
Loco-Regional Therapies in Oligometastatic Adrenocortical Carcinoma

 , ,
, ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
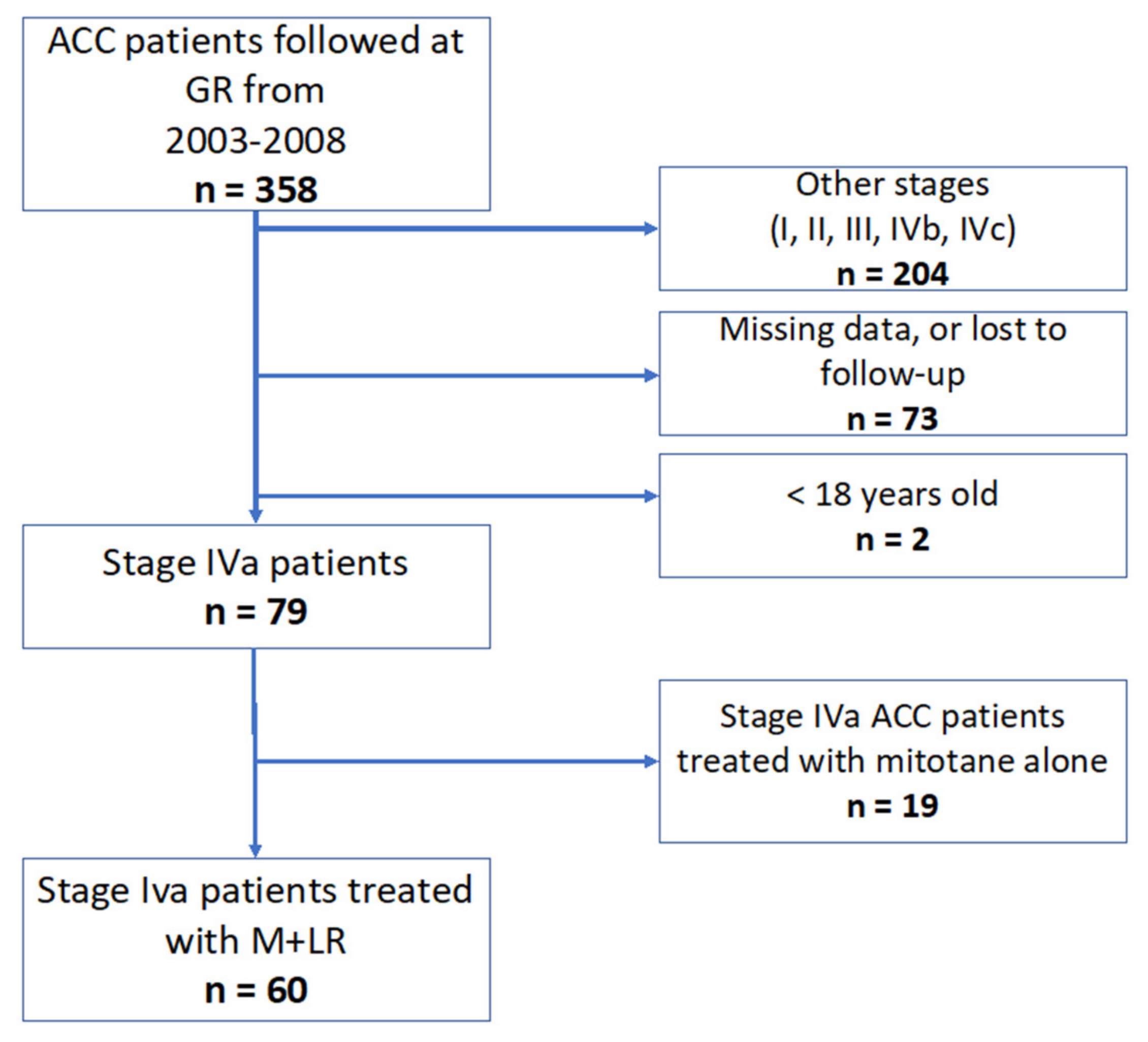
2.1. Patients and ACC Characteristics
2.2. Treatments and Complications
2.3. Best Response to Treatments and Follow-Up
2.4. TTC and OS
2.5. Statistical Analysis
3. Results
3.1. Patients Characteristics
3.2. Treatments and Complications
3.3. Best Response to Treatments and Follow-Up
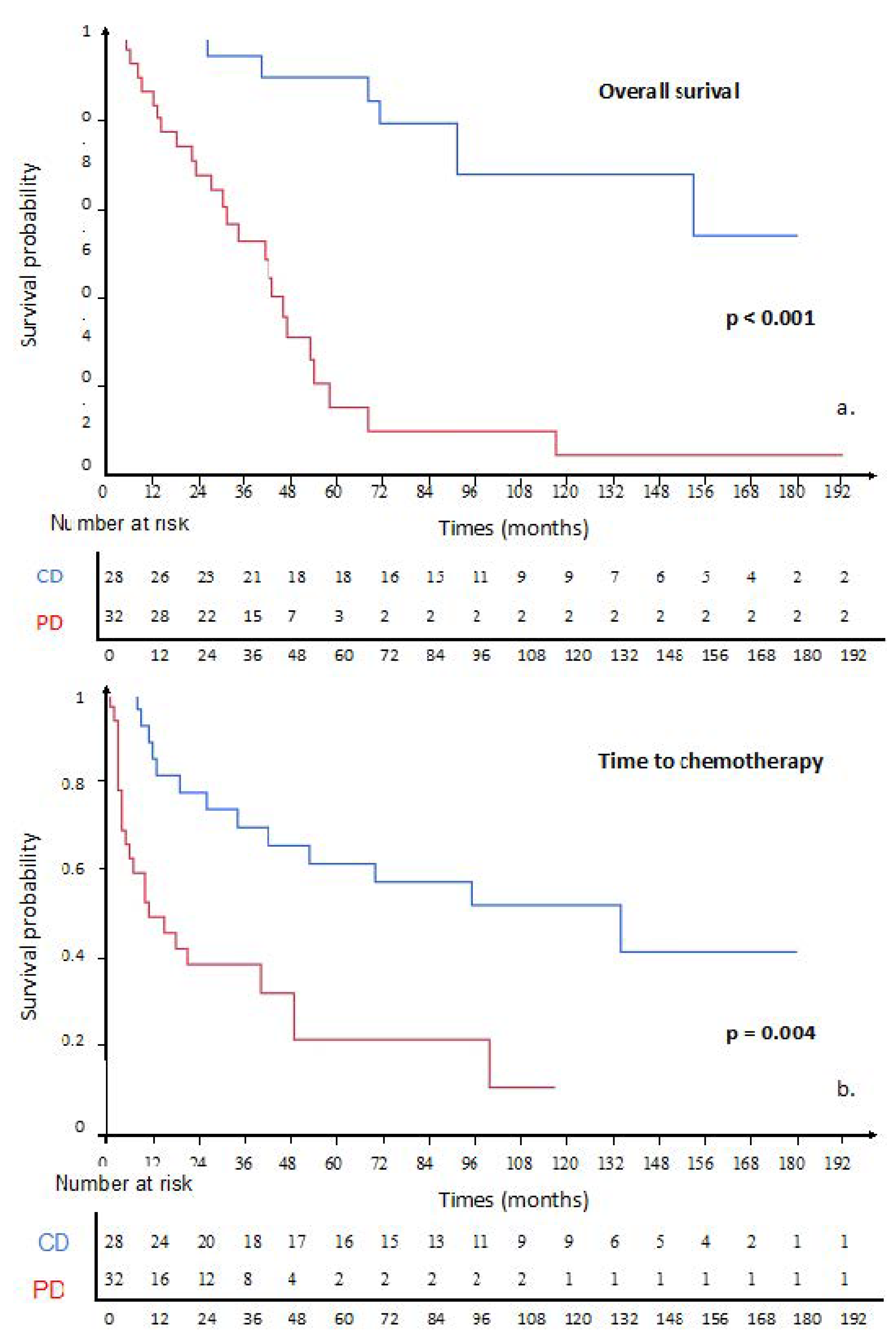
3.4. TTC and OS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACC | adrenocortical carcinoma |
| CHE | chemoembolization |
| CTCAE | common terminology criteria for adverse events |
| CT | computed tomography |
| DC | disease control |
| DFI | disease-free interval |
| ENSAT | European Network for the Study of Adrenal Tumors |
| GRAS | grade, R status, age, and symptoms |
| LR | local treatment |
| OS | overall survival |
| TTC | time to chemotherapy |
| RT | radiotherapy |
References
- Golden, S.H.; Robinson, K.A.; Saldanha, I.; Anton, B.; Ladenson, P.W. Prevalence and Incidence of Endocrine and Metabolic Disorders in the United States: A Comprehensive Review. J. Clin. Endocrinol. Metab. 2009, 94, 1853–1878. [Google Scholar] [CrossRef] [PubMed]
- Kerkhofs, T.M.A.; Verhoeven, R.H.A.; Van der Zwan, J.M.; Dieleman, J.; Kerstens, M.N.; Links, T.P.; Van de Poll-Franse, L.V.; Haak, H.R. Adrenocortical carcinoma: A population-based study on incidence and survival in The Netherlands since 1993. Eur. J. Cancer 2013, 49, 2579–2586. [Google Scholar] [CrossRef] [PubMed]
- Libé, R.; Borget, I.; Ronchi, C.L.; Zaggia, B.; Kroiss, M.; Kerkhofs, T.; Bertherat, J.; Volante, M.; Quinkler, M.; Chabre, O.; et al. Prognostic factors in stage III–IV adrenocortical carcinomas (ACC): An European Network for the Study of Adrenal Tumor (ENSAT) study. Ann. Oncol. 2015, 26, 2119–2125. [Google Scholar] [CrossRef] [PubMed]
- Lughezzani, G.; Sun, M.; Perrotte, P.; Jeldres, C.; Alasker, A.; Isbarn, H.; Budäus, L.; Shariat, S.F.; Guazzoni, G.; Montorsi, F.; et al. The European Network for the Study of Adrenal Tumors staging system is prognostically superior to the international union against cancer-staging system: A North American validation. Eur. J. Cancer 2010, 46, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Bilimoria, K.Y.; Shen, W.T.; Elaraj, D.; Bentrem, D.J.; Winchester, D.J.; Kebebew, E.; Sturgeon, C. Adrenocortical carcinoma in the United States: Treatment utilization and prognostic factors. Cancer 2008, 113, 3130–3136. [Google Scholar] [CrossRef] [PubMed]
