
Stress of Prematurity in the Experience of the COVID-19 Pandemic—Current State of Knowledge
 ,
,  , ,
, , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Influence of COVID-19 on Pregnancy
3. Long-Term Complications Caused by Stress on Maternal and Offspring Outcomes
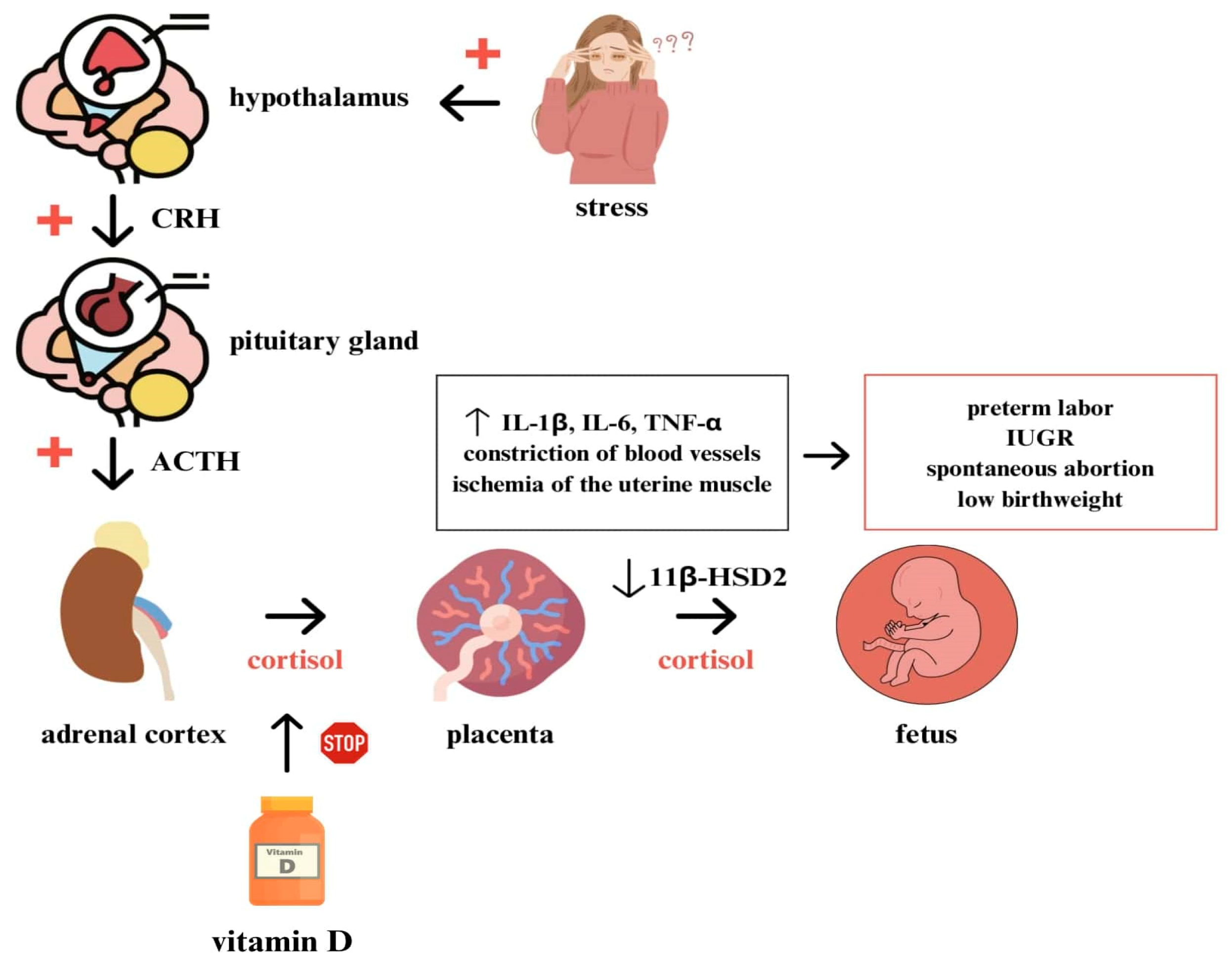
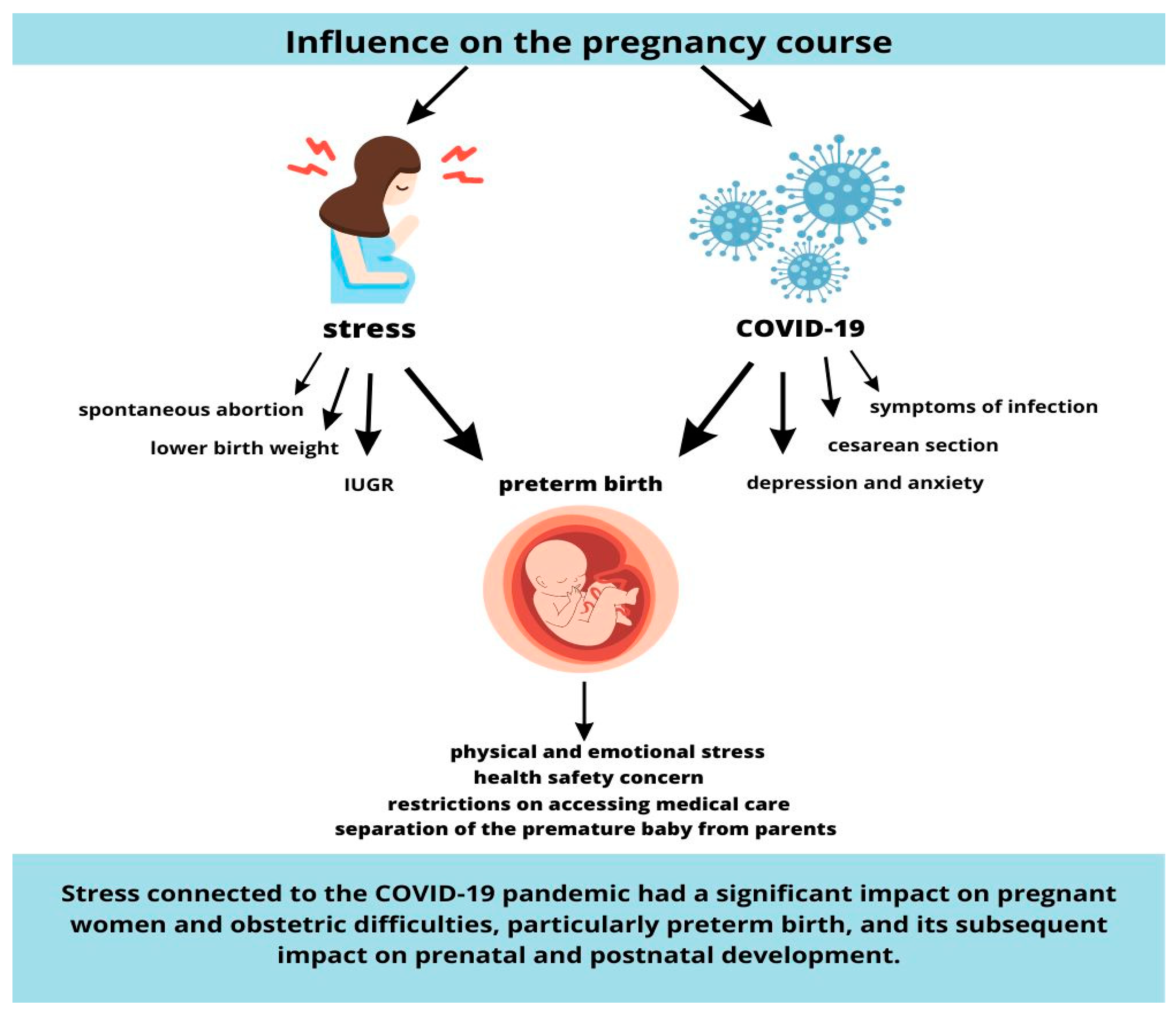
4. Influence of Stress on the Pregnancy Course
5. Influence of COVID-19 on the Pregnancy Course
6. Influence of Prematurity on the Mother and Family
7. The Impact of Vitamin D Deficiency Induced by the COVID-19 Pandemic on the Risk of Preterm Birth
- Impact on the Immune System:
- Regulation of Hormonal System:
- Inflammatory State:
- Impact on Vascular Function:
8. Influence of the COVID-19 Pandemic on the Stress
- Physical and emotional stress: Mothers of premature infants experience both physical and emotional stress, resulting from the need to adapt to new requirements related to caring for a premature baby in conditions of an epidemiological threat. In a published Italian study from 2021 that focused on the impact of the COVID-19 pandemic on parental stress, breastfeeding, and lactation success among mothers of premature infants whose children were in the neonatal intensive care unit (NICU), it was found that the availability of breast milk and breastfeeding decreased drastically (prior to the pandemic, the percentage of premature infants breastfed with breast milk was 86.1%, while during the pandemic, it was 44.8%). However, it was noted that the rate of breastfeeding was similar before and during the pandemic after the premature baby’s discharge from the hospital. Another study conducted by the University of Liverpool and the School of Health in Australia examined experiences related to the stress of prematurity using the social media platform Twitter. A total of 3161 tweets from parents of premature infants were analyzed. It was found that the COVID-19 pandemic and the associated restrictions, which affected parents’ contact with preterm infants, imposed significant emotional burdens on the studied group [76,80,88,89,90,91,92,93,94,95].
