
Allergic Diseases: A Comprehensive Review on Risk Factors, Immunological Mechanisms, Link with COVID-19, Potential Treatments, and Role of Allergen Bioinformatics


Abstract
:1. Introduction
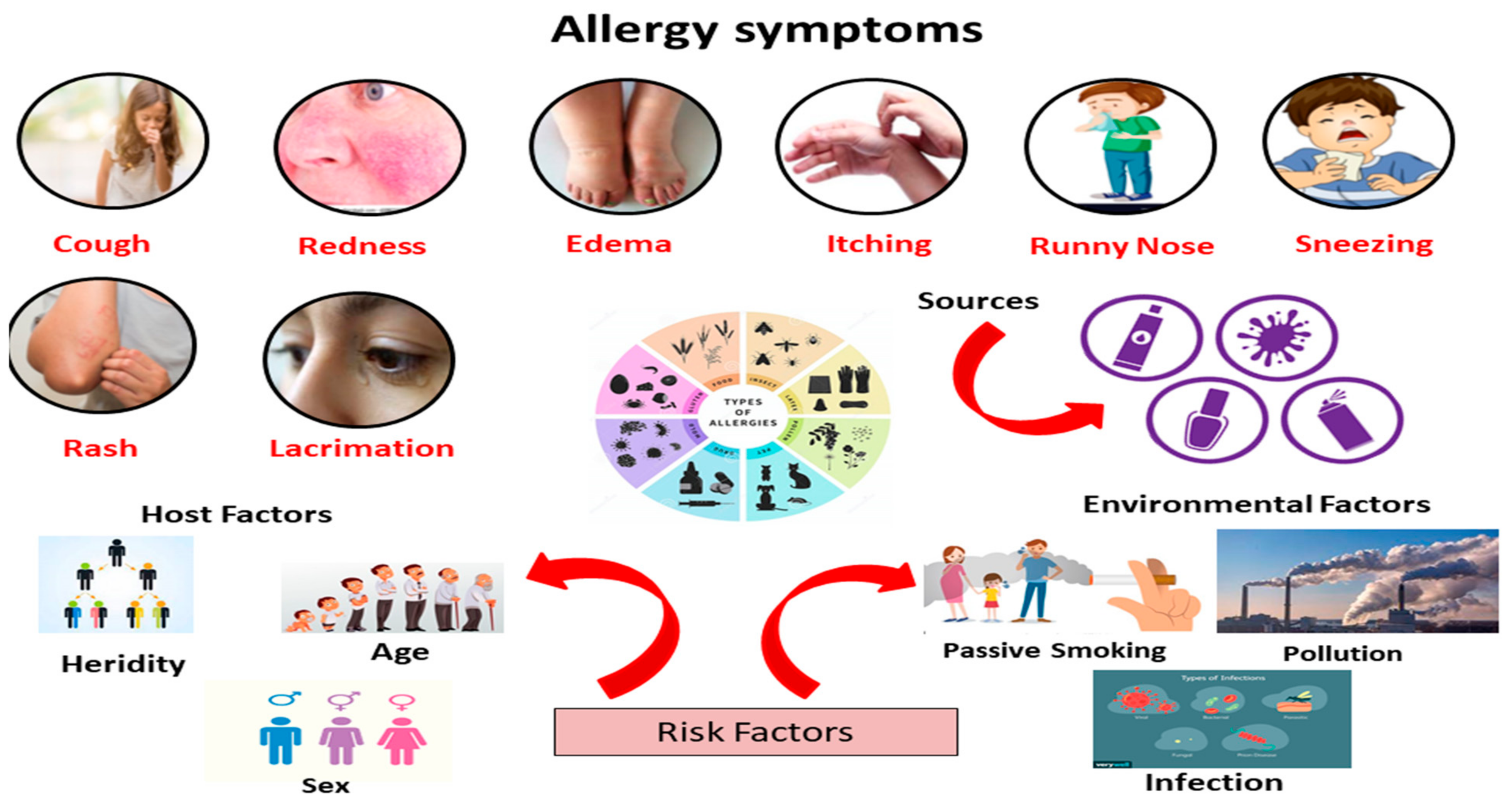
2. Signs and Symptoms
3. Epidemiology
4. Causes and Risk Factors of Allergy
4.1. Host Factors
4.1.1. Race
4.1.2. Heredity
4.1.3. Sex
4.1.4. Age
4.2. Environmental Factors
4.2.1. Passive Smoking
4.2.2. Pollution
4.2.3. Dietary Habits
4.2.4. Infections
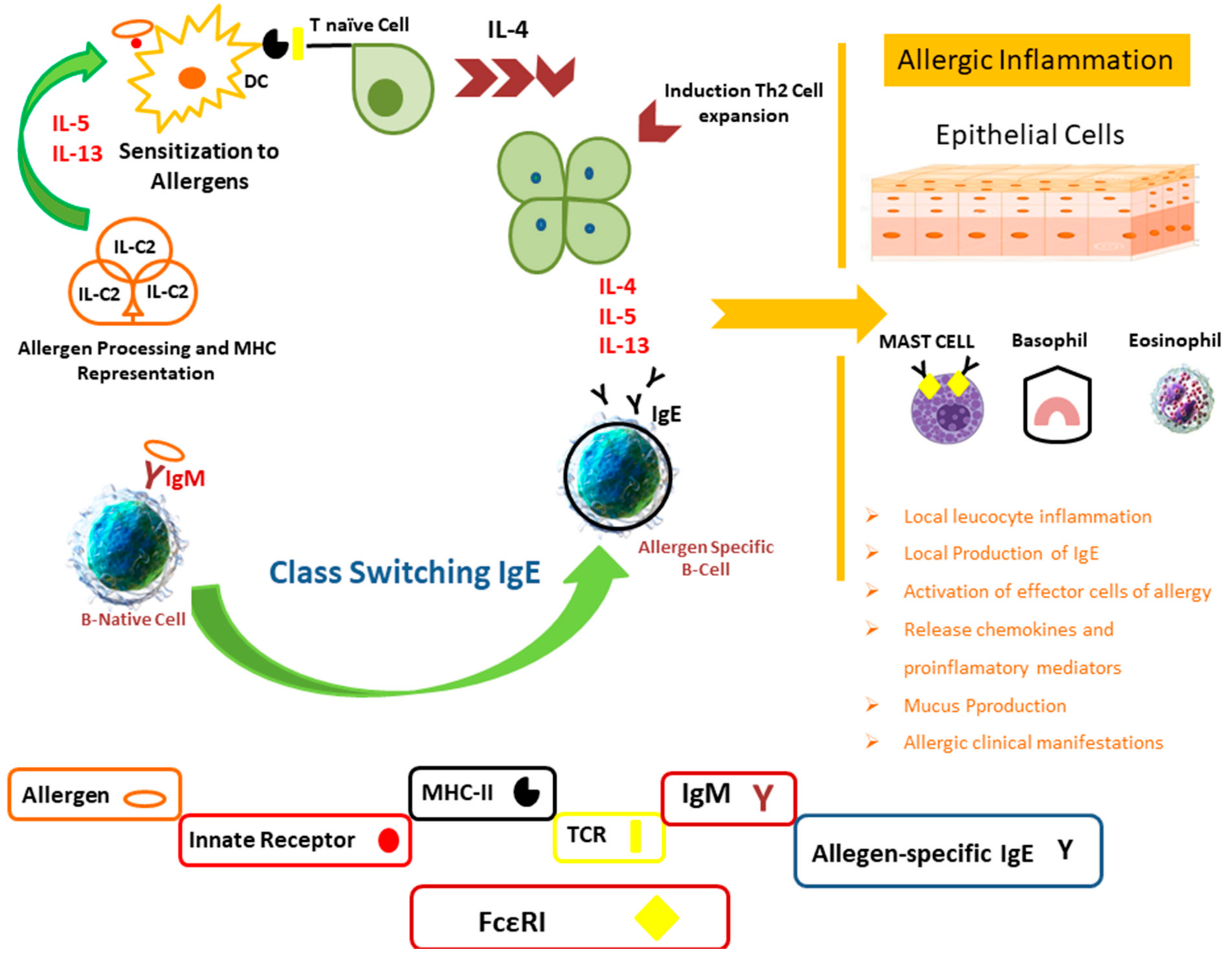
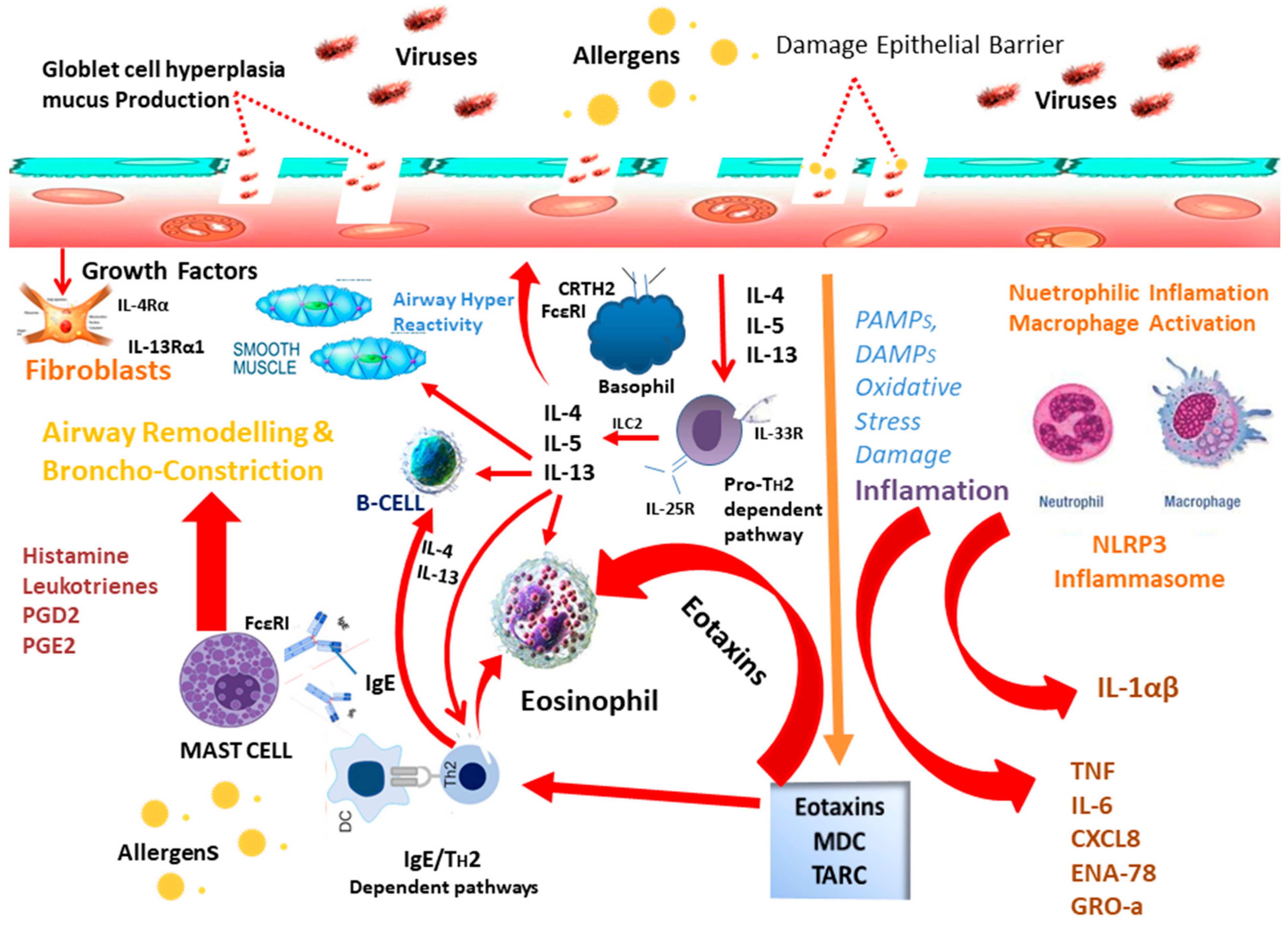
5. Mechanism of Allergy and Immune System
6. Allergy and Microbiota
7. Viral Infections in Allergy
7.1. Allergy Promoting Mechanism of Viruses
7.2. Allergy and COVID-19
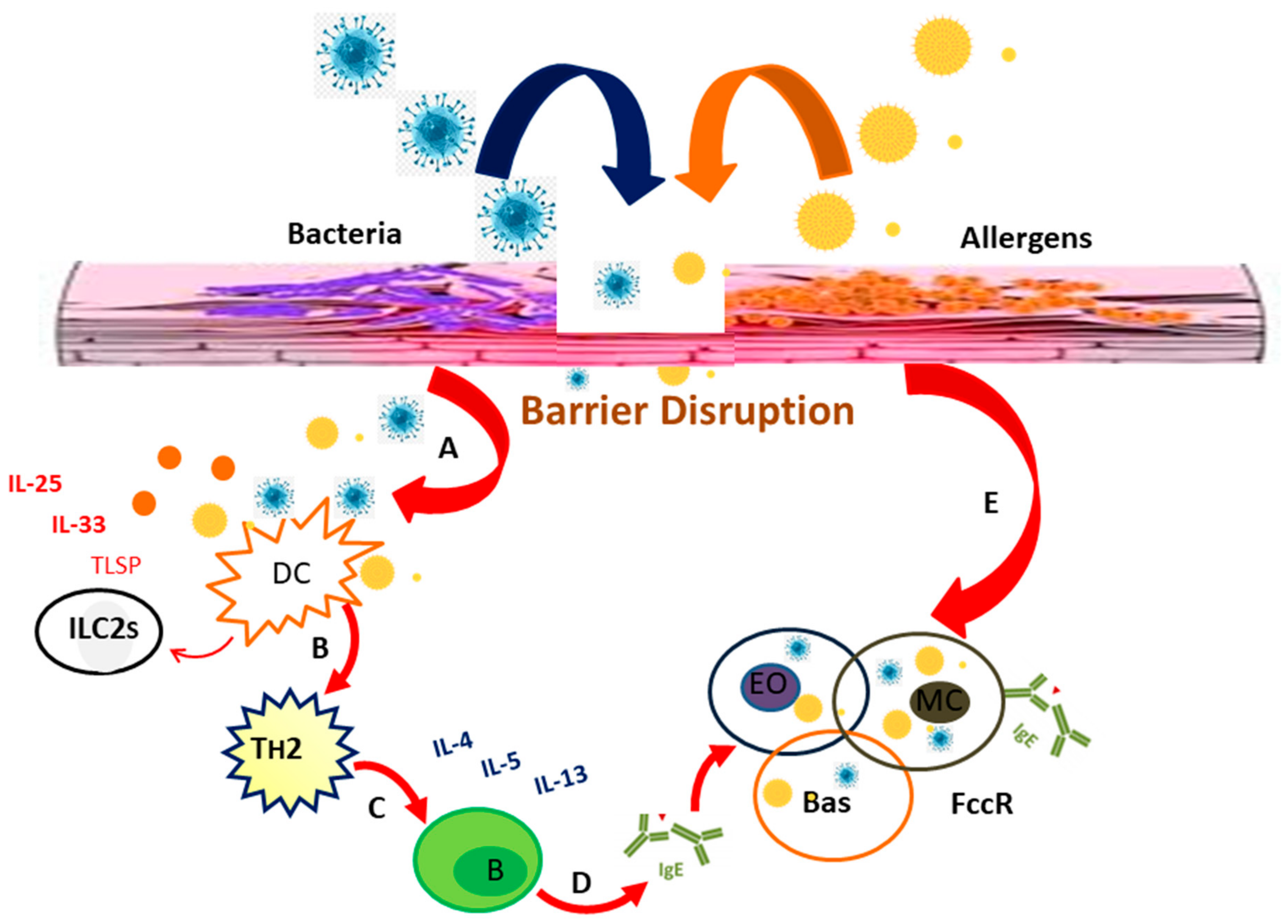
8. Bacterial Infections in Allergy
Allergy Promoting Mechanism of Bacteria
9. Treatments
9.1. Allergen Avoidance
9.2. Pharmacotherapy
9.3. Immunotherapy
9.4. Ineffective and Unproven Treatments
10. Role of Bioinformatics in Allergic Diseases Management
10.1. Allergen Cross-Reactivity Prediction
10.2. Allergen Databases
10.3. Allergen/Allergenicity Computational Prediction
10.4. Allergens Epitopes Computational Prediction
11. Conclusions and Future Perspectives
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Woodfolk, J.A.; Commins, S.P.; Schuyler, A.J.; Erwin, E.A.; Platts-Mills, T.A. Allergens, sources, particles, and molecules: Why do we make IgE responses? Allergol. Int. 2015, 64, 295–303. [Google Scholar] [CrossRef] [Green Version]
- Genuneit, J.; Seibold, A.M.; Apfelbacher, C.J.; Konstantinou, G.N.; Koplin, J.J.; La Grutta, S.; Logan, K.; Perkin, M.R.; Flohr, C. The Task Force ‘Overview of Systematic Reviews in Allergy Epidemiology (OSRAE)’ of the EAACI Interest Group on Epidemiology. Overview of systematic reviews in allergy epidemiology. Allergy 2017, 72, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Morgenstern, V.; Zutavern, A.; Cyrys, J.; Brockow, I.; Koletzko, S.; Kramer, U.; Behrendt, H.; Herbarth, O.; von Berg, A.; Bauer, C.P. Atopic diseases, allergic sensitization, and exposure to traffic-related air pollution in children. Am. J. Respir. Crit. Care Med. 2008, 177, 1331–1337. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.; Patiyal, S.; Dhall, A.; Pande, A.; Arora, C.; Raghava, G.P. AlgPred 2.0: An improved method for predicting allergenic proteins and mapping of IgE epitopes. Brief. Bioinform. 2021, 22, bbaa294. [Google Scholar] [CrossRef]
- Isaacs, K.K.; Goldsmith, M.-R.; Egeghy, P.; Phillips, K.; Brooks, R.; Hong, T.; Wambaugh, J.F. Characterization and prediction of chemical functions and weight fractions in consumer products. Toxicol. Rep. 2016, 3, 723–732. [Google Scholar] [CrossRef] [Green Version]
- Kimber, I.; Basketter, D.A.; Gerberick, G.F.; Ryan, C.A.; Dearman, R.J. Chemical allergy: Translating biology into hazard characterization. Toxicol. Sci. 2011, 120 (Suppl. 1), S238–S268. [Google Scholar] [CrossRef]
- Basu, S.; Banik, B. Hypersensitivity: An overview. Immunol. Curr. Res. 2018, 2, 1000105. [Google Scholar]
- Edwards, A. History of Allergy. In Allergy Frontiers: Diagnosis and Health Economics; Springer: Berlin/Heidelberg, Germany, 2009; pp. 3–19. [Google Scholar]
- Wani, N.A.; Mir, M.A.; Qayoom, H.; Mehraj, U.; Nisar, S.; Sheikh, B.A.; Suhail, S. Gell and coomb’s classification of hypersensitivity. In The Fundamentals of Hypersensitivities and Allergies; Nova Science Publishers Inc.: New York, NY, USA, 2020; pp. 35–74. [Google Scholar]
- Mir, M.A.; Mehraj, U.; Nisar, S.; Sheikh, B.A.; Suhail, S.; Qayoom, H. Hypersensitivity reaction. In The Fundamentals of Hypersensitivities and Allergies; Nova Science Publishers Inc.: New York, NY, USA, 2020; pp. 1–34. [Google Scholar]
- Platts-Mills, T.A. The continuing effect of the discovery of IgE by Kimishige Ishizaka. J. Allergy Clin. Immunol. 2018, 142, 788–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amarasekera, M. Immunoglobulin E in health and disease. Asia Pac. Allergy 2011, 1, 12–15. [Google Scholar] [CrossRef] [Green Version]
- Lei, D.K.; Grammer, L.C. An overview of allergens. Allergy Asthma Proc. 2019, 40, 362–365. [Google Scholar] [CrossRef]
- Baldacci, S.; Maio, S.; Cerrai, S.; Sarno, G.; Baïz, N.; Simoni, M.; Annesi-Maesano, I.; Viegi, G.; Study, H. Allergy and asthma: Effects of the exposure to particulate matter and biological allergens. Respir. Med. 2015, 109, 1089–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turnbull, J.; Adams, H.; Gorard, D. The diagnosis and management of food allergy and food intolerances. Aliment. Pharmacol. Ther. 2015, 41, 3–25. [Google Scholar] [CrossRef]
- Pramod, S.N. Immunological Basis for the Development of Allergic Diseases-Prevalence, Diagnosis and Treatment Strategies. In Cell Interaction-Molecular and Immunological Basis for Disease Management; IntechOpen: London, UK, 2021. [Google Scholar]
- Hossny, E.; Ebisawa, M.; El-Gamal, Y.; Arasi, S.; Dahdah, L.; El-Owaidy, R.; Galvan, C.A.; Lee, B.W.; Levin, M.; Martinez, S. Challenges of managing food allergy in the developing world. World Allergy Organ. J. 2019, 12, 100089. [Google Scholar] [CrossRef] [PubMed]
- Loh, W.; Tang, M.L. The epidemiology of food allergy in the global context. Int. J. Environ. Res. Public Health 2018, 15, 2043. [Google Scholar] [CrossRef] [Green Version]
- Wheatley, L.M.; Togias, A. Allergic Rhinitis. N. Engl. J. Med. 2015, 372, 456–463. [Google Scholar] [CrossRef] [Green Version]
- Hamid, Q.; Tulic, M. Immunobiology of asthma. Annu. Rev. Physiol. 2009, 71, 489–507. [Google Scholar] [CrossRef] [PubMed]
- Sicherer, S.H.; Sampson, H.A. Food allergy. J. Allergy Clin. Immunol. 2010, 125, S116–S125. [Google Scholar] [CrossRef]
- Incorvaia, C.; Frati, F.; Verna, N.; D’Alò, S.; Motolese, A.; Pucci, S. Allergy and the skin. Clin. Exp. Immunol. 2008, 153, 27–29. [Google Scholar] [CrossRef]
- Khan, D.A.; Solensky, R. Drug allergy. J. Allergy Clin. Immunol. 2010, 125, S126–S137.e1. [Google Scholar] [CrossRef]
- Golden, D.B. Insect allergy. In Middleton’s Allergy Essentials; Elsevier: Amsterdam, The Netherlands, 2017; pp. 377–393. [Google Scholar]
- Kemp, S.F.; Lockey, R.F. Anaphylaxis: A review of causes and mechanisms. J. Allergy Clin. Immunol. 2002, 110, 341–348. [Google Scholar] [CrossRef]
- Pawankar, R.; Canonica, G.W.; Holgate, S.T.; Lockey, R.F. Allergic diseases and asthma: A major global health concern. Curr. Opin. Allergy Clin. Immunol. 2012, 12, 39–41. [Google Scholar] [CrossRef]
- Wang, Z.; Sundy, J.S.; Foss, C.M.; Barnhart, H.X.; Palmer, S.M.; Allgood, S.D.; Trudeau, E.; Alexander, K.M.; Levesque, M.C. Racial differences in the association of CD14 polymorphisms with serum total IgE levels and allergen skin test reactivity. J. Asthma Allergy 2013, 6, 81–92. [Google Scholar] [CrossRef] [Green Version]
- Arbes Jr, S.J.; Gergen, P.J.; Elliott, L.; Zeldin, D.C. Prevalences of positive skin test responses to 10 common allergens in the US population: Results from the third National Health and Nutrition Examination Survey. J. Allergy Clin. Immunol. 2005, 116, 377–383. [Google Scholar] [CrossRef]
- Janumpally, S.R.; Feldman, S.R.; Gupta, A.K.; Fleischer, A.B. In the United States, blacks and Asian/Pacific Islanders are more likely than whites to seek medical care for atopic dermatitis. Arch. Dermatol. 2002, 138, 634–637. [Google Scholar] [CrossRef] [Green Version]
- Mahdavinia, M.; Tobin, M.C.; Fierstein, J.L.; Andy-Nweye, A.B.; Bilaver, L.A.; Fox, S.; Pappalardo, A.A.; Jiang, J.; Catlin, P.A.; Chura, A. African American Children Are More Likely to Be Allergic to Shellfish and Finfish: Findings from FORWARD, a Multisite Cohort Study. J. Allergy Clin. Immunol. Pract. 2021, 9, 2867–2873.e1. [Google Scholar] [CrossRef] [PubMed]
- Holt, P.; Macaubas, C.; Stumbles, P.; Sly, P. The role of allergy in the development of asthma. Nature 1999, 402, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Ownby, D.R. Environmental factors versus genetic determinants of childhood inhalant allergies. J. Allergy Clin. Immunol. 1990, 86, 279–287. [Google Scholar] [CrossRef]
- Knudsen, T.M.; Rezwan, F.I.; Jiang, Y.; Karmaus, W.; Svanes, C.; Holloway, J.W. Transgenerational and intergenerational epigenetic inheritance in allergic diseases. J. Allergy Clin. Immunol. 2018, 142, 765–772. [Google Scholar]