- Fassnacht, M.; Assie, G.; Baudin, E.; Eisenhofer, G.; de la Fouchardiere, C.; Haak, H.R.; de Krijger, R.; Porpiglia, F.; Terzolo, M.; Berruti, A. Adrenocortical carcinomas and malignant phaeochromocytomas: ESMO–EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1476–1490. [Google Scholar] [CrossRef] [PubMed]
- Schulick, R.D.; Brennan, M.F. Long-term survival after complete resection and repeat resection in patients with adrenocortical carcinoma. Ann. Surg. Oncol. 1999, 6, 719–726. [Google Scholar] [CrossRef]
- Erdogan, I.; Deutschbein, T.; Jurowich, C.; Kroiss, M.; Ronchi, C.; Quinkler, M.; Waldmann, J.; Willenberg, H.S.; Beuschlein, F.; Fottner, C.; et al. The Role of Surgery in the Management of Recurrent Adrenocortical Carcinoma. J. Clin. Endocrinol. Metab. 2013, 98, 181–191. [Google Scholar] [CrossRef] [Green Version]
- For Comete-Cancer Network; Vezzosi, D.; Do Cao, C.; Hescot, S.; Bertherat, J.; Haissaguerre, M.; Bongard, V.; Drui, D.; De La Fouchardière, C.; Illouz, F.; et al. Time Until Partial Response in Metastatic Adrenocortical Carcinoma Long-Term Survivors. Horm. Cancer 2018, 9, 62–69. [Google Scholar] [CrossRef]
- Tran, T.B.; Postlewait, L.M.; Maithel, S.K.; Prescott, J.D.; Wang, T.S.; Glenn, J.; Phay, J.E.; Keplinger, K.; Fields, R.C.; Jin, L.X.; et al. Actual 10-year survivors following resection of adrenocortical carcinoma: Adrenocortical Carcinoma Survivors. J. Surg. Oncol. 2016, 114, 971–976. [Google Scholar] [CrossRef] [Green Version]
- Wängberg, B.; Khorram-Manesh, A.; Jansson, S.; Nilsson, B.; Nilsson, O.; Jakobsson, C.E.; Lindstedt, S.; Odén, A.; Ahlman, H. The long-term survival in adrenocortical carcinoma with active surgical management and use of monitored mitotane. Endocr. Relat. Cancer 2010, 17, 265–272. [Google Scholar] [CrossRef] [Green Version]
- Bellantone, R.; Ferrante, A.; Boscherini, M.; Lombardi, C.P.; Crucitti, P.; Crucitti, F.; Favia, G.; Borrelli, D.; Boffi, L.; Capussotti, L.; et al. Role of reoperation in recurrence of adrenal cortical carcinoma: Results from 188 cases collected in the Italian National Registry for Adrenal Cortical Carcinoma. Surgery 1997, 122, 1212–1218. [Google Scholar] [CrossRef]
- Gonzalez, R.J.; Tamm, E.P.; Ng, C.; Phan, A.T.; Vassilopoulou-Sellin, R.; Perrier, N.D.; Evans, D.B.; Lee, J.E. Response to mitotane predicts outcome in patients with recurrent adrenal cortical carcinoma. Surgery 2007, 142, 867–875, discussion 867–875. [Google Scholar] [CrossRef]
