Benefits and Risks of Moderate Alcohol Consumption on Cardiovascular Disease: Current Findings and Controversies


1
Cardiovascular Program ICCC; Institut de Recerca Hospital Santa Creu i Sant Pau—IIB Sant Pau, Sant Antoni Maria Claret, 167, 08025 Barcelona, Spain
2
CIBER Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III (ISCIII), 28029 Madrid, Spain
*
Author to whom correspondence should be addressed.
Nutrients 2020, 12(1), 108; https://doi.org/10.3390/nu12010108
Submission received: 25 November 2019
/
Revised: 23 December 2019
/
Accepted: 25 December 2019
/
Published: 30 December 2019
(This article belongs to the Special Issue Alcoholic Beverages and Human Health)
Abstract
:Alcohol has a hormetic physiological behavior that results in either increased or decreased cardiovascular risk depending on the amount consumed, drinking frequency, pattern of consumption, and the outcomes under study or even the type of alcoholic beverage consumed. However, the vast majority of studies elucidating the role of alcohol in cardiovascular and in the global burden of disease relies on epidemiological studies of associative nature which carry several limitations. This is why the cardiovascular benefits of low–moderate alcohol consumption are being questioned and perhaps might have been overestimated. Thus, the aim of this review was to critically discuss the current knowledge on the relationship between alcohol intake and cardiovascular disease. Besides new evidence associating low and moderate alcohol consumption with decreased risk of cardiovascular disease, several questions remain unanswered related to the concrete amount of safe consumption, the type of alcoholic beverage, and the age-, sex-, and genetic/ethnical-specific differences in alcohol consumption.
Keywords:
alcohol; cardiovascular disease; polyphenols; wine; beer; spirits; myocardial infarction; stroke; hypertension; cholesterol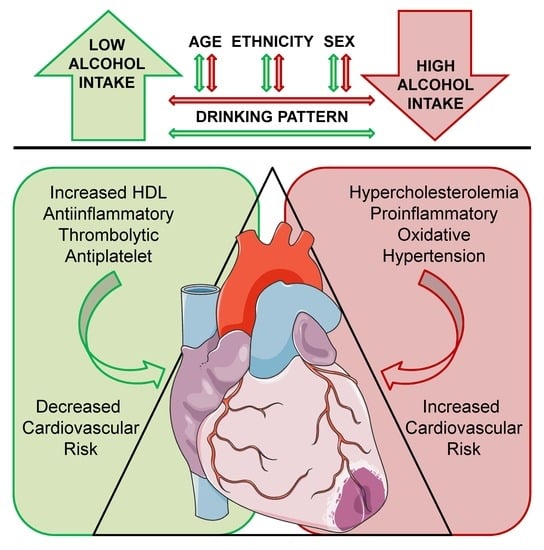
1. Introduction
Cardiovascular disease (CVD) is the leading cause of mortality in Europe (47% of total mortality) and one of the main causes of death worldwide (31% of all worldwide deaths) [1]. The influence of modifiable risk factors, such as smoking, high blood pressure, dyslipidemia, or poor diet, has been the object of investigation since the 1950s, and studies, such as the Framingham Heart Study [2] or the INTERHEART study [3], have shown that 90% of acute myocardial infarctions (AMIs) are attributable to potentially reversible risk factors, making the reduction of CV risk factors a high priority at the national and global levels. For health systems, alcohol consumption has been a matter of strong debate, because findings from different studies on the effects of alcohol in CVD have been contradictory. Whereas the majority of studies have found that low–moderate alcohol consumption may be beneficial [4]—or at least not harmful [5]—for the CV system by reducing the risk of major adverse CV events (MACE), excessive alcohol consumption increases the risk of CVD [6] and is associated with increased risk of more than 50 diseases [7]. As a matter of fact, alcohol use, besides the associated mental disorders caused by dependence [8], was the seventh leading risk factor for both deaths and disability-adjusted life years in 2016, accounting for 2.2% and 6.8% of total age-standardized deaths among females and males, respectively [9], and it has been identified as a major contributor to the burden of disease all over the globe [7,10].
According to the Dietary Guidelines Advisory Committee (US) [11], if alcohol is consumed, it should be consumed in moderation (≤1 and 2 drinks/day for women and men, respectively) and only by adults of legal drinking age. However, alcohol consumption guidelines vary substantially across the globe: low-risk guidelines range from 10–42 g/day or 98–140 g/week for women and 10–56 g/day or 150–280 g/week for men [12]. In 2016, 32.5% (25% women and 39% men) were current drinkers, and the mean amount of alcohol consumed was 0.73 standard drinks daily for females and 1.7 standard drinks daily for males [9].
Although moderate alcohol intake may have long-term CV benefits, even low consumption may have some risk. Alcohol has a hormetic physiological behavior that results in either increased or decreased CV risk depending on the amount consumed, drinking frequency, pattern of consumption (irregular or heavy/binge drinking, which is not uniformly defined), and the outcome under study [13,14], or even the type of alcoholic beverage consumed [15,16]. Added to this, some factors are critical in the interpretation of the health effects of alcohol consumption in available studies such as the measurement of alcohol consumption (and its misreporting) or the size of the drink (and the respective alcohol concentration). In addition, many individuals do not follow a regular pattern of alcohol drinking, and low–moderate consumption combined with episodes of heavy/binge alcohol drinking may not be beneficial for CVD. Moreover, alcohol intake in the majority of epidemiological studies is measured only once and through food frequency questionnaires or from quantity–frequency measures which may underestimate alcohol consumption, because the validity of self-reported alcohol intake has been questioned due to the fact of fear of stigmatization [10]. These questions need to be further addressed in epidemiological trials and alcohol exposure needs international standardization, because the cut-off points for the alcohol intake categories differ substantially among studies.
Considering all these limitations, the CV benefits of low–moderate alcohol consumption are being questioned, and it is considered that they might have been overestimated. Thus, the aim of this review was to critically discuss current knowledge on the relationship between alcohol intake and CVD.
2. Moderate versus Heavy Alcohol Intake
To analyze the effects of alcohol consumption in CVD and/or overall health, alcohol consumption levels must be defined. As summarized in Table 1, the US National Institute on Alcohol Abuse and Alcoholism defines drinking levels as low-risk drinking, moderate alcohol consumption, binge drinking, and heavy alcohol use [17], although some studies have their own classification. Moderate consumption of alcohol is referred to as regular daily consumption, whereas low intake, at the same maximum amount of alcohol intake as moderate consumption, is referred to as occasional and alternated with some days with no alcohol consumption. In this review, this classification will be used, and low-risk consumption will be referred to as low consumption.
As it will be further discussed, the relationship between CVD and alcohol intake is complex and responds to a hormetic behavior as reflected by U- or J-shaped relationships, with low–moderate intake being more protective than abstention or abusive drinking. However, and besides the drinking category, it is extremely important to consider that subjects in the non-drinker’s category (i.e, teetotalers) generally comprise both never drinkers and ex-drinkers (i.e., sick-quitters). Former drinkers may have ceased alcohol consumption because of serious or chronic illness, previous alcohol abuse, prodromal symptoms before clinical manifestations of major events, and/or because of prescription medications incompatible with alcohol consumption. It has been reported that teetotalers have significantly more prevalent CV risk factors than low to moderate drinkers which would overestimate the health benefits of alcohol intake [18,19,20] and bias or underestimate recent alcohol intake which might explain, in turn, the cross-study heterogeneity found in meta-analyses.
In addition, the main body of studies on alcohol’s impact on CVD relies on cohorts above 35 years of age which may bias the effect of lifetime drinking. It has been shown that drinking patterns vary during lifetime, whereas heavy intake of alcohol peaks in one’s 20s and is accompanied with episodes of binge drinking (in which, by coincidence, CVD controls are rare [21]) and decreases to minimum in one’s 40s. In fact, heavy and irregular binge drinking (>60 g alcohol) is associated to increased arterial stiffness [22], even at early ages [23], and with a 45% increased risk of ischemic heart disease compared to moderate drinking [24]. Therefore, subjects with heavy/binge regular drinking in their 20s are more prone to be abstainers above 35 years of age; therefore, the CV risk among these subjects—considered teetotalers in several studies—may be high compared to lifetime moderate drinkers because of underestimated heavy/binge drinking patterns during adolescence and early adulthood [21,25] and not because of the potential protective effects of moderate alcohol consumption.
A cross-sectional study showed that low, moderate, and heavy drinkers had significantly lower allostatic load scores, which includes measures of cardiovascular, autonomic, metabolic, neuro-endocrine, and immune systems [26], than lifelong abstainers or former low drinkers [27], and that score is associated with lower risk of CVD and all-cause mortality [28]. However, it is undeniable that chronic heavy and binge drinking is harmful at all levels. In the CV system, it has been extensively associated with increased risk of diabetes, hypertension, ischemic and hemorrhagic stroke, cardiomyopathy, atrial fibrillation, and with increased mortality after an (-but not with increased risk of) AMI [29] probably because of the hypertension provoked by alcohol [14,30]. In addition, irregular heavy drinking (to similar monthly amounts of alcohol consumption as moderate drinkers) is also associated to increased risk of overall CVD because of its negative impact on the lipid profile, arrhythmias, and increased blood pressure [10]. Nevertheless, even in countries with the highest intake of alcohol per capita, chronic heavy and irregular binge drinkers account for the minority of drinkers [31].
Besides the amount of alcohol ingested, the accompaniment may be of importance. When consumed with food or within meals, alcohol intake is associated with lower risk of acute AMI [13]. However, it has been recently reported that when consumed with energy drinks, they can induce an elevated risk of CVD, because energy drinks may influence consumption of higher amounts of alcohol, decrease the perception of intoxication, and induce impaired driving, risky sexual behavior, and alcohol dependence [32], especially in teenagers who are also more prone to binge drinking [33].
3. Acute versus Chronic Alcohol Consumption
The CV (and overall) health effects of drinking are both acute and chronic (accumulative) and are strongly determined by the quantity and pattern of alcohol intake. In turn, the acute response to alcohol may also be determined by drinking habits and alcohol tolerance [14].
Acute and excessive/binge alcohol intake is associated with the development of acute arrhythmias and ventricular function depression [34], although the clinical manifestations of alcohol-induced heart damage are more frequently presented after more than 10 years of alcohol abuse [35]. In fact, the patterns of drinking, more than the total amount consumed, determine CVD risk and, more specifically, the risk of AMI [36]. Along this line, it has been observed that irregular binge drinking (1–2 days per week with a similar total amount of alcohol as moderate drinking) is associated with increased CV risk compared to subjects drinking the same weekly amount on a regular daily basis (moderate consumption) [13].
In a recent meta-analysis, including 23 studies related to alcohol consumption, it was concluded that the risk of major adverse CV events may depend not only on the dosage of alcohol consumed but also on the differences in the time alcohol is consumed, being higher the risk at one hour consumption, event in moderate amounts, and decreasing at 24 h or one week [14]. In the same meta-analysis, the authors observed a U-shaped association between the amount of alcohol consumed and the acute and chronic risk of AMI, with the highest protection with approximately 2 drinks in one day and the highest risk at 9 drinks in a day [14].
