
Cardiovascular Risk Factors and Physical Activity for the Prevention of Cardiovascular Diseases in the Elderly

 , ,
, ,
Abstract
:1. Introduction
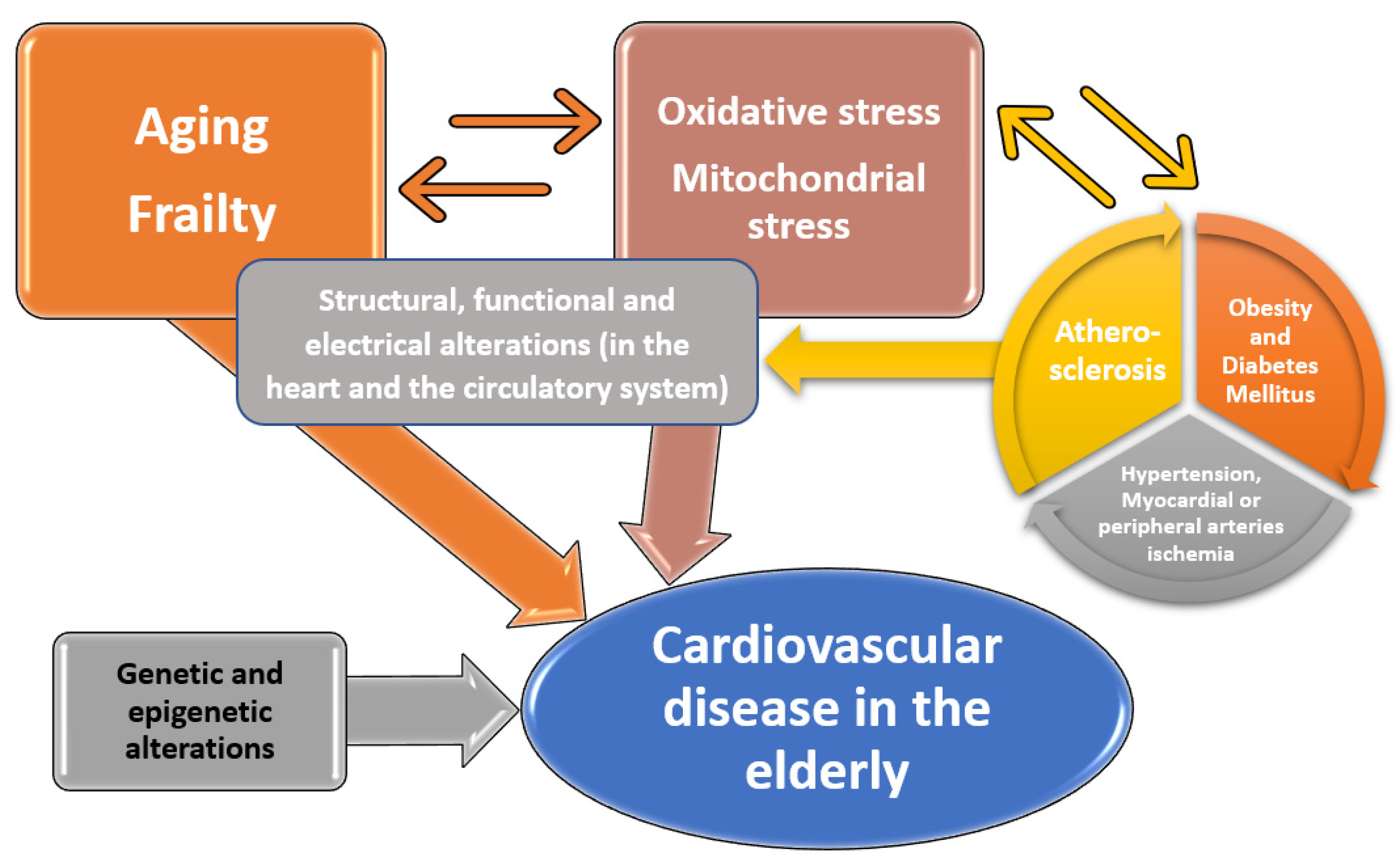
2. Pathophysiological Processes Encountered in Cardiovascular Diseases of the Elderly
3. Diabetes Mellitus and Cardiovascular Disease in Elderly Patients
4. Obesity and Cardiovascular Disease in Elderly Patients
5. Specific Interventions for Particular Clinical Settings
5.1. Stroke Prevention
5.2. Prevention of Coronary Artery Disease
5.3. Prevention of Peripheral Artery Disease
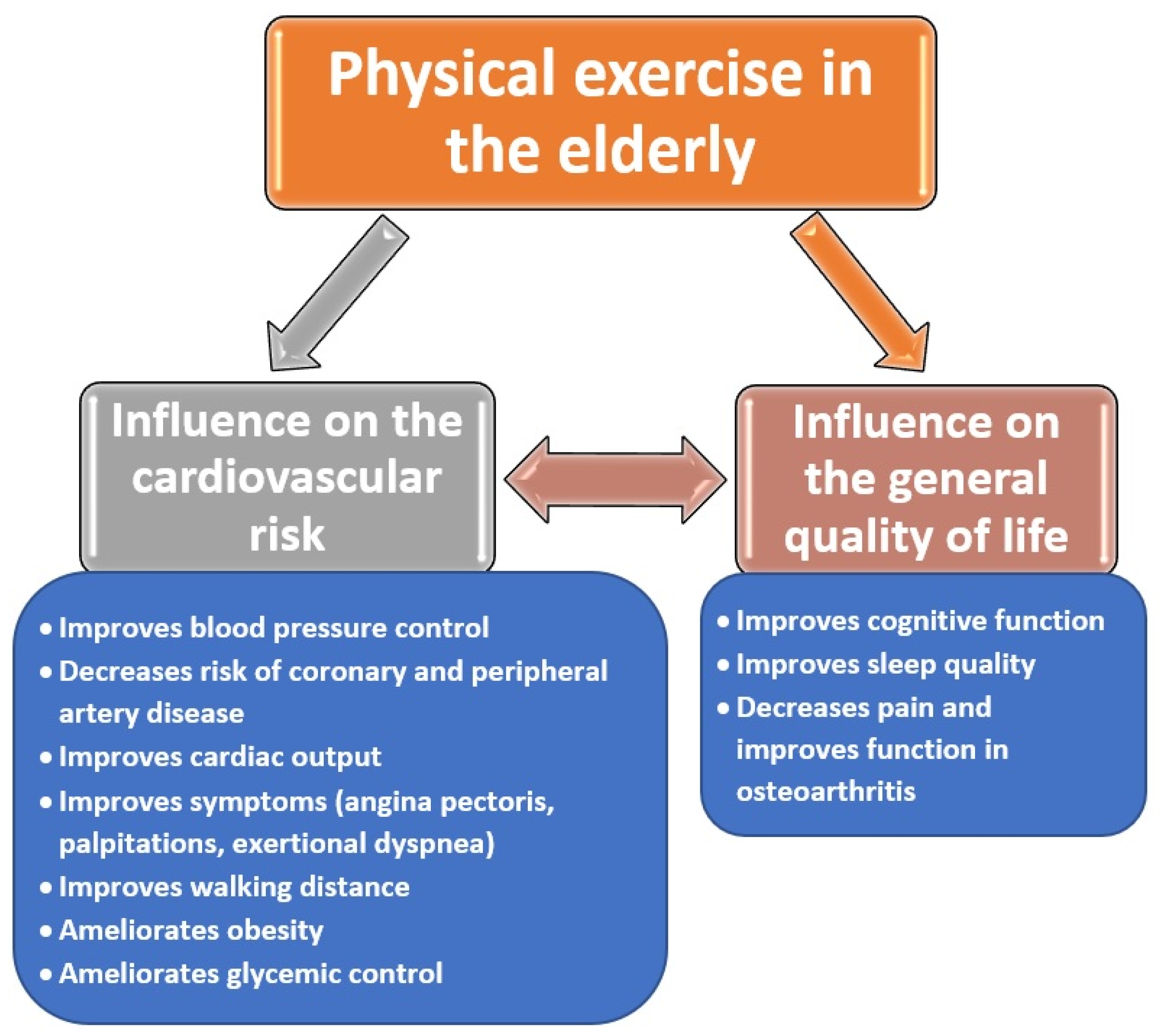
6. Physical Activity in the Elderly and the Prevention of Cardiovascular Diseases
6.1. Mechanisms and Effects
6.2. Types of Physical Activities Studied in the Elderly
6.3. Physical Activity, Insulin Sensitivity and Glycemic Control
6.4. Physical Activity and Blood Pressure Values
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Galiuto, L.; Locorotondo, G. Cardiovascular Aging. In Integrative Cardiology; Springer: Cham, Switzerland, 2017; Volume 9, pp. 109–120. [Google Scholar]
- Seco, M.; Edelman, J.J.B.; Forrest, P.; Nig, M.; Wilson, M.K.; Fraser, J.; Bannon, P.G.; Vallely, M.P. Geriatric cardiac surgery: Chronology vs. biology. Heart Lung Circ. 2014, 23, 794–801. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Bajorek, B. Defining ‘elderly’ in clinical practice guidelines for pharmacotherapy. Pharm. Pract. 2014, 12, 489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milanović, Z.; Pantelić, S.; Trajković, N.; Sporiš, G.; Kostić, R.; James, N. Age-related decrease in physical activity and functional fitness among elderly men and women. Clin. Interv. Aging 2013, 8, 549–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamin, E.J.; Muntner, P.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, J.L.; Jones, J.; Bolleddu, S.I.; Vanthenapalli, S.; Rodgers, L.E.; Shah, K.; Karia, K.; Panguluri, S.K. Cardiovascular Risk Associated with Gender and Aging. J. Cardiovasc. Dev. Dis. 2019, 6, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faulkner, J.L.; Belin De Cantemele, E.J. Sex hormones, aging and cardiometabolic syndrome. Biol. Sex Differ. 2019, 10, 30. [Google Scholar] [CrossRef]
- Garcia, M.; Mulvagh, S.L.; Noel Bairey Merz, C.; Buring, J.E.; Manson, J.E. Cardiovascular Disease in Women: Clinical Perspectives. Circ. Res. 2016, 118, 1273–1293. [Google Scholar] [CrossRef]
- Keto, J.; Ventola, H.; Jokelainen, J.; Linden, K.; Keinanen-Kiukaanniemi, S.; Timonen, M.; Ylisaukko-oja, T.; Auvinen, J. Cardiovascular disease risk factors in relation to smoking behavior and history: A population- based cohort study. Open Heart 2016, 3, e000358. [Google Scholar] [CrossRef] [Green Version]
- North, B.J.; Sinclair, V.A. The intersection between aging and cardiovascular disease. Circ. Res. 2012, 110, 1097–1108. [Google Scholar] [CrossRef]
- Yazdanyar, A.; Newman, A.B. The burden of cardiovascular disease in the elderly: Morbidity, mortality and costs. Clin. Geriatr. Med. 2009, 25, 563–577. [Google Scholar] [CrossRef] [Green Version]
- Spannella, F.; Di Pentima, C.; Giulietti, F.; Buscarini, S.; Giordano, P.; Sarzani, R. Prevalence of Sublinical Carotid Atherosclerosis and Role of Cardiovascular Risk Factors in Older Adults: Atherosclerosis and Aging are Not Synonyms. High Blood Press Cardiovasc Prev. 2020, 27, 231–238. [Google Scholar] [CrossRef]
- Bruno, R.M.; Masi, S.; Taddei, M.; Taddei, S.; Virdis, A. Essential Hypertension and Dunctional Microvascular Ageing. High Blood Press. Cardiovasc. Prev. 2018, 25, 35–40. [Google Scholar] [CrossRef]
- Nilsson, P.M. Early vascular aging (EVA): Consequences and prevention. Vasc. Health Risk Manag. 2008, 4, 547–552. [Google Scholar] [CrossRef] [Green Version]