- Dor-Wojnarowska, A.; Liebhart, J.; Miecielica, J.; Rabski, M.; Fal, A.; Samoliński, B.; Nittner-Marszalska, M. The impact of sex and age on the prevalence of clinically relevant sensitization and asymptomatic sensitization in the general population. Arch. Immunol. Ther. Exp. 2017, 65, 253–261. [Google Scholar] [CrossRef] [Green Version]
- Fuseini, H.; Newcomb, D.C. Mechanisms driving gender differences in asthma. Curr. Allergy Asthma Rep. 2017, 17, 19. [Google Scholar]
- Dharma, C.; Lefebvre, D.; Tran, M.; Lou, W.; Subbarao, P.; Becker, A.; Mandhane, P.; Turvey, S.; Sears, M.; investigators, C.S. Patterns of allergic sensitization and atopic dermatitis from 1 to 3 years: Effects on allergic diseases. Clin. Exp. Allergy 2018, 48, 48–59. [Google Scholar] [CrossRef] [PubMed]
- van Aalderen, W.M. Childhood asthma: Diagnosis and treatment. Scientifica 2012, 2012, 674204. [Google Scholar] [CrossRef] [Green Version]
- Hammer-Helmich, L.; Linneberg, A.; Thomsen, S.F.; Glümer, C. Association between parental socioeconomic position and prevalence of asthma, atopic eczema and hay fever in children. Scand. J. Public Health 2014, 42, 120–127. [Google Scholar] [CrossRef]
- Myers, J.M.B.; Hershey, G.K.K. Eczema in early life: Genetics, the skin barrier, and lessons learned from birth cohort studies. J. Pediatr. 2010, 157, 704–714. [Google Scholar] [CrossRef] [Green Version]
- Sicherer, S.H. Clinical aspects of gastrointestinal food allergy in childhood. Pediatrics 2003, 111 (Suppl. 3), 1609–1616. [Google Scholar] [PubMed]
- Kim, Y.S.; Kim, H.Y.; Ahn, H.-S.; Sohn, T.S.; Song, J.Y.; Lee, Y.B.; Lee, D.-H.; Lee, J.-I.; Jeong, S.C.; Chae, H.S. The association between tobacco smoke and serum immunoglobulin E levels in Korean adults. Intern. Med. 2017, 56, 2571–2577. [Google Scholar]
- Metsälä, J.; Lundqvist, A.; Kaila, M.; Gissler, M.; Klaukka, T.; Virtanen, S.M. Maternal and perinatal characteristics and the risk of cow’s milk allergy in infants up to 2 years of age: A case-control study nested in the Finnish population. Am. J. Epidemiol. 2010, 171, 1310–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bendtsen, P.; Grønbaek, M.; Kjaer, S.; Munk, C.; Linneberg, A.; Tolstrup, J. Alcohol consumption and the risk of self-reported perennial and seasonal allergic rhinitis in young adult women in a population-based cohort study. Clin. Exp. Allergy 2008, 38, 1179–1185. [Google Scholar] [CrossRef]
- Cakir, E.; Ersu, R.; Uyan, Z.S.; Oktem, S.; Varol, N.; Karakoc, F.; Karadag, B.; Akyol, M.; Dagli, E. The prevalence and risk factors of asthma and allergic diseases among working adolescents. Asian Pac. J. Allergy Immunol. 2010, 28, 122. [Google Scholar]
- Lee, C.; Chuang, H.; Hong, C.; Huang, S.; Chang, Y.; Ko, Y.; Yu, H. Lifetime exposure to cigarette smoking and the development of adult-onset atopic dermatitis. Br. J. Dermatol. 2011, 164, 483–489. [Google Scholar] [CrossRef] [Green Version]
- McKeever, T.; Lewis, S.; Smith, C.; Collins, J.; Heatlie, H.; Frischer, M.; Hubbard, R. Siblings, multiple births, and the incidence of allergic disease: A birth cohort study using the West Midlands general practice research database. Thorax 2001, 56, 758–762. [Google Scholar] [CrossRef] [Green Version]
- Wang, I.-J.; Guo, Y.L.; Lin, T.-J.; Chen, P.-C.; Wu, Y.-N. GSTM1, GSTP1, prenatal smoke exposure, and atopic dermatitis. Ann. Allergy Asthma Immunol. 2010, 105, 124–129. [Google Scholar] [CrossRef]
- Saxon, A.; Diaz-Sanchez, D. Air pollution and allergy: You are what you breathe. Nat. Immunol. 2005, 6, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Strand, V.; Svartengren, M.; Rak, S.; Barck, C.; Bylin, G. Repeated exposure to an ambient level of NO2 enhances asthmatic response to a nonsymptomatic allergen dose. Eur. Respir. J. 1998, 12, 6–12. [Google Scholar] [CrossRef] [Green Version]
- Just, J.; Segala, C.; Sahraoui, F.; Priol, G.; Grimfeld, A.; Neukirch, F. Short-term health effects of particulate and photochemical air pollution in asthmatic children. Eur. Respir. J. 2002, 20, 899–906. [Google Scholar] [CrossRef] [Green Version]
- Lin, S.; Liu, X.; Le, L.H.; Hwang, S.-A. Chronic exposure to ambient ozone and asthma hospital admissions among children. Environ. Health Perspect. 2008, 116, 1725–1730. [Google Scholar] [CrossRef] [PubMed]
- Gent, J.F.; Triche, E.W.; Holford, T.R.; Belanger, K.; Bracken, M.B.; Beckett, W.S.; Leaderer, B.P. Association of low-level ozone and fine particles with respiratory symptoms in children with asthma. JAMA 2003, 290, 1859–1867. [Google Scholar] [CrossRef] [Green Version]
- Penttinen, P.; Vallius, M.; Tiittanen, P.; Ruuskanen, J.; Pekkanen, J. Source-specific fine particles in urban air and respiratory function among adult asthmatics. Inhal. Toxicol. 2006, 18, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Gauderman, W.J.; Avol, E.; Gilliland, F.; Vora, H.; Thomas, D.; Berhane, K.; McConnell, R.; Kuenzli, N.; Lurmann, F.; Rappaport, E. The effect of air pollution on lung development from 10 to 18 years of age. N. Engl. J. Med. 2004, 351, 1057–1067. [Google Scholar] [CrossRef] [Green Version]
- Ackermann-Liebrich, U.; Leuenberger, P.; Schwartz, J.; Schindler, C.; Monn, C.; Bolognini, G.; Bongard, J.; Brändli, O.; Domenighetti, G.; Elsasser, S. Lung function and long term exposure to air pollutants in Switzerland. Study on Air Pollution and Lung Diseases in Adults (SAPALDIA) Team. Am. J. Respir. Crit. Care Med. 1997, 155, 122–129. [Google Scholar] [CrossRef]
- Brauer, M.; Hoek, G.; Smit, H.; De Jongste, J.; Gerritsen, J.; Postma, D.S.; Kerkhof, M.; Brunekreef, B. Air pollution and development of asthma, allergy and infections in a birth cohort. Eur. Respir. J. 2007, 29, 879–888. [Google Scholar] [CrossRef] [PubMed]
- Melén, E.; Nyberg, F.; Lindgren, C.M.; Berglind, N.; Zucchelli, M.; Nordling, E.; Hallberg, J.; Svartengren, M.; Morgenstern, R.; Kere, J. Interactions between glutathione S-transferase P1, tumor necrosis factor, and traffic-related air pollution for development of childhood allergic disease. Environ. Health Perspect. 2008, 116, 1077–1084. [Google Scholar] [CrossRef] [Green Version]
- Nagel, G.; Weinmayr, G.; Kleiner, A.; Garcia-Marcos, L.; Strachan, D.P.; Group, I.P.T.S. Effect of diet on asthma and allergic sensitisation in the International Study on Allergies and Asthma in Childhood (ISAAC) Phase Two. Thorax 2010, 65, 516–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenheck, R. Fast food consumption and increased caloric intake: A systematic review of a trajectory towards weight gain and obesity risk. Obes. Rev. 2008, 9, 535–547. [Google Scholar] [CrossRef]
- Mai, X.M.; Becker, A.; Liem, J.; Kozyrskyj, A. Fast food consumption counters the protective effect of breastfeeding on asthma in children? Clin. Exp. Allergy 2009, 39, 556–561. [Google Scholar] [CrossRef]
- Mi, Y.; Norbäck, D.; Tao, J.; Mi, Y.; Ferm, M. Current asthma and respiratory symptoms among pupils in Shanghai, China: Influence of building ventilation, nitrogen dioxide, ozone, and formaldehyde in classrooms. Indoor Air 2006, 16, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Marcos, L.; Canflanca, I.M.; Garrido, J.B.; Varela, A.L.-S.; Garcia-Hernandez, G.; Grima, F.G.; Gonzalez-Diaz, C.; Carvajal-Uruena, I.; Arnedo-Pena, A.; Busquets-Monge, R.M. Relationship of asthma and rhinoconjunctivitis with obesity, exercise and Mediterranean diet in Spanish schoolchildren. Thorax 2007, 62, 503–508. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.L.; Pan, W.H. Dietary fats and asthma in teenagers: Analyses of the first Nutrition and Health Survey in Taiwan (NAHSIT). Clin. Exp. Allergy 2001, 31, 1875–1880. [Google Scholar] [CrossRef]
- Lawson, J.A.; Rennie, D.C.; Dosman, J.A.; Cammer, A.L.; Senthilselvan, A. Obesity, diet, and activity in relation to asthma and wheeze among rural dwelling children and adolescents. J. Obes. 2013, 2013. [Google Scholar] [CrossRef]
- Wang, C.S.; Wang, J.; Zhang, X.; Zhang, L.; Zhang, H.P.; Wang, L.; Wood, L.G.; Wang, G. Is the consumption of fast foods associated with asthma or other allergic diseases? Respirology 2018, 23, 901–913. [Google Scholar] [CrossRef] [PubMed]
- Ellwood, P.; Asher, M.; Björkstén, B.; Burr, M.; Pearce, N.; Robertson, C. Diet and asthma, allergic rhinoconjunctivitis and atopic eczema symptom prevalence: An ecological analysis of the International Study of Asthma and Allergies in Childhood (ISAAC) data. Eur. Respir. J. 2001, 17, 436–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.-C.; Yang, Y.-H.; Chuang, S.-Y.; Liu, S.-C.; Yang, H.-C.; Pan, W.-H. Risk of asthma associated with energy-dense but nutrient-poor dietary pattern in Taiwanese children. Asia Pac. J. Clin. Nutr. 2012, 21, 73–81. [Google Scholar] [PubMed]