- Health safety concerns: Mothers of premature infants have heightened concerns about their children’s health in the context of the pandemic. These concerns primarily revolve around the risk of coronavirus infection, especially in the case of premature babies who are more susceptible to infections. This leads to increased anxiety and fear in women who have given birth before the due date. Spanish scientists from Torrecardenas University Hospital (between 2020 and 2022) focused on assessing the kangaroo mother care method in reducing anxiety and stress in women after preterm birth in the context of the COVID-19 pandemic. A cohort study was conducted on recruited mothers whose children were in the neonatal intensive care unit and participated in kangaroo mother care, and their stress levels were measured using the Parental Stressor: Neonatal Intensive Care Unit (PSS: NICU) scale and the STAI E/R questionnaire before and after implementing kangaroo care. It was proven that mothers in the group where kangaroo care had not yet been applied obtained higher scores on the PSS: NICU scale and the STAI E/R questionnaire compared to women who practiced kangaroo care. However, no statistically significant differences were found (p > 0.05). The result of this study highlights the importance of kangaroo care for the mental health of mothers, which was often impossible or limited during the COVID-19 pandemic. According to WHO, Kangaroo mother care has been demonstrated to reduce baby mortality by as much as 40%, hypothermia by more than 70%, and severe infections by 65% in infants delivered preterm or at low birthweight [76,80,88,89,90,91,92,93,94,95].
