
Life-Threatening Necrotizing Pneumonia with Panton–Valentine Leukocidin-Producing, Methicillin-Sensitive Staphylococcus aureus in a Healthy Male Co-Infected with Influenza B

 , , ,
, , ,
Abstract
:1. Introduction
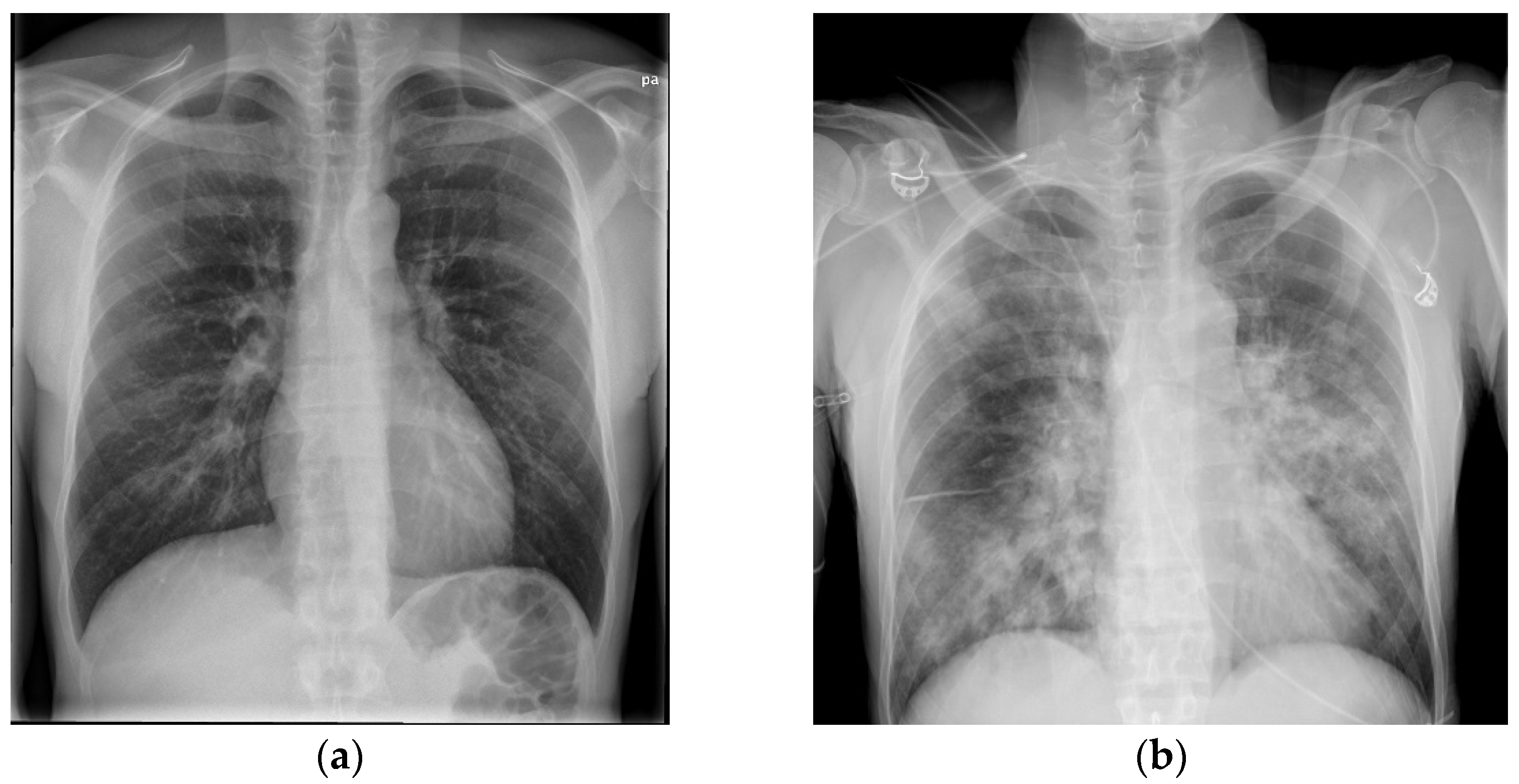
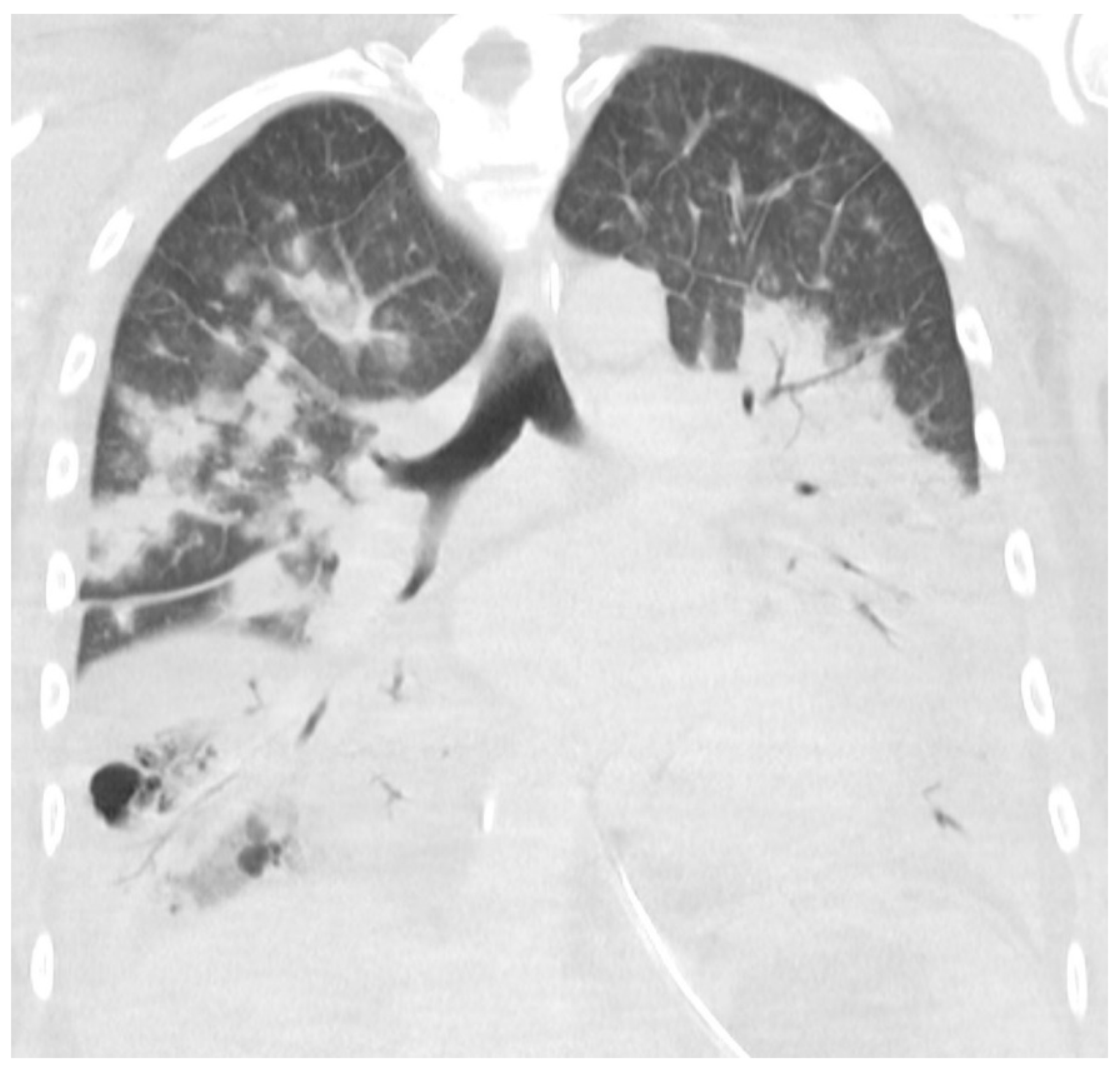
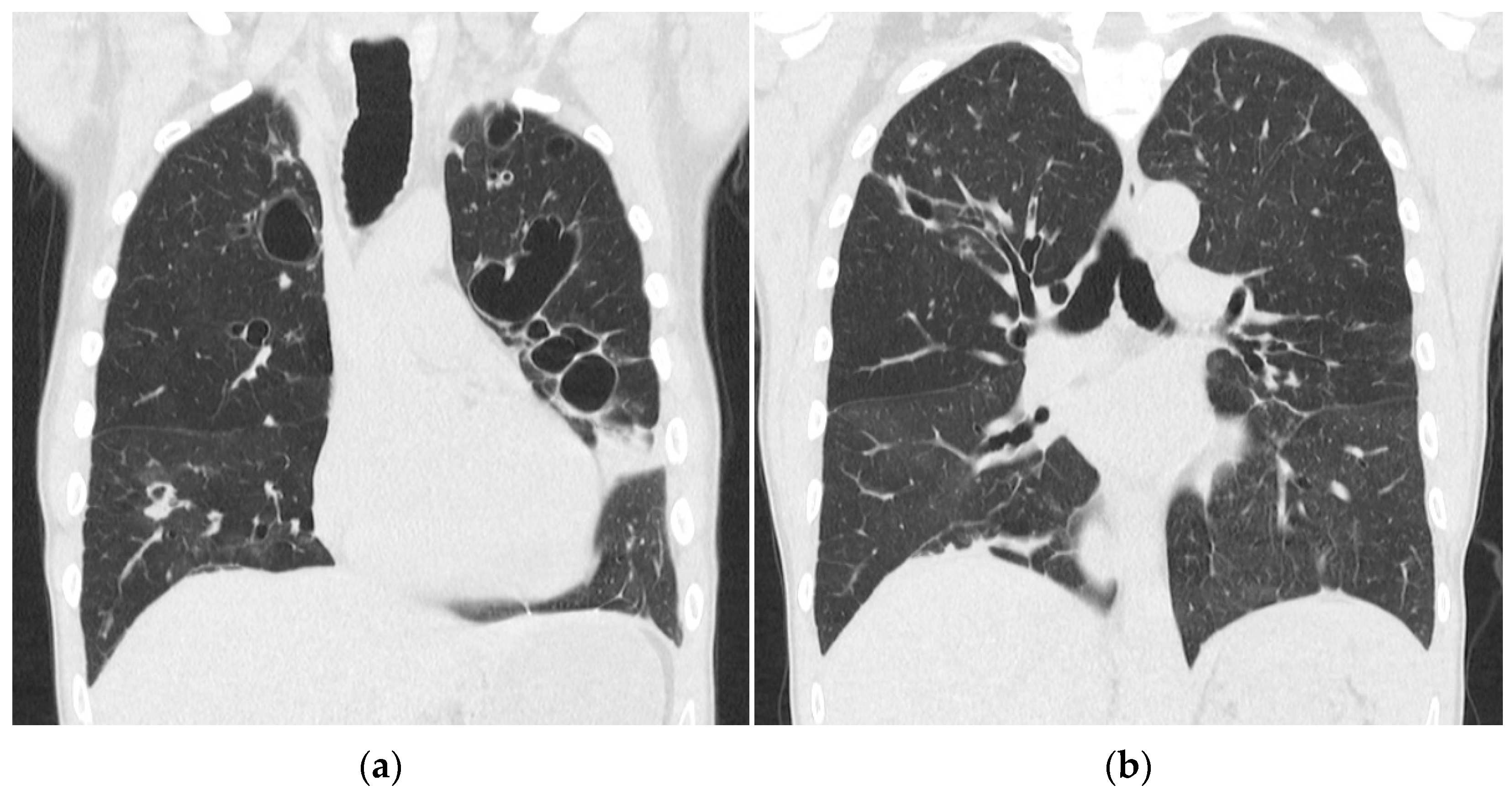
2. Case Presentation
3. Materials and Methods
Characterization of the Bacterial Isolate
4. Results
5. Discussion
6. Conclusions
- This case illustrates the rapid progression of necrotizing pneumonia causing severe lung damage.;
- Necrotizing pneumonia should be considered in critically ill, previously healthy patients with rapidly progressing symptoms;
- Necrotizing pneumonia should be considered if the patient has been traveling in places with a high prevalence of PVL-positive S. aureus during influenza season.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Larsen, A.R.; Stegger, M.; Sørum, M. Spa typing directly from a mecA, spa and pvl multiplex PCR assay-a cost-effective improvement for methicillin-resistant Staphylococcus aureus surveillance. Clin. Microbiol. Infect. 2008, 14, 611–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammerum, A.M.; Porsbo, L.J.; Hansen, F.; Roer, L.; Kaya, H.; Henius, A.; Møller, K.L.; Justesen, U.S.; Søes, L.; Røder, B.L.; et al. Surveillance of OXA-244-producing Escherichia coli and epidemiologic investigation of cases, Denmark, January 2016 to August 2019. Eurosurveillance 2020, 25, 1900742. [Google Scholar] [CrossRef] [PubMed]
