
Incidence of Asymptomatic Shigella Infection and Association with the Composite Index of Anthropometric Failure among Children Aged 1–24 Months in Low-Resource Settings

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Assessment of Nutritional Status
2.4. Laboratory Testing
2.5. Statistical Analysis
2.6. Ethics Statement
3. Results
3.1. General Characteristics
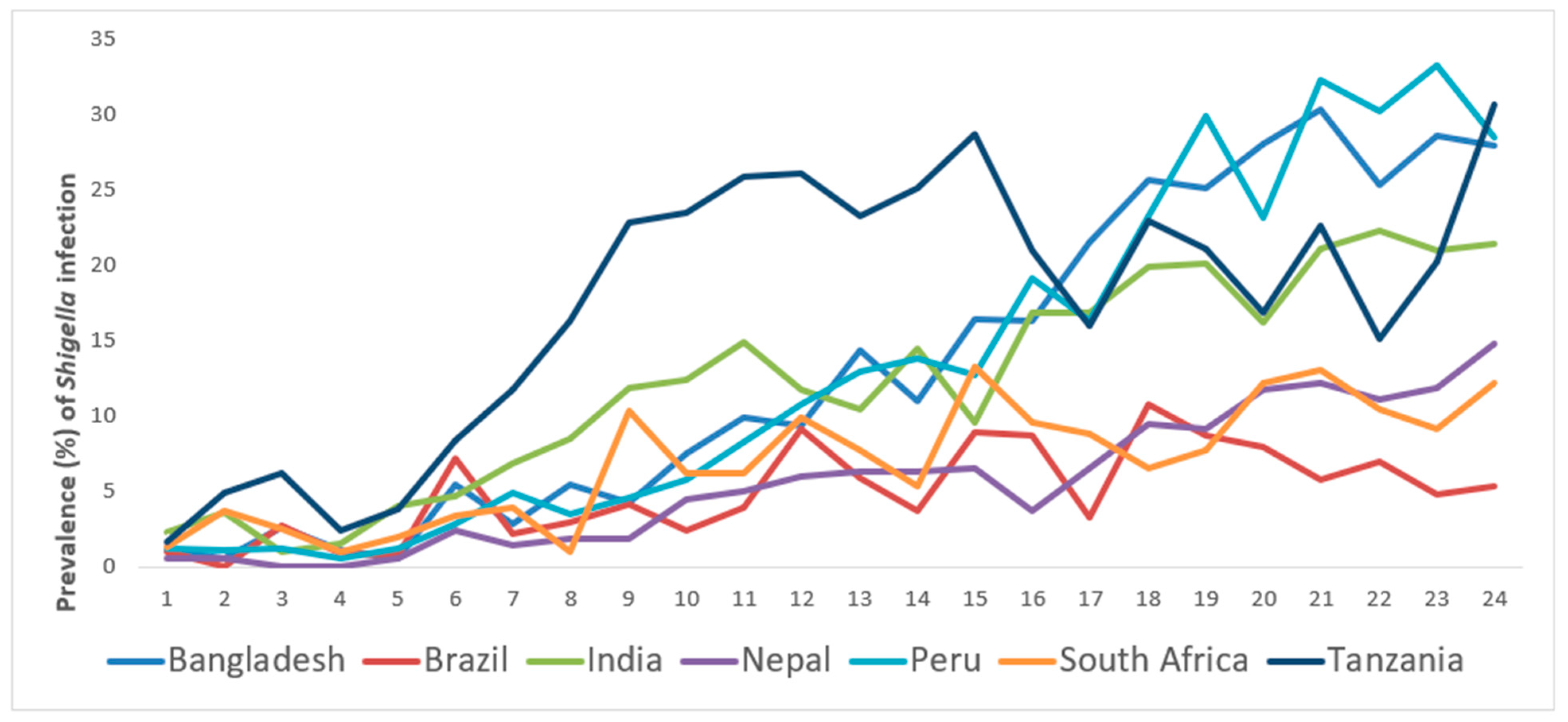
3.2. Incidence Rate of Asymptomatic Shigella Infection
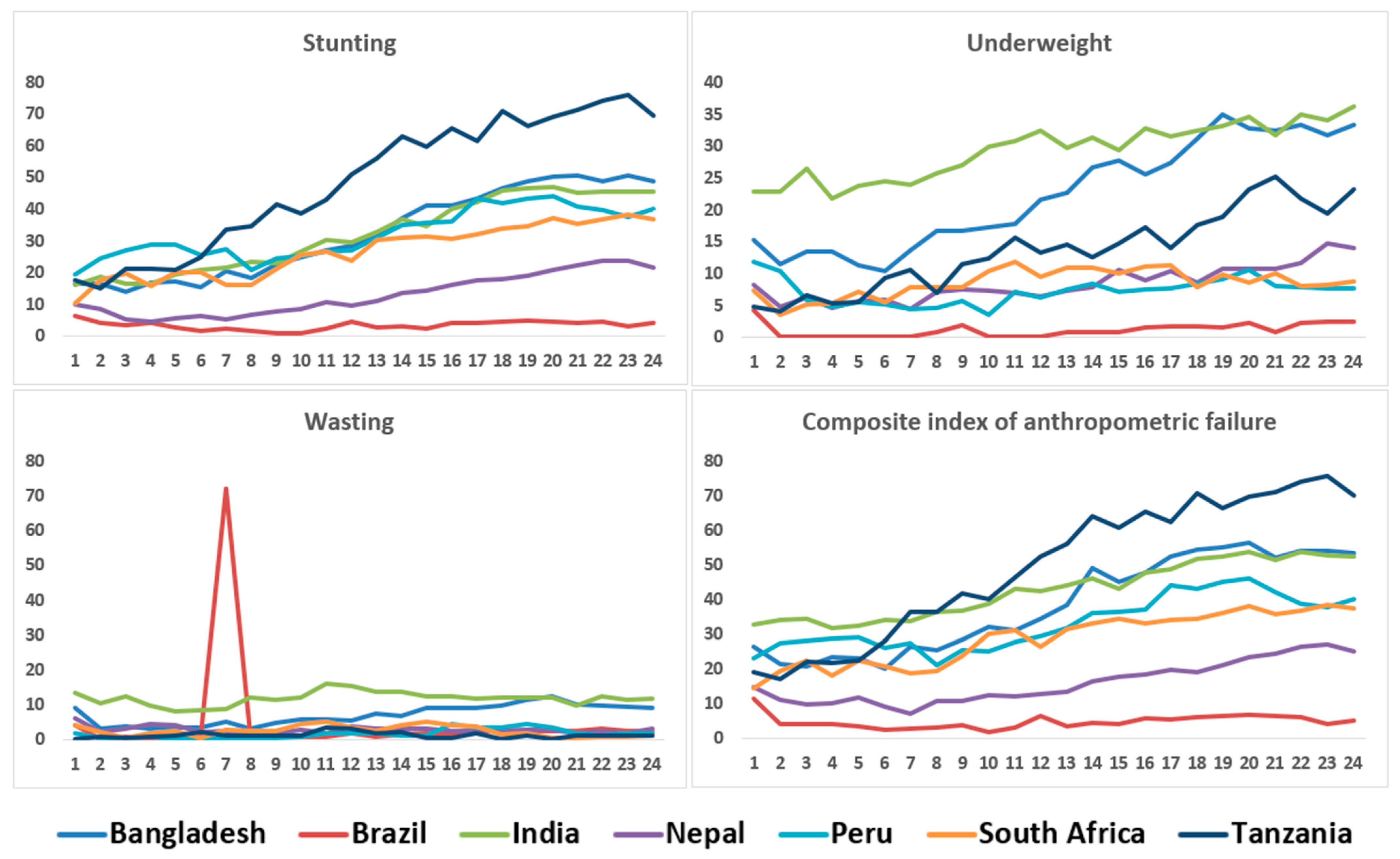
3.3. Association between Asymptomatic Shigella Infection and Childhood Malnutrition
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rogawski McQuade, E.T.; Shaheen, F.; Kabir, F.; Rizvi, A.; Platts-Mills, J.A.; Aziz, F.; Kalam, A.; Qureshi, S.; Elwood, S.; Liu, J.; et al. Epidemiology of Shigella infections and diarrhea in the first two years of life using culture-independent diagnostics in 8 low-resource settings. PLoS Negl. Trop. Dis. 2020, 14, e0008536. [Google Scholar] [CrossRef]
- Bengtsson, R.J.; Simpkin, A.J.; Pulford, C.V.; Low, R.; Rasko, D.A.; Rigden, D.J.; Hall, N.; Barry, E.M.; Tennant, S.M.; Baker, K.S. Pathogenomic analyses of Shigella isolates inform factors limiting shigellosis prevention and control across LMICs. Nat. Microbiol. 2022, 7, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Duchen, D.; Haque, R.; Chen, L.; Wojcik, G.; Korpe, P.; Nayak, U.; Mentzer, A.J.; Kirkpatrick, B.; Petri, W.A., Jr.; Duggal, P.J.I.; et al. Host Genome-Wide Association Study of Infant Susceptibility to Shigella-Associated Diarrhea. Infect. Immun. 2021, 89, e00012–e00021. [Google Scholar] [CrossRef] [PubMed]
- Khalil, I.A.; Troeger, C.; Blacker, B.F.; Rao, P.C.; Brown, A.; Atherly, D.E.; Brewer, T.G.; Engmann, C.M.; Houpt, E.R.; Kang, G.; et al. Morbidity and mortality due to shigella and enterotoxigenic Escherichia coli diarrhoea: The Global Burden of Disease Study 1990–2016. Lancet Infect. Dis. 2018, 18, 1229–1240. [Google Scholar] [CrossRef] [Green Version]
- Williams, P.C.; Berkley, J.A. Guidelines for the treatment of dysentery (shigellosis): A systematic review of the evidence. Paediatr. Int. Child Health 2018, 38, S50–S65. [Google Scholar] [CrossRef] [Green Version]
- Rogawski, E.T.; Guerrant, R.L. The burden of enteropathy and “subclinical” infections. Pediatric Clin. N. Am. 2017, 64, 815–836. [Google Scholar] [CrossRef]
- Ghosh, S.; Pazhani, G.P.; Niyogi, S.K.; Nataro, J.P.; Ramamurthy, T. Genetic characterization of Shigella spp. isolated from diarrhoeal and asymptomatic children. J. Med. Microbiol. 2014, 63, 903–910. [Google Scholar] [CrossRef]
- Tadesse, G.; Mitiku, H.; Teklemariam, Z.; Marami, D. Salmonella and Shigella Among Asymptomatic Street Food Vendors in the Dire Dawa city, Eastern Ethiopia: Prevalence, Antimicrobial Susceptibility Pattern, and Associated Factors. Environ. Health Insights 2019, 13, 1178630219853581. [Google Scholar] [CrossRef] [Green Version]
