
Anatomical-MRI Correlations in Adults and Children with Arrhythmogenic Right Ventricular Cardiomyopathy

 ,
,  , , , , and
, , , , and 
Abstract
:1. Introduction
2. Brief Pathology Considerations in ARVC
2.1. Right Ventricle Pathological Features in ARVC
2.2. Left Ventricle Pathological Features in ARVC
2.3. The Pathology of Right Atrium Involvement in ARVC
2.4. Moderator Band: Pathological Features in ARVC
3. Cardiac MRI Features in Arrhythmogenic Right Ventricular Cardiomyopathy
3.1. Right Ventricle CMR Evaluation in ARVC
- (a)
- RV contraction disorders and functional abnormalitiesUnlike the initial diagnostic criteria, the 2010 Revised Task Force Criteria [12] are quantitative rather than qualitative. Three types of changes were included: (1) segmental RV contraction abnormalities, (2) dilation of the RV, and (3) reduction of the RV ejection fraction. It is notable that intramyocardial fat or delayed enhancement are not included in the criteria for differential diagnosis strictly because these changes can be found in healthy people or in other diseases affecting the right ventricle. The association between akinesia/dyskinesia or RV regional contraction asynchrony with RV volume dilation or RV ejection fraction <40% is considered a major criterion for the diagnosis. As mentioned beforehand, the Revised Criteria are quantitative. Therefore, RV dilation is defined as the ratio of RV volume/body surface area > 110 mL/sqm in men or >100 mL/sqm in women. The minor criterion is defined as the presence of akinesia/dyskinesia with decreased ejection fraction of 40 to 45%, contraction abnormalities, or increased RV volume between 100 and 110 mL/sqm in men or 90 and 100 mL/sqm in women. It is worth noting that microaneurysms as well as segmental RV dilatations were removed from the Diagnostic Criteria because they are rather subjective and challenging to evaluate.
- (b)
- Decrease of the RV ejection fraction(EF) is a diagnostic key element and occurs when several areas of impaired contraction cumulate and impair the general contractility function or when the dilated right ventricle. Taking into consideration the degree of EF decrease <40% or between 41% and 45% is rather important, as this criterion, together with the contraction abnormalities, may represent either a minor or major diagnostic criterion for ARVC [12,45].
