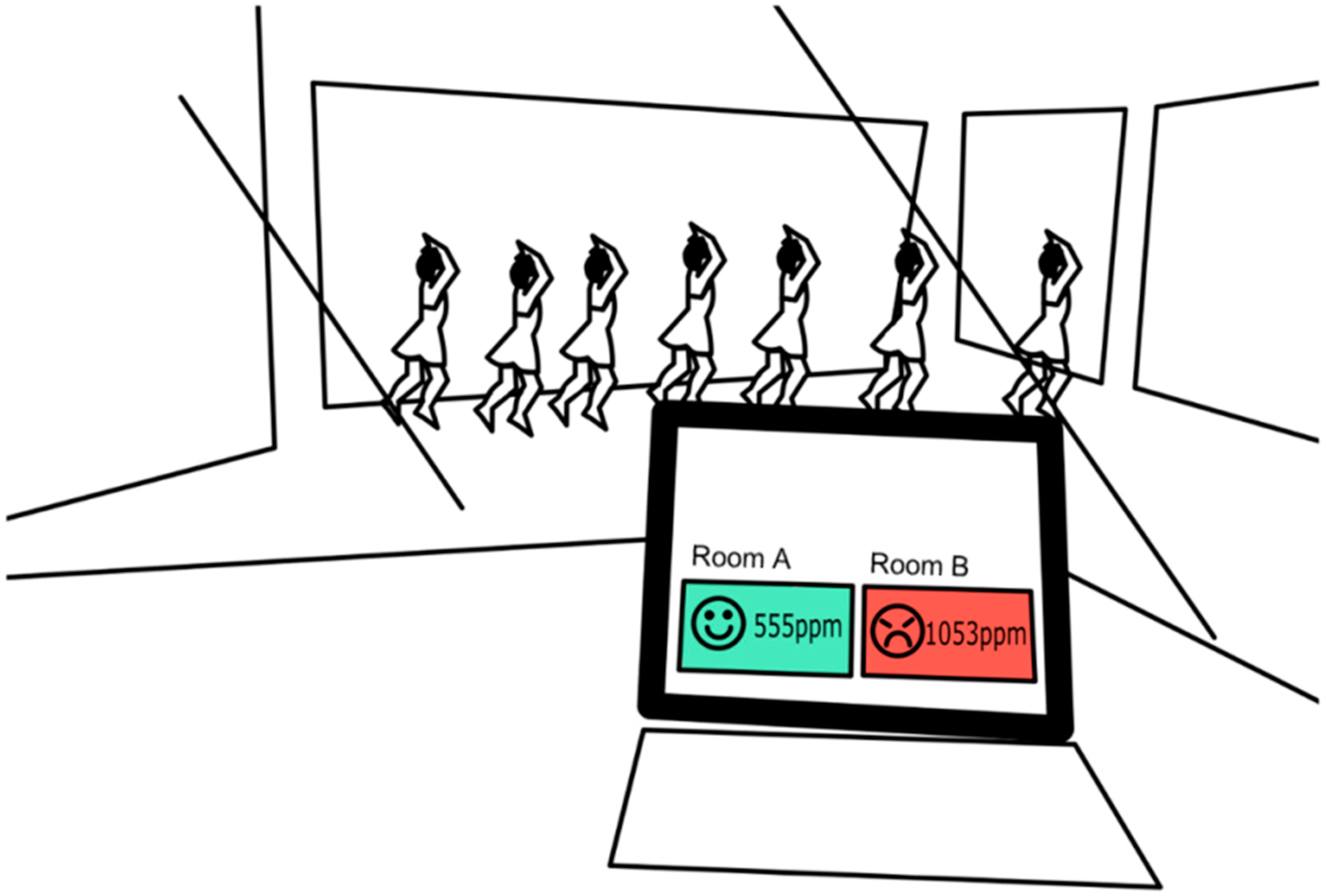
2. Atmospheric Carbon Dioxide Concentration
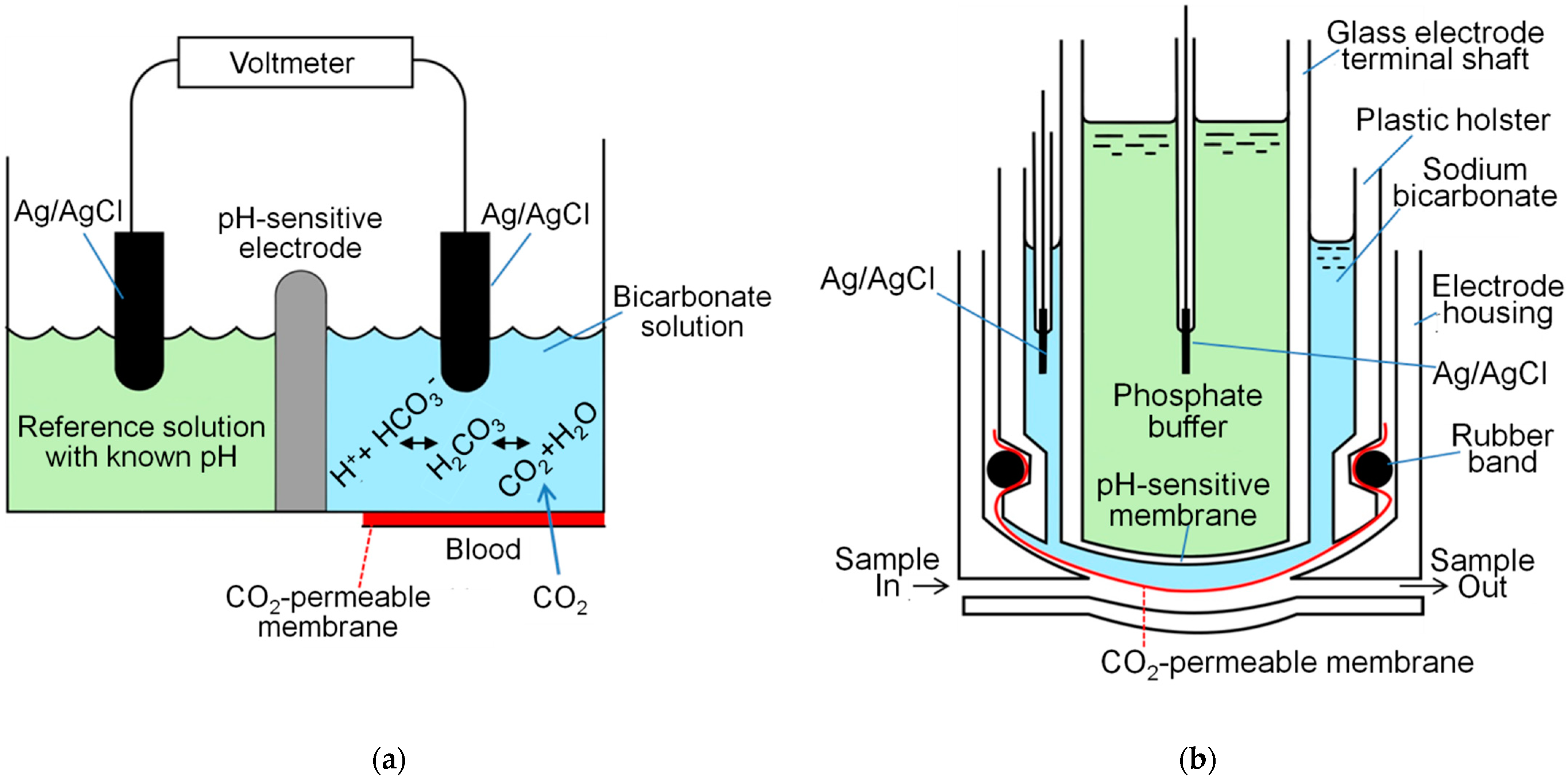
3. Blood Gas Analysis: Principle of PaCO2 Electrode
4. Non-Invasive Alternative Methods to Estimate PaCO2
4.1. Venous Blood Gas Analysis (VBGA)
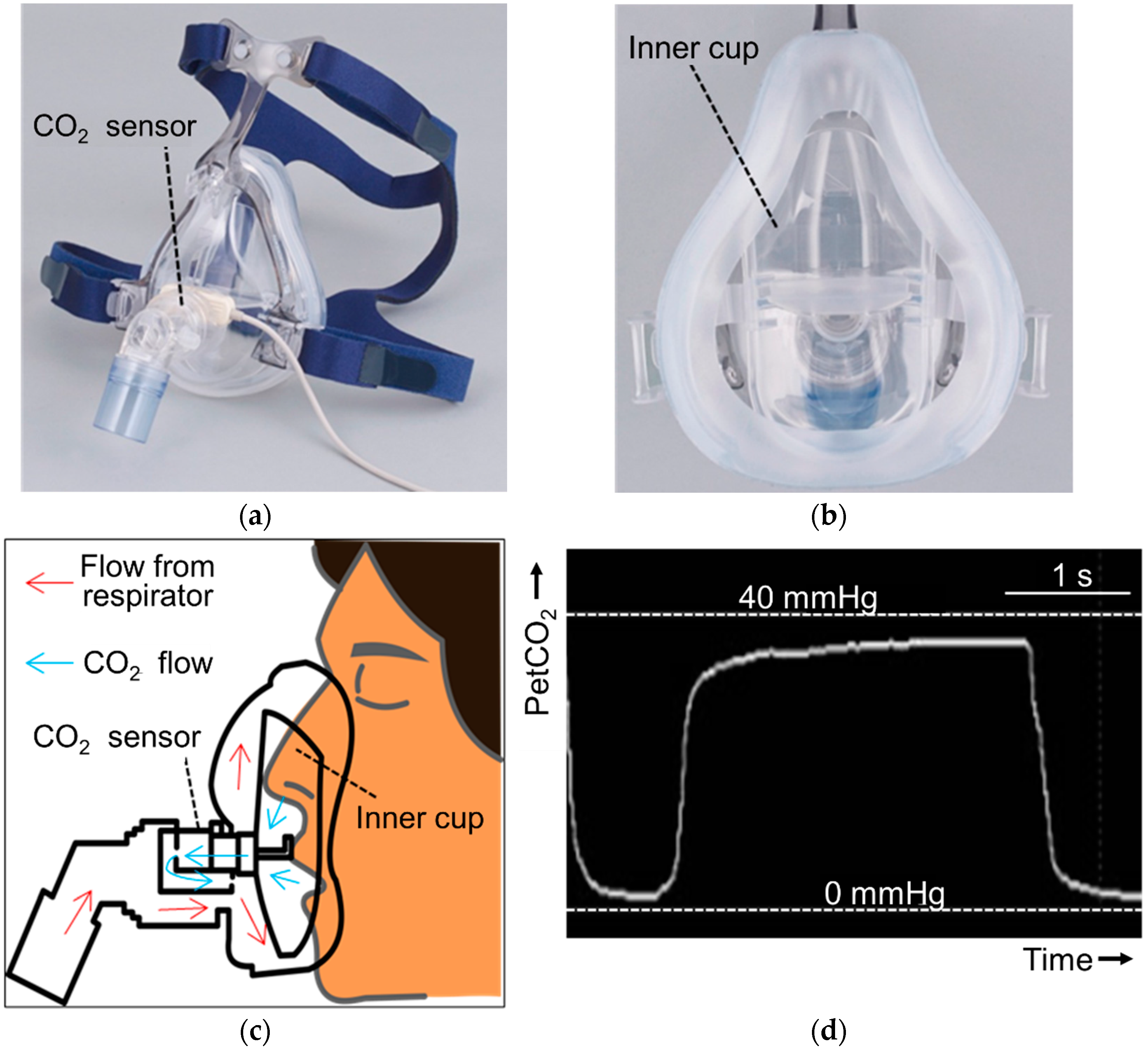
4.2. End-Tidal PCO2
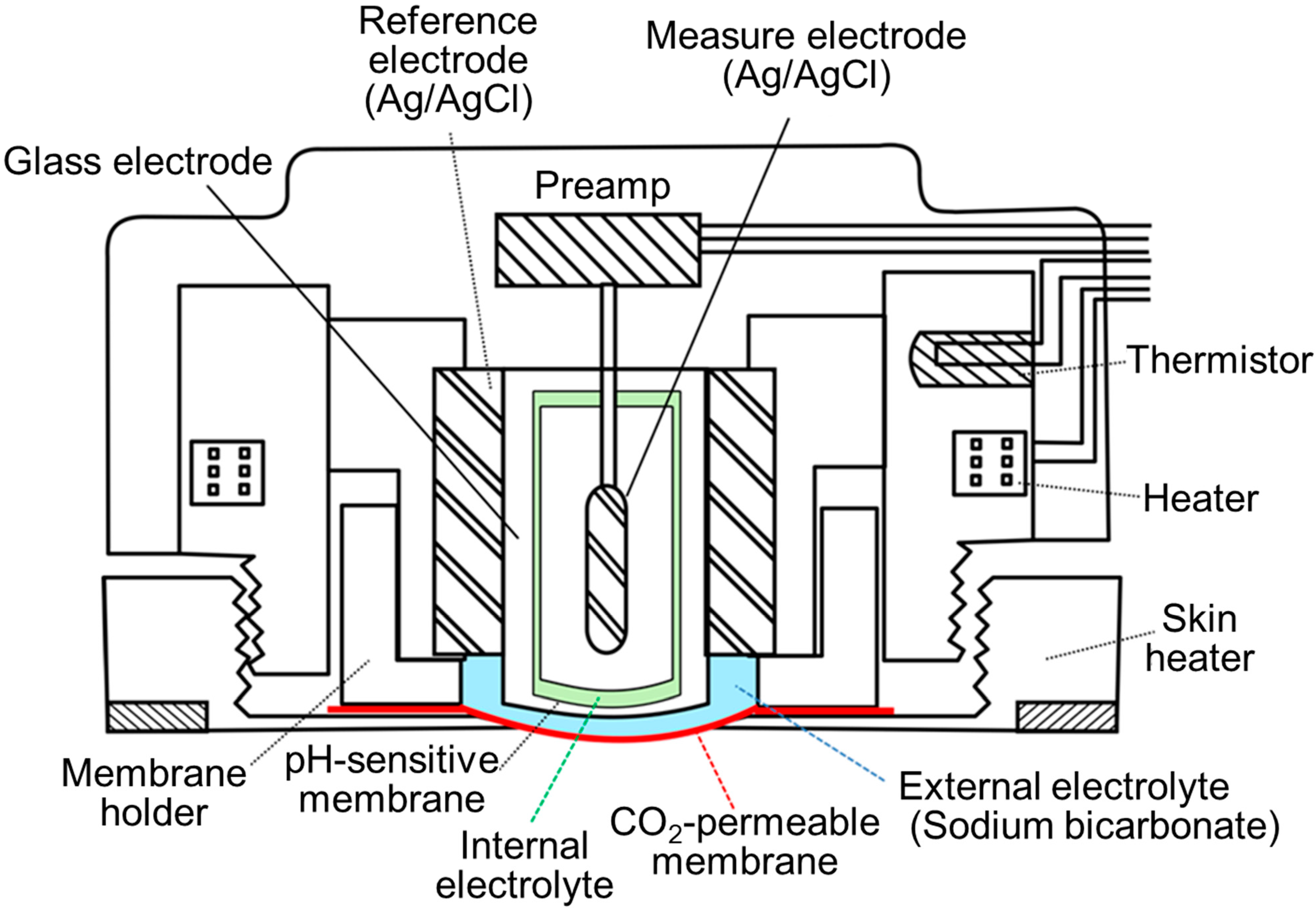
4.3. Transcutaneous Blood Gas Analysis
4.4. Comparison of Accuracy
5. Usefulness and limitation of Transcutaneous Blood Gas Analysis
5.1. Various Subgroup Analyses on the PtcCO2 Bias
5.1.1. Sex
5.1.2. Age
5.1.3. PaCO2 Level
5.1.4. PaO2 Level
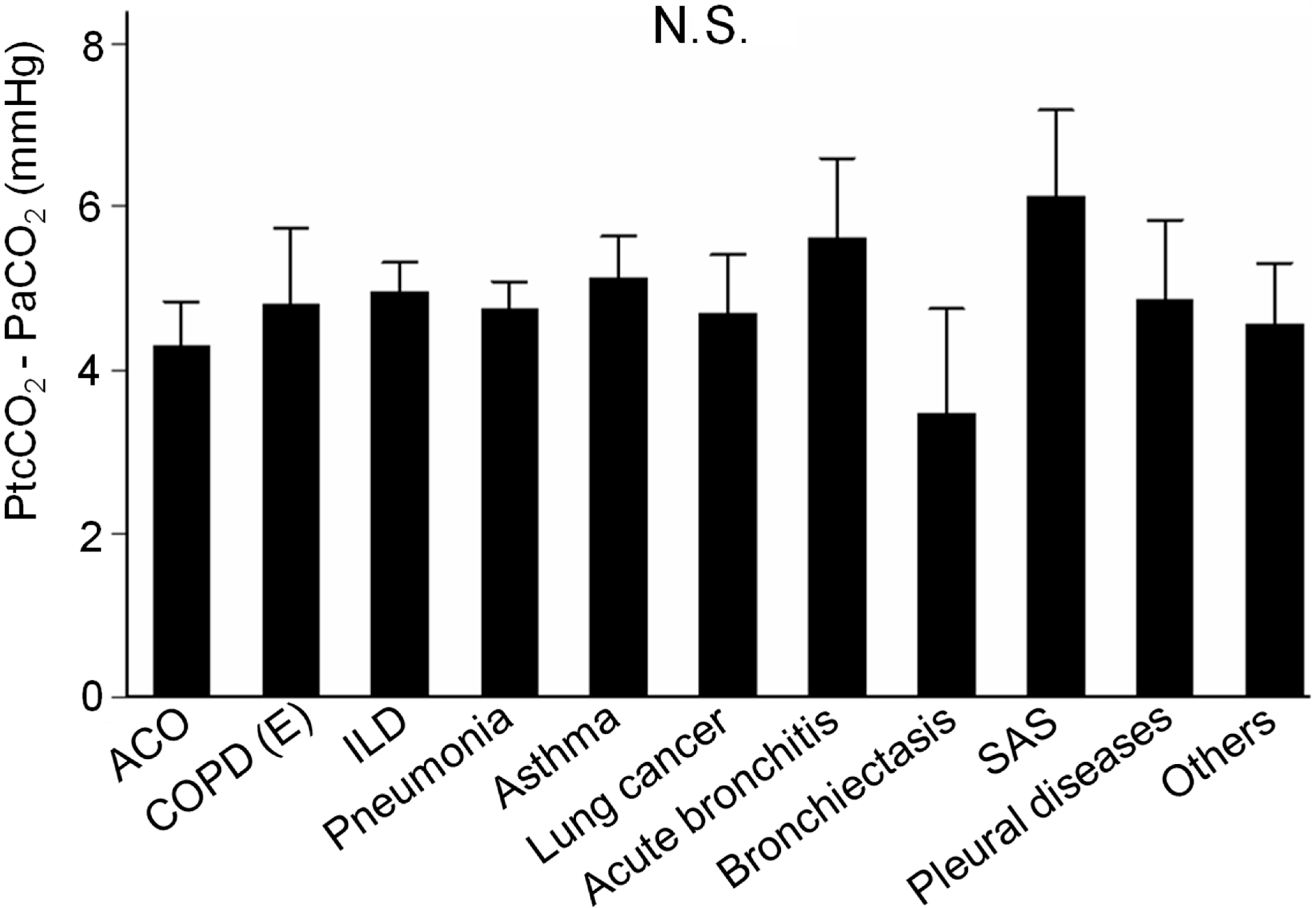
5.1.5. Among Various Respiratory Diseases
5.2. Usefulness
5.3. Limitations
5.4. Future Use
6. Other Applications of Measuring CO2 Mainly for Research Use
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ABGA | Arterial blood gas analysis |
| ACO | Asthma chronic obstructive pulmonary disease overlap |
| Ag/AgCl | Silver electrode plated with silver chloride |
| ANOVA | Analysis of variance |
| [Cl−] | Plasma chloride concentration |
| COPD | Chronic obstructive pulmonary disease |
| CO2 | Carbon dioxide |
| COVID-19 | Corona virus disease 2019 |
| CPAP | Continuous positive airway pressure |
| E | Emphysema |
| EE | Energy expenditure |
| H+ | Hydrogen ion |
| HCO3− | Bicarbonate ion |
| [HCO3−] | Bicarbonate concentration |
| H2CO3 | Carbonic acid |
| ILD | Interstitional lung disease |
| [Na+] | Plasma sodium concentration |
| NPPV | Non-invasive positive pressure ventilation |
| N.S. | Not significant |
| OSAS | Obstructive sleep apnea syndrome |
| O2 | Oxygen |
| PaCO2 | Arterial partial pressure of carbon dioxide |
| PaO2 | Arterial partial pressure of oxygen |
| PCO2 | Partial pressure of carbon dioxide |
