
Mind the Differences: How Diagnoses and Hospital Characteristics Influence Coordination in Cancer Patient Pathways

 ,
,  , and
, and
Abstract
:1. Introduction
1.1. The Lack of Contextual Understanding in Cancer Patient Pathway Implementation
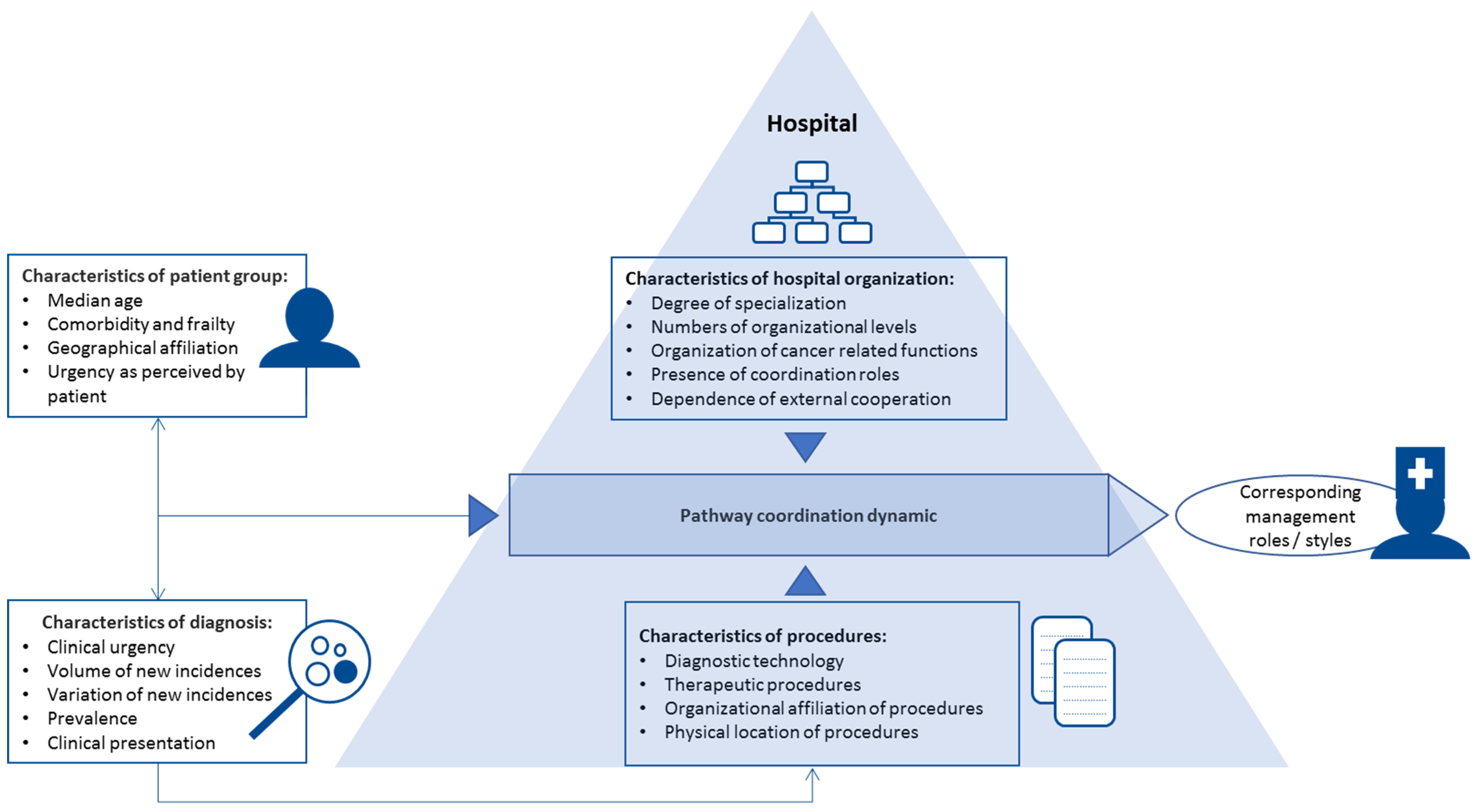
1.2. Analytical Approaches to Explore Understand Crucial Differences between CPP Processes
2. Materials and Methods
3. Results
3.1. Hospital-Related Variations
“Community hospital D is of the right size, there are short communication routes, there is the right number of specialties in the hospital, but still it’s easy to reach out to. It is not so big that you’ll lose track here. However, a hospital shouldn’t be too small because then there will be too few specialties and too few with cutting-edge competence.”(D4)
“I believe it’s simply that the silos are becoming bigger. When you’ve got more hospitals, each hospital can be seen as a silo. Then you’ve got smaller silos within the hospitals. So I believe it’s as simple as the organization is more complex, and that you have more of those lines or silos to deal with.”(A24)
“Specialization in the diagnostic functions and also the fact that we are allowed to be a distinctive elective hospital specialized in cancer care is extremely important. To run a business like this in addition to, for example, emergency operations would reduce the quality of care in my eyes. So we are, as we see it, extremely lucky to have the position we have.”(A22)
“That hybrid model is very difficult to handle. The acute care pathways destroys the whole planned structure that a top-notch competence need. Unpredictable, have to constantly run around. All the plans you’ve made, you must make again because they didn’t work. And we live with these challenges on a daily basis. And if you then collaborate closely with other areas that are more electively run and that have structure and order that also have local hospital patients, who will take care of them?”(C7)
“I saw the operational benefits of a sheltered elective arrangement. When you received referrals or attended an MDT meeting and planned four, six, eight weeks ahead in time, versus our internal arrangement where you experience these fluctuations that are not balanced to the acute flow of patients, but at least there was not the large amount of benign surgery where the waiting lists are 18 months for many patients no one want to operate. It’s surgery that means an intervention in their lives and should be planned well in advance. When we try long-term planning, the CPPs come and mess this up.”(A4)
“If there is someone you need to discuss or create an individual path for, you could just call and discuss and make an agreement, and that’s also how it works with the referring hospital, that is, if there’s anything they want, they’ll call. It does happen that one is unsure about something, that they’ll call from the community hospital and explain why they absolutely want to do it in that way.”(A4)
“In our hospital there are three persons who work with colorectal cancer as their primary task, and they know the environment at different locations in university hospital A, but in the management line there is not so much contact and I think that when we have a bottleneck, we would maybe benefit from having some arenas where the leaders could meet. The leader arenas that exist are clearly tied to level one or level two. There are not many meeting points at level three or four across the hospitals.”(B1)