- Swaminathan, S.; Hemalatha, R.; Pandey, A.; Kassebaum, N.J.; Laxmaiah, A.; Longvah, T.; Lodha, R.; Ramji, S.; Kumar, G.A.; Afshin, A.; et al. The burden of child and maternal malnutrition and trends in its indicators in the states of India: The Global Burden of Disease Study 1990–2017. Lancet Child Adolesc. Health 2019, 3, 855–870. [Google Scholar] [CrossRef] [Green Version]
- Olofin, I.; McDonald, C.M.; Ezzati, M.; Flaxman, S.; Black, R.E.; Fawzi, W.W.; Caulfield, L.E.; Danaei, G.; for the Nutrition Impact Model Study (anthropometry cohort pooling). Associations of suboptimal growth with all-cause and cause-specific mortality in children under five years: A pooled analysis of ten prospective studies. PLoS ONE 2013, 8, e64636. [Google Scholar] [CrossRef] [Green Version]
- Rogawski, E.T.; Liu, J.; Platts-Mills, J.A.; Kabir, F.; Lertsethtakarn, P.; Siguas, M.; Khan, S.S.; Praharaj, I.; Murei, A.; Nshama, R.; et al. Use of quantitative molecular diagnostic methods to investigate the effect of enteropathogen infections on linear growth in children in low-resource settings: Longitudinal analysis of results from the MAL-ED cohort study. Lancet Glob. Health 2018, 6, e1319–e1328. [Google Scholar] [CrossRef] [Green Version]
- Platts-Mills, J.A.; Taniuchi, M.; Uddin, M.J.; Sobuz, S.U.; Mahfuz, M.; Gaffar, S.A.; Mondal, D.; Hossain, M.I.; Islam, M.M.; Ahmed, A.S.; et al. Association between enteropathogens and malnutrition in children aged 6–23 mo in Bangladesh: A case-control study. Am. J. Clin. Nutr. 2017, 105, 1132–1138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, M.S.; Biswas, T. Prevalence and correlates of the composite index of anthropometric failure among children under 5 years old in Bangladesh. Matern. Child Nutr. 2020, 16, e12930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porwal, A.; Acharya, R.; Ashraf, S.; Agarwal, P.; Ramesh, S.; Khan, N.; Sarna, A.; Johnston, R. Socio-economic inequality in anthropometric failure among children aged under 5 years in India: Evidence from the Comprehensive National Nutrition Survey 2016–18. Int. J. Equity Health 2021, 20, 176. [Google Scholar] [CrossRef] [PubMed]
- Svedberg, P. Poverty and Undernutrition: Theory, Measurement, and Policy; Stockholm University: Stockholm, Sweden, 2000. [Google Scholar]
- Hasso-Agopsowicz, M.; Lopman, B.A.; Lanata, C.F.; McQuade, E.T.R.; Kang, G.; Prudden, H.J.; Khalil, I.; Platts-Mills, J.A.; Kotloff, K.; Jit, M.; et al. World Health Organization Expert Working Group: Recommendations for assessing morbidity associated with enteric pathogens. Vaccine 2021, 39, 7521–7525. [Google Scholar] [CrossRef]
- Hausdorff, W.P.; Scheele, S.; Giersing, B.K. What Drives the Value of a Shigella Vaccine? Vaccines 2022, 10, 282. [Google Scholar] [CrossRef]
- Livio, S.; Strockbine, N.A.; Panchalingam, S.; Tennant, S.M.; Barry, E.M.; Marohn, M.E.; Antonio, M.; Hossain, A.; Mandomando, I.; Ochieng, J.B.; et al. Shigella isolates from the global enteric multicenter study inform vaccine development. Clin. Infect. Dis. 2014, 59, 933–941. [Google Scholar] [CrossRef]
