
Hypoxic-Ischemic Brain Injury in ECMO: Pathophysiology, Neuromonitoring, and Therapeutic Opportunities
 , ,
, ,
Abstract
:1. Introduction
2. Clinical Evidence of HIBI in ECMO
2.1. Epidemiology
2.2. Timing and Etiology of HIBI
2.3. Risk Factors
2.4. Outcome
3. Preclinical Models of HIBI in ECMO
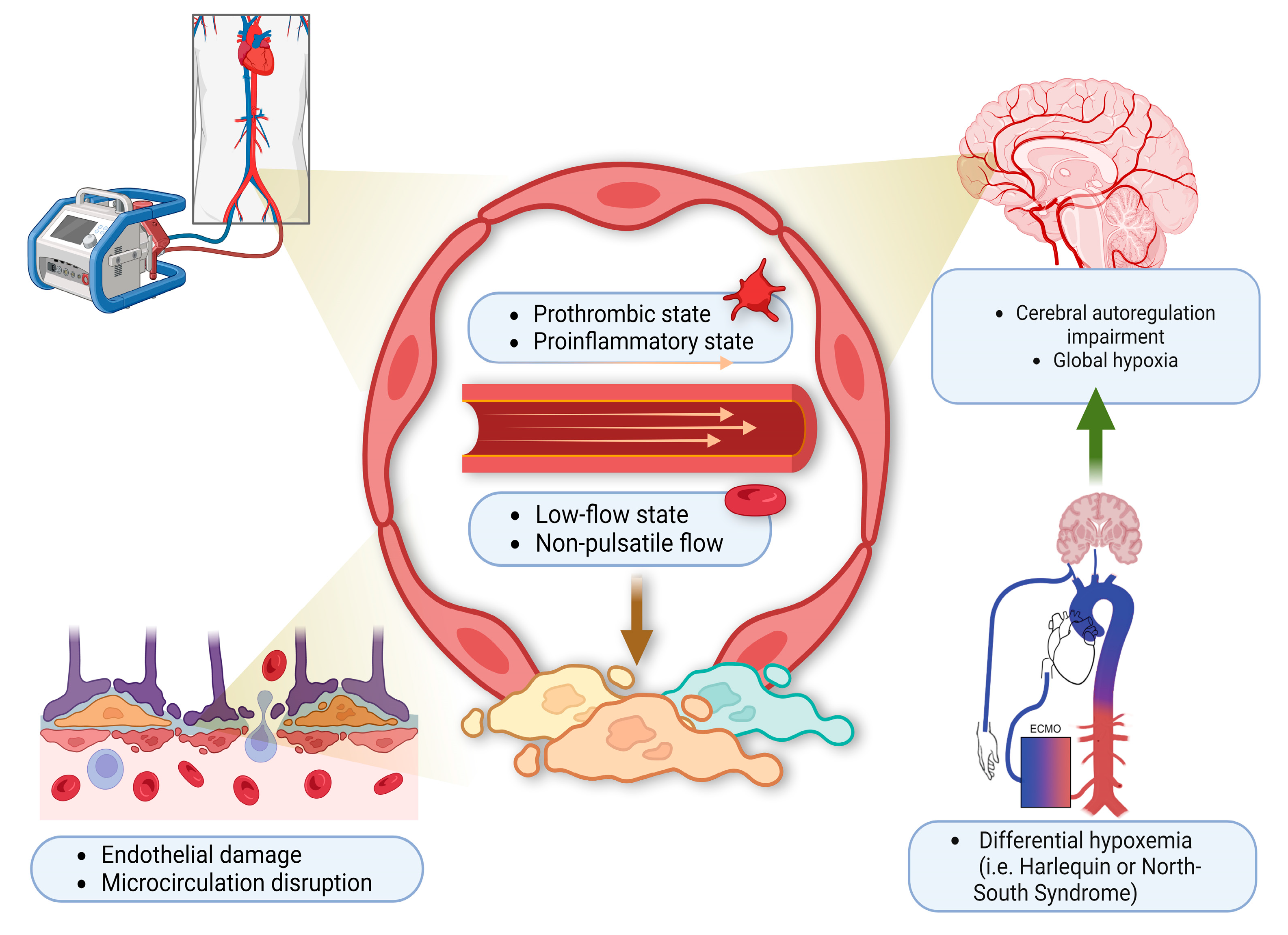
4. Pathophysiology
5. Neuromonitoring
5.1. Serial Neurological Examination
5.2. EEG
5.3. Cerebral NIRS
5.4. SSEP
5.5. SSEP and EEG
5.6. Transcranial Doppler
5.7. Plasma Biomarkers
5.8. Imaging
5.8.1. Brain CT
5.8.2. Brain MRI
6. Therapeutic Management
6.1. Temperature Control
6.2. Cerebral Edema and Elevated ICP
7. Future Directions
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- MacLaren, G.; Fisher, D.; Brodie, D. Preparing for the Most Critically Ill Patients with COVID-19: The Potential Role of Extracorporeal Membrane Oxygenation. JAMA 2020, 323, 1245–1246. [Google Scholar] [CrossRef]
- Migdady, I.; Rice, C.; Deshpande, A.; Hernandez, A.V.; Price, C.; Whitman, G.J.; Geocadin, R.G.; Cho, S.M. Brain Injury and Neurologic Outcome in Patients Undergoing Extracorporeal Cardiopulmonary Resuscitation: A Systematic Review and Meta-Analysis. Crit. Care Med. 2020, 48, e611–e619. [Google Scholar] [CrossRef]
- Cho, S.-M.; Lee, T.; Starling, R.C.; Thompson, N.R.; Uchino, K. The Impact of Infection and Elevated INR in LVAD-Associated Intracranial Hemorrhage: A Case-Crossover Study. ASAIO J. 2019, 65, 545–549. [Google Scholar] [CrossRef]
- Lee, T.; Buletko, A.B.; Matthew, J.; Cho, S.-M. Bloodstream infection is associated with subarachnoid hemorrhage and infectious intracranial aneurysm in left ventricular assist device. Perfusion 2020, 35, 117–120. [Google Scholar] [CrossRef]
- Trachtenberg, B.H.; Cordero-Reyes, A.M.; Aldeiri, M.; Alvarez, P.; Bhimaraj, A.; Ashrith, G.; Elias, B.; Suarez, E.E.; Bruckner, B.; Loebe, M.; et al. Persistent Blood Stream Infection in Patients Supported With a Continuous-Flow Left Ventricular Assist Device Is Associated With an Increased Risk of Cerebrovascular Accidents. J. Card. Fail. 2015, 21, 119–125. [Google Scholar] [CrossRef]
- Ruland, S.; Aiyagari, V. Cerebral Autoregulation and Blood Pressure Lowering. Hypertension 2007, 49, 977–978. [Google Scholar] [CrossRef] [Green Version]
- Jia, D.; Neo, R.; Lim, E.; Seng, T.C.; MacLaren, G.; Ramanathan, K. Autopsy and clinical discrepancies in patients undergoing extracorporeal membrane oxygenation: A case series. Cardiovasc. Pathol. 2019, 41, 24–28. [Google Scholar] [CrossRef]
- Cho, S.-M.; Ziai, W.; Mayasi, Y.; Gusdon, A.M.; Creed, J.; Sharrock, M.; Stephens, R.S.; Choi, C.W.; Ritzl, E.K.; Suarez, J.; et al. Noninvasive Neurological Monitoring in Extracorporeal Membrane Oxygenation. ASAIO J. 2020, 66, 388–393. [Google Scholar] [CrossRef]
- Lorusso, R.; Barili, F.; Mauro, M.D.; Gelsomino, S.; Parise, O.; Rycus, P.T.; Maessen, J.; Mueller, T.; Muellenbach, R.; Belohlavek, J.; et al. In-Hospital Neurologic Complications in Adult Patients Undergoing Venoarterial Extracorporeal Membrane Oxygenation: Results From the Extracorporeal Life Support Organization Registry. Crit. Care Med. 2016, 44, e964–e972. [Google Scholar] [CrossRef]
- Xie, A.; Lo, P.; Yan, T.D.; Forrest, P. Neurologic Complications of Extracorporeal Membrane Oxygenation: A Review. J. Cardiothorac. Vasc. Anesthesia 2017, 31, 1836–1846. [Google Scholar] [CrossRef]
- Cho, S.-M.; Ziai, W.; Geocadin, R.; Choi, C.W.; Whitman, G. Arterial-Sided Oxygenator Clot and Transcranial Doppler Ultrasound Emboli in Venoarterial Extracorporeal Membrane Oxygenation. Ann. Thorac. Surg. 2018, 107, 326–327. [Google Scholar] [CrossRef] [Green Version]
- Cho, S.-M.; Geocadin, R.G.; Caturegli, G.; Chan, V.; White, B.; Dodd-O, J.; Kim, B.S.; Sussman, M.; Choi, C.W.; Whitman, G.; et al. Understanding Characteristics of Acute Brain Injury in Adult Extracorporeal Membrane Oxygenation: An Autopsy Study. Crit. Care Med. 2020, 48, e532–e536. [Google Scholar] [CrossRef]
- Laver, S.; Farrow, C.; Turner, D.; Nolan, J. Mode of death after admission to an intensive care unit following cardiac arrest. Intensiv. Care Med. 2004, 30, 2126–2128. [Google Scholar] [CrossRef]
