
Association between Serum Triglycerides and Prostate Specific Antigen (PSA) among U.S. Males: National Health and Nutrition Examination Survey (NHANES), 2003–2010

 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Data Availability
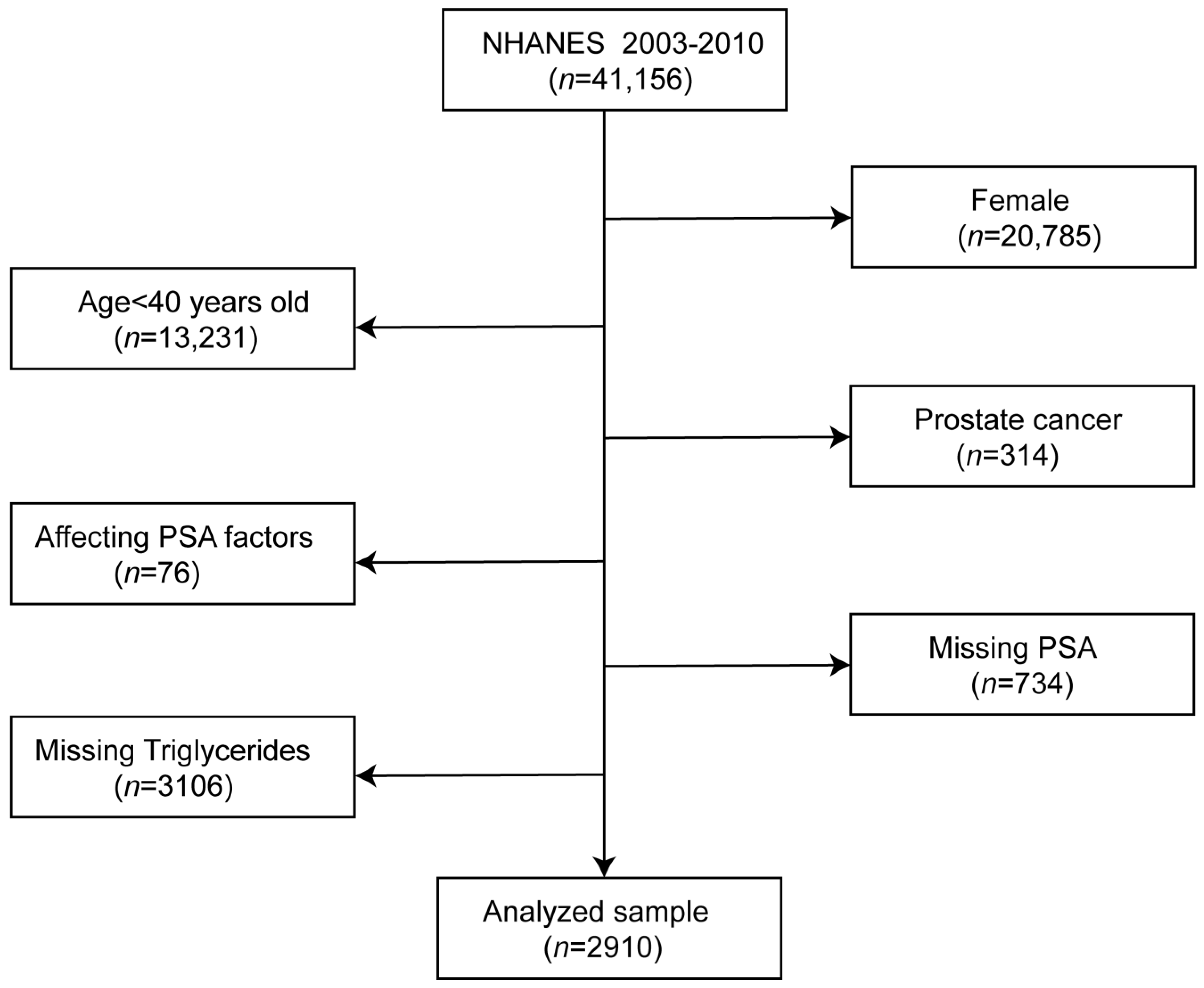
2.2. Study Population
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Selected Participants Subsection
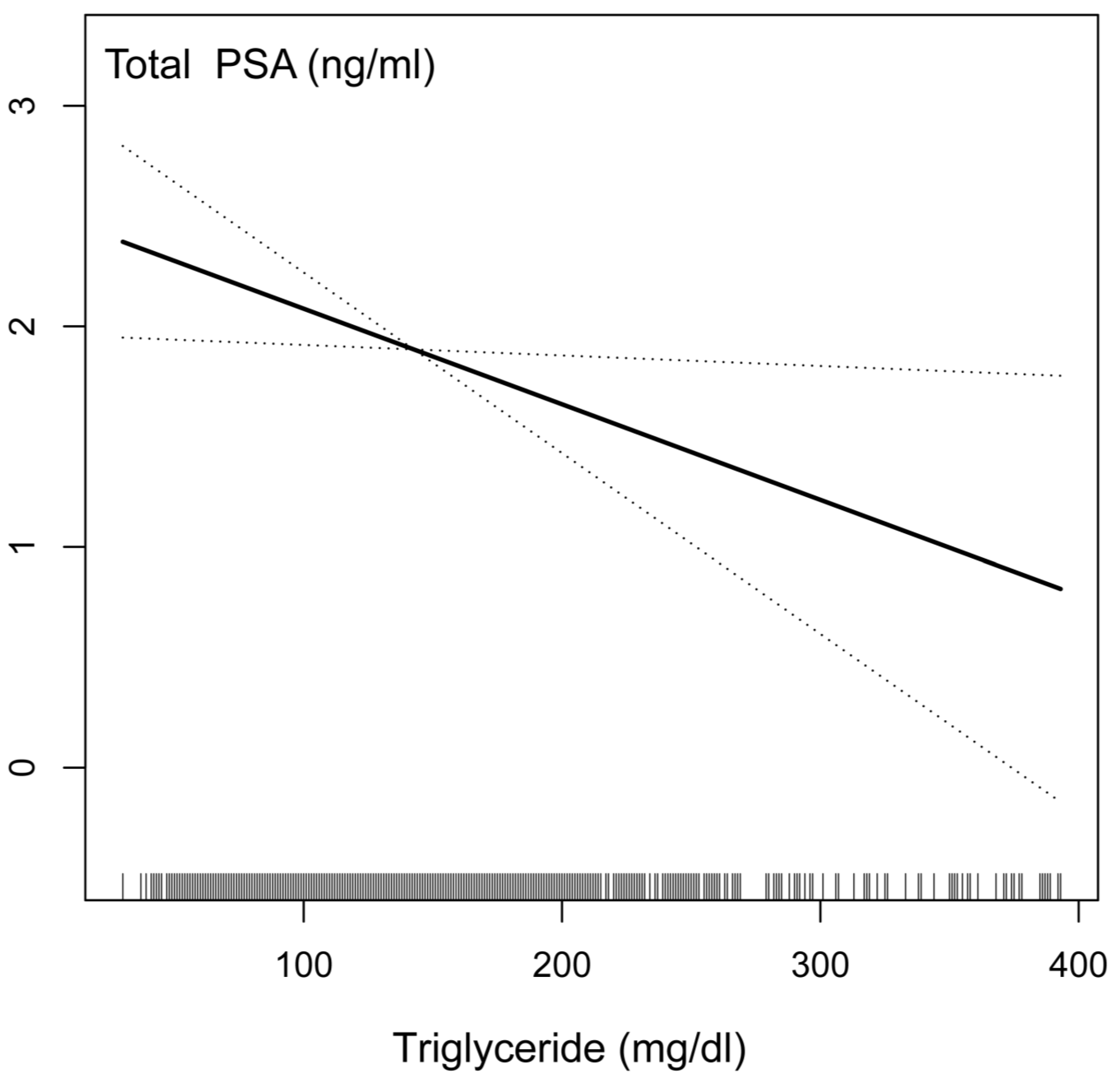
3.2. The Connection between PSA Concentrations and Serum Triglycerides
3.3. Stratified Associations between PSA Concentrations and Serum Triglycerides
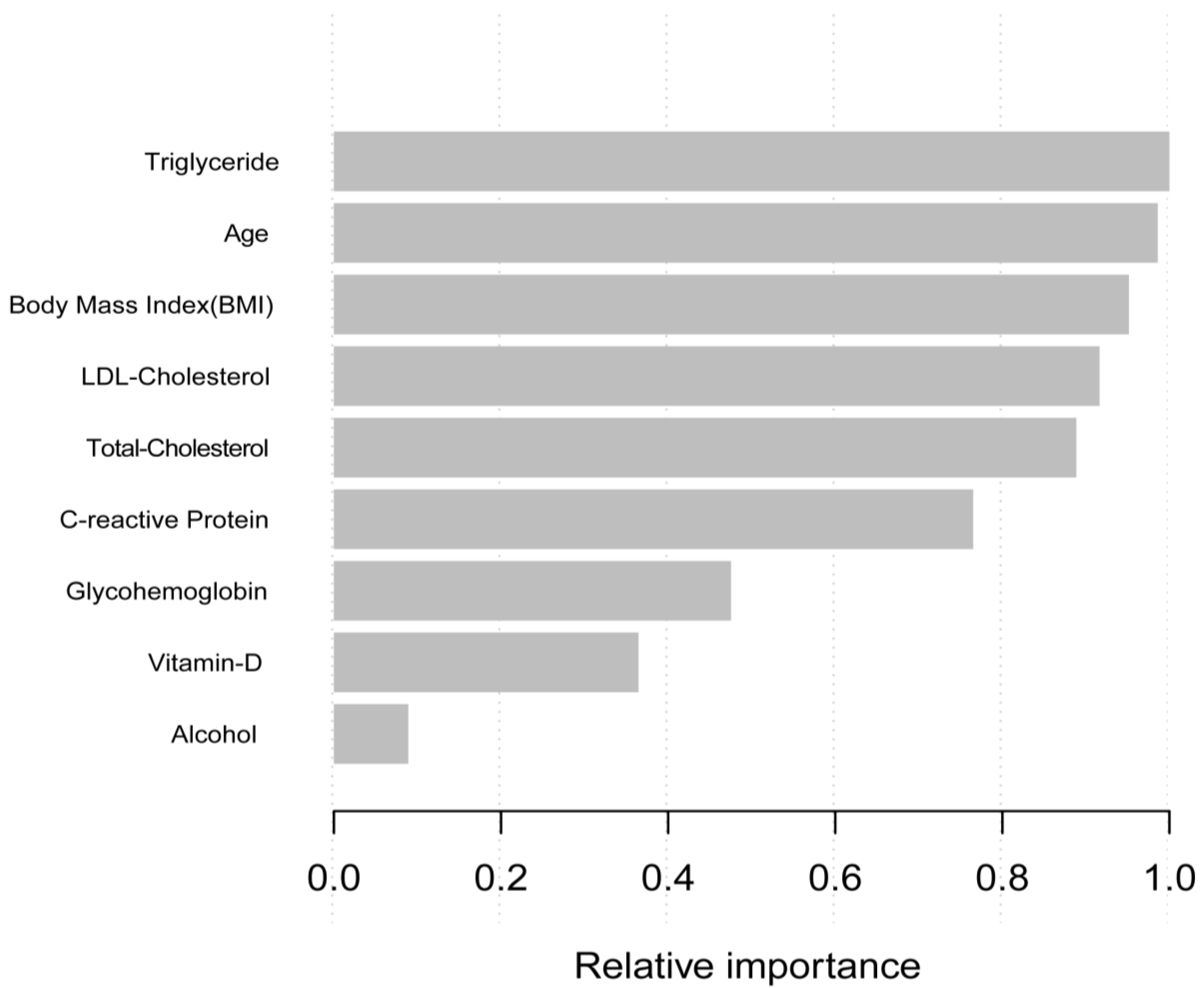
3.4. Machine Learning Using the XGBoost Algorithm Model
3.5. Identification of Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Grossman, D.C.; Curry, S.J.; Owens, D.K.; Bibbins-Domingo, K.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Ebell, M.; Epling, J.W., Jr.; Kemper, A.R.; et al. Screening for Prostate Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2018, 319, 1901–1913. [Google Scholar] [CrossRef] [PubMed]
- Vickers, A.J. Prostate Cancer Screening: Time to Question How to Optimize the Ratio of Benefits and Harms. Ann. Intern. Med. 2017, 167, 509–510. [Google Scholar] [CrossRef] [PubMed]
- Gudmundsson, J.; Sigurdsson, J.K.; Stefansdottir, L.; Agnarsson, B.A.; Isaksson, H.J.; Stefansson, O.A.; Gudjonsson, S.A.; Gudbjartsson, D.F.; Masson, G.; Frigge, M.L.; et al. Genome-wide associations for benign prostatic hyperplasia reveal a genetic correlation with serum levels of PSA. Nat. Commun. 2018, 9, 4568. [Google Scholar] [CrossRef] [Green Version]
- Kristal, A.R.; Chi, C.; Tangen, C.M.; Goodman, P.J.; Etzioni, R.; Thompson, I.M. Associations of demographic and lifestyle characteristics with prostate-specific antigen (PSA) concentration and rate of PSA increase. Cancer 2006, 106, 320–328. [Google Scholar] [CrossRef]
- Buddingh, K.T.; Maatje, M.G.F.; Putter, H.; Kropman, R.F.; Pelger, R.C.M. Do antibiotics decrease prostate-specific antigen levels and reduce the need for prostate biopsy in type IV prostatitis? A systematic literature review. Can. Urol. Assoc. J. 2018, 12, E25–E30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Xiao, G.; Zhou, J.W.; Yang, J.K.; Lu, L.; Bian, J.; Zhong, L.; Wei, Q.Z.; Zhou, Q.Z.; Xue, K.Y.; et al. Optimal Starting Age and Baseline Level for Repeat Tests: Economic Concerns of PSA Screening for Chinese Men-10-Year Experience of a Single Center. Urol. Int. 2020, 104, 230–238. [Google Scholar] [CrossRef]