- (c)
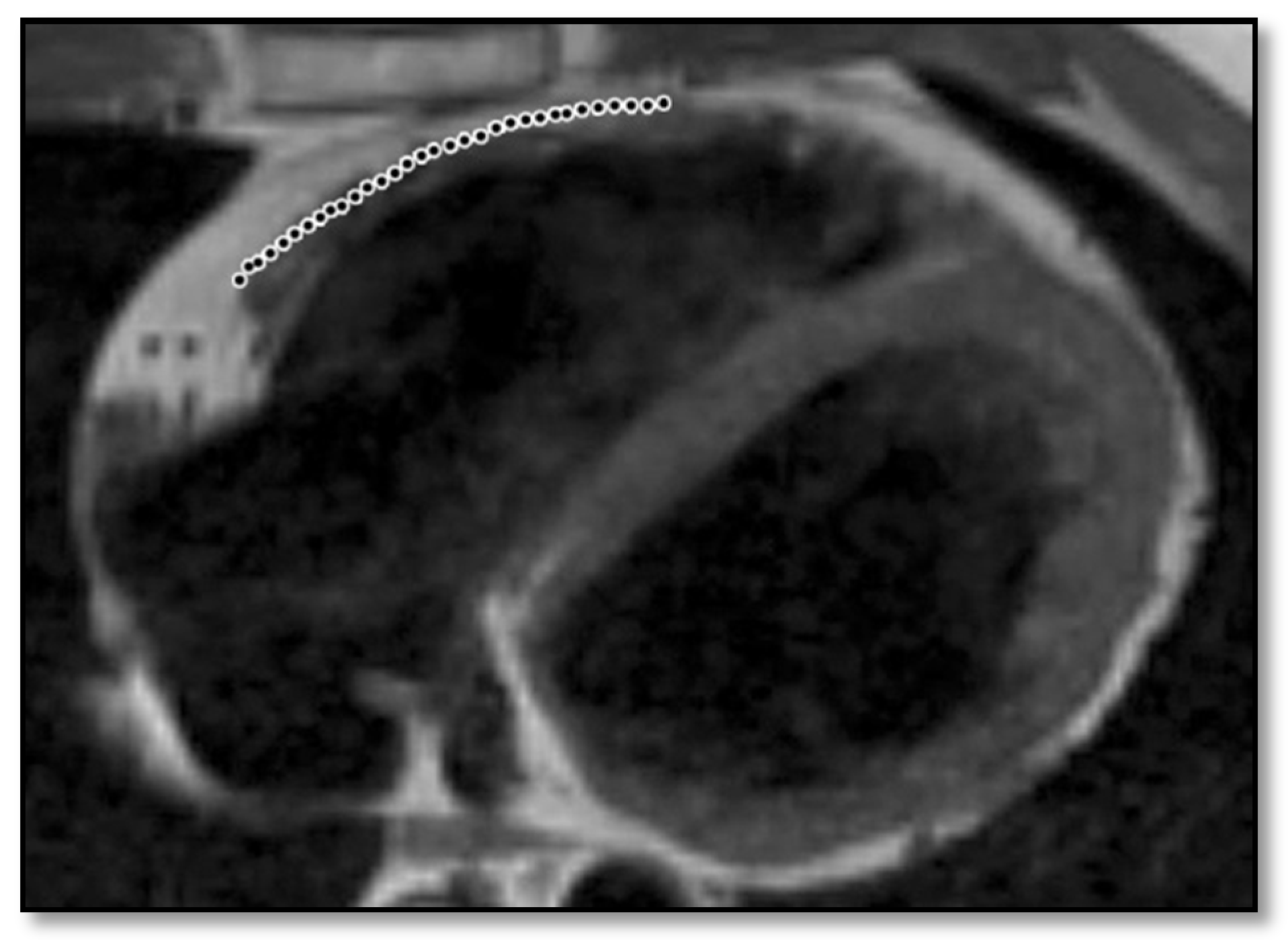
- RV dilation is also a key element for the diagnosis of ARVC. It can be segmental or global. Segmental expansion can affect only the RVOT or parts of the RV such as the basal free wall or the middle third of the free wall. It is a diagnostic criterion with high sensitivity and specificity for ARVC (Figure 3). Only the global dilation of RV is considered a diagnostic criterion for ARVC because segmental dilatation is rather difficult to interpret [12,45].
- (d)
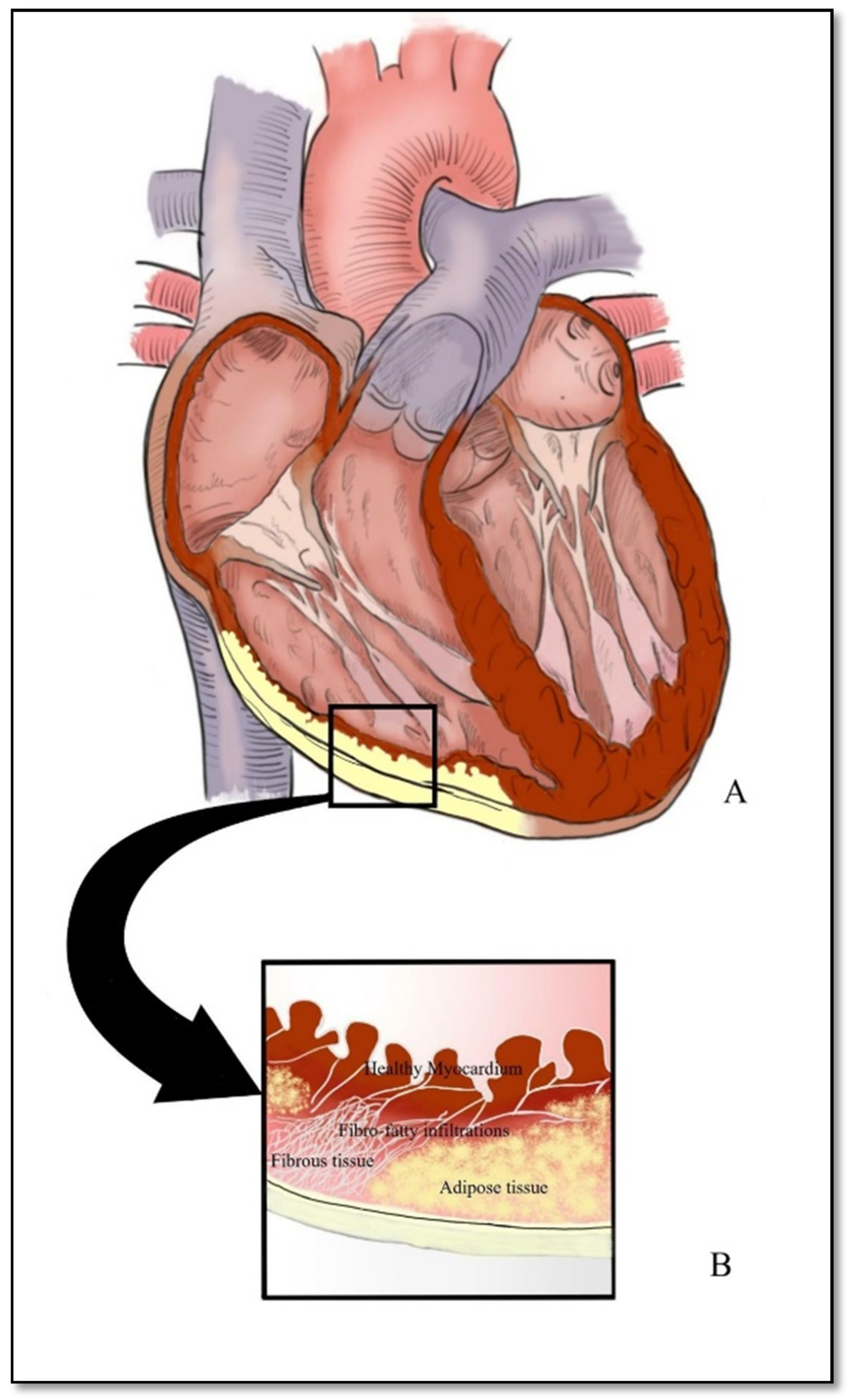
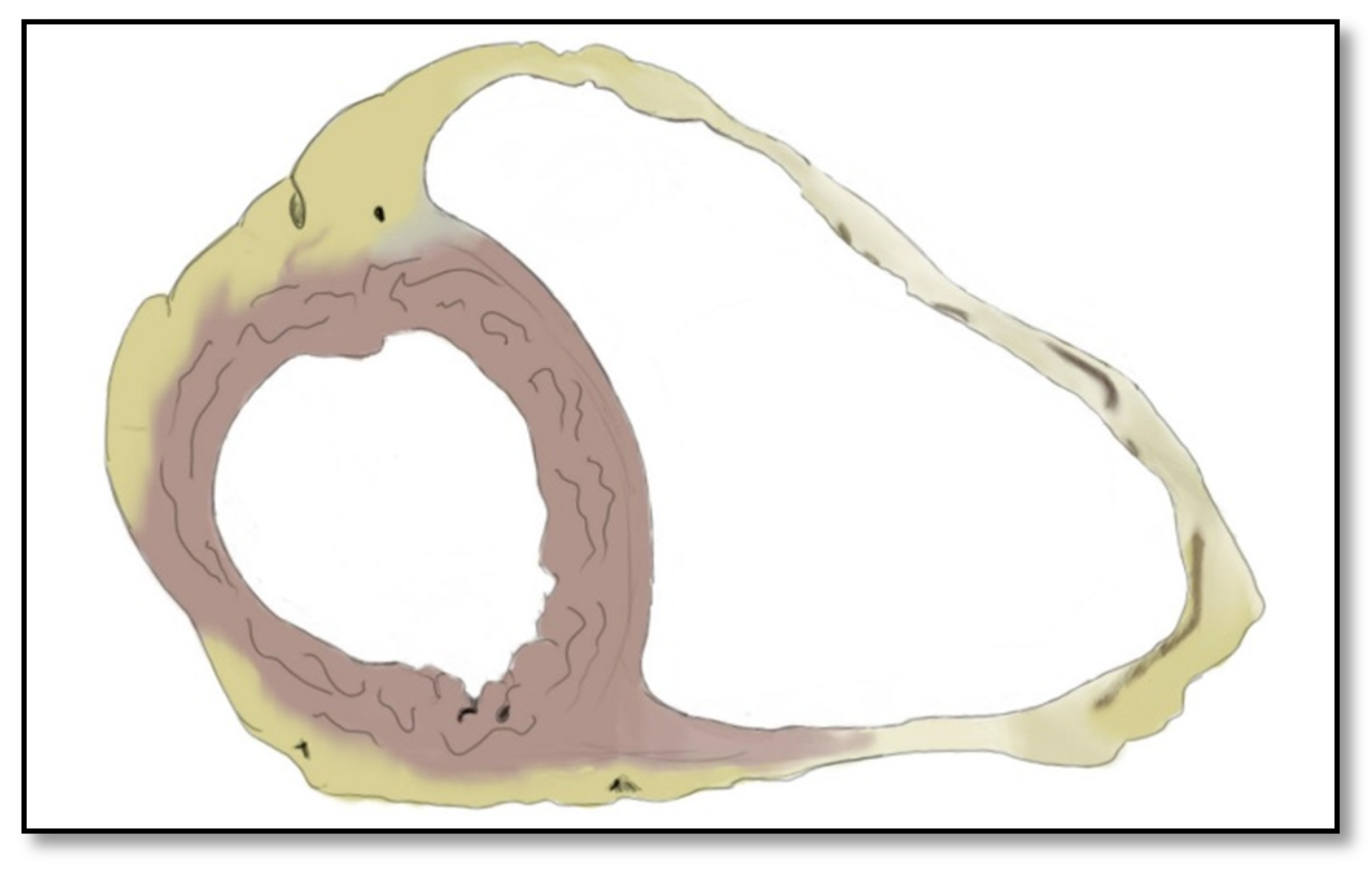
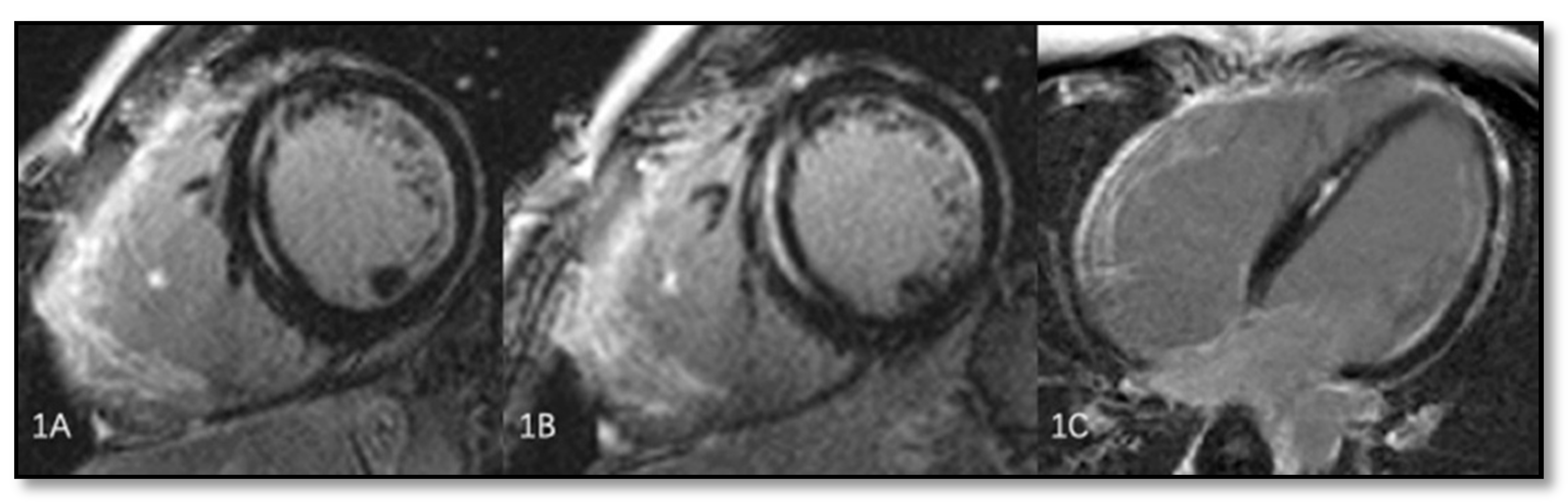
- Intramyocardial adipose tissue disposition—”obsolete”Although intramyocardial fat has long been a diagnostic criterion for ARVC, it is no longer used because other pathological or physiological conditions can lead to this appearance in cardiac MRI. In normal people, epicardial fat can penetrate to the myocardium and endocardium, with no clear demarcation between the epicardium and the myocardium, leading to misinterpreted images as ARVC. When intramyocardial fat is detected, it will be considered pathological only if it is associated with contraction abnormalities of the corresponding wall [12,45].Fat in ARVC appears as hyperintense intramyocardial signal at T1 spin-echo. Adipose tissue infiltrates mainly the RVOT, the free wall of the right ventricle, the intracavitary trabeculae, the moderating band, and the right side of the interventricular septum (Figure 4).Tansey et al. showed on autopsies of individuals without known heart disease that 85% of them had myocardial infiltrates with adipose tissue [46]. Mainly, the RVOT, free wall of RV wall, apex, and RV antero-lateral wall are affected, but these intramyocardial deposits do not change the thickness of the ventricular wall or the regional contraction. If the deposits extend from the epicardium to the endocardium, crossing the myocardium, then the ventricular wall may increase in size as a normal feature of the adipose distribution. It seems that these fat deposits in healthy people increase with age and are more common in obese people without being pathological [47].