- Nolan, J.P.; Neumar, R.W.; Adrie, C.; Aibiki, M.; Berg, R.A.; Böttiger, B.W.; Callaway, C.; Clark, R.S.; Geocadin, R.G.; Jauch, E.C.; et al. Post-cardiac arrest syndrome: Epidemiology, pathophysiology, treatment, and prognostication: A Scientific Statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; the Council on Stroke. Resuscitation 2008, 79, 350–379. [Google Scholar]
- Lorusso, R.; Gelsomino, S.; Parise, O.; Di Mauro, M.; Barili, F.; Geskes, G.; Vizzardi, E.; Rycus, P.T.; Muellenbach, R.; Mueller, T.; et al. Neurologic Injury in Adults Supported With Veno-Venous Extracorporeal Membrane Oxygenation for Respiratory Failure: Findings From the Extracorporeal Life Support Organization Database. Crit. Care Med. 2017, 45, 1389–1397. [Google Scholar] [CrossRef]
- Shoskes, A.D.; Migdady, I.; Rice, C.; Hassett, C.D.; Deshpande, A.; Price, C.M.; Hernandez, A.V.; Cho, S.-M.D. Brain Injury Is More Common in Venoarterial Extracorporeal Membrane Oxygenation Than Venovenous Extracorporeal Membrane Oxygenation: A Systematic Review and Meta-Analysis. Crit. Care Med. 2020, 48, 1799–1808. [Google Scholar] [CrossRef]
- Shou, B.L.; Ong, C.S.; Zhou, A.L.; Al-Kawaz, M.N.; Etchill, E.; Giuliano, K.; Dong, J.; Bush, E.; Kim, B.S.; Choi, C.W.; et al. Arterial Carbon Dioxide and Acute Brain Injury in Venoarterial Extracorporeal Membrane Oxygenation. ASAIO J. 2022, 68, 1501–1507. [Google Scholar] [CrossRef]
- Busl, K.M.; Greer, D.M. Hypoxic-ischemic brain injury: Pathophysiology, neuropathology and mechanisms. Neurorehabilitation 2010, 26, 5–13. [Google Scholar] [CrossRef] [Green Version]
- Ziai, W.C.; Cho, S.M.; Johansen, M.C.; Ergin, B.; Bahouth, M.N. Transcranial Doppler in Acute COVID-19 Infection: Unexpected Associations. Stroke 2021, 52, 2422–2426. [Google Scholar] [CrossRef]
- Le Gall, A.; Follin, A.; Cholley, B.; Mantz, J.; Aissaoui, N.; Pirracchio, R. Veno-arterial-ECMO in the intensive care unit: From technical aspects to clinical practice. Anaesth. Crit. Care Pain Med. 2018, 37, 259–268. [Google Scholar] [CrossRef] [Green Version]
- Loungani, R.S.; Fudim, M.; Ranney, D.; Kochar, A.; Samsky, M.D.; Bonadonna, D.; Itoh, A.; Takayama, H.; Takeda, K.; Wojdyla, D.; et al. Contemporary Use of Venoarterial Extracorporeal Membrane Oxygenation: Insights from the Multicenter RESCUE Registry. J. Card. Fail. 2021, 27, 327–337. [Google Scholar] [CrossRef]
- Wieruszewski, P.M.; Ortoleva, J.P.; Cormican, D.S.; Seelhammer, T.G. Extracorporeal Membrane Oxygenation in Acute Respiratory Failure. Pulm. Ther. 2023, 9, 109–126. [Google Scholar] [CrossRef] [PubMed]
- Shou, B.L.; Wilcox, C.; Florissi, I.; Kalra, A.; Caturegli, G.; Zhang, L.Q.; Bush, E.; Kim, B.; Keller, S.P.; Whitman, G.J.R.; et al. Early Low Pulse Pressure in VA-ECMO Is Associated with Acute Brain Injury. Neurocritical Care 2022, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, C.; Choi, C.W.; Cho, S.-M. Brain injury in extracorporeal cardiopulmonary resuscitation: Translational to clinical research. J. Neurocritical Care 2021, 14, 63–77. [Google Scholar] [CrossRef]
- Rupprecht, L.; Lunz, D.; Philipp, A.; Lubnow, M.; Schmid, C. Pitfalls in percutaneous ECMO cannulation. Heart lung Vessel. 2015, 7, 320–326. [Google Scholar]
- Haldenwang, P.L.; Baumann, A.; Elghannam, M.; Schlömicher, M.; Buchwald, D.; Klak, K.; Strauch, J.T. Two-stage weaning strategy using veno-veno-arterial perfusion for patients on extracorporeal membrane oxygenation following cardiogenic shock. Perfusion 2019, 34, 689–695. [Google Scholar] [CrossRef]
- Patel, B.; Arcaro, M.; Chatterjee, S. Bedside troubleshooting during venovenous extracorporeal membrane oxygenation (ECMO). J. Thorac. Dis. 2019, 11 (Suppl. 14), S1698–S1707. [Google Scholar] [CrossRef]
- Schmidt, M.; Tachon, G.; Devilliers, C.; Muller, G.; Hekimian, G.; Bréchot, N.; Merceron, S.; Luyt, C.E.; Trouillet, J.-L.; Chastre, J.; et al. Blood oxygenation and decarboxylation determinants during venovenous ECMO for respiratory failure in adults. Intensiv. Care Med. 2013, 39, 838–846. [Google Scholar] [CrossRef]
- Bishop, M.A.; Moore, A. Extracorporeal Membrane Oxygenation Weaning, in StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2023. [Google Scholar]