- Tan, G.H.; Nason, G.; Ajib, K.; Woon, D.T.S.; Herrera-Caceres, J.; Alhunaidi, O.; Perlis, N. Smarter screening for prostate cancer. World J. Urol. 2019, 37, 991–999. [Google Scholar] [CrossRef]
- Han, P.K.; Kobrin, S.; Breen, N.; Joseph, D.A.; Li, J.; Frosch, D.L.; Klabunde, C.N. National evidence on the use of shared decision making in prostate-specific antigen screening. Ann. Fam. Med. 2013, 11, 306–314. [Google Scholar] [CrossRef] [Green Version]
- Fenton, J.J.; Weyrich, M.S.; Durbin, S.; Liu, Y.; Bang, H.; Melnikow, J. Prostate-Specific Antigen-Based Screening for Prostate Cancer: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2018, 319, 1914–1931. [Google Scholar] [CrossRef]
- Misra-Hebert, A.D.; Hu, B.; Klein, E.A.; Stephenson, A.; Taksler, G.B.; Kattan, M.W.; Rothberg, M.B. Prostate cancer screening practices in a large, integrated health system: 2007–2014. BJU Int. 2017, 120, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.M.; Donovan, J.L.; Turner, E.L.; Metcalfe, C.; Young, G.J.; Walsh, E.I.; Lane, J.A.; Noble, S.; Oliver, S.E.; Evans, S.; et al. Effect of a Low-Intensity PSA-Based Screening Intervention on Prostate Cancer Mortality: The CAP Randomized Clinical Trial. JAMA 2018, 319, 883–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamnagerwalla, J.; Howard, L.E.; Allott, E.H.; Vidal, A.C.; Moreira, D.M.; Castro-Santamaria, R.; Andriole, G.L.; Freeman, M.R.; Freedland, S.J. Serum cholesterol and risk of high-grade prostate cancer: Results from the REDUCE study. Prostate Cancer Prostatic Dis. 2018, 21, 252–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz, P.M.; Mo, H.; McConathy, W.J.; Sabnis, N.; Lacko, A.G. The role of cholesterol metabolism and cholesterol transport in carcinogenesis: A review of scientific findings, relevant to future cancer therapeutics. Front. Pharmacol. 2013, 4, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zadra, G.; Photopoulos, C.; Loda, M. The fat side of prostate cancer. Biochim. Biophys. Acta 2013, 1831, 1518–1532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farwell, W.R.; D’Avolio, L.W.; Scranton, R.E.; Lawler, E.V.; Gaziano, J.M. Statins and prostate cancer diagnosis and grade in a veterans population. J. Natl. Cancer Inst. 2011, 103, 885–892. [Google Scholar] [CrossRef] [Green Version]