- Taylor, D.N.; Trofa, A.; Sadoff, J.; Chu, C.; Bryla, D.; Shiloach, J.; Cohen, D.; Ashkenazi, S.; Lerman, Y.; Egan, W.J.I.; et al. Synthesis, characterization, and clinical evaluation of conjugate vaccines composed of the O-specific polysaccharides of Shigella dysenteriae type 1, Shigella flexneri type 2a, and Shigella sonnei (Plesiomonas shigelloides) bound to bacterial toxoids. Infect. Immun. 1993, 61, 3678–3687. [Google Scholar] [CrossRef] [Green Version]
- Ravenscroft, N.; Braun, M.; Schneider, J.; Dreyer, A.M.; Wetter, M.; Haeuptle, M.A.; Kemmler, S.; Steffen, M.; Sirena, D.; Herwig, S.; et al. Characterization and immunogenicity of a Shigella flexneri 2a O-antigen bioconjugate vaccine candidate. Glycobiology 2019, 29, 669–680. [Google Scholar] [CrossRef]
- Cohen, D.; Atsmon, J.; Artaud, C.; Meron-Sudai, S.; Gougeon, M.-L.; Bialik, A.; Goren, S.; Asato, V.; Ariel-Cohen, O.; Reizis, A.; et al. Safety and immunogenicity of a synthetic carbohydrate conjugate vaccine against Shigella flexneri 2a in healthy adult volunteers: A phase 1, dose-escalating, single-blind, randomised, placebo-controlled study. Lancet Infect. Dis. 2021, 21, 546–558. [Google Scholar] [CrossRef]
- Kotloff, K.L.; Taylor, D.N.; Sztein, M.B.; Wasserman, S.S.; Losonsky, G.A.; Nataro, J.P.; Venkatesan, M.; Hartman, A.; Picking, W.D.; Katz, D.E.; et al. Phase I evaluation of ΔvirG Shigella sonnei live, attenuated, oral vaccine strain WRSS1 in healthy adults. Infect. Immun. 2002, 70, 2016–2021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barry, E.M.; Pasetti, M.F.; Sztein, M.B.; Fasano, A.; Kotloff, K.L.; Levine, M.M. Progress and pitfalls in Shigella vaccine research. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 245–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MAL-ED Network Investigators. The MAL-ED study: A multinational and multidisciplinary approach to understand the relationship between enteric pathogens, malnutrition, gut physiology, physical growth, cognitive development, and immune responses in infants and children up to 2 years of age in resource-poor environments %J Clinical Infectious Diseases. Clin. Infect. Dis. 2014, 59, S193–S206. [Google Scholar]
- Psaki, S.R.; Seidman, J.C.; Miller, M.; Gottlieb, M.; Bhutta, Z.A.; Ahmed, T.; Ahmed, A.S.; Bessong, P.; John, S.M.; Kang, G.; et al. Measuring socioeconomic status in multicountry studies: Results from the eight-country MAL-ED study. Popul. Health Metr. 2014, 12, 8. [Google Scholar] [CrossRef] [Green Version]
- WHO/UNICEF. WHO/UNICEF Joint Monitoring Programme for Water Supply and Sanitation. Progress on Drinking Water and Sanitation. Available online: https://www.unwater.org/publication_categories/whounicef-joint-monitoring-programme-for-water-supply-sanitation-hygiene-jmp/ (accessed on 14 April 2016).