- Hay, M.; Barnes, C.; Huentelman, M.; Brinton, R.; Ryan, L. Hypertension and Age-Related Cognitive Impairment: Common Risk Factors and a Role for Precision Aging. Curr. Hypertens. Rep. 2020, 22, 80. [Google Scholar] [CrossRef]
- Dhingra, R.; Vasan, R.S. Age as a cardiovascular risk factor. Med. Clin. N. Am. 2012, 96, 87–91. [Google Scholar] [CrossRef] [Green Version]
- Iorga, A.; Cunningham, C.M.; Moazeni, S.; Ruffenach, G.; Umar, S.; Eghbali, M. The protective role of estrogen and estrogen receptors in cardiovascular disease and the controversal use of estrogen therapy. Biol. Sex Differ. 2017, 8, 33. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Han, H.R.; Yang, W.; Zhang, H.; Zhang, J.; Ruan, H.; Tang, N.; Ren, J.; Sun, X.; Li, C.; et al. Association between risk factors for cardiovascular disease and frialty among community-dwelling older adults in Lanzhou, China. Int. J. Nurs. Sci. 2021, 8, 168–174. [Google Scholar]
- Yatsuya, H.; Matsunaga, M.; Li, Y.; Ota, A. Risk Factor of Cardiovascular Disease Among Older Individuals. J. Atheroscler. Thromb. 2017, 24, 258–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchner, D.M. Physical activity and prevention of cardiovascular disease in older adults. Clin. Geriatr. Med. 2009, 25, 661–675. [Google Scholar] [CrossRef] [PubMed]
- Steeman, M.; Lande, G. Cardiac aging and heart disease in humans. Biophys. Rev. 2017, 9, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Curtis, A.B.; Karki, R.; Hattoum, A.; Sharma, U.C. Arrhythmias in Patients ≥80 Years of Age: Pathophysiology, Management, and Outcomes. J. Am. Coll. Cardiol. 2018, 71, 2041–2057. [Google Scholar] [CrossRef]
- Meschiari, C.A.; Ero, O.K.; Pan, H.; Finkel, T.; Lindsey, M.L. The impact of aging on cardiac extracellular matrix. Geroscience 2017, 39, 7–18. [Google Scholar] [CrossRef]
- Meneses, M.J.; Silvester, R.; Sousa-Lima, I.; Macedo, M.P. Paraoxonase-1 as a Regulator of Glucose and Lipid Homeostasis: Impact on the Onset and Progression of Metabolic Disorders. Int. J Mol. Sci. 2019, 20, 4049. [Google Scholar] [CrossRef] [Green Version]
- Merino, J.; Udler, M.S.; Leong, A.; Meigs, J.B. A Decade of Genetic and Metabolomic Contributions to Type 2 Diabetes Risk Prediction. Curr. Diab. Rep. 2017, 17, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, M.; Liu, X.H.; Liu, Q.Q.; Chen, M.; Bai, H.; Jiang, C.Y.; Guan, L.B.; Fan, P. Lactonase activity and status of paraoxonase-1 and oxidative stress in neonates of women with gestational diabetes mellitus. Pediatr. Res. 2021, 89, 1192–1199. [Google Scholar] [CrossRef]
- Artasensi, A.; Pedretti, A.; Vistoli, G.; Fumagalli, L. Type 2 Diabetes Mellitus: A Review of Multi-Target Drugs. Molecules 2020, 25, 1987. [Google Scholar] [CrossRef] [PubMed]
- Martos, R.; Baugh, J.; Ledwidge, M.O.; Loughlin, C.; Conlon, C.; Patle, A.; Donnelly, S.C.; McDonald, K. Diastolic heart failure: Evidence of increased myocardial collagen turnover linked to diastolic dysfunction. Circulation 2007, 115, 888–895. [Google Scholar] [CrossRef] [Green Version]
- Burstein, B.; Nattel, S. Atrial fibrosis: Mechanisms and clinical relevance in atrial fibrillation. J. Am. Coll. Cardiol. 2008, 51, 802–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin-Fernandes, A.; Gredilla, R. Mitochondria and oxidative stress in heart aging. Age (Dordr) 2016, 38, 225–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakou, E.S.; Parthenakis, F.I.; Kallergis, E.M.; Marketou, M.E.; Nakos, K.S.; Vardas, P.E. Healthy aging and myocardium: A complicated process with various effects in cardiac structure and physiology. Int. J. Cardiol. 2016, 209, 167–175. [Google Scholar] [CrossRef]
- Xie, W.; Santulli, G.; Reiken, S.R.; Yuan, Q.; Osborne, B.W.; Chen, B.X.; Mark, A.R. Mitochondrial oxidative stress promotes atrial fibrillation. Sci. Rep. 2015, 5, 11427. [Google Scholar] [CrossRef] [Green Version]