- Restrictions on accessing medical care: The COVID-19 pandemic and the associated restrictions significantly hindered access to medical care and contact with doctors. The difficult access to specialized medical care for premature infants, such as specialist doctor visits, rehabilitation, or diagnostics, created a higher level of stress for parents of preterm newborns. At the beginning of the pandemic noticed that clinics and rehabilitation centers suspended their operations during the lockdown, follow-up appointments, therapy, and psychological support services have been discontinued in many locations around the world. This has many parents extremely concerned for the unpredictable effects on their child’s health [76,80,88,89,90,91,92,93,94].
- Separation of the premature baby from parents: Uncertainty related to coronavirus infection and its health consequences necessitated extraordinary precautions and safety measures in medical facilities. During the initial phase of the pandemic, mothers were completely isolated from their newborn babies and often saw them for the first time after completion of treatment in the NICU. This prolonged separation caused significant anxiety and stress in mothers of premature infants [76,80,89,90,91,92,93,94].
- Altered care conditions: Due to the pandemic, the standard procedures for care in neonatal intensive care units (NICUs) had to be modified to ensure the safety of both healthcare staff and patients. These changes, such as the use of personal protective equipment (PPE) and limitations on visitation, created additional challenges and emotional strain for parents, particularly mothers of premature infants [76,80,89,90,91,92,93,94].
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- GUS. Rocznik Demograficzny. 2019. Available online: https://stat.gov.pl/obszary-tematyczne/roczniki-statystyczne/roczniki-statystyczne/rocznik-demograficzny-2019,3,13.html (accessed on 18 June 2023).
- Preterm Birth. Available online: https://www.who.int/en/news-room/fact-sheets/detail/preterm-birth (accessed on 18 June 2023).
- Khandre, V.; Potdar, J.; Keerti, A. Preterm Birth: An Overview. Cureus 2022, 14, e33006. [Google Scholar] [CrossRef] [PubMed]
- Allotey, J.; Fernandez, S.; Bonet, M.; Stallings, E.; Yap, M.; Kew, T.; Zhou, D.; Coomar, D.; Sheikh, J.; Lawson, H.; et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.D.; Zhu, L.J.; Yin, J.; Wen, J. Impacts of COVID-19 pandemic on preterm birth: A systematic review and meta-analysis. Public Health 2022, 213, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Hedermann, G.; Hedley, P.L.; Bækvad-Hansen, M.; Hjalgrim, H.; Rostgaard, K.; Poorisrisak, P.; Breindahl, M.; Melbye, M.; Hougaard, D.M.; Christiansen, M.; et al. Danish premature birth rates during the COVID-19 lockdown. Arch. Dis. Child Fetal Neonatal Ed. 2021, 106, 93–95. [Google Scholar] [CrossRef]
- Woodworth, K.R.; Olsen, E.O.; Neelam, V.; Lewis, E.L.; Galang, R.R.; Oduyebo, T.; Aveni, K.; Yazdy, M.M.; Harvey, E.; Longcore, N.D.; et al. Birth and Infant Outcomes Following Laboratory-Confirmed SARS-CoV-2 Infection in Pregnancy—SET-NET, 16 Jurisdictions, March 29–October 14. MMWR 2020, 69, 1635–1640. [Google Scholar] [CrossRef]
- Ellington, S.; Strid, P.; Tong, V.T.; Woodworth, K.; Galang, R.R.; Zambrano, L.D.; Nahabedian, J.; Anderson, K.; Gilboa, S.M. Characteristics of Women of Reproductive Age with Laboratory-Confirmed SARS-CoV-2 Infection by Pregnancy Status—United States, January 22–June 7. MMWR 2020, 69, 769–775. [Google Scholar] [CrossRef]
- Wang, H.; Li, N.; Sun, C.; Guo, X.; Su, W.; Song, Q.; Liang, Q.; Liang, M.; Ding, X.; Lowe, S.; et al. The association between pregnancy and COVID-19: A Systematic Review and Meta-analysis. Am. J. Emerg. Med. 2022, 56, 188–195. [Google Scholar] [CrossRef]
- Dashraath, P.; Wong, J.L.J.; Lim, M.X.K.; Lim, L.M.; Li, S.; Biswas, A.; Choolani, M.; Mattar, C.; Su, L.L. Coronavirus disease 2019 (COVID-19) pandemic and pregnancy. AJOG 2020, 222, 521–531. [Google Scholar] [CrossRef]
- Delahoy, M.J.; Whitaker, M.; O’Halloran, A.; Chai, S.J.; Kirley, P.D.; Alden, N.; Kawasaki, B.; Meek, J.; Yousey-Hindes, K.; Anderson, E.J.; et al. Meador, Characteristics and Maternal and Birth Outcomes of Hospitalized Pregnant Women with Laboratory-Confirmed COVID-19—COVID-NET, 13 States, March 1–August 22. MMWR 2020, 69, 1347–1354. [Google Scholar] [CrossRef]
