
Evaluation of Potential Predictive Biomarkers for Defining Brain Radiotherapy Efficacy in Non-Small Cell Lung Cancer Patients with Brain Metastases: A Case Report and a Narrative Review
 , , and
, , and
Abstract
:1. Introduction
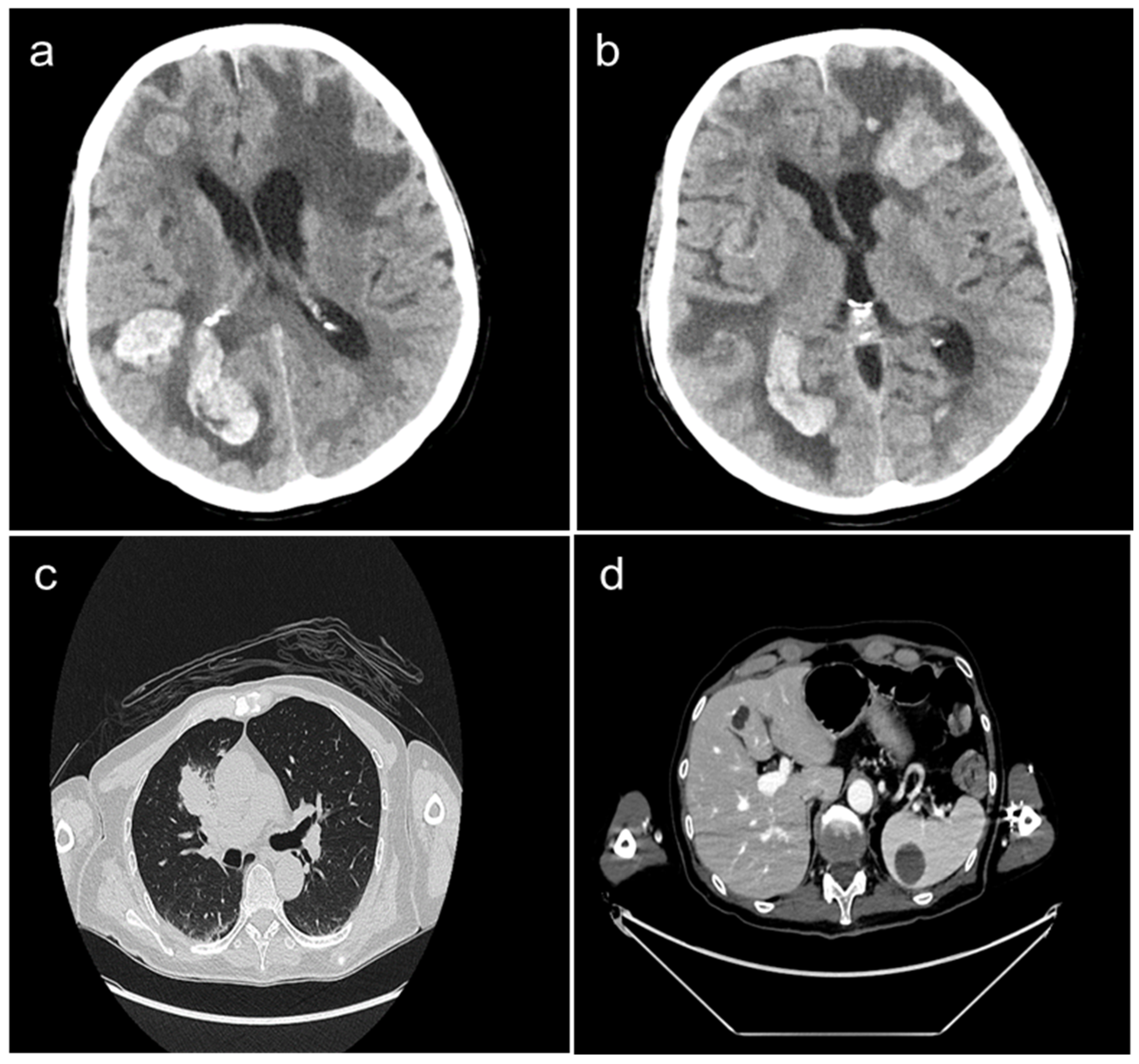
2. Case Presentation
3. Discussion
3.1. The Role of WBRT in Advanced NSCLC Patients with Brain Metastases
3.2. The Potential Role of BRAF Mutations and ICI-Based Immunotherapy in Advanced NSCLC Patients with Brain Metastases
3.3. The Role of the Scoring Systems to Predict the Benefit of WBRT in Advanced NSCLC Patients with Brain Metastases
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer Statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Duma, N.; Santana-Davila, R.; Molina, J.R. Non-Small Cell Lung Cancer: Epidemiology, Screening, Diagnosis, and Treatment. Mayo Clin. Proc. 2019, 94, 1623–1640. [Google Scholar] [CrossRef] [PubMed]
- Molina, J.R.; Yang, P.; Cassivi, S.D.; Schild, S.E.; Adjei, A.A. Non-Small Cell Lung Cancer: Epidemiology, Risk Factors, Treatment, and Survivorship. Mayo Clin. Proc. 2008, 83, 584–594. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, M.G.; Di Noia, V.; D’Argento, E.; Vita, E.; Damiano, P.; Cannella, A.; Ribelli, M.; Pilotto, S.; Milella, M.; Tortora, G.; et al. Oncogene-Addicted Non-Small-Cell Lung Cancer: Treatment Opportunities and Future Perspectives. Cancers 2020, 12, 1196. [Google Scholar] [CrossRef] [PubMed]
- Punekar, S.R.; Shum, E.; Grello, C.M.; Lau, S.C.; Velcheti, V. Immunotherapy in Non-Small Cell Lung Cancer: Past, Present, and Future Directions. Front. Oncol. 2022, 12, 877594. [Google Scholar] [CrossRef] [PubMed]
- Nayak, L.; Lee, E.Q.; Wen, P.Y. Epidemiology of Brain Metastases. Curr. Oncol. Rep. 2012, 14, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Ebben, J.D.; You, M. Brain Metastasis in Lung Cancer: Building a Molecular and Systems-Level Understanding to Improve Outcomes. Int. J. Biochem. Cell Biol. 2016, 78, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Nieder, C.; Guckenberger, M.; Gaspar, L.E.; Rusthoven, C.G.; De Ruysscher, D.; Sahgal, A.; Nguyen, T.; Grosu, A.L.; Mehta, M.P. Management of Patients with Brain Metastases from Non-Small Cell Lung Cancer and Adverse Prognostic Features: Multi-National Radiation Treatment Recommendations Are Heterogeneous. Radiat. Oncol. 2019, 14, 33. [Google Scholar] [CrossRef]