- Babušíková, E.; Lehotský, J.; Dobrota, D.; Račay, P.; Kaplán, P. Age-associated changes in Ca(2+)-ATPase and oxidative damage in sarcoplasmic reticulum of rat heart. Physiol. Res. 2012, 61, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Kain, V.; Ingle, K.A.; Kachman, M.; Baum, H.; Shanmugam, G.; Rajasekaran, N.S.; Young, M.E.; Halade, G.E. Excess ω-6 fatty acids influx in aging drives metabolic dysregulation, electrocardiographic alterations, and low-grade chronic inflammation. Am. J. Physiol. Heart Circ. Physiol. 2018, 314, H160–H169. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Campisi, J. Chronic inflammation (inflammaging) and its potential contribution to age-associated diseases. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69 (Suppl. 1), S4–S9. [Google Scholar] [CrossRef]
- Lu, Y.; Hajifathalian, K.; Ezzati, M.; Woodward, M.; Rimm, E.B.; Danaei, G. Metabolic mediators of the effects of body-mass index, overweight, and obesity on coronary heart disease and stroke: A pooled analysis of 97 prospective cohorts with 1.8 million participants. Lancet 2014, 383, 970–983. [Google Scholar] [PubMed] [Green Version]
- Paneni, F.; Diaz Canestro, C.; Libby, P.; Luscher, T.F.; Camici, G.G. The Aging Cardiovascular System: Understanding It at the Cellular and Clinical Levels. J. Am. Coll. Cardiol. 2017, 69, 1952–1967. [Google Scholar] [CrossRef]
- Haldar, S.R.; Chakrabarty, A.; Chowdhury, S.; Haldar, A.; Sengupta, S.; Bhattacharyya, M. Oxidative stress-related genes in type 2 diabetes: Association analysis and their clinical impact. Biochem. Genet. 2015, 53, 93–119. [Google Scholar] [CrossRef]
- Chatterjee, S.; Khunti, K.; Davies, M.J. Type 2 diabetes. Lancet 2017, 389, 2239–2251. [Google Scholar] [CrossRef]
- Galicia-Garcia, U.; Benito-Vicente, A.; Jebari, S.; Lerrea-Sebal, A.; Siddiqi, H.; Uribe, K.B.; Ostolaza, H.; Martín, C. Pathophysiology of Type 2 Diabetes Mellitus. Int. J. Mol. Sci. 2020, 21, 6275. [Google Scholar] [CrossRef]
- Dimas, A.S.; Lagou, V.; Barker, A.; Knowles, J.W.; Magi, R.; Hivert, M.F.; Benazzo, A.; Rybin, D.; Jackson, A.U.; Stringham, H.M. Impact of type 2 diabetes susceptibility variants on quantitative glycemic traits reveals mechanistic heterogeneity. Diabetes 2014, 63, 2158–2171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Florez, J.C. Leveraging Genetics to Advance Type 2 Diabetes Prevention. PLoS Med. 2016, 13, e1002102. [Google Scholar] [CrossRef] [Green Version]
- Leitner, D.R.; Fruhbeck, G.; Yumuk, V.; Schindler, K.; Micic, D.; Woodward, E.; Toplak, H. Obesity and Type 2 Diabetes: Two Diseases with a Need for Combined Treatment Strategies—EASO Can Lead the Way. Obes. Fact. 2017, 10, 483–492. [Google Scholar] [CrossRef]
- Mokdad, A.H.; Ford, E.S.; Bowman, B.A.; Dietz, W.H.; Vincor, F.; Bales, V.S.; Mark, J.S. Prevalence of obesity, diabetes, and obesity-related health risk factors. JAMA 2003, 289, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Oguntibeju, O.O. Type 2 diabetes mellitus, oxidative stress and inflammation: Examining the links. Int. J. Physiol. Pathophysiol. Pharmacol. 2019, 11, 45–63. [Google Scholar] [PubMed]
- Zadhoush, F.; Sadeghi, M.; Pourfarzam, M. Biochemical changes in blood of type 2 diabetes with and without metabolic syndrome and their association with metabolic syndrome components. J. Res. Med. Sci. 2015, 20, 763–770. [Google Scholar]
- Papatheodorou, K.; Banach, M.; Bekiari, E.; Rizzo, M.; Edmonds, M. Complications of Diabetes. J. Diabetes Res. 2018, 2018, 3086167. [Google Scholar] [CrossRef] [Green Version]
- Silva, E.F.F.; Memdes Ferreira, C.M.; De Pinho, L. Risk factors and complications in type 2 diabetes outpatients. Rev. Assoc. Med. Bras. (1992) 2017, 63, 621–627. [Google Scholar] [CrossRef] [Green Version]
