Correlation of the ALA-PDT Treatment Efficacy and the HPV Genotype Profile of Genital Warts after Cryotherapy Failure and Podophyllotoxin Therapy in Male Patients

 , , ,
, , ,
Abstract
:1. Introduction
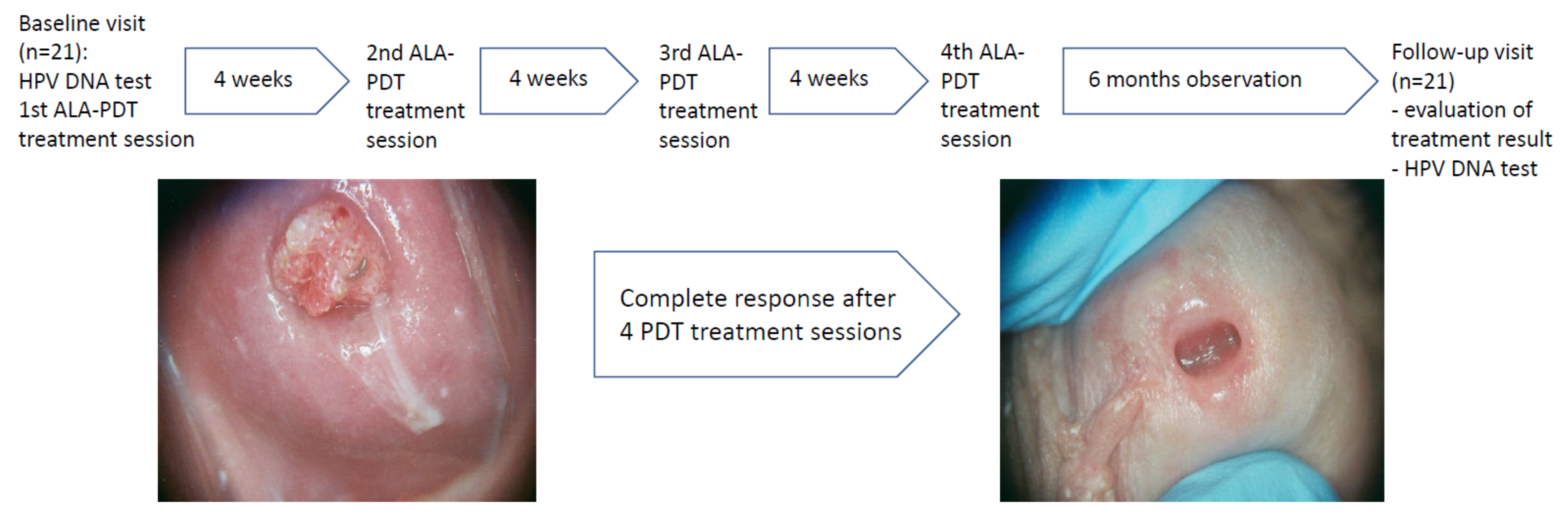
2. Material and Methods
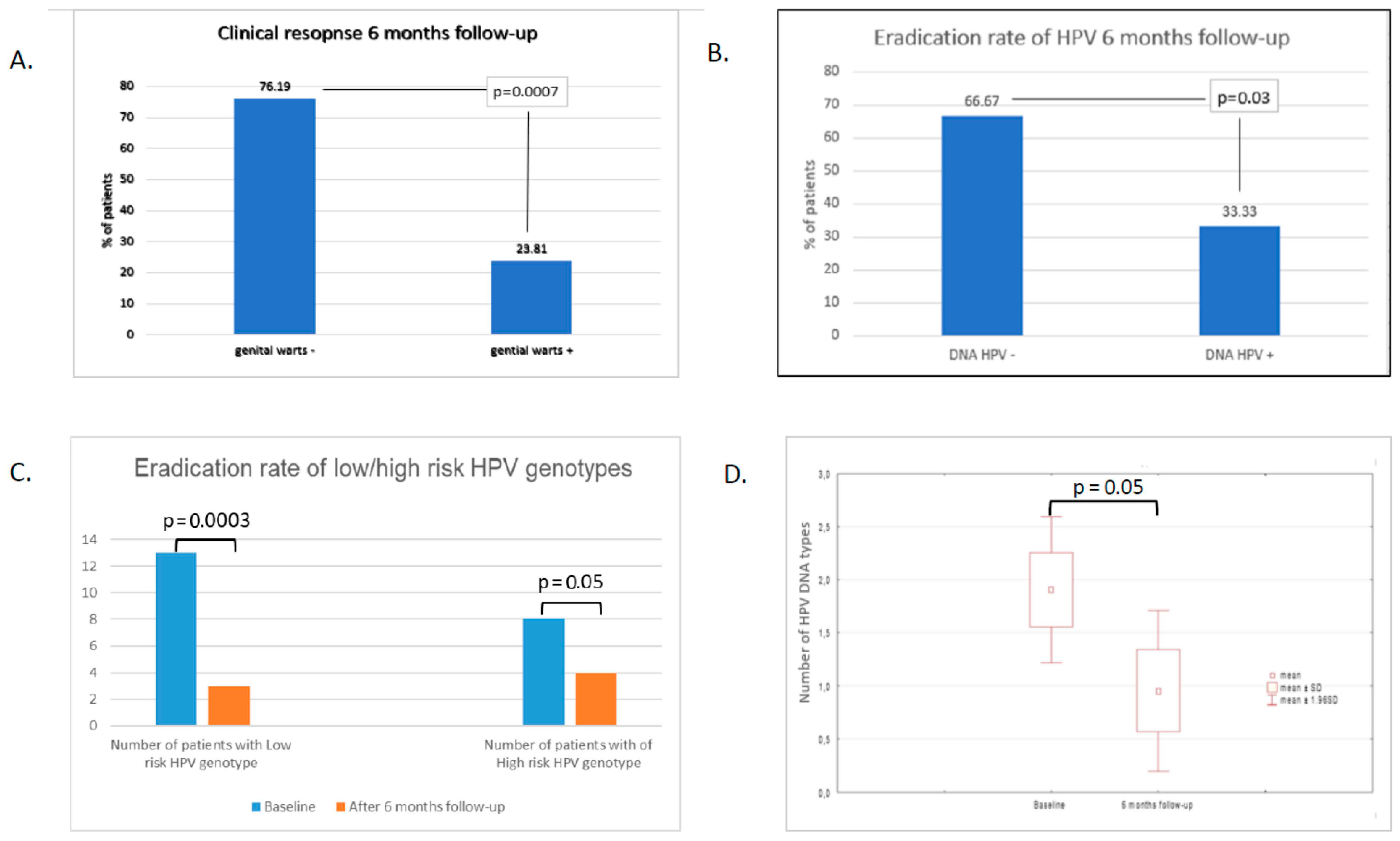
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Clanner-Engelshofen, B.M.; Marsela, E.; Engelsberger, N.; Guertler, A.; Schauber, J.; French, L.E.; Reinholz, M. Condylomata acuminata: A retrospective analysis on clinical characteristics and treatment options. Heliyon 2020, 6, e03547. [Google Scholar] [CrossRef]
- Dunne, E.F.; Nielson, C.M.; Stone, K.M.; Markowitz, L.E.; Giuliano, A.R. Prevalence of HPV Infection among Men: A Systematic Review of the Literature. J. Infect. Dis. 2006, 194, 1044–1057. [Google Scholar] [CrossRef] [PubMed]
- Ockenfels, H.M. Therapeutic management of cutaneous and genital warts. J. Dtsch. Dermatol. Ges. 2016, 14, 892–899. [Google Scholar] [CrossRef] [Green Version]
- Farahmand, M.; Moghoofei, M.; Dorost, A.; Abbasi, S.; Monavari, S.H.; Kiani, S.J.; Tavakoli, A. Prevalence and genotype distribution of genital human papillomavirus infection in female sex workers in the world: A systematic review and meta-analysis. BMC Public Health 2020, 20, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Liu, L.; Zhang, W.; Liu, H.; Li, J.; Jiang, L.; Zeng, K. Dynamics of HPV viral loads reflect the treatment effect of photodynamic therapy in genital warts. Photodiagnosis Photodyn. Ther. 2018, 21, 86–90. [Google Scholar] [CrossRef]
- Hawkins, M.G.; Winder, D.M.; Ball, S.L.R.; Vaughan, K.; Sonnex, C.; Stanley, M.A.; Sterling, J.C.; Goon, P.K.C. Detection of specific HPV subtypes responsible for the pathogenesis of condylomata acuminata. Virol. J. 2013, 10, 1–137. [Google Scholar] [CrossRef] [Green Version]
- Al-Awadhi, R.; Al-Mutairi, N.; Albatineh, A.N.; Chehadeh, W. Association of HPV genotypes with external anogenital warts: A cross sectional study. BMC Infect. Dis. 2019, 19, 375. [Google Scholar] [CrossRef]
- O’Mahony, C.; Gomberg, M.; Skerlev, M.; Alraddadi, A.; Heras-Alonso, M.D.L.; Majewski, S.; Nicolaidou, E.; Serdaroğlu, S.; Kutlubay, Z.; Tawara, M.; et al. Position statement for the diagnosis and management of anogenital warts. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1006–1019. [Google Scholar] [CrossRef] [Green Version]