“With metastatic colorectal cancer some of the patients are to have neoadjuvant chemotherapy so then there’s a consultation and the patients’ information is sent and the patients are discussed at an MDT meeting in university hospital A and then a path is planned, for example, if they are to have both rectal surgery and liver surgery and that they’ll get neoadjuvant treatment with us, and then a time path is created and in many ways I think that works very well.”(B1)
“We have regional meetings, so there is an oncologist in addition to a radiologist and a doctor from nuclear medicine and pathologist. And it depends what else we need. That is, if we need anesthesia or a gastro-intestinal surgeon or a sarcoma surgeon or any need in particular.”(C9)
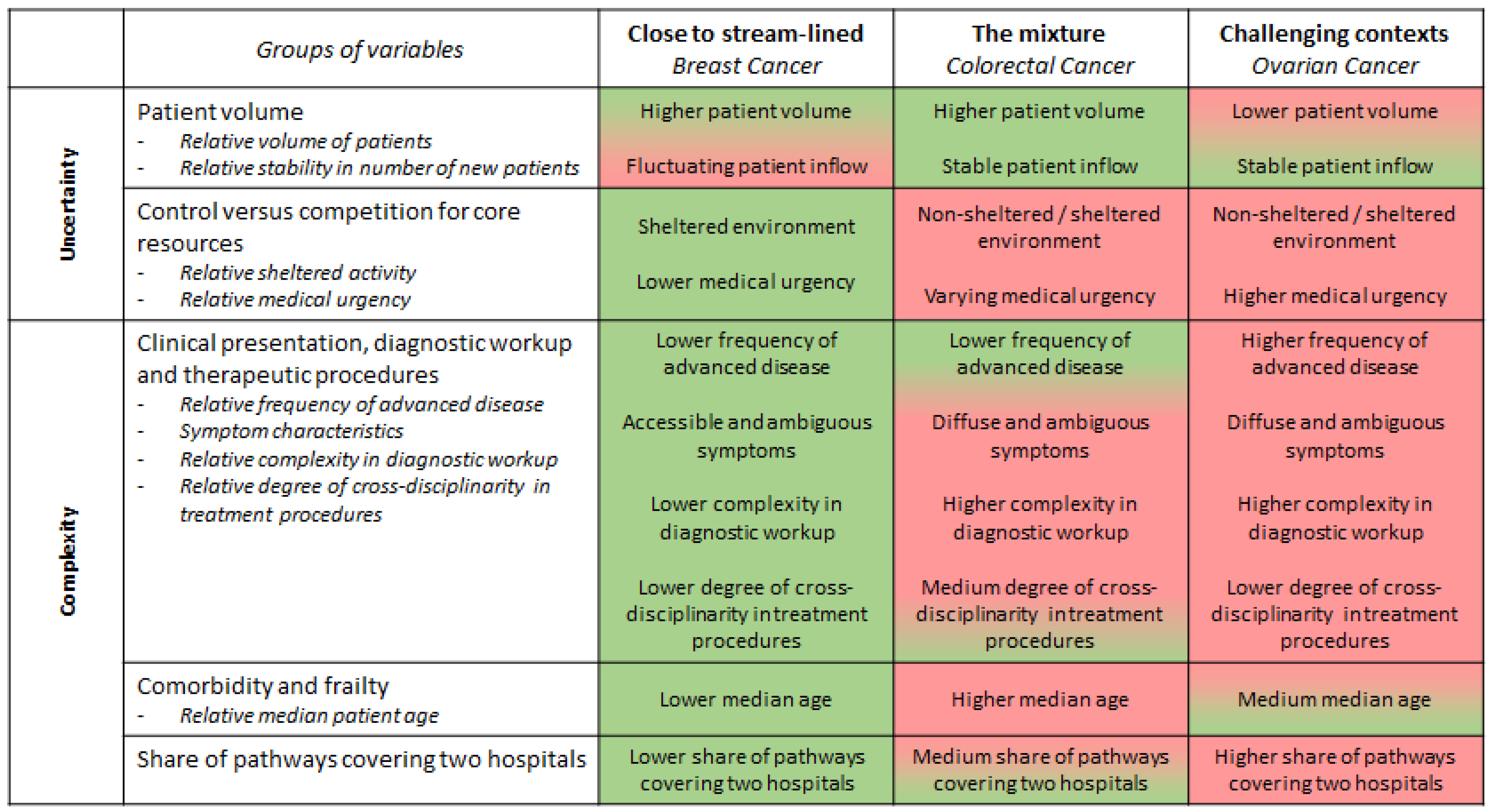
3.2. Diagnose Related Variation

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Breast Cancer [58] | Colorectal Cancer [59] | Ovarian Cancer [60] | |||
|---|---|---|---|---|---|
| Colon | Rectum | ||||
| Female, Male | Female, Male | ||||
| Incidence | Total | 3753 | 2979 | 1316 | 528 |
| 2019 | 1541, 1438 | 539, 777 | |||
| Screening | Women 50–69 years old [58] | 2019: no screening [59] | High risk-groups [60] | ||
| Fraction of patients by stage * 2015–2019 | I | 42.7% | 17.9%, 18.9% | 25.1%, 24.9% | 20.3% |
| II | 32.9% | ||||
| III | 10.6% | 52.1%, 51.3% | 44.7%, 46.2% | 20.7% | |
| IV | 4.1% | 22.3%, 23.3% | 19.3%, 19.4% | 52.0% | |
| Unknown | 9.8% | 7.7%, 6.5% | 10.8%, 9.5% | 7.0% | |
| Median age at diagnosis 2015–2019 | 62.0 | 73.0 | 70.0 | 67.0 | |
| 5-year relative survival by stage * 2015–2019 | Total | 92.0% | 71.1%, 68.1% | 71.5%, 71.1% | 50.3% |
| I | 100.9% | 98.9%, 98.3% | 96.1%, 98.0% | 97.4% | |
| II | 96.1% | ||||
| III | 79.4% | 85.4%, 84.4% | 80.8%, 82.3% | 61.9% | |
| IV | 34.0% | 20.8%, 15.1% | 24.0%, 20.4% | 37.1% | |
| Unknown | 78.2% | 35.3%, 31.4% | 46.0%, 46.3% | 40.5% | |
“Because I worked for a long time, I started with breast cancer and had both colorectal and breast cancer patients, and we had to get these breast cancer patients in before the colorectal cancer patients, because I believe it has to do with this is something you feel, it’s outside the body, and the breast cancer patients were more impatient than female colorectal patients who were more relaxed in a way.”(A2)
| Breast Cancer [58] | Colorectal Cancer [59] | Ovarian Cancer [60] | ||
|---|---|---|---|---|
| Colon | Rectum | |||
| Clinical presentation Characteristics and presentation of signs and symptoms | Visible or palpable lumps or changes in skin or tissue Changes seen on mammography screening | Ambiguous symptoms Tumor/polyp on ano-/rectoscopy/colonoscopy Acute intestinal perforation, bleeding or ileus | Ambiguous symptoms Acute ileus or thrombo-embolic event | |