- Gutiérrez-Delgado, R.I.; Barraza-Villarreal, A.; Escamilla-Núñez, M.C.; Solano-González, M.; Moreno-Macías, H.; Romieu, I. Food consumption and asthma in school children in Cuernavaca, Morelos, Mexico. Salud Publica Mex. 2009, 51, 202–211. [Google Scholar] [CrossRef] [Green Version]
- Farchi, S.; Forastiere, F.; Agabiti, N.; Corbo, G.; Pistelli, R.; Fortes, C.; Dell’Orco, V.; Perucci, C. Dietary factors associated with wheezing and allergic rhinitis in children. Eur. Respir. J. 2003, 22, 772–780. [Google Scholar] [CrossRef] [Green Version]
- Wickens, K.; Barry, D.; Friezema, A.; Rhodius, R.; Bone, N.; Purdie, G.; Crane, J. Fast foods–are they a risk factor for asthma? Allergy 2005, 60, 1537–1541. [Google Scholar] [CrossRef] [PubMed]
- Takaoka, M.; Norback, D. Diet among Japanese female university students and asthmatic symptoms, infections, pollen and furry pet allergy. Respir. Med. 2008, 102, 1045–1054. [Google Scholar] [CrossRef] [Green Version]
- Bueso, A.K.; Berntsen, S.; Mowinckel, P.; Andersen, L.F.; Lødrup Carlsen, K.C.; Carlsen, K.H. Dietary intake in adolescents with asthma—Potential for improvement. Pediatr. Allergy Immunol. 2011, 22 Pt. I, 19–24. [Google Scholar] [CrossRef]
- Sly, P.D.; Boner, A.L.; Björksten, B.; Bush, A.; Custovic, A.; Eigenmann, P.A.; Gern, J.E.; Gerritsen, J.; Hamelmann, E.; Helms, P.J. Early identification of atopy in the prediction of persistent asthma in children. Lancet 2008, 372, 1100–1106. [Google Scholar] [CrossRef] [Green Version]
- Jackson, D.J.; Evans, M.D.; Gangnon, R.E.; Tisler, C.J.; Pappas, T.E.; Lee, W.-M.; Gern, J.E.; Lemanske, R.F., Jr. Evidence for a causal relationship between allergic sensitization and rhinovirus wheezing in early life. Am. J. Respir. Crit. Care Med. 2012, 185, 281–285. [Google Scholar] [CrossRef] [Green Version]
- Holt, P.G.; Strickland, D.H.; Sly, P.D. Virus infection and allergy in the development of asthma: What is the connection? Curr. Opin. Allergy Clin. Immunol. 2012, 12, 151–157. [Google Scholar] [CrossRef]
- Jackson, D.J.; Gangnon, R.E.; Evans, M.D.; Roberg, K.A.; Anderson, E.L.; Pappas, T.E.; Printz, M.C.; Lee, W.-M.; Shult, P.A.; Reisdorf, E. Wheezing rhinovirus illnesses in early life predict asthma development in high-risk children. Am. J. Respir. Crit. Care Med. 2008, 178, 667–672. [Google Scholar] [CrossRef]
- Lemanske, R.F., Jr.; Jackson, D.J.; Gangnon, R.E.; Evans, M.D.; Li, Z.; Shult, P.A.; Kirk, C.J.; Reisdorf, E.; Roberg, K.A.; Anderson, E.L. Rhinovirus illnesses during infancy predict subsequent childhood wheezing. J. Allergy Clin. Immunol. 2005, 116, 571–577. [Google Scholar] [CrossRef]
- Jackson, D.J. Early Life Viral Infections and the Development of Asthma–A Target for Asthma Prevention? Curr. Opin. Allergy Clin. Immunol. 2014, 14, 131–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bisgaard, H.; Hermansen, M.N.; Bønnelykke, K.; Stokholm, J.; Baty, F.; Skytt, N.L.; Aniscenko, J.; Kebadze, T.; Johnston, S.L. Association of bacteria and viruses with wheezy episodes in young children: Prospective birth cohort study. BMJ 2010, 341, c4978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kloepfer, K.M.; Lee, W.M.; Pappas, T.E.; Kang, T.J.; Vrtis, R.F.; Evans, M.D.; Gangnon, R.E.; Bochkov, Y.A.; Jackson, D.J.; Lemanske, R.F., Jr. Detection of pathogenic bacteria during rhinovirus infection is associated with increased respiratory symptoms and asthma exacerbations. J. Allergy Clin. Immunol. 2014, 133, 1301–1307.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mills, K.H. Prior Exposure to Bacteria Attenuates Viral Disease of the Respiratory Tract: A Role for IL-17 and Innate Immune Memory? American Thoracic Society: New York, NY, USA, 2014. [Google Scholar]
- Calzada, D.; Baos, S.; Cremades, L.; Cardaba, B. New treatments for allergy: Advances in peptide immunotherapy. Curr. Med. Chem. 2018, 25, 2215–2232. [Google Scholar] [CrossRef] [PubMed]
- Soyer, O.; Akdis, M.; Ring, J.; Behrendt, H.; Crameri, R.; Lauener, R.; Akdis, C. Mechanisms of peripheral tolerance to allergens. Allergy 2013, 68, 161–170. [Google Scholar] [CrossRef]
- Akdis, C.A.; Akdis, M. Mechanisms of immune tolerance to allergens: Role of IL-10 and Tregs. J. Clin. Investig. 2014, 124, 4678–4680. [Google Scholar] [CrossRef] [Green Version]
- Shamji, M.H.; Durham, S.R. Mechanisms of allergen immunotherapy for inhaled allergens and predictive biomarkers. J. Allergy Clin. Immunol. 2017, 140, 1485–1498. [Google Scholar] [CrossRef] [Green Version]
- Larché, M.; Akdis, C.A.; Valenta, R. Immunological mechanisms of allergen-specific immunotherapy. Nat. Rev. Immunol. 2006, 6, 761–771. [Google Scholar] [CrossRef]
- Calzada, D.; Baos, S.; Cremades-Jimeno, L.; Cárdaba, B. Immunological mechanisms in allergic diseases and allergen tolerance: The role of treg cells. J. Immunol. Res. 2018, 2018, 6012053. [Google Scholar] [CrossRef] [PubMed]
- Hand, T.W.; Vujkovic-Cvijin, I.; Ridaura, V.K.; Belkaid, Y. Linking the microbiota, chronic disease, and the immune system. Trends Endocrinol. Metab. 2016, 27, 831–843. [Google Scholar] [CrossRef] [Green Version]
- Thaiss, C.A.; Levy, M.; Suez, J.; Elinav, E. The interplay between the innate immune system and the microbiota. Curr. Opin. Immunol. 2014, 26, 41–48. [Google Scholar] [CrossRef]
- Petrus, N.C.; Henneman, P.; Venema, A.; Mul, A.; van Sinderen, F.; Haagmans, M.; Mook, O.; Hennekam, R.C.; Sprikkelman, A.B.; Mannens, M. Cow’s milk allergy in Dutch children: An epigenetic pilot survey. Clin. Transl. Allergy 2016, 6, 16. [Google Scholar] [CrossRef] [Green Version]
- Kozakova, H.; Schwarzer, M.; Tuckova, L.; Srutkova, D.; Czarnowska, E.; Rosiak, I.; Hudcovic, T.; Schabussova, I.; Hermanova, P.; Zakostelska, Z. Colonization of germ-free mice with a mixture of three lactobacillus strains enhances the integrity of gut mucosa and ameliorates allergic sensitization. Cell. Mol. Immunol. 2016, 13, 251–262. [Google Scholar] [CrossRef]
- Hapfelmeier, S.; Lawson, M.A.; Slack, E.; Kirundi, J.K.; Stoel, M.; Heikenwalder, M.; Cahenzli, J.; Velykoredko, Y.; Balmer, M.L.; Endt, K. Reversible microbial colonization of germ-free mice reveals the dynamics of IgA immune responses. Science 2010, 328, 1705–1709. [Google Scholar] [CrossRef] [Green Version]
- Khor, B.; Gardet, A.; Xavier, R.J. Genetics and pathogenesis of inflammatory bowel disease. Nature 2011, 474, 307–317. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.J.; Marsland, B.J.; Bunyavanich, S.; O’Mahony, L.; Leung, D.Y.; Muraro, A.; Fleisher, T.A. The microbiome in allergic disease: Current understanding and future opportunities—2017 PRACTALL document of the American Academy of Allergy, Asthma & Immunology and the European Academy of Allergy and Clinical Immunology. J. Allergy Clin. Immunol. 2017, 139, 1099–1110. [Google Scholar] [PubMed] [Green Version]
- Canani, R.B.; De Filippis, F.; Nocerino, R.; Paparo, L.; Di Scala, C.; Cosenza, L.; Della Gatta, G.; Calignano, A.; De Caro, C.; Laiola, M. Gut microbiota composition and butyrate production in children affected by non-IgE-mediated cow’s milk allergy. Sci. Rep. 2018, 8, 12500. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Karlsson, C.; Olsson, C.; Adlerberth, I.; Wold, A.E.; Strachan, D.P.; Martricardi, P.M.; Åberg, N.; Perkin, M.R.; Tripodi, S. Reduced diversity in the early fecal microbiota of infants with atopic eczema. J. Allergy Clin. Immunol. 2008, 121, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, T.R.; Jakobsson, H.E.; Andersson, A.F.; Björkstén, B.; Engstrand, L.; Jenmalm, M.C. Low diversity of the gut microbiota in infants with atopic eczema. J. Allergy Clin. Immunol. 2012, 129, 434–440.e2. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.J.; Boushey, H.A. The microbiome in asthma. J. Allergy Clin. Immunol. 2015, 135, 25–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byrd, A.L.; Belkaid, Y.; Segre, J.A. The human skin microbiome. Nat. Rev. Microbiol. 2018, 16, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Paller, A.S.; Kong, H.H.; Seed, P.; Naik, S.; Scharschmidt, T.C.; Gallo, R.L.; Luger, T.; Irvine, A.D. The microbiome in patients with atopic dermatitis. J. Allergy Clin. Immunol. 2019, 143, 26–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nowak-Wegrzyn, A.; Szajewska, H.; Lack, G. Food allergy and the gut. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 241–257. [Google Scholar] [CrossRef]