- Yanofsky, V.R.; Patel, R.V.; Goldenberg, G. Genital warts: A comprehensive review. J. Clin. Aesthet. Dermatol. 2012, 5, 25–36. [Google Scholar] [PubMed]
- Du, J.; Lu, X.-N.; Li, F.; Wang, D.-Q.; Xu, M.; Sun, Y.; Liang, J.; Tang, H.; Yang, Y.-S.; Zhang, Z.; et al. Comparison between photodynamic therapy with topical application of 5-aminolevulinic acid and CO2 laser therapy in the treatment of cervical condylomata acuminate: A randomized controlled trial. Int. J. Clin. Exp. Med. 2015, 8, 11342–11346. [Google Scholar] [PubMed]
- Hu, Y.-E.; Dai, S.-F.; Wang, B.; Qu, W.; Gao, J.-L. Therapeutic effects of topical 5-aminolevulinic acid photodynamic therapy. Pak. J. Med Sci. 1969, 32, 961–964. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, S.; Li, J.; Li, Z.; Wang, Q.; Peng, X.; Shi, M.; Che, Q.; Liu, H.; Jiang, L.; et al. Evaluation of human papillomavirus DNA detection-guided aminolaevulinic acid-mediated photodynamic therapy for the treatment of condyloma acuminata. Photodiagnosis Photodyn. Ther. 2019, 28, 114–119. [Google Scholar] [CrossRef]
- Zhang, Z.; Lu, X.-N.; Liang, J.; Tang, H.; Yang, Y.-S.; Zhu, X.-H.; Du, J.; Shen, Y.-Y.; Xu, J.-H. Evaluation of photodynamic therapy using topical aminolevulinic acid hydrochloride in the treatment of condylomata acuminate. Int. J. Clin. Exp. Med. 2015, 8, 6517–6521. [Google Scholar] [PubMed]
- Wen, X.; Li, Y.; Hamblin, M.R. Photodynamic therapy in dermatology beyond non-melanoma cancer: An update. Photodiagnosis Photodyn. Ther. 2017, 19, 140–152. [Google Scholar] [CrossRef]
- Giuliano, A.R.; Lee, J.-H.; Fulp, W.; Villa, L.L.; Lazcano, E.; Papenfuss, M.R.; Abrahamsen, M.; Salmeron, J.; Anic, G.M.; Rollison, D.E.; et al. Incidence and clearance of genital human papillomavirus infection in men (HIM): A cohort study. Lancet 2011, 377, 932–940. [Google Scholar] [CrossRef] [Green Version]
- Lu, B.; Wu, Y.; Nielson, C.M.; Flores, R.; Abrahamsen, M.; Papenfuss, M.; Harris, R.B.; Giuliano, A.R. Factors Associated with Acquisition and Clearance of Human Papillomavirus Infection in a Cohort of US Men: A Prospective Study. J. Infect. Dis. 2009, 199, 362–371. [Google Scholar] [CrossRef] [Green Version]