| Diagnostic workup Essential procedures and technology | Triple diagnostics: Clinical examination Clinical mammography and/or ultrasound (radiologist) Fine-needle aspiration cytology (FNAC)/cyst puncture/core needle biopsy (CNB)/vacuum-assisted core biopsy (radiologist, examined by pathologist) If incomplete needle biopsy or malignant finding: Open biopsy (surgeon) Neoadjuvant treatment: MRI breast (radiologist) | Clinical examination with digital rectal exploration (DRE)/rectoscopy Colonoscopy with biopsy (gastroenterologist, examined by pathologist) If incomplete colonoscopy: CT-colography (supported by radiologist) For TNM * stage: CT thorax, abdomen and pelvis (radiologist) Acute presentation: CT abdomen and pelvis (radiologist) | Ano-rectoscopy with biopsy For TN * stage: High-res MRI with surface coils (radiologist) For T1/T2 * stage: Ultrasound rectum (surgeon) For M * status: CT thorax, abdomen and pelvis (radiologist) | CT thorax, abdomen and pelvis (radiologist) Blood sample Genetic test Clinical and gynecological examination with ultrasound (UL) (gynecologist) Calculation of Risk of Malignancy Index (gynecologist) Stage III-IV: UL-guided biopsy(gynecologist and radiologist, examined by pathologist) |
| Treatment Essential procedures | Conventional breast conservation surgery (BCT)/oncoplastic breast conservation surgery (OBCS)/ablation/mastectomy/sentinel lymph node biopsy (SNB)/axillary dissection (AD) Radiotherapy Adjuvant and neoadjuvant systemic therapy: Hormone therapy/ Chemotherapy/ Targeted medical therapy | Lymph node dissection/colon resection/dissection in circumference of tumor Adjuvant chemotherapy Acute presentation: Resection with or without anastomosis/ colostomy/stent | Total mesorectal excision (TME)/Partial mesorectal excision (PME) Neoadjuvant and adjvuvant therapy: Concomitant radiotherapy and chemotherapy | Cytoreductive surgery/fertility-preserving surgery Neoadjuvant and adjuvant chemotherapy |
| Palliative treatment: Palliative surgery Palliative radiotherapy | ||||
“It’s up to our department head to contact the head of the local gynecological department when something is not working, to put pressure on the person in question so that things go faster. But I have to say, it’s noticeable that for these departments, cancer is only a part of their task. They have a lot of births and do a lot of other things as well. So it’s not always the case that cancer is perceived to have the highest priority.”(A8)
“If we were more like a cancer hospital where we could have gastro surgeons, gastro oncologists and palliative professionals more integrated, so that the patients could stay with us like they do in other diagnosis groups like breast cancer, lymphoma, and sarcoma, they belong to the cancer department their whole pathway.”(C16)
“My perception is that many specialties are quite clear, such as what they say in community hospital D: “this is what we are doing here, and we are sending these patients away to the level above.” However, in radiology and laboratory, it has become the case that one has to be able to serve the whole spectrum—everything in diagnostics and controls regarding these patients. Even if the patient had been referred to a higher level of care, there is little to say about what we are doing. In a way, we have to follow them the whole pathway.”(D2B)
“Because our radiologists and pathologists are dedicated to one field, whereas if you work as a radiologist or pathologist in a community hospital, you need to know all sorts of stuff, which doesn’t make it strange that one can disagree and assess things differently.”(A8)