- Boileve, A.; Mathy, E.; Roux, C.; Faron, M.; Hadoux, J.; Tselikas, L.; Al Ghuzlan, A.; Hescot, S.; Leboulleux, S.; de Baere, T.; et al. Combination of mitotane and locoregional treatments in low-volume metastatic adrenocortical carcinoma. J. Clin. Endocrinol. Metab. 2021, 106, e4698–e4707. [Google Scholar] [CrossRef]
- Fassnacht, M.; Dekkers, O.M.; Else, T.; Baudin, E.; Berruti, A.; de Krijger, R.R.; Haak, H.R.; Mihai, R.; Assie, G.; Terzolo, M. European Society of Endocrinology Clinical Practice Guidelines on the management of adrenocortical carcinoma in adults, in collaboration with the European Network for the Study of Adrenal Tumors. Eur. J. Endocrinol. 2018, 179, G1–G46. [Google Scholar] [CrossRef]
- De Baère, T.; Aupérin, A.; Deschamps, F.; Chevallier, P.; Gaubert, Y.; Boige, V.; Fonck, M.; Escudier, B.; Palussiére, J. Radiofrequency ablation is a valid treatment option for lung metastases: Experience in 566 patients with 1037 metastases. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2015, 26, 987–991. [Google Scholar] [CrossRef]
- Cazejust, J.; De Baère, T.; Auperin, A.; Deschamps, F.; Hechelhammer, L.; Abdel-Rehim, M.; Schlumberger, M.; Leboulleux, S.; Baudin, E. Transcatheter Arterial Chemoembolization for Liver Metastases in Patients with Adrenocortical Carcinoma. J. Vasc. Interv. Radiol. 2010, 21, 1527–1532. [Google Scholar] [CrossRef]
- Cardella, J.F.; Kundu, S.; Miller, D.L.; Millward, S.F.; Sacks, D. Society of Interventional Radiology Society of Interventional Radiology clinical practice guidelines. J. Vasc. Interv. Radiol. JVIR 2009, 20 (Suppl. S7), S189–S191. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Hescot, S.; Seck, A.; Guerin, M.; Cockenpot, F.; Huby, T.; Broutin, S.; Young, J.; Paci, A.; Baudin, E.; Lombès, M. Lipoprotein-Free Mitotane Exerts High Cytotoxic Activity in Adrenocortical Carcinoma. J. Clin. Endocrinol. Metab. 2015, 100, 2890–2898. [Google Scholar] [CrossRef] [Green Version]
- Kroiss, M.; Quinkler, M.; Lutz, W.K.; Allolio, B.; Fassnacht, M. Drug interactions with mitotane by induction of CYP3A4 metabolism in the clinical management of adrenocortical carcinoma: CYP3A4 induction by mitotane. Clin. Endocrinol. 2011, 75, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Puglisi, S.; Calabrese, A.; Basile, V.; Pia, A.; Reimondo, G.; Perotti, P.; Terzolo, M. New perspectives for mitotane treatment of adrenocortical carcinoma. Best Pract. Res. Clin. Endocrinol. Metab. 2020, 34, 101415. [Google Scholar] [CrossRef] [PubMed]