- Halter, J.B.; Musi, N.; Horne McFarland, F.; Crandall, J.P.; Goldberg, A.; Harkless, L.; Hazzard, W.R.; Huang, E.S.; Kirkman, M.S.; Plutzky, J. Diabetes and cardiovascular disease in older adults: Current status and future directions. Diabetes 2014, 63, 2578–2589. [Google Scholar] [CrossRef] [Green Version]
- Athithan, L.; Gulsin, G.S.; McCann, G.P.; Levelt, E. Diabetic cardiomyopathy: Pathophysiology, theories and evidence to date. World J. Diabetes 2019, 10, 490–510. [Google Scholar] [CrossRef] [PubMed]
- Kaur, N.; Guan, Y.; Raja, R.; Ruiz-Velasco, A.; Liu, W. Mechanisms and Therapeutic Prospects of Diabetic Cardiomyopathy Through the Inflammatory Response. Front. Physiol. 2021, 12, 694864. [Google Scholar] [CrossRef]
- Teodebusch, R.; Belenchia, A.; Pulakat, L. Diabetic Cardiomyopathy: Impact of Biological Sex on Disease Development and Molecular Signatures. Front. Physiol. 2018, 9, 453. [Google Scholar] [CrossRef] [Green Version]
- Jia, G.; Hill, A.M.; Sowers, J.R. Diabetic cardiomyopathy: An update of mechanisms contributing to this clinical entity. Circ. Res. 2018, 122, 624–638. [Google Scholar] [CrossRef]
- Miki, T.; Yuda, S.; Kouzu, H.; Miura, T. Diabetic cardiomyopathy: Pathophysiology and clinical features. Heart Fail. Rev. 2013, 18, 149–166. [Google Scholar] [CrossRef] [Green Version]
- Seferovic, P.M.; Petrie, M.C.; Filippatos, G.S.; Anker, S.D.; Rosano, G.; Bauersachs, J.; Paulus, W.J.; Komajda, M.; Cosentino, F.; A de Boer, R. Type 2 diabetes mellitus and heart failure: A position statement from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2018, 20, 853–872. [Google Scholar] [CrossRef] [PubMed]
- Paolillo, S.; Marsico, F.; Prastaro, M.; Renga, F.; Esposito, L.; De Martino, F.; Di Napoli, P.; Esposito, I.; Ambrosio, A.; Ianniruberto, M. Diabetic Cardiomyopathy: Definition, Diagnosis, and Therapeutic Implications. Heart Fail. Clin. 2019, 15, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Li, C.L.; Chiu, Y.C.; Chang, H.Y.; Hsu, K.H.; Bai, Y.B.; Wang, H.H. Association of geriatric conditions and cardiovascular diseases with disability in older adults with diabetes: Findings from a nationally representative survey. Geriatr. Gerontol. Int. 2013, 13, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Kautzky-Willer, A.; Harreiter, J.; Pacini, G. Sex and Gender Differences in Risk, Pathophysiology and Complications of Type 2 Diabetes Mellitus. Endocr. Rev. 2016, 37, 278–316. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.G.; Halter, J.B. The Pathophysiology of Hyperglycemia in Older Adults: Clinical Considerations. Diabetes Care 2017, 40, 444–452. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Feng, X.; Li, Q.; Wang, Y.; Li, Q.; Hua, M. Adiponectin, TNF-α and inflammatory cytokines and risk of type 2 diabetes: A systematic review and meta-analysis. Cytokine 2016, 86, 100–109. [Google Scholar] [CrossRef]
- El Assar, M.; Angulo, J.; Rodriguez-Manas, L. Diabetes and ageing-induced vascular inflammation. J. Physiol. 2016, 594, 2125–2146. [Google Scholar] [CrossRef] [Green Version]
- Tian, R.; Tian, M.; Wang, L.; Qian, H.; Zhang, S.; Pang, H.; Liu, Z.; Fang, L.; Shen, Z. C-reactive protein for predicting cardiovascular and all-cause mortality in type 2 diabetic patients: A meta-analysis. Cytokine 2019, 117, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.K.; Bartz, T.M.; Mukamal, K.J.; Djousse, L.; Kizer, J.R.; Tracy, R.P.; Zieman, S.J.; Rimm, E.B.; Siscovick, D.S.; Shlipak, M.; et al. Fetuin-A, type 2 diabetes, and risk of cardiovascular disease in older adults: The cardiovascular health study. Diabetes Care 2013, 36, 1222–1228. [Google Scholar] [CrossRef] [Green Version]
- Icer, M.A.; Yıldıran, H. Effects of fetuin-A with diverse functions and multiple mechanisms on human health. Clin. Biochem. 2021, 88, 1–10. [Google Scholar] [CrossRef]