- Sampson, H.A.; O’Mahony, L.; Burks, A.W.; Plaut, M.; Lack, G.; Akdis, C.A. Mechanisms of food allergy. J. Allergy Clin. Immunol. 2018, 141, 11–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arrieta, M.-C.; Stiemsma, L.T.; Dimitriu, P.A.; Thorson, L.; Russell, S.; Yurist-Doutsch, S.; Kuzeljevic, B.; Gold, M.J.; Britton, H.M.; Lefebvre, D.L. Early infancy microbial and metabolic alterations affect risk of childhood asthma. Sci. Transl. Med. 2015, 7, 307ra152. [Google Scholar] [CrossRef]
- Fujimura, K.E.; Sitarik, A.R.; Havstad, S.; Lin, D.L.; Levan, S.; Fadrosh, D.; Panzer, A.R.; LaMere, B.; Rackaityte, E.; Lukacs, N.W. Neonatal gut microbiota associates with childhood multisensitized atopy and T cell differentiation. Nat. Med. 2016, 22, 1187–1191. [Google Scholar] [CrossRef] [Green Version]
- Hilty, M.; Burke, C.; Pedro, H.; Cardenas, P.; Bush, A.; Bossley, C.; Davies, J.; Ervine, A.; Poulter, L.; Pachter, L. Disordered microbial communities in asthmatic airways. PLoS ONE 2010, 5, e8578. [Google Scholar] [CrossRef] [Green Version]
- Fazlollahi, M.; Chun, Y.; Grishin, A.; Wood, R.A.; Burks, A.W.; Dawson, P.; Jones, S.M.; Leung, D.Y.; Sampson, H.A.; Sicherer, S.H. Early-life gut microbiome and egg allergy. Allergy 2018, 73, 1515–1524. [Google Scholar] [CrossRef]
- Ege, M.; Mayer, M.; Schwaiger, K.; Mattes, J.; Pershagen, G.; Van Hage, M.; Scheynius, A.; Bauer, J.; Von Mutius, E. Environmental bacteria and childhood asthma. Allergy 2012, 67, 1565–1571. [Google Scholar] [CrossRef]
- Vickers, N.J. Animal communication: When I’m calling you, will you answer too? Curr. Biol. 2017, 27, R713–R715. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, T.; Jakobsson, H.; Andersson, A.F.; Björkstén, B.; Engstrand, L.; Jenmalm, M. Low gut microbiota diversity in early infancy precedes asthma at school age. Clin. Exp. Allergy 2014, 44, 842–850. [Google Scholar] [CrossRef] [Green Version]
- Eidelman, A.I.; Schanler, R.J. Breastfeeding and the use of human milk. Pediatrics 2012, 129, e827–e841. [Google Scholar]
- Matheson, M.; Allen, K.; Tang, M. Understanding the evidence for and against the role of breastfeeding in allergy prevention. Clin. Exp. Allergy 2012, 42, 827–851. [Google Scholar] [CrossRef] [PubMed]
- León-Cava, N.; Lutter, C.; Ross, J.; Martin, L. Quantifying the Benefits of Breastfeeding: A Summary of the Evidence; Pan American Health Organization: Washington, DC, USA, 2002. [Google Scholar]
- Oddy, W.H. Breastfeeding, childhood asthma, and allergic disease. Ann. Nutr. Metab. 2017, 70 (Suppl. 2), 26–36. [Google Scholar] [CrossRef] [PubMed]
- Muraro, A.; Dreborg, S.; Halken, S.; Høst, A.; Niggemann, B.; Aalberse, R.; Arshad, S.H.; Berg, A.v.; Carlsen, K.H.; Duschén, K. Dietary prevention of allergic diseases in infants and small children: Part III: Critical review of published peer-reviewed observational and interventional studies and final recommendations. Pediatric Allergy Immunol. 2004, 15, 291–307. [Google Scholar] [CrossRef]
- Gdalevich, M.; Mimouni, D.; Mimouni, M. Breast-feeding and the risk of bronchial asthma in childhood: A systematic review with meta-analysis of prospective studies. J. Pediatr. 2001, 139, 261–266. [Google Scholar] [CrossRef]
- Friedman, N.J.; Zeiger, R.S. The role of breast-feeding in the development of allergies and asthma. J. Allergy Clin. Immunol. 2005, 115, 1238–1248. [Google Scholar] [CrossRef]
- Kramer, M.S.; Matush, L.; Vanilovich, I.; Platt, R.; Bogdanovich, N.; Sevkovskaya, Z.; Dzikovich, I.; Shishko, G.; Mazer, B. Effect of prolonged and exclusive breast feeding on risk of allergy and asthma: Cluster randomised trial. Bmj 2007, 335, 815. [Google Scholar] [CrossRef] [Green Version]
- Wright, A.; Holberg, C.; Taussig, L.; Martinez, F. Factors influencing the relation of infant feeding to asthma and recurrent wheeze in childhood. Thorax 2001, 56, 192–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mihrshahi, S.; Ampon, R.; Webb, K.; Almqvist, C.; Kemp, A.; Hector, D.; Marks, G.B.; Team, C. The association between infant feeding practices and subsequent atopy among children with a family history of asthma. Clin. Exp. Allergy 2007, 37, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Sears, M.R.; Greene, J.M.; Willan, A.R.; Taylor, D.R.; Flannery, E.M.; Cowan, J.O.; Herbison, G.P.; Poulton, R. Long-term relation between breastfeeding and development of atopy and asthma in children and young adults: A longitudinal study. Lancet 2002, 360, 901–907. [Google Scholar] [CrossRef]
- Milani, C.; Duranti, S.; Bottacini, F.; Casey, E.; Turroni, F.; Mahony, J.; Belzer, C.; Delgado Palacio, S.; Arboleya Montes, S.; Mancabelli, L. The first microbial colonizers of the human gut: Composition, activities, and health implications of the infant gut microbiota. Microbiol. Mol. Biol. Rev. 2017, 81, e00036-17. [Google Scholar] [CrossRef] [Green Version]
- Bunyavanich, S.; Berin, M.C. Food allergy and the microbiome: Current understandings and future directions. J. Allergy Clin. Immunol. 2019, 144, 1468–1477. [Google Scholar] [CrossRef] [PubMed]
- Atarashi, K.; Tanoue, T.; Shima, T.; Imaoka, A.; Kuwahara, T.; Momose, Y.; Cheng, G.; Yamasaki, S.; Saito, T.; Ohba, Y. Induction of colonic regulatory T cells by indigenous Clostridium species. Science 2011, 331, 337–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, S.L.; Gold, M.J.; Hartmann, M.; Willing, B.P.; Thorson, L.; Wlodarska, M.; Gill, N.; Blanchet, M.R.; Mohn, W.W.; McNagny, K.M. Early life antibiotic-driven changes in microbiota enhance susceptibility to allergic asthma. EMBO Rep. 2012, 13, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Geuking, M.B.; Cahenzli, J.; Lawson, M.A.; Ng, D.C.; Slack, E.; Hapfelmeier, S.; McCoy, K.D.; Macpherson, A.J. Intestinal bacterial colonization induces mutualistic regulatory T cell responses. Immunity 2011, 34, 794–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, P.M.; Howitt, M.R.; Panikov, N.; Michaud, M.; Gallini, C.A.; Bohlooly-y, M.; Glickman, J.N.; Garrett, W.S. The microbial metabolites, short-chain fatty acids, regulate colonic Treg cell homeostasis. Science 2013, 341, 569–573. [Google Scholar] [CrossRef] [Green Version]
- Feehley, T.; Plunkett, C.H.; Bao, R.; Hong, S.M.C.; Culleen, E.; Belda-Ferre, P.; Campbell, E.; Aitoro, R.; Nocerino, R.; Paparo, L. Healthy infants harbor intestinal bacteria that protect against food allergy. Nat. Med. 2019, 25, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Gadir, A.; Stephen-Victor, E.; Gerber, G.K.; Rivas, M.N.; Wang, S.; Harb, H.; Wang, L.; Li, N.; Crestani, E.; Spielman, S. Microbiota therapy acts via a regulatory T cell MyD88/RORγt pathway to suppress food allergy. Nat. Med. 2019, 25, 1164–1174. [Google Scholar] [CrossRef]
- Berin, M.C. Dysbiosis in food allergy and implications for microbial therapeutics. J. Clin. Investig. 2021, 131, e144994. [Google Scholar] [CrossRef]
- Gern, J.E.; Rosenthal, L.A.; Sorkness, R.L.; Lemanske Jr, R.F. Effects of viral respiratory infections on lung development and childhood asthma. J. Allergy Clin. Immunol. 2005, 115, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Wark, P.; Johnston, S.; Moric, I.; Simpson, J.; Hensley, M.; Gibson, P. Neutrophil degranulation and cell lysis is associated with clinical severity in virus-induced asthma. Eur. Respir. J. 2002, 19, 68–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holtzman, M.J.; Morton, J.D.; Shornick, L.P.; Tyner, J.W.; O’Sullivan, M.P.; Antao, A.; Lo, M.; Castro, M.; Walter, M.J. Immunity, inflammation, and remodeling in the airway epithelial barrier: Epithelial-viral-allergic paradigm. Physiol. Rev. 2002, 82, 19–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gavala, M.L.; Bashir, H.; Gern, J.E. Virus/allergen interactions in asthma. Curr. Allergy Asthma Rep. 2013, 13, 298–307. [Google Scholar] [CrossRef] [Green Version]
- Fahy, J.V. Type 2 inflammation in asthma—Present in most, absent in many. Nat. Rev. Immunol. 2015, 15, 57–65. [Google Scholar] [CrossRef]
- Bizzintino, J.; Lee, W.; Laing, I.; Vang, F.; Pappas, T.; Zhang, G.; Martin, A.; Khoo, S.; Cox, D.; Geelhoed, G. Association between human rhinovirus C and severity of acute asthma in children. Eur. Respir. J. 2011, 37, 1037–1042. [Google Scholar] [CrossRef]
- Sigurs, N.; Gustafsson, P.M.; Bjarnason, R.; Lundberg, F.; Schmidt, S.; Sigurbergsson, F.; Kjellman, B. Severe respiratory syncytial virus bronchiolitis in infancy and asthma and allergy at age 13. Am. J. Respir. Crit. Care Med. 2005, 171, 137–141. [Google Scholar] [CrossRef]