4. Sex Differences
As depicted in Table 1, the beneficial amount of alcohol intake is approximately double in men than in women because of sex differences associated with alcohol metabolism and, thus, sex differences in health effects of alcohol consumption. In both men and women, regular moderate alcohol intake is associated with decreased risk of CVD; however, women absorb alcohol differently because of their lower body water content and generally smaller stature [37]. In addition, because of their lower gastric alcohol dehydrogenase activity [38,39] leading to lower alcohol metabolism and clearance [40], they present higher vulnerability to the organ injury effects of acute and chronic alcohol consumption such as alcoholic cardiomyopathy [41]. In fact, women are more sensitive to the adverse effects at a similar level of alcohol consumption [42]. Moreover, it is well documented that CVD differs significantly between men and women at fertile ages in which women are more protected, whereas, at menopause, CVD incidence tends to be similar between women and men [43]. Cardiovascular disease is the main cause of mortality in women ≥65 years old, and, at those ages, CVD kills about 51% women and 42% men, at least in Europe [40]. Therefore, the cardioprotective effects of moderate alcohol consumption will be more visible in older adults who are at increased CV risk.
Some authors have observed sex-specific differences in the association between alcohol intake, heart failure, and non-CV mortality. Women who consumed alcohol in a heavy and moderate manner showed decreased risk of heart failure compared to abstainers [29]. In parallel, other researchers have found that, whereas in men, the frequency of alcohol intake, independently of the amount consumed, was inversely associated with the risk of coronary heart disease, in women, the amount of alcohol but not the frequency was responsible for such an association [44]. In addition, the authors also observed that moderate alcohol consumption reduced the risk of hypertension in women but increased the risk of hypertension in men [44]. In a meta-analysis of the results reported by 14 intervention studies, alcohol consumption was associated with reduced fasting insulin concentrations and improved insulin sensitivity among women only [45]. In this line, a meta-analysis comprising over 2 million individuals supported the assumption that alcohol consumption in women decreased the risk of type 2 diabetes, independently of the amount consumed, compared to life-long and current abstainers, whereas in men, such a protective effect was not observed [46]. Sex-specific differences in the effects of alcohol in atrial fibrillation have been described as well. In men, even moderate alcohol consumption is associated with increased risk of atrial fibrillation, whereas moderate alcohol consumption is not associated to increased risk of atrial fibrillation in women [47,48,49]. However, a prospective study of Swedish men and women did not observe sex differences in this regard [50]. Oppositely, alcohol consumption was positively associated with increased blood pressure only in men in a French cohort [51]. The inverse relationship between moderate alcohol consumption and overall mortality has been shown to be apparent with up to 3 drinks per day in men but only up to 2 drinks per day in women, while the maximum risk reduction was similar in men and women [52], suggesting that women are more exposed than men to death for any cause at moderate to heavy levels of alcohol consumption, probably because of the increased risk of cancer. In fact, it has been shown that women who consume alcohol in moderate amounts have a 10% increased relative risk of overall mortality compared with men [53].
Besides intrinsic sex differences in the metabolism and biological effects of alcohol, patterns of alcohol consumption are different between men and women. Women tend to drink less amounts of alcohol than men [7,54], which, in turn, may be related to the differences in sensitivity to alcohol. Moreover, life-long abstainers and teetotalers are women to a higher extent [7,55,56,57,58], probably because of religious and cultural character traits and social inequalities. In addition, as premenopausal women have a low incidence of CVD, the benefits of alcohol on total mortality may be blunted. This should also be considered when interpreting the relationship between alcohol and health from a global perspective, and also considering that both in epidemiological and clinical trials women have been underrepresented.
5. Ethnic Differences
Unfortunately, the vast majority of epidemiological studies and clinical trials linking alcohol consumption and CVD are performed in caucasic males and females to a lesser extent. Therefore, the results may not be extrapolable to non-White, non-caucasic populations.
Whereas different ethnicities may show different drinking patterns [59] and lifestyle features, the protective effects associated to low/moderate alcohol intake differ substantially among ethnicities and cultures, and also because of genetic differences in alcohol metabolizing enzymes [60]. The lower risk of all-cause mortality has been found only in White and Hispanic [61] but not in Black [62], Indian [3] or Chinese cohorts [63]. These differences have also been observed for the risk of coronary heart disease in which alcohol intake, independently of the amount consumed, was found to be protective for White but not for Black people [64].
Asian populations appear to have increased risk of hypertension and ischemic and hemorrhagic stroke [6] at the same amount of alcohol consumption compared to non-Asian populations [65,66], and, in a Japanese cohort, the cardioprotective effects of moderate alcohol consumption was more apparent in non-obese subjects [67].
Besides the ethnic nuances on the effects of moderate alcohol consumption in CVD, the harmful effects of abusive or heavy alcohol drinking are the same all over the globe [10,68]. In a population-based study of Korean adults, consumption of 5 or more drinks per week was associated with increased CV and non-CV mortality [69], and these findings have been supported by other epidemiologic observations in different areas such as Norway [70] and Australia [71]. However, more research is needed to guarantee the generalizability of these results across cultures and ethnicities.
6. Cardiovascular Disease
The hormetic effects of long-term and regular alcohol consumption in CVD will be briefly discussed below and are summarized in Table 2.
6.1. Intermediate Biomarkers of Cardiovascular Disease
Cardiovascular disease is a life-long, low-grade chronic inflammatory and oxidative disease, initiated by elevated low density lipoprotein (LDL) cholesterol levels and deposition in the intima forming atheromatous plaque. This plaque may eventually rupture, triggering thrombus formation which may occlude the blood vessel leading to a MACE [72]. In this setting, reduced concentrations of intermediate biomarkers of inflammation, oxidation, and coagulation as well as improving the lipid profile may decrease the risk of an eventual MACE.
Moderate alcohol consumption seems to attenuate inflammation by modulating soluble inflammatory markers such as adiponectin [73], soluble intercellular adhesion molecule-1 [74], interleukin 10 [15] or the neutrophil-to-lymphocyte ratio [75], among others [76]. In turn, whereas alcohol is a well-known pro-oxidant agent [77], the modulation of inflammatory and oxidative biomarkers largely depends on the type of beverage consumed [76,78,79], and part of these effects may be mediated by non-alcoholic components of alcoholic beverages as is further discussed. Again, heavy drinking increases the concentration of inflammatory and oxidative parameters [80,81,82] leading to CV morbidity.
Moderate alcohol consumption decreases fibrinogen and fibrin D-dimer [74] and increases tissue plasminogen activator and plasminogen concentrations [73,83,84,85], although no effect has been observed in plasminogen activator inhibitor-1, factor VII, and von Willebrand factor concentrations [74,84]. In healthy young men and, to a lesser extent, women, alcohol consumption has been shown to inhibit platelet reactivity [86,87] without altering platelet count [88]. However, the relationship between heavy alcohol consumption and thrombosis remains blurred because of the controversial results found in different trials [89].
6.2. Classical Cardiovascular Risk Factors
It is widely accepted that alcohol consumption increases high density lipoprotein (HDL) cholesterol levels in a dose-dependent manner [73,83] in both men and women and, more specifically, the HDL2 particle and apoliprotein A-I [90]. However, the effects on LDL and triglycerides have not been completely elucidated [91]. Whereas heavy alcohol consumption is associated with hypercholesterolemia [13], the cardioprotective effect of high plasma concentrations of HDL cholesterol is currently under debate [92,93].
Low/moderate alcohol consumption has been associated with decreased incidence of type 2 diabetes compared to abstainers and heavy drinkers [94], although some studies have observed a linear inverse trend in both men and women in which even heavier drinkers had a lower risk of developing type 2 diabetes than teetotalers [95]. Other authors differ, and evidence this inverse relationship exclusively in non-Asiatic women [46]. Notwithstanding, in patients with type 2 diabetes, a reduction by two or more drinks (including total abstention) per week decreased CVD risk at 10 years by approximately 44% compared with patients who maintained their (moderate) alcohol intake [96].
Heavy alcohol consumption is one of the main reversible causes of hypertension [63]. Excessive alcohol intake is associated with a higher incidence of hypertension [58,83] and isolated diastolic hypertension [97]. In fact, it has been observed that the risk for hypertension increases linearly with alcohol consumption [65,98] with almost no minimum safe dose and even irrespective of the amount consumed [99] in both men and women, although less than 1–2 daily drinks accompanying meals may not be detrimental for blood pressure [63]. However, the alcohol–risk relationship tends to be J-shaped in women and linear in men, although certain ethnic or socioeconomic groups may be more vulnerable to hypertension induced by alcohol consumption [91].
6.3. Major Adverse Cardiovascular Events
In the Prospective Urban and Rural Epidemiological (PURE) study [100], which included countries across a broad range of economic levels, social circumstances and health policies, low alcohol consumers, but not moderate or former alcohol drinkers, showed an approximately 17% decrease in the incidence of CVD [101] (estimated as a composite of cardiovascular death, AMI, stroke, and heart failure) compared to teetotalers, whereas heavy alcohol drinkers showed a subtle increased risk of CVD but a high increase in the risk of death for any cause [100].
In probably the largest cohort study performed in this field, it was shown that abstainers had increased risk of unstable angina, AMI, ischemic stroke, heart failure, peripheral arterial disease, abdominal aortic aneurysm, and unheralded coronary death compared to moderate alcohol drinkers [29]. Moreover, low/moderate alcohol consumption is associated with decreased risk of heart failure [102], whereas heavy and former drinkers showed increased risk of fatal AMI, heart failure, cardiac arrest/sudden coronary death, and transient ischemic attack and ischemic stroke, intracerebral hemorrhage and peripheral arterial disease, and decreased risk of primary AMI and stable angina [29]. In fact, recent analyses have shown that alcohol abuse is associated with a greater risk of emergency department visits, hospitalizations and rehospitalizations for heart failure [103], and all-cause hospitalizations [104]. Whereas heavy alcohol intake is associated with an increased risk of atrial fibrillation [49] but not heart failure [105], some studies have observed an association between low–moderate alcohol intake and the risk of atrial fibrillation [47,48,106], suggesting that not only binge drinkers but also regular drinkers of moderate amounts of alcohol have an increased risk of developing atrial fibrillation. However, another study observed that moderate alcohol consumption was associated with a lower risk of heart failure [102,105] with a less pronounced association in women than in men [107] and not associated with atrial fibrillation.
Moderate alcohol intake is associated with lower levels of high-sensitivity cardiac troponin T (hs-cTnT) and N-terminal pro B-type natriuretic peptide (NT-proBNP), whereas abusive intake is associated with increased levels of these biomarkers of cardiac damage [108]. It is noteworthy that alcohol consumption is also responsible for alcoholic cardiomyopathy (as its name defines it), characterized by a dilation and impairment of the left ventricle which is a considerable risk factor for AMI and sudden death [109]. Although the number of deaths attributed to alcoholic cardiomyopathy may be overestimated, at least for adults aged 65 years or older [110], it has been shown that the estimated total lifetime dose of ethanol correlates inversely with muscular strength and ejection fraction and directly correlates with the left ventricular mass [111].