- Mancio, J.; Barros, A.S.; Conceicao, G.; Pessoa-Amorim, G.; Santa, C.; Bartosch, C.; Ferreira, W.; Carvalho, M.; Ferreira, N.; Vouga, L.; et al. Epicardial adipose tissue volume and annexin A2/fetuin-A signalling are linked to coronary calcification in advanced coronary artery disease: Computed tomography and proteomic biomarkers from the EPICHEART study. Atherosclerosis 2020, 292, 75–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eleftheriadou, I.; Grigoropoulou, P.; Kokkinos, A.; Mourouzis, I.; Perrea, D.; Katsilambros, N.; Sfikakis, P.P.; Tentolouri, N. Association of plasma fetuin-a levels with peripheral arterial disease and lower extremity arterial calcification in subjects with type 2 diabetes mellitus. J. Diabetes Complicat. 2017, 31, 599–604. [Google Scholar] [CrossRef]
- Marseglia, L.; Manti, S.; D’Angelo, G.; Nicotera, A.; Parisi, E.; Di Rosa, G.; Gitto, E.; Arrigo, T. Oxidative stress in obesity: A critical component in human diseases. Int. J. Mol. Sci. 2014, 16, 378–400. [Google Scholar] [CrossRef] [Green Version]
- Roh, H.T.; Cho, S.Y.; So, W.Y. Obesity promotes oxidative stress and exacerbates blood-brain barrier disruption after high-intensity exercise. J. Sport Health Sci. 2017, 6, 225–230. [Google Scholar] [CrossRef] [Green Version]
- Dudina, A.; Cooney, M.T.; De Bacquer, D.; De Backer, G.; Ducimetiere, P.; Jousilahti, P.; Keil, K.; Menotti, A.; Njølstad, I.; Oganov, R. Relationships between body mass index, cardiovascular mortality, and risk factors: A report from the SCORE investigators. Eur. J. Cardiovasc. Prev. Rehabil. 2011, 18, 731–742. [Google Scholar] [CrossRef] [PubMed]
- Khosravi, A.; Tabib, A.A.; Golshadi, I.; Siadat, Z.D.; Bahonar, A.; Zarfeshani, S. The Relationship between Weight and CVD Risk Factors in a Sample Population from Central Iran (Based on IHHP). ARYA Atheroscler. 2012, 8, 82–89. [Google Scholar]
- Fan, H.; Li, X.; Zheng, L.; Chen, X.; Lan, Q.; Wu, H.; Ding, X.; Qian, D.; Shen, Y.; Yu, Z. Abdominal obesity is strongly associated with Cardiovascular Disease and its Risk Factors in Elderly and very Elderly Community-dwelling Chinese. Sci. Rep. 2016, 6, 21521. [Google Scholar] [CrossRef] [Green Version]
- Schneider, H.J.; Friedrich, N.; Klotsche, J.; Pieper, L.; Nauck, M.; John, U.; Dörr, M.; Felix, S.; Lehnert, H.; Pittrow, D.; et al. The predictive value of different measures of obesity for incident cardiovascular events and mortality. J. Clin. Endocrinol. Metab. 2010, 95, 1777–1785. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Zagaria, A.B. Addressing Obesity in Aging Patients. Med. Clin. N. Am. 2018, 102, 65–85. [Google Scholar] [CrossRef] [PubMed]
- Decaria, J.E.; Sharp, C.; Petrella, R.J. Scoping review report: Obesity in older adults. Int. J. Obes. (Lond). 2012, 36, 1141–1150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maas, A.H.E.M.; Appelman, Y.E.A. Gender differences in coronary heart disease. Neth. Heart J. 2010, 18, 598–602. [Google Scholar] [CrossRef] [PubMed]
- Coll, P.P.; Roche, V.; Olsen, J.S.; Voit, J.H.; Bowen, E.; Kumar, M. The Prevention of Cardiovascular Disease in Older Adults. J. Am. Geriatr. Soc. 2020, 68, 1096–1106. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef]
- Forti, P.; Maioli, F.; Procaccianti, G.; Nativio, V.; Lega, M.V.; Coveri, M.; Zoli, M.; Sacquegna, T. Independent predictors of ischemic stroke in the elderly: Prospective data from a stroke unit. Neurology 2013, 80, 29–38. [Google Scholar] [CrossRef]
- Howard, G.; Goff, D.C. Population shifts and the future of stroke: Forecasts of the future burden of stroke. Ann. N. Y. Acad. Sci. 2012, 1268, 14–20. [Google Scholar] [CrossRef]
- Pase, M.P. Modifiable vascular markers for cognitive decline and dementia: The importance of arterial aging and hemodynamic factors. J. Alzheimers Dis. 2012, 32, 653–663. [Google Scholar] [CrossRef]