- Kok, D.E.; van Roermund, J.G.; Aben, K.K.; den Heijer, M.; Swinkels, D.W.; Kampman, E.; Kiemeney, L.A. Blood lipid levels and prostate cancer risk; a cohort study. Prostate Cancer Prostatic Dis. 2011, 14, 340–345. [Google Scholar] [CrossRef] [Green Version]
- Van Hemelrijck, M.; Walldius, G.; Jungner, I.; Hammar, N.; Garmo, H.; Binda, E.; Hayday, A.; Lambe, M.; Holmberg, L. Low levels of apolipoprotein A-I and HDL are associated with risk of prostate cancer in the Swedish AMORIS study. Cancer Causes Control CCC 2011, 22, 1011–1019. [Google Scholar] [CrossRef]
- YuPeng, L.; YuXue, Z.; PengFei, L.; Cheng, C.; YaShuang, Z.; DaPeng, L.; Chen, D. Cholesterol Levels in Blood and the Risk of Prostate Cancer: A Meta-analysis of 14 Prospective Studies. Cancer Epidemiol. Prev. Biomark. 2015, 24, 1086–1093. [Google Scholar] [CrossRef] [Green Version]
- Guo, H.; Jia, X.; Liu, H. Based on biomedical index data: Risk prediction model for prostate cancer. Medicine 2021, 100, e25602. [Google Scholar] [CrossRef]
- Garrido, M.M.; Marta, J.C.; Ribeiro, R.M.; Pinheiro, L.C.; Guimarães, J.T. Serum lipids and prostate cancer. J. Clin. Lab. Anal. 2021, 35, e23705. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.L.; Harshman, L.C.; Presti, J.C., Jr. Impact of common medications on serum total prostate-specific antigen levels: Analysis of the National Health and Nutrition Examination Survey. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 3951–3957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Zipf, G.; Chiappa, M.; Porter, K.S.; Ostchega, Y.; Lewis, B.G.; Dostal, J. National health and nutrition examination survey: Plan and operations, 1999–2010. Vital Health Stat. Ser. 1 Programs Collect. Proced. 2013, 1–37. Available online: https://stacks.cdc.gov/view/cdc/21304 (accessed on 7 October 2021).