- Bortolaia, V.; Kaas, R.S.; Ruppe, E.; Roberts, M.C.; Schwarz, S.; Cattoir, V.; Philippon, A.; Allesoe, R.L.; Rebelo, A.R.; Florensa, A.F.; et al. ResFinder 4.0 for predictions of phenotypes from genotypes. J. Antimicrob. Chemother. 2020, 75, 3471–3500. [Google Scholar] [CrossRef] [PubMed]
- Joensen, K.G.; Scheutz, F.; Lund, O.; Hasman, H.; Kaas, R.S.; Nielsen, E.M.; Aarestrup, F.M. Real-time whole-genome sequencing for routine typing, surveillance, and outbreak detection of verotoxigenic Escherichia coli. J. Clin. Microbiol. 2014, 52, 1501–1510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahl, J.W.; Lemmer, D.; Travis, J.; Schupp, J.M.; Gillece, J.D.; Aziz, M.; Driebe, E.M.; Drees, K.P.; Hicks, N.D.; Williamson, C.H.D.; et al. NASP: An accurate, rapid method for the identification of SNPs in WGS datasets that supports flexible input and output formats. Microb. Genom. 2016, 2, e000074. [Google Scholar] [CrossRef] [PubMed]
- Leopold, S.R.; Goering, R.V.; Witten, A.; Harmsen, D.; Mellmann, A. Bacterial whole-genome sequencing revisited: Portable, scalable, and standardized analysis for typing and detection of virulence and antibiotic resistance genes. J. Clin. Microbiol. 2014, 52, 2365–2370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baig, S.; Larsen, A.R.; Simões, P.M.; Laurent, F.; Johannesen, T.B.; Lilje, B.; Tristan, A.; Schaumburg, F.; Egyir, B.; Cirkovic, I.; et al. Evolution and Population Dynamics of Clonal Complex 152 Community-Associated Methicillin-Resistant Staphylococcus aureus. MSphere 2020, 5, 4. [Google Scholar] [CrossRef] [PubMed]
