
Midline and Mediolateral Episiotomy: Risk Assessment Based on Clinical Anatomy


 and
and
Abstract
:1. Introduction
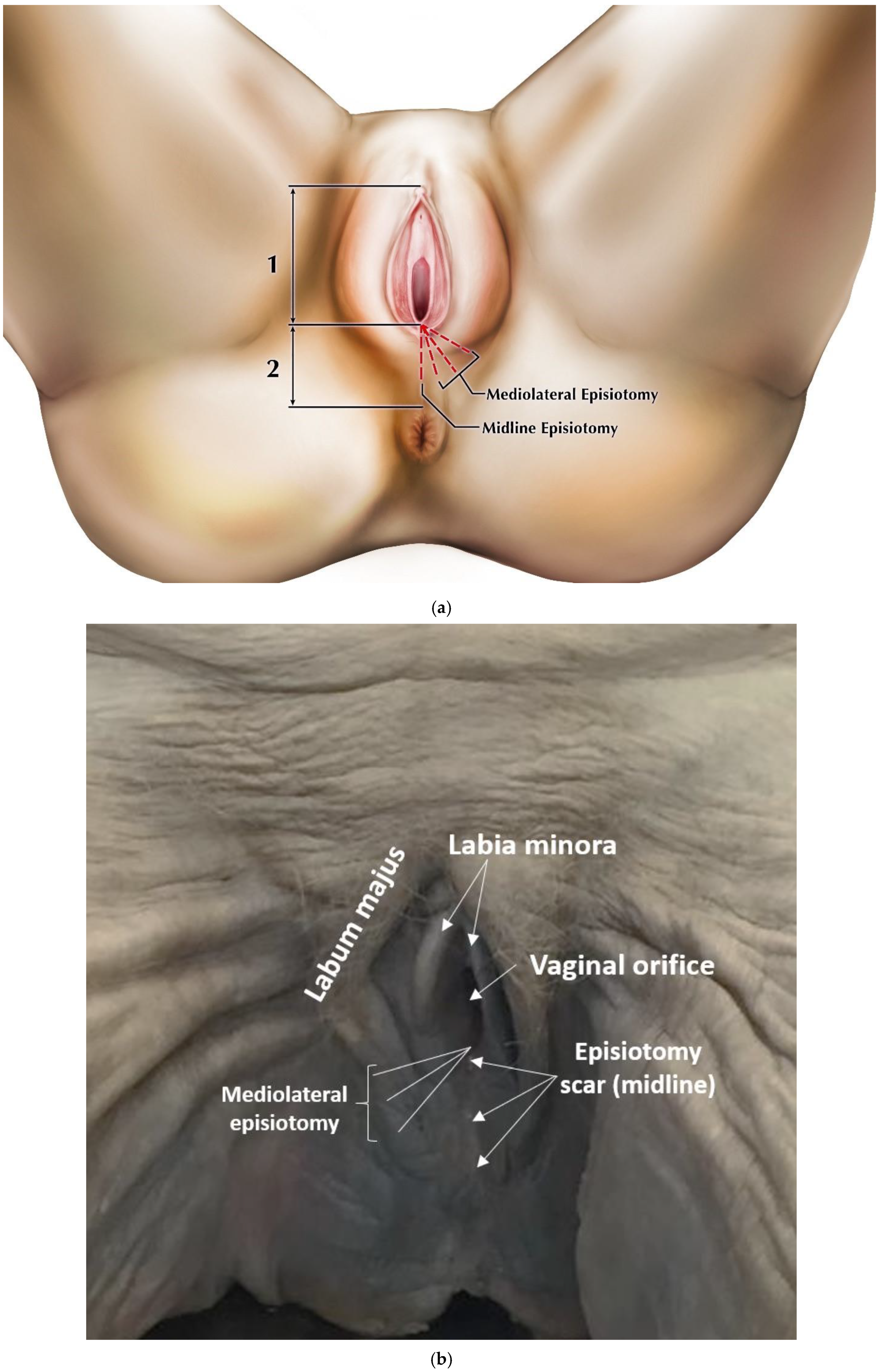
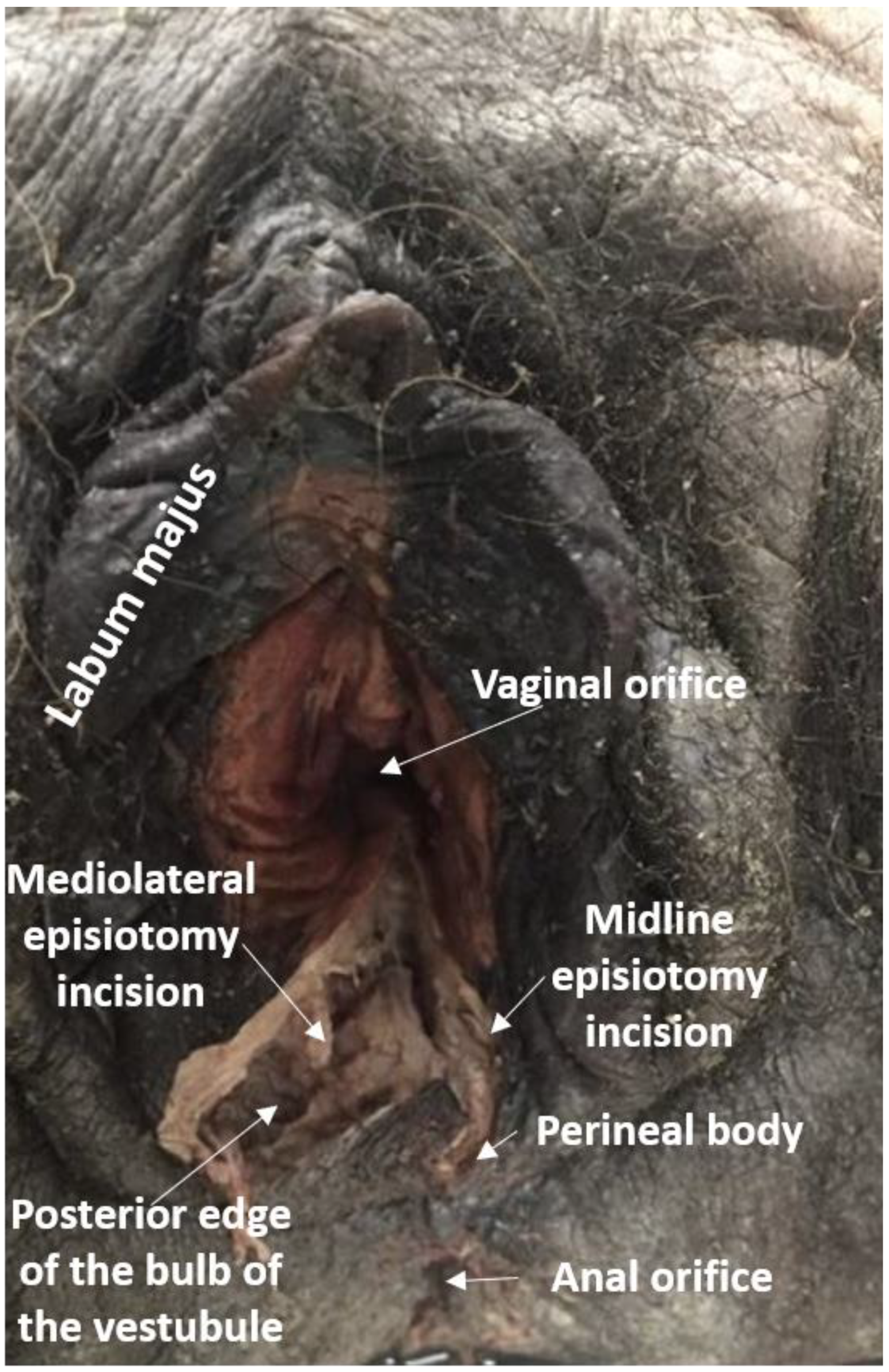
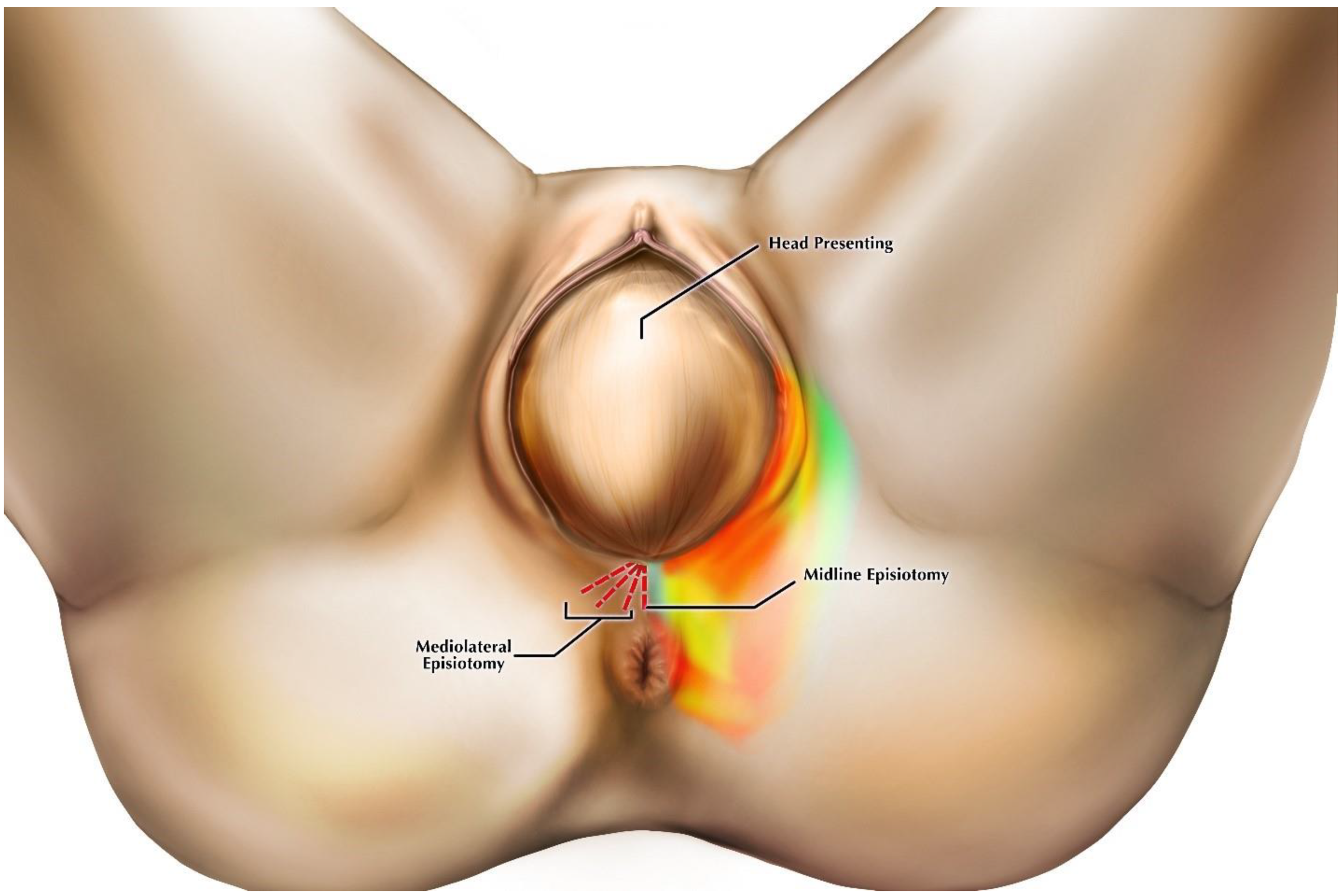
2. Materials and Methods
3. Results
3.1. Midline Incision
3.2. High-Angle Mediolateral Incision
3.3. Medium-Angle Mediolateral Incision
3.4. Low-Angle Mediolateral Incision
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 71: Episiotomy. Obstet. Gynecol. 2006, 107, 956–962. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. Practice Bulletin No. 165: Prevention and Management of Obstetric Lacerations at Vaginal Delivery. Obstet. Gynecol. 2016, 128, e1–e15. [Google Scholar] [CrossRef] [PubMed]
- Cargill, Y.M.; MacKinnon, C.J. SOGC Clinical Practice Guidelines, No. 148, August 2004. J. Obstet. Gynaecol. Can. 2004, 26, 747–753. [Google Scholar] [PubMed]
- Royal College of Obstetricians and Gynaecologists. Operative Vaginal Delivery; Green-Top Guideline No. 26; Royal College of Obstetricians and Gynaecologists: London, UK, 2011. [Google Scholar]
- Sagi-Dain, L.; Sagi, S. The role of episiotomy in prevention and management of shoulder dystocia: A systematic review. Obstet. Gynecol. Surv. 2015, 70, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, K.; Viswanathan, M.; Palmieri, R.; Gartlehner, G.; Thorp, J., Jr.; Lohr, K.N. Outcomes of routine episiotomy: A systematic review. JAMA 2005, 293, 214148. [Google Scholar] [CrossRef]
- Dahlen, H.G.; Priddis, H.; Thornton, C. Severe perineal trauma is rising, but let us not overreact. Midwifery 2015, 31, 1–8. [Google Scholar] [CrossRef]
- Ekeus, C.; Nilsson, E.; Gottvall, K. Increasing incidence of anal sphincter tears among primiparas in Sweden: A population-based register study. Acta Obstet. Gynecol. Scand. 2008, 87, 564–573. [Google Scholar] [CrossRef]
- Gurol-Urganci, I.; Cromwell, D.A.; Edozien, L.C.; Mahmood, T.A.; Adams, E.J.; Richmond, D.H.; Templeton, A.; van der Meulen, J.H. Third- and fourth-degree perineal tears among primiparous women in England between 2000 and 2012: Time trends and risk factors. BJOG 2013, 120, 1516–1525. [Google Scholar] [CrossRef]