- (e)
- Thinning of the RV wallThis is a component that was not included in the Task Force Criteria for the diagnosis of ARVC [12,45]. This is because the reports of different authors were not consistent with regards to the thinning or thickening of the ventricular wall. Therefore, thinning of the wall is considered pathological only when associated with contraction abnormalities at the same level [48] (Figure 6).
- (f)
- Hypertrabeculation of intracavitary structures such as papillary muscles or moderator band occurs as a result of infiltration with adipose tissue. Although it can be present in up to 40% of patients with ARVC, it can also occur in various other diseases; therefore, it is not considered a Task Force Criterion for the diagnosis of ARVC.
- (g)
- Delayed enhancementThe significance of delayed enhancement in cardiac MRI is fibrosis, edema, or inflammation [49]. It is not possible to clearly differentiate the exact cause of the increase in the extracellular volume. The abnormal tissue causes gadolinium retention while normal myocardial tissue does not. It is estimated that approximately 67% of patients with ARVC have delayed enhancement of the ventricular walls. In the study of Tandri et al. [49], 6 out of 10 patients with ARVC presented induced VT during electrophysiological study, and 4 did not have induced VT. It is relevant to mention that among patients with inducible VT, all six had delayed enhancement in cardiac MRI, and among those who were not inducible, only one had delayed enhancement in MRI.
3.2. Left Ventricle CMR Evaluation in ARVC
3.3. Right Atrium Involvement: CMR Evaluation of ARVC
3.4. Moderator Band Involvement in ARVC: CMR Features
4. Review of Unique ARVC Characteristics in Children
5. Cardiac MRI Pitfalls in ARVC
6. Concluding Remarks
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Priori, S.G.; Aliot, E.; Blomstrom-Lundqvist, C.; Bossaert, L.; Breithardt, G. Task Force on Sudden Cardiac Death of the European Society of Cardiology. Eur. Heart J. 2001, 22, 1374–1450. [Google Scholar] [CrossRef] [PubMed]
- Sen-Chowdhry, S.; Lowe, M.D.; Sporton, S.C.; McKenna, W.J. Arrhythmogenic right ventricular cardiomyopathy: Clinical presentation, diagnosis, and management. Am. J. Med. 2004, 117, 685–695. [Google Scholar] [CrossRef] [PubMed]
- Boxt, L.M. Cardiac MR Imaging: A guide for the beginner. RadioGraphics 1999, 19, 1009–1025, discussion, 1026–1028. [Google Scholar] [CrossRef]
- Martin, E.T.; Coman, J.A.; Shellock, F.G.; Pulling, C.C.; Fair, R.; Jenkins, K. Magnetic resonance imaging and cardiac pacemaker safety at 1.5-Tesla. J. Am. Coll. Cardiol. 2004, 43, 1315–1324. [Google Scholar] [CrossRef] [Green Version]
- Daubert, C.; Descaves, C.; Foulgoc, J.-L.; Bourdonnec, C.; Laurent, M.; Gouffault, J. Critical analysis of cineangiographic criteria for diagnosis of arrhythmogenic right ventricular dysplasia. Am. Heart J. 1988, 115, 448–459. [Google Scholar] [CrossRef]
- Pennell, D.; Casolo, G. Right ventricular arrhythmia: Emergence of magnetic resonance imaging as an investigative tool. Eur. Heart J. 1997, 18, 1843–1845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campuzano, O.; Sarquella-Brugada, G.; Arbelo, E.; Cesar, S.; Jordà, P.; Pérez-Serra, A.; Toro, R.; Brugada, J.; Brugada, R. Genetic Variants as Sudden-Death Risk Markers in Inherited Arrhythmogenic Syndromes: Personalized Genetic Interpretation. J. Clin. Med. 2020, 9, 1866. [Google Scholar] [CrossRef]