- Gillet, Y.; Issartel, B.; Vanhems, P.; Fournet, J.-C.; Lina, G.; Bes, M.; Vandenesch, F.; Piémont, Y.; Brousse, N.; Floret, D.; et al. Association between Staphylococcus aureus strains carrying gene for Panton-Valentine leukocidin and highly lethal necrotising pneumonia in young immunocompetent patients. Lancet 2002, 359, 753–759. [Google Scholar] [CrossRef]
- Löffler, B.; Hussain, M.; Grundmeier, M.; Brück, M.; Holzinger, D.; Varga, G.; Roth, J.; Kahl, B.; Proctor, R.A.; Peters, G. Staphylococcus aureus panton-valentine leukocidin is a very potent cytotoxic factor for human neutrophils. PLoS Pathog. 2010, 6, e1000715. [Google Scholar] [CrossRef] [PubMed]
- Lina, G.; Piémont, Y.; Godail-Gamot, F.; Bes, M.; Peter, M.-O.; Gauduchon, V.; Vandenesch, F.; Etienne, J. Involvement of Panton-Valentine Leukocidin-Producing Staphylococcus aureus in Primary Skin Infections and Pneumonia. Clin. Infect. Dis. 1999, 29, 1128–1132. [Google Scholar] [CrossRef] [PubMed]
- Löffler, B.; Niemann, S.; Ehrhardt, C.; Horn, D.; Lanckohr, C.; Lina, G.; Lugwig, S.; Peters, G. Pathogenesis of Staphylococcus aureus necrotizing pneumonia: The role of PVL and an influenza coinfection. Expert. Rev. Anti. Infect. Ther. 2013, 11, 1041–1051. [Google Scholar] [CrossRef] [PubMed]
- de la Santé, O.M.; World Health Organization. Review of Global Influenza Activity, October 2016–October 2017. Wkly Epidemilogical Rec. 2017, 92, 761–779. [Google Scholar]
- Zanger, P.; Nurjadi, D.; Schleucher, R.; Scherbaum, H.; Wolz, C.; Kremsner, P.G.; Schulte, B. Import and Spread of Panton-Valentine Leukocidin–Positive Staphylococcus aureus Through Nasal Carriage and Skin Infections in Travelers Returning From the Tropics and Subtropics. Clin. Infect. Dis. 