- Veltri, A.; Basile, D.; Calandri, M.; Bertaggia, C.; Volante, M.; Porpiglia, F.; Calabrese, A.; Puglisi, S.; Basile, V.; Terzolo, M. Oligometastatic adrenocortical carcinoma: The role of image-guided thermal ablation. Eur. Radiol. 2020, 30, 6958–6964. [Google Scholar] [CrossRef] [PubMed]
- Bukowski, R.M.; Wolfe, M.; Levine, H.S.; Crawford, D.E.; Stephens, R.L.; Gaynor, E.; Harker, W.G. Phase II trial of mitotane and cisplatin in patients with adrenal carcinoma: A Southwest Oncology Group study. J. Clin. Oncol. 1993, 11, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Malandrino, P.; Al Ghuzlan, A.; Castaing, M.; Young, J.; Caillou, B.; Travagli, J.-P.; Elias, D.; de Baere, T.; Dromain, C.; Paci, A.; et al. Prognostic markers of survival after combined mitotane- and platinum-based chemotherapy in metastatic adrenocortical carcinoma. Endocr. Relat. Cancer 2010, 17, 797–807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berruti, A.; Grisanti, S.; Pulzer, A.; Claps, M.; Daffara, F.; Loli, P.; Mannelli, M.; Boscaro, M.; Arvat, E.; Tiberio, G.; et al. Long-Term Outcomes of Adjuvant Mitotane Therapy in Patients with Radically Resected Adrenocortical Carcinoma. J. Clin. Endocrinol. Metab. 2017, 102, 1358–1365. [Google Scholar] [CrossRef] [PubMed]
- Hellman, S.; Weichselbaum, R.R. Oligometastases. J. Clin. Oncol. 1995, 13, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Guckenberger, M.; Lievens, Y.; Bouma, A.B.; Collette, L.; Dekker, A.; deSouza, N.M.; Dingemans, A.-M.C.; Fournier, B.; Hurkmans, C.; Lecouvet, F.E.; et al. Characterisation and classification of oligometastatic disease: A European Society for Radiotherapy and Oncology and European Organisation for Research and Treatment of Cancer consensus recommendation. Lancet Oncol. 2020, 21, e18–e28. [Google Scholar] [CrossRef] [Green Version]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 2830–2838. [Google Scholar] [CrossRef]
- Ost, P.; Reynders, D.; Decaestecker, K.; Fonteyne, V.; Lumen, N.; De Bruycker, A.; Lambert, B.; Delrue, L.; Bultijnck, R.; Claeys, T.; et al. Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. J. Clin. Oncol. 2018, 36, 446–453. [Google Scholar] [CrossRef] [Green Version]