- Corrado, D.; Thiene, G.; Nava, A.; Rossi, L.; Pennelli, N. Sudden death in young competitive athletes: Clinicopathologic correlations in 22 cases. Am. J. Med. 1990, 89, 588–596. [Google Scholar] [CrossRef]
- Basso, C.; Corrado, D.; Thiene, G. Cardiovascular causes of sudden death in young individuals including athletes. Cardiol. Rev. 1999, 7, 127–135. [Google Scholar] [CrossRef]
- Dalal, D.; Nasir, K.; Bomma, C.; Prakasa, K.; Tandri, H.; Piccini, J.; Roguin, A.; Tichnell, C.; James, C.; Russell, S.D.; et al. Arrhythmogenic right ventricular dysplasia a United States experience. Circulation 2005, 112, 3823–3832. [Google Scholar] [CrossRef]
- Firoozi, S.; Sharma, S.; Hamid, M.S.; McKenna, W.J. Sudden death in young athletes: HCM or ARVC? Cardiovasc. Drugs Ther. 2002, 16, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Marcus, F.I.; McKenna, W.J.; Sherrill, D.L.; Basso, C.; Bauce, B.; Bluemke, D.; Calkins, H.; Corrado, D.; Cox, M.G.; Daubert, J.P.; et al. Diagnosis of arrhythmogenic right ventricular cardiomyopathy/dysplasia: Proposed Modification of the Task Force Criteria. Eur. Heart J. 2010, 31, 806–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, A.P.; Farb, A.; Tashko, G.; Virmani, R. Arrhythmogenic Right Ventricular Cardiomyopathy and Fatty Replacement of the Right Ventricular Myocardium: Are They Different Diseases? Circulation 1998, 97, 1571–1580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saberniak, J.; Leren, I.S.; Haland, T.F.; Beitnes, J.O.; Hopp, E.; Borgquist, R.; Edvardsen, T.; Haugaa, K.H. Comparison of patients with early-phase arrhythmogenic right ventricular cardiomyopathy and right ventricular outflow tract ventricular tachycardia. Eur. Heart J. Cardiovasc. Imaging 2016, 18, 62–69. [Google Scholar] [CrossRef] [Green Version]
- Wei, J.; Tang, J.; Xia, L.; Chen, X.; Wang, D.W. A case of Arrhythmogenic right ventricular cardiomyopathy without arrhythmias. Diagnostic Pathol. 2012, 7, 67. [Google Scholar] [CrossRef] [Green Version]
- Marcus, I.F.; Fontaine, G.H.; Guiraudon, G.; Frank, R.; Laurenceau, J.L.; Malergue, C.; Grosgogeat, Y. Right ventricular dysplasia: A report of 24 adult cases. Circulation 1982, 65, 384–398. [Google Scholar] [CrossRef] [Green Version]
- Celbis, O.; Aydin, N.; Mizrak, B.; Ozdemir, B. Arrhythmogenic Right Ventricular Dysplasia Cases in Forensic Autopsies. Am. J. Forensic Med. Pathol. 2007, 28, 235–237. [Google Scholar] [CrossRef]
- Mu, J.; Zhang, G.; Xue, D.; Xi, M.; Qi, J.; Dong, H. Sudden cardiac death owing to arrhythmogenic right ventricular cardiomyopathy: Two case reports and systematic literature review. Medicine 2017, 96, 47. [Google Scholar] [CrossRef]
- Nava, A.; Thiene, G.; Canciani, B.; Scognamiglio, R.; Daliento, L.; Buja, G.; Martini, B.; Stritoni, P.; Fasoli, G. Familial occurrence of right ventricular dysplasia: A study involving nine families. J. Am. Coll. Cardiol. 1988, 12, 1222–1228. [Google Scholar] [CrossRef] [Green Version]
- Basso, C.; Thiene, G.; Corrado, D.; Angelini, A.; Nava, A.; Valente, M. Arrhythmogenic Right Ventricular Cardiomyopathy Dysplasia, Dystrophy, or Myocarditis? Circulation 1996, 94, 983–991. [Google Scholar] [CrossRef]