- Singh, V.; Choudhary, A.; Datta, M.R.; Ray, A. Maternal and Neonatal Outcomes of COVID-19 in Pregnancy: A Single-Centre Observational Study. Cureus 2020, 13, e13184. [Google Scholar] [CrossRef]
- Smithgall, M.C.; Liu-Jarin, X.; Hamele-Bena, D.; Cimic, A.; Mourad, M.; Debelenko, L.; Chen, X. Third-trimester placentas of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-positive women: Histomorphology, including viral immunohistochemistry and in-situ hybridization. Histopathology 2020, 77, 994–999. [Google Scholar] [CrossRef] [PubMed]
- Shanes, E.D.; Mithal, L.B.; Otero, S.; Azad, H.A.; Miller, E.S.; Goldstein, J.A. Placental Pathology in COVID-19. Am. J. Clin. Pathol. 2020, 154, 23–32. [Google Scholar] [CrossRef]
- Ferraz, T.; Benton, S.J.; Zareef, I.; Aribaloye, O.; Bloise, E.; Connor, K.L. Impact of Co-Occurrence of Obesity and SARS-CoV-2 Infection during Pregnancy on Placental Pathologies and Adverse Birth Outcomes: A Systematic Review and Narrative Synthesis. Pathogens 2023, 12, 524. [Google Scholar] [CrossRef] [PubMed]
- Jafari, M.; Pormohammad, A.; Sheikh Neshin, S.A.; Ghorbani, S.; Bose, D.; Alimohammadi, S.; Basirjafari, S.; Mohammadi, M.; Rasmussen-Ivey, C.; Razizadeh, M.H.; et al. Clinical characteristics and outcomes of pregnant women with COVID-19 and comparison with control patients: A systematic review and meta-analysis. Rev. Med. Virol 2020, 31, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Wing, D.A.; Ortega-Villa, A.M.; Grobman, W.A.; Hediger, M.L.; Grewal, J.; Pugh, S.J.; Kim, S.; Newman, R.; Chien, E.; Owen, J.; et al. Maternal stress and neonatal anthropometry: The NICHD Fetal Growth Studies. Am. J. Obstet. Gynecol. 2017, 217, e1–e82. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, K.L.; Buss, C.; Wadhwa, P.D.; Entringer, S. The Interplay Between Nutrition and Stress in Pregnancy: Implications for Fetal Programming of Brain Development. Biol. Psychiatry 2019, 85, 135–149. [Google Scholar] [CrossRef]
- Nobile, S.; Di Sipio Morgia, C.; Vento, G. Perinatal Origins of Adult Disease and Opportunities for Health Promotion: A Narrative Review. J. Pers. Med. 2022, 12, 157. [Google Scholar] [CrossRef]
- Marciniak, A.; Patro-Małysza, J.; Kimber-Trojnar, Ż.; Marciniak, B.; Oleszczuk, J.; Leszczyńska-Gorzelak, B. Fetal programming of the metabolic syndrome. Taiwan J. Obstet. Gynecol. 2017, 56, 133–138. [Google Scholar] [CrossRef]
- Solano, M.E.; Holmes, M.C.; Mittelstadt, P.R.; Chapman, K.E.; Tolosa, E. Antenatal endogenous and exogenous glucocorticoids and their impact on immune ontogeny and long-term immunity. Semin. Immunopathol. 2016, 38, 739–763. [Google Scholar] [CrossRef]
- Elad, D.; Jaffa, A.J.; Grisaru, D.; Leibovitch, I. In Utero Programming of Testicular Cancer. J. Dev. Biol. 2021, 9, 35. [Google Scholar] [CrossRef] [PubMed]
- Heck, J.E.; He, D.; Janzen, C.; Federman, N.; Olsen, J.; Ritz, B.; Hansen, J. Fetal programming and Wilms tumor. Pediatr. Blood Cancer 2019, 66, e27461. [Google Scholar] [CrossRef]
- Sandman, C.A.; Davis, E.P.; Buss, C.; Glynn, L.M. Exposure to prenatal psychobiological stress exerts programming influences on the mother and her fetus. Neuroendocrinology 2012, 95, 7–21. [Google Scholar] [CrossRef]
- Herrera, C.L.; Bowman, M.E.; McIntire, D.D.; Nelson, D.B.; Smith, R. Revisiting the placental clock: Early corticotrophin-releasing hormone rise in recurrent preterm birth. PLoS ONE 2021, 16, e0257422. [Google Scholar] [CrossRef]
- Thomason, M.E.; Hect, J.L.; Waller, R.; Curtin, P. Interactive relations between maternal prenatal stress, fetal brain connectivity, and gestational age at delivery. Neuropsychopharmacology 2021, 46, 1839–1847. [Google Scholar] [CrossRef] [PubMed]
- Eberle, C.; Fasig, T.; Brüseke, F.; Stichling, S. Impact of maternal prenatal stress by glucocorticoids on metabolic and cardiovascular outcomes in their offspring: A systematic scoping review. PLoS ONE 2021, 16, e0245386. [Google Scholar] [CrossRef] [PubMed]
- Van den Bergh, B.R.H.; Van den Heuvel, M.I.; Lahti, M.; Braeken, M.; De Rooij, S.R.; Entringer, S.; Schwab, M. Prenatal developmental origins of behavior and mental health: The influence of maternal stress in pregnancy. Neurosci. Biobehav. Rev. 2017, 117, 26–64. [Google Scholar] [CrossRef]
- Kim, D.R.; Bale, T.L.; Epperson, C.N. Prenatal programming of mental illness: Current understanding of relationship and mechanisms. Curr. Psychiatry Rep. 2015, 17, 5. [Google Scholar] [CrossRef]
