
Prevalence and Implications of Low Reticulocyte–Hemoglobin Levels among Extreme Preterm Neonates: A Single-Center Retrospective Study

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Clinical Characteristics
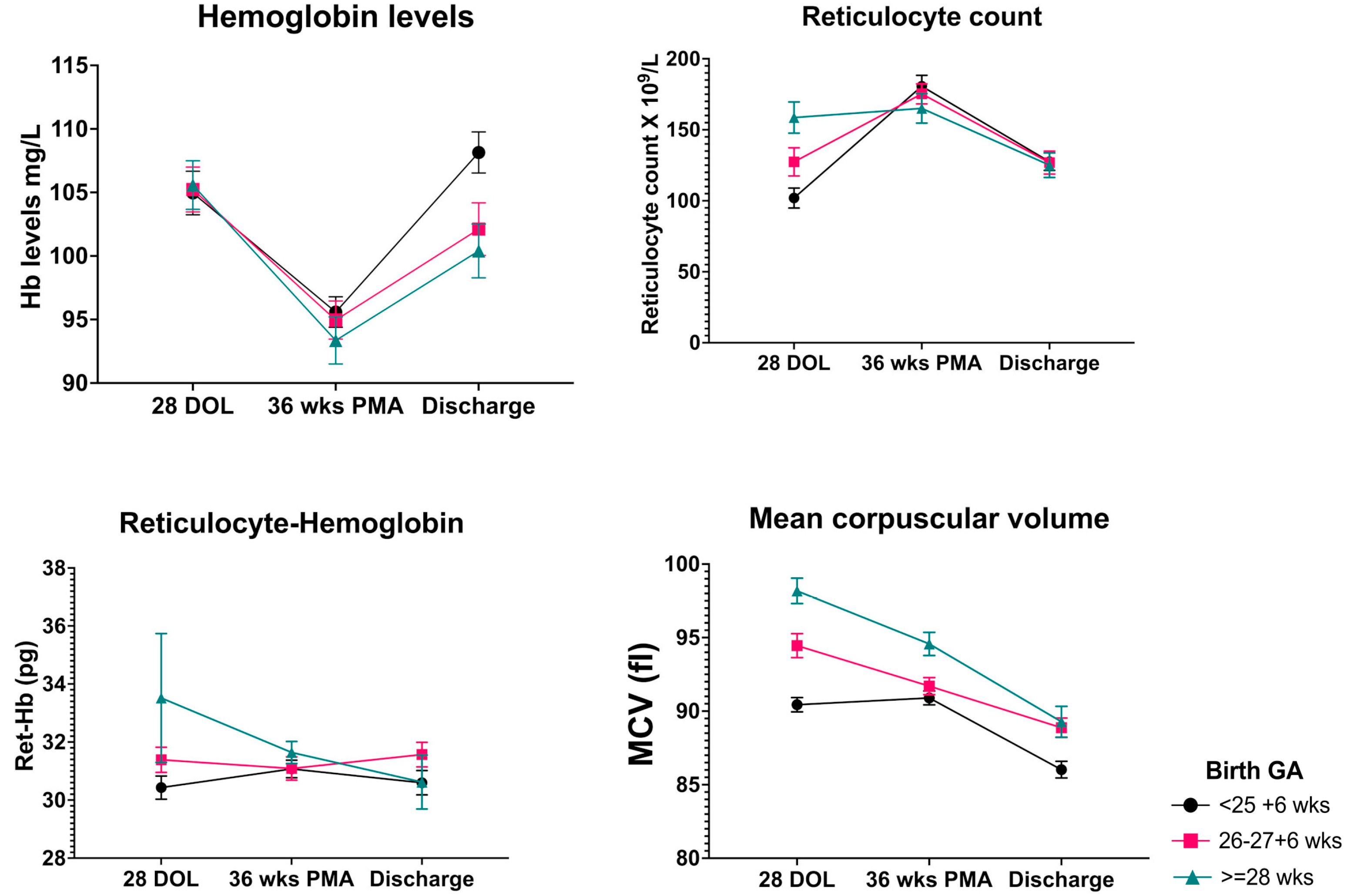
3.2. Hematological Parameters
3.3. Neurodevelopmental Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Le, N.T.; Richardson, D.R. The role of iron in cell cycle progression and the proliferation of neoplastic cells. Biochim. Biophys. Acta Rev. Cancer 2002, 1603, 31–46. [Google Scholar] [CrossRef]
- Tierney, A.L.; Nelson III, C.A. Brain development and the role of experience in the early years. Zero Three 2009, 30, 9. [Google Scholar]
- Arpino, C.; Compagnone, E.; Montanaro, M.L.; Cacciatore, D.; De Luca, A.; Cerulli, A.; Di Girolamo, S.; Curatolo, P. Preterm birth and neurodevelopmental outcome: A review. Child’s Nerv. Syst. 2010, 26, 1139–1149. [Google Scholar] [CrossRef] [PubMed]
- Armony-Sivan, R.; Eidelman, A.I.; Lanir, A.; Sredni, D.; Yehuda, S. Iron status and neurobehavioral development of premature infants. J. Perinatol. 2004, 24, 757–762. [Google Scholar] [PubMed] [Green Version]
- Radlowski, E.C.; Johnson, R.W. Perinatal iron deficiency and neurocognitive development. Front. Hum. Neurosci. 2013, 7, 585. [Google Scholar] [CrossRef] [Green Version]
- Zamora, T.G.; Guiang, S.F., 3rd; Widness, J.A.; Georgieff, M.K. Iron is prioritized to red blood cells over the brain in phlebotomized anemic newborn lambs. Pediatr. Res. 2016, 79, 922–928. [Google Scholar] [CrossRef] [Green Version]
- Mills, R.J.; Davies, M.W. Enteral iron supplementation in preterm and low birth weight infants. Cochrane Database Syst. Rev. 2012, 14, CD00509. [Google Scholar] [CrossRef] [Green Version]
- Siddappa, A.M.; Rao, R.; Long, J.D.; Widness, J.A.; Georgieff, M.K. The assessment of newborn iron stores at birth: A review of the literature and standards for ferritin concentrations. Neonatology 2007, 92, 73–82. [Google Scholar] [CrossRef] [Green Version]
- Christensen, R.D.; Henry, E.; Bennett, S.T.; Yaish, H.M. Reference intervals for reticulocyte parameters of infants during their first 90 days after birth. J. Perinatol. 2016, 36, 61–66. [Google Scholar] [CrossRef]
- Lorenz, L.; Arand, J.; Büchner, K.; Wacker-Gussmann, A.; Peter, A.; Poets, C.F.; Franz, A.R. Reticulocyte haemoglobin content as a marker of iron deficiency. Arch. Dis. Child.-Fetal Neonatal Ed. 2015, 100, F198–F202. [Google Scholar] [CrossRef]
