
Renal Cell Carcinoma or Oncocytoma? The Contribution of Diffusion-Weighted Magnetic Resonance Imaging to the Differential Diagnosis of Renal Masses

Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
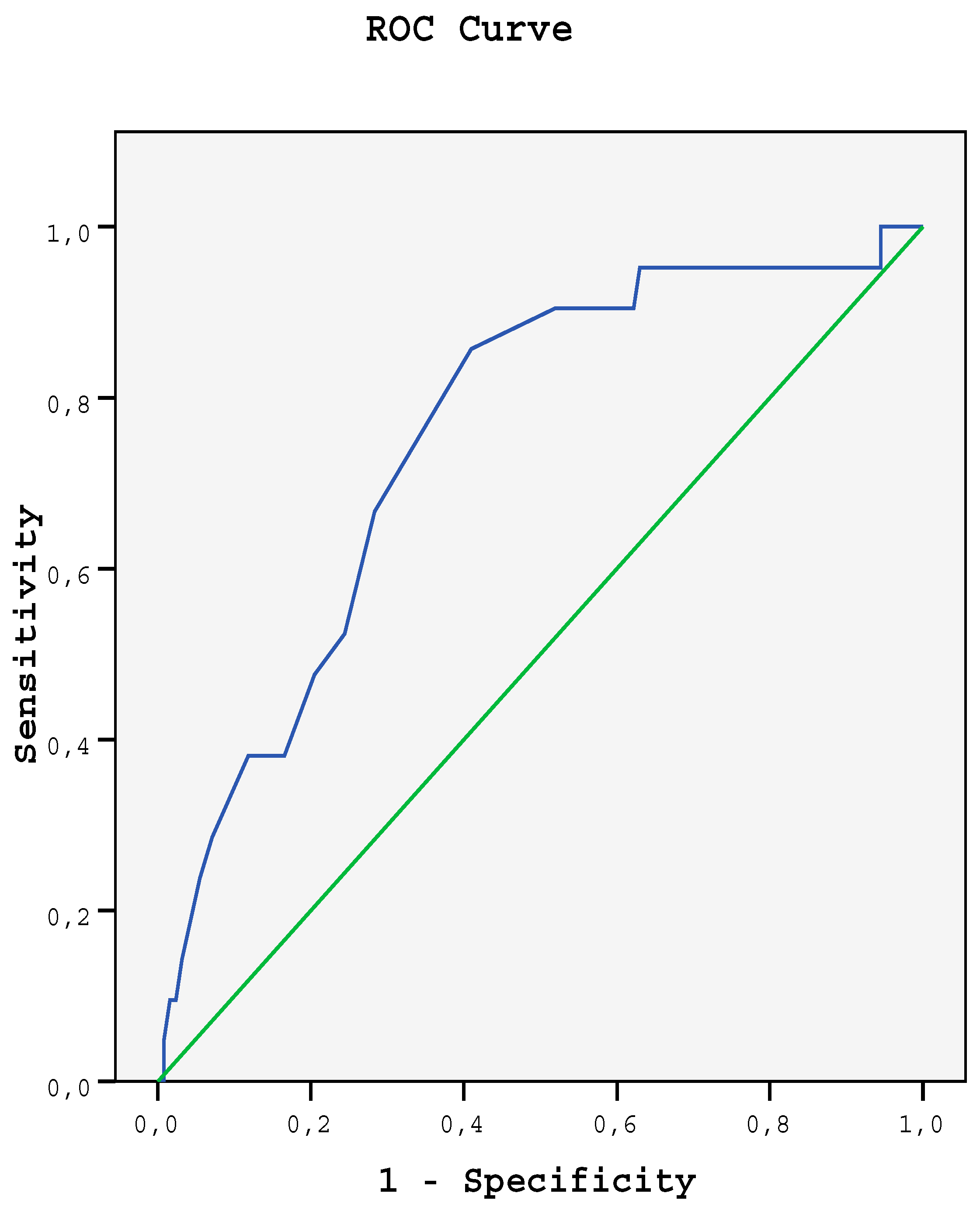
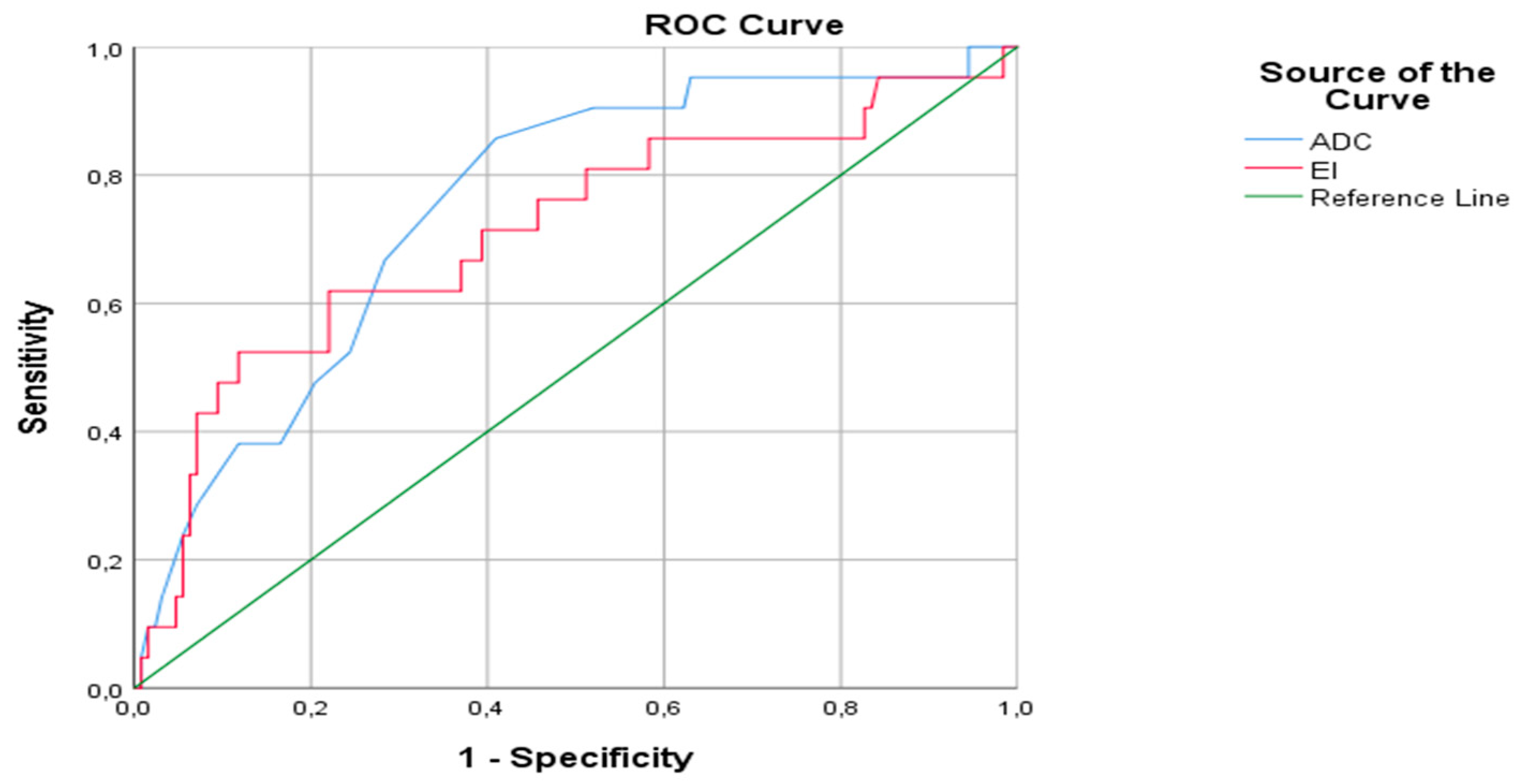
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| RCC | Renal cell carcinoma |
| DWI | Diffusion-weighted imaging |
| MRI | Magnetic resonance imaging |
| ADC | Apparent diffusion coefficient |
| FOV | The field of view |
| CI | The contrasting index |
| SI | Signal intensity |
| Statistical Package for Social Sciences | The SPSS |
| USG | Ultrasonography |
| CT | Computed tomography |
References
- Mytsyk, Y.; Dutka, I.; Borys, Y.; Komnatska, I.; Shatynska-Mytsyk, I.; Farooqi, A.A.; Gazdikova, K.; Caprida, M.; Rodrigo, L.; Kruzliak, P. Renal cell carcinoma: Applicability of the apparent coefficient of the diffusion-weighted estimated by MRI for improving their differential diagnosis, histologic subtyping, and differentiation grade. Int. Urol. Nephrol. 2017, 49, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Lin, M.; Ouyang, H.; Zhou, C.; Zhang, H. Application of ADC measurement in characterization of renal cell carcinomas with different pathological types and grades by 3.0 T diffusion-weighted MRI. Eur. J. Radiol. 2012, 81, 3061–3066. [Google Scholar] [CrossRef] [PubMed]
- Lassel, E.; Rao, R.; Schwenke, C.; Schoenberg, S.; Michaely, H. Diffusion-weighted imaging of focal renal lesions: A meta-analysis. Eur. Radiol. 2014, 24, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Perez-Ordonez, B.; Hamed, G.; Campbell, S.; Erlandson, R.A.; Russo, P.; Gaudin, P.B.; Reuter, V.E. Renal oncocytoma: A clinicopathologic study of 70 cases. Am. J. Surg. Pathol. 1997, 21, 871–883. [Google Scholar] [CrossRef] [PubMed]
- Gakis, G.; Kramer, U.; Schilling, D.; Kruck, S.; Stenzl, A.; Schlemmer, H.P. Small renal oncocytomas: Differentiation with multiphase CT. Eur. J. Radiol. 2011, 80, 274–278. [Google Scholar] [CrossRef]
- Cornelis, F.; Lasserre, A.S.; Tourdias, T.; Deminière, C.; Ferrière, J.M.; Le Bras, Y.; Grenier, N. Combined late gadolinium-enhanced and doubleecho chemical-shiftMRI help to differentiate renal oncocytomas with high central T2 signal intensity from renal cell carcinomas. Am. J. Roentgenol. 2013, 200, 830–838. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Lefkowitz, R.A.; Ishill, N.M.; Wang, L.; Moskowitz, C.S.; Russo, P.; Eisenberg, H.; Hricakm, H. Solid renal cortical tumors: Differentiation with CT. Radiology 2007, 244, 494–504. [Google Scholar] [CrossRef]
