
How to Manage a Patient with Haemophilia and ACS Requiring PCI: A Battle between Bleeding and Thrombosis

 ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
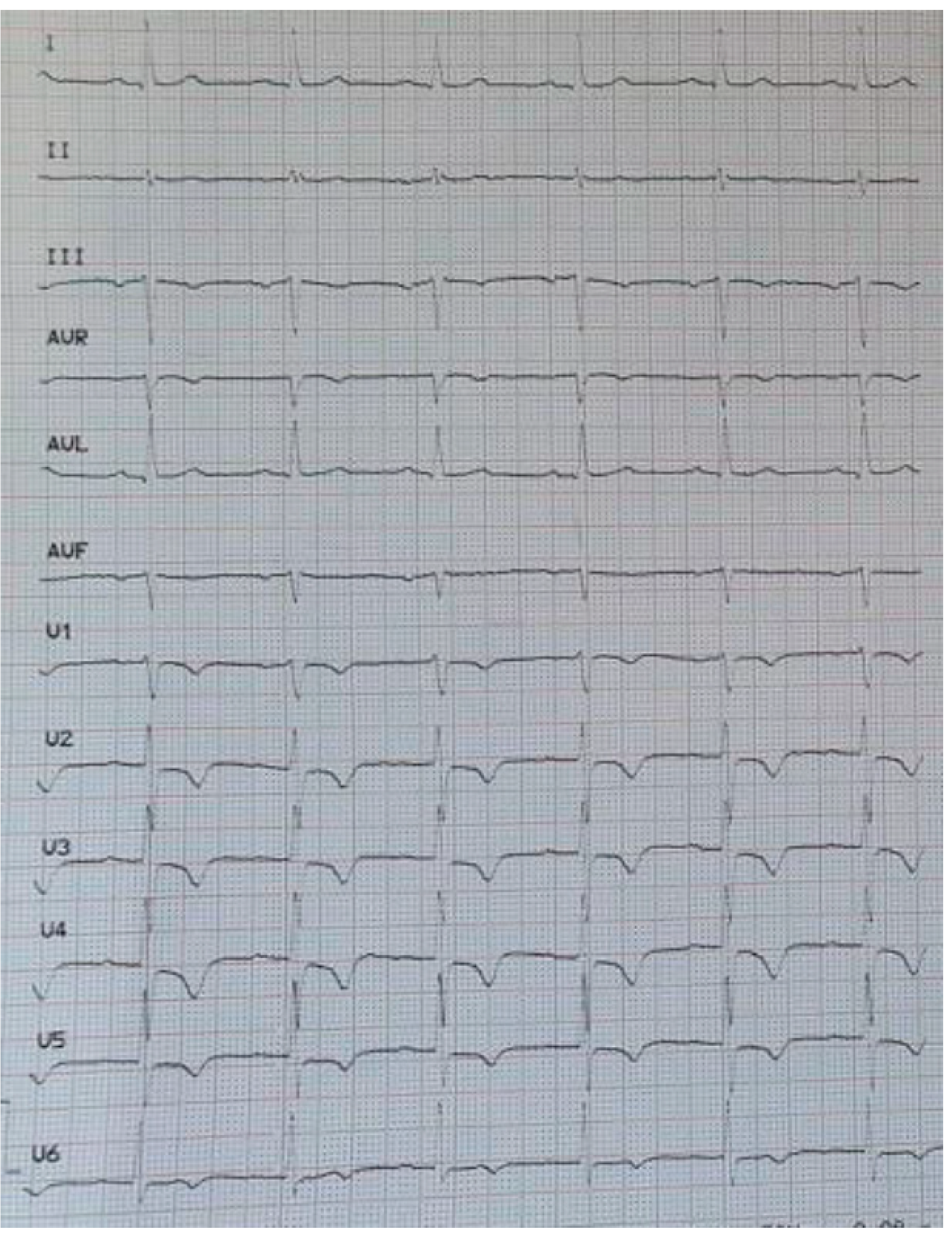
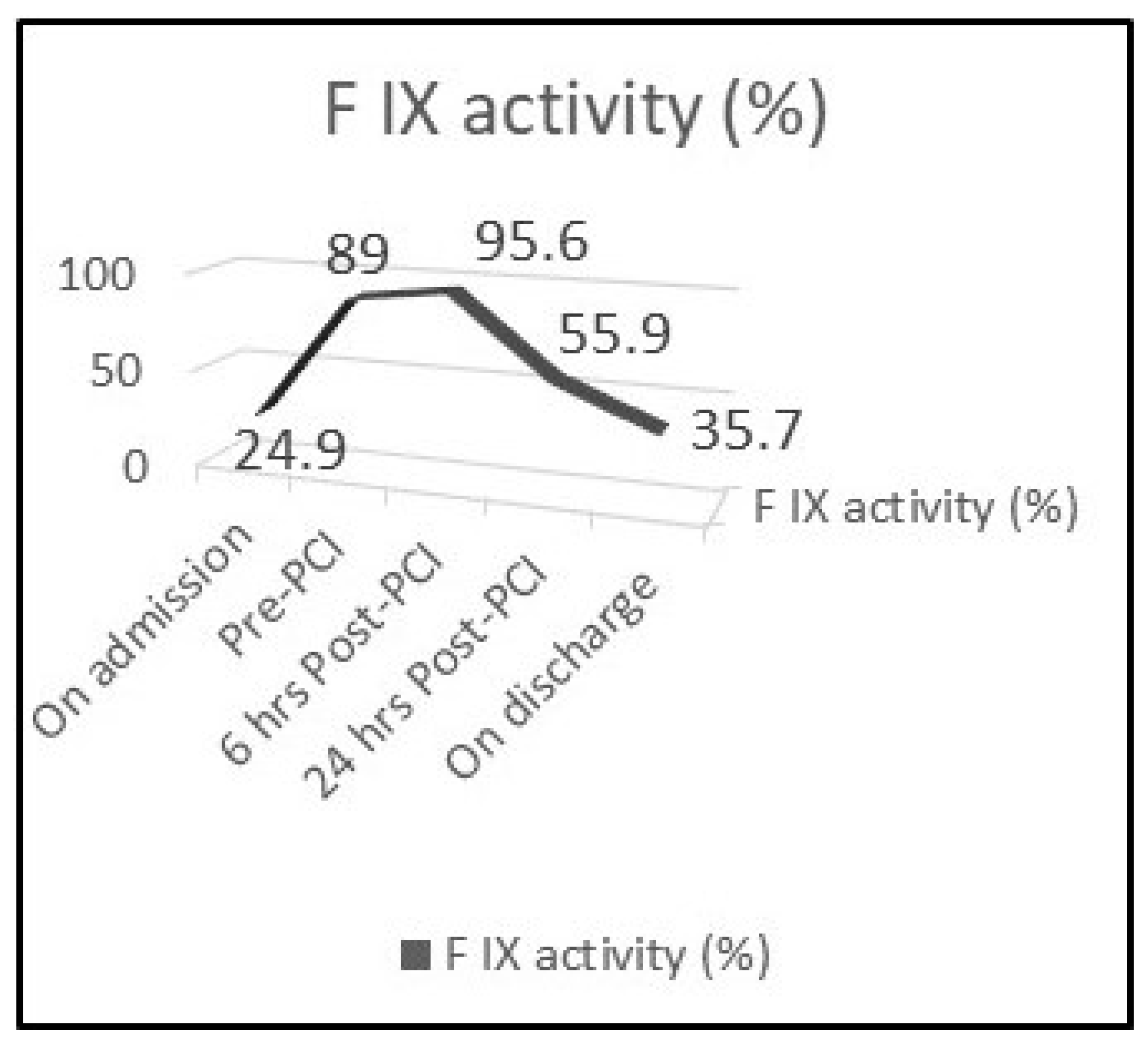
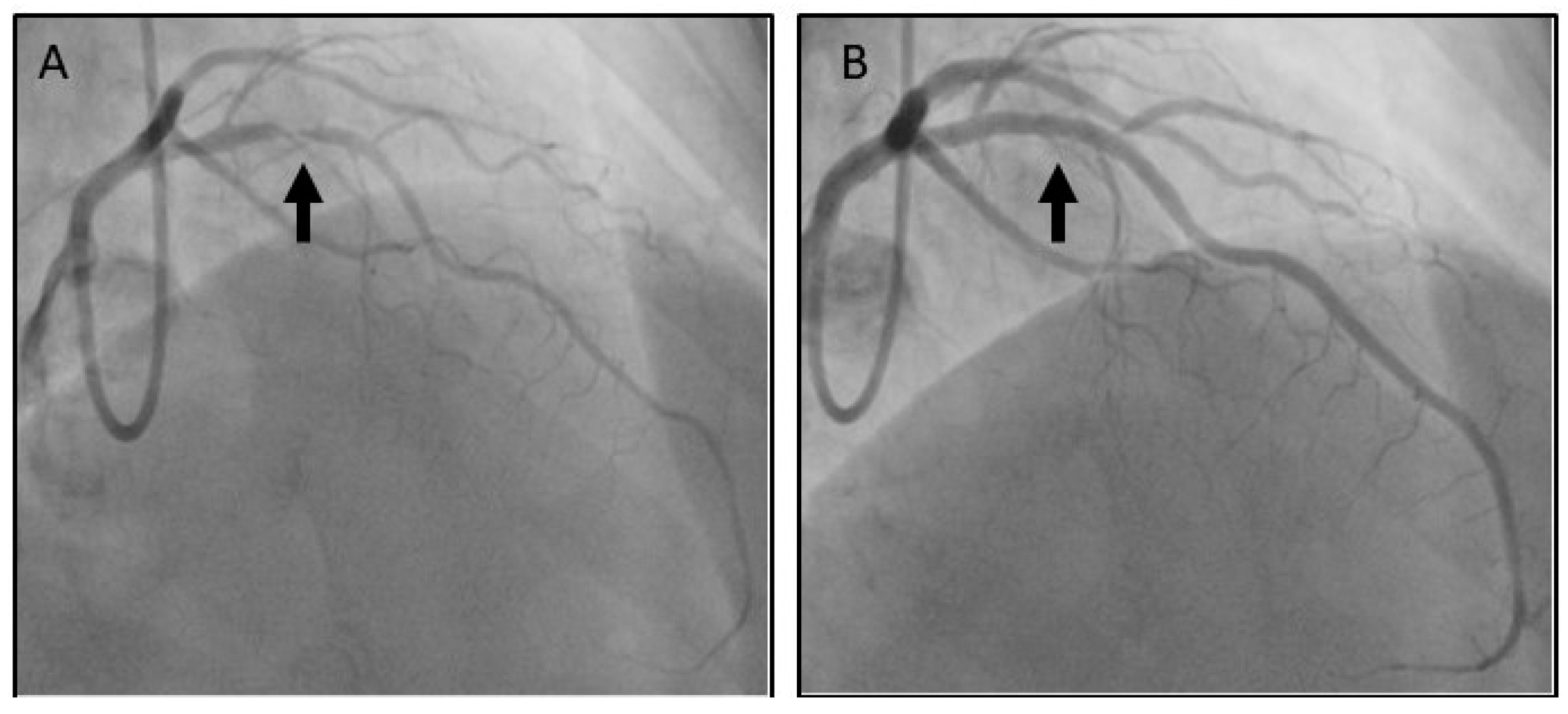
2. Case Presentation
3. Discussion
3.1. Haemophilia and Coronary Artery Disease
3.2. Haemophilia and Acute Coronary Syndromes
3.3. Selection of Access Site
3.4. Selection of Stent
3.5. Selection of Anticoagulant Therapy
3.6. Selection of Antiplatelet Therapy
3.7. Management of Bleeding Risk Associated with Antiplatelet Therapy
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Nowbar, A.N.; Gitto, M.; Howard, J.P.; Francis, D.P.; Al-Lamee, R. Mortality From Ischemic Heart Disease. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005375. [Google Scholar] [CrossRef]
- Amsterdam, E.A.; Wenger, N.K.; Brindis, R.G.; Casey, D.E., Jr.; Ganiats, T.G.; Holmes, D.R., Jr.; Jaffe, A.S.; Jneid, H.; Kelly, R.F.; Kontos, M.C.; et al. ACC/AHA Task Force Members; Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 130, e344–e426. [Google Scholar] [PubMed]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2020, ehaa575. [Google Scholar] [CrossRef]
- Ndrepepa, G.; Berger, P.B.; Mehilli, J.; Seyfarth, M.; Neumann, F.J.; Schömig, A.; Kastrati, A. Periprocedural bleeding and 1-year outcome after percutaneous coronary interventions: Appropriateness of including bleeding as a component of a quadruple end point. J. Am. Coll. Cardiol. 2008, 5, 690–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escobar, M.; Sallah, S. Hemophilia A and hemophilia B: Focus on arthropathy and variables affecting bleeding severity and prophylaxis. J. Thromb. Haemost. 2013, 11, 1449–1453. [Google Scholar] [CrossRef]
