1. Introduction
Renal Cell Carcinoma (RCC) has the highest mortality rates of all genitourinary malignancies, and its prevalence has been gradually increasing [
1,
2,
3]. In recent years, there has been an upsurge in the number of cases of RCC all over the world [
4,
5,
6,
7,
8]. RCC incidences have continuously increased by 2–4% per year, and RCC is now the seventh most common cancer type in the United States [
9]. According to Sung et al. [
10], kidney cancer was mainly accountable for 431,288 clinically diagnosed cases and 179,368 deaths in 2020 globally. In the UK alone, kidney cancers accounted for 4% of all cancer occurrences between 2016 and 2018. Twelve deaths were reported daily in 2017 in the UK [
11] and RCC contributed immensely to these statistics, as it is responsible for more than 90% of kidney cancers [
12].
Renal tumors are quite diverse, having at least 16 distinct subtypes [
13], out of which chromophobe renal cell carcinoma (ChRCC) and renal oncocytomas (RO) are very similar to each other. ChRCC is responsible for at least 5% of the diagnosed malignant renal tumors each year [
14,
15]. In contrast, RO accounts for 3–7% of all benign renal tumor diagnoses [
16]. RO was initially characterized by Zippel in 1942 [
17,
18], whereas ChRCCs were first described by Theones et al. in 1985 [
19,
20]. Because ChRCCs were described four decades later than ROs, many renal tumors that were suspected to be ChRCCs were characterized as ROs throughout that period [
13]. Nestled pattern, myxoid stroma, granular cytoplasm, and round nuclei are all likely signs of RO, whereas varied nuclear size, raisinoid nuclei, and reticular cytoplasm are more likely signs of ChRCC. Typically, RO cells have round nuclei, but in an investigation of RO cells, a raisinoid nuclei was observed, which is a key feature of ChRCCs [
21]. Surprisingly, components of RCC can be seen in 10–30% of ROs; hence, the presence of an RO in a sample does not confirm the absence of renal cancer [
21]. So, there is a clinical challenge in identifying RO from ChRCCs in a given sample.
Various conventional methods have been used to diagnose and differentiate between these two highly similar subtypes of renal masses such as biopsy, MRI and CT scans. Each of these methods has limitations in diagnosing and differentiating the two. Currently, no proposed CT scan markers can reliably distinguish ROs from RCCs. As a result, most ROs are classified as suspicious of RCCs on the basis of imaging and are usually exposed to surgical excision [
22]. Similarly, research on the potential of MRI to identify ROs from ChRCCs concluded that both groups had comparable characteristics, and no MRI clinical features could help differentiate the two [
23].
Unlike MRI and CT scans, a renal mass biopsy presents an opportunity for a pre-operative diagnosis. However, this approach has various potential problems, making surgical resection unavoidable. One of the significant disadvantages of using biopsy is that it is difficult for a pathologist to diagnose renal tumor subtypes accurately from insufficient tissue biopsy samples, as a whole range of cyto-architectural features are usually required for analysis to come to a diagnosis [
24]. Generally, a lesion is reported as ChRCC if it looks exactly the same as a chromophobe in the needle biopsy. However, if the pathologist identifies the lesion as RO in the needle biopsy, it is concluded that more tissue sampling for diagnosis is needed because of tumor heterogeneity. This is because there are many variants of ChRCC that are more similar to RO than to ChRCC. In addition to the difficulty in clinically distinguishing ROs from ChRCCs, the characteristics of these pathological tumors following renal biopsy sometimes coincide, making diagnosis particularly problematic for pathologists [
13].
Moreover, the available methods of tumor identification are not conclusive, as they are subjective. Likewise, a biopsy, which is the method in use currently, although accurate, is an invasive technique that has its own limitations [
25]. On the other hand, according to the literature [
26,
27,
28], the prevalence of benign tumors ranges between 13 to 30% of all surgically resected lesions as the possibility of benign renal histopathology in small renal masses is determined by the size, with about 40% of the tumors being smaller than a centimeter in diameter [
27]. This, as a result, further leads patients to undergo expensive and unnecessary surgery.
Recent studies show that ROs and ChRCCs have similar histological and cytologic characteristics and immunohistochemistry (IHC) markers for S100A1 and CD117 KIT [
29]. However, varied forms of renal tumors act differently and have different prognoses. They may be difficult to distinguish due to some overlapping morphological traits and immunohistochemical staining patterns [
29]. Similarly, non-diagnostic core-needle biopsy and errors due to sampling, both quite typical with percutaneous biopsy, are limiting factors in correctly diagnosing these two RCC subtypes [
30]. Therefore, it is essential to tell the difference between ChRCCs and ROs before surgery to manage a patient’s condition better.
Due to the challenges in differentiating RO from ChRCC clinically and histopathologically through biopsy [
29], there is a need to develop a more accurate, reliable, and clinically applicable method in differentiating RO from ChRCCs. Recently, there has been technological advancement in medical imaging, enabling medical researchers to capture tissue anatomy characteristics, physiological functions and quantitative features through images that help in precision medicine [
31]. The advantage of this is that non-invasive methods of tumor identification have been investigated, hence assisting in solving the shortcomings of biopsy and efficiently detecting tumor differences.
Quantitative imaging is now possible through advancements such as improved technology, imaging agents, and standardized protocols. Radiomics is the recent variety of medical imaging signature breakthroughs, focusing on image analysis enhancements, employing automatic high-dimension extraction of large volumes of quantitative aspects of medical image data [
32,
33]. Ten years ago, Lambin et al. [
32] proposed the possibility of extracting radiomics features based on the differences in solid renal tumors. By extracting such features from high-dimensional image data, valuable meaningful information can be extracted instead of visually observing the features [
32]. Many studies have investigated the potential of radiomics texture analysis as an alternative to the traditional imaging methods of differentiating RO from ChRCC. However, these studies have focused on the theoretical aspects rather than the practical application of radiomics texture analysis. Likewise, there is limited research on the use of radiomic feature analysis on rare types of renal tumors. Moreover, according to our knowledge, no paper has attempted to investigate the effect of filter features as well as a hybrid study, i.e., the combination of both prospective and retrospective research in a single study on the accuracy of radiomic models. The use of all tumor slices for the prediction of patient histopathology has also not been investigated before. This is the first paper, according to our knowledge, that has used the highest number of participants in the differentiation of ChRCC from RO using ML-based radiomic signature.