- Khetsuriani, N.; Kazerouni, N.N.; Erdman, D.D.; Lu, X.; Redd, S.C.; Anderson, L.J.; Teague, W.G. Prevalence of viral respiratory tract infections in children with asthma. J. Allergy Clin. Immunol. 2007, 119, 314–321. [Google Scholar] [CrossRef]
- Arden, K.E.; Chang, A.B.; Lambert, S.B.; Nissen, M.D.; Sloots, T.P.; Mackay, I.M. Newly identified respiratory viruses in children with asthma exacerbation not requiring admission to hospital. J. Med. Virol. 2010, 82, 1458–1461. [Google Scholar] [CrossRef] [PubMed]
- Jackson, D.J.; Makrinioti, H.; Rana, B.M.; Shamji, B.W.; Trujillo-Torralbo, M.-B.; Footitt, J.; Del-Rosario, J.; Telcian, A.G.; Nikonova, A.; Zhu, J. IL-33–dependent type 2 inflammation during rhinovirus-induced asthma exacerbations in vivo. Am. J. Respir. Crit. Care Med. 2014, 190, 1373–1382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beale, J.; Jayaraman, A.; Jackson, D.J.; Macintyre, J.D.; Edwards, M.R.; Walton, R.P.; Zhu, J.; Ching, Y.M.; Shamji, B.; Edwards, M. Rhinovirus-induced IL-25 in asthma exacerbation drives type 2 immunity and allergic pulmonary inflammation. Sci. Transl. Med. 2014, 6, 256ra134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, M.R.; Strong, K.; Cameron, A.; Walton, R.P.; Jackson, D.J.; Johnston, S.L. Viral infections in allergy and immunology: How allergic inflammation influences viral infections and illness. J. Allergy Clin. Immunol. 2017, 140, 909–920. [Google Scholar] [CrossRef] [Green Version]
- Mehmood, I.; Ijaz, M.; Ahmad, S.; Ahmed, T.; Bari, A.; Abro, A.; Allemailem, K.S.; Almatroudi, A.; Tahir ul Qamar, M. SARS-CoV-2: An update on genomics, risk assessment, potential therapeutics and vaccine development. Int. J. Environ. Res. Public Health 2021, 18, 1626. [Google Scholar] [CrossRef]
- Alamri, M.A.; ul Qamar, M.T.; Afzal, O.; Alabbas, A.B.; Riadi, Y.; Alqahtani, S.M. Discovery of anti-MERS-CoV small covalent inhibitors through pharmacophore modeling, covalent docking and molecular dynamics simulation. J. Mol. Liq. 2021, 330, 115699. [Google Scholar] [CrossRef]
- Hosoki, K.; Chakraborty, A.; Sur, S. Molecular mechanisms and epidemiology of COVID-19 from an allergist’s perspective. J. Allergy Clin. Immunol. 2020, 146, 285–299. [Google Scholar] [CrossRef]
- Chhiba, K.D.; Patel, G.B.; Vu, T.H.T.; Chen, M.M.; Guo, A.; Kudlaty, E.; Mai, Q.; Yeh, C.; Muhammad, L.N.; Harris, K.E. Prevalence and characterization of asthma in hospitalized and nonhospitalized patients with COVID-19. J. Allergy Clin. Immunol. 2020, 146, 307–314.e4. [Google Scholar] [CrossRef]
- Recalcati, S. Cutaneous manifestations in COVID-19: A first perspective. J. Eur. Acad. Derm. Venereol 2020, 34, e212–e213. [Google Scholar] [CrossRef]
- Malipiero, G.; Heffler, E.; Pelaia, C.; Puggioni, F.; Racca, F.; Ferri, S.; Spinello, L.; Merigo, M.; Lamacchia, D.; Cataldo, G. Allergy clinics in times of the SARS-CoV-2 pandemic: An integrated model. Clin. Transl. Allergy 2020, 10, 23. [Google Scholar] [CrossRef] [PubMed]
- Cuffel, B.; Wamboldt, M.; Borish, L.; Kennedy, S.; Crystal-Peters, J. Economic consequences of comorbid depression, anxiety, and allergic rhinitis. Psychosomatics 1999, 40, 491–496. [Google Scholar] [CrossRef]
- Goodwin, R.D.; Castro, M.; Kovacs, M. Major depression and allergy: Does neuroticism explain the relationship? Psychosom. Med. 2006, 68, 94–98. [Google Scholar] [CrossRef] [Green Version]
- Goodwin, R.D.; Galea, S.; Perzanowski, M.; Jacobi, F. Impact of allergy treatment on the association between allergies and mood and anxiety in a population sample. Clin. Exp. Allergy 2012, 42, 1765–1771. [Google Scholar] [CrossRef]
- Gonzalez-Diaz, S.N.; Martin, B.; Villarreal-Gonzalez, R.V.; de Lira-Quezada, C.E.; Macouzet-Sanchez, C.; Macias-Weinmann, A.; Guzman-Avilan, R.I.; Garcia-Campa, M.; Noyola-Perez, A.; Garcia-Gonzalez, D.U. Psychological impact of the COVID-19 pandemic on patients with allergic diseases. World Allergy Organ. J. 2021, 14, 100510. [Google Scholar] [CrossRef] [PubMed]
- Camacho-Rivera, M.; Islam, J.Y.; Vidot, D.C. Associations between chronic health conditions and COVID-19 preventive behaviors among a nationally representative sample of US adults: An analysis of the COVID impact survey. Health Equity 2020, 4, 336–344. [Google Scholar] [CrossRef]
- Galea, S.; Merchant, R.M.; Lurie, N. The mental health consequences of COVID-19 and physical distancing: The need for prevention and early intervention. JAMA Intern. Med. 2020, 180, 817–818. [Google Scholar] [CrossRef] [Green Version]
- Tzeng, N.-S.; Chang, H.-A.; Chung, C.-H.; Kao, Y.-C.; Chang, C.-C.; Yeh, H.-W.; Chiang, W.-S.; Chou, Y.-C.; Chang, S.-Y.; Chien, W.-C. Increased risk of psychiatric disorders in allergic diseases: A nationwide, population-based, cohort study. Front. Psychiatry 2018, 9, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olaguibel, J.M.; Alobid, I.; Alvarez Puebla, M.; Crespo-Lessmann, A.; Domínguez Ortega, J.; García-Rio, F.; Izquierdo-Domínguez, A.; Mullol, J.; Plaza, V.; Quirce, S. Upper and lower airways functional examination in asthma and respiratory allergic deseases. Considerations in the SARS-CoV-2 post-pandemic situation. J. Investig. Allergol. Clin. Immunol. 2020, 31, 17–35. [Google Scholar] [CrossRef]
- Izquierdo-Domínguez, A.; Rojas-Lechuga, M.J.; Alobid, I. Management of Allergic Diseases during COVID-19 Outbreak. Curr. Allergy Asthma Rep. 2021, 21, 8. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-J.; Kim, H.-J.; Kang, M.-J.; Yu, H.-S.; Seo, J.-H.; Kim, H.-Y.; Park, S.-J.; Lee, Y.-C.; Hong, S.-J. Bacillus Calmette-Guérin suppresses asthmatic responses via CD4+ CD25+ regulatory T cells and dendritic cells. Allergy Asthma Immunol. Res. 2014, 6, 201–207. [Google Scholar] [CrossRef]
- Choi, I.S. Immunomodulating approach to asthma using mycobacteria. Allergy Asthma Immunol. Res. 2014, 6, 187–188. [Google Scholar] [CrossRef] [Green Version]
- Choi, I.S.; Koh, Y.I. Therapeutic effects of BCG vaccination in adult asthmatic patients: A randomized, controlled trial. Ann. Allergy Asthma Immunol. 2002, 88, 584–591. [Google Scholar] [CrossRef]
- Chandler, C.E.; Ernst, R.K. Bacterial lipids: Powerful modifiers of the innate immune response. F1000Research 2017, 6, F1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bach, J.-F. The effect of infections on susceptibility to autoimmune and allergic diseases. N. Engl. J. Med. 2002, 347, 911–920. [Google Scholar] [CrossRef]
- Ribet, D.; Cossart, P. How bacterial pathogens colonize their hosts and invade deeper tissues. Microbes Infect. 2015, 17, 173–183. [Google Scholar] [CrossRef]
- Edwards, M.R.; Bartlett, N.W.; Hussell, T.; Openshaw, P.; Johnston, S.L. The microbiology of asthma. Nat. Rev. Microbiol. 2012, 10, 459–471. [Google Scholar] [CrossRef]
- Medina, J.L.; Coalson, J.J.; Brooks, E.G.; Winter, V.T.; Chaparro, A.; Principe, M.F.; Kannan, T.R.; Baseman, J.B.; Dube, P.H. Mycoplasma pneumoniae CARDS toxin induces pulmonary eosinophilic and lymphocytic inflammation. Am. J. Respir. Cell Mol. Biol. 2012, 46, 815–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chua, K.J.; Kwok, W.C.; Aggarwal, N.; Sun, T.; Chang, M.W. Designer probiotics for the prevention and treatment of human diseases. Curr. Opin. Chem. Biol. 2017, 40, 8–16. [Google Scholar] [CrossRef]
- Chung, K.F. Airway microbial dysbiosis in asthmatic patients: A target for prevention and treatment? J. Allergy Clin. Immunol. 2017, 139, 1071–1081. [Google Scholar] [CrossRef] [Green Version]
- West, C.E.; Dzidic, M.; Prescott, S.L.; Jenmalm, M.C. Bugging allergy; role of pre-, pro-and synbiotics in allergy prevention. Allergol. Int. 2017, 66, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Seggev, J.S.; Sedmak, G.V.; Kurup, V.P. Isotype-specific antibody responses to acute Mycoplasma pneumoniae infection. Ann. Allergy Asthma Immunol. 1996, 77, 67–73. [Google Scholar] [CrossRef]
- Darveaux, J.I.; Lemanske, R.F., Jr. Infection-related asthma. J. Allergy Clin. Immunol. Pract. 2014, 2, 658–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, P. Intrinsic asthma: Not so different from allergic asthma but driven by superantigens? Clin. Exp. Allergy 2009, 39, 1145–1151. [Google Scholar] [CrossRef]