- Biggs, R.; Douglas, A.S.; MacFarlane, R.G.; Dacie, J.V.; Pitney, W.R.; Merskey, C.; O’Brien, J.R. Christmas disease: A condition previously mistaken for haemophilia. Br. Med. J. 1952, 2, 1378–1382. [Google Scholar] [CrossRef] [PubMed]
- Blanchette, V.S.; Key, N.S.; Ljung, L.R.; Manco-Johnson, M.J.; van den Berg, H.M.; Srivastava, A. Subcommittee on Factor VIII, Factor IX and Rare Coagulation Disorders of the Scientific and Standardization Committee of the International Society on Thrombosis and Hemostasis. Definitions in hemophilia: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2014, 12, 19351939. [Google Scholar]
- Knobe, K.; Berntorp, E. New treatments in hemophilia: Insights for the clinician. Ther. Adv. Hematol. 2012, 3, 165–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamphuisen, P.W.; ten Cate, H. Cardiovascular risk in patients with hemophilia. Blood 2014, 123, 1297–1301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuinenburg, A.; Mauser-Bunschoten, E.P.; Verhaar, M.C.; Biesma, D.H.; Schutgens, R.E. Cardiovascular disease in patients with hemophilia. J. Thromb. Haemost. 2009, 7, 247–254. [Google Scholar] [CrossRef]
- Staritz, P.; de Moerloose, P.; Schutgens, R.; Dolan, G.; ADVANCE Working Group. Applicability of the European Society of Cardiology guidelines on management of acute coronary syndromes to people with haemophilia—An assessment by the ADVANCE Working Group. Haemophilia 2013, 19, 833–840. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. ESC Scientific Document Group. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar]