Therefore, in this research, the prospects of a hybrid study, effects of filter features and all tumor slices analysis combined with ML techniques have been investigated in an effort to differentiate RO from ChRCC in order to develop better non-invasive pre-operative diagnostic models than the traditional methods.
4. Discussion
ChRCC was formally categorized as a type of renal tumor in 1998 by the World Health Organization (WHO) [
20]. ChRCC is the third most common type of RCC, which has a high tendency to metastasize. RO is the most frequent type of benign tumor and was discovered in 1942 [
58]. RO accounts for between 3% to 7% of all diagnosed renal tumors. RO characteristics mimic those of RCC; hence in most cases, they are diagnosed incidentally, as they are mistaken for ChRCC [
59]. Moch and Ohashi [
20] assert that RO has a morphological heterogeneity similar to that of ChRCC. Baghdadi et al. [
26] stated that both ChRCC and RO have CD117 (+) protein biomarkers, unavailable in other RCC tumors; hence, it is difficult to distinguish between the two tumors, as their morphological characteristics overlap.
Currently, the most effective treatment method for renal tumors is surgical resection. However, both radical and partial nephrectomy have complications. For instance, radical nephrectomy increases the chances of chronic renal diseases, which leads to cardiovascular diseases and mortality [
16]. Research shows that up to 30% of surgically resected renal masses are ultimately benign [
26], leading many patients to undergo unnecessary surgery. Biopsy is the most popular pre-operative examination technique, with almost 97% accuracy for differentiating malignant from benign renal masses in general [
16]. However, renal biopsy has specifically reported difficulties in differentiating ChRCC from RO [
20]. Therefore, this present research focused on ML-based radiomic analysis to distinguish between ChRCC and RO.
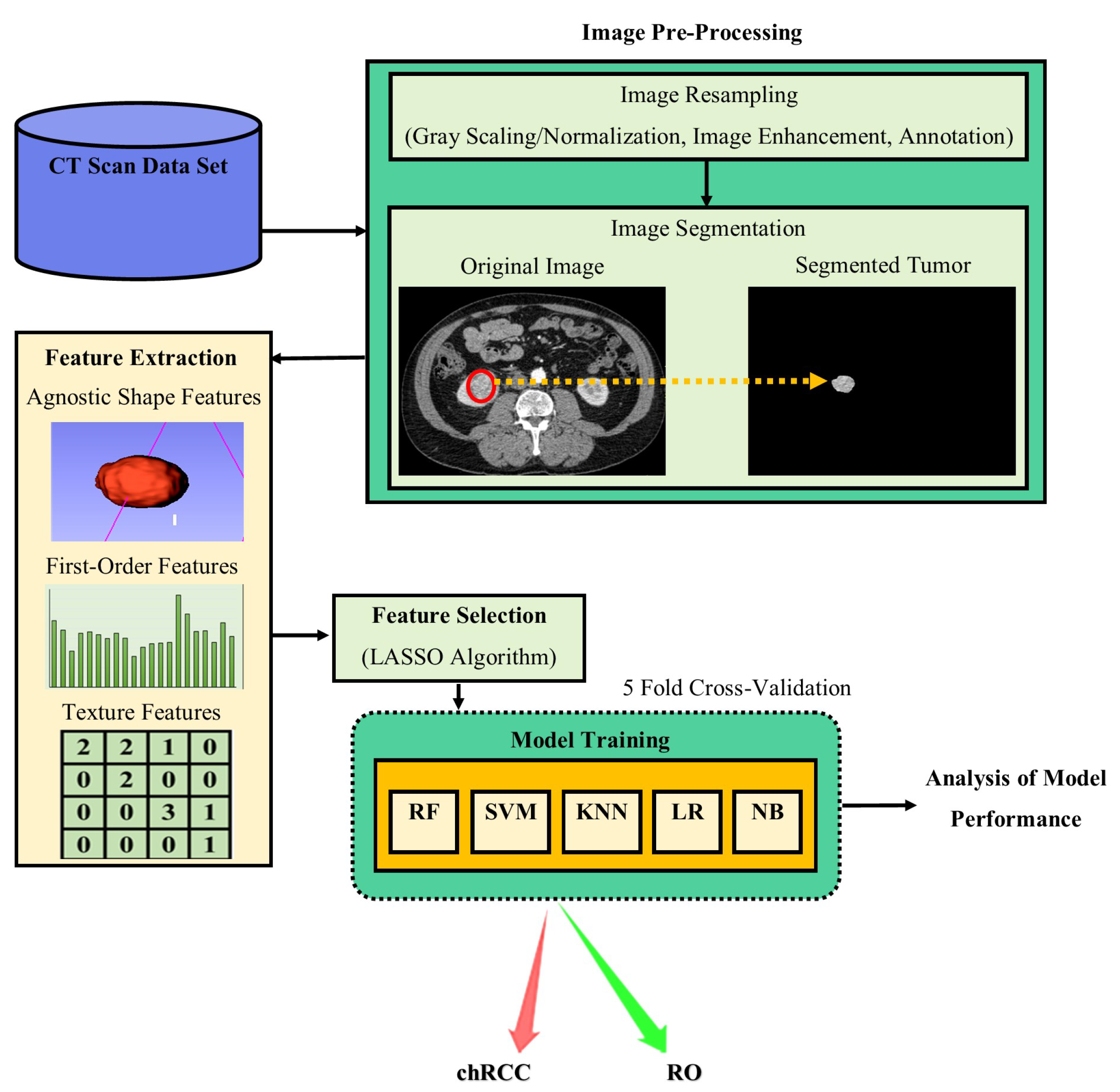
Radiomic analyses refers to the calculation of high dimension texture features using complex image processing technologies to obtain quantitative texture representations [
32]. Using radiomics analysis, very important but small differences that are not detectable visually can be extracted and analyzed [
31]. Radiomics, sometimes also referred to as a “virtual biopsy“, is advantageous in several ways, as it can capture both intra-tumoral (within-tumor) and inter-tumor (between-tumors) heterogeneity, and can be performed multiple times as opposed to biopsy. Therefore, this advanced image processing technique is potentially a more objective method for tumor analysis.