- Arthur, R.; Møller, H.; Garmo, H.; Holmberg, L.; Stattin, P.; Malmstrom, H.; Lambe, M.; Hammar, N.; Walldius, G.; Robinson, D.; et al. Association between baseline serum glucose, triglycerides and total cholesterol, and prostate cancer risk categories. Cancer Med. 2016, 5, 1307–1318. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Zhang, Y.; Wang, X.; Lin, D.; Chen, Z. Relationship between body mass index and concentrations of prostate specific antigen: A cross-sectional study. Scand. J. Clin. Lab. Investig. 2020, 80, 162–167. [Google Scholar] [CrossRef]
- Mydlo, J.H.; Tieng, N.L.; Volpe, M.A.; Chaiken, R.; Kral, J.G. A pilot study analyzing PSA, serum testosterone, lipid profile, body mass index and race in a small sample of patients with and without carcinoma of the prostate. Prostate Cancer Prostatic Dis. 2001, 4, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Capitanio, U.; Perrotte, P.; Hutterer, G.C.; Suardi, N.; Jeldres, C.; Shariat, S.F.; Duclos, A.; Arjane, P.; Montorsi, F.; Karakiewicz, P.I. Effect of body mass index on prostate-specific antigen and percentage free prostate-specific antigen: Results from a prostate cancer screening cohort of 1490 men. Int. J. Urol. Off. J. Jpn. Urol. Assoc. 2009, 16, 91–95. [Google Scholar] [CrossRef]
- Barqawi, A.B.; Golden, B.K.; O’Donnell, C.; Brawer, M.K.; Crawford, E.D. Observed effect of age and body mass index on total and complexed PSA: Analysis from a national screening program. Urology 2005, 65, 708–712. [Google Scholar] [CrossRef]
- Bañez, L.L.; Hamilton, R.J.; Partin, A.W.; Vollmer, R.T.; Sun, L.; Rodriguez, C.; Wang, Y.; Terris, M.K.; Aronson, W.J.; Presti, J.C., Jr.; et al. Obesity-related plasma hemodilution and PSA concentration among men with prostate cancer. JAMA 2007, 298, 2275–2280. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Ho, K.M.; Hong, Y. Machine learning for the prediction of volume responsiveness in patients with oliguric acute kidney injury in critical care. Crit. Care 2019, 23, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livne, M.; Boldsen, J.K.; Mikkelsen, I.K.; Fiebach, J.B.; Sobesky, J.; Mouridsen, K. Boosted Tree Model Reforms Multimodal Magnetic Resonance Imaging Infarct Prediction in Acute Stroke. Stroke 2018, 49, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.H.; Yu, M. Cox regression analysis with missing covariates via nonparametric multiple imputation. Stat. Methods Med. Res. 2019, 28, 1676–1688. [Google Scholar] [CrossRef] [PubMed]