- Ismail, S.I.; Puyk, B. The rise of obstetric anal sphincter injuries (OASIS): 11-year trend analysis using Patient Episode Database for Wales (PEDW) data. Obstet. Gynecol. 2014, 34, 495–498. [Google Scholar] [CrossRef]
- Mous, M.; Muller, S.; de Leeuw, J. Long-term effects of anal sphincter rupture during vaginal delivery: Faecal incontinence and sexual complaints. BJOG 2008, 115, 234–238. [Google Scholar] [CrossRef]
- Samarasekera, D.N.; Bekhit, M.T.; Wright, Y.; Lowndes, R.H.; Stanley, K.P.; Preston, J.P.; Preston, P.; Speakman, C.T.M. Long-term anal continence and quality of life following postpartum anal sphincter injury. Colorectal Dis. 2008, 10, 793–799. [Google Scholar] [CrossRef] [PubMed]
- van Brummen, H.; Bruinse, H.; van de Pol, G.; Heintz, A.; van der Vaart, G. Which factors determine the sexual function 1 year after childbirth? BJOG 2006, 113, 914–918. [Google Scholar] [CrossRef] [PubMed]
- Harvey, M.A.; Pierce, M. Obstetrical anal sphincter injuries (OASIS): Prevention, recognition, and repair. SOGC Clinical Practice Guideline, No. 330. J. Obstet. Gynaecol. Can. 2015, 37, 1131–1149. [Google Scholar] [CrossRef] [Green Version]
- Royal College of Obstetricians and Gynaecologists. Third- and Fourth-Degree Perineal Tears, Management; Green Top Guideline No. 29; Royal College of Obstetricians and Gynaecologists: London, UK, 2017. [Google Scholar]
- Gonzalez-Díaz, E.; Cea, L.M.; Corona, A.F. Trigonometric characteristics of episiotomy and risks for obstetric anal sphincter injuries in operative vaginal delivery. Int. Urogynecol. J. 2015, 26, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Lund, N.S.; Persson, L.K.; Jangö, H.; Gommesen, D.; Westergaard, H.B. Episiotomy in vacuum-assisted delivery affects the risk of obstetric anal sphincter injury: A systematic review and meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 207, 193–199. [Google Scholar] [CrossRef] [PubMed]