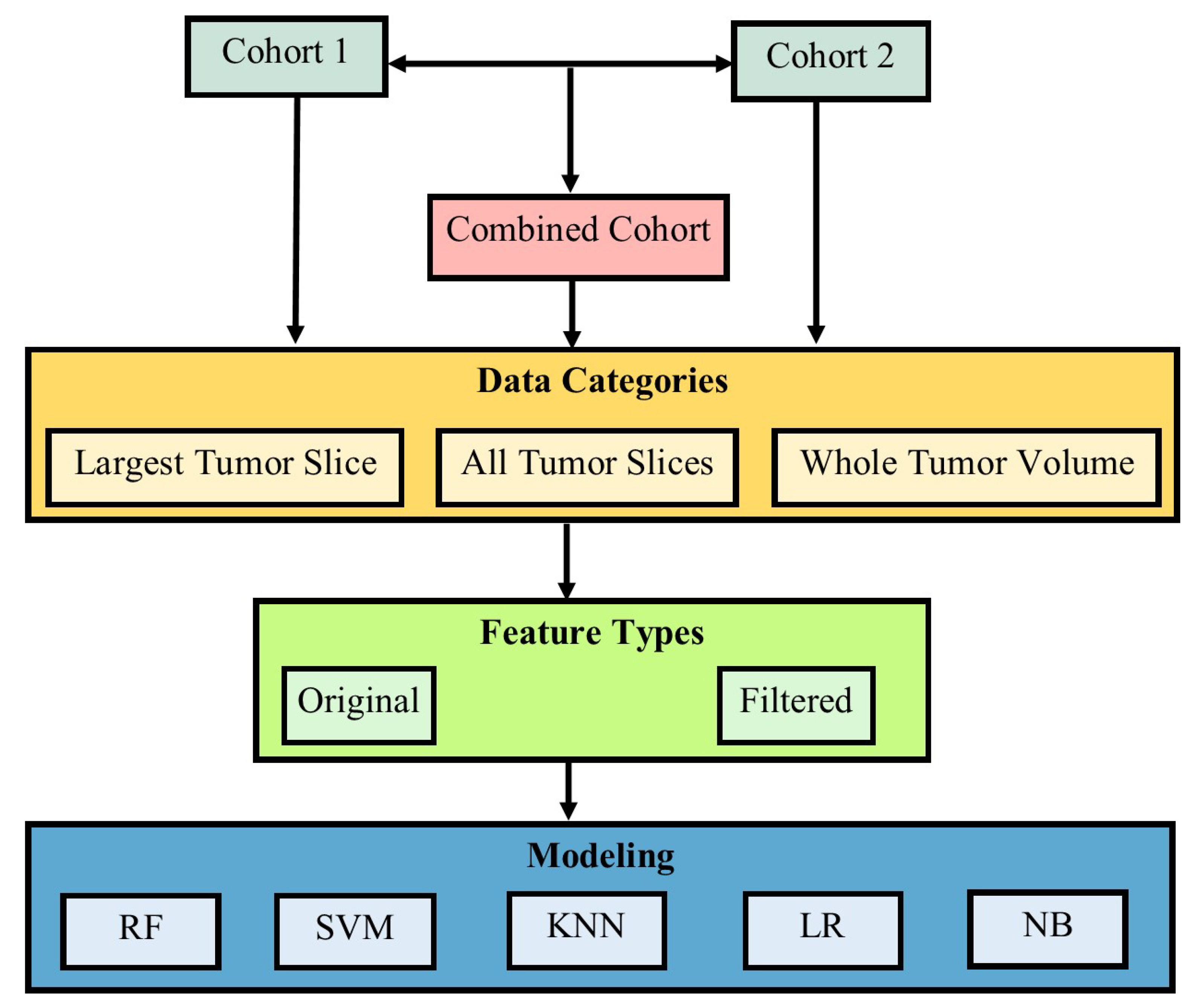
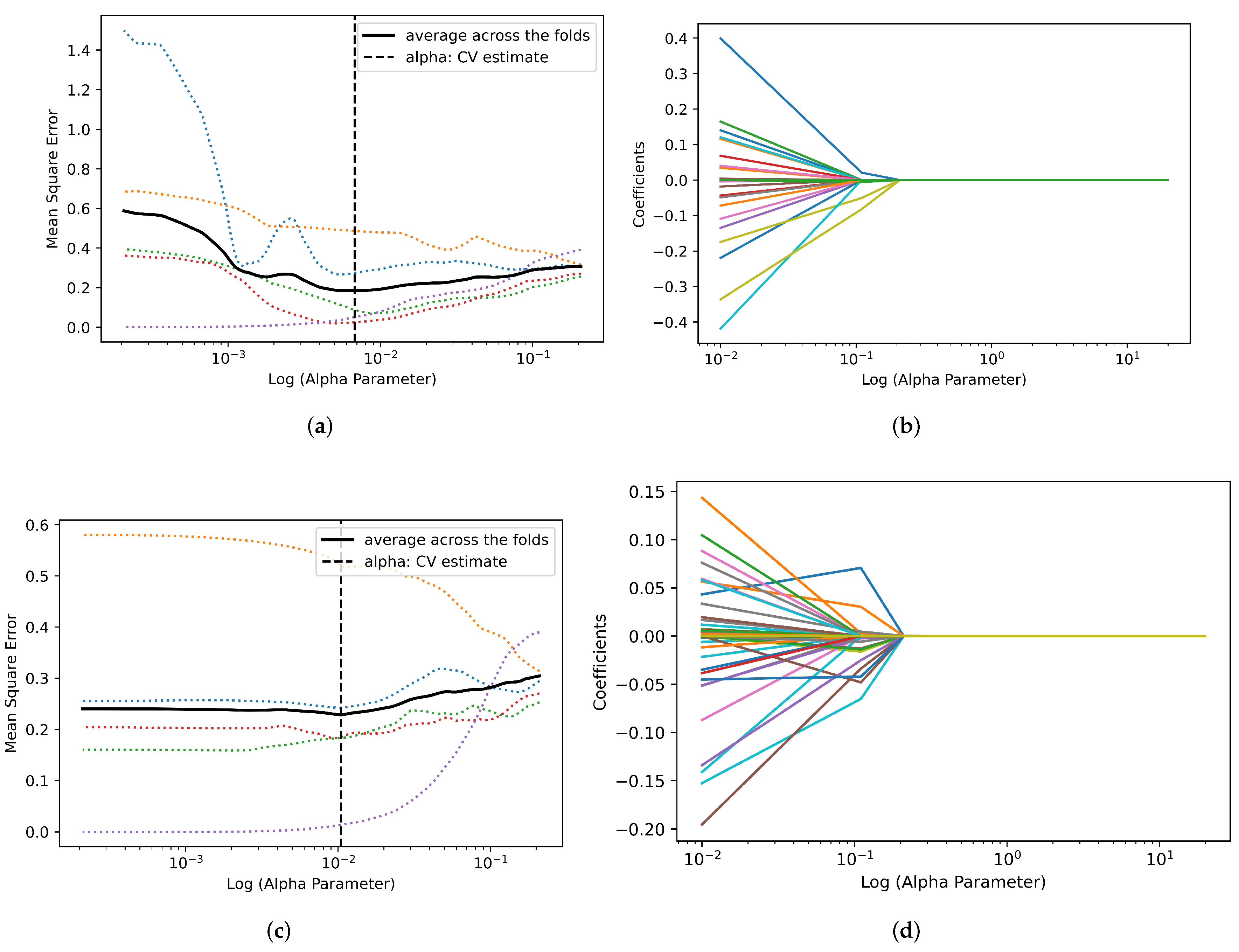
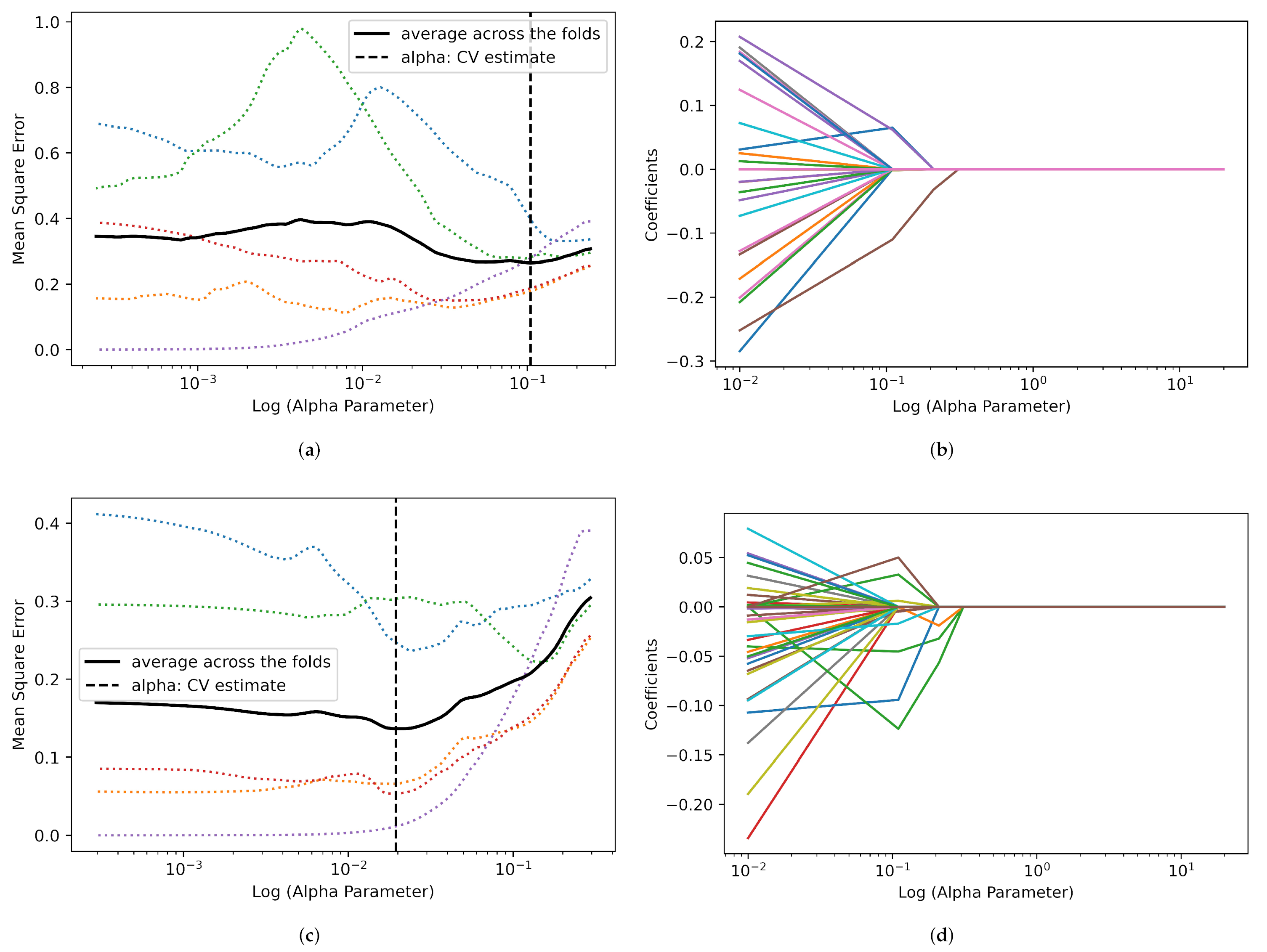
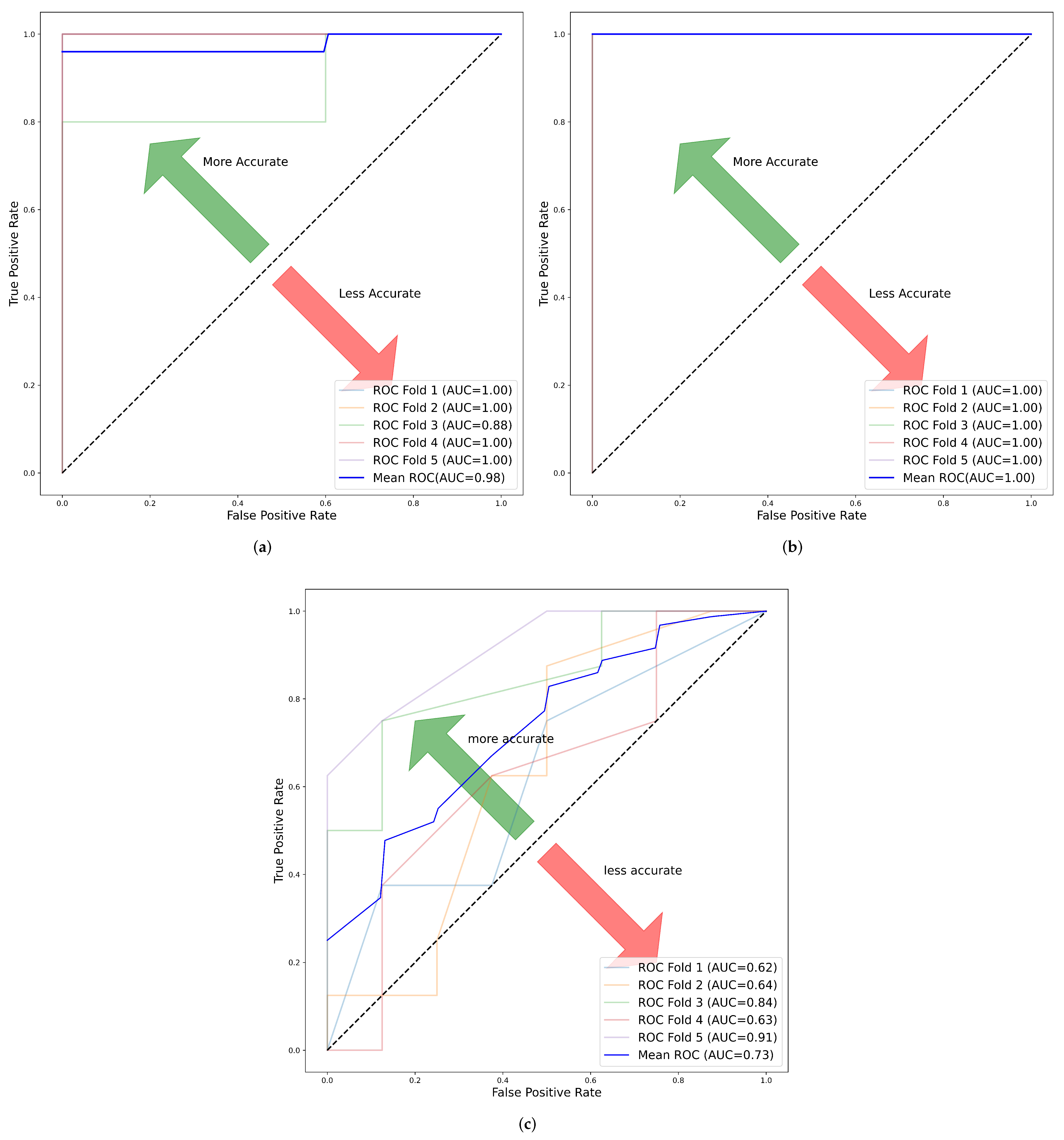
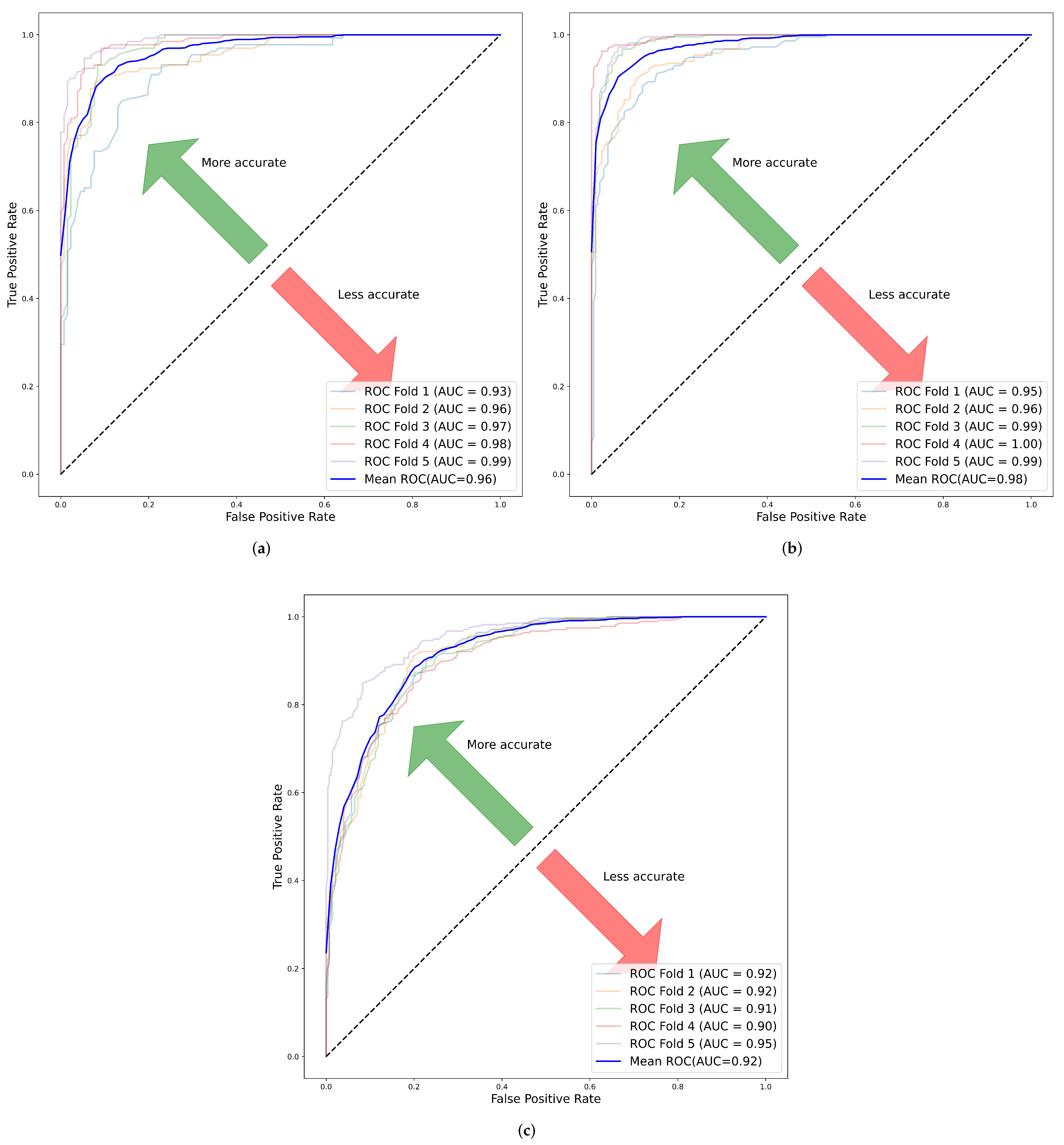
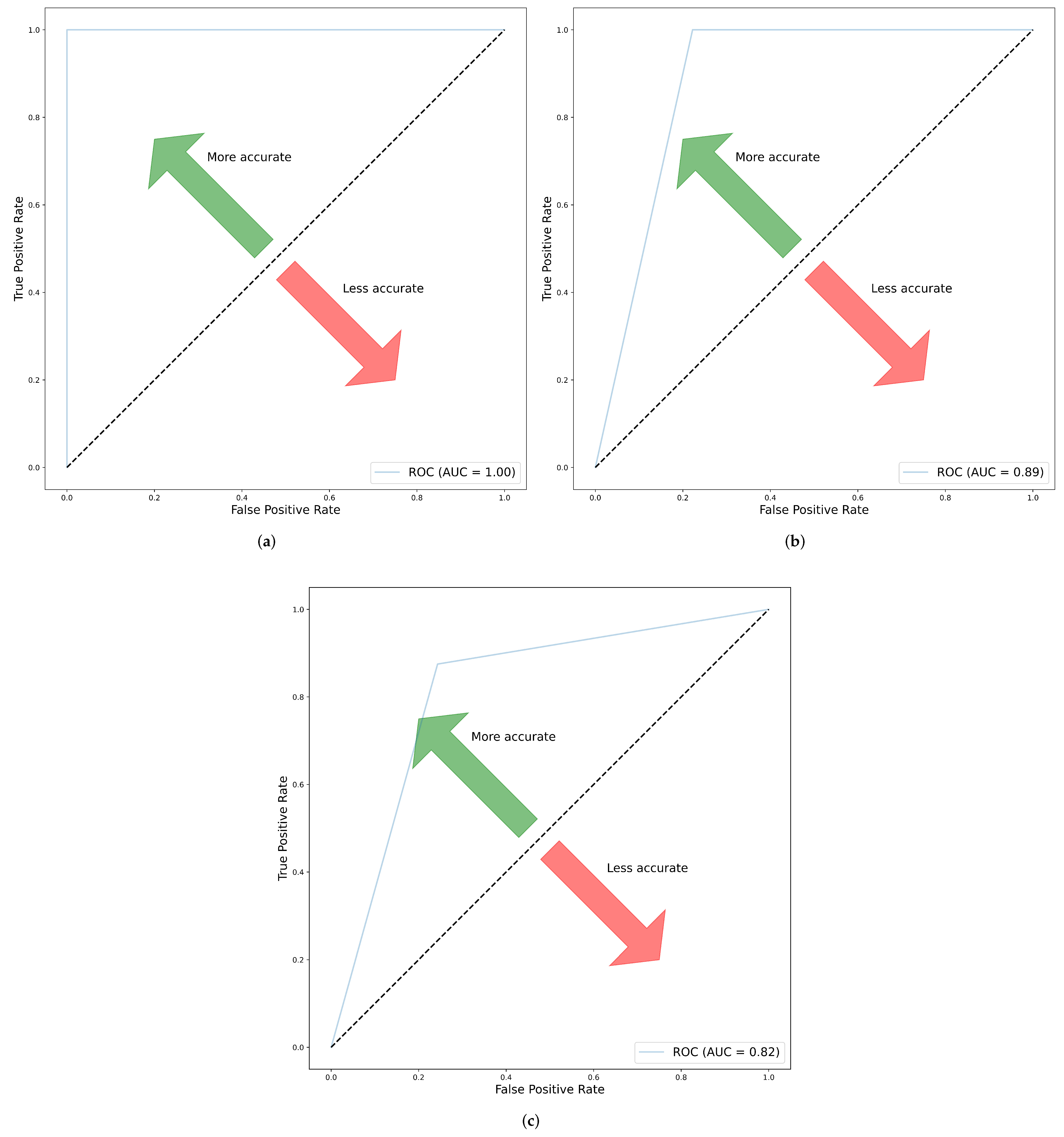
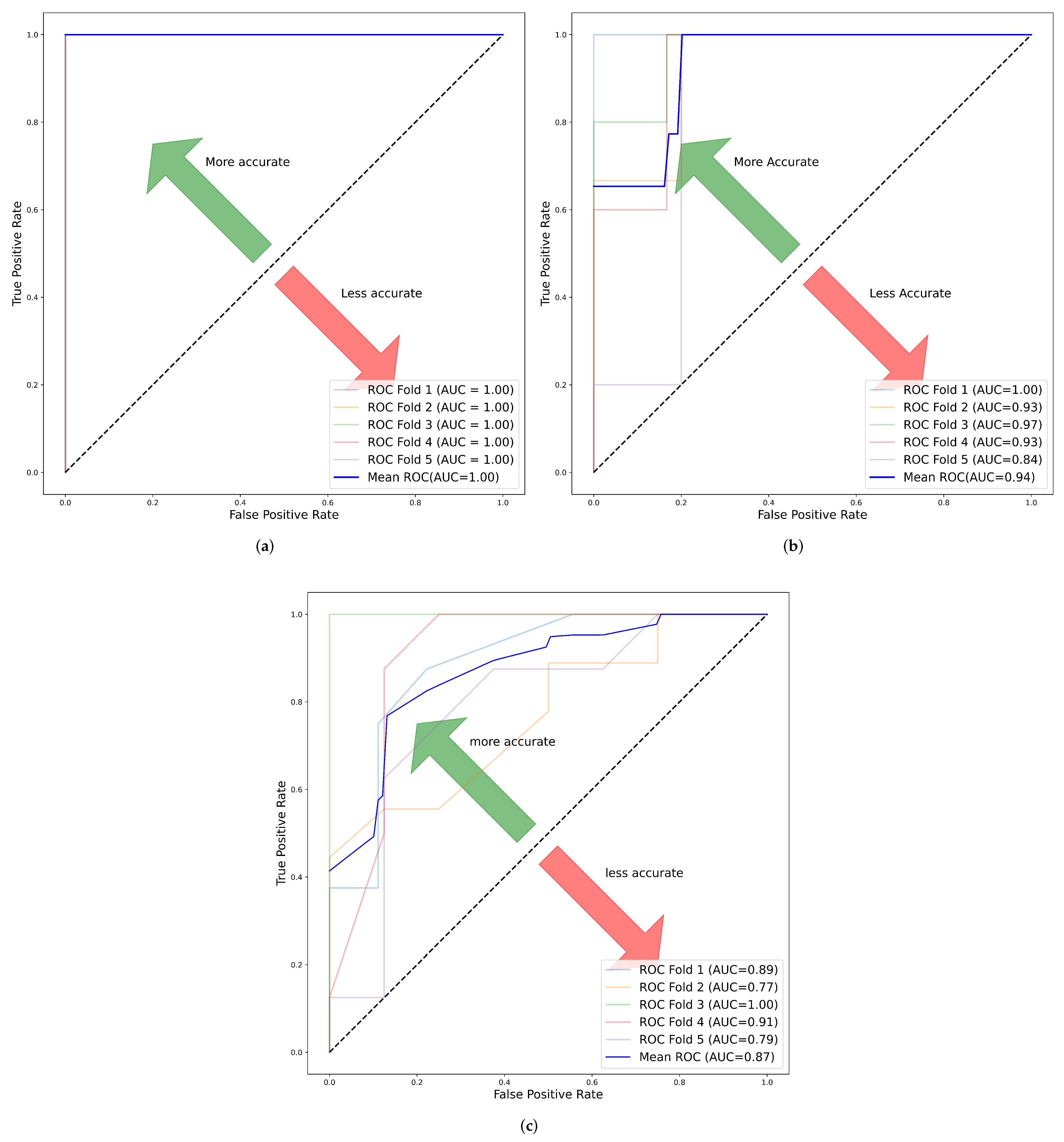
Experimental results from this study indicated that for cohort 1, the per patient prediction with original features had the best predictive performance with an AUC of 1.00 ± 0.000. In cohort 2, largest tumor slice with filter features had the best performance with an AUC of 1.00 ± 0.000. Finally, in cohort 3, whole tumor