- Ruers, T.; Van Coevorden, F.; Punt, C.J.A.; Pierie, J.-P.E.N.; Borel-Rinkes, I.; Ledermann, J.A.; Poston, G.; Bechstein, W.; Lentz, M.-A.; Mauer, M.; et al. Local Treatment of Unresectable Colorectal Liver Metastases: Results of a Randomized Phase II Trial. JNCI J. Natl. Cancer Inst. 2017, 109, djx015. [Google Scholar] [CrossRef]
- Huang, A.C.; Postow, M.A.; Orlowski, R.J.; Mick, R.; Bengsch, B.; Manne, S.; Xu, W.; Harmon, S.; Giles, J.R.; Wenz, B.; et al. T-cell invigoration to tumour burden ratio associated with anti-PD-1 response. Nature 2017, 545, 60–65. [Google Scholar] [CrossRef] [Green Version]
- Oppel, F.; Görner, M.; Sudhoff, H. The Potential of Tumor Debulking to Support Molecular Targeted Therapies. Front. Oncol. 2020, 10, 801. [Google Scholar] [CrossRef]
- Conibear, J.; Chia, B.; Ngai, Y.; Bates, A.T.; Counsell, N.; Patel, R.; Eaton, D.; Faivre-Finn, C.; Fenwick, J.; Forster, M.; et al. Study protocol for the SARON trial: A multicentre, randomised controlled phase III trial comparing the addition of stereotactic ablative radiotherapy and radical radiotherapy with standard chemotherapy alone for oligometastatic non-small cell lung cancer. BMJ Open 2018, 8, e020690. [Google Scholar] [CrossRef]
- Früh, M.; De Ruysscher, D.; Popat, S.; Crinò, L.; Peters, S.; Felip, E. Small-cell lung cancer (SCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24, vi99–vi105. [Google Scholar] [CrossRef]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; et al. Non-Small Cell Lung Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. JNCCN 2022, 20, 497–530. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Patients |
|---|---|
| Patients charactristics | n = 60 |
| Age at stade IV diagnosis (year, IQR) | 48.1 (38.3–59.8) |
| <50 | 34 (57%) |
| ≥50 | 26 (43%) |
| Gender | |
| Male | 26 (43%) |
| Female | 34 (57%) |
| Tumor characteristics | |
| Tumor related symptoms | |
| Y | 43 (72%) |
| N | 10 (16%) |
| Unknown | 1 (2%) |
| R status in resected patients | |
| R0 | 22 (37%) |
| R1 | 7 (12%) |
| R2 | 0 (0%) |
| Rx | 31 (52%) |
| Weiss score | |
| ≤6 | 39 (68%) |
| >6 | 11 (32%) |
| Ki67% | |
| <20% | 18 (34%) |
| ≥20% | 18 (25%) |
| Unknown | 24 (41%) |
| Metastases (IVA) | |
| DFI | |
| Median time (months, IQR) | 9.3 (0.8–22.0) |
| synchronous | 21 (38%) |
| metachronous | 37 (62%) |
| Lung | |
| Y | 36 (60%) |
| N | 24 (40%) |
| Liver | |
| Y | 28 (47%) |
| N | 32 (53%) |
| Nodes | |
| Y | 8 (13%) |
| N | 52 (87%) |
| Bone | |
| Y | 4 (7%) |
| N | 56 (93%) |