- Zabel, A.; Debus, J. Treatment of Brain Metastases from Non-Small-Cell Lung Cancer (NSCLC): Radiotherapy. Lung Cancer 2004, 45 (Suppl. 2), S247–S252. [Google Scholar] [CrossRef]
- Trikhirhisthit, K.; Setakornnukul, J.; Thephamongkhol, K. Added Survival Benefit of Whole Brain Radiotherapy in Brain Metastatic Non-Small Cell Lung Cancer: Development and External Validation of an Individual Prediction Model. Front. Oncol. 2022, 12, 911835. [Google Scholar] [CrossRef]
- Rades, D.; Hansen, H.C.; Schild, S.E.; Janssen, S. A New Diagnosis-Specific Survival Score for Patients to Be Irradiated for Brain Metastases from Non-Small Cell Lung Cancer. Lung 2019, 197, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Rades, D.; Dunst, J.; Schild, S.E. A New Scoring System to Predicting the Survival of Patients Treated with Whole-Brain Radiotherapy for Brain Metastases. Strahlenther. Onkol. 2008, 184, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Shaw, M.G.; Ball, D.L. Treatment of Brain Metastases in Lung Cancer: Strategies to Avoid/Reduce Late Complications of Whole Brain Radiation Therapy. Curr. Treat. Options Oncol. 2013, 14, 553–567. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Smit, E.F.; Groen, H.J.M.; Mazieres, J.; Besse, B.; Helland, Å.; Giannone, V.; D’Amelio, A.M.; Zhang, P.; Mookerjee, B.; et al. Dabrafenib plus Trametinib in Patients with Previously Untreated BRAFV600E-Mutant Metastatic Non-Small-Cell Lung Cancer: An Open-Label, Phase 2 Trial. Lancet Oncol. 2017, 18, 1307–1316. [Google Scholar] [CrossRef] [PubMed]
- Becco, P.; Gallo, S.; Poletto, S.; Frascione, M.P.M.; Crotto, L.; Zaccagna, A.; Paruzzo, L.; Caravelli, D.; Carnevale-Schianca, F.; Aglietta, M. Melanoma Brain Metastases in the Era of Target Therapies: An Overview. Cancers 2020, 12, 1640. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, E.J.; McKenna, W.G.; Hamilton, A.D.; Sebti, S.M.; Qian, Y.; Wu, J.M.; Muschel, R.J. Inhibiting Ras Prenylation Increases the Radiosensitivity of Human Tumor Cell Lines with Activating Mutations of Ras Oncogenes. Cancer Res. 1998, 58, 1754–1761. [Google Scholar]
- Sambade, M.J.; Peters, E.C.; Thomas, N.E.; Kaufmann, W.K.; Kimple, R.J.; Shields, J.M. Melanoma Cells Show a Heterogeneous Range of Sensitivity to Ionizing Radiation and Are Radiosensitized by Inhibition of B-RAF with PLX-4032. Radiother. Oncol. 2011, 98, 394–399. [Google Scholar] [CrossRef]