Alcohol consumption is inversely associated with the risk of AMI [13], even at high doses, although this observation has been shown in high- and middle-income countries [112]. A meta-analysis from 599,912 current drinkers showed an inverse and approximately log-linear association of alcohol consumption with AMI [113], although these inverse associations were possibly more pronounced for non-fatal than for fatal outcomes. Controversially, a large case-control study including 5000 participants in which lifetime alcohol drinking patterns were assessed, teetotalers and occasional (heavy) drinkers were at increased risk of AMI compared to regular drinkers [25,114]. Supporting these findings, moderate alcohol consumption has been shown protective for AMI presentation in comparison with consuming more than 3–4 daily drinks, especially in women [36]. In a large cohort or more than 11 million subjects, which used electronic health record data and were monitored for 6 years, non-drinkers had increased risk of coronary artery disease, whereas no differences were observed in moderate compared to heavy drinkers [29]. Oppositely, moderate drinkers with episodes of heavy or binge drinking presented the same risk of AMI as teetotalers [115].
In a specific region of Poland with the highest prevalence of CVD within the country (26% higher than the average), low–moderate alcohol consumption was related to a smaller risk of coronary disease and stroke [55]. A relatively recent meta-analysis reporting data from 1,425,513 subjects showed that, compared to non-drinkers, low alcohol consumption was associated with a 15% reduced risk of stroke. Moderate alcohol consumption was not associated with the risk of stroke, whereas heavy alcohol intake increased the risk of stroke by approximately 20% [116]. In the same meta-analysis, the authors did not observe any association between alcohol consumption and the risk of hemorrhagic stroke. However, heavy alcohol drinking was associated with increased risk of hemorrhagic stroke compared to abstainers and moderate drinkers [117]. Oppositely, heavy alcohol consumption was associated with a 26%–38% increased risk of hemorrhagic stroke for both men and women [14]. In another study, low intake of alcohol was associated with decreased risk of ischemic stroke or stroke mortality. However, no such associations have been found in moderate or heavy drinkers [116]. Moreover, low–moderate alcohol consumption has been associated with a lower risk of ischemic stroke, whereas high and heavy drinking has been associated with an increased risk [118], although in this meta-analysis, low–moderate and heavy alcohol drinking was not associated with any hemorrhagic stroke subtype, and heavy drinking was associated with increased risk of intracerebral and subarachnoid hemorrhage [118]. Conversely, a meta-analysis from 599,912 current drinkers showed a linear association between alcohol consumption and risk of fatal and non-fatal stroke [113]. Overall, the relationship between alcohol consumption and both hemorrhagic and ischemic stroke remains controversial.
In patients with coronary artery disease, moderate but not heavy alcohol consumption was associated with lower severity of the disease, quantified with the Friesinger score, compared to abstainers [56]. Along this line, heavy alcohol consumption was associated with increased prevalence of coronary artery calcium but not thoracic aortic calcium [119]. In addition, low–moderate alcohol consumption has been associated with a lower incidence of CV and all-cause mortality in patients with established CVD [63,120].
7. Cardiovascular and All-Cause Mortality
A meta-analysis including 1 million people observed that low–moderate alcohol consumption was inversely associated with total mortality in both men and women, while higher doses of alcohol were associated with increased mortality in a J-shaped relationship between alcohol consumption and total mortality [52]. Moreover, recently pooled data from 83 studies showed a positive and curvilinear association of alcohol consumption with all-cause mortality with the lowest risk for those consuming below 100 g per week, and these associations were similar for men and women but weaker at older ages. In addition, there was a J-shaped association for the aggregate of cardiovascular disease outcomes, and these associations were stronger for fatal than non-fatal outcomes. However, this was attributed principally to AMI. In fact, authors described a linear association between alcohol consumption and risk of coronary disease excluding AMI, fatal hypertensive disease, heart failure, and fatal aortic aneurysm. When including both never-drinkers and ex-drinkers, a U-shaped association of alcohol consumption with total CVD and all-cause mortality was reported, and the threshold for lowest risk for all-cause mortality and AMI was about 100 g per week [113]. Controversially, data from the Health Survey for England shows that the protective associations between low alcohol intake and death for any cause may be partially attributable to the reference group that was not adjusted by age and sex which are determinant factors of these associations. In fact, it appears that the associations between low alcohol intake and decreased risk of all-cause mortality are significant only in men 50–64 years and in women ≥65 years compared with never drinkers with a neutral association in other age and sex groups [121]. Supporting these findings, in a meta-analysis, occasional drinkers presented a similar relative risk for all-cause mortality than low alcohol drinkers in several models of adjustment, implying that alcohol consumption, at any amount consumed, would no longer be protective compared to occasional drinkers instead of lifetime teetotalers [112,122].
Low-moderate alcohol consumers showed a 20% and 25% reduced risk for all-cause and CVD mortality, respectively, compared with lifetime abstainers in subjects from the US National Health Interview Surveys, whereas heavy/binge alcohol consumption was associated with increased risk of mortality for all causes and cancer [123]. In this study, only low but not moderate alcohol consumption was associated with a reduced risk of cancer mortality [123]. In the Health Professionals Follow-up Study (HPFS), among AMI survivors, moderate alcohol consumption was associated with lower risk of all-cause and CV mortality, and the relationship between alcohol consumption and with CV and overall mortality responded to a U-shaped association [124]. In a large cohort of more than 11 million subjects, a J-shaped association for fatal and non-fatal CVD and all-cause mortality was observed, with moderate alcohol drinkers in the bottom of the J [29].
Overall, low–moderate usual alcohol intake is associated with lower risk for type 2 diabetes, stroke, heart failure, and all-cause mortality [125,126]. Despite this analysis, it is worth mentioning that excessive alcohol intake is responsible for 4% of total deaths [7,63], including cirrhosis and cancer. The risk of all-cause mortality [114] and of cancers specifically rises with increasing levels of alcohol consumption, and the level of consumption that minimizes health loss has been considered to be zero [9]. In addition, the fact that alcohol consumption has been considered “healthy for the heart” by the scientific community may have produced a justification for alcohol consumption, and consumers who understand alcohol intake as healthy for CVD have been shown to consume 1.5 times more alcohol than those who did not consider alcohol as healthy for CVD [127]. However, while the causal harmful effects of heavy alcohol intake are evident and undeniable [128], moderate alcohol consumption associates with decreased risk of AMI and CV death and even a 13% lower risk of death for any cause [101]. Although Mendelian randomization studies may be challenging these associations [66], some pitfalls must be overcome before achieving definitive conclusions [129]. Therefore, while waiting these conclusions, the benefit-risk balance of alcohol consumption should be considered individually.
8. Type of Alcoholic Beverage Consumed
In general terms, fermented alcoholic beverages are the product of the fermentation of hydrolyzed sugar from cereals (beer) or fruits (wine) to alcohol by the Saccharomyces cerevisiae yeast. Liquors and spirits (distilled alcoholic beverages) are the product of the distillation of beer or wine. Consequently, the molecular composition of fermented (i.e., beer and wine) and distilled beverages (i.e., liquors and spirits) is very different. Fermented beverages contain a significant and declining concentration of bioactive compounds in this order: red wine > white wine > beer, namely, polyphenols [15,130], known to exert antioxidant and anti-inflammatory effects [131], of which the consumption of is associated to decreased incidence of chronic low-grade inflammatory diseases such as CVD [132] or cancer [133]. In addition, fermented beverages contain about 14%, 11%, and 5% of alcohol, for red wine, white wine, and beer, respectively. On the other hand, spirits contain approximately 35% alcohol, whereas liquors contain the same amount of alcohol with different percentages of sugar, both distilled beverages with negligible amounts of bioactive compounds such as polyphenols. Considering the differences in the composition of beer, wine, and liquors/spirits, it is plausible that their consumption elicits differential health effects, liquor and spirits being the worst in terms of bioactive components.
Dissecting the concrete effects of each type of alcoholic beverage has been hampered in epidemiological trials because of the lack of data, the associations with socioeconomic status, beverage quality, and drinking patterns, among other potential confounding factors. Indeed, while some authors have postulated that the differential effects of fermented and distilled alcoholic beverages are the product of lifestyle differences and the pattern of alcohol consumption, several epidemiologic and clinical trials point to another direction.
In a pooled cohort study, moderate wine drinkers had lower relative risk of overall mortality compared to non-drinkers, and moderate wine drinkers also showed lower overall mortality compared to non-wine drinkers [134]. In a three-country cohort, moderate wine consumers showed lower concentrations of intermediate markers of inflammation than beer drinkers [135]. However, subgroup analysis with spirit drinkers was not possible in this study. In women, the risk of stroke was lower in low–moderate wine drinkers compared to never drinkers and compared to low–moderate beer or spirits drinkers [136]. In another cohort, the risk of AMI appears weak in red wine drinkers, intermediate for white wine drinkers, and high for beer and spirits [13]. In this line, a recent meta-analysis has reported that associations of baseline alcohol consumption with all-cause mortality were stronger in drinkers of beer or spirits than of wine, not without warning about the potential for confounding effects [113], as beer and spirits were the predominant types of drinks consumed and, thus, most likely to be heavily/binge consumed, and also because other studies showed no relevant differences according to the type of beverage consumed [50]. In type 2 diabetic patients, moderate wine but not beer or spirit drinkers presented a 22%–23% lower risk of MACE and overall mortality compared to abstainers, with no differences in microvascular complications. However, compared to beer or spirits drinkers, wine drinkers showed no differences in the risk of MACE, although a reduced mortality trend was observed [101].
Besides alcohol, wine, specifically red wine, contains high amounts of polyphenols which have been shown to have metabolic and cardioprotective effects in a non-additive fashion to alcohol by lowering plasma concentrations of pro-oxidant and inflammatory molecules, leukocyte adhesion molecules, and improving homeostasis model assessment of insulin resistance values (HOMA-IR) and blood pressure [15,16,79,137,138]. Although in lower amounts, beer also contains polyphenols and other bioactive compounds [130]. In healthy overweight individuals, moderate alcoholic and non-alcoholic beer consumption increased the antioxidant capacity of HDL [139], and in high CV risk men, the non-alcoholic fraction of beer reduced proinflammatory cellular and soluble biomarkers involved in atherosclerosis progression [140]. A relatively recent international consensus document on the health effects of beer concluded that moderate consumption of fermented beverages (i.e., wine and beer) confer greater cardiovascular protection than spirits because of their non-alcoholic components (mainly polyphenols) [141]. This should be emphasized in the context of a safe and moderate consumption considering the fact that worldwide approximately 45% of alcohol is consumed in the form of spirits, 34% in the form of beer, and only about 12% in the form of wine [7]. However, despite the fact that wine and beer improve the profile of intermediate CV biomarkers, the question whether the risk of MACE is lower for wine and/or beer consumers compared to spirits consumers is still open and difficult to assess because drinkers often do not consume a single type of beverage.
9. Conclusions
The relationship between alcohol consumption and CVD appears in general terms biphasic, being protective at low and moderate amounts and detrimental at high intakes, even when occasionally consumed. Although several authors defend that the harmful effects of alcohol, even at low amounts, outweigh their benefits [142,143], current evidence supports that low amounts of alcohol are safe and beneficial for the CV system.
As per evident ethical and logistical reasons, the main body of evidence relies on epidemiological studies of associative nature which carry several limitations such as the quantification of alcohol consumption. In the future, these studies should include reliable measurements of biological biomarkers of alcohol exposure such as urinary ethyl glucuronide [144] which may better reflect short-term and habitual alcohol consumption than self-reported intake and should also include repeated measures over time.