| PetCO2 | End-tidal carbon dioxide partial pressure of exhaled gas |
| PO2 | Partial pressure of oxygen |
| PtcCO2 | Transcutaneous partial pressure of carbon dioxide |
| RQ | Respiratory quotient |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| SAS | Sleep apnea syndrome |
| SD | Standard deviation |
| SEM | Standard error of the mean |
| SpO2 | Percutaneous oxygen saturation |
| VBGA | Venous blood gas analysis |
| CO2 | Carbon dioxide production |
| O2 | Oxygen consumption |
| Ventilation/perfusion |
References
- Bernstein, A.S. Climate change and infectious disease. In Harrison’s Principles of Internal Medicine, 20th ed.; McGraw-Hill Education: New York, NY, USA, 2018; pp. 900–908. [Google Scholar]
- The World Data Centre for Greenhouse Gases. World Meteorological Organization. WMO WDCGG Data Summary. WDCGG No. 44. Available online: https://gaw.kishou.go.jp/publications/summary (accessed on 18 August 2021).
- Eliseeva, O.V. On the determination of maximum permissible carbon dioxide concentrations in the air of apartment buildings and public buildings. Gig Sanit. 1964, 29, 10–15. [Google Scholar]
- Goromosov, M.S. The Physiological Basis of Health Standards for Dwellings; Public Health Papers No. 33; World Health Organization: Geneva, Switzerland, 1968; Available online: https://apps.who.int/iris/handle/10665/39749 (accessed on 18 August 2021).
- Peng, Z.; Jimenez, J.L. Exhaled CO2 as COVID-19 infection risk proxy for different indoor environments and activities. Environ. Sci. Technol. Lett. 2021, 8, 392–397. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. For the China Novel Coronavirus investigating and research team. A novel coronavirus from patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Goyal, P.; Choi, J.J.; Pinheiro, L.C.; Schenck, E.J.; Chen, R.; Jabri, A.; Satlin, M.J.; Campion, T.R., Jr.; Nahid, M.; Ringel, J.B.; et al. Clinical characteristics of COVID-19 in New York City. N. Engl. J. Med. 2020, 382, 2372–2374. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, transmission, diagnosis and treatment of coronavirus disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Stoller, J.K.; Hill, N.S. Respiratory monitoring in critical care. In Goldman-Cecil Medicine, 26th ed.; Goldman, L., Schhafer, A.I., Eds.; Elsevier: Philadelphia, PA, USA, 2020; pp. 622–625. [Google Scholar]
- Matthay, M.A.; Ware, L.B. Acute respiratory failure. In Goldman-Cecil Medicine, 26th ed.; Goldman, L., Schhafer, A.I., Eds.; Elsevier: Philadelphia, PA, USA, 2020; pp. 625–635. [Google Scholar]
- Malley, W.J. Arterial blood gases. In Clinical Blood Gases: Assessment and Intervention, 2nd ed.; Elsevier Saunders: St. Louis, MO, USA; Elsevier: Philadelphia, PA, USA, 2005; pp. 3–34. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- West, J.B. Ventilation/Blood Flow and Gas Exchange, 4th ed.; Blackwell Scientific Publications: Oxford, UK, 1985. [Google Scholar]
- Tachikawa, R.; Ikeda, K.; Minami, T.; Matsumoto, T.; Hamada, S.; Murase, K.; Tanizawa, K.; Inouchi, M.; Oga, T.; Akamizu, T.; et al. Changes in energy metabolism after continuous positive airway pressure for obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 2016, 194, 729–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bate, G.C.; D’Aoust, A.; Canvin, D.T. Calibration of Infra-Red CO2 Gas Analyzers. Plant. Physiol. 1969, 44, 1122–1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramwell, P.W.; Dawson, J.B. The calibration of infra-red gas analysers for use in the estimation of carbon dioxide. Phys. Med. Biol. 1958, 2, 280–286. [Google Scholar] [CrossRef]
- Fowler, R.C. A rapid infra-red gas analyzer. Rev. Sci Instrum. 1949, 20, 175–178. [Google Scholar] [CrossRef]