- Leroux, A.; Di, J.; Smirnova, E.; McGuffey, E.J.; Cao, Q.; Bayatmokhtari, E.; Tabacu, L.; Zipunnikov, V.; Urbanek, J.K.; Crainiceanu, C. Organizing and analyzing the activity data in NHANES. Stat. Biosci. 2019, 11, 262–287. [Google Scholar] [CrossRef] [PubMed]
- Van Hemelrijck, M.; Garmo, H.; Holmberg, L.; Walldius, G.; Jungner, I.; Hammar, N.; Lambe, M. Prostate cancer risk in the Swedish AMORIS study: The interplay among triglycerides, total cholesterol, and glucose. Cancer 2011, 117, 2086–2095. [Google Scholar] [CrossRef]
- Mondul, A.M.; Clipp, S.L.; Helzlsouer, K.J.; Platz, E.A. Association between plasma total cholesterol concentration and incident prostate cancer in the CLUE II cohort. Cancer Causes Control 2010, 21, 61–68. [Google Scholar] [CrossRef] [Green Version]
- Platz, E.A.; Till, C.; Goodman, P.J.; Parnes, H.L.; Figg, W.D.; Albanes, D.; Neuhouser, M.L.; Klein, E.A.; Thompson, I.M., Jr.; Kristal, A.R. Men with low serum cholesterol have a lower risk of high-grade prostate cancer in the placebo arm of the prostate cancer prevention trial. Cancer Epidemiol. Prev. Biomark. 2009, 18, 2807–2813. [Google Scholar] [CrossRef] [Green Version]
- Morote, J.; Celma, A.; Planas, J.; Placer, J.; de Torres, I.; Olivan, M.; Carles, J.; Reventós, J.; Doll, A. Role of serum cholesterol and statin use in the risk of prostate cancer detection and tumor aggressiveness. Int. J. Mol. Sci. 2014, 15, 13615–13623. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, E.J.; Stevens, V.L.; Newton, C.C.; Gapstur, S.M. Plasma total, LDL, and HDL cholesterol and risk of aggressive prostate cancer in the Cancer Prevention Study II Nutrition Cohort. Cancer Causes Control 2012, 23, 1289–1296. [Google Scholar] [CrossRef]
- Liu, M.; Wang, J.Y.; Zhu, L.; Wan, G. Body mass index and serum lipid profile influence serum prostate-specific antigen in Chinese men younger than 50 years of age. Asian J. Androl. 2011, 13, 640–643. [Google Scholar] [CrossRef] [Green Version]