- Kinsley, C.H.; Trainer, R.; Stafisso-Sandoz, G.; Quadros, P.; Marcus, L.K.; Hearon, C.; Meyer, E.A.; Hester, N.; Morgan, M.; Kozub, F.J.; et al. Motherhood and the hormones of pregnancy modify concentrations of hippocampal neuronal dendritic spines. Horm. Behav. 2006, 49, 131–142. [Google Scholar] [CrossRef]
- Štěpáníková, I.; Baker, E.; Oates, G.; Bienertova-Vasku, J.; Klánová, J. Assessing Stress in Pregnancy and Postpartum: Comparing Measures. Matern. Child Health J. 2020, 24, 1193–1201. [Google Scholar] [CrossRef]
- Bertozzi, S.; Corradetti, B.; Seriau, L.; Diaz Ñañez, J.A.; Cedolini, C.; Fruscalzo, A.; Cesselli, D.; Cagnacci, A.; Londero, A.P. Nanotechnologies in Obstetrics and Cancer during Pregnancy: A Narrative Review. J. Pers. Med. 2022, 12, 1324. [Google Scholar] [CrossRef] [PubMed]
- Burns, E.R.; Farr, S.L.; Howards, P.P. Stressful life events experienced by women in the year before their infants’ births—United States, 2000–2010. Morb. Mortal. Wkly. Rep. 2015, 64, 247–251. [Google Scholar]
- Traylor, C.S.; Johnson, J.D.; Kimmel, M.C.; Manuck, T.A. Effects of psychological stress on adverse pregnancy outcomes and nonpharmacologic approaches for reduction: An expert review. Am. J. Obstet. Gynecol. MFM 2020, 2, 100229. [Google Scholar] [CrossRef] [PubMed]
- Lebel, C.; MacKinnon, A.; Bagshawe, M.; Tomfohr-Madsen, L.; Giesbrecht, G. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J. Affect. Disord. 2020, 277, 5–13. [Google Scholar] [CrossRef]
- Duthie, L.; Reynolds, R.M. Changes in the maternal hypothalamic-pituitary-adrenal axis in pregnancy and postpartum: Influences on maternal and fetal outcomes. Neuroendocrinology 2013, 98, 106–115. [Google Scholar] [CrossRef]
- Garcia-Flores, V.; Romero, R.; Furcron, A.E.; Levenson, D.; Galaz, J.; Zou, C.; Hassan, S.S.; Hsu, C.D.; Olson, D.; Metz, G.A.S.; et al. Prenatal Maternal Stress Causes Preterm Birth and Affects Neonatal Adaptive Immunity in Mice. Front. Immunol. 2020, 11, 254. [Google Scholar] [CrossRef]
- Marinescu, I.P.; Foarfă, M.C.; Pîrlog, M.C.; Turculeanu, A. Prenatal depression and stress—Risk factors for placental pathology and spontaneous abortion. Rom. J. Morphol. Embryol. 2014, 55, 1155–1160. [Google Scholar]
- Duran-Chávez, J.; Grandi, C.; Dos S Rodrigues, L.; de Freitas, S.F.; Cardoso, V.C.; Carvalho Cavalli, R. Relationship between metalloproteinase-2 and -9 levels in plasma and vaginal secretion with preterm birth. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 261, 217–221. [Google Scholar] [CrossRef]
- Wadhwa, P.D.; Entringer, S.; Buss, C.; Lu, M.C. The contribution of maternal stress to preterm birth: Issues and considerations. Clin. Perinatol. 2011, 38, 351–384. [Google Scholar] [CrossRef]
- Kawanishi, Y.; Yoshioka, E.; Saijo, Y.; Itoh, T.; Miyamoto, T.; Sengoku, K.; Ito, Y.; Ito, S.; Miyashita, C.; Araki, A.; et al. The relationship between prenatal psychological stress and placental abruption in Japan, The Japan Environment and Children’s Study (JECS). PLoS ONE 2019, 14, e0219379. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Jamieson, D.J.; Rasmussen, S.A. An update on COVID-19 and pregnancy. Am. J. Obstet. Gynecol. 2022, 226, 177–186. [Google Scholar] [CrossRef]
- Geng, J.; Huang, C.; Jiang, S. Roles and regulation of the matrix metalloproteinase system in parturition. Mol. Reprod. Dev. 2016, 83, 276–286. [Google Scholar] [CrossRef]
- Al-Dujaili, E.A.; Munir, N.; Iniesta, R.R. Effect of vitamin D supplementation on cardiovascular disease risk factors and exercise performance in healthy participants: A randomized placebo-controlled preliminary study. Ther. Adv. Endocrinol. Metab. 2016, 7, 153–165. [Google Scholar] [CrossRef]
- Monk, C.; Webster, R.S.; McNeil, R.B.; Parker, C.B.; Catov, J.M.; Greenland, P.; Bairey Merz, C.N.; Silver, R.M.; Simhan, H.N.; Ehrenthal, D.B.; et al. Associations of perceived prenatal stress and adverse pregnancy outcomes with perceived stress years after delivery. Arch. Womens Ment. Health 2020, 23, 361–369. [Google Scholar] [CrossRef]
- Lilliecreutz, C.; Larén, J.; Sydsjö, G.; Josefsson, A. Effect of maternal stress during pregnancy on the risk for preterm birth. BMC Pregnancy Childbirth 2016, 16, 5. [Google Scholar] [CrossRef]
- Freedman, A.A.; Miller, G.E.; Keenan-Devlin, L.S.; Smart, B.P.; Romero, J.; Borders, A.; Ernst, L.M. Adverse Pregnancy Outcomes Following the Assassination of John F. Kennedy in 1963. Matern. Child Health J. 2021, 25, 1455–1464. [Google Scholar] [CrossRef]