- HORIBA, Ltd. NDIR: Non Dispersive Infrared. Available online: https://www.horiba.com/jp/scientific/core-technology/ndir/ (accessed on 9 May 2021).
- Permentier, K.; Vercammen, S.; Soetaert, S.; Schellemans, C. Carbon dioxide poisoning: A literature review of an often forgotten cause of intoxication in the emergency department. Int. J. Emerg. Med. 2017, 10, 14. [Google Scholar] [CrossRef] [PubMed]
- Duarte, C.M.; Jaremko, Ł.; Jaremko, M. Hypothesis: Potentially systemic impacts of elevated CO2 on the human proteome and health. Front. Public Health. 2020, 8, 543322. [Google Scholar] [CrossRef]
- Martin, A.K.T. Shut that window! Open that window! Coronavirus in winter presents new challenge. Japan Times, 28 December 2020. [Google Scholar]
- Gilio, A.D.; Palmisani, J.; Pulimeno, M.; Cerino, F.; Cacace, M.; Miani, A.; Gennaroa, G.D. CO2 concentration monitoring inside educational buildings as a strategic tool to reduce the risk of SARS-CoV-2 airborne transmission. Environ. Res. 2021, 202, 111560. [Google Scholar] [CrossRef]
- Morawska, L.; Cao, J. Airborne transmission of SARS-CoV-2: The world should face the reality. Environ. Int. 2020, 139, 105730. [Google Scholar] [CrossRef] [PubMed]
- Correia, G.; Rodrigues, L.; Silva, M.G.D.; Gonçalves, T. Airborne route and bad use of ventilation systems as non-negligible factors in SARS-CoV-2 transmission. Med. Hypotheses 2020, 141, 109781. [Google Scholar] [CrossRef]
- Office for Novel Coronavirus Disease Control, Cabinet Secretariat, Government of Japan. Suggestion to the Japanese Governmental Officers to Facilitate the Important Writings to Various Guidelines in Order to Prevent COVID-19. 11 November 2020. Available online: https://www.mhlw.go.jp/content/000695178.pdf (accessed on 14 May 2021).