- Sutter, R.; Tisljar, K.; Marsch, S. Acute Neurologic Complications During Extracorporeal Membrane Oxygenation: A Systematic Review. Crit. Care Med. 2018, 46, 1506–1513. [Google Scholar] [CrossRef]
- Zhang, H.; Xu, J.; Yang, X.; Zou, X.; Shu, H.; Liu, Z.; Shang, Y. Narrative Review of Neurologic Complications in Adults on ECMO: Prevalence, Risks, Outcomes, and Prevention Strategies. Front. Med. 2021, 8, 713333. [Google Scholar] [CrossRef]
- Godoy, D.A.; Seifi, A.; Garza, D.; Lubillo-Montenegro, S.; Murillo-Cabezas, F. Hyperventilation Therapy for Control of Posttraumatic Intracranial Hypertension. Front. Neurol. 2017, 8, 250. [Google Scholar] [CrossRef] [Green Version]
- Harper, A.M.; Bell, R.A. The effect of metabolic acidosis and alkalosis on the blood flow through the cerebral cortex. J. Neurol. Neurosurg. Psychiatry 1963, 26, 341–344. [Google Scholar] [CrossRef] [Green Version]
- Rout, M.W.; Lane, D.J.; Wollner, L. Prognosis in Acute Cerebrovascular Accidents in Relation to Respiratory Pattern and Blood--gas Tensions. BMJ 1971, 3, 7–9. [Google Scholar] [CrossRef] [Green Version]
- Heffner, J.E.; Sahn, S.A. Controlled hyperventilation in patients with intracranial hypertension: Application and management. Arch. Intern. Med. 1983, 143, 765–769. [Google Scholar] [CrossRef] [PubMed]
- Dulla, C.G.; Dobelis, P.; Pearson, T.; Frenguelli, B.G.; Staley, K.J.; Masino, S.A. Adenosine and ATP Link PCO2 to Cortical Excitability via pH. Neuron 2005, 48, 1011–1023. [Google Scholar] [CrossRef] [Green Version]
- Shou, B.L.; Ong, C.S.; Premraj, L.; Brown, P.; Tonna, J.E.; Dalton, H.J.; Kim, B.S.; Keller, S.P.; Whitman, G.J.; Cho, S.-M. Arterial oxygen and carbon dioxide tension and acute brain injury in extracorporeal cardiopulmonary resuscitation patients: Analysis of the extracorporeal life support organization registry. J. Heart Lung Transplant. 2023, 42, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.-M.; Canner, J.; Caturegli, G.; Choi, C.W.; Etchill, E.; Giuliano, K.; Chiarini, G.; Calligy, K.; Rycus, P.; Lorusso, R.; et al. Risk Factors of Ischemic and Hemorrhagic Strokes During Venovenous Extracorporeal Membrane Oxygenation: Analysis of Data From the Extracorporeal Life Support Organization Registry. Crit. Care Med. 2021, 49, 91–101. [Google Scholar] [CrossRef] [PubMed]
- De Chambrun, M.P.; Bréchot, N.; Lebreton, G.; Schmidt, M.; Hekimian, G.; Demondion, P.; Trouillet, J.-L.; Leprince, P.; Chastre, J.; Combes, A. Venoarterial extracorporeal membrane oxygenation for refractory cardiogenic shock post-cardiac arrest. Intensive Care Med. 2016, 42, 1999–2007. [Google Scholar] [CrossRef]
- Ryu, J.-A.; Cho, Y.H.; Sung, K.; Choi, S.H.; Yang, J.H.; Choi, J.-H.; Lee, D.-S.; Yang, J.-H. Predictors of neurological outcomes after successful extracorporeal cardiopulmonary resuscitation. BMC Anesthesiol. 2015, 15, 26. [Google Scholar] [CrossRef] [Green Version]
- Carlson, J.M.; Etchill, E.; Whitman, G.; Kim, B.S.; Choi, C.W.; Tonna, J.E.; Geocadin, R.; Cho, S.-M. Early withdrawal of life sustaining therapy in extracorporeal cardiopulmonary resuscitation (ECPR): Results from the Extracorporeal Life Support Organization registry. Resuscitation 2022, 179, 71–77. [Google Scholar] [CrossRef]
- Foerster, K.; D’inka, M.; Beyersdorf, F.; Benk, C.; Nguyen-Thanh, T.; Mader, I.; Fritsch, B.; Ihling, C.; Mueller, K.; Heilmann, C.; et al. Prolonged cardiac arrest and resuscitation by extracorporeal life support: Favourable outcome without preceding anticoagulation in an experimental setting. Perfusion 2013, 28, 520–528. [Google Scholar] [CrossRef] [PubMed]
- Putzer, G.; Martini, J.; Spraider, P.; Abram, J.; Hornung, R.; Schmidt, C.; Bauer, M.; Pinggera, D.; Krapf, C.; Hell, T.; et al. Adrenaline improves regional cerebral blood flow, cerebral oxygenation and cerebral metabolism during CPR in a porcine cardiac arrest model using low-flow extracorporeal support. Resuscitation 2021, 168, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Rozencwajg, S.; Heinsar, S.; Wildi, K.; Jung, J.; Colombo, S.M.; Palmieri, C.; Sato, K.; Ainola, C.; Wang, X.; Abbate, G.; et al. Effect of flow change on brain injury during an experimental model of differential hypoxaemia in cardiogenic shock supported by extracorporeal membrane oxygenation. Sci. Rep. 2023, 13, 4002. [Google Scholar] [CrossRef]