- German, K.; Vu, P.T.; Irvine, J.D.; Juul, S.E. Trends in reticulocyte hemoglobin equivalent values in critically ill neonates, stratified by gestational age. J. Perinatol. 2019, 39, 1268–1274. [Google Scholar] [CrossRef] [PubMed]
- Piva, E.; Brugnara, C.; Spolaore, F.; Plebani, M. Clinical utility of reticulocyte parameters. Clin. Lab. Med. 2015, 35, 133–163. [Google Scholar] [CrossRef] [PubMed]
- Pomrop, M.; Manopunya, S.; Tantiprabha, W.; Khuwuthyakorn, V.; Kosarat, S.; Natesirinilkul, R. Reticulocyte hemoglobin concentration for screening iron deficiency in very low birth weight preterm neonates. J. Matern.-Fetal Neonatal Med. 2020, 35, 3348–3352. [Google Scholar] [CrossRef] [PubMed]
- Bode, M.M.; D′Eugenio, D.B.; Mettelman, B.B.; Gross, S.J. Predictive validity of the Bayley, Third Edition at 2 years for intelligence quotient at 4 years in preterm infants. J. Dev. Behav. Pediatr. 2014, 35, 570–575. [Google Scholar] [CrossRef] [PubMed]
- Richardson, D.K.; Corcoran, J.D.; Escobar, G.J.; Lee, S.K. SNAP-II and SNAPPE-II: Simplified newborn illness severity and mortality risk scores. J. Pediatr. 2001, 138, 92–100. [Google Scholar] [CrossRef]
- Papile, L.-A.; Burstein, J.; Burstein, R.; Koffler, H. Incidence and evolution of subependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1500 gm. J. Pediatr. 1978, 92, 529–534. [Google Scholar] [CrossRef]
- Bell, M.J.; Ternberg, J.L.; Feigin, R.D.; Keating, J.P.; Marshall, R.; Barton, L.; Brotherton, T. Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann. Surg. 1978, 187, 1–7. [Google Scholar] [CrossRef]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef]
- Mast, A.E.; Blinder, M.A.; Lu, Q.; Flax, S.; Dietzen, D.J. Clinical utility of the reticulocyte hemoglobin content in the diagnosis of iron deficiency. Blood J. Am. Soc. Hematol. 2002, 99, 1489–1491. [Google Scholar] [CrossRef]
- Al-Ghananim, R.T.; Nalbant, D.; Schmidt, R.L.; Cress, G.A.; Zimmerman, M.B.; Widness, J.A. Reticulocyte Hemoglobin Content During the First Month of Life in Critically Ill Very Low Birth Weight Neonates Differs From Term Infants, Children, and Adults. J. Clin. Lab. Anal. 2016, 30, 326–334. [Google Scholar] [CrossRef]
- Juul, S. Erythropoiesis and the approach to anemia in premature infants. J. Matern.-Fetal Neonatal Med. 2012, 25, 97–99. [Google Scholar] [CrossRef] [PubMed]