- Corrado, D.; Basso, C.; Judge, D. Arrhythmogenic Cardiomyopathy. Circ. Res. 2017, 121, 784–802. [Google Scholar] [CrossRef] [Green Version]
- Sen-Chowdhry, S.; Syrris, P.; Ward, D.; Asimaki, A.; Sevdalis, E.; McKenna, W.J. Clinical and genetic characterization of families with arrhythmogenic right ventricular dysplasia/cardiomyopathy provides novel insights into patterns of disease expression. Circulation 2007, 115, 1710–1720. [Google Scholar] [CrossRef] [Green Version]
- Zghaib, T.; Ghasabeh, M.A.; Assis, F.R.; Chrispin, J.; Keramati, A.; Misra, S.; Tandri, H. Regional Strain by Cardiac Magnetic Resonance Imaging Improves Detection of Right Ventricular Scar Compared With Late Gadolinium Enhancement on a Multimodality Scar Evaluation in Patients With Arrhythmogenic Right Ventricular Cardiomyopathy. Circ. Cardiovasc. Imaging 2018, 11, e007546. [Google Scholar] [CrossRef] [Green Version]
- Zhang, P.; Dasaro, A. Arrhythmogenic right ventricular dysplasia/cardiomyopathy versus dilated right ventricular cardiomyopathy: A problematic autopsy diagnosis? Int. J. Clin. Exp. Pathol. 2016, 9, 3373–3380. [Google Scholar]
- Nava, A.; Bauce, B.; Basso, C.; Muriago, M.; Rampazzo, A.; Villanova, C.; Daliento, L.; Buja, G.; Corrado, D.; Danieli, G.A.; et al. Clinical profile and long-term follow-up of 37 families with arrhythmogenic right ventricular cardiomyopathy. J. Am. Coll. Cardiol. 2000, 36, 2226–2233. [Google Scholar] [CrossRef] [Green Version]
- Rastegar, N.; Zimmerman, S.L.; Te Riele, A.S.J.M.; James, C.; Burt, J.R.; Bhonsale, A.; Kamel, I.R. Spectrum of Biventricular Involvement on CMR Among Carriers of ARVD/C-Associated Mutations. JACC Cardiovasc. Imaging 2015, 8, 863–864. [Google Scholar] [CrossRef] [Green Version]
- Fox, P.R.; Maron, B.J.; Basso, C.; Liu, S.K.; Thiene, G. Spontaneously occurring arrhythmogenic right ventricular cardiomyopathy in the domestic cat: A new animal model similar to the human disease. Circulation 2000, 102, 1863–1870. [Google Scholar] [CrossRef] [Green Version]
- Basso, C.; Fox, P.R.; Meurs, K.M.; Towbin, J.A.; Spier, A.W.; Calabrese, F.; Maron, B.J.; Thiene, G. Arrhythmogenic right ventricular cardiomyopathy causing sudden cardiac death in boxer dogs: A new animal model of human disease. Circulation 2004, 109, 1180–1185. [Google Scholar] [CrossRef] [Green Version]
- Li, G.; Fontaine, G.H.; Fan, S.; Yan, Y.; Bode, P.K.; Duru, F.; Frank, R.; Sagunetr, A.M. Right atrial pathology in arrhythmogenic right ventricular dysplasia. Cardiol. J. 2019, 26, 736–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cismaru, G.; Grosu, A.; Istratoaie, S.; Mada, L.; Ilea, M.; Gusetu, G.; Zdrenghea, D.; Pop, D.; Rosu, R. Transesophageal and intracardiac ultrasound in arrhythmogenic right ventricular dysplasia/cardiomyopathy. Medicine 2020, 99, e19817-7. [Google Scholar] [CrossRef]
- Gemayel, C.; Pelliccia, A.; Thompson, P.D. Arrhythmogenic right ventricular cardiomyopathy. J. Am. Coll. Cardiol. 2001, 38, 1773–1781. [Google Scholar] [CrossRef] [Green Version]