It is worth mentioning that, despite the cardioprotective effects derived from low/moderate alcohol consumption, these benefits may be weighed against the potential harms from an individual perspective and addressing serious issues such as the propensity to alcohol dependence and collateral social harms, genetic vulnerability, pregnancy or even the family history of cancer. On the other hand, heavy and binge alcohol consumption should be categorically discouraged without any exception or pretext. Along this line, national and international guidelines should be better implemented and updated.
Notwithstanding, alcohol consumption is increasing worldwide and consumed by about half of the population over 15 years of age [7]. As no large randomized trials have been able to be performed at the moment, from a public health perspective, several questions remain open: (1) Which daily amount of alcohol consumption can be considered as safe and truly cardioprotective? (2) Which type of alcoholic beverage is really more beneficial? (3) Do the effects of alcohol vary according to the region and socioeconomic status of the countries and because of genetic and ethnical traits? (4) Are the effects of alcohol consumption specific at different ages? (5) Do sex-specific differences in the pathophysiological effects of alcohol consumption disappear at a certain age? To summarize: to drink or not to drink? This question was launched in 2007 [145] and remains unanswered 13 years after. This is of especial importance considering the fact that the majority of disease endpoints attributable to alcohol consumption are also associated with aging [146], and also considering that the main body of evidence relies in countries with the highest life expectancy. Meanwhile, as alcohol consumption is part of the lifestyle of several cultures, it would be wise to suggest low–moderate alcohol consumption among current drinkers and never recommending drinking in order to improve health outcomes.
Author Contributions
Conceptualization, G.C.-B. and L.B.; writing—original draft preparation, G.C.-B.; writing—review and editing, L.B.; funding acquisition, L.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Spanish Ministry of Economy and Competitiveness of Science (SAF2016-76819-R); the Institute of Health Carlos III (ISCIII) (TERCEL—RD16/0011/0018 and CIBERCV CB16/11/00411); FEDER “Una Manera de Hacer Europa”; and by the Agency for Management of University and Research Grants (2017SGR1480). The APC was funded by SAF2016-76819-R.
Acknowledgments
We thank the Fundació d’Investigació Cardiovascular (FIC)-Fundación Jesús Serra, Barcelona, Spain, for their continuous support.
Conflicts of Interest
The authors declare no conflict of interest. L.B. is member of the Scientific Advisory Board of the Research Forum on Beer and Lifestyle (FICYE). The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- ESC Cardiovascular Realities 2019 by-Flipsnack. Available online: https://www.flipsnack.com/Escardio/esc-cardiovascular-realities-2019/full-view.html (accessed on 21 October 2019).
- Mahmood, S.S.; Levy, D.; Vasan, R.S.; Wang, T.J. The Framingham Heart Study and the epidemiology of cardiovascular disease: A historical perspective. Lancet 2014, 383, 999–1008. [Google Scholar] [CrossRef] [Green Version]
- Yusuf, S.; Hawken, S.; Ôunpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; Mcqueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Ronksley, P.E.; Brien, S.E.; Turner, B.J.; Mukamal, K.J.; Ghali, W.A. Association of alcohol consumption with selected cardiovascular disease outcomes: A systematic review and meta-analysis. BMJ 2011, 342, d671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marmot, M.; Brunner, E. Alcohol and cardiovascular disease. BMJ 1991, 303, 565. Available online: https://www.bmj.com/content/356/bmj.j1340.long (accessed on 6 November 2019). [CrossRef] [Green Version]
- Millwood, I.Y.; Walters, R.G.; Mei, X.W.; Guo, Y.; Yang, L.; Bian, Z.; Bennett, D.A.; Chen, Y.; Dong, C.; Hu, R.; et al. Conventional and genetic evidence on alcohol and vascular disease aetiology: A prospective study of 500 000 men and women in China. Lancet 2019, 393, 1831–1842. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Status Report on Alcohol and Health 2018; WHO: Geneva, Italy, 2018. [Google Scholar]
- Cheng, Y.-C.; Huang, Y.-C.; Huang, W.-L. Heart rate variability as a potential biomarker for alcohol use disorders: A systematic review and meta-analysis. Drug Alcohol Depend. 2019, 204, 107502. [Google Scholar] [CrossRef]
- Griswold, M.G.; Fullman, N.; Hawley, C.; Arian, N.; Zimsen, S.R.; Tymeson, H.D. Alcohol use and burden for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016-ClinicalKey. Lancet 2018, 392, 1015–1035. Available online: https://www.clinicalkey.es/#!/content/playContent/1-s2.0-S0140673618313102?returnurl=https:%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS0140673618313102%3Fshowall%3Dtrue&referrer=https:%2F%2Fwww.ncbi.nlm.nih.gov%2F (accessed on 22 October 2019). [CrossRef] [Green Version]
- Rehm, J.; Gmel, G.E.; Gmel, G.; Hasan, O.S.M.; Imtiaz, S.; Popova, S.; Probst, C.; Roerecke, M.; Room, R.; Samokhvalov, A.V.; et al. The relationship between different dimensions of alcohol use and the burden of disease—An update. Addiction 2017, 112, 968–1001. [Google Scholar] [CrossRef] [Green Version]
- 2015–2020 Dietary Guidelines for Americans; United States. Available online: https://health.gov/dietaryguidelines/2015/resources/2015-2020_Dietary_Guidelines.pdf (accessed on 10 October 2019).
- Kalinowski, A.; Humphreys, K. Governmental standard drink definitions and low-risk alcohol consumption guidelines in 37 countries. Addiction 2016, 111, 1293–1298. [Google Scholar] [CrossRef] [Green Version]
- Mukamal, K.J.; Conigrave, K.M.; Mittleman, M.A.; Camargo, C.A.; Stampfer, M.J.; Willett, W.C.; Rimm, E.B. Roles of drinking pattern and type of alcohol consumed in coronary heart disease in men. N. Engl. J. Med. 2003, 348, 109–118. [Google Scholar] [CrossRef]
- Mostofsky, E.; Chahal, H.S.; Mukamal, K.J.; Rimm, E.B.; Mittleman, M.A. Alcohol and immediate risk of cardiovascular events. Circulation 2016, 133, 979–987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiva-Blanch, G.; Urpi-Sarda, M.; Llorach, R.; Rotches-Ribalta, M.; Guilleń, M.; Casas, R.; Arranz, S.; Valderas-Martinez, P.; Portoles, O.; Corella, D.; et al. Differential effects of polyphenols and alcohol of red wine on the expression of adhesion molecules and inflammatory cytokines related to atherosclerosis: A randomized clinical trial. Am. J. Clin. Nutr. 2012, 95, 326–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiva-Blanch, G.; Urpi-Sarda, M.; Ros, E.; Arranz, S.; Valderas-Martínez, P.; Casas, R.; Sacanella, E.; Llorach, R.; Lamuela-Raventos, R.M.; Andres-Lacueva, C.; et al. Dealcoholized red wine decreases systolic and diastolic blood pressure and increases plasma nitric oxide: Short communication. Circ. Res. 2012, 111, 1065–1068. [Google Scholar] [CrossRef] [Green Version]
- Drinking Levels Defined; National Institute on Alcohol Abuse and Alcoholism (NIAAA): Bethesda, MD, USA, 2019. Available online: https://www.niaaa.nih.gov/alcohol-health/overview-alcohol-consumption/moderate-binge-drinking (accessed on 6 November 2019).
- Jackson, R.; Broad, J.; Connor, J.; Wells, S. Alcohol and ischaemic heart disease: Probably no free lunch. Lancet 2005, 366, 1911–1912. [Google Scholar] [CrossRef]
- Tsubono, Y.; Yamada, S.; Nishino, Y.; Tsuji, I.; Hisamichi, S. Choice of comparison group in assessing the health effects of moderate alcohol consumption. Jama 2001, 286, 1177–1178. [Google Scholar] [CrossRef]
- Fillmore, K.M.; Stockwell, T.; Chikritzhs, T.; Bostrom, A.; Kerr, W. Moderate Alcohol Use and Reduced Mortality Risk: Systematic Error in Prospective Studies and New Hypotheses-ClinicalKey. Ann. Epidemiol. 2007, 17, S16–S23. Available online: https://www.clinicalkey.es/#!/content/playContent/1-s2.0-S1047279707000075?returnurl=https:%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS1047279707000075%3Fshowall%3Dtrue&referrer=https:%2F%2Fwww.ncbi.nlm.nih.gov%2F (accessed on 22 October 2019). [CrossRef]
- Britton, A.; Ben-Shlomo, Y.; Benzeval, M.; Kuh, D.; Bell, S. Life course trajectories of alcohol consumption in the United Kingdom using longitudinal data from nine cohort studies. BMC Med. 2015, 13, 47. [Google Scholar] [CrossRef] [Green Version]
- Hwang, C.-L.; Piano, M.R.; Thur, L.A.; Peters, T.A.; da Silva, A.L.G.; Phillips, S.A. The effects of repeated binge drinking on arterial stiffness and urinary norepinephrine levels in young adults. J. Hypertens. 2020, 38, 111–117. [Google Scholar] [CrossRef]
- Charakida, M.; Georgiopoulos, G.; Dangardt, F.; Chiesa, S.T.; Hughes, A.D.; Rapala, A.; Davey Smith, G.; Lawlor, D.; Finer, N.; Deanfield, J.E. Early vascular damage from smoking and alcohol in teenage years: The ALSPAC study. Eur. Heart J. 2019, 40, 345–353. [Google Scholar] [CrossRef] [Green Version]
- Roerecke, M.; Rehm, J. Irregular heavy drinking occasions and risk of ischemic heart disease: A systematic review and meta-analysis. Am. J. Epidemiol. 2010, 171, 633–644. [Google Scholar] [CrossRef] [Green Version]
- Russell, M.; Fan, A.Z.; Freudenheim, J.L.; Dorn, J.; Trevisan, M. Lifetime drinking trajectories and nonfatal acute myocardial infarction. Alcohol. Clin. Exp. Res. 2019, 43, 2384–2394. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S. Protective and damaging effects of stress mediators. N. Engl. J. Med. 1998, 338, 171–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldwater, D.; Karlamangla, A.; Merkin, S.S.; Seeman, T. Compared to non-drinkers, individuals who drink alcohol have a more favorable multisystem physiologic risk score as measured by allostatic load. PLoS ONE 2019, 14, e0223168. [Google Scholar] [CrossRef] [PubMed]
- Karlamangla, A.S.; Singer, B.H.; Seeman, T.E. Reduction in allostatic load in older adults is associated with lower all-cause mortality risk: MacArthur studies of successful aging. Psychosom. Med. 2006, 68, 500–507. [Google Scholar] [CrossRef]
- Bell, S.; Daskalopoulou, M.; Rapsomaniki, E.; George, J.; Britton, A.; Bobak, M.; Casas, J.P.; Dale, C.E.; Denaxas, S.; Shah, A.D.; et al. Association between clinically recorded alcohol consumption and initial presentation of 12 cardiovascular diseases: Population based cohort study using linked health records. BMJ 2017, 356, j909. [Google Scholar] [CrossRef] [Green Version]