- Strauss, R.G. Anaemia of prematurity: Pathophysiology and treatment. Blood Rev. 2010, 24, 221–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiza, V.; Giapros, V.; Pantou, K.; Theocharis, P.; Challa, A.; Andronikou, S. Serum transferrin receptor, ferritin, and reticulocyte maturity indices during the first year of life in ‘large’ preterm infants. Eur. J. Haematol. 2007, 79, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Takala, T.I.; Mäkelä, E.; Suominen, P.; Matomäki, J.; Lapinleimu, H.; Lehtonen, L.; Rajamäki, A.; Irjala, K.; Lähteenmäki, P.M. Blood cell and iron status analytes of preterm and full-term infants from 20 weeks onwards during the first year of life. Clin. Chem. Lab. Med. 2010, 48, 1295–1301. [Google Scholar] [CrossRef]
- Widness, J.A. Pathophysiology of Anemia During the Neonatal Period, Including Anemia of Prematurity. Neoreviews 2008, 9, e520–e525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mäkelä, E.; Takala, T.I.; Suominen, P.; Matomäki, J.; Salmi, T.T.; Rajamäki, A.; Lapinleimu, H.; Lehtonen, L.; Irjala, K.; Lähteenmäki, P.M. Hematological parameters in preterm infants from birth to 16 weeks of age with reference to iron balance. Clin. Chem. Lab. Med. 2008, 46, 551–557. [Google Scholar] [CrossRef] [PubMed]
- King, D.J.; Brunton, J.; Barr, R.D. The influence of corticosteroids on human erythropoiesis. An in vivo study. Am. J. Pediatr. Hematol. Oncol. 1988, 10, 313–315. [Google Scholar] [CrossRef]
- Löfving, A.; Domellöf, M.; Hellström-Westas, L.; Andersson, O. Reference intervals for reticulocyte hemoglobin content in healthy infants. Pediatr. Res. 2018, 84, 657–661. [Google Scholar] [CrossRef]
- Choi, J.W.; Pai, S.H.; Im, M.W.; Kim, S.K. Change in transferrin receptor concentrations with age. Clin. Chem. 1999, 45, 1562–1563. [Google Scholar] [CrossRef] [Green Version]
- Domellöf, M.; Lönnerdal, B.; Dewey, K.G.; Cohen, R.J.; Rivera, L.L.; Hernell, O. Sex differences in iron status during infancy. Pediatrics 2002, 110, 545–552. [Google Scholar] [CrossRef]