- Marr, L.; Miller, S.; Prather, K.; Haas, C.; Bahnfleth, W.; Corsi, R.; Tang, J.; Herrmann, H.; Pollitt, K.; Ballester, J.; et al. FAQs on Protecting Yourself from COVID-19 Aerosol Transmission. Version: 1.87. 9 December 2020. Available online: http://tinyurl.com/faqs-aerosol (accessed on 31 July 2021).
- Jiji, K. Four die in fire suppression system accident in Tokyo parking garage. Japan Times, 16 April 2021. [Google Scholar]
- Malley, W.J. Blood gas electrodes and quality assurance. In Clinical Blood Gases: Assessment and Intervention, 2nd ed.; Elsevier Saunders: St. Louis, MO, USA; Elsevier: Philadelphia, PA, USA, 2005; pp. 82–113. [Google Scholar]
- Severinghaus, J.W.; Astrup, P.B. History of blood gas analysis. III. Carbon dioxide tension. J. Clin. Monit. 1986, 2, 60–73. [Google Scholar] [CrossRef]
- McConville, J.F.; Solway, J.; Mokhlesi, B. Disorders of venntilation. In Harrison’s Principles of Internal Medicine, 20th ed.; McGraw-Hill Education: New York, NY, USA, 2018; pp. 2010–2013. [Google Scholar]
- Silverman, E.K.; Crapo, J.D.; Make, B.J. Chronic obstructive pulmonary disease. In Harrison’s Principles of Internal Medicine, 20th ed.; McGraw-Hill Education: New York, NY, USA, 2018; pp. 1990–1999. [Google Scholar]
- DuBose, T.D., Jr. Acidosis and alkalosis. In Harrison’s Principles of Internal Medicine, 20th ed.; McGraw-Hill Education: New York, NY, USA, 2018; pp. 315–324. [Google Scholar]
- Goldring, R.M.; Kazemi, H. Regulation of ventilation in metabolic acidosis and alkalosis. In Pulmonary Diseases and Disorders, 2nd ed.; Fisherman, A.P., Ed.; McGraw-Hill: New York, NY, USA, 1988; pp. 281–288. [Google Scholar]
- Sharma, S.; Hashmi, M.F.; Aggarwal, S. Hyperchloremic Acidosis; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://pubmed.ncbi.nlm.nih.gov/29493965/ (accessed on 18 August 2021).
- Malley, W.J. Blood gas classification. In Clinical Blood Gases: Assessment and Intervention, 2nd ed.; Elsevier Saunders: St. Louis, MO, USA; Elsevier: Philadelphia, PA, USA, 2005; pp. 35–57. [Google Scholar]
- Malley, W.J. Regulation of acids, bases, and electrolytes. In Clinical Blood Gases: Assessment and Intervention, 2nd ed.; Elsevier Saunders: St. Louis, MO, USA; Elsevier: Philadelphia, PA, USA, 2005; pp. 307–331. [Google Scholar]
- American Association for Respiratory Care. AARC clinical practice guideline. Sampling for arterial blood gas analysis. Respir. Care 1992, 37, 913–917. [Google Scholar]
- Slutsky, A.S.; Brochard, L. Mechanical ventilation. In Goldman-Cecil Medicine, 26th ed.; Goldman, L., Schhafer, A.I., Eds.; Elsevier: Philadelphia, PA, USA, 2020; pp. 635–641. [Google Scholar]
- Severinghaus, J.W.; Honda, Y. History of blood gas analysis. VII. Pulse oximetry. J. Clin. Monit. 1987, 3, 135–138. [Google Scholar] [CrossRef]
- Lee, W.W.; Mayberry, K.; Crapo, R.; Jensen, R.L. The accuracy of pulse oximetry in the emergency department. Am. J. Emerg. Med. 2000, 18, 427–431. [Google Scholar] [CrossRef] [PubMed]
- Brooks, D.; Wynn, V. Use of venous blood for pH and carbon-dioxide studies: Especially in respiratory failure and during anaesthesia. Lancet. 1959, 1, 227–230. [Google Scholar] [CrossRef]
- Harrison, E.M.; Galloon, S. Venous blood as an alternative to arterial blood for the measurement of carbon dioxide tensions. Br. J. Anaesth. 1965, 37, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Brandenburg, M.A.; Dire, D.J. Comparison of arterial and venous blood gas values in the initial emergency department evaluation of patients with diabetic ketoacidosis. Ann. Emerg. Med. 1998, 31, 459–465. [Google Scholar] [CrossRef]
- Gokel, Y.; Paydas, S.; Koseoglu, Z.; Alparslan, N.; Seydaoglu, G. Comparison of blood gas and acid-base measurements in arterial and venous blood samples in patients with uremic acidosis and diabetic ketoacidosis in the emergency room. Am. J. Nephrol. 2000, 20, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Kelly, A.M.; Kyle, E.; McAlpine, R. Venous pCO2 and pH can be used to screen for significant hypercarbia in emergency patients with acute respiratory disease. J. Emerg. Med. 2002, 22, 15–19. [Google Scholar] [CrossRef]
- Rang, L.C.F.; Murray, H.E.; Wells, G.A.; MacGougan, C.K. Can peripheral venous blood gases replace arterial blood gases in emergency department patients? Can. J. Emerg. Med. 2002, 4, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Harrison, A.M.; Lynch, J.M.; Dean, J.M.; White, M.K. Comparison of simultaneously obtained arterial and capillary blood gases in pediatric intensive care unit patients. Crit. Care Med. 1997, 25, 1904–1908. [Google Scholar] [CrossRef] [PubMed]
- McGillivray, D.; Ducharme, F.M.; Charron, Y.; Mattimoe, C.; Treherne, S. Clinical decision making based on venous versus capillary blood gas values in the wellperfused child. Ann. Emerg. Med. 1999, 34, 58–63. [Google Scholar] [CrossRef]
- Zavorsky, G.S.; Cao, J.; Mayo, N.E.; Gabbay, R.; Murias, J.M. Arterial versus capillary blood gases: A meta-analysis. Respir. Physiol. Neurobiol. 2007, 155, 268–279. [Google Scholar] [CrossRef] [PubMed]
- Umeda, A.; Kawasaki, K.; Abe, T.; Watanabe, M.; Ishizaka, A.; Okada, Y. Hyperventilation and finger exercise increase venous-arterial PCO2 and pH differences. Am. J. Emerg. Med. 2008, 26, 975–980. [Google Scholar] [CrossRef]