- Hahn, D.L.; Schure, A.; Patel, K.; Childs, T.; Drizik, E.; Webley, W. Chlamydia pneumoniae-specific IgE is prevalent in asthma and is associated with disease severity. PLoS ONE 2012, 7, e35945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, K.K.; Anderson, E.; Salva, P.S.; Webley, W.C. The prevalence and identity of Chlamydia-specific IgE in children with asthma and other chronic respiratory symptoms. Respir. Res. 2012, 13, 32. [Google Scholar] [CrossRef] [Green Version]
- Hahn, D.L.; Peeling, R.W. Airflow limitation, asthma, and Chlamydia pneumoniae-specific heat shock protein 60. Ann. Allergy Asthma Immunol. 2008, 101, 614–618. [Google Scholar] [CrossRef]
- Webley, W.; Tilahun, Y.; Lay, K.; Patel, K.; Stuart, E.; Andrzejewski, C.; Salva, P. Occurrence of Chlamydia trachomatis and Chlamydia pneumoniae in paediatric respiratory infections. Eur. Respir. J. 2009, 33, 360–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bisgaard, H.; Hermansen, M.N.; Buchvald, F.; Loland, L.; Halkjaer, L.B.; Bønnelykke, K.; Brasholt, M.; Heltberg, A.; Vissing, N.H.; Thorsen, S.V. Childhood asthma after bacterial colonization of the airway in neonates. N. Engl. J. Med. 2007, 357, 1487–1495. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.F.; Peng, R.D.; McCormack, M.C.; Matsui, E.C. Staphylococcus aureus colonization is associated with wheeze and asthma among US children and young adults. J. Allergy Clin. Immunol. 2015, 135, 811–813.e5. [Google Scholar] [CrossRef] [Green Version]
- Inoshima, I.; Inoshima, N.; Wilke, G.A.; Powers, M.E.; Frank, K.M.; Wang, Y.; Wardenburg, J.B. A Staphylococcus aureus pore-forming toxin subverts the activity of ADAM10 to cause lethal infection in mice. Nat. Med. 2011, 17, 1310–1314. [Google Scholar] [CrossRef] [Green Version]
- Ye, Q.; Xu, X.-J.; Shao, W.-X.; Pan, Y.-X.; Chen, X.-J. Mycoplasma pneumoniae infection in children is a risk factor for developing allergic diseases. Sci. World J. 2014, 2014, 986527. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, Y.; Oscherwitz, J.; Cease, K.B.; Chan, S.M.; Muñoz-Planillo, R.; Hasegawa, M.; Villaruz, A.E.; Cheung, G.Y.; McGavin, M.J.; Travers, J.B. Staphylococcus δ-toxin induces allergic skin disease by activating mast cells. Nature 2013, 503, 397–401. [Google Scholar] [CrossRef] [Green Version]
- Smith-Norowitz, T.A.; Chotikanatis, K.; Erstein, D.P.; Perlman, J.; Norowitz, Y.M.; Joks, R.; Durkin, H.G.; Hammerschlag, M.R.; Kohlhoff, S. Chlamydia pneumoniae enhances the Th2 profile of stimulated peripheral blood mononuclear cells from asthmatic patients. Hum. Immunol. 2016, 77, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Yeh, J.-J.; Wang, Y.-C.; Hsu, W.-H.; Kao, C.-H. Incident asthma and Mycoplasma pneumoniae: A nationwide cohort study. J. Allergy Clin. Immunol. 2016, 137, 1017–1023.e6. [Google Scholar] [CrossRef]
- Hales, B.J.; Chai, L.Y.; Elliot, C.E.; Pearce, L.J.; Zhang, G.; Heinrich, T.K.; Smith, W.-A.; Kusel, M.M.; Holt, P.G.; Sly, P.D. Antibacterial antibody responses associated with the development of asthma in house dust mite-sensitised and non-sensitised children. Thorax 2012, 67, 321–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordengrün, M.; Michalik, S.; Völker, U.; Bröker, B.M.; Gómez-Gascón, L. The quest for bacterial allergens. Int. J. Med. Microbiol. 2018, 308, 738–750. [Google Scholar] [CrossRef] [PubMed]
- Dzoro, S.; Mittermann, I.; Resch-Marat, Y.; Vrtala, S.; Nehr, M.; Hirschl, A.M.; Wikberg, G.; Lundeberg, L.; Johansson, C.; Scheynius, A. House dust mites as potential carriers for IgE sensitization to bacterial antigens. Allergy 2018, 73, 115–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonyadi, M.; Hassanzadeh, D.; Seyfizadeh, N.; Borzoueisileh, S. Assessment of allergen-specific IgE by immunoblotting method in atopic dermatitis. Eur. Ann. Allergy Clin. Immunol. 2017, 49, 213–219. [Google Scholar] [CrossRef] [Green Version]
- Pullerits, T.; Praks, L.; Ristioja, V.; Lötvall, J. Comparison of a nasal glucocorticoid, antileukotriene, and a combination of antileukotriene and antihistamine in the treatment of seasonal allergic rhinitis. J. Allergy Clin. Immunol. 2002, 109, 949–955. [Google Scholar] [CrossRef]
- Chad, Z. Allergies in children. Paediatr. Child. Health 2001, 6, 555–566. [Google Scholar] [CrossRef] [Green Version]
- Wert, A.; Posa, D.; Tsilochristou, O.; Schwerk, N. Treatment of allergic children—Where is the progress (for the practicing allergist)? Pediatric Allergy Immunol. 2016, 27, 671–681. [Google Scholar] [CrossRef] [PubMed]
- Van Bever, H.P.; Lee, B.W.; Shek, L. The future of research in pediatric allergy: What should the focus be? Pediatric Allergy Immunol. 2012, 23, 5–10. [Google Scholar] [CrossRef]
- Douglass, J.A.; O’Hehir, R.E. 1. Diagnosis, treatment and prevention of allergic disease: The basics. Med. J. Aust. 2006, 185, 228–233. [Google Scholar] [CrossRef]
- Gardner, L.M.; Thien, F.; Douglass, J.A.; Rolland, J.M.; O’Hehir, R.E. Induction of T ‘regulatory’cells by standardized house dust mite immunotherapy: An increase in CD4+ CD25+ interleukin-10+ T cells expressing peripheral tissue trafficking markers. Clin. Exp. Allergy 2004, 34, 1209–1219. [Google Scholar] [CrossRef]
- Wong, A.G.; Lomas, J.M. Allergy testing and immunotherapy. Pediatr. Rev. 2019, 40, 219–228. [Google Scholar] [CrossRef]
- Scurlock, A.M. Oral and sublingual immunotherapy for treatment of IgE-mediated food allergy. Clin. Rev. Allergy Immunol. 2018, 55, 139–152. [Google Scholar] [CrossRef]
- Astarita, C.; Scala, G.; Sproviero, S.; Franzese, A. Effects of enzyme-potentiated desensitization in the treatment of pollinosis: A double-blind placebo-controlled trial. J. Investig. Allergol. Clin. Immunol. 1996, 6, 248–255. [Google Scholar]
- Bochner, B.S.; Rothenberg, M.E.; Boyce, J.A.; Finkelman, F. Advances in mechanisms of allergy and clinical immunology in 2012. J. Allergy Clin. Immunol. 2013, 131, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Ismail, S.; Shahid, F.; Khan, A.; Bhatti, S.; Ahmad, S.; Naz, A.; Almatroudi, A.; ul Qamar, M.T. Pan-vaccinomics approach towards a universal vaccine candidate against WHO priority pathogens to address growing global antibiotic resistance. Comput. Biol. Med. 2021, 136, 104705. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, D.; Gupta-Bhattacharya, S. Allergen bioinformatics: Recent trends and developments. Sel. Work. Bioinform. 2011, 49, 1–14. [Google Scholar] [CrossRef] [Green Version]
- George, A.; Georrge, J.J. Viroinformatics: Databases and tools. Recent Trends Sci. Technol. 2019, 2019, 117–126. [Google Scholar]
- George, R.; Jacob, S.; Thomas, S.; Georrge, J.J. Approaches for novel drug target identification. In Proceedings of the International Science Symposium on Recent Trends in Science and Technology, New Delhi, India, 6–10 January 2020; Bharti Publications: New Delhi, India, 2017; pp. 399–421. [Google Scholar]
- Zhang, Y.; Huang, Y.; Chen, W.-X.; Xu, Z.-M. Identification of key genes in allergic rhinitis by bioinformatics analysis. J. Int. Med. Res. 2021, 49. [Google Scholar] [CrossRef]
- Le Chen, L.S.; Ma, Y.; Zheng, C. Hub Genes Identification in a Murine Model of Allergic Rhinitis Based on Bioinformatics Analysis. Front. Genet. 2020, 11, 970. [Google Scholar] [CrossRef] [PubMed]
- Deocaris, C.C.; Rumbaoa, R.G.; Gavarra, A.M.; Alinsug, M.V. A Preliminary analysis of potential allergens in a GMO Rice: A Bioinformatics approach. Open J. Bioinform. Biostat. 2020, 4, 12–16. [Google Scholar]
- L’Hocine, L.; Pitre, M.; Achouri, A. Detection and identification of allergens from Canadian mustard varieties of Sinapis alba and Brassica juncea. Biomolecules 2019, 9, 489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, C.; Kan, A.; Zeng, X. Bioinformatics Analysis in Different Expression Genes and Potential Pathways of CD4+ Cells in Childhood Allergic Asthma. Res. Sq. 2021, preprint. [Google Scholar] [CrossRef]
- Qamar, M.T.U.; Saba Ismail, S.A.; Mirza, M.U.; Abbasi, S.W.; Ashfaq, U.A.; Chen, L.-L. Development of a Novel Multi-Epitope Vaccine Against Crimean-Congo Hemorrhagic Fever Virus: An Integrated Reverse Vaccinology, Vaccine Informatics and Biophysics Approach. Front. Immunol. 2021, 12, 669812. [Google Scholar] [CrossRef] [PubMed]
- Aalberse, R.C. Assessment of allergen cross-reactivity. Clin. Mol. Allergy 2007, 5, 2. [Google Scholar] [CrossRef] [Green Version]
- Aalberse, R.C.; Stadler, B.M. In silico predictability of allergenicity: From amino acid sequence via 3-D structure to allergenicity. Mol. Nutr. Food Res. 2006, 50, 625–627. [Google Scholar] [CrossRef]
- Stadler, M.B.; Stadler, B.M. Allergenicity prediction by protein sequence. FASEB J. 2003, 17, 1141–1143. [Google Scholar] [CrossRef]