4. Discussion
4.1. Horizontal Coordination—Differences in Complexity and Predictability
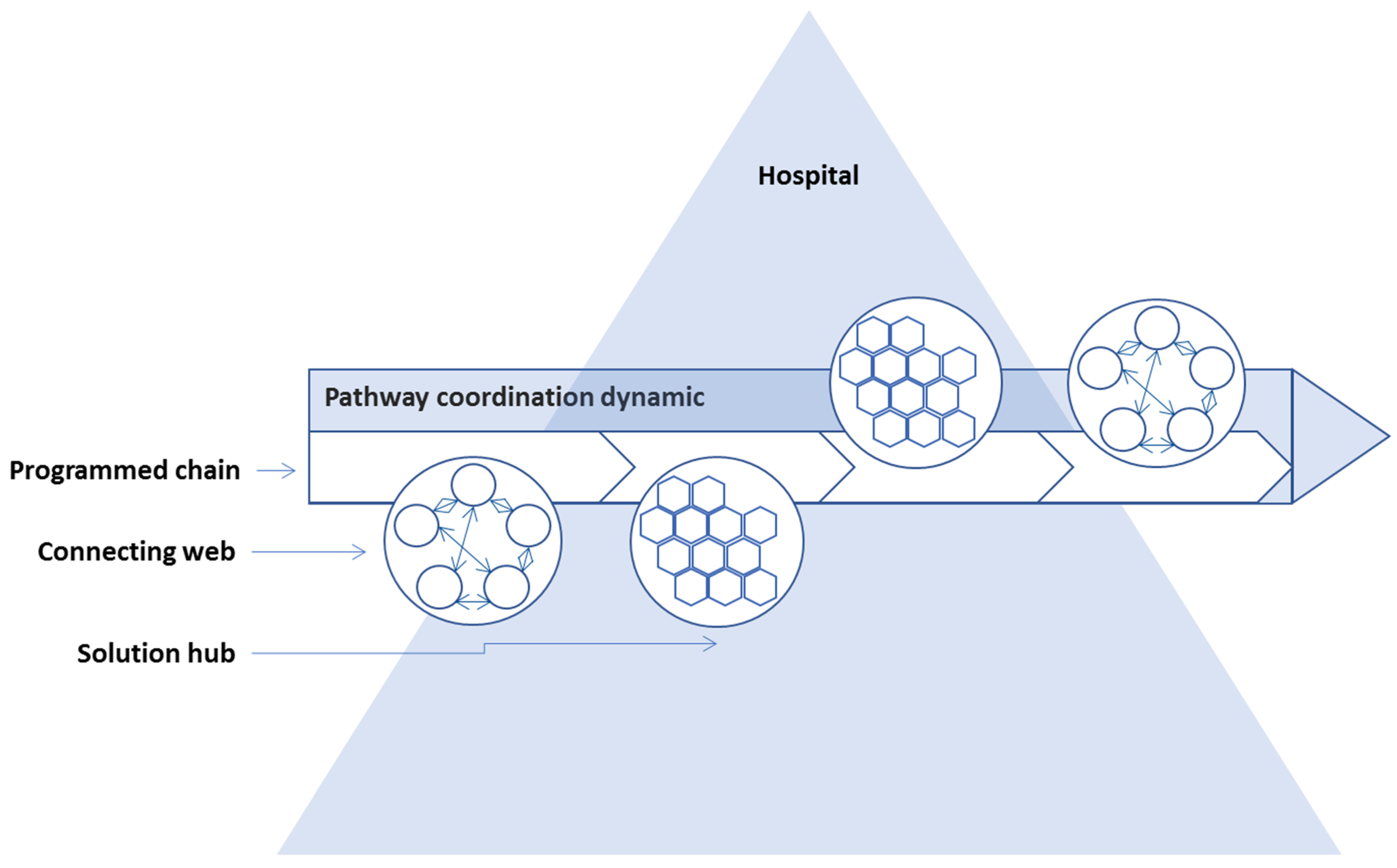
4.2. The Dynamic of Processes—Does One Pattern Fit All Patients, Pathways and Hospitals
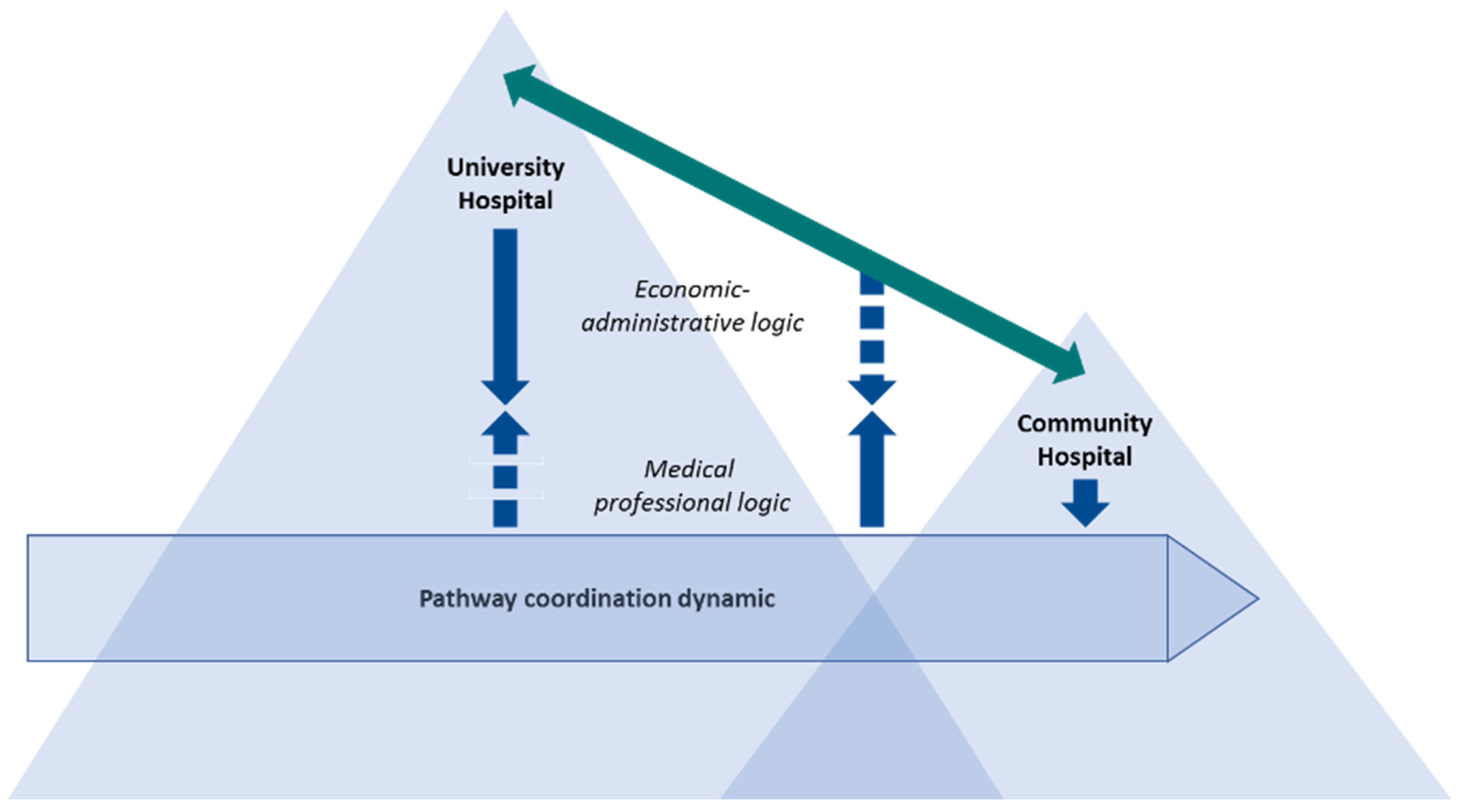
4.3. Characteristics of Hierarchical Coordination in and between Hospitals
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Trosman, J.R.; Carlos, R.C.; Simon, M.A.; Madden, D.L.; Gradishar, W.J.; Benson, A.B.; Rapkin, B.D.; Weiss, E.S.; Gareen, I.F.; Wagner, L.I.; et al. Care for a patient with cancer as a project: Management of complex task interdependence in cancer care delivery. J. Oncol. Pract. 2016, 12, 1101–1113. [Google Scholar] [CrossRef]
- Ouwens, M.; Wollersheim, H.; Hermens, R.; Hulscher, M.; Grol, R. Integrated care programmes for chronically ill patients: A review of systematic reviews. Int. J. Qual. Health Care 2005, 17, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Pless, S.; van Hootegem, G.; Dessers, E. Making care organizations great again? A comparison of care pathways, lean thinking, relational coordination, and modern sociotechnical design. Int. J. Care Coord. 2017, 20, 64–75. [Google Scholar] [CrossRef]
- Mintzberg, H. Structures in 5’s—A synthesis of the research on organization design. Manag. Sci. 1980, 26, 322–341. [Google Scholar] [CrossRef]
- Khan, A.I.; Arthurs, E.; Gradin, S.; MacKinnon, M.; Sussman, J.; Kukreti, V. Integrated care planning for cancer patients: A scoping review. Int. J. Integr. Care 2017, 17, 5. [Google Scholar] [CrossRef] [Green Version]
- Lawal, A.K.; Rotter, T.; Kinsman, L.; Machotta, A.; Ronellenfitsch, U.; Scott, S.D.; Goodridge, D.; Plishka, C.; Groot, G. What is a clinical pathway? Refinement of an operational definition to identify clinical pathway studies for a Cochrane systematic review. BMC Med. 2016, 14, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whittle, C.; Hewison, A. Integrated care pathways: Pathways to change in health care? J. Health Organ. Manag. 2007, 21, 297–306. [Google Scholar] [CrossRef]
- Martin, G.P.; Kocman, D.; Stephens, T.; Peden, C.J.; Pearse, R.M. Pathways to professionalism? Quality improvement, care pathways, and the interplay of standardisation and clinical autonomy. Sociol. Health Illn. 2017, 39, 1314–1329. [Google Scholar] [CrossRef] [Green Version]
- Seys, D.; Panella, M.; VanZelm, R.; Sermeus, W.; Aeyels, D.; Bruyneel, L.; Coeckelberghs, E.; Vanhaecht, K. Care pathways are complex interventions in complex systems: New european pathway association framework. Int. J. Care Coord. 2019, 22, 5–9. [Google Scholar] [CrossRef]
- Coffey, R.J.; Richards, J.S.; Remmert, C.S.; LeRoy, S.S.; Schoville, R.R.; Baldwin, P.J. An introduction to critical paths. Qual. Manag. Health Care. 2005, 14, 46–55. [Google Scholar] [CrossRef]
- Bohmer, R. Critical pathways at Massachusetts General Hospital. J. Vasc. Surg. 1998, 28, 373–377. [Google Scholar] [CrossRef] [Green Version]
- Morris, M.; Levenback, C.; Burke, T.W.; Dejesus, Y.; Lucas, K.R.; Gershenson, D.M. An outcomes management program in gynecologic oncology. Obstet. Gynecol. 1997, 89, 485–492. [Google Scholar] [CrossRef]