- Richard, S.A.; Barrett, L.J.; Guerrant, R.L.; Checkley, W.; Miller, M.A. Disease surveillance methods used in the 8-site MAL-ED cohort study. Clin. Infect. Dis. 2014, 59, S220–S224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houpt, E.; Gratz, J.; Kosek, M.; Zaidi, A.K.; Qureshi, S.; Kang, G.; Babji, S.; Mason, C.; Bodhidatta, L.; Samie, A. Microbiologic methods utilized in the MAL-ED cohort study. Clin. Infect. Dis. 2014, 59, S225–S232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. WHO Child Growth Standards: Length/height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age, Methods and Development; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Kosek, M.; Guerrant, R.L.; Kang, G.; Bhutta, Z.; Yori, P.P.; Gratz, J.; Gottlieb, M.; Lang, D.; Lee, G.; Haque, R.; et al. Assessment of environmental enteropathy in the MAL-ED cohort study: Theoretical and analytic framework. Clin. Infect. Dis. 2014, 59, S239–S247. [Google Scholar] [CrossRef]
- Kosek, M.N.; Ahmed, T.; Bhutta, Z.; Caulfield, L.; Guerrant, R.; Houpt, E.; Kang, G.; Kosek, M.; Lee, G.; Lima, A.J.E. Causal pathways from enteropathogens to environmental enteropathy: Findings from the MAL-ED birth cohort study. EBioMedicine 2017, 18, 109–117. [Google Scholar] [CrossRef]
- Liu, J.; Kabir, F.; Manneh, J.; Lertsethtakarn, P.; Begum, S.; Gratz, J.; Becker, S.M.; Operario, D.J.; Taniuchi, M.; Janaki, L.; et al. Development and assessment of molecular diagnostic tests for 15 enteropathogens causing childhood diarrhoea: A multicentre study. Lancet Infect. Dis. 2014, 14, 716–724. [Google Scholar] [CrossRef]
- Platts-Mills, J.A.; Liu, J.; Rogawski, E.T.; Kabir, F.; Lertsethtakarn, P.; Siguas, M.; Khan, S.S.; Praharaj, I.; Murei, A.; Nshama, R.; et al. Use of quantitative molecular diagnostic methods to assess the aetiology, burden, and clinical characteristics of diarrhoea in children in low-resource settings: A reanalysis of the MAL-ED cohort study. Lancet Glob. Health 2018, 6, e1309–e1318. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Gratz, J.; Amour, C.; Nshama, R.; Walongo, T.; Maro, A.; Mduma, E.; Platts-Mills, J.; Boisen, N.; Nataro, J.; et al. Optimization of quantitative PCR methods for enteropathogen detection. PLoS ONE 2016, 11, e0158199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taniuchi, M.; Platts-Mills, J.A.; Begum, S.; Uddin, M.J.; Sobuz, S.U.; Liu, J.; Kirkpatrick, B.D.; Colgate, E.R.; Carmolli, M.P.; Dickson, D.M.; et al. Impact of enterovirus and other enteric pathogens on oral polio and rotavirus vaccine performance in Bangladeshi infants. Vaccine 2016, 34, 3068–3075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Platts-Mills, J.A.; Juma, J.; Kabir, F.; Nkeze, J.; Okoi, C.; Operario, D.J.; Uddin, J.; Ahmed, S.; Alonso, P.L.; et al. Use of quantitative molecular diagnostic methods to identify causes of diarrhoea in children: A reanalysis of the GEMS case-control study. Lancet Infect. Dis. 2016, 388, 1291–1301. [Google Scholar]