- Le Bihan, D.; Turner, R.; Douek, P.; Patronas, N. Diffusion MR imaging: Clinical applications. AJR Am. J. Roentgenol. 1992, 159, 591–599. [Google Scholar] [CrossRef]
- Tordjman, M.; Mali, R.; Madelin, G.; Prabhu, V.; Kang, S.K. Diagnostic test accuracy of ADC values for identification of clear cell renal cell carcinoma: Systematic review and meta-analysis. Eur. Radiol. 2020, 30, 4023–4038. [Google Scholar] [CrossRef]
- Celik, A. Effect of imaging parameters on the accuracy of apparent diffusion coefficient and optimization strategies. Diagn. Interv. Radiol. 2016, 22, 101–107. [Google Scholar] [CrossRef]
- Corcoran, A.T.; Russo, P.; Lowrance, W.T.; Asnis-Alibozek, A.; Libertino, A.J.; Pryma, A.D.; Divgi, C.R.; Uzzo, R.G. A review of contemporary data on surgically resected renal masses: Benign or malignant? Urology 2013, 81, 707–713. [Google Scholar] [CrossRef]
- Lane, B.R.; Babineau, D.C.; Poggio, E.D.; Weight, C.J.; Larson, B.T.; Gill, I.S.; Novick, A.C. Factors predicting renal functional outcome after partial nephrectomy. J. Urol. 2008, 180, 2363–2368. [Google Scholar] [CrossRef]
- Leveridge, M.J.; Finelli, A.; Kachura, J.R.; Evans, A.; Chung, H.; Shiff, D.A.; Fernandes, K.; Jewett, M.A.S. Outcomes of small renal mass needle core biopsy, nondiagnostic percutaneous biopsy, and the role of repeat biopsy. Eur. Urol. 2011, 60, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Pierorazio, P.M.; Johnson, M.H.; Ball, M.W.; Gorin, M.A.; Trock, B.J.; Chang, P.; Wagner, A.A.; McKiernan, J.M.; Allaf, M.E. Five-year analysis of a multi-institutional prospective clinical trial of delayed intervention and surveillance for small renal masses: The DISSRM registry. Eur. Urol. 2015, 68, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Nickerson, M.L.; Jaeger, E.; Shi, Y.; Durocher, J.A.; Mahurkar, S.; Zaridze, D.; Matveev, V.; Janout, V.; Kollarova, H.; Bencko, V.; et al. Improved identification of von Hippel-Lindau gene alterations in clear cell renal tumors. Clin. Cancer Res. 2008, 14, 4726–4734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crepel, M.; Jeldres, C.; Perrotte, P.; Capitanio, U.; Isbarn, H.; Shariat, S.F.; Liebermann, D.; Sun, M.; Lughezzani, G.; Arjane, P.; et al. Nephron-sparing surgery is equally effective to radical nephrectomy for T1BN0M0 renal cell carcinoma: A population-based assessment. Urology 2010, 75, 271–275. [Google Scholar] [CrossRef]