- Umeda, A.; Kawasaki, K.; Abe, T.; Yamane, T.; Okada, Y. Effects of hyperventilation on venous-arterial bicarbonate concentration difference: A possible pitfall in venous blood gas analysis. Int. J. Clin. Med. 2014, 5, 76–80. [Google Scholar] [CrossRef] [Green Version]
- Scholander, P.F. Analyzer for accurate estimation of respiratory gases in one-half cubic centimeter samples. J. Biol Chem. 1947, 167, 235–250. [Google Scholar] [CrossRef]
- Forbes, A.M.; Behar, M.G.; Smith, T.C. Analysis of oxygen, carbon dioxide and nitrous oxide mixtures with the Scholander apparatus. Anesthesiology 1967, 28, 928–933. [Google Scholar] [CrossRef]
- Siobal, M.S. Monitoring Exhaled Carbon Dioxide. Respir. Care 2016, 61, 1397–1416. [Google Scholar] [CrossRef] [Green Version]
- Johansson, U.B. Determination of respiratory gases (CO2, O2, Ar and N2) with gas solid chromatography. Scand. J. Clin. Lab. Investig. 1983, 43, 91–94. [Google Scholar] [CrossRef]
- Whitesell, R.; Asiddao, C.; Gollman, D.; Jablonski, J. Relationship between arterial and peak expired carbon dioxide pressure during anesthesia and factors influencing the difference. Anesth. Analg. 1981, 60, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Arieli, R. Mass spectrometer for respiratory research. Respir. Physiol. Neurobiol. 2010, 170, 183–184. [Google Scholar] [CrossRef]
- Malley, W.J. Noninvasive blood gas monitoring. In Clinical Blood Gases: Assessment and Intervention, 2nd ed.; Elsevier Saunders: St. Louis, MO, USA; Elsevier: Philadelphia, PA, USA, 2005; pp. 387–418. [Google Scholar]
- Walsh, B.K.; Crotwell, D.N.; Restrepo, R.D. AARC clinical practice guideline: Capnography/Capnometry during mechanical ventilation: 2011. Respir. Care 2011, 56, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Falk, J.L.; Rackow, E.C.; Weil, M.H. End-tidal carbon dioxide concentration during cardiopulmonary resuscitation. N. Engl. J. Med. 1988, 318, 607–611. [Google Scholar] [CrossRef]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P.T.; et al. Adult basic and advanced life support writing group. Part 3: Adult Basic and advanced life support: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2020, 142, S366–S468. [Google Scholar] [CrossRef]
- Soar, J.; Böttiger, B.W.; Carli, P.; Couper, K.; Deaking, C.D.; Djärv, T.; Carsten, L.; Olasveengen, T.; Paal, P.; Pellis, T.; et al. European Resuscitation Council Guidelines 2021: Adult advanced life support. Resuscitation 2021, 161, 115–151. [Google Scholar] [CrossRef] [PubMed]
- American College of Emergency Physicians. Policy Statement: Verification of Endotracheal Tube Placement. Revised January 2016. Available online: https://www.acep.org/patient-care/policy-statements/verification-of-endotracheal-tube-placement/ (accessed on 19 August 2021).
- Sanders, A.B.; Kern, K.B.; Otto, C.W.; Milander, M.M.; Ewy, G.A. End-Tidal carbon dioxide monitoring during cardiopulmonary resuscitation. A prognostic indicator for survival. JAMA 1989, 262, 1347–1351. [Google Scholar] [CrossRef]
- Cheifetz, I.M.; Myers, T.R. Respiratory therapies in the critical care setting. Should every mechanically ventilated patient be monitored with capnography from intubation to extubation? Respir. Care 2007, 52, 423–442. [Google Scholar]
- American Society of Anesthesiologists. Standards for Basic Anesthetic Monitoring. Developed By: Committee on Standards and Practice Parameters. Available online: https://www.asahq.org/standards-and-guidelines/standards-for-basic-anesthetic-monitoring (accessed on 18 August 2021).
- Restrepo, R.D.; Nuccio, P.; Spratt, G.; Waugh, J. Current applications of capnography in non-intubated patients. Expert. Rev. Respir. Med. 2014, 8, 629–639. [Google Scholar] [CrossRef]
- Duyu, M.; Bektas, A.D.; Karakaya, Z.; Bahar, M.; Gunalp, A.; Caglar, Y.M.; Yersel, M.N.; Bozkurt, O. Comparing the novel microstream and the traditional mainstream method of end-tidal CO2 monitoring with respect to PaCO2 as gold standard in intubated critically ill children. Sci. Rep. 2020, 10, 22042. [Google Scholar] [CrossRef]
- Severinghaus, J.W.; Bradley, A.F.; Stafford, M.J. Transcutaneous PCO2 electrode design with internal silver heat path. Birth Defects Orig. Artic. Ser. 1979, 15, 265–270. [Google Scholar]
- Severinghaus, J.W.; Stafford, M.; Bradley, A.F. tcPCO2 electrode design, calibration and temperature gradient problems. Acta Anaesthesiol. Scand. Suppl. 1978, 68, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Huch, R.; Huch, A.; Albani, M.; Gabriel, M.; Schulte, F.J.; Wolf, H.; Rupprath, G.; Emmrich, P.; Stechele, U.; Duc, G.; et al. Transcutaneous PO2 monitoring in routine management of infants and children with cardiorespiratory problems. Pediatrics 1976, 57, 681–690. [Google Scholar] [PubMed]
- Huch, A.; Seiler, D.; Meinzer, K.; Huch, R.; Galster, H.; Lübbers, D.W. Transcutaneous PCO2 measurement with a miniaturised electrode. Lancet 1977, 1, 982–983. [Google Scholar] [CrossRef]
- Hagiwara, B. Transcutaneous electrodes for blood gas determination. Jpn. J. Med. Electron. Biol. Eng. Iyodenshi Seitai Kogaku 1983, 21, 524–530. [Google Scholar]
- Lucey, J.F. Clinical uses of transcutaneous oxygen monitoring. Adv. Pediatr. 1981, 28, 27–56. [Google Scholar]