- van Bavel, J.; Hukkelhoven, C.W.; de Vries, C.; Papatsonis, D.N.; de Vogel, J.; Roovers, J.P.; Mol, B.W.; de Leeuw, J.W. The effectiveness of mediolateral episiotomy in preventing obstetric anal sphincter injuries during operative vaginal delivery: A ten-year analysis of a national registry. Int. Urogynecol. J. 2018, 29, 407–413. [Google Scholar] [CrossRef]
- Correa, M.D.; Passini, R. Selective episiotomy: Indications, technique, and association with severe perineal lacerations. Rev. Bras. Ginecol. Obstet. 2016, 38, 301–307. [Google Scholar] [CrossRef] [Green Version]
- Eogan, M.; Daly, L.; O’connell, P.R.; O’herlihy, C. Does the angle of episiotomy affect the incidence of anal sphincter injury? BJOG 2006, 113, 190–194. [Google Scholar]
- Menzies, R.; Leung, M.; Chandrasekaran, N.; Lausman, A.; Geary, M. Episiotomy Technique and Management of Anal Sphincter Tears—A Survey of Clinical Practice and Education. J. Obstet. Gynaecol. Can. 2016, 38, 1091–1099. [Google Scholar] [CrossRef]
- Sooklim, R.; Thinkhamrop, J.; Lumbiganon, P.; Prasertcharoensuk, W.; Pattamadilok, J.; Seekorn, K.; Chongsomchai, C.; Pitak, P.; Chansamak, S. The outcomes of midline versus medio-lateral episiotomy. Reprod. Health 2007, 4, 10. [Google Scholar] [CrossRef] [Green Version]
- Andrews, V.; Thakar, R.; Sultan, A.H.; Jones, P.W. Are mediolateral episiotomies actually mediolateral? BJOG 2005, 112, 1156–1158. [Google Scholar] [CrossRef] [PubMed]
- Silf, K.; Woodhead, N.; Kelly, J.; Fryer, A.; Kettle, C.; Ismail, K.M. Evaluation of accuracy of mediolateral episiotomy incisions using a training model. Midwifery 2015, 31, 197–200. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.W.; Ravindran, K.; Thomas, J.M.; Andrews, V. Mediolateral episiotomy: Are trained midwives and doctors approaching it from a different angle? Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 174, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Kalis, V.; Karbanova, J.; Horak, M.; Lobovsky, L.; Kralickova, M.; Rokyta, Z. The incision angle of mediolateral episiotomy before delivery and after repair. Int. J. Gynecol. Obstet. 