- Fefer, P.; Gannot, S.; Lubetsky, A.; Martinowitz, U.; Matetzky, S.; Guetta, V.; Segev, A. Percutaneous coronary intervention in patients with haemophilia presenting with acute coronary syndrome: An interventional dilemma: Case series, review of the literature, and tips for management. J. Thromb. Thrombolysis. 2013, 35, 271–278. [Google Scholar] [CrossRef]
- Kassimis, G.; Banning, A.P. Is it time to take bare metal stents off the catheter laboratory shelf? Eur. Heart J. 2016, 37, 33723375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valgimigli, M.; Patialiakas, A.; Thury, A.; McFadden, E.; Colangelo, S.; Campo, G.; Tebaldi, M.; Ungi, I.; Tondi, S.; Roffi, M.; et al. Zotarolimus-eluting versus bare-metal stents in uncertain drug-eluting stent candidates. J. Am. Coll. Cardiol. 2015, 65, 805–815. [Google Scholar] [CrossRef] [Green Version]
- Varenne, O.; Cook, S.; Sideris, G.; Kedev, S.; Cuisset, T.; Carrié, D.; Hovasse, T.; Garot, P.; El Mahmoud, R.; Spaulding, C.; et al. Drugeluting stents in elderly patients with coronary artery disease (SENIOR): A randomised single-blind trial. Lancet 2018, 391, 41–50. [Google Scholar] [CrossRef]
- Urban, P.; Meredith, I.T.; Abizaid, A.; Pocock, S.J.; Carrié, D.; Naber, C.; Lipiecki, J.; Richardt, G.; Iñiguez, A.; Brunel, P.; et al. Polymer-free Drug-Coated Coronary Stents in Patients at High Bleeding Risk. N. Engl. J. Med. 2015, 373, 2038–2047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Windecker, S.; Latib, A.; Kedhi, E.; Kirtane, A.J.; Kandzari, D.E.; Mehran, R.; Price, M.J.; Abizaid, A.; Simon, D.I.; Worthley, S.G.; et al. Polymerbased or Polymer-free Stents in Patients at High Bleeding Risk. N. Engl. J. Med. 2020, 382, 1208–1218. [Google Scholar] [CrossRef]