- Puddey, I.B.; Mori, T.A.; Barden, A.E.; Beilin, L.J. Alcohol and hypertension—New insights and lingering controversies. Curr. Hypertens. Rep. 2019, 21, 79. [Google Scholar] [CrossRef]
- Rehm, J.; Roerecke, M. Cardiovascular effects of alcohol consumption. Trends Cardiovasc. Med. 2017, 27, 534–538. [Google Scholar] [CrossRef]
- Lévy, S.; Santini, L.; Capucci, A.; Oto, A.; Santomauro, M.; Riganti, C.; Raviele, A.; Cappato, R. European Cardiac Arrhythmia Society Statement on the cardiovascular events associated with the use or abuse of energy drinks. J. Interv. Card. Electrophysiol. 2019, 56, 99–115. [Google Scholar] [CrossRef]
- Matshipi, M.; Monyeki, K.D.; Mafumo, N.; Monyeki, S.M.; Siweya, H.J.; Kemper, H.C.G. The use of alcohol and knowledge of cardiovascular diseases among ellisras rural children aged 14–22 years: Ellisras longitudinal study. Int. J. Environ. Res. Public Health 2019, 16, 2650. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Solà, J. Cardiovascular risks and benefits of moderate and heavy alcohol consumption. Nat. Rev. Cardiol. 2015, 12, 576–587. [Google Scholar] [CrossRef]
- Guzzo-Merello, G. Alcoholic cardiomyopathy. World J. Cardiol. 2014, 6, 771. [Google Scholar] [CrossRef]
- Russell, M.; Chu, B.C.; Banerjee, A.; Fan, A.Z.; Trevisan, M.; Dorn, J.M.; Gruenewald, P. Drinking patterns and myocardial infarction: A linear dose-response model. Alcohol. Clin. Exp. Res. 2009, 33, 324–331. [Google Scholar] [CrossRef] [Green Version]
- Vatsalya, V.; Liaquat, H.B.; Ghosh, K.; Mokshagundam, S.P.; McClain, C.J. A review on the sex differences in organ and system pathology with alcohol drinking. Curr. Drug Abuse Rev. 2016, 9, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Ely, M. Gender differences in the relationship between alcohol consumption and drink problems are largely accounted for by body water. Alcohol Alcohol. 1999, 34, 894–902. [Google Scholar] [CrossRef]
- Thomasson, H.R. Gender differences in alcohol metabolism. In Recent Developments in Alcoholism; Springer: Boston, MA, USA, 2002; pp. 163–179. [Google Scholar]
- Tamargo, J.; Rosano, G.; Walther, T.; Duarte, J.; Niessner, A.; Kaski, J.C.; Ceconi, C.; Drexel, H.; Kjeldsen, K.; Savarese, G.; et al. Gender differences in the effects of cardiovascular drugs. Eur. Hear. J.-Cardiovasc. Pharmacother. 2017, 3, 163–182. [Google Scholar] [CrossRef] [Green Version]
- Urbano-Márquez, A. The greater risk of alcoholic cardiomyopathy and myopathy in women compared with men. JAMA J. Am. Med. Assoc. 1995, 274, 149. [Google Scholar] [CrossRef]
- El-Mas, M.M.; Abdel-Rahman, A.A. Role of alcohol oxidative metabolism in its cardiovascular and autonomic effects. In Aldehyde Dehydrogenases; Springer: Singapore, 2019; pp. 1–33. [Google Scholar]
- Colditz, G.A.; Willett, W.C.; Stampfer, M.J.; Rosner, B.; Speizer, F.E.; Hennekens, C.H. Menopause and the risk of coronary heart disease in women. N. Engl. J. Med. 1987, 316, 1105–1110. [Google Scholar] [CrossRef]
- Tolstrup, J.; Jensen, M.K.; Tjønneland, A.; Overvad, K.; Mukamal, K.J.; Grønbæk, M. Prospective study of alcohol drinking patterns and coronary heart disease in women and men. Br. Med. J. 2006, 332, 1244–1247. [Google Scholar] [CrossRef] [Green Version]
- Schrieks, I.C.; Heil, A.L.J.; Hendriks, H.F.J.; Mukamal, K.J.; Beulens, J.W.J. The Effect of alcohol consumption on insulin sensitivity and glycemic status: A systematic review and meta-analysis of intervention studies. Diabetes Care 2015, 38, 723–732. [Google Scholar]
- Knott, C.; Bell, S.; Britton, A. Alcohol consumption and the risk of type 2 diabetes: A systematic review and Dose-Response Meta-analysis of more than 1.9 million individuals from 38 observational studies. Diabetes Care 2015, 38, 1804–1812. [Google Scholar] [CrossRef] [Green Version]
- Liang, Y.; Mente, A.; Yusuf, S.; Gao, P.; Sleight, P.; Zhu, J.; Fagard, R.; Lonn, E.; Teo, K.K. Alcohol consumption and the risk of incident atrial fibrillation among people with cardiovascular disease. CMAJ 2012, 184, E857–E866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conen, D.; Tedrow, U.B.; Cook, N.R.; Moorthy, M.V.; Buring, J.E.; Albert, C.M. Alcohol consumption and risk of incident atrial fibrillation in women. JAMA-J. Am. Med. Assoc. 2008, 300, 2489–2496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frost, L.; Vestergaard, P. Alcohol and risk of atrial fibrillation or flutter: a cohort study. Arch. Intern. Med. 2004, 164, 1993–1998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsson, S.C.; Drca, N.; Wolk, A. Alcohol consumption and risk of atrial fibrillation: A prospective study and dose-response meta-analysis. J. Am. Coll. Cardiol. 2014, 64, 281–289. [Google Scholar] [CrossRef]
- Vallée, A.; Gabet, A.; Deschamps, V.; Blacher, J.; Olié, V. Relationship between nutrition and alcohol consumption with blood pressure: The ESTEBAN survey. Nutrients 2019, 11, 1433. [Google Scholar] [CrossRef] [Green Version]
- Di Castelnuovo, A.; Costanzo, S.; Bagnardi, V.; Donati, M.B.; Iacoviello, L.; De Gaetano, G. Alcohol dosing and total mortality in men and women: An updated meta-analysis of 34 prospective studies. Arch. Intern. Med. 2006, 166, 2437–2445. [Google Scholar] [CrossRef]
- Zheng, Y.-L.; Lian, F.; Shi, Q.; Zhang, C.; Chen, Y.-W.; Zhou, Y.-H.; He, J. Alcohol intake and associated risk of major cardiovascular outcomes in women compared with men: A systematic review and meta-analysis of prospective observational studies. BMC Public Health 2015, 15, 773. [Google Scholar] [CrossRef] [Green Version]
- Cheung, J.W.; Cheng, E.P.; Wu, X.; Yeo, I.; Christos, P.J.; Kamel, H.; Markowitz, S.M.; Liu, C.F.; Thomas, G.; Ip, J.E.; et al. Sex-based differences in outcomes, 30-day readmissions, and costs following catheter ablation of atrial fibrillation: The United States Nationwide Readmissions Database 2010–14. Eur. Heart J. 2019, 40, 3035–3043. [Google Scholar]
- Suliga, E.; Kozieł, D.; Ciesla, E.; Rebak, D.; Głuszek-Osuch, M.; Naszydłowska, E.; Głuszek, S. The consumption of alcoholic beverages and the prevalence of cardiovascular diseases in men and women: A cross-sectional study. Nutrients 2019, 11, 1318. [Google Scholar] [CrossRef] [Green Version]
- Chaga, P.; Mazocco, L.; Piccoli, J.D.C.E.; Ardenghi, T.M.; Badimon, L.; Caramori, P.R.A.; Pellanda, L.; Gomes, I.; Schwanke, C.H.A. Association of alcohol consumption with coronary artery disease severity-ClinicalKey. Clin. Nutr. 2017, 36, 1036–1039. Available online: https://www.clinicalkey.es/#!/content/playContent/1-s2.0-S0261561416301510?returnurl=https:%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS0261561416301510%3Fshowall%3Dtrue&referrer=https:%2F%2Fwww.ncbi.nlm.nih.gov%2F (accessed on 29 October 2019). [CrossRef]
- Nansseu, J.R.; Kameni, B.S.; Assah, F.K.; Bigna, J.J.; Petnga, S.-J.; Tounouga, D.N.; Tchokfe Ndoula, S.; Noubiap, J.J.; Kamgno, J. Prevalence of major cardiovascular disease risk factors among a group of sub-Saharan African young adults: a population-based cross-sectional study in Yaoundé, Cameroon. BMJ Open 2019, 9, e029858. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.P.; Xu, L.W.; Sun, T.; Wu, Y.Y.; Zhu, X.W.; Zhang, B.; Cheng, Z.; Cai, X.; Liu, Y.C.; Zhao, T.T.; et al. Relationship between alcohol use, blood pressure and hypertension: An association study and a Mendelian randomisation study. J. Epidemiol. Community Health 2019, 73, 796–801. [Google Scholar] [CrossRef] [PubMed]
- Mulia, N.; Karriker-Jaffe, K.J.; Witbrodt, J.; Bond, J.; Williams, E.; Zemore, S.E. Racial/ethnic differences in 30-year trajectories of heavy drinking in a nationally representative U.S. sample. Drug Alcohol Depend. 2017, 170, 133–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hui, P.; Nakayama, T.; Morita, A.; Sato, N.; Hishiki, M.; Saito, K.; Yoshikawa, Y.; Tamura, M.; Sato, I.; Takahashi, T.; et al. Common single nucleotide polymorphisms in Japanese patients with essential hypertension: aldehyde dehydrogenase 2 gene as a risk factor independent of alcohol consumption. Hypertens. Res. 2007, 30, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Kerr, W.C.; Greenfield, T.K.; Bond, J.; Ye, Y.; Rehm, J. Racial and ethnic differences in all-cause mortality risk according to alcohol consumption patterns in the national alcohol surveys. Am. J. Epidemiol. 2011, 174, 769–778. [Google Scholar] [CrossRef] [Green Version]
- Sempos, C.T.; Rehm, J.; Wu, T.; Crespo, C.J.; Trevisan, M. Average volume of alcohol consumption and all-cause mortality in African Americans: The NHEFS cohort. Alcohol. Clin. Exp. Res. 2003, 27, 88–92. [Google Scholar] [CrossRef]
- O’Keefe, E.L.; DiNicolantonio, J.J.; O’Keefe, J.H.; Lavie, C.J. Alcohol and cv health: Jekyll and Hyde J-Curves. Prog. Cardiovasc. Dis. 2018, 61, 68–75. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, F.D.; Chambless, L.E.; Folsom, A.R.; Eigenbrodt, M.L.; Duncan, B.B.; Gilbert, A.; Szklo, M. Association between alcoholic beverage consumption and incidence of coronary heart disease in Whites and Blacks: The Atherosclerosis Risk in Communities Study. Am. J. Epidemiol. 2004, 160, 466–474. [Google Scholar] [CrossRef]
- Taylor, B.; Irving, H.M.; Baliunas, D.; Roerecke, M.; Patra, J.; Mohapatra, S.; Rehm, J. Alcohol and hypertension: Gender differences in dose-response relationships determined through systematic review and meta-analysis: REVIEW. Addiction 2009, 104, 1981–1990. [Google Scholar] [CrossRef]
- Holmes, M.V.; Dale, C.E.; Zuccolo, L.; Silverwood, R.J.; Guo, Y.; Ye, Z.; Prieto-Merino, D.; Dehghan, A.; Trompet, S.; Wong, A.; et al. Association between alcohol and cardiovascular disease: Mendelian randomisation analysis based on individual participant data. BMJ 2014, 349, g4164. [Google Scholar] [CrossRef] [Green Version]
- Makita, S.; Onoda, T.; Ohsawa, M.; Tanaka, F.; Segawa, T.; Takahashi, T.; Satoh, K.; Itai, K.; Tanno, K.; Sakata, K.; et al. Influence of mild-to-moderate alcohol consumption on cardiovascular diseases in men from the general population-ClinicalKey. Atherosclerosis 2012, 224, 222–227. Available online: https://www.clinicalkey.es/#!/content/playContent/1-s2.0-S0021915012004492?returnurl=https:%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS0021915012004492%3Fshowall%3Dtrue&referrer=https:%2F%2Fwww.ncbi.nlm.nih.gov%2F (accessed on 13 November 2019).