2008, 103, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Kalis, V.; Stepan, J., Jr.; Horak, M.; Roztocil, A.; Kralickova, M.; Rokyta, Z. Definitions of mediolateral episiotomy in Europe. Int. J. Gynecol. Obstet. 2008, 100, 188–189. [Google Scholar]
- Lappen, J.R.; Isaacs, M. Episiotomy and Repair Technique; 2016; Available online: https://emedicine.medscape.com/article/2047173-technique (accessed on 9 July 2019).
- Friedman, A.M.; Ananth, C.V.; Prendergast, E.; D’alton, M.E.; Wright, J.D. Variation in and factors associated with use of episiotomy. JAMA 2015, 313, 197–199. [Google Scholar] [CrossRef]
- Handa, V.L.; Blomquist, J.L.; McDermott, K.C.; Friedman, S.; Muñoz, A. Pelvic floor disorders after vaginal birth: Effect of episiotomy, perineal laceration, and operative birth. Obstet. Gynecol. 2012, 119, 233–239. [Google Scholar] [CrossRef] [Green Version]
- Thacker, S.B. Midline versus mediolateral episiotomy: We still don’t know which cut is better or how beneficial the procedure is. BMJ 2000, 320, 1615–1616. [Google Scholar] [CrossRef]
- Kudish, B.; Blackwell, S.; Mcneely, S.G.; Bujold, E.B.; Kruger, M.; Hendrix, S.L.; Sokol, R. Operative vaginal delivery and midline episiotomy: A bad combination for the perineum. AJOG 2006, 195, 749–754. [Google Scholar] [CrossRef]
- Shionio, P.; Klebaof, M.A.; Carey, J.C. Midline episiotomies: More harm than good? Obstet. Gynecol. 1990, 75, 765–770. [Google Scholar]
- Plochocki, J.H.; Rodriguez-Sosa, J.R.; Adrian, B.; Ruiz, S.A.; Hall, M.I. A functional and clinical reinterpretation of human perineal neuromuscular anatomy: Application to sexual function and continence. Clin. Anat. 2016, 29, 1053–1058. [Google Scholar] [CrossRef]
- Shafik, A.; El Sibai, O.; Shafik, A.A.; Shafik, I.A. A novel concept for the surgical anatomy of the perineal body. Dis. Colon Rectum 2007, 50, 2120–2125. [Google Scholar] [CrossRef] [PubMed]