- Allen, D. Lost in translation? ‘Evidence’ and the articulation of institutional logics in integrated care pathways: From positive to negative boundary object? Sociol. Health Illn. 2014, 36, 807–822. [Google Scholar] [CrossRef] [PubMed]
- Dourish, P. Process descriptions as organisational accounting devices: The dual use of workflow technologies. In Proceedings of the Conference on Supporting Group Work ACM, Boulder, CO, USA, 30 September–3 October 2001; pp. 52–60. [Google Scholar]
- De Luc, K. Are different models of care pathways being developed? Int. J. Health Care Qual. Assur. 2000, 13, 80–87. [Google Scholar] [CrossRef]
- Vanhaecht, K.; Witte, K.D.; Depreitere, R.; Sermeus, W. Clinical pathway audit tools: A systematic review. J. Nurs. Manag. 2006, 14, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Vanhaecht, K.; de Witte, K.; Sermeus, W. The care process organization triangle: A framework to better understand how clinical pathways work. J. Integr. Care Pathw. 2007, 11, 54–61. [Google Scholar]
- Bragato, L.; Jacobs, K. Care pathways: The road to better health services? J. Health Organ Manag. 2003, 17, 164–180. [Google Scholar] [CrossRef] [PubMed]
- Schrijvers, G.; van Hoorn, A.; Huiskes, N. The care pathway: Concepts and theories: An introduction. Int. J. Integr. Care 2012, 12, e192. [Google Scholar] [CrossRef]
- Deneckere, S.; Euwema, M.; Van Herck, P.; Lodewijckx, C.; Panella, M.; Sermeus, W.; Vanhaecht, K. Care pathways lead to better teamwork: Results of a systematic review. Soc. Sci. Med. 2012, 75, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Pearson, S.D.; Goulart-Fisher, D.; Lee, T.H. Critical pathways as a strategy for improving care: Problems and potential. Ann. Intern. Med. 1995, 123, 941. [Google Scholar] [CrossRef]
- Parry, C.; Kent, E.E.; Forsythe, L.P.; Alfano, C.M.; Rowland, J.H. Can’t see the forest for the care plan: A call to revisit the context of care planning. J. Clin. Oncol. 2013, 31, 2651–2653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, D.; Gillen, E.; Rixson, L. Systematic review of the effectiveness of integrated care pathways: What works, for whom, in which circumstances? Int. J. Evid. Based Healthc. 2009, 7, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Dy, S.M.; Garg, P.; Nyberg, D.; Dawson, P.B.; Pronovost, P.J.; Morlock, L.; Rubin, H.; Wu, A.W. Critical pathway effectiveness: Assessing the impact of patient, hospital care, and pathway characteristics using qualitative comparative analysis. Health Serv. Res. 2005, 40, 499–516. [Google Scholar] [CrossRef]
- Mæhle, P.M.; Small Hanto, I.K.; Smeland, S. Practicing integrated care pathways in norwegian hospitals: Coordination through industrialized standardization, value chains, and quality management or an organizational equivalent to improvised jazz standards. Int. J. Environ. Res. Publ. Health 2020, 17, 9199. [Google Scholar] [CrossRef] [PubMed]
- Checkland, K.; Hammond, J.; Allen, P.; Coleman, A.; Warwick-Giles, L.; Hall, A.; MAYS, N.; SUTTON, M. Road to Nowhere? A Critical Consideration of the Use of the Metaphor ‘Care Pathway’ in Health Services Planning, Organisation and Delivery. J. Soc. Policy 2019, 42, 1–20. [Google Scholar] [CrossRef]