- Leong, D.P.; Smyth, A.; Teo, K.K.; McKee, M.; Rangarajan, S.; Pais, P.; Liu, L.; Anand, S.S.; Yusuf, S. INTERHEART Investigators Patterns of alcohol consumption and myocardial infarction risk: observations from 52 countries in the INTERHEART case-control study. Circulation 2014, 130, 390–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, I.; Kim, S.; Kang, H. Lifestyle Risk Factors and All-Cause and Cardiovascular Disease Mortality: Data from the Korean Longitudinal Study of Aging. Int. J. Environ. Res. Public Health 2019, 16, 3040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krokstad, S.; Ding, D.; Grunseit, A.C.; Sund, E.R.; Holmen, T.L.; Rangul, V.; Bauman, A. Multiple lifestyle behaviours and mortality, findings from a large population-based Norwegian cohort study-The HUNT Study. BMC Public Health 2017, 17, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, D.; Rogers, K.; van der Ploeg, H.; Stamatakis, E.; Bauman, A.E. Traditional and emerging lifestyle risk behaviors and all-cause mortality in middle-aged and older adults: Evidence from a large population-based Australian cohort. PLoS Med. 2015, 12, e1001917. [Google Scholar] [CrossRef] [PubMed]
- Badimon, L.; Suades, R.; Vilella-Figuerola, A.; Crespo, J.; Vilahur, G.; Escate, R.; Padro, T.; Chiva-Blanch, G. Liquid Biopsies: microvesicles in cardiovascular disease. Antioxid. Redox Signal. 2019, in press. [Google Scholar] [CrossRef] [PubMed]
- Brien, S.E.; Ronksley, P.E.; Turner, B.J.; Mukamal, K.J.; Ghali, W.A. Effect of alcohol consumption on biological markers associated with risk of coronary heart disease: Systematic review and meta-analysis of interventional studies. BMJ 2011, 342, 480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stote, K.S.; Tracy, R.P.; Taylor, P.R.; Baer, D.J. The effect of moderate alcohol consumption on biomarkers of inflammation and hemostatic factors in postmenopausal women. Eur. J. Clin. Nutr. 2016, 70, 470–474. [Google Scholar] [CrossRef]
- Howard, R.; Scheiner, A.; Kanetsky, P.A.; Egan, K.M. Sociodemographic and lifestyle factors associated with the neutrophil-to-lymphocyte ratio. Ann. Epidemiol. 2019, 38, 11–21. [Google Scholar] [CrossRef]
- Chiva-Blanch, G.; Arranz, S.; Lamuela-Raventos, R.M.; Estruch, R. Effects of wine, alcohol and polyphenols on cardiovascular disease risk factors: Evidences from human studies. Alcohol Alcohol. 2013, 48, 270–277. [Google Scholar] [CrossRef] [Green Version]
- Wu, D.; Cederbaum, A.I. Alcohol, oxidative stress, and free radical damage. Alcohol Res. Health 2003, 27, 277–284. [Google Scholar]
- Nova, E.; San Mauro-Martín, I.; Díaz-Prieto, L.E.; Marcos, A. Wine and beer within a moderate alcohol intake is associated with higher levels of HDL-c and adiponectin. Nutr. Res. 2019, 63, 42–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estruch, R.; Sacanella, E.; Mota, F.; Chiva-Blanch, G.; Antúnez, E.; Casals, E.; Deulofeu, R.; Rotilio, D.; Andres-Lacueva, C.; Lamuela-Raventos, R.M.; et al. Moderate consumption of red wine, but not gin, decreases erythrocyte superoxide dismutase activity: A randomised cross-over trial. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 46–53. [Google Scholar] [CrossRef] [PubMed]
- So-Armah, K.A.; Cheng, D.M.; Freiberg, M.S.; Gnatienko, N.; Patts, G.; Ma, Y.; White, L.; Blokhina, E.; Lioznov, D.; Doyle, M.F.; et al. Association between alcohol use and inflammatory biomarkers over time among younger adults with HIV—The Russia ARCH Observational Study. PLoS ONE 2019, 14, e0219710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjørkhaug, S.T.; Neupane, S.P.; Bramness, J.G.; Aanes, H.; Skar, V.; Medhus, A.W.; Valeur, J. Plasma cytokine levels in patients with chronic alcohol overconsumption: relations to gut microbiota markers and clinical correlates. Alcohol 2019, in press. [Google Scholar]
- Kuprys, P.V.; Tsukamoto, H.; Gao, B.; Jia, L.; McGowan, J.; Coopersmith, C.M.; Moreno, M.C.; Hulsebus, H.; Meena, A.S.; Souza-Smith, F.M.; et al. Summary of the 2018 alcohol and immunology research interest group (AIRIG) meeting-ClinicalKey. Alcohol 2019, 77, 11–18. Available online: https://www.clinicalkey.es/#!/content/playContent/1-s2.0-S0741832918302076?scrollTo=%23hl0000358 (accessed on 19 November 2019). [CrossRef] [Green Version]
- Lawlor, D.A.; Nordestgaard, B.G.; Benn, M.; Zuccolo, L.; Tybjaerg-Hansen, A.; Davey Smith, G. Exploring causal associations between alcohol and coronary heart disease risk factors: findings from a Mendelian randomization study in the Copenhagen General Population Study. Eur. Heart J. 2013, 34, 2519–2528. [Google Scholar] [CrossRef] [Green Version]
- Rimm, E.B.; Williams, P.; Fosher, K.; Criqui, M.; Stampfer, M.J. Moderate alcohol intake and lower risk of coronary heart disease: Meta-analysis of effects on lipids and haemostatic factors. Br. Med. J. 1999, 319, 1523–1528. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M.; Vaughan, D.E.; Stampfer, M.J.; Glynn, R.J.; Hennekens, C.H. Association of moderate alcohol consumption and plasma concentration of endogenous tissue-type plasminogen activator. JAMA J. Am. Med. Assoc. 1994, 272, 929–933. [Google Scholar] [CrossRef]
- Smith, S.; Fair, K.; Goodman, A.; Watson, J.; Dodgion, C.; Schreiber, M. Consumption of alcohol leads to platelet inhibition in men. Am. J. Surg. 2019, 217, 868–872. [Google Scholar] [CrossRef]
- Mukamal, K.J.; Massaro, J.M.; Ault, K.A.; Mittleman, M.A.; Sutherland, P.A.; Lipinska, I.; Levy, D.; D’Agostino, R.B.; Tofler, G.H. Alcohol consumption and platelet activation and aggregation among women and men: The Framingham Offspring Study. Alcohol. Clin. Exp. Res. 2005, 29, 1906–1912. [Google Scholar] [CrossRef]
- Wakabayashi, I. Platelet count in men with a habit of alcohol drinking. Platelets 2019, 1–3, in press. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Mattiuzzi, C.; Franchini, M. Alcohol consumption and venous thromboembolism: friend or foe? Intern. Emerg. Med. 2015, 10, 907–913. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, E.; Silva, E.R.; Foster, D.; McGee Harper, M.; Seidman, C.E.; Smith, J.D.; Breslow, J.L.; Brinton, E.A. Alcohol consumption raises HDL cholesterol levels by increasing the transport rate of apolipoproteins A-I and A-II. Circulation 2000, 102, 2347–2352. [Google Scholar] [CrossRef] [PubMed]
- Piano, M.R. Alcohol’s effects on the cardiovascular system. Alcohol Res. 2017, 38, 219–241. [Google Scholar]
- Voight, B.F.; Peloso, G.M.; Orho-Melander, M.; Frikke-Schmidt, R.; Barbalic, M.; Jensen, M.K.; Hindy, G.; Hólm, H.; Ding, E.L.; Johnson, T.; et al. Plasma HDL cholesterol and risk of myocardial infarction: A mendelian randomisation study. Lancet 2012, 380, 572–580. [Google Scholar] [CrossRef] [Green Version]
- Ben-Aicha, S.; Escate, R.; Casaní, L.; Padró, T.; Peña, E.; Arderiu, G.; Mendieta, G.; Badimón, L.; Vilahur, G. High-density lipoprotein remodelled in hypercholesterolaemic blood induce epigenetically driven down-regulation of endothelial HIF-1α expression in a preclinical animal model. Cardiovasc. Res. 2019, in press. [Google Scholar] [CrossRef] [Green Version]
- Li, X.H.; Yu, F.F.; Zhou, Y.H.; He, J. Association between alcohol consumption and the risk of incident type 2 diabetes: A systematic review and dose-response meta-analysis1. Am. J. Clin. Nutr. 2016, 103, 818–829. [Google Scholar] [CrossRef] [Green Version]
- Joosten, M.M.; Grobbee, D.E.; Van Der A, D.L.; Verschuren, W.M.M.; Hendriks, H.F.J.; Beulens, J.W.J. Combined effect of alcohol consumption and lifestyle behaviors on risk of type 2 diabetes. Am. J. Clin. Nutr. 2010, 91, 1777–1783. [Google Scholar] [CrossRef]
- Strelitz, J.; Ahern, A.L.; Long, G.H.; Boothby, C.E.; Wareham, N.J.; Griffin, S.J. Changes in behaviors after diagnosis of type 2 diabetes and 10-year incidence of cardiovascular disease and mortality. Cardiovasc. Diabetol. 2019, 18, 98. [Google Scholar] [CrossRef] [Green Version]
- Mahajan, S.; Zhang, D.; He, S.; Lu, Y.; Gupta, A.; Spatz, E.S.; Lu, J.; Huang, C.; Herrin, J.; Liu, S.; et al. Prevalence, Awareness, and Treatment of Isolated Diastolic Hypertension: Insights from the China PEACE Million Persons Project. J. Am. Heart Assoc. 2019, 8, e012954. [Google Scholar] [CrossRef] [Green Version]