- McCubrey, J.A.; Steelman, L.S.; Chappell, W.H.; Abrams, S.L.; Wong, E.W.; Chang, F.; Lehmann, B.; Terrian, D.M.; Milella, M.; Tafuri, A.; et al. Roles of the Raf/MEK/ERK pathway in cell growth, malignant transformation and drug resistance. Biochim. Biophys. Acta 2007, 1773, 1263–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sekine, Y.; Koike, H.; Nakano, T.; Nakajima, K.; Takahashi, S.; Suzuki, K. Remnant lipoproteins induced proliferation of human prostate cancer cell, PC-3 but not LNCaP, via low density lipoprotein receptor. Cancer Epidemiol. 2009, 33, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Sekine, Y.; Koike, H.; Nakano, T.; Nakajima, K.; Suzuki, K. Remnant lipoproteins stimulate proliferation and activate MAPK and Akt signaling pathways via G protein-coupled receptor in PC-3 prostate cancer cells. Clin. Chim. Acta Int. J. Clin. Chem. 2007, 383, 78–84. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Triglycerides (mg/dL) | Q1 | Q2 | Q3 | Q4 | p-Value |
|---|---|---|---|---|---|
| N | 718 | 719 | 744 | 729 | |
| PSA ng/ml | 1.56 ± 2.60 | 1.74 ± 3.11 | 1.40 ± 1.86 | 1.30 ± 1.62 | 0.0023 |
| Sociodemographic variables | |||||
| Age, mean ± SD (years) | 56.16 ± 11.94 | 55.84 ± 11.31 | 56.46 ± 11.36 | 54.48 ± 10.70 | 0.0041 |
| Poverty to income ratio, mean ± SD (years) | 3.31 ± 1.57 | 3.40 ± 1.55 | 3.32 ± 1.56 | 3.30 ± 1.61 | 0.6691 |
| Race/ethnicity (%) | <0.0001 | ||||
| Mexican American | 3.91 | 5.39 | 6.57 | 8.30 | |
| Other Hispanic | 2.47 | 2.69 | 3.72 | 4.16 | |
| Non-Hispanic White | 76.52 | 75.82 | 78.13 | 75.67 | |
| Non-Hispanic Black | 13.07 | 10.12 | 5.56 | 5.38 | |
| Other race/ethnicity | 4.02 | 5.98 | 6.02 | 6.50 | |
| Education (%) | 0.0335 | ||||
| Less than high school | 19.27 | 16.60 | 21.00 | 20.20 | |
| High school | 22.65 | 23.99 | 22.76 | 27.83 | |
| More than high school | 58.08 | 59.41 | 56.24 | 51.97 | |
| Marital status (%) | 0.2121 | ||||
| Married | 71.14 | 75.20 | 69.96 | 73.24 | |
| Single | 24.19 | 19.50 | 25.35 | 21.98 | |
| Living with a partner | 4.67 | 5.30 | 4.69 | 4.77 | |
| Variables of laboratory data | |||||
| VITD, mean ± SD (ng/mL) | 68.95 ± 21.51 | 60.86 ± 19.91 | 64.92 ± 19.99 | 60.63 ± 19.22 | <0.0001 |
| LDL-C, mean ± SD (mg/dL) | 112.74 ± 32.98 | 121.48 ± 31.45 | 123.05 ± 36.68 | 119.55 ± 36.91 | <0.0001 |
| HDL-C, mean ± SD (mg/dL) | 58.95 ± 15.70 | 51.76 ± 13.34 | 45.75 ± 9.90 | 40.82 ± 9.75 | <0.0001 |
| Glycohemoglobin (%) | 5.59 ± 0.80 | 5.68 ± 0.87 | 5.70 ± 0.89 | 5.90 ± 1.27 | <0.0001 |
| C-reactive protein, mean ± SD (mg/dL) | 0.37 ± 0.97 | 0.38 ± 1.07 | 0.47 ± 1.36 | 0.35 ± 0.40 | 0.0743 |