- Shiell, A.; Hawe, P.; Gold, L. Complex interventions or complex systems? Implications for health economic evaluation. BMJ 2008, 336, 1281–1283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinder, R.; Petchey, R.; Shaw, S.; Carter, Y. What’s in a care pathway? Towards a cultural cartography of the new NHS. Sociol. Health Illn. 2005, 27, 759–779. [Google Scholar] [CrossRef]
- Helsedirektoratet. Implementering av Pakkeforløp for Kreft; Helsedirektoratet: Oslo, Norway, 2014. [Google Scholar]
- Mæhle, P.M.; Hajdarevic, S.; Håland, E.; Aarhus, R.; Smeland, S.; Mørk, B.E. Exploring the triggering process of a cancer care reform in three Scandinavian countries. Int. J. Health Plan. Manag. 2021, 1–17. [Google Scholar] [CrossRef]
- Han, P.K.J.; Klein, W.M.P.; Arora, N.K. Varieties of uncertainty in health care: A conceptual taxonomy. Med. Decis. Mak. 2011, 31, 828–838. [Google Scholar] [CrossRef]
- Slack, N.; Brandon-Jones, A.; Johnston, R. Operations Management, 7th ed.; Pearson: Harlow, UK, 2013. [Google Scholar]
- Larson, E.W.; Gray, C.F. Project Management: The Managerial Process, 8th ed.; McGraw-Hill Education: New York, NY, USA, 2021. [Google Scholar]
- Djulbegovic, B.; Hozo, I.; Dale, W. Transforming clinical practice guidelines and clinical pathways into fast-and-frugal decision trees to improve clinical care strategies.(Report). J. Eval. Clin. Pract. 2018, 24, 1247. [Google Scholar] [CrossRef]
- Campbell, H.; Hotchkiss, R.; Bradshaw, N.; Porteous, M. Integrated care pathways. Br. Med. J. Publ. Gr. 1998, 316, 133–137. [Google Scholar] [CrossRef] [Green Version]
- Van Dam, P.A.; Verheyden, G.; Sugihara, A.; Trinh, X.B.; Van Der Mussele, H.; Wuyts, H.; Verkinderen, L.; Hauspy, J.; Vermeulen, P.; Dirix, L. A dynamic clinical pathway for the treatment of patients with early breast cancer is a tool for better cancer care: Implementation and prospective analysis between 2002–2010. World J. Surg. Oncol. 2013, 11, 70. [Google Scholar] [CrossRef] [Green Version]
- Zuiderent-Jerak, T. Situated Intervention: Sociological Experiments in Health Care; The MIT Press: Cambridge, MA, USA, 2015. [Google Scholar]
- Llewellyn, H.; Higgs, P.; Sampson, E.L.; Jones, L.; Thorne, L. Topographies of ‘care pathways’ and ‘healthscapes’: Reconsidering the multiple journeys of people with a brain tumour. Soc. Health Illn. 2018, 40, 410–425. [Google Scholar] [CrossRef]
- Fjeldstad, Ø.D.; Johnson, J.K.; Margolis, P.A.; Seid, M.; Höglund, P.; Batalden, P.B. Networked health care: Rethinking value creation in learning health care systems. Learn. Health Syst. 2020, 4, e10212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, D.; Thompson, J.E.; Habermann, E.B.; Visscher, S.L.; Dearani, J.A.; Roger, V.L.; Borah, B.J. From ‘solution shop’ model to ‘focused factory’ in hospital surgery: Increasing care value and predictability. Health Aff. (Millwood) 2014, 33, 746–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glouberman, S.; Mintzberg, H. Managing the care of health and the cure of disease—Part II: Integration. Health Care Manag. Rev. 2001, 26, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, R.; Raynard, M.; Kodeih, F.; Micoletta, E.R.; Lounsbury, M.M. Institutional Complexity and Organizational Responses. Accademy Manag. Ann. 2011, 5, 317–371. [Google Scholar] [CrossRef]
- Alford, R.R.; Friedland, R. Powers of Theory Capitalism, the State, and Democracy; Cambridge University Press: Cambridge, MA, USA, 1985. [Google Scholar]