- Kirino, T. Ischemic tolerance. J. Cereb. Blood Flow Metab. 2002, 22, 1283–1296. [Google Scholar] [CrossRef] [Green Version]
- Liang, D.; Bhatta, S.; Gerzanich, V.; Simard, J.M. Cytotoxic edema: Mechanisms of pathological cell swelling. Neurosurg. Focus 2007, 22, E2. [Google Scholar] [CrossRef] [Green Version]
- Solaini, G.; Baracca, A.; Lenaz, G.; Sgarbi, G. Hypoxia and mitochondrial oxidative metabolism. Biochim. Biophys. Acta 2010, 1797, 1171–1177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiessling, M.; Stumm, G.; Xie, Y.; Herdegen, T.; Aguzzi, A.; Bravo, R.; Gass, P. Differential Transcription and Translation of Immediate Early Genes in the Gerbil Hippocampus after Transient Global Ischemia. J. Cereb. Blood Flow Metab. 1993, 13, 914–924. [Google Scholar] [CrossRef] [Green Version]
- Kristián, T.; Siesjö, B.K. Calcium in Ischemic Cell Death. Stroke 1998, 29, 705–718. [Google Scholar] [CrossRef] [Green Version]
- Sekhon, M.S.; Ainslie, P.N.; Griesdale, D.E. Clinical pathophysiology of hypoxic ischemic brain injury after cardiac arrest: A “two-hit” model. Crit. Care 2017, 21, 90. [Google Scholar] [CrossRef] [Green Version]
- Cho, S.-M.; Farrokh, S.; Whitman, G.; Bleck, T.P.; Geocadin, R.G. Neurocritical Care for Extracorporeal Membrane Oxygenation Patients. Crit. Care Med. 2019, 47, 1773–1781. [Google Scholar] [CrossRef]
- Hu, Z.; Zhong, B.; Tan, J.; Chen, C.; Lei, Q.; Zeng, L. The Emerging Role of Epigenetics in Cerebral Ischemia. Mol. Neurobiol. 2016, 54, 1887–1905. [Google Scholar] [CrossRef]
- Yuan, Y.; Wang, J.Y.; Xu, L.Y.; Cai, R.; Chen, Z.; Luo, B.Y. MicroRNA expression changes in the hippocampi of rats subjected to global ischemia. J. Clin. Neurosci. 2010, 17, 774–778. [Google Scholar] [CrossRef] [PubMed]
- Cui, H.; Yang, L. Analysis of microRNA Expression Detected by Microarray of the Cerebral Cortex After Hypoxic-Ischemic Brain Injury. J. Craniofacial Surg. 2013, 24, 2147–2152. [Google Scholar] [CrossRef] [PubMed]
- Qu, Y.; Wu, J.; Chen, D.; Zhao, F.; Liu, J.; Yang, C.; Wei, D.; Ferriero, D.M.; Mu, D. RETRACTED: MiR-139-5p inhibits HGTD-P and regulates neuronal apoptosis induced by hypoxia–ischemia in neonatal rats. Neurobiol. Dis. 2014, 63, 184–193. [Google Scholar] [CrossRef]
- Qiu, J.; Zhou, X.-Y.; Cheng, R.; Liu, H.-Y.; Li, Y. Neuroprotective effects of microRNA-210 against oxygen-glucose deprivation through inhibition of apoptosis in PC12 cells. Mol. Med. Rep. 2013, 7, 1955–1959. [Google Scholar] [CrossRef] [Green Version]
- Chiarini, G.; Cho, S.-M.; Whitman, G.; Rasulo, F.; Lorusso, R. Brain Injury in Extracorporeal Membrane Oxygenation: A Multidisciplinary Approach. Semin. Neurol. 2021, 41, 422–436. [Google Scholar] [CrossRef] [PubMed]
- Peluso, L.; Rechichi, S.; Franchi, F.; Pozzebon, S.; Scolletta, S.; Brasseur, A.; Legros, B.; Vincent, J.-L.; Creteur, J.; Gaspard, N.; et al. Electroencephalographic features in patients undergoing extracorporeal membrane oxygenation. Crit. Care 2020, 24, 629. [Google Scholar] [CrossRef]
- Ong, C.S.; Etchill, E.; Dong, J.; Shou, B.L.; Shelley, L.; Giuliano, K.; Al-Kawaz, M.; Ritzl, E.K.; Geocadin, R.G.; Kim, B.S.; et al. Neuromonitoring detects brain injury in patients receiving extracorporeal membrane oxygenation support. J. Thorac. Cardiovasc. Surg. 2021, 165, 2104–2110.e1. [Google Scholar] [CrossRef]
- Perera, K.; Khan, S.; Singh, S.; Kromm, J.; Wang, M.; Sajobi, T.; Jetté, N.; Wiebe, S.; Josephson, C.B. EEG Patterns and Outcomes After Hypoxic Brain Injury: A Systematic Review and Meta-analysis. Neurocritical Care 2021, 36, 292–301. [Google Scholar] [CrossRef]
- Monteiro, M.L.; Taccone, F.S.; Depondt, C.; Lamanna, I.; Gaspard, N.; Ligot, N.; Mavroudakis, N.; Naeije, G.; Vincent, J.-L.; Legros, B. The Prognostic Value of 48-h Continuous EEG During Therapeutic Hypothermia After Cardiac Arrest. Neurocritical Care 2016, 24, 153–162. [Google Scholar] [CrossRef]
- Hwang, J.; Geocadin, R.; Ritzl, E.K.; Cho, S.-M. Continuous EEG in patients with extracorporeal membrane oxygenation support: Clinical need in multidisciplinary collaboration and standardized monitoring. Clin. Neurophysiol. 2022, 142, 273–274. [Google Scholar] [CrossRef]