- Jasinski, R.W.; Amendola, M.A.; Glazer, G.M.; Bree, R.L.; Gikas, P.W. Computed tomography of renal oncocytomas. Comput. Radiol. 1985, 9, 307–314. [Google Scholar] [CrossRef] [Green Version]
- Quinn, M.J.; Hartman, D.S.; Friedman, A.C.; Sherman, J.L.; Lautin, E.M.; Pyatt, R.S.; Ho, C.K.; Csere, R.; Fromowitz, F.B. Renal oncocytoma: New observations. Radiology 1984, 153, 49–53. [Google Scholar] [CrossRef]
- Cochand-Priollet, B.; Molinie, V.; Bougaran, J.; Bouvier, R.; Dauge-Geffroy, M.C.; Deslignières, S.; Fournet, J.C.; Gros, P.; Lesourd, A.; Saint-Andre, J.P.; et al. Renal chromophobe cell carcinoma and oncocytoma: A comparative morphologic, histochemical, and immunohistochemical study of 124 cases. Arch. Pathol. Lab. Med. 1997, 121, 1081–1086. [Google Scholar]
- Holdsworth, S.J.; Bammer, R. Magnetic resonance imaging techniques: fMRI, DWI, and PWI. Semin. Neurol. 2008, 28, 395–406. [Google Scholar] [CrossRef] [Green Version]
- Koh, D.M.; Collins, D.J. Diffusion-weighted MRI in the body: Applications and challenges in oncology. AJR Am. J. Roentgenol. 2007, 188, 1622–1635. [Google Scholar] [CrossRef] [Green Version]
- Metin, M.R.; Aydın, H.; Çetin, H.; Özmen, E.; Kayaçetin, S. The efficacy of diffusion weighted imaging and apparent diffusion coefficients mapping for liver metastasis of colonic adenocarcinomas. Saudi Med. J. 2016, 37, 379–385. [Google Scholar] [CrossRef]
- Taouli, B.; Thakur, R.K.; Mannelli, L.; Babb, J.S.; Kim, S.; Hecht, E.M.; Lee, V.S.; Israel, G.M. Renal lesions: Characterization with diffusion-weighted imaging versus contrast-enhanced MR imaging. Radiology 2009, 251, 398–407. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Cheng, L.; Zhang, X.; Wang, D.; Guo, A.; Gao, Y.; Ye, H. Renal cell carcinoma: Diffusion-weighted MR imaging for subtype differentiation at 3.0 T. Radiology 2010, 257, 135–143. [Google Scholar] [CrossRef]
- Anna, K.; Paschall, S.; Mirmomen, M.; Symons, R.; Pourmorteza, A.; Gautam, R.; Sahai, A.; Dwyer, A.J.; Merino, M.J.; Metwalli, A.R.; et al. Differentiating papillary type I RCC from clear cell RCC and oncocytoma: Application of whole lesion volumetric ADC measurement. Abdom. Radiol. 2018, 43, 2424–2430. [Google Scholar] [CrossRef]