- Briasoulis, A.; Agarwal, V.; Messerli, F.H. Alcohol consumption and the risk of hypertension in men and women: A systematic review and meta-analysis. J. Clin. Hypertens. 2012, 14, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Xing, L.; Jing, L.; Tian, Y.; Lin, M.; Du, Z.; Yan, H.; Ren, G.; Dong, Y.; Sun, Q.; Liu, S. Urban-Rural disparities in status of hypertension in northeast China: A population-based study, 2017–2019. Clin. Epidemiol. 2019, 11, 801–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yusuf, S.; Joseph, P.; Rangarajan, S.; Islam, S.; Mente, A.; Hystad, P.; Brauer, M.; Kutty, V.R.; Gupta, R.; Wielgosz, A.; et al. Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): A prospective cohort study. Lancet 2019, in press. [Google Scholar]
- Blomster, J.I.; Zoungas, S.; Chalmers, J.; Li, Q.; Chow, C.K.; Woodward, M.; Mancia, G.; Poulter, N.; Williams, B.; Harrap, S.; et al. The relationship between alcohol consumption and vascular complications and mortality in individuals with type 2 diabetes. Diabetes Care 2014, 37, 1353–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Castelnuovo, A.; Costanzo, S.; Bonaccio, M.; Rago, L.; De Curtis, A.; Persichillo, M.; Bracone, F.; Olivieri, M.; Cerletti, C.; Donati, M.B.; et al. Moderate alcohol consumption is associated with lower risk for heart failure but not atrial fibrillation. JACC Heart Fail. 2017, 5, 837–844. [Google Scholar] [CrossRef]
- Nishimura, M.; Bhatia, H.; Ma, J.; Dickson, S.D.; Alshawabkeh, L.; Adler, E.; Maisel, A.; Criqui, M.H.; Greenberg, B.; Thomas, I.C. The impact of substance abuse on heart failure hospitalizations-Clinicalkey. Am. J. Med. 2019, in press. [Google Scholar] [CrossRef]
- Costanzo, S.; Mukamal, K.J.; Di Castelnuovo, A.; Bonaccio, M.; Olivieri, M.; Persichillo, M.; De Curtis, A.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; et al. Alcohol consumption and hospitalization burden in an adult Italian population: prospective results from the Moli-sani study. Addiction 2019, 114, 636–650. [Google Scholar] [CrossRef]
- Larsson, S.C.; Orsini, N.; Wolk, A. Alcohol consumption and risk of heart failure: A dose-response meta-analysis of prospective studies. Eur. J. Heart Fail. 2015, 17, 367–373. [Google Scholar] [CrossRef] [Green Version]
- Amabile, N.; Cheng, S.; Renard, J.M.; Larson, M.G.; Ghorbani, A.; McCabe, E.; Griffin, G.; Guerin, C.; Ho, J.E.; Shaw, S.Y.; et al. Association of circulating endothelial microparticles with cardiometabolic risk factors in the Framingham Heart Study. Eur. Heart J. 2014, 35, 2972–2979. [Google Scholar] [CrossRef]
- Goncalves, A.; Claggett, B.; Jhund, P.S.; Rosamond, W.; Deswal, A.; Aguilar, D.; Shah, A.M.; Cheng, S.; Solomon, S.D. Alcohol consumption and risk of heart failure: The Atherosclerosis Risk in Communities Study. Eur. Heart J. 2015, 36, 939–945. [Google Scholar] [CrossRef] [Green Version]
- Lazo, M.; Chen, Y.; McEvoy, J.W.; Ndumele, C.; Konety, S.; Ballantyne, C.M.; Sharrett, A.R.; Selvin, E. Alcohol consumption and cardiac biomarkers: The atherosclerosis risk in communities (ARIC) study. Clin. Chem. 2016, 62, 1202–1210. [Google Scholar] [CrossRef] [Green Version]
- Weintraub, R.G.; Semsarian, C.; Macdonald, P. Dilated cardiomyopathy. Lancet 2017, 390, 400–414. [Google Scholar] [CrossRef]
- Manthey, J.; Rehm, J. Mortality from alcoholic cardiomyopathy: Exploring the gap between estimated and civil registry data. J. Clin. Med. 2019, 8, 1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urbano-Marquez, A.; Estruch, R.; Navarro-Lopez, F.; Grau, J.M.; Mont, L.; Rubin, E. The effects of alcoholism on skeletal and cardiac muscle. N. Engl. J. Med. 1989, 320, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Smyth, A.; Teo, K.K.; Rangarajan, S.; O’Donnell, M.; Zhang, X.; Rana, P.; Leong, D.P.; Dagenais, G.; Seron, P.; Rosengren, A.; et al. Alcohol consumption and cardiovascular disease, cancer, injury, admission to hospital, and mortality: A prospective cohort study. Lancet 2015, 386, 1945–1954. [Google Scholar] [CrossRef]
- Wood, A.M.; Kaptoge, S.; Butterworth, A.; Willeit, P.; Warnakula, S.; Bolton, T.; Paige, E.; Paul, D.S.; Sweeting, M.; Burgess, S.; et al. Risk thresholds for alcohol consumption: combined analysis of individual-participant data for 599 912 current drinkers in 83 prospective studies. Lancet 2018, 391, 1513–1523. [Google Scholar] [CrossRef] [Green Version]
- Naimi, T.S.; Stadtmueller, L.A.; Chikritzhs, T.; Stockwell, T.; Zhao, J.; Britton, A.; Saitz, R.; Sherk, A. Alcohol, age, and mortality: Estimating selection bias due to premature death. J. Stud. Alcohol Drugs 2019, 80, 63–68. [Google Scholar] [CrossRef]
- Roerecke, M.; Rehm, J. Alcohol consumption, drinking patterns, and ischemic heart disease: A narrative review of meta-analyses and a systematic review and meta-analysis of the impact of heavy drinking occasions on risk for moderate drinkers. BMC Med. 2014, 12, 182. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Qin, Y.-Y.; Chen, Q.; Jiang, H.; Chen, X.-Z.; Xu, C.-L.; Mao, P.-J.; He, J.; Zhou, Y.-H. Alcohol intake and risk of stroke: a dose-response meta-analysis of prospective studies. Int. J. Cardiol. 2014, 174, 669–677. [Google Scholar] [CrossRef]
- Costa, P.; Grassi, M.; Iacoviello, L.; Zedde, M.; Marcheselli, S.; Silvestrelli, G.; DeLodovici, M.L.; Sessa, M.; Zini, A.; Paciaroni, M.; et al. Alcohol intake and the risk of intracerebral hemorrhage in the elderly: The MUCH-Italy. Neurology 2018, 91, e227–e235. [Google Scholar] [CrossRef]
- Larsson, S.C.; Wallin, A.; Wolk, A.; Markus, H.S. Differing association of alcohol consumption with different stroke types: A systematic review and meta-analysis. BMC Med. 2016, 14, 178. [Google Scholar] [CrossRef] [Green Version]
- Pedrosa, J.F.; Ribeiro, A.L.P.; Santana, P.C.; Araújo, L.F.; Barreto, S.M. Relation of thoracic aortic and coronary artery calcium to cardiovascular risk factors (from The Brazilian Longitudinal Study of Adult Health [ELSA-Brazil])-ClinicalKey. Am. J. Cardiol. 2019, 124, 1655–1661. Available online: https://www.clinicalkey.es/#!/content/playContent/1-s2.0-S0002914919309956?returnurl=https:%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS0002914919309956%3Fshowall%3Dtrue&referrer=https:%2F%2Fwww.ncbi.nlm.nih.gov%2F (accessed on 29 October 2019). [CrossRef] [PubMed]
- Costanzo, S.; Di Castelnuovo, A.; Donati, M.B.; Iacoviello, L.; de Gaetano, G. Alcohol consumption and mortality in patients with cardiovascular disease: A Meta-Analysis. J. Am. Coll. Cardiol. 2010, 55, 1339–1347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knott, C.S.; Coombs, N.; Stamatakis, E.; Biddulph, J.P. All cause mortality and the case for age specific alcohol consumption guidelines: Pooled analyses of up to 10 population based cohorts. BMJ 2015, 350, h384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stockwell, T.; Zhao, J.; Panwar, S.; Roemer, A.; Naimi, T.; Chikritzhs, T. Do “Moderate” Drinkers have reduced mortality risk? A systematic review and meta-analysis of alcohol consumption and all-cause mortality. J. Stud. Alcohol Drugs 2016, 77, 185–198. [Google Scholar] [CrossRef] [Green Version]
- Xi, B.; Veeranki, S.P.; Zhao, M.; Ma, C.; Yan, Y.; Mi, J. Relationship of alcohol consumption to all-cause, cardiovascular, and cancer-related mortality in U.S. adults-ClinicalKey. J. Am. Coll. Cardiol. 2017, 70, 913–922. Available online: https://www.clinicalkey.es/#!/content/playContent/1-s2.0-S0735109717379986?returnurl=https:%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS0735109717379986%3Fshowall%3Dtrue&referrer=https:%2F%2Fwww.ncbi.nlm.nih.gov%2F (accessed on 8 November 2019). [CrossRef]
- Pai, J.K.; Mukamal, K.J.; Rimm, E.B. Long-term alcohol consumption in relation to all-cause and cardiovascular mortality among survivors of myocardial infarction: The Health Professionals Follow-up Study. Eur. Heart J. 2012, 33, 1598–1605. [Google Scholar] [CrossRef] [Green Version]
- O’Keefe, J.H.; Bybee, K.A.; Lavie, C.J. Alcohol and cardiovascular health: The razor-sharp double-edged sword. J. Am. Coll. Cardiol. 2007, 50, 1009–1014. [Google Scholar] [CrossRef] [Green Version]