- Hwang, J.; Bronder, J.; Martinez, N.C.; Geocadin, R.; Kim, B.S.; Bush, E.; Whitman, G.; Choi, C.W.; Ritzl, E.K.; Cho, S.-M. Continuous Electroencephalography Markers of Prognostication in Comatose Patients on Extracorporeal Membrane Oxygenation. Neurocritical Care 2022, 37, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Herman, S.T.; Abend, N.S.; Bleck, T.P.; Chapman, K.E.; Drislane, F.W.; Emerson, R.G.; Gerard, E.E.; Hahn, C.D.; Husain, A.M.; Kaplan, P.W.; et al. Consensus Statement on Continuous EEG in Critically Ill Adults and Children, Part I. J. Clin. Neurophysiol. 2015, 32, 87–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maldonado, Y.; Singh, S.; Taylor, M.A. Cerebral near-infrared spectroscopy in perioperative management of left ventricular assist device and extracorporeal membrane oxygenation patients. Curr. Opin. Anaesthesiol. 2014, 27, 81–88. [Google Scholar] [CrossRef]
- Said, A.S.; Guilliams, K.P.; Bembea, M.M. Neurological Monitoring and Complications of Pediatric Extracorporeal Membrane Oxygenation Support. Pediatr. Neurol. 2020, 108, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.; Rehan, M.; Parikh, G.; Zammit, C.; Badjatia, N.; Herr, D.; Kon, Z.; Hogue, C.; Mazzeffi, M. Regional Cerebral Oximetry as an Indicator of Acute Brain Injury in Adults Undergoing Veno-Arterial Extracorporeal Membrane Oxygenation–A Prospective Pilot Study. Front. Neurol. 2018, 9, 993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunt, M.F.; Clark, K.T.; Whitman, G.; Choi, C.W.; Geocadin, R.G.; Cho, S.-M. The Use of Cerebral NIRS Monitoring to Identify Acute Brain Injury in Patients with VA-ECMO. J. Intensiv. Care Med. 2021, 36, 1403–1409. [Google Scholar] [CrossRef]
- Andresen, B.; Greisen, G.; Hyttel-Sorensen, S. Comparison of INVOS 5100C and Nonin SenSmart X-100 oximeter performance in preterm infants with spontaneous apnea. Pediatr. Res. 2020, 87, 1244–1250. [Google Scholar] [CrossRef]
- Waldman, S.D. CHAPTER 221—Evoked Potential Testing. In Pain Review; Waldman, S.D., Ed.; W.B. Saunders: Philadelphia, PA, USA, 2009; pp. 372–375. [Google Scholar]
- Uk, M.; Al, E. Clinical Neurophysiology, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2010. [Google Scholar]
- Nolan, J.P.; Soar, J.; Cariou, A.; Cronberg, T.; Moulaert, V.R.; Deakin, C.D.; Bottiger, B.W.; Friberg, H.; Sunde, K.; Sandroni, C. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines for Post-resuscitation Care 2015: Section 5 of the European Resuscitation Council Guidelines for Resuscitation 2015. Resuscitation 2015, 95, 202–222. [Google Scholar] [CrossRef]
- Sandroni, C.; D’Arrigo, S.; Nolan, J.P. Prognostication after cardiac arrest. Crit Care 2018, 22, 150. [Google Scholar] [CrossRef] [Green Version]
- Tjepkema-Cloostermans, M.C.; Horn, J. Somatosensory Evoked Potentials in Patients with Hypoxic-Ischemic Brain Injury. Semin. Neurol. 2017, 37, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Scarpino, M.; Lolli, F.; Lanzo, G.; Carrai, R.; Spalletti, M.; Valzania, F.; Lombardi, M.; Audenino, D.; Contardi, S.; Celani, M.G.; et al. Do changes in SSEP amplitude over time predict the outcome of comatose survivors of cardiac arrest? Resuscitation 2022, 181, 133–139. [Google Scholar] [CrossRef]
- van Soest, T.M.; Van Rootselaar, A.F.; Admiraal, M.M.; Potters, W.V.; Koelman, J.H.; Horn, J. SSEP amplitudes add information for prognostication in postanoxic coma. Resuscitation 2021, 163, 172–175. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.; Kurfess, J.; Treggiari, M.M. Basics of Neuromonitoring and Anesthetic Considerations. Anesthesiol. Clin. 2021, 39, 195–209. [Google Scholar] [CrossRef] [PubMed]
- Singh, G. Somatosensory evoked potential monitoring. J. Neuroanaesth. Crit. Care 2018, 3, S97–S104. [Google Scholar] [CrossRef]
- Scarpino, M.; Lolli, F.; Lanzo, G.; Carrai, R.; Spalletti, M.; Valzania, F.; Lombardi, M.; Audenino, D.; Contardi, S.; Celani, M.G.; et al. SSEP amplitude accurately predicts both good and poor neurological outcome early after cardiac arrest; a post-hoc analysis of the ProNeCA multicentre study. Resuscitation 2021, 163, 162–171. [Google Scholar] [CrossRef]