- Zhang, Z.H.; Koh, J.L.; Zhang, G.L.; Choo, K.H.; Tammi, M.T.; Tong, J.C. AllerTool: A web server for predicting allergenicity and allergic cross-reactivity in proteins. Bioinformatics 2007, 23, 504–506. [Google Scholar] [CrossRef]
- Schein, C.H.; Ivanciuc, O.; Braun, W. Structural database of allergenic proteins (SDAP). Food Allergy 2006, 117, 257–283. [Google Scholar] [CrossRef]
- Muh, H.C.; Tong, J.C.; Tammi, M.T. AllerHunter: A SVM-pairwise system for assessment of allergenicity and allergic cross-reactivity in proteins. PLoS ONE 2009, 4, e5861. [Google Scholar] [CrossRef] [Green Version]
- Vijayakumar, S.; Lakshmi, P. A fuzzy inference system for predicting allergenicity and allergic cross-reactivity in proteins. In Proceedings of the 2013 IEEE International Conference on Bioinformatics and Biomedicine, Shanghai, China, 18–21 December 2013; pp. 49–52. [Google Scholar]
- Rehman, A.; Ahmad, S.; Shahid, F.; Albutti, A.; Alwashmi, A.S.; Aljasir, M.A.; Alhumeed, N.; Qasim, M.; Ashfaq, U.A.; Tahir ul Qamar, M. Integrated Core Proteomics, Subtractive Proteomics, and Immunoinformatics Investigation to Unveil a Potential Multi-Epitope Vaccine against Schistosomiasis. Vaccines 2021, 9, 658. [Google Scholar] [CrossRef]
- Ahmad, S.; Shahid, F.; Tahir ul Qamar, M.; Abbasi, S.W.; Sajjad, W.; Ismail, S.; Alrumaihi, F.; Allemailem, K.S.; Almatroudi, A.; Ullah Saeed, H.F. Immuno-Informatics Analysis of Pakistan-Based HCV Subtype-3a for Chimeric Polypeptide Vaccine Design. Vaccines 2021, 9, 293. [Google Scholar] [CrossRef] [PubMed]
- Solanki, D.; Mandaliya, V.; Georrge, J.J. Allergen Bioinformatics: Repositories and Tools to Predict Allergic Proteins. Recent Trends Sci. Technol. 2020, 2020, 162–172. [Google Scholar]
- Chapman, M.D.; Pomés, A.; Breiteneder, H.; Ferreira, F. Nomenclature and structural biology of allergens. J. Allergy Clin. Immunol. 2007, 119, 414–420. [Google Scholar] [CrossRef]
- Kadam, K.; Karbhal, R.; Jayaraman, V.; Sawant, S.; Kulkarni-Kale, U. AllerBase: A comprehensive allergen knowledgebase. Database 2017, 2017, bax066. [Google Scholar] [CrossRef]
- Radauer, C.; Bublin, M.; Wagner, S.; Mari, A.; Breiteneder, H. Allergens are distributed into few protein families and possess a restricted number of biochemical functions. J. Allergy Clin. Immunol. 2008, 121, 847–852.e7. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R.E.; Ebisawa, M.; Ferreira, F.; Sampson, H.A.; van Ree, R.; Vieths, S.; Baumert, J.L.; Bohle, B.; Lalithambika, S.; Wise, J. AllergenOnline: A peer-reviewed, curated allergen database to assess novel food proteins for potential cross-reactivity. Mol. Nutr. Food Res. 2016, 60, 1183–1198. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, R.; Teshima, R.; Takagi, K.; Sawada, J.-I. Development of Allergen Database for Food Safety (ADFS): An integrated database to search allergens and predict allergenicity. Kokuritsu Iyakuhin Shokuhin Eisei Kenkyujo Hokoku = Bull. Natl. Inst. Health Sci. 2005, 132, 32–36. [Google Scholar]
- Kim, C.-K.; Seol, Y.-J.; Lee, D.-J.; Jeong, I.-S.; Yoon, U.-H.; Lee, J.-Y.; Lee, G.-S.; Park, D.-S. AllergenPro: An integrated database for allergenicity analysis and prediction. Bioinformation 2014, 10, 378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mari, A.; Scala, E.; Palazzo, P.; Ridolfi, S.; Zennaro, D.; Carabella, G. Bioinformatics applied to allergy: Allergen databases, from collecting sequence information to data integration. The Allergome platform as a model. Cell. Immunol. 2006, 244, 97–100. [Google Scholar] [CrossRef]
- ul Qamar, M.T.; Ahmad, S.; Fatima, I.; Ahmad, F.; Shahid, F.; Naz, A.; Abbasi, S.W.; Khan, A.; Mirza, M.U.; Ashfaq, U.A. Designing multi-epitope vaccine against Staphylococcus aureus by employing subtractive proteomics, reverse vaccinology and immuno-informatics approaches. Comput. Biol. Med. 2021, 132, 104389. [Google Scholar] [CrossRef]
- Brusic, V.; Petrovsky, N.; Gendel, S.; Millot, M.; Gigonzac, O.; Stelman, S. Computational tools for the study of allergens. Allergy 2003, 58, 1083–1092. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Zhang, D.; Li, J. PREAL: Prediction of allergenic protein by maximum Relevance Minimum Redundancy (mRMR) feature selection. BMC Syst. Biol. 2013, 7, S9. [Google Scholar] [CrossRef] [Green Version]
- Dimitrov, I.; Naneva, L.; Doytchinova, I.; Bangov, I. AllergenFP: Allergenicity prediction by descriptor fingerprints. Bioinformatics 2014, 30, 846–851. [Google Scholar] [CrossRef]
- Dimitrov, I.; Bangov, I.; Flower, D.R.; Doytchinova, I. AllerTOP v. 2—A server for in silico prediction of allergens. J. Mol. Modeling 2014, 20, 2278. [Google Scholar] [CrossRef]
- Maurer-Stroh, S.; Krutz, N.L.; Kern, P.S.; Gunalan, V.; Nguyen, M.N.; Limviphuvadh, V.; Eisenhaber, F.; Gerberick, G.F. AllerCatPro—prediction of protein allergenicity potential from the protein sequence. Bioinformatics 2019, 35, 3020–3027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadam, K.; Sawant, S.; Jayaraman, V.; Kulkarni-Kale, U. Databases and Algorithms in Allergen Informatics. In Bioinformatics—Updated Features and Applications; IntechOpen: London, UK, 2016; p. 53. [Google Scholar]
- Yang, X.; Yu, X. An introduction to epitope prediction methods and software. Rev. Med. Virol. 2009, 19, 77–96. [Google Scholar] [CrossRef]
- Wang, H.-W.; Pai, T.-W. Machine learning-based methods for prediction of linear B-cell epitopes. In Immunoinformatics; Humana Press: New York, NY, USA, 2014; pp. 217–236. [Google Scholar]
- Saha, S.; Raghava, G.P. Prediction methods for B-cell epitopes. In Immunoinformatics; Springer: Berlin/Heidelberg, Germany, 2007; pp. 387–394. [Google Scholar]
- Jespersen, M.C.; Peters, B.; Nielsen, M.; Marcatili, P. BepiPred-2.0: Improving sequence-based B-cell epitope prediction using conformational epitopes. Nucleic Acids Res. 2017, 45, W24–W29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, H.; Ansari, H.R.; Raghava, G.P. Improved method for linear B-cell epitope prediction using antigen’s primary sequence. PLoS ONE 2013, 8, e62216. [Google Scholar] [CrossRef] [Green Version]
- EL-Manzalawy, Y.; Dobbs, D.; Honavar, V. Predicting linear B-cell epitopes using string kernels. J. Mol. Recognit. Interdiscip. J. 2008, 21, 243–255. [Google Scholar] [CrossRef] [Green Version]
- Gao, J.; Faraggi, E.; Zhou, Y.; Ruan, J.; Kurgan, L. BEST: Improved prediction of B-cell epitopes from antigen sequences. PLoS ONE 2012, 7, e40104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, B.; Zhang, L.; Liang, S.; Zhang, C. SVMTriP: A method to predict antigenic epitopes using support vector machine to integrate tri-peptide similarity and propensity. PLoS ONE 2012, 7, e45152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kringelum, J.V.; Lundegaard, C.; Lund, O.; Nielsen, M. Reliable B cell epitope predictions: Impacts of method development and improved benchmarking. PLoS Comput. Biol. 2012, 8, e1002829. [Google Scholar] [CrossRef]
- Giacò, L.; Amicosante, M.; Fraziano, M.; Gherardini, P.F.; Ausiello, G.; Helmer-Citterich, M.; Colizzi, V.; Cabibbo, A. B-Pred, a structure based B-cell epitopes prediction server. Adv. Appl. Bioinform. Chem. AABC 2012, 5, 11. [Google Scholar] [PubMed] [Green Version]
- Ponomarenko, J.; Bui, H.-H.; Li, W.; Fusseder, N.; Bourne, P.E.; Sette, A.; Peters, B. ElliPro: A new structure-based tool for the prediction of antibody epitopes. BMC Bioinform. 2008, 9, 514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansari, H.R.; Raghava, G.P. Identification of conformational B-cell Epitopes in an antigen from its primary sequence. Immunome Res. 2010, 6, 6. [Google Scholar] [CrossRef] [Green Version]
- Krawczyk, K.; Liu, X.; Baker, T.; Shi, J.; Deane, C.M. Improving B-cell epitope prediction and its application to global antibody-antigen docking. Bioinformatics 2014, 30, 2288–2294. [Google Scholar] [CrossRef] [PubMed]
- Dimitrov, I.; Garnev, P.; Flower, D.R.; Doytchinova, I. EpiTOP—A proteochemometric tool for MHC class II binding prediction. Bioinformatics 2010, 26, 2066–2068. [Google Scholar] [CrossRef] [Green Version]
- Bhasin, M.; Raghava, G.P. Prediction of CTL epitopes using QM, SVM and ANN techniques. Vaccine 2004, 22, 3195–3204. [Google Scholar] [CrossRef] [PubMed]
- Oyarzún, P.; Ellis, J.J.; Bodén, M.; Kobe, B. PREDIVAC: CD4+ T-cell epitope prediction for vaccine design that covers 95% of HLA class II DR protein diversity. BMC Bioinform. 2013, 14, 52. [Google Scholar] [CrossRef] [PubMed]