- Beard, J.L.; Wiesinger, J.A.; Connor, J.R. Pre-and postweaning iron deficiency alters myelination in Sprague-Dawley rats. Dev. Neurosci. 2003, 25, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Jorgenson, L.A.; Wobken, J.D.; Georgieff, M.K. Perinatal iron deficiency alters apical dendritic growth in hippocampal CA1 pyramidal neurons. Dev. Neurosci. 2003, 25, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Youdim, M.; Sills, M.A.; Heydorn, W.E.; Creed, G.J.; Jacobowitz, D.M. Iron deficiency alters discrete proteins in rat caudate nucleus and nucleus accumbens. J. Neurochem. 1986, 47, 794–799. [Google Scholar] [CrossRef] [PubMed]
- Amin, S.B.; Orlando, M.; Wang, H. Latent iron deficiency in utero is associated with abnormal auditory neural myelination in ≥ 35 weeks gestational age infants. J. Pediatr. 2013, 163, 1267–1271. [Google Scholar] [CrossRef]
- Tamura, T.; Goldenberg, R.L.; Hou, J.; Johnston, K.E.; Cliver, S.P.; Ramey, S.L.; Nelson, K.G. Cord serum ferritin concentrations and mental and psychomotor development of children at five years of age. J. Pediatr. 2002, 140, 165–170. [Google Scholar] [CrossRef]
- Siddappa, A.M.; Georgieff, M.K.; Wewerka, S.; Worwa, C.; Nelson, C.A.; Deregnier, R.A. Iron deficiency alters auditory recognition memory in newborn infants of diabetic mothers. Pediatr. Res. 2004, 55, 1034–1041. [Google Scholar] [CrossRef] [Green Version]
- Choudhury, V.; Amin, S.B.; Agarwal, A.; Srivastava, L.M.; Soni, A.; Saluja, S. Latent iron deficiency at birth influences auditory neural maturation in late preterm and term infants. Am. J. Clin. Nutr. 2015, 102, 1030–1034. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, E.K.; Dempsey, E.M.; Kiely, M.E. Iron supplementation in preterm and low-birth-weight infants: A systematic review of intervention studies. Nutr. Rev. 2019, 77, 865–877. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Ret-Hb > 29 | Ret-Hb ≤ 29 | p Value | |
|---|---|---|---|
| N = 168 | N = 47 | ||
| Gender (Male) n (%) | 74 (44) | 31 (65%) | 0.008 |
| Gestational age (weeks) mean (SD) | 26 (1.6) | 25.5 (1.6) | 0.07 |
| Birth Weight (g) mean (SD) | 898 (237) | 837 (207) | 0.11 |
| Apgar score at 5 min median (IQR) | 7 (6–8) | 7 (6–8) | 0.99 |
| Cord arterial pH or postnatal gas pH | 7.28 (0.09) | 7.29 (0.08) | 0.53 |
| Delayed Cord Clamping n (%) | 75 (44) | 22 (46) | 0.81 |
| SNAPPE-II score mean (SD) | 26.7 (18) | 31.3 (21) | 0.15 |
| No of transfusions median (IQR) | 3 (1–5) | 3 (1–5) | 0.68 |
| Gestation at discharge mean (SD) | 41.6 (6.9) | 42.5 (8.4) | 0.45 |
| Small for gestation n (%) | 11 (6.5) | 1 (2.1) | 0.24 |
| Vaginal delivery n (%) | 67 (39) | 16 (34) | 0.46 |
| Outborn n (%) | 28 (16%) | 9 (19%) | 0.69 |