- Cho, S.-M.; Choi, C.W.; Whitman, G.; Suarez, J.I.; Martinez, N.C.; Geocadin, R.G.; Ritzl, E.K. Neurophysiological Findings and Brain Injury Pattern in Patients on ECMO. Clin. EEG Neurosci. 2021, 52, 462–469. [Google Scholar] [CrossRef]
- Caturegli, G.; Zhang, L.Q.; Mayasi, Y.; Gusdon, A.M.; Ergin, B.; Ponomarev, V.; Kim, B.S.; Keller, S.; Geocadin, R.G.; Whitman, G.J.R.; et al. Characterization of Cerebral Hemodynamics with TCD in Patients Undergoing VA-ECMO and VV-ECMO: A Prospective Observational Study. Neurocritical Care 2022, 38, 407–413. [Google Scholar] [CrossRef]
- Caturegli, G.; Kapoor, S.; Ponomarev, V.; Kim, B.S.; Whitman, G.J.; Ziai, W.; Cho, S.-M.; Zhang, L.Q.; Mayasi, Y.; Gusdon, A.; et al. Transcranial Doppler microemboli and acute brain injury in extracorporeal membrane oxygenation: A prospective observational study. JTCVS Technol. 2022, 15, 111–122. [Google Scholar] [CrossRef]
- Petermichl, W.; Philipp, A.; Hiller, K.-A.; Foltan, M.; Floerchinger, B.; Graf, B.; Lunz, D. Reliability of prognostic biomarkers after prehospital extracorporeal cardiopulmonary resuscitation with target temperature management. Scand. J. Trauma, Resusc. Emerg. Med. 2021, 29, 147. [Google Scholar] [CrossRef]
- Nolan, J.P.; Sandroni, C.; Böttiger, B.W.; Cariou, A.; Cronberg, T.; Friberg, H.; Genbrugge, C.; Haywood, K.; Lilja, G.; Moulaert, V.R.M.; et al. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines 2021: Post-resuscitation care. Resuscitation 2021, 161, 220–269. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, S.; Braga, F.; Luksch, R.; Terenziani, M.; Caruso, S.; Panteghini, M. Measurement of Serum Neuron-Specific Enolase in Neuroblastoma: Is There a Clinical Role? Clin. Chem. 2020, 66, 667–675. [Google Scholar] [CrossRef]
- Böttiger, B.W.; Möbes, S.; Glätzer, R.; Bauer, H.; Gries, A.; Bärtsch, P.; Motsch, J.; Martin, E. Astroglial Protein S-100 Is an Early and Sensitive Marker of Hypoxic Brain Damage and Outcome After Cardiac Arrest in Humans. Circulation 2001, 103, 2694–2698. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.-H.; Chang, W.-T.; Su, K.-I.; Huang, C.-H.; Tsai, M.-S.; Chou, E.; Lu, T.-C.; Chen, W.-J.; Lee, C.-C.; Chen, S.-C. Neuroprognostic accuracy of blood biomarkers for post-cardiac arrest patients: A systematic review and meta-analysis. Resuscitation 2020, 148, 108–117. [Google Scholar] [CrossRef]
- Bembea, M.M.; Rizkalla, N.; Freedy, J.; Barasch, N.; Vaidya, D.; Pronovost, P.J.; Everett, A.D.; Mueller, G. Plasma Biomarkers of Brain Injury as Diagnostic Tools and Outcome Predictors After Extracorporeal Membrane Oxygenation*. Crit. Care Med. 2015, 43, 2202–2211. [Google Scholar] [CrossRef] [PubMed]
- Hoiland, R.L.; Rikhraj, K.J.; Thiara, S.; Fordyce, C.; Kramer, A.H.; Skrifvars, M.B.; Cheryl, L.W.; Donald, E.G.; Nicholas, A.F.; Mypinder, S. Sekhon Neurologic Prognostication After Cardiac Arrest Using Brain Biomarkers: A Systematic Review and Meta-analysis. JAMA Neurol 2022, 79, 390–398. [Google Scholar] [CrossRef]
- Illum, B.; Odish, M.; Minokadeh, A.; Yi, C.; Owens, R.L.; Pollema, T.; LaBuzetta, J.N. Evaluation, Treatment, and Impact of Neurologic Injury in Adult Patients on Extracorporeal Membrane Oxygenation: A Review. Curr. Treat. Options Neurol. 2021, 23, 15. [Google Scholar] [CrossRef]
- Gutierrez, L.G.; Rovira, À.; Portela, L.A.P.; Leite, C.D.C.; Lucato, L. CT and MR in non-neonatal hypoxic–ischemic encephalopathy: Radiological findings with pathophysiological correlations. Neuroradiology 2010, 52, 949–976. [Google Scholar] [CrossRef]
- Huang, B.Y.; Castillo, M. Hypoxic-Ischemic Brain Injury: Imaging Findings from Birth to Adulthood. Radiographics 2008, 28, 417–439. [Google Scholar] [CrossRef] [PubMed]
- Zotzmann, V.; Rilinger, J.; Lang, C.N.; Duerschmied, D.; Benk, C.; Bode, C.; Wengenmayer, T.; Staudacher, D.L. Early full-body computed tomography in patients after extracorporeal cardiopulmonary resuscitation (eCPR). Resuscitation 2020, 146, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Barrett, K.M.; Freeman, W.D.; Weindling, S.M.; Brott, T.G.; Broderick, D.F.; Heckman, M.G.; Crook, J.E.; Divertie, G.D.; Meschia, J.F. Brain Injury After Cardiopulmonary Arrest and Its Assessment With Diffusion-Weighted Magnetic Resonance Imaging. Mayo Clin. Proc. 2007, 82, 828–835. [Google Scholar] [CrossRef] [Green Version]