- Pulvirenti, T.; Hong, A.; Clements, A.; Forstner, D.; Suchowersky, A.; Guminski, A.; McNeil, C.; Hersey, P.; Fogarty, G.; Kefford, R.; et al. Acute Radiation Skin Toxicity Associated with BRAF Inhibitors. J. Clin. Oncol. 2016, 34, e17–e20. [Google Scholar] [CrossRef]
- Castellani, G.; Buccarelli, M.; Arasi, M.B.; Rossi, S.; Pisanu, M.E.; Bellenghi, M.; Lintas, C.; Tabolacci, C. BRAF Mutations in Melanoma: Biological Aspects, Therapeutic Implications, and Circulating Biomarkers. Cancers 2023, 15, 4026. [Google Scholar] [CrossRef]
- Tonse, R.; Rubens, M.; Appel, H.; Tom, M.C.; Hall, M.D.; Odia, Y.; McDermott, M.W.; Ahluwalia, M.S.; Mehta, M.P.; Kotecha, R. Systematic Review and Meta-Analysis of PD-L1 Expression Discordance between Primary Tumor and Lung Cancer Brain Metastasis. Neuro-Oncol. Adv. 2021, 3, vdab166. [Google Scholar] [CrossRef]
- Lorger, M.; Andreou, T.; Fife, C.; James, F. Immune Checkpoint Blockade—How Does It Work in Brain Metastases? Front. Mol. Neurosci. 2019, 12, 282. [Google Scholar] [CrossRef] [PubMed]
- Albarrán, V.; Chamorro, J.; Rosero, D.I.; Saavedra, C.; Soria, A.; Carrato, A.; Gajate, P. Neurologic Toxicity of Immune Checkpoint Inhibitors: A Review of Literature. Front. Pharmacol. 2022, 13, 774170. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, P.A.; Mandalà, M.; Ferrucci, P.F.; Guidoboni, M.; Rutkowski, P.; Ferraresi, V.; Arance, A.; Guida, M.; Maiello, E.; Gogas, H.; et al. Sequencing of Ipilimumab Plus Nivolumab and Encorafenib Plus Binimetinib for Untreated BRAF-Mutated Metastatic Melanoma (SECOMBIT): A Randomized, Three-Arm, Open-Label Phase II Trial. J. Clin. Oncol. 2023, 41, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Atkins, M.B.; Lee, S.J.; Chmielowski, B.; Tarhini, A.A.; Cohen, G.I.; Truong, T.-G.; Moon, H.H.; Davar, D.; O’Rourke, M.; Stephenson, J.J.; et al. Combination Dabrafenib and Trametinib Versus Combination Nivolumab and Ipilimumab for Patients with Advanced BRAF-Mutant Melanoma: The DREAMseq Trial-ECOG-ACRIN EA6134. J. Clin. Oncol. 2023, 41, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, L.; Scott, C.; Rotman, M.; Asbell, S.; Phillips, T.; Wasserman, T.; McKenna, W.G.; Byhardt, R. Recursive Partitioning Analysis (RPA) of Prognostic Factors in Three Radiation Therapy Oncology Group (RTOG) Brain Metastases Trials. Int. J. Radiat. Oncol. Biol. Phys. 1997, 37, 745–751. [Google Scholar] [CrossRef]