- Bagamian, K.H.; Anderson IV, J.D.; Muhib, F.; Cumming, O.; Laytner, L.A.; Wierzba, T.F.; Rheingans, R. Heterogeneity in enterotoxigenic Escherichia coli and shigella infections in children under 5 years of age from 11 African countries: A subnational approach quantifying risk, mortality, morbidity, and stunting. Lancet Glob. Health 2020, 8, e101–e112. [Google Scholar] [CrossRef] [Green Version]
- Reiner, R.C., Jr.; Graetz, N.; Casey, D.C.; Troeger, C.; Garcia, G.M.; Mosser, J.F.; Deshpande, A.; Swartz, S.J.; Ray, S.E.; Blacker, B.F.; et al. Variation in childhood diarrheal morbidity and mortality in Africa, 2000–2015. N. Engl. J. Med. 2018, 379, 1128–1138. [Google Scholar] [CrossRef] [PubMed]
- Amour, C.; Gratz, J.; Mduma, E.; Svensen, E.; Rogawski, E.T.; McGrath, M.; Seidman, J.C.; McCormick, B.J.; Shrestha, S.; Samie, A.; et al. Epidemiology and impact of campylobacter infection in children in 8 low-resource settings: Results from the MAL-ED study. Clin. Infect. Dis. 2016, 63, 1171–1179. [Google Scholar]
- Mahbub, M.M.; Ahsan, C.R.; Yasmin, M.; Nessa, J. Analysis of Different Prognostic Indicators for Malnutrition and Shigella flexneri Infection Among the Children in Bangladesh. Indian J. Med. 2012, 52, 400–405. [Google Scholar] [CrossRef]
- Hien, B.T.T.; Scheutz, F.; Cam, P.D.; Serichantalergs, O.; Huong, T.T.; Thu, T.M.; Dalsgaard, A. Diarrheagenic Escherichia coli and Shigella strains isolated from children in a hospital case-control study in Hanoi, Vietnam. J. Clin. Microbiol. 2008, 46, 996–1004. [Google Scholar] [CrossRef] [Green Version]
- Albert, M.J.; Faruque, A.; Faruque, S.; Sack, R.; Mahalanabis, D. Case-control study of enteropathogens associated with childhood diarrhea in Dhaka, Bangladesh. J. Clin. Microbiol. 1999, 37, 3458–3464. [Google Scholar] [CrossRef] [Green Version]
- McQuade, E.T.R.; Clark, S.; Bayo, E.; Scharf, R.J.; DeBoer, M.D.; Patil, C.L.; Gratz, J.C.; Houpt, E.R.; Svensen, E.; Mduma, E.R.; et al. Seasonal food insecurity in Haydom, Tanzania, is associated with low birthweight and acute malnutrition: Results from the MAL-ED study. Am. J. Trop. Med. Hyg. 2019, 100, 681. [Google Scholar] [CrossRef] [Green Version]
- Mazumder, R.N.; Hoque, S.S.; Ashraf, H.; Kabir, I.; Wahed, M.A. Early feeding of an energy dense diet during acute shigellosis enhances growth in malnourished children. Community Int. Nutr. 1997, 127, 51–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, K.H. Diarrhea and malnutrition. J. Nutr. 2003, 133, 328S–332S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Speelman, P.; Kabir, I.; Islam, M. Distribution and spread of colonic lesions in shigellosis: A colonoscopic study. J. Infect. Dis. 1984, 150, 899–903. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E.; Levine, M. Intestinal protein loss in shigellosis. Nutr. Res. 1991, 11, 1215–1220. [Google Scholar] [CrossRef]