- Kim, J.I.; Cho, J.Y.; Moon, K.C.; Lee, H.J.; Kim, S.H. Segmental enhancement inversion at biphasic multidetector CT: Characteristic finding of small renal oncocytoma. Radiology 2009, 252, 441–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bird, V.G.; Kanagarajah, P.; Morillo, G.; Caruso, D.J.; Ayyathurai, R.; Leveillee, R.; Jorda, M. Differentiation of oncocytoma and renal cell carcinoma in small renal masses (<4 cm): The role of 4-phase computerized tomography. World J. Urol. 2011, 29, 787–792. [Google Scholar] [CrossRef]
- Pierorazio, P.M.; Hyams, E.S.; Tsai, S.; Feng, Z.; Trock, B.J.; Mullins, J.K.; Johnson, P.T.; Fishman, E.K.; Allaf, M.E. Multiphasic enhancement patterns of small renal masses (≤4 cm) on preoperative computed tomography: Utility for distinguishing subtypes of renal cell carcinoma, angiomyolipoma, and oncocytoma. Urology 2013, 81, 1265–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, J.R.; Coy, H.; Kim, H.J.; Douek, M.; Lo, P.; Pantuck, A.J.; Raman, S.S. Performance of relative enhancement on multiphasic MRI for the differentiation of clear cell renal cell carcinoma (RCC) from papillary and chromophobe RCC subtypes and oncocytoma. AJR Am. J. Roentgenol. 2017, 208, 812–819. [Google Scholar] [CrossRef] [PubMed]
- Galmiche, C.; Bernhard, J.C.; Yacoub, M.; Ravaud, A.; Grenier, N.; Cornelis, F. Is multiparametric MRI useful for differentiating oncocytomas from chromophobe renal cell carcinomas? AJR Am. J. Roentgenol. 2017, 208, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Başara, I.A.; Altay, C.; Güler, E.; Çamlıdağ, I.; Harman, M.; Danacı, M.; Tuna, B.; Yörükoğlu, K.; Seçil, M. Discrimination of oncocytoma and chromophobe renal cell carcinoma using MRI. Diagn. Interv. Radiol. 2019, 25, 5–13. [Google Scholar] [CrossRef]
- Li, A.; Xing, W.; Li, H.; Hu, Y.; Hu, D.; Li, Z.; Kamel, I.R. Subtype differentiation of small (≤4 cm) solid renal mass using volumetric histogram analysis of DWI at 3-T MRI. AJR Am. J. Roentgenol. 2018, 211, 614–623. [Google Scholar] [CrossRef]