- Guan, P.; Hattotuwagama, C.K.; Doytchinova, I.A.; Flower, D.R. MHCPred 2.0. Appl. Bioinform. 2006, 5, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Karosiene, E.; Rasmussen, M.; Blicher, T.; Lund, O.; Buus, S.; Nielsen, M. NetMHCIIpan-3. 0, a common pan-specific MHC class II prediction method including all three human MHC class II isotypes, HLA-DR, HLA-DP and HLA-DQ. Immunogenetics 2013, 65, 711–724. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Allergy | Symptoms | Prevalence | Affected Organ | Causes | Reference |
|---|---|---|---|---|---|
| Allergic rhinatisis | Sneezing, itchy, watery, and red eyes, stuffy or runny nose, swelling around the eyes. | Affects 10–30% of the population worldwide | Nose | Genetic and environmental factors | [19] |
| Asthma | Wheezing, coughing, shortness of breath, and chest tightness | Affects 3 to 9% of the population worldwide | Airways of lungs | Genetic and environmental factors | [20] |
| Food allergy | Itchiness, vomiting, swelling of the tongue, hives, diarrhea, low blood pressure, trouble breathing | Affects 8% of the population worldwide | Skin, respiratory system, gastrointestinal tract | Immune response to food | [21] |
| Skin allergy | Rash, itching, swelling, redness, cracked skin, flaking or scaling of skin, raised bumps | Worldwide, lifetime prevalence of above 20% | Skin | Latex, food, drugs, water, sunlight, nickel, chemicals, soap, poison oak or poison ivy | [22] |
| Drug allergy | Itching, rash, fever, facial swelling, hives, shortness of breath, cardiac symptoms | Affects 10% of the population worldwide | Nose, lungs, throat, ear, lining of the stomach, and skin | Reactions to medications | [23] |
| Insect allergy | Itching, pain, and swelling and appearance of redness at the sting/bite or surrounding affected areas | Many allergic severe cases have been documented with insect bites worldwide; however, there has been no systemic report. | Skin, eyes, throat, tongue | Insects bite or sting | [24] |
| Anaphylaxis | Itchy rash, numbness, throat swelling, lightheadedness, shortness of breath | Affects 0.05–2% of the population worldwide | Skin, nose, throat, lungs, gastrointestinal tract | Foods, insects bites, medications | [25] |
| Database | URL | Maintained by | Type of Data Archived | Last Update | Number of Allergens/Haptens/Epitopes | Reference |
|---|---|---|---|---|---|---|
| IUIS Allergen | http://www.allergen.org (Accessed on: 19 August 2021) | World Health Organization (WHO) and International Union of Immunological Societies (IUIS) | Allergenicity, structure, sequence (isoforms/isoallergens) | Updated continuously | 853 | [216] |
| Structural Database of Allergenic Proteins (SDAP) | https://fermi.utmb.edu (Accessed on: 19 August 2021) | Sealy Centre for Structural Biology, University of Texas, USA | IgE epitopes, structure, sequence, structural models | 2013 | 1526 | [210] |
| AllerBase | www.bioinfo.net.in/AllerBase/Home.html (Accessed on: 19 August 2021) | Bioinformatics Centre, Savitribai Phule PuneUniversity, India | Structure and sequence (cross-links), IgE epitopes, IgE cross-reactivity, experimental evidences of allergenicity, IgE antibody | Updated continuously | 2311 | [217] |
| AllFam | http://www.meduniwien.ac.at/allfam (Accessed on: 19 August 2021) | Department of Pathophysiology and Allergy Research, Medical University of Vienna, Austria | Cross-link to Pfam database, allergen family data | 2011 | 936 | [218] |
| Allergen Online | http://www.allergenonline.Org (Accessed on: 20 August 2021) | Food Allergy Research and Resource Program (FARRP) at the University of Nebraska-Lincoln | Allergenicity, sequence | 2016 | 1956 | [219] |
| Allergen Database For Food Safety (ADFS) | http://allergen.nihs.go.jp/ADFS/ (Accessed on: 20 August 2021) | National Institute of Health, Japan | IgE epitopes, sequence, structure, small molecule allergens | 2016 | 2028 | [220] |
| AllergenPro | http://nabic.rda.go.kr/allergen (Accessed on: 20 August 2021) | The National Agricultural Biotechnology Information Center (NABIC), Korea | IgE epitopes, sequence | 2015 | 2434 | [221] |
| Allergome | http://www.allergome.org (Accessed on: 20 August 2021) | Centre for Clinical and Experimental Allergology, Italy | Sequence (isoforms/isoallergens), clinical, cross-reactivity, structure, epidemiologically | Updated continuously | 3075 | [222] |
| Server | URL | Method | Efficiency | Reference |
|---|---|---|---|---|
| AlgPred | http://www.imtech.res.in/raghava/algpred/ (Accessed on: 21 August 2021) | SVM and allergen sequence features, epitopes, sequence motifs | Accuracy: 85% Specificity: 88.1% | [4] |
| AllerHunter | http://tiger.dbs.nus.edu.sg/AllerHunter/ (Accessed on: 21 August 2021) | SVM and iterative pairwise sequence similarity | Accuracy: 95.3% Specificity: 96.41% | [211] |
| PREAL | http://gmobl.sjtu.edu.cn/PREAL/index.php (Accessed on: 21 August 2021) | Physicochemical and biochemical descriptors, sequence features, subcellular locations, SVM, and mRMR | Accuracy: 93.42% | [225] |
| AllergenFP | http://ddg-pharmfac.net/AllergenFP/ (Accessed on: 21 August 2021) | Descriptor-based fingerprints of residues, auto and cross-covariance | Accuracy: 88% | [226] |
| AllerTOP | http://www.ddg-pharmfac.net/AllerTOP (Accessed on: 22 August 2021) | Machine learning, sequence based descriptors, cross and auto -covariance, | Accuracy: 85.3% Specificity: 88.1% | [227] |
| AllerCatPro | https://allercatpro.bii.a-star.edu.sg/ (Accessed on: 22 August 2021) | Sequence similarity, structure similarity | Accuracy: 84% Specificity: 67% | [228] |
| Type | Server | URL/Website | Method | Reference |
|---|---|---|---|---|
| Linear B cell Epitope | ABCPred | (http://www.imtech.res.in/raghava/abcpred/) (Accessed on: 25 August 2021) | ANN | [232] |
| BepiPred | (http://www.cbs.dtu.dk/services/BepiPred/) (Accessed on: 25 August 2021) | HMM | [233] | |
| LBtope | (http://www.imtech.res.in/raghava/lbtope/) (Accessed on: 25 August 2021) | SVM | [234] | |
| BCPreds | (http://crdd.osdd.net/raghava/bcepred/) (Accessed on: 25 August 2021) | SVM | [235] | |
| BEST | (http://biomine.ece.ualberta.ca/BEST/) (Accessed on: 25 August 2021) | SVM | [236] | |
| SVMTriP | (http://sysbio.unl.edu/SVMTriP/) (Accessed on: 25 August 2021) | SVM | [237] | |
| Conformational/Discontinuous B cell Epitope | DiscoTope 2.0 | (http://www.cbs.dtu.dk/services/DiscoTope/) (Accessed on: 27 August 2021) | Structure-based method | [238] |
| B-Pred | (http://immuno.bio.uniroma2.it/bpred) (Accessed on: 27 August 2021) | SVM | [239] | |
| ElliPro | (http://tools.immuneepitope.org/tools/ElliPro) (Accessed on: 27 August 2021) | Thornton’s method | [240] | |
| CBTOPE | (http://crdd.osdd.net/raghava/cbtope/) (Accessed on: 27 August 2021) | SVM | [241] | |
| EpiPred | (http://opig.stats.ox.ac.uk/webapps/newsabdab/sabpred/epipred/) (Accessed on: 27 August 2021) | Structure-based method | [242] | |
| T cell Epitope | EpiTOP | (http://www.pharmfac.net/EpiTOP/) (Accessed on: 29 August 2021) | QSAR | [243] |
| CTLPred | (http://www.imtech.res.in/raghava/ctlpred/index.html) (Accessed on: 29 August 2021) | ANN, SVM | [244] | |
| PREDIVAC | (http://predivac.biosci.uq.edu.au/) (Accessed on: 29 August 2021) | MM | [245] | |
| MHCPred | (http://www.ddgpharmfac.net/mhcpred/MHCPred/) (Accessed on: 29 August 2021) | QSAR | [246] | |
| NetMHCIIpan-3.0 | (http://www.cbs.dtu.dk/services/NetMHCIIpan-3.0/) (Accessed on: 29 August 2021) | ANN | [247] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aldakheel, F.M. Allergic Diseases: A Comprehensive Review on Risk Factors, Immunological Mechanisms, Link with COVID-19, Potential Treatments, and Role of Allergen Bioinformatics. Int. J. Environ. Res. Public Health 2021, 18, 12105. https://doi.org/10.3390/ijerph182212105
Aldakheel FM. Allergic Diseases: A Comprehensive Review on Risk Factors, Immunological Mechanisms, Link with COVID-19, Potential Treatments, and Role of Allergen Bioinformatics. International Journal of Environmental Research and Public Health. 2021; 18(22):12105. https://doi.org/10.3390/ijerph182212105
Chicago/Turabian StyleAldakheel, Fahad M. 2021. "Allergic Diseases: A Comprehensive Review on Risk Factors, Immunological Mechanisms, Link with COVID-19, Potential Treatments, and Role of Allergen Bioinformatics" International Journal of Environmental Research and Public Health 18, no. 22: 12105. https://doi.org/10.3390/ijerph182212105