- Salisbury, A.L.; O’Grady, K.E.; Battle, C.L.; Wisner, K.L.; Anderson, G.M.; Stroud, L.R.; Miller-Loncar, C.L.; Young, M.E.; Lester, B.M. The Roles of Maternal Depression, Serotonin Reuptake Inhibitor Treatment, and Concomitant Benzodiazepine Use on Infant Neurobehavioral Functioning Over the First Postnatal Month. Am. J. Psychiatry 2016, 173, 147–157. [Google Scholar] [CrossRef]
- Nadholta, P.; Bali, P.; Singh, A.; Anand, A. Potential benefits of Yoga in pregnancy-related complications during the COVID-19 pandemic and implications for working women. Work 2020, 67, 269–279. [Google Scholar] [CrossRef]
- Pilarska, I.; Bizon, M.; Sawicki, W. Influence of COVID-19 Infection on Placental Function. Ginekol. Pol. 2023, 94, 79–83. [Google Scholar] [CrossRef]
- Al-kuraishy, H.M.; Al-Gareeb, A.I.; Albezrah, N.K.A.; Bahaa, H.A.; El-Bouseary, M.M.; Alexiou, A.; Al-Ziyadi, S.H.; Batiha, G.E.-S. Pregnancy and COVID-19: High or Low Risk of Vertical Transmission. Clin. Exp. Med. 2023, 23, 957–967. [Google Scholar] [CrossRef]
- Sánchez-García, J.C.; Carrascosa Moreno, N.P.; Tovar-Gálvez, M.I.; Cortés-Martín, J.; Liñán-González, A.; Alvarado Olmedo, L.; Rodríguez-Blanque, R. COVID-19 in Pregnant Women, Maternal—Fetal Involvement, and Vertical Mother-to-Child Transmission: A Systematic Review. Biomedicines 2022, 10, 2554. [Google Scholar] [CrossRef]
- Obuchowska, A.; Standyło, A.; Obuchowska, K.; Kimber-Trojnar, Ż.; Leszczyńska-Gorzelak, B. Cytokine Storms in the Course of COVID-19 and Haemophagocytic Lymphohistiocytosis in Pregnant and Postpartum Women. Biomolecules 2021, 11, 1202. [Google Scholar] [CrossRef]
- Giuliani, F.; Oros, D.; Gunier, R.B.; Deantoni, S.; Rauch, S.; Casale, R.; Nieto, R.; Bertino, E.; Rego, A.; Menis, C.; et al. Effects of Prenatal Exposure to Maternal COVID-19 and Perinatal Care on Neonatal Outcome: Results from the INTERCOVID Multinational Cohort Study. Am. J. Obstet. Gynecol. 2022, 227, 488.e1–488.e17. [Google Scholar] [CrossRef]
- Matar, R.; Alrahmani, L.; Monzer, N.; Debiane, L.G.; Berbari, E.; Fares, J.; Fitzpatrick, F.; Murad, M.H. Clinical Presentation and Outcomes of Pregnant Women With Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. Clin. Infect. Dis. 2021, 72, 521–533. [Google Scholar] [CrossRef]
- Sánchez, J.; Espinosa, J.; Caballero, L.C.; Campana, B.S.; Quintero, A.; Luo, C.; Ng, C.J.; De Gracia, R.; Vigil-De Gracia, P. COVID 19 and High Pregnancy and Perinatal Complications in Panama. J. Matern. Fetal Neonatal Med. 2022, 35, 8245–8248. [Google Scholar] [CrossRef]
- Seok, D.; Ju, H.O. Impact of the COVID-19 Pandemic on Depression during Pregnancy: A Cross-Sectional Study. Korean J. Women Health Nurs. 2023, 29, 44–54. [Google Scholar] [CrossRef]
- Machluf, Y.; Rosenfeld, S.; Ben Shlomo, I.; Chaiter, Y.; Dekel, Y. The Misattributed and Silent Causes of Poor COVID-19 Outcomes Among Pregnant Women. Front. Med. 2021, 8, 745797. [Google Scholar] [CrossRef]
- Heeralall, C.; Ibrahim, U.H.; Lazarus, L.; Gathiram, P.; Mackraj, I. The Effects of COVID-19 on Placental Morphology. Placenta 2023, 138, 88–96. [Google Scholar] [CrossRef]
- Meyer, J.A.; Roman, A.S.; Limaye, M.; Grossman, T.B.; Flaifel, A.; Vaz, M.J.; Thomas, K.M.; Penfield, C.A. Association of SARS-CoV-2 Placental Histopathology Findings with Maternal–Fetal Comorbidities and Severity of COVID-19 Hypoxia. J. Matern. Fetal Neonatal Med. 2022, 35, 8412–8418. [Google Scholar] [CrossRef]
- Garg, R.; Agarwal, R.; Yadav, D.; Singh, S.; Kumar, H.; Bhardwaj, R. Histopathological Changes in Placenta of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-Cov-2) Infection and Maternal and Perinatal Outcome in COVID-19. J. Obstet. Gynecol. India 2023, 73, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Tosto, V.; Meyyazhagan, A.; Alqasem, M.; Tsibizova, V.; Di Renzo, G.C. SARS-CoV-2 Footprints in the Placenta: What We Know after Three Years of the Pandemic. J. Pers. Med. 2023, 13, 699. [Google Scholar] [CrossRef] [PubMed]
- King, L.S.; Feddoes, D.E.; Kirshenbaum, J.S.; Humphreys, K.L.; Gotlib, I.H. Pregnancy during the Pandemic: The Impact of COVID-19-Related Stress on Risk for Prenatal Depression. Psychol. Med. 2023, 53, 170–180. [Google Scholar] [CrossRef] [PubMed]
- Hessami, K.; Romanelli, C.; Chiurazzi, M.; Cozzolino, M. COVID-19 Pandemic and Maternal Mental Health: A Systematic Review and Meta-Analysis. J. Matern. Fetal Neonatal Med. 2022, 35, 4014–4021. [Google Scholar] [CrossRef]