- Hötker, A.M.; Mazaheri, Y.; Wibmer, A.; Zheng, J.; Moskowitz, C.S.; Tickoo, S.K.; Russo, P.; Hricak, H.; Akın, O. Use of DWI in the differentiation of renal cortical tumors. AJR Am. J. Roentgenol. 2016, 206, 100–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafiee, M.J.; Haider, A.S.; Wong, A.; Lui, D.; Cameron, A.; Modhafar, A.; Fieguth, P.; Haider, M.A. Apparent ultra-high b-value diffusion-weighted image reconstruction via hidden conditional random fields. IEEE Trans. Med. Imaging 2015, 34, 1111–1124. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Xu, Q.; Dou, W.; Zhu, W.; Wu, J.; Chen, W.; Ye, J. Diffusion kurtosis imaging features of renal cell carcinoma: A preliminary study. Br. J. Radiol. 2021, 94, 20201374. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RCC | Oncocytoma | p | |||
|---|---|---|---|---|---|
| N | % | n | % | ||
| Sex | 0.616 | ||||
| Male | 90 | 70.9 | 16 | 76.2 | |
| Female | 37 | 29.1 | 5 | 23.8 | |
| Localization | 0.211 | ||||
| Right | 61 | 48.0 | 7 | 33.3 | |
| Left | 66 | 52.0 | 14 | 66.7 | |
| RCC | Oncocytoma | p | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Median | Range | Mean | SD | Median | Range | ||
| Age | 59.47 | 12.15 | 61.00 | 21.00–84.00 | 64.29 | 14.71 | 71.00 | 36.00–87.00 | 0.070 |
| Diameter of the mass | 49.07 | 27.86 | 40.00 | 12.00–130.00 | 39.05 | 19.60 | 37.00 | 15.00–90.00 | 0.135 |
| ADC | 1.15 | 0.73 | 1.10 | 0.18–7.70 | 1.55 | 0.53 | 1.40 | 0.50–2.80 | <0.001 |
| Contrasting index | 1.520 | 0.551 | 1.378 | 0.867–3.413 | 2.112 | 0.799 | 2.200 | 0.900–3.870 | 0.001 |
| Mean | SD | Median | Range | p | |
|---|---|---|---|---|---|
| Clear cell | 1.241 | 0.818 | 1.200 | 0.18–7.70 | 0.112 |
| Chromophobe | 0.929 | 0.296 | 0.900 | 0.49–1.50 | |
| Papillary | 0.950 | 0.447 | 0.800 | 0.22–2.40 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Metin, M.; Aydın, H.; Karaoğlanoğlu, M. Renal Cell Carcinoma or Oncocytoma? The Contribution of Diffusion-Weighted Magnetic Resonance Imaging to the Differential Diagnosis of Renal Masses. Medicina 2022, 58, 221. https://doi.org/10.3390/medicina58020221
Metin M, Aydın H, Karaoğlanoğlu M. Renal Cell Carcinoma or Oncocytoma? The Contribution of Diffusion-Weighted Magnetic Resonance Imaging to the Differential Diagnosis of Renal Masses. Medicina. 2022; 58(2):221. https://doi.org/10.3390/medicina58020221
Chicago/Turabian StyleMetin, Melike, Hasan Aydın, and Mustafa Karaoğlanoğlu. 2022. "Renal Cell Carcinoma or Oncocytoma? The Contribution of Diffusion-Weighted Magnetic Resonance Imaging to the Differential Diagnosis of Renal Masses" Medicina 58, no. 2: 221. https://doi.org/10.3390/medicina58020221