2012, 54, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Correa-Jiménez, O.; Pinzón-Redondo, H.; Reyes, N. High frequency of Panton-Valentine leukocidin in Staphylococcus aureus causing pediatric infections in the city of Cartagena-Colombia. J. Infect. Public Health 2016, 9, 415–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bybeck Nielsen, A.; Larsen, A.R.; Petersen, A.; Schønheyder, H.C.; Westh, H.; Benfield, T.; Nygaard, U. Clinical Manifestations in Children with Staphylococcal Bacteremia Positive for Panton-Valentine Leucocidin: A Nationwide Survey in a Low Methicillin-Resistance Setting. Pediatr. Infect. Dis. J. 2020, 39, e274–e276. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Unit | Ref | Day 1 | Day 3 1 | Day 4 | |
|---|---|---|---|---|---|
| B-hemoglobin | micromol/L | 8.0–10.5 | 7.7 | 8.7 | 8.2 |
| B-leukocytes | ×109/L | 3.0–10.0 | 5 | 1.1 | 1.3 |
| B-thrombocytes | ×109/L | 120–350 | 145 | 113 | 46 |
| B-neutrophils | ×109/L | 2.0–8.0 | 3.08 | 0.45 | 0.28 |
| P-potassium | mmol/L | 3.5–4.6 | 3.4 | 3.3 | 4.7 |
| P-sodium | mmol/L | 137–144 | 133 | 127 | 142 |
| P-creatinine | μmol/L | 60–105 | 83 | 160 | 206 |
| P-carbamide | mmol/L | 3.2–8.1 | - | 14.4 | 17.4 |
| P-albumin | g/L | 35–52 | - | 26 | 24 |
| INR | 0.8–1.2 | - | 1.6 | 1.8 | |
| APTT | s | 23–35 | - | 41 | 36 |
| CRP | mg/L | <6 | 11 | 370 | 494 |
| Day 3 | Benzylpenicillin 1.2 g × 4 | Ciprofloxacin 400 mg × 2 | - |
| Day 3 | Meropenem 2 g × 3 | Ciprofloxacin 400 mg × 2 | - |
| Day 4 | Meropenem 2 g × 3 | Moxifloxacin 400 mg × 1 1 | - |
| Day 6 | Meropenem 2 g × 3 | Moxifloxacin 400 mg × 1 | Clindamycin 600 mg × 3 2 |