- Chowdhary, M.; Switchenko, J.M.; Press, R.H.; Jhaveri, J.; Buchwald, Z.S.; Blumenfeld, P.A.; Marwaha, G.; Diaz, A.; Wang, D.; Abrams, R.A.; et al. Post-Treatment Neutrophil-to-Lymphocyte Ratio Predicts for Overall Survival in Brain Metastases Treated with Stereotactic Radiosurgery. J. Neurooncol 2018, 139, 689–697. [Google Scholar] [CrossRef]
- Doi, H.; Nakamatsu, K.; Anami, S.; Fukuda, K.; Inada, M.; Tatebe, H.; Ishikawa, K.; Kanamori, S.; Monzen, H.; Nishimura, Y. Neutrophil-to-Lymphocyte Ratio Predicts Survival after Whole-Brain Radiotherapy in Non-Small Cell Lung Cancer. In Vivo 2019, 33, 195–201. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Description |
|---|---|
| Brain metastases | Alone |
| With other brain metastases | |
| Primary lesion | Controlled |
| Uncontrolled | |
| Primary lesion site | Lung |
| Breast | |
| Other | |
| Histology | Squamous |
| Adenocarcinoma | |
| Large cell | |
| Small cell | |
| Melanoma | |
| NSC | |
| Other | |
| Prior brain surgery | None |
| Yes | |
| Time interval from diagnosis of primary to brain metastases | ≤2 years |
| >2 years | |
| Headache | Absent |
| Present | |
| Seizure | Absent |
| Present | |
| Visual disturbance | Absent |
| Present | |
| Neurologic function | None |
| Minor | |
| Moderate | |
| Major | |
| Midline shift | No |
| Yes | |
| Mass effect | No |
| Yes | |
| Location of lesions | Frontal |
| Temporal | |
| Parietal | |
| Occipital | |
| Basal ganglia/thalamus | |
| Cerebellum | |
| Brainstem | |
| Sentinel location of lesions | Frontal |
| Temporal | |
| Parietal | |
| Occipital | |
| Basal ganglia/thalamus | |
| Cerebellum | |
| Brainstem | |
| Sentinel lesion side | Left |
| Right | |
| Midline | |
| Necrotic center | No |
| Yes | |
| Number of lesions | Single |
| Multiple | |
| Tumor response | Complete |
| Partial | |
| Stable | |
| Progression | |
| KPS | 30–40 |
| 50–60 | |
| 70–80 | |
| 90–100 | |
| Area (mm2) | 0–400 |
| 401–900 | |
| 901–1600 | |
| >1601 | |
| Age (years) | <40 |
| 40–44 | |
| 45–49 | |
| 50–54 | |
| 55–59 | |
| 60–64 | |
| 65–69 | |
| >70 | |
| Total dose (cGy) | 2400–3499 |
| 3500–4000 | |
| 4001–5279 | |
| 5280–6079 | |
| 6080–6719 | |
| 6720–9000 |
| Variable | Comparison | p-Value |
|---|---|---|
| Brain metastases | alone vs. with other metastases | <0.0001 |
| KPS | ≥70 vs. <70 | <0.0001 |
| Age (years) | <65 vs. ≥65 | <0.0001 |
| Prior surgery | no vs. yes | 0.005 |
| Histology | squamous vs. small cell vs. others | <0.0001 |