- Soga, H.; Nagata, J.; Murakami, G.; Yajima, T.; Takenaka, A.; Fujisawa, M.; Koyama, M. A histotopographic study of the perineal body in elderly women: The surgical applicability of novel histological findings. Int. Urogynecol. J. 2007, 18, 1423–1430. [Google Scholar] [CrossRef] [PubMed]
- Geller, E.J.; Robinson, B.L.; Matthews, C.A.; Celauro, K.P.; Dunivan, G.C.; Crane, A.K.; Ivins, A.R.; Woodham, P.C.; Fielding, J.R. Perineal body length as a risk for ultrasound-diagnosed anal sphincter tear at first delivery. Int. Urogynecol. J. 2014, 25, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Kalis, V.; Chaloupka, P.; Turek, J.; Rokyta, Z. The perineal body length and injury at delivery. Ceska Gynekol. 2005, 70, 355–361. [Google Scholar]
- Fernando, R.J.; Sultan, A.H.; Freeman, R.H.; Williams, A.A.; Adams, E.A. The management of third- and fourth-degree perineal tears. Green Top. Guideline No. 29. London: Royal College of Obstetricians and Gynaecologists. BJOG 2015, 6, 1–19. [Google Scholar]
- Nygaard, I.E.; Rao, S.S.; Dawson, J.D. Anal incontinence after anal sphincter disruption: A 30-year retrospective cohort study. Obstet. Gynecol. 1997, 89, 896–901. [Google Scholar]
- Tincello, D.G.; Williams, A.; Fowler, G.E.; Adams, E.J.; Richmond, D.H.; Alfirevic, Z. Differences in episiotomy technique between midwives and doctors. BJOG 2003, 110, 1041–1044. [Google Scholar] [CrossRef]
- Andrews, V.; Thakar, R.; Sultan, A.H.; Jones, P.W. Occult anal sphincter injuries—Myth or reality? BJOG 2006, 113, 195–200. [Google Scholar] [CrossRef]
- Staric, K.D.; Lukanovic, A.; Petrocnik, P.; Zacesta, V.; Cescon, C.; Lucovnik, M. Impact of mediolateral episiotomy on incidence of obstetrical anal sphincter injury diagnosed by endoanal ultrasound. Midwifery 2017, 51, 40–43. [Google Scholar] [CrossRef]
- Sudoł-Szopinńska, I.; Radkiewicz, J.; Szopiński, T.; Panorska, A.K.; Jakubowski, W.; Kawka, J. Postpartum endoanal ultrasound findings in primiparous women after vaginal delivery. Acta Radiol. 2010, 51, 819–824. [Google Scholar] [CrossRef]