- Seshadri, S.; Wolf, P.A. Lifetime risk of stroke and dementia: Current concepts, and estimates from the Framingham Study. Lancet Neurol. 2007, 6, 1106–1114. [Google Scholar] [CrossRef]
- Garrison, S.R.; Kolber, M.R.; Korownyk, C.S.; McCracken, R.K.; Heran, B.S.; Allan, G.M. Blood pressure targets for hypertension in older adults. Cochrane Database Syst. Rev. 2017, 8, CD011575. [Google Scholar] [CrossRef]
- Cornelius, M.E.; Wang, T.W.; Jamal, A.; Loretan, C.G.; Neff, L.J. Tobacco Product Use Among Adults—United States, 2019. MMWR Morb. Mortal Wkly Rep. 2020, 69, 1736–1742. [Google Scholar] [CrossRef]
- Bennett, D.A.; Krishnamurthi, R.V.; Barker-Collo, S.; Forouzanfar, M.H.; Naghavi, M.; Connor, M.; Lawes, C.M.M.; Moran, A.E.; AndersonM, L.M.; Roth, G.A.; et al. The global burden of ischemic stroke: Findings of the GBD 2010 study. Glob. Heart 2014, 9, 107–112. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Li, S.; Zhend, K.; Wang, H.; Xie, Y.; Xu, P.; Dai, Z.; Gu, M.; Xia, Y.; Zhao, M.; et al. Impact of Smoking Status on Stroke Recurrence. J. Am. Heart Assoc. 2019, 8, e011696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paterson, K.E.; Myint, P.K.; Jennings, A.; Bain, L.K.M.; Lentjes, M.A.H.; Khaw, K.T.; Welch, A.A. Mediterranean Diet Reduces Risk of Incident Stroke in a Population with Varying Cardiovascular Disease Risk Profiles. Stroke 2018, 49, 2415–2420. [Google Scholar] [CrossRef]
- Rippe, J.M. Lifestyle Strategies for Risk Factor Reduction, Prevention, and Treatment of Cardiovascular Disease. Am. J. Lifestyle Med. 2019, 13, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.K.; Bluementhal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef] [PubMed]
- Blood Pressure Lowering Treatment Trialists Collaboration. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: An individual participant-level data meta-analysis. Lancet 2021, 397, 1625–1636. [Google Scholar] [CrossRef]
- Teo, K.K.; Ounpuu, S.; Hawken, S.; Pandey, M.R.; Valentin, V.; Hunt, D.; Diaz, R.; Rashed, W.; Freeman, R.; Jiang, L.; et al. Tobacco use and risk of myocardial infarction in 52 countries in the INTERHEART study: A case-control study. Lancet 2006, 368, 647–658. [Google Scholar] [CrossRef]
- Johanneke Van Den Berg, M.; Graaff, Y.; Deckers, J.W.; De Kanter, W.; Algra, A.; Kappelle, L.J.; de Borst, G.J.; Cramer, M.J.M.; Visseren, F.L.J.; SMART study group. Smoking cessation and risk of recurrent cardiovascular events and mortality after a first manifestation of arterial disease. Am. Heart J. 2019, 213, 112–122. [Google Scholar] [CrossRef]
- Ramsden, C.E.; Zamora, D.; Majchzak-Hong, S.; Faurot, K.R.; Broste, S.K.; Frantz, R.P.; Davis, J.M.; Ringel, A.; Suchindran, C.M.; Hibbeln, J.R. Re-evaluation of the traditional diet-heart hypothesis: Analysis of recovered data from Minnesota Coronary Experiment (1968–1973). BMJ 2016, 353, i1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koolhaas, C.M.; Dhana, K.; Golubic, R.; Schoufour, J.D.; Hofman, A.; Rooij, F.J.A.; Franco, O.H. Physical Activity Types and Coronary Heart Disease Risk in Middle-Aged and Elderly Persons: The Rotterdam Study. Am. J. Epidemiol. 2016, 183, 729–738. [Google Scholar] [CrossRef] [PubMed]
- Han, B.H.; Sutin, D.; Williamson, J.D.; Davis, B.R.; Piller, L.B.; Pervin, H.; Pressel, S.P.; Blaum, C.S.; ALLHAT Collaborative Research Group. Effect of Statin Treatment vs Usual Care on Primary Cardiovascular Prevention Among Older Adults: The ALLHAT-LLT Randomized Clinical Trial. JAMA Intern. Med. 2017, 177, 955–965. [Google Scholar] [CrossRef] [PubMed]