| Primary lesion | controlled vs. uncontrolled | <0.0001 |
| Primary site | breast vs. lung and others | 0.001 |
| Time interval | <2 years vs. >2 years | 0.004 |
| Number of lesions | single vs. multiple | 0.021 |
| Sentinel lesion side | left and/or right vs. midline | 0.038 |
| Sentinel location | frontal, temporal, parietal, occipital, and basal ganglia/thalamus vs. cerebellum and brainstem | 0.033 |
| Neurologic function | no vs. yes | <0.0001 |
| Headache | no vs. yes | 0.003 |
| Total dose (cGy) | ≥5200 vs. <5200 | <0.0001 |
| Tumor response | complete or partial vs. stable or progressive | 0.019 |
| Variable | Description |
|---|---|
| Age (years) | ≤62 |
| ≥63 | |
| Gender | Male |
| Female | |
| KPS | <70 |
| 70 | |
| >70 | |
| Interval from diagnosis of NSCLC to WBRT | ≤1 months |
| ≥2 months | |
| Pre-WBRT systemic treatment | No |
| Yes | |
| Control of the primary tumor | No |
| Yes | |
| Number of intracerebral metastases | 1–3 |
| ≥4 | |
| Metastasis outside the brain | No |
| Yes |
| Variable | Factor Score |
|---|---|
| Age (years) | |
| ≤62 | 4 |
| ≥63 | 2 |
| KPS | |
| <70 | 1 |
| 70 | 3 |
| >70 | 5 |
| Pre-WBRT systemic treatment | |
| No | 2 |
| Yes | 4 |
| Number of intracerebral metastases | |
| 1–3 | 4 |
| ≥4 | 2 |
| Metastasis outside the brain | |
| No | 5 |
| Yes | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luciano, A.; Liguori, L.; Polcaro, G.; Sabbatino, F.; Pepe, S. Evaluation of Potential Predictive Biomarkers for Defining Brain Radiotherapy Efficacy in Non-Small Cell Lung Cancer Patients with Brain Metastases: A Case Report and a Narrative Review. Clin. Pract. 2023, 13, 1549-1560. https://doi.org/10.3390/clinpract13060136
Luciano A, Liguori L, Polcaro G, Sabbatino F, Pepe S. Evaluation of Potential Predictive Biomarkers for Defining Brain Radiotherapy Efficacy in Non-Small Cell Lung Cancer Patients with Brain Metastases: A Case Report and a Narrative Review. Clinics and Practice. 2023; 13(6):1549-1560. https://doi.org/10.3390/clinpract13060136
Chicago/Turabian StyleLuciano, Angelo, Luigi Liguori, Giovanna Polcaro, Francesco Sabbatino, and Stefano Pepe. 2023. "Evaluation of Potential Predictive Biomarkers for Defining Brain Radiotherapy Efficacy in Non-Small Cell Lung Cancer Patients with Brain Metastases: A Case Report and a Narrative Review" Clinics and Practice 13, no. 6: 1549-1560. https://doi.org/10.3390/clinpract13060136