- McDonald, C.M.; Olofin, I.; Flaxman, S.; Fawzi, W.W.; Spiegelman, D.; Caulfield, L.E.; Black, R.E.; Ezzati, M.; Danaei, G.; on behalf of the Nutrition Impact Model Study. The effect of multiple anthropometric deficits on child mortality: Meta-analysis of individual data in 10 prospective studies from developing countries. Am. J. Clin. Nutr. 2013, 97, 896–901. [Google Scholar] [CrossRef] [Green Version]
- Khamis, A.G.; Mwanri, A.W.; Kreppel, K.; Kwesigabo, G. The burden and correlates of childhood undernutrition in Tanzania according to composite index of anthropometric failure. BMC Nutr. 2020, 6, 39. [Google Scholar] [CrossRef]
- Nahar, B.; Hossain, M.; Mahfuz, M.; Islam, M.M.; Hossain, M.I.; Murray-Kolb, L.E.; Seidman, J.C.; Ahmed, T. Early childhood development and stunting: Findings from the MAL-ED birth cohort study in Bangladesh. Matern. Child Nutr. 2020, 16, e12864. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, T.; Hossain, M.; Mahfuz, M.; Choudhury, N.; Ahmed, S. Imperatives for reducing child stunting in Bangladesh. Matern. Child Nutr. 2016, 12 (Suppl. 1), 242–245. [Google Scholar] [CrossRef] [Green Version]
- Modern, G.; Sauli, E.; Mpolya, E. Correlates of diarrhea and stunting among under-five children in Ruvuma, Tanzania; a hospital-based cross-sectional study. Sci. Afr. 2020, 8, e00430. [Google Scholar] [CrossRef]
- Canella, D.S.; Duran, A.C.; Claro, R.M. Malnutrition in all its forms and social inequalities in Brazil. Public Health Nutr. 2020, 23, s29–s38. [Google Scholar] [CrossRef]
- Lima, A.A.; Leite, Á.M.; Di Moura, A.; Lima, N.L.; Soares, A.M.; Abreu, C.B.; Quirino Filho, J.; Mota, R.M.; Lima, I.F.; Havt, A. Determinant variables, enteric pathogen burden, gut function, and immune-related inflammatory biomarkers associated with childhood malnutrition: A prospective case-control study in Northeastern Brazil. Pediatric Infect. Dis. J. 2017, 36, 1177. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics, n (%) | Bangladesh | Brazil | India | Nepal | Peru | Pakistan | South Africa | Tanzania | Overall |
|---|---|---|---|---|---|---|---|---|---|
| Male sex | 108 (51.4) | 89 (53.9) | 105 (46.3) | 122 (53.7) | 105 (54.1) | 120 (48.8) | 120 (50.6) | 105 (50.2) | 874 (51.0) |
| Birth weight (kg) † | 2.8 ± 0.4 | 3.4 ± 0.5 | 2.9 ± 0.4 | 3 ± 0.4 | 3.1 ± 0.4 | 2.7 ± 0.4 | 3.2 ± 0.5 | 3.2 ± 0.5 | 3.0 ± 0.5 |
| Days of exclusive breastfeeding † | 143.2 ± 42.7 | 93.7 ± 57.8 | 105.4 ± 42.9 | 92.5 ± 54.5 | 89.5 ± 61.3 | 19.9 ± 22.7 | 38.6 ± 26.3 | 62.2 ± 35 | 78.6 ± 57.7 |
| Weight for age z-score at enrolment † | −1.3 ± 0.9 | −0.2 ± 1 | −1.3 ± 1 | −0.9 ± 1 | −0.6 ± 0.9 | −1.4 ± 1 | −0.4 ± 1 | −0.1 ± 0.9 | −0.8 ± 1.1 |
| Length for age z-score at enrolment † | −0.96 ± 1 | −0.8 ± 1.1 | −1 ± 1.1 | −0.7 ± 1 | −0.9 ± 1 | −1.3 ± 1.1 | −0.7 ± 1 | −1 ± 1.1 | −0.9 ± 1.1 |
| Length for age z-score at 24 months † | −2.0 ± 0.9 | 0 ± 1.1 | −1.9 ± 1 | −1.3 ± 0.9 | −1.9 ± 0.9 | N/A | −1.7 ± 1.1 | −2.7 ± 1 | −1.7 ± 1.2 |
| Maternal age (years) † | 25.0 ± 5.0 | 25.4 ± 5.6 | 23.9 ± 4.2 | 26.6 ± 3.7 | 24.8 ± 6.3 | 28.1 ± 5.9 | 27 ± 7.2 | 29.1 ± 6.5 | 26.3 ± 5.9 |