- Shaw, J.A.; Kontos, P.; Martin, W.; Victor, C. The institutional logic of integrated care: An ethnography of patient transitions. J. Health Organ. Manag. 2017, 31, 82–95. [Google Scholar] [CrossRef] [Green Version]
- Ranmuthugala, G.; Plumb, J.J.; Cunningham, F.C.; Georgiou, A.; Westbrook, J.I.; Braithwaite, J. How and why are communities of practice established in the healthcare sector? A systematic review of the literature. BMC Health Serv. Res. 2011, 11, 273–289. [Google Scholar] [CrossRef] [Green Version]
- Delilovic, S.; Hasson, H.; Åhström, M.; von Knorring, M. Implementing standardized cancer patient pathways (CPPs)—A qualitative study exploring the perspectives of health care professionals. BMC Health Serv. Res. 2019, 19, 577. [Google Scholar] [CrossRef]
- Buchanan, D.A.; Addicott, R.; Fitzgerald, L.; Ferlie, E.; Baeza, J.I. Nobody in charge: Distributed change agency in healthcare. Hum. Relat. 2007, 60, 1065–1090. [Google Scholar] [CrossRef]
- Plowman, D.A.; Solansky, S.; Beck, T.E.; Baker, L.; Kulkarni, M.; Travis, D.V. The role of leadership in emergent, self-organization. Leadersh. Q. 2007, 18, 341–356. [Google Scholar] [CrossRef] [Green Version]
- Vilkinas, T.; Murray, D.W.; Chua, S.M.Y. Effective leadership: Considering the confluence of the leader’s motivations, behaviours and their reflective ability. Leadersh. Organ. Dev. J. 2020, 41, 147–163. [Google Scholar] [CrossRef]
- Turner, J.R.; Keegan, A. Mechanisms of governance in the project-based organization: Roles of the broker and steward. Eur. Manag. J. 2001, 19, 254–267. [Google Scholar] [CrossRef]
- Berwick, D.M. The Science of Improvement. JAMA 2008, 299, 1182–1184. [Google Scholar] [CrossRef]
- Vugts, M.A.P.; Liu, H.; Boumans, J.; Boydell, E. The need for theory-based evaluation of care coordination initiatives: Considerations from the 2017 International Conference on Realist Research, Evaluation and Synthesis. Int. J. Care Coord. 2018, 21, 61–67. [Google Scholar] [CrossRef]
- Green, J.T. Nicki Qualitative Methods for Health Research, 4th ed.; Sage: London, UK, 2018. [Google Scholar]
- May, C.; Finch, T.; Mair, F.; Ballini, L.; Dowrick, C.; Eccles, M.; Gask, L.; MacFarlane, A.; Murray, E.; Rapley, T.; et al. Understanding the implementation of complex interventions in health care: The normalization process model. BMC Health Serv. Res. 2007, 7, 148. [Google Scholar] [CrossRef] [PubMed]
- Timmermans, S.; Tavory, I. Theory construction in qualitative research: From grounded theory to abductive analysis. Sociol. Theory 2012, 30, 167–186. [Google Scholar] [CrossRef]
- Dash Board standardized Cancer Patient Pathways. Available online: https://statistikk.helsedirektoratet.no/bi/Dashboard/71613538-62de-4ab2-8409-8638fc6c25db?e=false&vo=viewonly (accessed on 4 April 2021).
- Cancer in Norway 2019; Cancer Registry of Norway: Oslo, Norway, 2020.
- National Program for Breast Cancer: Guide Lines for Diagnostics, Treatment and Follow-Up; Norwegian Directorate of Health: Oslo, Norway, 2019.
- National Program for Colorectal Cancer: Guide Lines for Diagnostics, Treatment and Follow-Up; Norwegian Directorate of Health: Oslo, Norway, 2020.
- National Program for Ovarian Cancer: Guide Lines for Diagnostics, Treatment and Follow-Up; Norwegian Directorate of Health: Oslo, Norway, 2020.