- Martin, K.; Key, N.S. How I treat patients with inherited bleeding disorders who need anticoagulant therapy. Blood 2016, 128, 178–184. [Google Scholar] [CrossRef] [Green Version]
- Boehnel, C.; Rickli, H.; Graf, L.; Maeder, M.T. Coronary angiography with or without percutaneous coronary intervention in patients with hemophilia-Systematic review. Catheter. Cardiovasc. Interv. 2018, 92, 1–15. [Google Scholar] [CrossRef]
- Guillet, B.; Cayla, G.; Lebreton, A.; Trillot, N.; Wibaut, B.; Falaise, C.; Castet, S.; Gautier, P.; Claeyssens, S.; Schved, J.F. Long-Term An tithrombotic Treatments Prescribed for Cardiovascular Diseases in Patients with Hemophilia: Results from the French Registry. Thromb. Haemost. 2021, 121, 287–296. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Theodoropoulos, K.C.; Vakalopoulou, S.; Oikonomou, M.; Stavropoulos, G.; Ziakas, A.; Kanonidis, I.; Kassimis, G. How to Manage a Patient with Haemophilia and ACS Requiring PCI: A Battle between Bleeding and Thrombosis. Medicina 2021, 57, 352. https://doi.org/10.3390/medicina57040352
Theodoropoulos KC, Vakalopoulou S, Oikonomou M, Stavropoulos G, Ziakas A, Kanonidis I, Kassimis G. How to Manage a Patient with Haemophilia and ACS Requiring PCI: A Battle between Bleeding and Thrombosis. Medicina. 2021; 57(4):352. https://doi.org/10.3390/medicina57040352
Chicago/Turabian StyleTheodoropoulos, Konstantinos C., Sofia Vakalopoulou, Maria Oikonomou, George Stavropoulos, Antonios Ziakas, Ioannis Kanonidis, and George Kassimis. 2021. "How to Manage a Patient with Haemophilia and ACS Requiring PCI: A Battle between Bleeding and Thrombosis" Medicina 57, no. 4: 352. https://doi.org/10.3390/medicina57040352