volume with filters exhibited the best performance with AUC of 0.87 ± 0.073. Filtered features were better than the original features for most models in their ability to distinguish ChRCC from RO. Overall, whole tumor volume was the best category to represent the heterogeneity of the tumor. SVM, KNN and RF models all offered promising results in radiomic feature analysis.
The combined cohort had the lowest diagnostic performance in all the categories. This is likely due to the fact that the cohort is a combination of two different data sets captured using different scanners and protocols. This led to poor generalization compared to the other cohorts. However, it is worth noting that the least performance was in the largest tumor slice with an AUC of 0.73, while the best performance was in whole tumor volume with AUC 0.87. Therefore, we concluded that in general the model generalized well in the multi-center study.
There exist limited studies on the differentiation of ChRCC from RO. This is largely because ChRCC and RO are rarely occurring renal tumors compared to other renal tumor subtypes. Therefore, most studies focus on the analysis of clear cell RCC (ccRCC) and papillary RCC (PRCC), which are more common. Sun et al. [
60] implemented an SVM recursive feature elimination (SVM-RFE) classifier with 100 samples (64 malignant and 36 benign) to differentiate between malignant and benign renal tumor subtypes consisting of one group of PRCC and ChRCC versus another of angiomyolipoma without visible fat (AMLwvf) and RO. The model yielded a sensitivity of 83.3% and a specificity of 91.7%. In the paper by Sun et al. [
60], 11 features were extracted from the CECT scan, which was then applied to the ML algorithm. Erdim et al. [
61], just like Sun et al. [
60] did not focus on a single malignant and benign renal cell subtype. However, the paper compared the performance of several ML radiomic feature analysis models between unenhanced and contrast-enhanced CT phases. The paper conducted a study using a total sample size of 84 renal tumors consisting of 63 malignant (ccRCC, PRCC and ChRCC) and 21 benign (AMLwvf and RO) [
61]. These two studies are general in nature and cannot be used as diagnostic predictors in the differentiation of ChRCC from RO; as such, our study has limited the scope of tumor subtypes to only the rarely occurring tumors with similar morphological characteristics, i.e., ChRCC and RO.