| Medical examination and personal life history | |||||
| Physical activity (MET-based rank) (%) | |||||
| Sits | 0.0013 | ||||
| Walks | 21.14 | 18.46 | 25.42 | 19.91 | |
| Light loads | 41.71 | 50.94 | 50.31 | 51.50 | |
| Heavy work | 22.80 | 24.21 | 15.82 | 20.17 | |
| Body mass index, mean ± SD (Kg/m2) | 14.35 | 6.40 | 8.45 | 8.41 | |
| Smoked at least 100 cigarettes in life | 27.38 ± 5.39 | 28.46 ± 6.47 | 29.58 ± 5.59 | 30.60 ± 5.17 | <0.0001 |
| Yes | 0.0253 | ||||
| No | 54.13 | 58.29 | 59.17 | 61.96 | |
| Dietary interview-individual foods | 45.87 | 41.71 | 40.83 | 38.04 | |
| Alcohol, mean ± SD (gm) | |||||
| Comorbidities (%) | 19.45 ± 36.73 | 14.22 ± 34.31 | 13.77 ± 29.79 | 15.30 ± 34.20 | 0.0079 |
| Hypertension history | |||||
| Yes | 0.0245 | ||||
| No | 35.25 | 36.41 | 46.94 | 46.49 | |
| Coronary heart disease | 64.75 | 63.59 | 53.06 | 53.51 | |
| Yes | 0.1771 | ||||
| No | 8.08 | 6.56 | 9.71 | 7.97 | |
| Diabetes history | 91.92 | 93.44 | 90.29 | 92.03 | |
| Yes | 0.0629 | ||||
| No | 9.35 | 11.41 | 13.16 | 13.39 | |
| Borderline | 88.81 | 86.27 | 84.55 | 83.16 | |
| Stroke | 1.84 | 2.31 | 2.29 | 3.45 | |
| Yes | 0.4934 | ||||
| No | 2.86 | 3.49 | 4.22 | 4.12 | |
| 97.14 | 96.51 | 95.78 | 95.88 |
| Exposure | Non-Adjusted Model | Minimally Adjusted Model | Fully Adjusted Model |
|---|---|---|---|
| Triglyceride | −0.0014 (−0.0023, −0.0005), 0.001309 | −0.0013 (−0.0022, −0.0004), 0.003832 | −0.0043 (−0.0082, −0.0005), 0.027856 |
| Triglyceride | |||
| Q1 Q2 Q3 Q4 | Ref 0.1045 (−0.2349,0.4439), 0.546189 −0.3022 (−0.6387,0.0343), 0.078467 −0.4598 (−0.7980, −0.1216) 0.007755 | Ref 0.0684 (−0.2852, 0.4220) 0.704653 −0.2621 (−0.6169, 0.0927) 0.147739 −0.4501 (−0.8093, −0.0909) 0.014117 | Ref 0.2846 (−0.3559, 0.9250) 0.384057 −0.4040 (−1.0497, 0.2416) 0.220247 −0.5155 (−1.2396, 0.2085) 0.163151 |
| p for trend | <0.001 | 0.002 | 0.049 |
| Triglycerides (mg/dL) | N | β | 95% CI | p-Value | p for Interaction |
|---|---|---|---|---|---|
| Stratified by age | <0.0001 | ||||
| <60 | 1475 | −0.0012 | (−0.0028, 0.0003) | 0.1241 | |
| 60–80 | 1153 | −0.0038 | (−0.0090, 0.0014) | 0.1557 | |
| >80 | 282 | −0.0225 | (−0.0472, 0.0023) | 0.078 | |
| Stratified by race | 0.3315 | ||||
| Mexican American | 496 | −0.0012 | (−0.0054, 0.0031) | 0.5987 | |