| Day 7 | Meropenem 2 g × 3 | Moxifloxacin 400 mg × 1 | Clindamycin 600 mg × 3 |
| Day 8 | Meropenem 2 g × 3 | Moxifloxacin 400 mg × 1 | Clindamycin 600 mg × 3 |
| Day 11 | Meropenem 2 g × 3 | Moxifloxacin 400 mg × 1 | Clindamycin 600 mg × 3 |
| Day 12 | Meropenem 2 g × 3 | - | Clindamycin 600 mg × 3 |
| Day 15 | - | - | Clindamycin 900 mg × 3 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Larsen, S.A.H.; Kyhl, K.; Baig, S.; Petersen, A.; av Steinum, M.R.; Clemmensen, S.; Jensen, E.; á Steig, T.; Gaini, S. Life-Threatening Necrotizing Pneumonia with Panton–Valentine Leukocidin-Producing, Methicillin-Sensitive Staphylococcus aureus in a Healthy Male Co-Infected with Influenza B. Infect. Dis. Rep. 2022, 14, 12-19. https://doi.org/10.3390/idr14010002
Larsen SAH, Kyhl K, Baig S, Petersen A, av Steinum MR, Clemmensen S, Jensen E, á Steig T, Gaini S. Life-Threatening Necrotizing Pneumonia with Panton–Valentine Leukocidin-Producing, Methicillin-Sensitive Staphylococcus aureus in a Healthy Male Co-Infected with Influenza B. Infectious Disease Reports. 2022; 14(1):12-19. https://doi.org/10.3390/idr14010002
Chicago/Turabian StyleLarsen, Sara Agnete Hjort, Kasper Kyhl, Sharmin Baig, Andreas Petersen, Marita Reginsdóttir av Steinum, Sissal Clemmensen, Elin Jensen, Torkil á Steig, and Shahin Gaini. 2022. "Life-Threatening Necrotizing Pneumonia with Panton–Valentine Leukocidin-Producing, Methicillin-Sensitive Staphylococcus aureus in a Healthy Male Co-Infected with Influenza B" Infectious Disease Reports 14, no. 1: 12-19. https://doi.org/10.3390/idr14010002