- Greer, D.; Scripko, P.; Bartscher, J.; Sims, J.; Camargo, E.; Singhal, A.; Furie, K. Serial MRI Changes in Comatose Cardiac Arrest Patients. Neurocritical Care 2011, 14, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.-M.; Wilcox, C.; Keller, S.; Acton, M.; Rando, H.; Etchill, E.; Giuliano, K.; Bush, E.L.; Sair, H.I.; Pitts, J.; et al. Assessing the SAfety and FEasibility of bedside portable low-field brain Magnetic Resonance Imaging in patients on ECMO (SAFE-MRI ECMO study): Study protocol and first case series experience. Crit. Care 2022, 26, 119. [Google Scholar] [CrossRef]
- Sheth, K.N.; Mazurek, M.H.; Yuen, M.M.; Cahn, B.A.; Shah, J.T.; Ward, A.; Kim, J.A.; Gilmore, E.J.; Falcone, G.J.; Petersen, N.; et al. Assessment of Brain Injury Using Portable, Low-Field Magnetic Resonance Imaging at the Bedside of Critically Ill Patients. JAMA Neurol. 2020, 78, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Beekman, R.; Crawford, A.; Mazurek, M.H.; Prabhat, A.M.; Chavva, I.R.; Parasuram, N.; Kim, N.; Kim, J.A.; Petersen, N.; de Havenon, A.; et al. Bedside monitoring of hypoxic ischemic brain injury using low-field, portable brain magnetic resonance imaging after cardiac arrest. Resuscitation 2022, 176, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Shoskes, A.; Migdady, I.; Amin, M.; Hasan, L.; Price, C.; Uchino, K.; Choi, C.W.; Hernandez, A.V.; Cho, S.-M. Does Targeted Temperature Management Improve Neurological Outcome in Extracorporeal Cardiopulmonary Resuscitation (ECPR)? J. Intensive Care Med. 2022, 37, 157–167. [Google Scholar] [CrossRef]
- Kim, Y.S.; Cho, Y.H.; Sung, K.; Ryu, J.-A.; Chung, C.R.; Suh, G.Y.; Yang, J.H.; Yang, J.-H. Target Temperature Management May Not Improve Clinical Outcomes of Extracorporeal Cardiopulmonary Resuscitation. J. Intensiv. Care Med. 2018, 34, 790–796. [Google Scholar] [CrossRef]
- Levy, B.; Girerd, N.; Amour, J.; Besnier, E.; Nesseler, N.; Helms, J.; Delmas, C.; Sonneville, R.; Guidon, C.; Rozec, B. Effect of Moderate Hypothermia vs Normothermia on 30-Day Mortality in Patients with Cardiogenic Shock Receiving Venoarterial Extracorporeal Membrane Oxygenation: A Randomized Clinical Trial. JAMA 2022, 327, 442–453. [Google Scholar] [CrossRef]
- Dankiewicz, J.; Cronberg, T.; Lilja, G.; Jakobsen, J.C.; Levin, H.; Ullén, S.; Rylander, C.; Wise, M.P.; Oddo, M.; Cariou, A.; et al. Hypothermia versus Normothermia after Out-of-Hospital Cardiac Arrest. N. Engl. J. Med. 2021, 384, 2283–2294. [Google Scholar] [CrossRef]
- Nolan, J.P.; Sandroni, C.; Andersen, L.W.; Böttiger, B.W.; Cariou, A.; Cronberg, T.; Friberg, H.; Genbrugge, C.; Lilja, G.; Morley, P.T.; et al. ERC-ESICM guidelines on temperature control after cardiac arrest in adults. Resuscitation 2022, 172, 229–236. [Google Scholar] [CrossRef]
- Laptook, A.R.; Corbett, R.J. The effects of temperature on hypoxic-ischemic brain injury. Clin. Perinatol. 2002, 29, 623–649. [Google Scholar] [CrossRef]
- Balu, R.; Rajagopalan, S.; Baghshomali, S.; Kirschen, M.; Amurthur, A.; Kofke, W.A.; Abella, B.S. Cerebrovascular pressure reactivity and intracranial pressure are associated with neurologic outcome after hypoxic-ischemic brain injury. Resuscitation 2021, 164, 114–121. [Google Scholar] [CrossRef]
- Sekhon, M.S.; Griesdale, D.E.; Ainslie, P.N.; Gooderham, P.; Foster, D.; Czosnyka, M.; Robba, C.; Cardim, D. Intracranial pressure and compliance in hypoxic ischemic brain injury patients after cardiac arrest. Resuscitation 2019, 141, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Fergusson, N.A.; Hoiland, R.L.; Thiara, S.; Foster, D.; Gooderham, P.; Rikhraj, K.; Grunau, B.; Christenson, J.; Ainslie, P.N.; Griesdale, D. EGGoal-Directed Care Using Invasive Neuromonitoring Versus Standard of Care After Cardiac Arrest: A Matched Cohort Study. Crit Care Med. 2021, 49, 1333–1346. [Google Scholar] [PubMed]