- Wimberley, P.D.; Pedersen, K.G.; Thode, J.; Fogh-Andersen, N.; Sørensen, A.M.; Siggaard-Andersen, O. Transcutaneous and capillary pCO2 and pO2 measurements in healthy adults. Clin. Chem. 1983, 29, 1471–1473. [Google Scholar] [CrossRef]
- Rüdiger, M.; Töpfer, K.; Hammer, H.; Schmalisch, G.; Wauer, R.R. A survey of transcutaneous blood gas monitoring among European neonatal intensive care units. BMC Pediatr. 2005, 5, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delerme, S.; Montout, V.; Goulet, H.; Arhan, A.; Le Saché, F.; Devilliers, C.; Riou, B.; Ray, P. Concordance between transcutaneous and arterial measurements of carbon dioxide in an ED. Am. J. Emerg. Med. 2012, 30, 1872–1876. [Google Scholar] [CrossRef] [PubMed]
- Stieglitz, S.; Matthes, S.; Priegnitz, C.; Hagmeyer, L.; Randerath, W. Comparison of transcutaneous and capillary measurement of PCO2 in hypercapnic subjects. Respir. Care 2016, 61, 98–105. [Google Scholar] [CrossRef] [Green Version]
- Nishiyama, T.; Nakamura, S.; Yamashita, K. Effects of the electrode temperature of a new monitor, TCM4, on the measurement of transcutaneous oxygen and carbon dioxide tension. J. Anesth. 2006, 20, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Restrepo, R.D.; Hirst, K.R.; Wittnebel, L.; Wettstein, R. AARC clinical practice guideline: Transcutaneous monitoring of carbon dioxide and oxygen: 2012. Respir. Care 2012, 57, 1955–1962. [Google Scholar] [CrossRef]
- Ruangsetakit, C.; Chinsakchai, K.; Mahawongkajit, P.; Wongwanit, C.; Mutirangura, P. Transcutaneous oxygen tension: A useful predictor of ulcer healing in critical limb ischaemia. J. Wound Care 2010, 19, 202–206. [Google Scholar] [CrossRef] [Green Version]
- Umeda, A.; Okada, Y. Comparison of Accuracy: Bland-Altman analysis of alternative examinations in the field of respiratory medicine. Kokyu Junkan Respir. Circ. 2012, 60, 840–848. [Google Scholar]
- Aliwalas, L.L.; Noble, L.; Nesbitt, K.; Fallah, S.; Shah, V.; Shah, P.S. Agreement of carbon dioxide levels measured by arterial, transcutaneous and end tidal methods in preterm infants <or = 28 weeks gestation. J. Perinatol. 2005, 25, 26–29. [Google Scholar]
- Tobias, J.D.; Meyer, D.J. Noninvasive monitoring of carbon dioxide during respiratory failure in toddlers and infants: End-tidal versus transcutaneous carbon dioxide. Anesth. Analg. 1997, 85, 55–58. [Google Scholar]
- Oshibuchi, M.; Cho, S.; Hara, T.; Tomiyasu, S.; Makita, T.; Sumikawa, K. A comparative evaluation of transcutaneous and end-tidal measurements of CO2 in thoracic anesthesia. Anesth. Analg. 2003, 97, 776–779. [Google Scholar] [CrossRef]
- Tingay, D.G.; Stewart, M.J.; Morley, C.J. Monitoring of end tidal carbon dioxide and transcutaneous carbon dioxide during neonatal transport. Arch. Dis. Child. Fetal Neonatal Ed. 2005, 90, F523–F526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirabayashi, M.; Fujiwara, C.; Ohtani, N.; Kagawa, S.; Kamide, M. Transcutaneous PCO2 monitors are more accurate than end-tidal PCO2 monitors. J. Anesth. 2009, 23, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, S.B.; Wolfram Windisch, W.; Magnet, F.S.; Schmoor, C.; Karagiannidis, C.; Callegari, J.; Huttmann, S.E.; Storre, J.H. Continuous non-invasive PCO2 monitoring in weaning patients: Transcutaneous is advantageous over end-tidal PCO2. Respirology 2017, 22, 1579–1584. [Google Scholar] [CrossRef]
- Umeda, A.; Ishizaka, M.; Tasaki, M.; Yamane, T.; Watanabe, T.; Inoue, Y.; Mochizuki, T.; Okada, Y.; Kesler, S. Evaluation of time courses of agreement between minutely obtained transcutaneous blood gas data and the gold standard arterial data from spontaneously breathing Asian adults, and various subgroup analyses. BMC Pulm. Med. 2020, 20, 151. [Google Scholar] [CrossRef]
- Kulandavelu, S.; Balkan, W.; Hare, J.M. Regulation of oxygen delivery to the body via hypoxic vasodilation. Proc. Natl. Acad. Sci. USA. 2015, 112, 6254–6255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huttmann, S.E.; Windisch, W.; Storre, J.H. Techniques for the measurement and monitoring of carbon dioxide in the blood. Ann. Am. Thorac. Soc. 2014, 11, 645–652. [Google Scholar] [CrossRef]
- Janssens, J.P.; Perrin, E.; Bennani, I.; Muralt, B.; Titelion, V.; Picaud, C. Is continuous transcutaneous monitoring of PCO2 (Tc P CO2) over 8 h reliable in adults? Respir. Med. 2001, 95, 331–335. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, P.; Lellouche, F.; Aboab, J.; Buisson, C.B.; Brochard, L. Transcutaneous arterial carbon dioxide pressure monitoring in critically ill adult patients. Intensive Care Med. 2006, 32, 309–312. [Google Scholar] [CrossRef]
- Gerdung, C.A.; Adeleye, A.; Kirk, V.G. Noninvasive monitoring of CO2 during polysomnography: A review of the recent literature. Curr. Opin. Pulm. Med. 2016, 22, 527–534. [Google Scholar] [CrossRef]
- Trucco, F.; Pedemonte, M.; Fiorillo, C.; Tan, H.-L.; Carlucci, A.; Brisca, G.; Tacchetti, P.; Bruno, C.; Minetti, C. Detection of early nocturnal hypoventilation in neuromuscular disorders. J. Int. Med. Res. 2018, 46, 1153–1161. [Google Scholar] [CrossRef] [Green Version]
- Buekers, J.; Boever, P.D.; Theunis, J.; Houben-Wilke, S.; Vaes, A.W.; Franssen, F.M.E.; Wouters, E.F.M.; Simons, S.; Aerts, J.-M.; Spruit, M.A. Physiological changes differ between responders and nonresponders to pulmonary rehabilitation in COPD. Med. Sci. Sports Exerc. 2021, 53, 1125–1133. [Google Scholar] [CrossRef]