- Kolbjørnsrud, V. Agency problems and governance mechanisms in collaborative communities. Strateg. Organ. 2017, 15, 141–173. [Google Scholar] [CrossRef]
- Axelsson, R.; Axelsson, S.B. Integration and collaboration in public health—A conceptual framework. Int. J. Health Plan. Manag. 2006, 21, 75–88. [Google Scholar] [CrossRef]




| Hospital 1 | Hospital 2 | Hospital 3 | Hospital 4 | Total | |
|---|---|---|---|---|---|
| Ovarian cancer | 5 | 4 | 2 | 1 | 12 |
| Breast cancer | 6 | 4 | 2 | 1 | 13 |
| Colorectal cancer | 10 | 9 | 4 | 3 | 26 |
| Two or three cancers | 3 | 1 | 4 | 7 | 15 |
| Total | 24 | 18 | 12 | 12 | 66 |
| General Characteristics | University Hospital A | Community Hospital B | University Hospital C | Community Hospital D |
|---|---|---|---|---|
| No of patients newly diagnosed with all cancers | 4715 | 1340 | 2545 | 513 |
| Population served | Local: 550,000 Regional: 3,000,000 | Local: 250,000 | Local: 460,000 Regional: 1,100,000 | Local: 110,000 |
| No of patients starting standardized CPPs | 5985 | 3134 | 4235 | 1005 |
| No of organizational levels involved | 4–5 levels | 4 levels | 3 levels | 3 levels |
| No of units involved | Level 2: 12 of 15 units Level 3: 31 units | Level 2: 3 of 7 units | Level 2: 11 of 22 units | Level 2: 2 units Level 3: 7 units |
| No of cancer care sites | 4 sites | 1 site | 3 sites | 3 sites (2 satellites) |
| Coordinating function of cancer care | Cancer Center Board organized as a leadership matrix | Head of one division has a major coordinating role | The hospital management and medical director | Medical director coordinating role in problem-solving |
| Navigators organized in each department involved | Navigators organized in a centralized unit at hospital level | Navigators organized in each department involved | Navigators organized in a centralized unit at hospital level |
| University Hospital A | Community Hospital B | University Hospital C | Community Hospital D | |
|---|---|---|---|---|
| No of patients diagnosed with cancer | 588 | 223 | 412 | 66 |
| Variation in monthly number of patients starting standardized CPP | Average: 69 | Average: 35 | Average: 77 | Average: 14 |
| Max/Min: 84/52 | Max/Min: 47/19 | Max/Min: 113/40 | Max/Min: 23/7 | |
| No of patients in standardized pathway receiving their first cancer treatment | S *: 389 | S *: 157 | S *: 249 | S *: 48 |
| C *: 218 | C *: 15 | C *: 179 | C *: 18 | |
| Sum: 607 | Sum: 172 | Sum: 428 | Sum: 66 |
| University Hospital A | Community Hospital B | University Hospital C | Community Hospital D | |
|---|---|---|---|---|
| No of patients diagnosed with cancer | 330 | 230 | 186 | 95 |
| Variation in monthly number of patients starting standardized pathway | Average: 49 | Average: 73 | Average: 35 | Average: 21 |
| Max/Min: 64/36 | Max/Min: 91/60 | Max/Min: 43/13 | Max/Min: 29/12 | |
| No of patients in standardized pathway receiving their first cancer treatment | S *: 174 | S *: 161 | S *: 183 | S *: 61 |
| C *: 34 | C *: 15 | C *: 75 | C *: 11 | |
| R *: 138 | R *: 0 | R *: 62 | R *: 1 | |
| Sum: 346 | Sum: 176 | Sum: 320 | Sum: 73 |
| University Hospital A | Community Hospital B | University Hospital C | Community Hospital D | |
|---|---|---|---|---|
| No diagnosed with cancer | 251 | 27 | 46 | 9 |
| Variation in monthly number of patients starting standardized pathway | Average: 14.6 | Average: 4.9 | Average: 6.2 | Average: 1.1 |
| Max/Min: 21/12 | Max/Min: 11/3 | Max/Min: 11/3 | Max/Min: 3/0 | |
| No of patients in standardized pathway receiving their first cancer treatment (surgery) | 175 | 59 | 75 | 13 |
| Breast Cancer | Colorectal Cancer | Ovarian Cancer | ||
|---|---|---|---|---|
| Colon | Rectum | |||
| Organization of referral and the diagnostic workup | Referrals to local hospitals by GPs, or after positive screening: Initial diagnostic workup in sheltered environment managed by radiologists Referrals to regional hospitals from local hospitals: Specialized diagnostic imaging in sheltered environment | Referrals to local and regional hospitals, from GPs or local hospitals: Diagnostic workup in general gastrointestinal department with allocated slots for CPPs, otherwise non-sheltered environment | Referrals from GPs, private providers and local hospitals: Suspected or detected in non-sheltered gynecology or gastro-medicine department Referrals to regional hospitals: Sheltered gynecological cancer departments | |
| Participants in MDT meetings | Radiologist, breast surgeon, pathologist and oncologist (except university hospital C) | Gastro surgeon, radiologist, oncologist, pathologist and, only in community hospital B, gastro-intestinal physician | Gynecologist, radiologist and pathologist | |
| Organization of treatment | Surgery: Specialized surgeons. Primary reconstructive surgery performed cross-disciplinary with plastic surgeons Regional breast cancer: Initial oncological treatment demanding close dialogue between oncologist and surgeon | Local colon cancer: Surgery in community hospital also comprising other elective and acute diagnoses | Local rectum cancer: Surgery in community hospital also comprising other elective and acute diagnoses Regional rectum cancer: Possible cross-disciplinary surgery at regional hospital | Surgical and oncological treatment managed by specialized regional department for gynecological cancer |
| Metastases: Cross-disciplinary decision process in MDTs and possibly synchronic surgery if detected simultaneously | ||||
| Organization of state of remission follow-up | Surgery as primary treatment: Follow-up by breast surgeon at local hospital Neoadjuvant treatment: Follow-up by oncologist at local hospital | Surgery as first treatment: Follow-up by gastro surgeon at local hospital Neoadjuvant treatment: Follow-up by oncologist at local hospital Metastatic surgery or advanced rectum surgery at regional hospital: Follow-up by the treating unit | First follow-up by gynecological cancer unit at regional hospital and subsequently at local hospital | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mæhle, P.M.; Hanto, I.K.S.; Simensen, V.C.; Smeland, S. Mind the Differences: How Diagnoses and Hospital Characteristics Influence Coordination in Cancer Patient Pathways. Int. J. Environ. Res. Public Health 2021, 18, 8818. https://doi.org/10.3390/ijerph18168818
Mæhle PM, Hanto IKS, Simensen VC, Smeland S. Mind the Differences: How Diagnoses and Hospital Characteristics Influence Coordination in Cancer Patient Pathways. International Journal of Environmental Research and Public Health. 2021; 18(16):8818. https://doi.org/10.3390/ijerph18168818
Chicago/Turabian StyleMæhle, Per Magnus, Ingrid Kristine Small Hanto, Victoria Charlotte Simensen, and Sigbjørn Smeland. 2021. "Mind the Differences: How Diagnoses and Hospital Characteristics Influence Coordination in Cancer Patient Pathways" International Journal of Environmental Research and Public Health 18, no. 16: 8818. https://doi.org/10.3390/ijerph18168818