| Peritoneum | |
| Y | 7 (12%) |
| N | 53 (88%) |
| Local relapse | |
| Y | 21 (35%) |
| N | 39 (65%) |
| Oligometastasis | |
| Y | 35 (58%) |
| N | 25 (42%) |
| High tumor burden | |
| Y | 37 (62%) |
| N | 23 (38%) |
| Metastatic organs | |
| n = 1 | 41 (68%) |
| n > 1 | 19 (32) |
| Parameters | n (60) of Patients (%) |
|---|---|
| Treatments | |
| Adrenal space radiotherapy | 14 (23%) |
| Second surgery | 34 (57%) |
| Locoregional | 25 (42%) |
| Hepatic | 9 (15%) |
| Pulmonary | 8 (13%) |
| Other | 3 (5%) |
| Interventional radiology | 35 (58%) |
| Cryotherapy | 7 (12%) |
| Radiofrequency | 18 (20%) |
| Microwaves | 5 (8%) |
| Chemoembolization | 20 (33%) |
| Outcomes | |
| Median follow-up (months) | 104 (40–164) |
| Chemotherapy | |
| Within 6 month | 8 (13%) |
| Overall | 35 (58%) |
| Survival | |
| 5-year OS | 36 (60%) |
| Median OS (months) | 68 (43–117) |
| Death | |
| Y | 31 (52%) |
| N | 22 (36%) |
| Lost to follow-up | 7 (11%) |
| Parameters | Patients with PD | Patients with CD | p |
|---|---|---|---|
| Patients | n = 20 | n = 40 | |
| Age at stade IV diagnosis (year, IQR) | 43.5 (31.7–59.2) | 48.5 (39.3–61.2) | 0.29 |
| <50 | 11 (55%) | 23 (57.5%) | |
| ≥50 | 9 (45%) | 17 (42.5%) | |
| Gender | |||
| Male | 7 (35%) | 19 (47.5%) | 0.41 |
| Female | 13 (65%) | 21 (52.5%) | |
| GRAS parameters | >0.9 | ||
| <1 | 2 (10%) | 3 (7.5%) | |
| ≥1 | 18 (90%) | 37 (92.5%) | |
| DFI | |||
| Median time (months, IQR) | 9.0 (2.3–24.6) | 11.5 (7–20.8) | 0.68 |
| Synchronous | 7 (35%) | 16 (40%) | |
| Metachronous | 13 (65%) | 24 (60%) | |
| Metastases (IVa) | |||
| Lung | 0.46 | ||
| Y | 13 (65%) | 23 (57.5%) | |
| N | 7 (35%) | 17 (43.5%) | |
| Liver | 0.41 | ||
| Y | 11 (55%) | 17 (42.5%) | |
| N | 9 (45%) | 23 (57.5%) | |
| Nodes | 0.70 | ||
| Y | 2 (10%) | 6 (15%) | |
| N | 18 (90%) | 34 (85%) | |
| Bone | >0.9 | ||
| Y | 1 (5%) | 3 (7.5%) | |
| N | 19 (95%) | 37 (92.5%) | |
| Peritoneum | 0.40 | ||
| Y | 1 (5%) | 6 (15%) | |
| N | 19 (95%) | 34 (85%) | |
| Local relapse | 0.58 | ||
| Y | 8 (40%) | 13 (32.5%) | |
| N | 12 (60%) | 27 (67.5%) | |
| Oligometastasis | |||
| Y | 6 (30%) | 29 (72.5%) | 0.002 * |
| N | 14 (70%) | 11 (27.5%) | |
| Dmax > 3 cm | |||
| Y | 3 (15%) | 20 (50%) | 0.011 * |
| N | 17 (85%) | 20 (50%) | |
| Metastatic organ | |||
| n = 1 | 11 (55%) | 30 (75%) | 0.150 |
| n > 1 | 9 (45%) | 10 (25%) |
| Parameters | Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|---|