| Other Hispanic | 213 | 0.0017 | (−0.0061, 0.0094) | 0.678 | |
| Non-Hispanic White | 1585 | −0.006 | (−0.0100, −0.0020) | 0.0036 | |
| Non-Hispanic Black | 498 | −0.0125 | (−0.0281, 0.0031) | 0.1184 | |
| Other race/ethnicity | 118 | −0.0092 | (−0.0228, 0.0044) | 0.1946 | |
| Stratified by education | 0.1640 | ||||
| Less than high school | 935 | −0.0082 | (−0.0173, 0.0009) | 0.0791 | |
| High school | 669 | −0.0055 | (−0.0124, 0.0014) | 0.1168 | |
| More than high school | 1306 | −0.0059 | (−0.0094, −0.0024) | 0.0012 | |
| Stratified by marital status | 0.8274 | ||||
| Married | 1981 | −0.0073 | (−0.0113, −0.0033) | 0.0004 | |
| Single | 789 | −0.0038 | (−0.0123, 0.0047) | 0.3763 | |
| Living with a partner | 136 | −0.0064 | (−0.0126, −0.0001) | 0.0527 | |
| Stratified by BMI | 0.1168 | ||||
| <25 | 710 | −0.0092 | (−0.0184, −0.0000) | 0.0504 | |
| 25–28 | 718 | −0.0052 | (−0.0172, 0.0068) | 0.3964 | |
| >28 | 1424 | −0.0029 | (−0.0056, −0.0003) | 0.0305 | |
| Stratified by ratio of family income | 0.5872 | ||||
| Low group | 896 | −0.0038 | (−0.0081, 0.0005) | 0.0873 | |
| Median group | 898 | −0.0066 | (−0.0157, 0.0026) | 0.1594 | |
| High group | 906 | −0.0093 | (−0.0142, −0.0044) | 0.0002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, C.; Tian, L.; Jia, B.; Wang, M.; Xiong, M.; Hu, B.; Deng, C.; Hou, Y.; Hou, T.; Yang, X.; et al. Association between Serum Triglycerides and Prostate Specific Antigen (PSA) among U.S. Males: National Health and Nutrition Examination Survey (NHANES), 2003–2010. Nutrients 2022, 14, 1325. https://doi.org/10.3390/nu14071325
Wei C, Tian L, Jia B, Wang M, Xiong M, Hu B, Deng C, Hou Y, Hou T, Yang X, et al. Association between Serum Triglycerides and Prostate Specific Antigen (PSA) among U.S. Males: National Health and Nutrition Examination Survey (NHANES), 2003–2010. Nutrients. 2022; 14(7):1325. https://doi.org/10.3390/nu14071325
Chicago/Turabian StyleWei, Chengcheng, Liang Tian, Bo Jia, Miao Wang, Ming Xiong, Bo Hu, Changqi Deng, Yaxin Hou, Teng Hou, Xiong Yang, and et al. 2022. "Association between Serum Triglycerides and Prostate Specific Antigen (PSA) among U.S. Males: National Health and Nutrition Examination Survey (NHANES), 2003–2010" Nutrients 14, no. 7: 1325. https://doi.org/10.3390/nu14071325