| Maternal weight (kg) † | 49.7 ± 8.5 | 62 ± 11.5 | 50.3 ± 9.3 | 56.2 ± 8.3 | 56.3 ± 9.6 | 50.7 ± 9.6 | 68 ± 15.3 | 55.7 ± 8.8 | 55.9 ± 12 |
| Maternal height (cm) † | 149.0 ± 5.0 | 155.1 ± 6.7 | 151.1 ± 5.2 | 149.7 ± 5.3 | 150.2 ± 5.5 | 153.4 ± 5.7 | 158.7 ± 6.6 | 155.9 ± 5.9 | 152.9 ± 6.6 |
| Maternal educational level < 6 y | 133 (63.3) | 22 (13.3) | 80 (35.2) | 59 (26) | 44 (22.7) | 202 (82.1) | 5 (2.1) | 75 (35.9) | 620 (36.2) |
| Mother has less than 3 alive children | 160 (76.2) | 113 (68.5) | 157 (69.8) | 199 (87.7) | 111 (57.2) | 105 (42.7) | 141 (59.5) | 58 (27.8) | 1044 (61) |
| Routine treatment of drinking water | 130 (61.9) | 10 (6.1) | 7 (3.1) | 98 (43.2) | 32 (16.5) | 0 (0) | 12 (5.1) | 12 (5.7) | 301 (17.6) |
| Improved drinking water source | 210 (100) | 165 (100) | 227 (100) | 227 (100) | 184 (94.9) | 246 (100) | 196 (82.7) | 89 (42.6) | 1544 (90.0) |
| Improved floor | 204 (97.1) | 165 (100) | 222 (97.8) | 109 (48) | 69 (35.6) | 81 (32.9) | 231 (97.5) | 13 (6.2) | 1094 (63.8) |
| Improved latrine | 210 (100) | 165 (100) | 121 (53.3) | 227 (100) | 66 (34) | 197 (80.1) | 232 (97.9) | 19 (9.1) | 1237 (72.1) |
| Monthly income < $150 | 69 (32.9) | 161 (97.6) | 19 (8.4) | 106 (46.7) | 58 (29.9) | 115 (46.8) | 179 (75.5) | 0 (0) | 707 (41.2) |
| Incidence Rate per 100 Child-Months (95% CI) | Adjusted Incidence Rate Ratio (95% CI) * | p Value | |
|---|---|---|---|
| Shigella | |||
| Overall | 10.78 (10.42, 11.16) | ||
| Bangladesh | 13.06 (12.02, 14.18) | Reference | |
| Brazil | 4.89 (4.15, 5.78) | 0.49 (0.39, 0.60) | <0.001 |
| India | 12.41 (11.45, 13.46) | 0.91 (0.81, 1.02) | 0.136 |
| Nepal | 5.75 (5.12, 6.45) | 0.49 (0.42, 0.57) | <0.001 |
| Peru | 13.63 (12.56, 14.79) | 1.04 (0.92, 1.16) | 0.549 |
| South Africa | 7.01 (6.28, 7.82) | 0.64 (0.55, 0.76) | <0.001 |
| Tanzania | 17.80 (16.57, 19.11) | 1.07 (0.91, 1.25) | 0.379 |
| Unadjusted OR (95% CI) | p Value | Adjusted OR (95% CI) | p Value | |
|---|---|---|---|---|
| Stunting [LAZ<-2] | ||||
| Overall | 1.54 (1.45, 1.62) | <0.001 | 1.60 (1.50, 1.70) | <0.001 |
| Bangladesh | 1.97 (1.73, 2.24) | <0.001 | 2.09 (1.81, 2.41) | <0.001 |
| Brazil | 1.36 (0.69, 2.64) | 0.368 | 1.33 (0.64, 2.79) | 0.447 |
| India | 1.40 (1.23, 1.58) | <0.001 | 1.41 (1.24, 1.61) | <0.001 |
| Nepal | 1.54 (1.24, 1.91) | <0.001 | 1.62 (1.26, 2.08) | <0.001 |
| Peru | 1.44 (1.26, 1.65) | <0.001 | 1.50 (1.29, 1.73) | <0.001 |
| South Africa | 1.32 (1.11, 1.57) | 0.002 | 1.35 (1.12, 1.63) | 0.002 |
| Tanzania | 1.58 (1.40, 1.79) | <0.001 | 1.65 (1.44, 1.89) | <0.001 |
| Wasting [WLZ<-2] | ||||
| Overall | 1.26 (1.10, 1.44) | 0.001 | 1.26 (1.09, 1.46) | 0.002 |
| Bangladesh | 1.49 (1.15, 1.93) | 0.003 | 1.50 (1.15, 1.95) | 0.003 |
| Brazil | 0.54 (0.16, 1.83) | 0.325 | 0.57 (0.14, 2.35) | 0.433 |
| India | 1.15 (0.95, 1.40) | 0.146 | 1.15 (0.95, 1.40) | 0.143 |
| Nepal | 1.22 (0.69, 2.20) | 0.487 | 1.24 (0.67, 2.29) | 0.488 |
| Peru | 0.47 (0.19, 1.12) | 0.088 | 0.45 (0.17, 1.19) | 0.109 |