- Awad, K.; Mohammed, M.; Zaki, M.M.; Abushouk, A.I.; Lip, G.Y.H.; Lavie, C.J.; Toth, P.P.; Jukema, J.W.; Sattar, N. Lipid and Blood Pressure Meta-analysis Collaboration (LBPMC) Group and the International Lipid Expert Panel (ILEP). Association of statin use in older people primary prevention group with risk of cardiovascular events and mortality: A systematic review and meta-analysis of observational studies. BMC Med. 2021, 19, 139. [Google Scholar]
- Brach, J.S.; Solomon, C.; Naydeck, B.L.; Sutton-Tyrrell, K.; Enright, P.L.; Swords-Jenny, N. Incident physical disability in people with lower extremity peripheral arterial disease: The role of cardiovascular disease. J. Am. Geriatr. Soc. 2008, 56, 1037–1044. [Google Scholar] [CrossRef]
- Paneni, F.; Beckman, J.; Creager, M.A.; Cosentino, F. Diabetes and vascular disease: Pathophysiology, clinical consequences, and medical therapy: Part I. Eur. Heart J. 2013, 34, 2436–2443. [Google Scholar] [CrossRef]
- Velescu, A.; Clara, A.; Penafiel, J.; Grau, M.; Degano, I.R.; Ramos, R.; Ramos, R.; Marrugat, J.; Elosua, R. Peripheral Arterial Disease Incidence and Associated Risk Factors in a Mediterranean Population-Based Cohort. The REGICOR Study. Eur. J. Vascul. Endovasc. Surg. 2016, 51, 696–705. [Google Scholar] [CrossRef]
- Conen, D.; Everett, B.M.; Kurth, T.; Creager, M.A.; Buring, J.E.; Ridker, P.M.; Pradhan, R.D. Smoking, Smoking Cessation and Risk of Symptomatic Peripheral Artery Disease in Women: A Prospective Study. Ann. Intern. Med. 2011, 154, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Olin, J.W.; White, C.J.; Armstrong, E.J.; Kadian-Dodov, D.; Hiatt, W.R. Peripheral Artery Disease: Evolving Role of Exercise, Medical Therapy, and Endovascular Options. J. Am. Coll. Cardiol. 2016, 67, 1338–1357. [Google Scholar] [CrossRef]
- Hussain, M.A.; Al-Omran, M.; Creager, M.A.; Anand, S.S.; Verma, S.; Bhatt, D.L. Antithrombotic Therapy for Peripheral Artery Disease: Recent Advances. J. Am. Coll. Cardiol. 2018, 71, 2450–2467. [Google Scholar] [CrossRef]
- Alexa, I.D.; Prada, G.I.; Donca, V.I.; Mos, L.M.; Alexa, O. Improving Quality of Life of Elderly People Aged 85 and Older by Improving Treatment Adherence. In Proceedings of the 4th IEEE International Conference on E-Health and Bioengineering, Iaşi, Romania, 21–23 November 2013. [Google Scholar]
- Langhammer, B.; Bergland, A.; Rydwik, E. The Importance of Physical Activity Exercise among Older People. Bio. Med. Res. Int. 2018, 7856823. [Google Scholar] [CrossRef] [PubMed]
- Nied, R.J.; Franklin, B. Promoting and Prescribing Exercise for the Elderly. Am. Fam. Physician 2002, 65, 419–427. [Google Scholar]
- Ko, G.; Davidson, L.E.; Brennan, A.M.; Lam, M.; Ross, R. Abdominal Adiposity, Not Cardiorespiratory Fitness, Mediates the Exercise-Induced Change in Insulin Sensitivity in Older Adults. PLoS ONE 2016, 11, e0167734. [Google Scholar] [CrossRef]
- Stewart, J.; Manmathan, G.; Wilkinson, P. Primary prevention of cardiovascular disease: A review of contemporary guidance and literature. JRSM Cardiovasc. Dis. 2017, 6, 2048004016687211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, D.; Meng, J. Exercise for Prevention and Relief of Cardiovascular Disease: Prognoses, Mechanisms, and Approaches. Oxid. Med. Cell. Longev. 2019, 2019, 3756750. [Google Scholar] [CrossRef] [Green Version]
- Mandolesi, L.; Polverino, A.; Montuori, S.; Foti, F.; Ferraioli, G.; Sorrentino, P.; Sorrentino, G. Effects of Physical Exercise on Cognitive Functioning and Wellbeing: Biological and Psychological Benefits. Front. Psychol. 2018, 9, 509. [Google Scholar] [CrossRef]
- Cheng, S.J.; Yu, H.K.; Chen, Y.C.; Chen, C.Y.; Lien, W.C.; Yang, P.Y.; Hu, G.C. Physical Activity and Risk of Cardiovascular Disease Among Older Adults. Int. J. Gerontol. 2013, 7, 133–136. [Google Scholar] [CrossRef] [Green Version]
- NHS. Physical Activity Guidelines for Older Adults. Available online: https://www.nhs.uk/live-well/exercise/physical-activity-guidelines-older-adults (accessed on 10 August 2021).