| OS | Total (n = 60) | Hazard ratio | 95% CI | p-value | Hazard ratio | 95% CI | p-value |
| Sex | |||||||
| Female | 34 | 0.89 | 0.43–1.79 | 0.730 | - | - | - |
| Male | 26 | 1 | - | - | - | - | - |
| GRAS factor | |||||||
| n = 0 | 5 | 0.25 | 0.03–1.80 | 0.080 | - | - | - |
| n > 0 | 55 | 1 | - | - | - | - | - |
| Metastatic organ | |||||||
| n = 1 | 41 | 0.30 | 0.13–0.64 | 0.003 * | 0.31 | 0.14–0.69 | 0.005 * |
| n > 1 | 19 | 1 | - | - | 1 | - | - |
| Oligometastatic | |||||||
| Yes | 25 | 0.37 | 0.18–0.77 | 0.008 * | 0.40 | 0.19–0.82 | 0.014 * |
| No | 35 | 1 | - | - | 1 | - | - |
| Dmax < 3 cm | |||||||
| Yes | 37 | 0.49 | 0.22–1.04 | 0.055 | - | - | - |
| No | 23 | 1 | - | - | - | - | - |
| DFI | |||||||
| synchronous | 23 | 0.86 | 0.39–1.73 | 0.610 | - | - | - |
| metachronous | 37 | 1 | - | - | - | - | - |
| TTC | |||||||
| Sex | |||||||
| Female | 1.20 | 0.60–2.37 | 0.600 | - | - | - | |
| Male | 1 | - | - | - | - | - | |
| GRAS factor | |||||||
| n = 0 | 5 | 0.90 | 0.27–2.97 | 0.870 | - | - | - |
| n > 0 | 55 | 1 | - | - | - | - | - |
| Metastatic organ | |||||||
| n = 1 | 41 | 0.50 | 0.24–1.03 | 0.072 | - | - | - |
| n > 1 | 19 | 1 | - | - | - | - | - |
| Oligometastatic | |||||||
| Yes | 25 | 0.35 | 0.18–0.68 | 0.002 * | 0.32 | 0.16–0.64 | 0.001 * |
| No | 35 | 1 | - | - | 1 | - | - |
| Dmax < 3 cm | |||||||
| Yes | 0.47 | 0.22–0.99 | 0.039 * | 0.41 | 0.19–0.89 | 0.024 * | |
| No | 1 | - | - | 1 | - | - | |
| DFI | |||||||
| synchronous | 23 | 0.68 | 0.35 - 1.3 | 0.270 | - | - | - |
| metachronous | 37 | 1 | - | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roux, C.; Boileve, A.; Faron, M.; Lamartina, L.; Delpla, A.; Tselikas, L.; Durand-Labrunie, J.; Hescot, S.; de Baere, T.; Hadoux, J.; et al. Loco-Regional Therapies in Oligometastatic Adrenocortical Carcinoma. Cancers 2022, 14, 2730. https://doi.org/10.3390/cancers14112730
Roux C, Boileve A, Faron M, Lamartina L, Delpla A, Tselikas L, Durand-Labrunie J, Hescot S, de Baere T, Hadoux J, et al. Loco-Regional Therapies in Oligometastatic Adrenocortical Carcinoma. Cancers. 2022; 14(11):2730. https://doi.org/10.3390/cancers14112730
Chicago/Turabian StyleRoux, Charles, Alice Boileve, Matthieu Faron, Livia Lamartina, Alexandre Delpla, Lambros Tselikas, Jérome Durand-Labrunie, Segolène Hescot, Thierry de Baere, Julien Hadoux, and et al. 2022. "Loco-Regional Therapies in Oligometastatic Adrenocortical Carcinoma" Cancers 14, no. 11: 2730. https://doi.org/10.3390/cancers14112730