| Antenatal Steroids n (%) | 93 (55%) | 20 (42%) | 0.12 |
| Chorioamnionitis n (%) | 45 (28%) | 14 (32%) | 0.56 |
| Sepsis n (%) | 48 (28%) | 16 (34%) | 0.46 |
| Necrotising Enterocolitis n (%) | 12 (7%) | 6 (13%) | 0.21 |
| Postnatal steroids n (%) | 85 (50%) | 33 (70%) | 0.02 |
| Laparotomy n (%) | 15 (8%) | 6 (12%) | 0.78 |
| Hemodynamically significant PDA n (%) | 68 (39%) | 23 (48%) | 0.48 |
| Mod-severe Bronchopulmonary Dysplasia n (%) | 44 (30%) | 18 (40%) | 0.14 |
| Retinopathy of Prematurity treatment n (%) | 20 (12%) | 7 (14%) | 0.58 |
| Mod-severe Intraventricular hemorrhage n (%) | 24 (14%) | 9 (19%) | 0.41 |
| Ret-Hb > 29 pg | Ret-Hb ≤ 29 pg | p Value | |
|---|---|---|---|
| N = 168 | N = 47 | ||
| Hemoglobin at day 28 (g/L) | 103 (96–115) | 103 (92–116) | 0.85 |
| Hemoglobin at 36 weeks PMA (g/L) | 94 (87–101) | 89 (84–96) | 0.04 |
| Hemoglobin at discharge (g/L) | 105 (93–114) | 105 (96–117) | 0.45 |
| Reticulocyte count at day 28 (×109/L) | 116 (72–161) | 130 (53–130) | 0.06 |
| Reticulocyte count at 36 weeks CGA (×109/L) | 163 (120–213) | 182 (137–222) | 0.23 |
| Reticulocyte count at discharge (×109/L) | 129 (92–160) | 106 (89–141) | 0.36 |
| Ret-Hb at day 28 (pg) | 31.5 (29.4–33.4) | 30.2 (27.3–33) | 0.04 |
| Ret-Hb at discharge (pg) | 31.9 (30–33) | 29.7 (27–31) | 0.002 |
| MCV at day 28 (fL) | 93.4 (89–97) | 91.9 (87–96) | 0.05 |
| MCV at 36 weeks PMA (fL) | 91.9 (89–95) | 90.2 (87–95) | 0.07 |
| MCV at discharge (fL) | 88.7 (84–91) | 84.7 (81–88) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sriranjan, J.; Kalata, C.; Fusch, G.; Thomas, K.; Goswami, I. Prevalence and Implications of Low Reticulocyte–Hemoglobin Levels among Extreme Preterm Neonates: A Single-Center Retrospective Study. Nutrients 2022, 14, 5343. https://doi.org/10.3390/nu14245343
Sriranjan J, Kalata C, Fusch G, Thomas K, Goswami I. Prevalence and Implications of Low Reticulocyte–Hemoglobin Levels among Extreme Preterm Neonates: A Single-Center Retrospective Study. Nutrients. 2022; 14(24):5343. https://doi.org/10.3390/nu14245343
Chicago/Turabian StyleSriranjan, Jhanahan, Christine Kalata, Gerhard Fusch, Karen Thomas, and Ipsita Goswami. 2022. "Prevalence and Implications of Low Reticulocyte–Hemoglobin Levels among Extreme Preterm Neonates: A Single-Center Retrospective Study" Nutrients 14, no. 24: 5343. https://doi.org/10.3390/nu14245343