- Centers for Disease Control and Prevention. How Much Physical Activity Do Older Adults Need? Available online: https://www.cdc.gov/physicalactivity/basics/older_adults/index.htm (accessed on 28 August 2021).
- Shaked, O.; Cohen, G.; Goshen, A.; Shimony, T.; Shohat, T.; Gerber, Y. Physical Activity and Long-Term Mortality Risk in Older Adults with and without Cardiovascular Disease: A Nationwide Cohort Study. Gerontology 2021, 25, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lachman, S.; Boekholdt, S.M.; Luben, R.N.; Sharp, S.J.; Brage, S.; Khaw, K.T.; Peters, R.J.; Wareham, N.J. Impact of physical activity on the risk of cardiovascular disease in middle-aged and older adults: EPIC Norfolk prospective population study. Eur. J. Prev. Cardiol. 2018, 25, 200–208. [Google Scholar] [CrossRef]
- Izquierdo, M.; Duque, G.; Morley, J.E. Physical activity guidelines for older people: Knowledge gaps and future directions. Lancet Health Longev. 2021, 2, e380–e383. [Google Scholar] [CrossRef]
- Muntaner-Mas, A.; Vidal-Conti, J.; Borràs, P.A.; Ortega, F.B.; Palou, P. Effects of a Whatsapp-delivered physical activity intervention to enhance health-related physical fitness components and cardiovascular disease risk factors in older adults. J. Sports Med. Phys. Fit. 2017, 57, 90–102. [Google Scholar] [CrossRef]
- McGarrigle, L.; Todd, C. Promotion of Physical Activity in Older People Using mHealth and eHealth Technologies: Rapid Review of Reviews. J. Med. Internet Res. 2020, 22, e22201. [Google Scholar] [CrossRef]
- Filar-Mierzwa, K.; Długosz-Boś, M.; Marchewka, A.; Aleksander-Szymanowicz, P. Effect of different forms of physical activity on balance in older women. J. Women Aging 2021, 33, 487–502. [Google Scholar] [CrossRef]
- Hall, K.E.; McDonald, M.W.; Grise, K.N.; Campos, O.A.; Noble, E.G.; Melling, C.W.J. The role of resistance and aerobic exercise training on insulin sensitivity measures in STZ-induced Type 1 diabetic rodents. Metabolism 2013, 62, 1485–1494. [Google Scholar] [CrossRef] [PubMed]
- Zheng, F.; Cai, Y. Concurrent exercise improves insulin resistance and nonalcoholic fatty liver disease by upregulating PPAR-γ and genes involved in the beta-oxidation of fatty acids in ApoE-KO mice fed a high-fat diet. Lipids Health Dis. 2019, 18, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, C.H.; Youg, J.H.; Park, J.Y.; Hong, S.K.; Park, K.S.; Park, S.W. Effects of high-fat diet and exercise training on intracellular glucose metabolism in rats. Am. J. Physiol. Endocrinol. Metab. 2000, 278, E977–E984. [Google Scholar] [CrossRef]
- Diaz, K.M.; Schimbo, D. Physical activity and the prevention of hypertension. Curr. Hypertens. Rep. 2013, 15, 659–668. [Google Scholar] [CrossRef] [Green Version]
- Carpio-Rivera, E.; Moncada-Jimenez, J.; Salazar-Rojas, W.; Solera-Herrera, A. Acute Effects of Exercise on Blood Pressure: A Meta-Analytic Investigation. Arquivos Brasileiros de Cardiologia. 2016, 106, 422–433. [Google Scholar] [CrossRef]
- Tsukiyama, Y.; Ito, T.; Nagaoka, K.; Eguchi, E.; Ogino, K. Effects of exercise training on nitric oxide, blood pressure and antioxidant enzymes. J. Clin. Biochem. Nutr. 2017, 60, 180–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roque, F.R.; Briones, A.M.; Garcia-Redondo, A.B.; Galan, M.; Martinez-Revelles, S.; Avendano, M.S.; Cachofeiro, V.; Fernandes, T.; Vassallo, D.V.; Oliveira, E.D. Aerobic exercise reduces oxidative stress and improves vascular changes of small mesenteric and coronary arteries in hypertension. Br. J. Pharmacol. 2013, 168, 686–703. [Google Scholar] [CrossRef] [Green Version]
- Brito, A.F.; Silva, A.S.; Souza, I.L.L.; Pereira, J.C.; Da Silva, B.A. Intensity of swimming exercise influences aortic reactivity in rats. Braz. J. Med. Biol. Res. 2015, 48, 996–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciumărnean, L.; Milaciu, M.V.; Negrean, V.; Orășan, O.H.; Vesa, S.C.; Sălăgean, O.; Iluţ, S.; Vlaicu, S.I. Cardiovascular Risk Factors and Physical Activity for the Prevention of Cardiovascular Diseases in the Elderly. Int. J. Environ. Res. Public Health 2022, 19, 207. https://doi.org/10.3390/ijerph19010207
Ciumărnean L, Milaciu MV, Negrean V, Orășan OH, Vesa SC, Sălăgean O, Iluţ S, Vlaicu SI. Cardiovascular Risk Factors and Physical Activity for the Prevention of Cardiovascular Diseases in the Elderly. International Journal of Environmental Research and Public Health. 2022; 19(1):207. https://doi.org/10.3390/ijerph19010207
Chicago/Turabian StyleCiumărnean, Lorena, Mircea Vasile Milaciu, Vasile Negrean, Olga Hilda Orășan, Stefan Cristian Vesa, Octavia Sălăgean, Silvina Iluţ, and Sonia Irina Vlaicu. 2022. "Cardiovascular Risk Factors and Physical Activity for the Prevention of Cardiovascular Diseases in the Elderly" International Journal of Environmental Research and Public Health 19, no. 1: 207. https://doi.org/10.3390/ijerph19010207