- Hall, M.I.; Rodriguez-Sosa, J.R.; Plochocki, J.R. Reorganization of mammalian body wall patterning with cloacal septation. Sci. Rep. 2017, 7, 9182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neill, S.M.; Lewis, F.M. Ridley’s the Vulva; Wiley-Blackwell: Hoboken, NJ, USA, 2009. [Google Scholar]
- Pauls, R.N. Anatomy of the clitoris and the female sexual response. Clin. Anat. 2015, 28, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Puppo, V. Anatomy and physiology of the clitoris, vestibular bulbs, and labia minora with a review of the female orgasm and the prevention of female sexual dysfunction. Clin. Anat. 2013, 26, 134–152. [Google Scholar] [CrossRef] [PubMed]
- Masters, W.H.; Johnson, V.E. Human Sexual Response; Little Brown: Boston, MA, USA, 1966. [Google Scholar]
- Coats, P.M.; Chan, K.K.; Wilkins, M.; Beard, R.J. A comparison between midline and mediolateral episiotomies. BJOG 1980, 87, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Connolly, A.; Thorp, J.; Pahel, L. Effects of pregnancy and childbirth on postpartum sexual function: A longitudinal prospective study. Int. Urogynecol. J. 2005, 16, 263–267. [Google Scholar] [CrossRef]
- Glazener, C.M.A. Sexual function after childbirth: Women’s experiences, persistent morbidity and lack of professional recognition. Br. J. Obstet. Gynaecol. 1997, 104, 330–333. [Google Scholar] [CrossRef]
- Ergenoglu, A.M.; Yeniel, A.Ö.; Itil, I.M.; Askar, N.; Meseri, R.; Petri, E. Overactive bladder and its effects on sexual dysfunction among women. Acta Obstet. Gynecol. Scand. 2013, 92, 1202–1207. [Google Scholar] [CrossRef]
- Signorello, L.B.; Harlow, B.L.; Chekos, A.K.; Repke, J.T. Midline episiotomy and anal incontinence: Retrospective cohort study. BMJ 2000, 320, 86–90. [Google Scholar] [CrossRef] [Green Version]
- Faltin, D.L.; Otero, M.; Petignat, P.; Sangalli, M.R.; Floris, L.A.; Boulvain, M.; Irion, O. Women’s health 18 years after rupture of the anal sphincter during childbirth: I. Fecal incontinence. AJOG 2006, 194, 1255–1259. [Google Scholar] [CrossRef]