- Giuliano, A.R.; Lazcano-Ponce, E.; Villa, L.L.; Flores, R.; Salmeron, J.; Lee, J.-H.; Papenfuss, M.R.; Abrahamsen, M.; Jolles, E.; Nielson, C.M.; et al. The Human Papillomavirus Infection in Men Study: Human Papillomavirus Prevalence and Type Distribution among Men Residing in Brazil, Mexico, and the United States. Cancer Epidemiol. Biomark. Prev. 2008, 17, 2036–2043. [Google Scholar] [CrossRef] [Green Version]
- Doorbar, J. Latent papillomavirus infections and their regulation. Curr. Opin. Virol. 2013, 3, 416–421. [Google Scholar] [CrossRef]
- Hu, Z.; Li, J.; Liu, H.; Liu, L.; Jiang, L.; Zeng, K. Treatment of latent or subclinical Genital HPV Infection with 5-aminolevulinic acid-based photodynamic therapy. Photodiagnosis Photodyn. Ther. 2018, 23, 362–364. [Google Scholar] [CrossRef]
- Blomberg, M.F.S.; Munk, C.; Bautz, A.; Kjaer, S.K. Genital warts and risk of cancer: A danish study of nearly 50,000 patients with genital warts. J. Infect. Dis. 2012, 205, 1544–1553. [Google Scholar] [CrossRef]
- Hasanzadeh, M.; Rejali, M.; Mehramiz, M.; Akbari, M.; Seresht, L.M.; Yazdandoost, Y.; Farokhi, S.; Mahdian, Z.; Maleki, F.; Emamdadi-Aliabad, Z.; et al. The interaction of high and low-risk human papillomavirus genotypes increases the risk of developing genital warts: A population-based cohort study. J. Cell. Biochem. 2019, 120, 12870–12874. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, S.R.; Le, T.; Lockhart, A.; Sanusi, A.; Santo, L.D.; Davis, M.; McKinney, D.A.; Brown, M.; Poole, C.; Willame, C.; et al. Patterns of persistent HPV infection after treatment for cervical intraepithelial neoplasia (CIN): A systematic review. Int. J. Cancer 2017, 141, 8–23. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.K.; Barankin, B.; Leong, K.F.; Hon, K.L. Penile warts: An update on their evaluation and management. Drugs Context 2018, 7, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Lopaschuk, C.C. New approach to managing genital warts. Can. Fam. Physician Med. Fam. Can. 2013, 59, 731–736. [Google Scholar]
- Gilson, R.; Nugent, D.; Werner, R.; Ballesteros, J.; Ross, J. 2019 IUSTI-Europe guideline for the management of anogenital warts. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1644–1653. [Google Scholar] [CrossRef]