Li et al. [
16] explored how enhanced CT quantitative feature analysis can be used for the differentiation of RO from ChRCC. The paper’s authors conducted a retrospective study using 61 (17 RO, 44 ChRCC) pathologically confirmed cases of renal tumors. The paper implemented five ML algorithms for corticomidulary-phase (CMP), nephrographic-phase (NP), excretory-phase (EP) and combined CMP with NP, out of which the SVM classifier had the highest accuracy of 0.945. This was done after applying the LASSO technique for feature selection [
16]. Whereas our paper focused on the differentiation of RO from ChRCC, the central point of departure from the paper by Li et al. [
16] was that our research was based on the comparison between radiomic analysis for original and filtered radiomic features. Nonetheless, our study went further and did a 2D maximal axial tumor slice radiomic feature analysis in addition to the 3D analysis. All tumor slices were also analyzed and a majority voting technique was used to perform the per patient prediction. Through such analysis, we were able to determine the best criteria for radiomic feature analysis. Feng et al. [
62] indicated that the use of a small data set, especially due to class imbalance, increased over-fitting and recommended using SMOTE to mitigate such challenges. Li et al. [
16] did not describe how they mitigated the class imbalance in the data; this was addressed in our paper by implementing SMOTE. Moreover, the paper never looked at the prospect of a prospective and multi-center study as an alternative and even a better discriminant compared to a retrospective and single center study. In our research, this was adequately tackled by conducting both retrospective and prospective research as well as a single center and multi-center study.
Baghdadi et al. [
26] investigated the possibility of using Artificial Intelligence (AI) in combination with an image processing signature in a semi-automatic design, using the tumor to cortex peak early phase enhanced ratio (PEER) to distinguish ChRCC from RO using convolutional neural network (CNN) segmentation in CT images. The authors had 192 participants for the training cohort and 20 for the testing cohort. As opposed to Baghdadi et al. [
26], our paper analyzed both 2D and 3D images. Baghdadi et al. [
26] did not investigate the possible importance of radiomics texture analysis for the purpose of differentiating renal tumors.
Uchida et al. [
63] developed a diffusion coefficient map to assist in the distinction of RO from ChRCC using MRI texture features. The research focused on the analysis of important texture features in 3D MRI volume. The sample size of the study was 49 (ChRCC:41, RO:8); despite the small sample size and class imbalance in the data, the authors did not attempt to mitigate or solve the problem, this could have possibly affected the model performance leading to over-fitting.
Li et al. [
16] suggested the use of contrast-enhanced CT images to increase the accuracy of classification models. Kocak, Ates et al. [
64] analyzed the importance of edge segmentation on the performance of a model. The authors concluded that contracting the tumor edges of segmentation by about 2mm leads to better reproducibility and model performance [
64]. In our paper, both manual and semi-automatic methods were explored for the purpose of segmentation. Lee et al. [
65] developed a RF algorithm with an automated deep learning CNN feature extraction model to differentiate angiomyolipoma without visible fat (AMLwvf) from ccRCC in CECT images. The model achieved an accuracy of 76.6% for data of 80 samples [
65]. Erdim et al. [
61] reported that CECT images yielded comparatively superior predictive performance in comparison to unenhanced CT in texture analysis. In the paper, the authors compared results from both unenhanced and contrast-enhanced using different ML algorithms. RF model had the highest accuracy with 88.1% and 90.5% for unenhanced and contrast-enhanced, respectively [
61]. For this reason, our paper performed an analysis on the CECT scan.
The present study comprehensively explores the possibility of “virtual biopsy” of renal masses in distinguishing chromophobe renal cell carcinomas from oncocytomas using radiomics and machine learning techniques. The cohorts used were from two different institutions, therefore, they provided some assurance of its external validity, however further research is needed to consolidate this. Our study addressed a specific challenge of distinguishing oncocytic renal masses. Our observations in combination with other reported studies of more common clear cell carcinoma may make it possible to spare patients from more biopsies and move us closer to having a more precise diagnosis. Radiomics based tumor maps, with the ability to capture the patchwork of different types of cancer cells (heterogeneity), may allow clinicians to obtain a more precise tissue sample during biopsies as well. The research in virtual biopsy is growing, and since 2015, publications in this area have doubled [
66], as this appeals to two desired end goals in clinical diagnosis of cancers; improved precision and less invasiveness.
There are a few potential limitations in this study that might have had an effect on the results. First, the sample-size was small, primarily because we differentiated rarely occurring tumors so limited data was available. Second, investigation of unenhanced CT images may lead to an analysis of critical internal masses. We did not use unenhanced plain CT to minimize errors in segmentation of the tumors. Due to the rarity of studies in this area, we were unable to validate our results using an independent external data set. Erdim et al. [
61] and Lee et al. [
67] recommended using deep learning to overcome the problem of false-negative errors in the existing ML classification algorithms, thereby improving the predictive performance in clinical practice. However, this was not implemented in our radiomic engineered-hand-crafted study, as the deep learning model requires a great deal of data to train.
In future research, we propose to explore the use of deep learning models. Likewise, in addition to radiomic signature, other radiomic clusters such as radio-genomics, radio-proteomics and radio-metabolomics need to be studied and compared with the conventional radiomics.















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}