- Rabinowitz, E.P.; Kutash, L.A.; Richeson, A.L.; Sayer, M.A.; Samii, M.R.; Delahanty, D.L. Depression, Anxiety, and Stress in Pregnancy and Postpartum: A Longitudinal Study during the COVID-19 Pandemic. Midwifery 2023, 121, 103655. [Google Scholar] [CrossRef]
- DiGregory, S.; Githere, N.; Crites, K.; Rouse, C.; Shanks, A. The Impact of COVID-19 on Postpartum Depression and the Responsibility of the Healthcare System. Cureus 2022, 14, e27805. [Google Scholar] [CrossRef]
- Treyvaud, K.; Doyle, L.W.; Lee, K.J.; Ure, A.; Inder, T.E.; Hunt, R.W.; Anderson, P.J. Parenting behavior at 2 years predicts school-age performance at 7 years in very preterm children. J. Child Psychol. Psychiatr. 2016, 57, 814–821. [Google Scholar] [CrossRef]
- Mesa Mesa, S.; Gómez García, A.; Naranjo Pérez, L.F.; Tobón Montoya, L.; Ocampo Saldarriaga, M.V.; Velásquez Tirado, J.D.; Constaín González, G.A.; Ricardo Ramírez, C.; Gutiérrez Vélez, Y.F.; Franco Vásquez, J.G. Psychological stress in mothers of neonates admitted to an intensive care unit. Salud Ment. 2021, 44, 241–248. [Google Scholar] [CrossRef]
- Persson, C.; Ericson, J.; Salari, R.; Eriksson, M.H.; Flacking, R. NICU parents’ mental health: A comparative study with parents of term and healthy infants. Acta Paediatr. 2023, 112, 954–966. [Google Scholar] [CrossRef]
- Chen, H.; Selix, N.; Nosek, M. Perinatal Anxiety and Depression During COVID-19. J. Nurse Pract. 2021, 17, 26–31. [Google Scholar] [CrossRef]
- Zheng, Z.; Zhang, R.; Liu, T.; Cheng, P.; Zhou, Y.; Lu, W.; Xu, G.; So, K.-F.; Lin, K. The Psychological Impact of the Coronavirus Disease 2019 Pandemic on Pregnant Women in China. Front. Psychiatry 2021, 12, 628835. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Ding, Y.; Guo, W. Mental Health of Pregnant and Postpartum Women During the Coronavirus Disease 2019 Pandemic: A Systematic Review and Meta-Analysis. Front. Psychol. 2020, 11, 617001. [Google Scholar] [CrossRef]
- Cheung, R.Y.M.; Cheng, W.Y.; Li, J.-B.; Lau, E.Y.H.; Chung, K.K.H. Mothers’ and fathers’ stress and severity of depressive symptoms during the COVID-19 pandemic: Actor-partner effects with parental negative emotions as a moderator. BMC Psychol. 2022, 10, 294. [Google Scholar] [CrossRef] [PubMed]
- Grumi, S.; Provenzi, L.; Accorsi, P.; Biasucci, G.; Cavallini, A.; Decembrino, L.; Falcone, R.; Fazzi, E.M.; Gardella, B.; Giacchero, R.; et al. Depression and Anxiety in Mothers Who Were Pregnant During the COVID-19 Outbreak in Northern Italy: The Role of Pandemic-Related Emotional Stress and Perceived Social Support. Front. Psychiatry 2021, 12, 716488. [Google Scholar] [CrossRef] [PubMed]
- Fekadu Dadi, A.; Miller, E.R.; Mwanri, L. Antenatal depression and its association with adverse birth outcomes in low and middle-income countries: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0227323. [Google Scholar] [CrossRef]
- Racine, N.; Hetherington, E.; McArthur, B.A.; McDonald, S.; Edwards, S.; Tough, S.; Madigan, S. Maternal depressive and anxiety symptoms before and during the COVID-19 pandemic in Canada: A longitudinal analysis. Lancet Psychiatry 2021, 8, 405–415. [Google Scholar] [CrossRef]
- Pacheco, F.; Sobral, M.; Guiomar, R.; De La Torre-Luque, A.; Caparros-Gonzalez, R.A.; Ganho-Ávila, A. Breastfeeding during COVID-19: A Narrative Review of the Psychological Impact on Mothers. Behav. Sci. 2021, 11, 34. [Google Scholar] [CrossRef]
- Gath, M.E.; Lee, S.J.; Austin, N.C.; Woodward, L.J. Increased Risk of Parental Instability for Children Born Very Preterm and Impacts on Neurodevelopmental Outcomes at Age 12. Children 2021, 9, 304. [Google Scholar] [CrossRef]
- Vescovi, G.; Riter, H.D.S.; Azevedo, E.C.; Pedrotti, B.G.; Frizzo, G.B. Parenting, mental health, and Covid-19: A rapid systematic review. Psicol. Teor. Prática 2021, 23, TPC1913554. [Google Scholar] [CrossRef]
- Durankuş, F.; Aksu, E. Effects of the COVID-19 pandemic on anxiety and depressive symptoms in pregnant women: A preliminary study. J. Mater. Fetal Neonatal Med. 2022, 35, 205–211. [Google Scholar] [CrossRef]
- New Research Highlights Risks of Separating Newborns from Mothers during COVID-19 Pandemic. Available online: https://www.who.int/news/item/16-03-2021-new-research-highlights-risks-of-separating-newborns-from-mothers-during-covid-19-pandemic (accessed on 16 March 2021).