- Canel, C.; Moraes, R.M.; Dayan, F.E.; Ferreira, D. Podophyllotoxin. Phytochemistry 2000, 54, 115–120. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age | Site of Genital Warts | HPV Genotype before PDT Treatment | PDT Treatment Cycles | Response after 4 PDT Treatment Cycles | HPV Genotype Testing after 6 Months Follow-up |
|---|---|---|---|---|---|
| 49 | Penis | 6 | 4 | CR | Not detected |
| 30 | Penis, Perianal area | 6,16,18,59 | 4 | PR | 6,16,18,59 |
| 27 | Penis, Perianal area | 6,31,39,45,51 | 4 | CR | 31,39,45 |
| 43 | Penis | 6 | 4 | CR | Not detected |
| 39 | Penis | 18,58 | 4 | CR | Not detected |
| 28 | Penis | 6 | 4 | CR | Not detected |
| 29 | Penis | 6 | 4 | CR | Not detected |
| 27 | Penis, Perianal area | 6 | 4 | CR | Not detected |
| 25 | Penis | 6 | 4 | PR | 6 |
| 32 | Penis | 51 | 4 | CR | Not detected |
| 58 | Penis | 6,16,51,52,56,59 | 4 | PR | 6,16,35,51,52,56,59 |
| 37 | Penis, Perianal area | 11,33,56,58 | 4 | CR | Not detected |
| 25 | Penis | 6 | 4 | CR | Not detected |
| 29 | Penis, Perianal area | 6 | 4 | CR | Not detected |
| 29 | Penis, Perianal area | 56 | 4 | PR | 56 |
| 22 | Penis | 6 | 4 | CR | Not detected |
| 30 | Penis | 6,11,31,58 | 4 | CR | Not detected |
| 28 | Penis, Perianal area | 6 | 4 | PR | 6,51 |
| 25 | Penis | 6 | 4 | CR | Not detected |
| 47 | Penis | 6 | 4 | CR | 16 |
| 39 | Penis | 6 | 4 | CR | Not detected |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Owczarek, W.; Slowinska, M.; Walecka, I.; Ciazynska, M.; Nowicka, D.; Walczak, L.; Paluchowska, E. Correlation of the ALA-PDT Treatment Efficacy and the HPV Genotype Profile of Genital Warts after Cryotherapy Failure and Podophyllotoxin Therapy in Male Patients. Life 2021, 11, 146. https://doi.org/10.3390/life11020146
Owczarek W, Slowinska M, Walecka I, Ciazynska M, Nowicka D, Walczak L, Paluchowska E. Correlation of the ALA-PDT Treatment Efficacy and the HPV Genotype Profile of Genital Warts after Cryotherapy Failure and Podophyllotoxin Therapy in Male Patients. Life. 2021; 11(2):146. https://doi.org/10.3390/life11020146
Chicago/Turabian StyleOwczarek, Witold, Monika Slowinska, Irena Walecka, Magdalena Ciazynska, Dorota Nowicka, Leszek Walczak, and Elwira Paluchowska. 2021. "Correlation of the ALA-PDT Treatment Efficacy and the HPV Genotype Profile of Genital Warts after Cryotherapy Failure and Podophyllotoxin Therapy in Male Patients" Life 11, no. 2: 146. https://doi.org/10.3390/life11020146