- Sultan, A.H.; Kamm, M.A.; Hudson, C.N. Obstetric perineal tears: An audit of training. J. Obstet. Gynaecol. 1995, 15, 19–23. [Google Scholar] [CrossRef]
- Frankman, E.A.; Wang, L.; Bunker, C.H.; Lowder, J.L. Episiotomy in the United States: Has anything changed? AJOG 2009, 200, 573.e1–573.e7. [Google Scholar] [CrossRef] [PubMed]
- Iwanga, I.; Singh, V.; Ohtsuka, A.; Hwang, Y.; Kim, H.-J.; Morys, J.; Ravi, K.S.; Ribatti, D.; Trainor, P.A.; Sanudo, J.R.; et al. Acknowledging the use of human cadaveric tissues in research papers: Recommendations from anatomical journal editors. Clin. Anat. 2021, 34, 2–4. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Structures in the Incisive Plane | Midline Incision N = 31 | Mediolateral Incision N = 30 | ||
|---|---|---|---|---|
| Angle: 0° | Low Angle: 10–15° N = 9 | Medium Angle: 16–44° N = 10 | High Angle: ≥45° N = 11 | |
| Perineal body | 14.3% | 0.0% | 0.0% | 0.0% |
| Fibers of external anal sphincter | 16.6% | 0.0% | 0.0% | 0.0% |
| Bulbospongiosus | 0.0% | 75.0% | 80.0% | 100% |
| Bulb of the vestibule | 0.0% | 75.0% | 80.0% | 100% |
| Deep perineal nerve branches | 0.0% | 25.0% | 100% | 40.0% |
| Greater vestibular gland | 0.0% | 75.0% | 40.0% | 0.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garner, D.K.; Patel, A.B.; Hung, J.; Castro, M.; Segev, T.G.; Plochocki, J.H.; Hall, M.I. Midline and Mediolateral Episiotomy: Risk Assessment Based on Clinical Anatomy. Diagnostics 2021, 11, 221. https://doi.org/10.3390/diagnostics11020221
Garner DK, Patel AB, Hung J, Castro M, Segev TG, Plochocki JH, Hall MI. Midline and Mediolateral Episiotomy: Risk Assessment Based on Clinical Anatomy. Diagnostics. 2021; 11(2):221. https://doi.org/10.3390/diagnostics11020221
Chicago/Turabian StyleGarner, Danielle K., Akash B. Patel, Jun Hung, Monica Castro, Tamar G. Segev, Jeffrey H. Plochocki, and Margaret I. Hall. 2021. "Midline and Mediolateral Episiotomy: Risk Assessment Based on Clinical Anatomy" Diagnostics 11, no. 2: 221. https://doi.org/10.3390/diagnostics11020221