| South Africa | 1.53 (0.88, 2.66) | 0.133 | 1.53 (0.88, 2.64) | 0.129 |
| Tanzania | 2.06 (1.13, 3.77) | 0.019 | 2.06 (1.12, 3.77) | 0.020 |
| Underweight [WAZ<-2] | ||||
| Overall | 1.42 (1.33, 1.51) | <0.001 | 1.45 (1.35, 1.56) | <0.001 |
| Bangladesh | 1.81 (1.58, 2.07) | <0.001 | 1.90 (1.64, 2.20) | <0.001 |
| Brazil | 0.52 (0.07, 3.93) | 0.529 | 0.56 (0.11, 2.85) | 0.485 |
| India | 1.31 (1.16, 1.48) | <0.001 | 1.31 (1.16, 1.48) | <0.001 |
| Nepal | 1.63 (1.28, 2.08) | <0.001 | 1.71 (1.27, 2.30) | <0.001 |
| Peru | 1.06 (0.84, 1.33) | 0.649 | 1.06 (0.82, 1.38) | 0.646 |
| South Africa | 1.36 (1.06, 1.76) | 0.016 | 1.38 (1.05, 1.80) | 0.019 |
| Tanzania | 1.38 (1.17, 1.63) | <0.001 | 1.40 (1.18, 1.68) | <0.001 |
| Composite index of anthropometric failure [LAZ<-2 or WLZ<-2 or WAZ<-2] | ||||
| Overall | 1.49 (1.41, 1.58) | <0.001 | 1.55 (1.46, 1.65) | <0.001 |
| Bangladesh | 1.95 (1.71, 2.22) | <0.001 | 2.02 (1.77, 2.33) | <0.001 |
| Brazil | 1.05 (0.58, 1.87) | 0.881 | 1.02 (0.58, 1.83) | 0.924 |
| India | 1.31 (1.16, 1.48) | <0.001 | 1.32 (1.16, 1.50) | <0.001 |
| Nepal | 1.54 (1.25, 1.89) | <0.001 | 1.61 (1.27, 2.04) | <0.001 |
| Peru | 1.39 (1.22, 1.59) | <0.001 | 1.45 (1.25, 1.67) | <0.001 |
| South Africa | 1.33 (1.12, 1.58) | 0.001 | 1.36 (1.13, 1.63) | 0.001 |
| Tanzania | 1.54 (1.36, 1.75) | <0.001 | 1.60 (1.40, 1.84) | <0.001 |
| Stunting and underweight only [LAZ<-2 and WAZ<-2] | ||||
| Overall | 1.42 (1.30, 1.56) | <0.001 | 1.42 (1.29, 1.56) | <0.001 |
| Bangladesh | 1.73 (1.45, 2.07) | <0.001 | 1.79 (1.47, 2.17) | <0.001 |
| Brazil | - | - | - | - |
| India | 1.29 (1.08, 1.54) | 0.005 | 1.27 (1.06, 1.52) | 0.011 |
| Nepal | 1.54 (1.09, 2.16) | 0.013 | 1.59 (1.08, 2.34) | 0.019 |
| Peru | 1.26 (0.94, 1.68) | 0.117 | 1.28 (0.94, 1.75) | 0.117 |
| South Africa | 1.23 (0.87, 1.73) | 0.238 | 1.24 (0.86, 1.77) | 0.246 |
| Tanzania | 1.37 (1.15, 1.65) | 0.001 | 1.40 (1.15, 1.69) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nasrin, S.; Haque, M.A.; Palit, P.; Das, R.; Mahfuz, M.; Faruque, A.S.G.; Ahmed, T. Incidence of Asymptomatic Shigella Infection and Association with the Composite Index of Anthropometric Failure among Children Aged 1–24 Months in Low-Resource Settings. Life 2022, 12, 607. https://doi.org/10.3390/life12050607
Nasrin S, Haque MA, Palit P, Das R, Mahfuz M, Faruque ASG, Ahmed T. Incidence of Asymptomatic Shigella Infection and Association with the Composite Index of Anthropometric Failure among Children Aged 1–24 Months in Low-Resource Settings. Life. 2022; 12(5):607. https://doi.org/10.3390/life12050607
Chicago/Turabian StyleNasrin, Sabiha, Md. Ahshanul Haque, Parag Palit, Rina Das, Mustafa Mahfuz, Abu S. G. Faruque, and Tahmeed Ahmed. 2022. "Incidence of Asymptomatic Shigella Infection and Association with the Composite Index of Anthropometric Failure among Children Aged 1–24 Months in Low-Resource Settings" Life 12, no. 5: 607. https://doi.org/10.3390/life12050607