- Manca, A.; Cosma, S.; Palermiti, A.; Costanzo, M.; Antonucci, M.; De Vivo, E.D.; Ianniello, A.; Borella, F.; Carosso, A.R.; Corcione, S.; et al. Pregnancy and COVID-19: The Possible Contribution of Vitamin D. Nutrients 2022, 14, 3275. [Google Scholar] [CrossRef]
- Sinaci, S.; Ocal, D.F.; Yucel Yetiskin, D.F.; Uyan Hendem, D.; Buyuk, G.N.; Goncu Ayhan, S.; Tanacan, A.; Ozgu-Erdinc, A.S.; Moraloglu Tekin, O.; Sahin, D. Impact of vitamin D on the course of COVID-19 during pregnancy: A case control study. J. Steroid Biochem. Mol. Biol. 2021, 213, 105964. [Google Scholar] [CrossRef]
- Woo, J.; Giurgescu, C.; Wagner, C.L. Evidence of an Association Between Vitamin D Deficiency and Preterm Birth and Preeclampsia: A Critical Review. J. Midwifery Womens Health 2019, 64, 613–629. [Google Scholar] [CrossRef] [PubMed]
- Tahsin, T.; Khanam, R.; Chowdhury, N.H.; Hasan, A.S.M.T.; Hosen, M.B.; Rahman, S.; Roy, A.K.; Ahmed, S.; Raqib, R.; Baqui, A.H. Vitamin D deficiency in pregnancy and the risk of preterm birth: A nested case-control study. BMC Pregnancy Childbirth 2023, 23, 322. [Google Scholar] [CrossRef] [PubMed]
- Vavouraki, E. The Impact of COVID-19 Pandemic on the Healthcare of Premature Babies. Eur. J. Midwifery 2020, 4, 21. [Google Scholar] [CrossRef] [PubMed]
- Bresesti, I.; Morlacchi, L.; Cazzaniga, C.; Sangiorgio, C.; Bertù, L.; Bolis, M.E.; Bossi, A.; Agosti, M. Breastfeeding and human milk bank in a neonatal intensive care unit: Impact of the COVID-19 pandemic in an Italian cohort of very low birth weight infants. IBJ 2022, 17, 94. [Google Scholar] [CrossRef]
- Manuela, F.; Barcos-Munoz, F.; Monaci, M.G.; Lordier, L.; Camejo, M.P.; De Almeida, J.S.; Grandjean, D.; Hüppi, P.S.; Borradori-Tolsa, C. Maternal Stress, Depression, and Attachment in the Neonatal Intensive Care Unit Before and During the COVID Pandemic: An Exploratory Study. Front. Psychol. 2021, 12, 734640. [Google Scholar] [CrossRef]
- Mohammadi, F.; ShoaaKazemi, M. The relationship between emotional intelligence and parental stress management during the COVID-19 pandemic. Brain Behav. 2022, 12, e2692. [Google Scholar] [CrossRef]
- Osorio Galeano, S.P.; Salazar Maya, Á.M. Experiences of Parents of Preterm Children Hospitalized Regarding Restrictions to Interact with Their Children Imposed Because of the COVID-19 Pandemic. Investig. Educ. Enferm. 2021, 39, e10. [Google Scholar] [CrossRef]
- Cristóbal-Cañadas, D.; Parrón-Carreño, T.; Nievas-Soriano, B.J. Effect of the Kangaroo Mother Method after Preterm Delivery on Maternal Stress and Anxiety in the Context of the COVID-19 Pandemic—A Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 16432. [Google Scholar] [CrossRef]
- Erdei, C.; Feldman, N.; Koire, A.; Mittal, L.; Liu, C.H.J. COVID-19 Pandemic Experiences and Maternal Stress in Neonatal Intensive Care Units. Children 2022, 9, 251. [Google Scholar] [CrossRef] [PubMed]
- Reichert, A.P.D.S.; Guedes, A.T.A.; Soares, A.R.; Brito, P.K.H.; Dias, T.K.C.; Santos, N.C.C.D.B. Covid-19 pandemic: Experiences of mothers of infants who were born premature. Rev. Gaúcha Enferm. 2022, 42, e20200364. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagner, E.; Bień, K.; Łomża, A.; Grunwald, A.; Kimber-Trojnar, Ż.; Libera, A.; Leszczyńska-Gorzelak, B. Stress of Prematurity in the Experience of the COVID-19 Pandemic—Current State of Knowledge. Life 2023, 13, 1757. https://doi.org/10.3390/life13081757
Wagner E, Bień K, Łomża A, Grunwald A, Kimber-Trojnar Ż, Libera A, Leszczyńska-Gorzelak B. Stress of Prematurity in the Experience of the COVID-19 Pandemic—Current State of Knowledge. Life. 2023; 13(8):1757. https://doi.org/10.3390/life13081757
Chicago/Turabian StyleWagner, Emilia, Katarzyna Bień, Aleksandra Łomża, Arkadiusz Grunwald, Żaneta Kimber-Trojnar, Aneta Libera, and Bożena Leszczyńska-Gorzelak. 2023. "Stress of Prematurity in the Experience of the COVID-19 Pandemic—Current State of Knowledge" Life 13, no. 8: 1757. https://doi.org/10.3390/life13081757