- Prieur, G.; Medrinal, C.; Combret, Y.; Lozeron, E.D.; Bonnevie, T.; Gravier, F.E.; Quieffin, J.; Lamia, B.; Borel, J.C.; Reychler, G. Nasal high flow does not improve exercise tolerance in COPD patients recovering from acute exacerbation: A randomized crossover study. Respirology 2019, 24, 1088–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, T.; Ishizaka, M.; Kaneko, J.; Umeda, A. Effect of resistance exercise and aerobic exercise on percutaneous oxygen pressure in the lower extremities. Rigakuryoho Kagaku 2020, 35, 855–859. [Google Scholar] [CrossRef]
- Mori, M.; Nakagami, H.; Rodriguez-Araujo, G.; Nimura, K.; Kaneda, Y. Essential role for miR-196a in brown adipogenesis of white fat progenitor cells. PLoS Biol. 2012, 10, e1001314. [Google Scholar] [CrossRef] [Green Version]
- Umeda, A.; Miyagawa, K.; Mochida, A.; Takeda, T.; Takeda, K.; Okada, Y.; Gozal, D. Intermittent hypoxia, energy expenditure, and visceral adipocyte recovery. Respir. Physiol. Neurobiol. 2020, 273, 103332. [Google Scholar] [CrossRef]
- Shimizu, N.; Maruyama, T.; Yoshikawa, N.; Matsumiya, R.; Ma, Y.; Ito, N.; Tasaka, Y.; Kuribara-Souta, A.; Miyata, K.; Oike, Y.; et al. A muscle-liver-fat signalling axis is essential for central control of adaptive adipose remodeling. Nat. Commun. 2015, 6, 6693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pauling, L.; Wood, R.E.; Sturdivant, J.H. An instrument for determining the partial pressure of oxygen in a gas. J. Am. Chem Soc. 1946, 68, 795–798. [Google Scholar] [CrossRef] [PubMed]
- Drager, L.F.; Brunoni, A.R.; Jenner, R.; Lorenzi-Filho, G.; Bensenor, I.M.; Lotufo, P.A. Effects of CPAP on body weight in patients with obstructive sleep apnoea: A meta-analysis of randomised trials. Thorax 2015, 70, 258–264. [Google Scholar] [CrossRef] [Green Version]
- Chen, B.; Drager, L.F.; Peker, Y.; Vgontzas, A.N.; Phillips, C.L.; Hoyos, C.M.; Salles, G.F.; Guo, M.; Li, Y. Effect of CPAP on Weight and Local Adiposity in Adults with Obstructive Sleep Apnea: A Meta-Analysis. Ann. Am. Thorac. Soc. 2021. [Google Scholar] [CrossRef]
- Dedual, M.A.; Wueest, S.; Borsigova, M.; Konrad, D. Intermittent fasting improves metabolic flexibility in short-term high-fat dietfed mice. Am. J. Physiol. Endocrinol. Metab. 2019, 317, E773–E782. [Google Scholar] [CrossRef] [PubMed]
- Grandl, G.; Straub, L.; Rudigier, C.; Arnold, M.; Wueest, S.; Konrad, D.; Wolfrum, C. Short-term feeding of a ketogenic diet induces more severe hepatic insulin resistance than an obesogenic high-fat diet. J. Physiol. 2018, 596, 4597–4609. [Google Scholar] [CrossRef] [PubMed]
- Umeda, A.; Miyagawa, K.; Mochida, A.; Takeda, H.; Takeda, K.; Okada, Y.; Gozal, D. Effects of normoxic recovery on intima-media thickness of aorta and pulmonary artery following intermittent hypoxia in mice. Front. Physiol. 2020, 11, 583735. [Google Scholar] [CrossRef]
- Patel, H.; Kerndt, C.C.; Bhardwaj, A. NCBI Resources: Physiology, Respiratory Quotient. Available online: https://www.ncbi.nlm.nih.gov/books/NBK531494/ (accessed on 4 May 2021).
- Lin, C.-H.; Wu, L.-X.; Chen, K.-H.; Lo, H.-F.; Lin, K.-C.; Kasai, T.; Chen, C.-C.; Shih, C.-H.; Manzano, M.C.; Santos, G.N.; et al. Non-Invasive and time-dependent blood-sugar monitoring via breath-derived CO2 correlation using gas chromatograph with a Milliwhistle gas analyzer. Anal. Sci. 2020, 36, 739–743. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Li, M.; Fan, J.; Peng, X. Activity-Based sensing and theranostic probes based on photoinduced electron transfer. Acc. Chem. Res. 2019, 52, 2818–2831. [Google Scholar] [CrossRef]
- Herman, P.; Murtaza, Z.; Lakowicz, J.R. Sensing of carbon dioxide by a decrease in photoinduced electron transfer quenching. Anal. Biochem. 1999, 272, 87–93. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surrogate | Average Bias | 1.96 SD | Accuracy | Usefulness for Patients with Pulmonary Diseases | References |
|---|---|---|---|---|---|
| PvCO2 | Approximately 5 mmHg higher than PaCO2 | 14.7–15.0 mmHg | Worst | Limited | [45,50] |
| PetCO2 | 2–5 mmHg lower than PaCO2 | 6.9–14.4 mmHg | Second best | Limited | [83,84,85,86,87,88] |
| PtcCO2 | 4–5 mmHg higher than PaCO2 | 4.6–10.4 mmHg | Best | Good (still not replaceable) | [83,84,85,86,87,88,89] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Umeda, A.; Ishizaka, M.; Ikeda, A.; Miyagawa, K.; Mochida, A.; Takeda, H.; Takeda, K.; Fukushi, I.; Okada, Y.; Gozal, D. Recent Insights into the Measurement of Carbon Dioxide Concentrations for Clinical Practice in Respiratory Medicine. Sensors 2021, 21, 5636. https://doi.org/10.3390/s21165636
Umeda A, Ishizaka M, Ikeda A, Miyagawa K, Mochida A, Takeda H, Takeda K, Fukushi I, Okada Y, Gozal D. Recent Insights into the Measurement of Carbon Dioxide Concentrations for Clinical Practice in Respiratory Medicine. Sensors. 2021; 21(16):5636. https://doi.org/10.3390/s21165636
Chicago/Turabian StyleUmeda, Akira, Masahiro Ishizaka, Akane Ikeda, Kazuya Miyagawa, Atsumi Mochida, Hiroshi Takeda, Kotaro Takeda, Isato Fukushi, Yasumasa Okada, and David Gozal. 2021. "Recent Insights into the Measurement of Carbon Dioxide Concentrations for Clinical Practice in Respiratory Medicine" Sensors 21, no. 16: 5636. https://doi.org/10.3390/s21165636