- Schulz-Stübner, S.; Thiex, R. Raising the head-of-bed by 30 degrees reduces ICP and improves CPP without compromising cardiac output in euvolemic patients with traumatic brain injury and subarachnoid haemorrhage: A practice audit. Eur. J. Anaesthesiol. 2006, 23, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Callaway, C.W.; Donnino, M.W.; Fink, E.L.; Geocadin, R.G.; Golan, E.; Kern, K.B.; Leary, M.; Meurer, W.J.; Peberdy, M.A.; Thompson, T.M. Part 8: Post-Cardiac Arrest Care: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132 (Suppl. 2), S465–S482. [Google Scholar] [CrossRef] [Green Version]
- Carney, N.; Totten, A.M.; O’Reilly, C.; Ullman, J.S.; Hawryluk, G.W.; Bell, M.J.; Bratton, S.L.; Chesnut, R.; Harris, O.A.; Kissoon, N.; et al. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery 2016, 80, 6–15. [Google Scholar] [CrossRef]
- Farrokh, S.; Cho, S.M.; Suarez, J.I. Fluids and hyperosmolar agents in neurocritical care: An update. Curr. Opin. Crit. Care 2019, 25, 105–109. [Google Scholar] [CrossRef]
- Meloni, B.P. Pathophysiology and Neuroprotective Strategies in Hypoxic-Ischemic Brain Injury and Stroke. Brain Sci. 2017, 7, 110. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Population Characteristics | |||||
| Author, Year | Study Design | Sample Size (n) | Inclusion Criteria | Risk Factors | Overall (%) |
| Cho, 2020 [12] | Retrospective Cohort (Autopsy) | 25 | ECMO (88% VA-ECMO) | Hypertension history, high day 1 lactate level, low pH level | ABI (68%) HIBI (44%) |
| Shoskes, 2020 [16] | Systematic Review and Meta-analysis | 16,063 | VA-ECMO vs. VV-ECMO | Cannulation method (VA-ECMO) | VA-ECMO vs. VV-ECMO: ABI (19% vs. 10%; p = 0.002) HIBI (13% vs. 1%; p < 0.001) |
| Shou, 2022 [17] | Retrospective Cohort | 129 | VA-ECMO | High pre-cannulation PaCO2, large peri-cannulation PaCO2 drop (ΔPaCO2) | ABI (33%) HIBI (12%) |
| Shou, 2022 [23] | Retrospective Cohort | 123 | VA-ECMO | Early low pulse pressure (<20 mmHg) | ABI (33%) HIBI (11%) |
| Author, Year | Objective | Animal | Size | ECMO Type | ECMO Duration | Intervention | HIBI Findings |
|---|---|---|---|---|---|---|---|
| Foerster, 2013 [42] | To investigate the effect of anticoagulation during ECPR | Pig | 12 | ECPR | 60 min | ECPR (80–100 mL/kg/min) started after 15 min of cardiac arrest No anticoagulation before ECPR reperfusion (n = 6) Heparinized saline solution flush (n = 3) Anticoagulant-coated cannulae and normal saline solution flush (n = 3) | No difference between the two groups Brain histology after 7 days of cardiac arrest in both groups showed dark neurons and eosinophilic neurons in hippocampus, cerebellum, and frontal lobe |
| Putzer, 2021 [43] | To investigate options for the use of ECPR without preceding systemic heparinization after cardiac arrest and the effect on survival and neurological outcome | Pig | 14 | ECPR | 10 min | ECPR (30 mL/kg/min) started after 8 min of cardiac arrest Adrenaline infusion for goal MAP 40 (n = 7) vs. MAP 60 (n = 7) | Microdialysis markers (lactate, pyruvate, and lactate to pyruvate ratio) significantly decreased in MAP 60 group with adrenaline infusion |
| Rozencwajg, 2023 [44] | To study the impact of the ECMO flow on brain injury | Sheep | 6 | VA-ECMO | 300 min | Low-flow at 2.5 L/min (n = 3) High-flow at 4.5 L/min (n = 3) | Neuronal shrinkage, congestion, and perivascular edema were higher in the low-flow group PbtO2 levels were lower in the low-flow group NIRS was lower in the low-flow group |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khanduja, S.; Kim, J.; Kang, J.K.; Feng, C.-Y.; Vogelsong, M.A.; Geocadin, R.G.; Whitman, G.; Cho, S.-M. Hypoxic-Ischemic Brain Injury in ECMO: Pathophysiology, Neuromonitoring, and Therapeutic Opportunities. Cells 2023, 12, 1546. https://doi.org/10.3390/cells12111546
Khanduja S, Kim J, Kang JK, Feng C-Y, Vogelsong MA, Geocadin RG, Whitman G, Cho S-M. Hypoxic-Ischemic Brain Injury in ECMO: Pathophysiology, Neuromonitoring, and Therapeutic Opportunities. Cells. 2023; 12(11):1546. https://doi.org/10.3390/cells12111546
Chicago/Turabian StyleKhanduja, Shivalika, Jiah Kim, Jin Kook Kang, Cheng-Yuan Feng, Melissa Ann Vogelsong, Romergryko G. Geocadin, Glenn Whitman, and Sung-Min Cho. 2023. "Hypoxic-Ischemic Brain Injury in ECMO: Pathophysiology, Neuromonitoring, and Therapeutic Opportunities" Cells 12, no. 11: 1546. https://doi.org/10.3390/cells12111546