- Costanzo, S.; de Gaetano, G.; Di Castelnuovo, A.; Djoussé, L.; Poli, A.; van Velden, D.P. Moderate alcohol consumption and lower total mortality risk: Justified doubts or established facts? Nutr. Metab. Cardiovasc. Dis. 2019, 29, 1003–1008. [Google Scholar] [CrossRef]
- Toma, A.; Paré, G.; Leong, D.P. Alcohol and cardiovascular disease: How much is too much? Curr. Atheroscler. Rep. 2017, 19, 13. [Google Scholar] [CrossRef]
- Sipilä, P.; Rose, R.J.; Kaprio, J. Drinking and mortality: long-term follow-up of drinking-discordant twin pairs. Addiction 2016, 111, 245–254. [Google Scholar] [CrossRef]
- Glymour, M.M. Alcohol and cardiovascular disease: New research tools will help us untangle this enigmatic association, eventually. BMJ 2014, 349, g4334. [Google Scholar] [CrossRef] [PubMed]
- Quifer-Rada, P.; Vallverdú-Queralt, A.; Martínez-Huélamo, M.; Chiva-Blanch, G.; Jáuregui, O.; Estruch, R.; Lamuela-Raventós, R. A comprehensive characterisation of beer polyphenols by high resolution mass spectrometry (LC-ESI-LTQ-Orbitrap-MS). Food Chem. 2015, 169, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Chiva-Blanch, G.; Visioli, F. Polyphenols and health: Moving beyond antioxidants. J. Berry Res. 2012, 2, 63–71. [Google Scholar] [CrossRef] [Green Version]
- Chiva-Blanch, G.; Badimon, L. Effects of polyphenol intake on metabolic syndrome: Current evidences from human trials. Oxid. Med. Cell. Longev. 2017, 2017, 5812401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arora, I.; Sharma, M.; Tollefsbol, T.O. Combinatorial epigenetics impact of polyphenols and phytochemicals in cancer prevention and therapy. Int. J. Mol. Sci. 2019, 20, 4567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gronbaek, M.; Becker, U.; Johansen, D.; Gottschau, A.; Schnohr, P.; Hein, H.O.; Jensen, G.; Sorensen, T.I.A. Type of alcohol consumed and mortality from all causes, coronary heart disease, and cancer. Ann. Intern. Med. 2000, 133, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Imhof, A.; Woodward, M.; Doering, A.; Helbecque, N.; Loewel, H.; Amouyel, P.; Lowe, G.; Koenig, W. Overall alcohol intake, beer, wine, and systemic markers of inflammation in western Europe: results from three MONICA samples (Augsburg, Glasgow, Lille). Eur. Heart J. 2004, 25, 2092–2100. [Google Scholar] [CrossRef] [Green Version]
- Malarcher, A.M.; Giles, W.H.; Croft, J.B.; Wozniak, M.A.; Wityk, R.J.; Stolley, P.D.; Stern, B.J.; Sloan, M.A.; Sherwin, R.; Price, T.R.; et al. Alcohol intake, type of beverage, and the risk of cerebral infarction in young women. Stroke 2001, 32, 77–83. [Google Scholar] [CrossRef] [Green Version]
- Chiva-Blanch, G.; Urpi-Sarda, M.; Ros, E.; Valderas-Martinez, P.; Casas, R.; Arranz, S.; Guillén, M.; Lamuela-Raventós, R.M.; Llorach, R.; Andres-Lacueva, C.; et al. Effects of red wine polyphenols and alcohol on glucose metabolism and the lipid profile: A randomized clinical trial. Clin. Nutr. 2013, 32, 200–206. [Google Scholar] [CrossRef]
- Castaldo, L.; Narváez, A.; Izzo, L.; Graziani, G.; Gaspari, A.; Di Minno, G.; Ritieni, A. Red wine consumption and cardiovascular health. Molecules 2019, 24, 3626. [Google Scholar] [CrossRef] [Green Version]
- Padro, T.; Muñoz-García, N.; Vilahur, G.; Chagas, P.; Deyà, A.; Antonijoan, R.M.; Badimon, L. Moderate beer intake and cardiovascular health in overweight individuals. Nutrients 2018, 10, 1237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiva-Blanch, G.; Magraner, E.; Condines, X.; Valderas-Martínez, P.; Roth, I.; Arranz, S.; Casas, R.; Navarro, M.; Hervas, A.; Sisó, A.; et al. Effects of alcohol and polyphenols from beer on atherosclerotic biomarkers in high cardiovascular risk men: A randomized feeding trial. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 36–45. [Google Scholar] [CrossRef] [PubMed]
- De Gaetano, G.; Costanzo, S.; Di Castelnuovo, A.; Badimon, L.; Bejko, D.; Alkerwi, A.; Chiva-Blanch, G.; Estruch, R.; La Vecchia, C.; Panico, S.; et al. Effects of moderate beer consumption on health and disease: A consensus document. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 443–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piepoli, M.F.; Abreu, A.; Albus, C.; Ambrosetti, M.; Brotons, C.; Catapano, A.L.; Corra, U.; Cosyns, B.; Deaton, C.; Graham, I.; et al. Update on cardiovascular prevention in clinical practice: A position paper of the European Association of Preventive Cardiology of the European Society of Cardiology. Eur. J. Prev. Cardiol. 2019, in press. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albert, M.A.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; Michos, E.D.; Miedema, M.D.; Muñoz, D.; Smith, S.C.; et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: A report of the American college of cardiology/American heart association task force on clinical practice guidelines. Circulation 2019, 140, e596–e646. [Google Scholar]
- Van de Luitgaarden, I.A.T.; Beulens, J.W.J.; Schrieks, I.C.; Kieneker, L.M.; Touw, D.J.; van Ballegooijen, A.J.; van Oort, S.; Grobbee, D.E.; Bakker, S.J.L. Urinary ethyl glucuronide can be used as a biomarker of habitual alcohol consumption in the general population. J. Nutr. 2019, 149, 2199–2205. [Google Scholar] [CrossRef]
- Kloner, R.A.; Rezkalla, S.H. To drink or not to drink? That is the question. Circulation 2007, 116, 1306–1317. [Google Scholar] [CrossRef]
- Abat, C.; Roussel, Y.; Chaudet, H.; Raoult, D. Alcohol and the global burden of disease. Lancet 2019, 393, 2390–2391. [Google Scholar] [CrossRef] [Green Version]

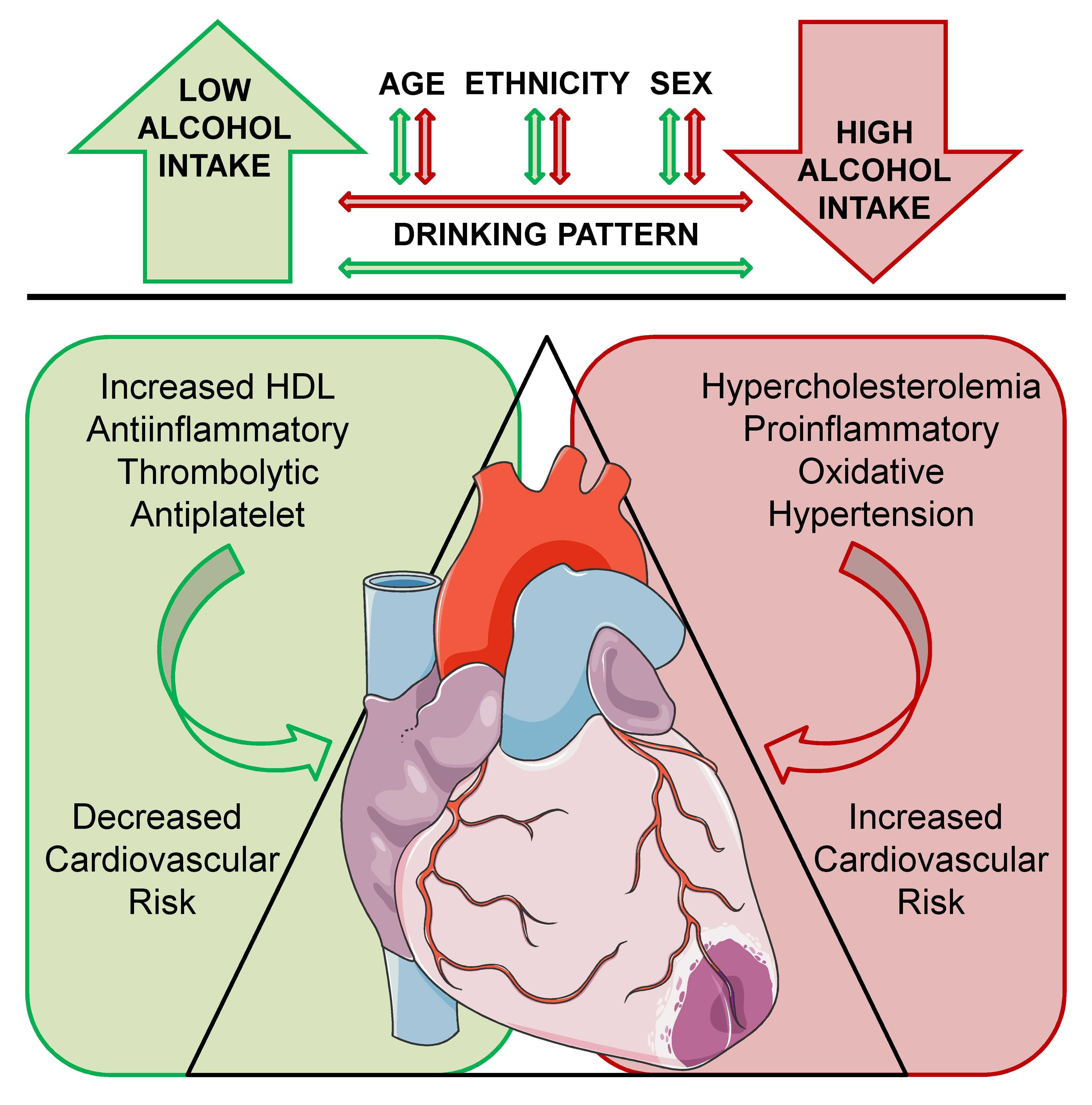{kind=link}
Table 1.
Definition of drinking levels according to the US National Institute on Alcohol Abuse and Alcoholism.
Table 1.
Definition of drinking levels according to the US National Institute on Alcohol Abuse and Alcoholism.
| Drinking Level | Number of Drinks 1 | Amount of Alcohol |
|---|---|---|
| Low-risk consumption | ≤3 drinks on a single day for women | ≤32 g/single day (occasional) |
| ≤7 drinks/week for women | ≤14 g/day (regular) | |
| ≤4 drinks on a single day for men | ≤46 g/single day (occasional) | |
| ≤14 drinks/week for men | ≤28 g/day (regular) | |
| Moderate | ≤1 drink/day for women | ≤14 g/day (regular) |
| ≤2 drink/day for men | ≤28 g/day (regular) | |
| Binge | ≥4 drinks in 2 h for women | 56 g in one occasion |
| ≥5 drinks in 2 h for men | 70 g in one occasion | |
| Heavy | ≥5 binge drinking days in a month | ≥280 g in a month |
1 A drink is defined as 14 g of pure alcohol.
Table 2.
Effects of alcohol consumption in cardiovascular risk biomarkers, classical risk factors, and major events according to the amount of alcohol consumed.
Table 2.
Effects of alcohol consumption in cardiovascular risk biomarkers, classical risk factors, and major events according to the amount of alcohol consumed.
| Cardiovascular Parameter | Low/Moderate Alcohol Consumption | Heavy/Binge Drinking |
|---|---|---|
| Intermediate biomarkers | ||
| Inflammation | + 1 | − |
| Oxidation | ± 1 | − |
| Thrombosis | + | ± |
| Classical risk factors | ||
| Lipid profile | + | − |
| Glucose metabolism | + | ± |
| Blood pressure | − | − |
| Major adverse cardiovascular events | ||
| Acute myocardial infarction | + | ± |
| Stroke | + | − |
| Cardiovascular mortality | + | − |
1 Differences observed depending on the type of alcoholic beverage consumed. “+” indicates protective effects (inverse association); “−” denotes detrimental effects (positive association); and “±” signifies neutral effects (lack of association) or inconclusive/contradictory results.
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chiva-Blanch, G.; Badimon, L. Benefits and Risks of Moderate Alcohol Consumption on Cardiovascular Disease: Current Findings and Controversies. Nutrients 2020, 12, 108. https://doi.org/10.3390/nu12010108
AMA Style
Chiva-Blanch G, Badimon L. Benefits and Risks of Moderate Alcohol Consumption on Cardiovascular Disease: Current Findings and Controversies. Nutrients. 2020; 12(1):108. https://doi.org/10.3390/nu12010108
Chicago/Turabian StyleChiva-Blanch, Gemma, and Lina Badimon. 2020. "Benefits and Risks of Moderate Alcohol Consumption on Cardiovascular Disease: Current Findings and Controversies" Nutrients 12, no. 1: 108. https://doi.org/10.3390/nu12010108
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.