- Bauce, B.; Frigo, G.; Benini, G.; Michieli, P.; Basso, C.; Folino, A.F.; Nava, A. Differences and similarities between arrhythmogenic right ventricular cardiomyopathy and athlete’s heart adaptations. Br. J. Sports Med. 2010, 44, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Yoerger, D.M.; Marcus, F.; Sherrill, D.; Calkins, H.; Towbin, J.A.; Zareba, W.; Picard, M.A.; Multidisciplinary Study of Right Ventricular Dysplasia Investigators. Echocardiographic findings in patients meeting task force criteria for arrhythmogenic right ventricular dysplasia: New insights from the multidisciplinary study of right ventricular dysplasia. J. Am. Coll. Cardiol. 2005, 6, 860–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Ascenzi, F.; Pisicchio, C.; Caselli, S.; Di Paolo, F.M.; Spataro, A.; Pelliccia, A. RV Remodeling in Olympic Athletes. JACC Cardiovasc. Imaging 2017, 4, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Basso, C.; Tiene, G. Adipositas cordis, fatty infltration of the right ventricle, and arrhythmogenic right ventricular cardiomyopathy. Just a matter of fat? Cardiovasc. Pathol. 2005, 14, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Tandri, H.; Saranathan, M.; Rodriguez, E.R.; Martinez, C.; Bomma, C.; Nasir, K.; Rosen, B.; Lima, J.A.; Calkins, H.; Bluemke, D.A. Noninvasive detection of myocardial fibrosis in arrhythmogenic right ventricular cardiomyopathy using delayed-enhancement magnetic resonance imaging. J. Am. Coll. Cardiol. 2005, 45, 98–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrado, D.; Basso, C.; Thiene, G.; McKenna, W.J.; Davies, M.J.; Fontaliran, F.; Nava, A.; Silvestri, F.; Blomstrom-Lundqvist, C.; Wlodarska, E.K.; et al. Spectrum of clinicopathologic manifestations of arrhythmogenic right ventricular cardiomyopathy/dysplasia: A multicenter study. J. Am. Coll. Cardiol. 1997, 30, 1512–1520. [Google Scholar] [CrossRef] [Green Version]
- Zghaib, T.; Bourfiss, M.; van der Heijden, J.F.; Loh, P.; Hauer, R.N.; Tandri, H.; Calkins, H.; Nazarian, S.; Te Riele, A.S.J.M.; Zimmerman, S.L.; et al. Atrial Dysfunction in Arrhythmogenic Right Ventricular Cardiomyopathy. Circ. Cardiovasc. Imaging 2018, 11, e007344. [Google Scholar] [CrossRef] [Green Version]
- Chu, A.F.; Zado, E.; Marchlinski, F.E. Atrial arrhythmias in patients with arrhythmogenic right ventricular cardiomyopathy/dysplasia and ventricular tachycardia. Am. J. Cardiol. 2010, 106, 720–722. [Google Scholar] [CrossRef]
- Bourfiss, M.; Te Riele, A.S.; Mast, T.P.; Cramer, M.J.; Van Der Heijden, J.F.; Van Veen, T.A.; Loh, P.; Dooijes, D.; Hauer, R.N.; Velthuis, B.K. Influence of genotype on structural atrial abnormalities and atrial fibrillation or flutter in arrhythmogenic right ventricular dysplasia/cardiomyopathy. J. Cardiovasc. Electrophysiol. 2016, 27, 1420–1428. [Google Scholar] [CrossRef] [PubMed]
- Brembilla-Perrot, B.; Jacquemin, L.; Houplon, P.; Houriez, P.; Beurrier, D.; Berder, V.; Terrier de la Chaise, A.; Louis, P. Increased atrial vulnerability in arrhythmogenic right ventricular disease. Am. Heart J. 1998, 135, 748–754. [Google Scholar] [CrossRef]
- Casolo, G.C.; Poggesi, L.; Boddi, M.; Fazi, A.; Bartolozzi, C.; Lizzadro, G.; Dabizzi, R.P. ECG-gated magnetic resonance imaging in right ventricular dysplasia. Am. Heart J. 1987, 113, 1245–1248. [Google Scholar] [CrossRef]
- Motevali, M.; Siahi, Z.; Mohammadzadeh, A.; Sangi, A. Cardiac Magnetic Resonance Imaging (MRI) Findings in Arrhythmogenic Right Ventricular Dysplasia (ARVD) Compared with Echocardiography. Med. Sci. 2018, 6, 80. [Google Scholar] [CrossRef] [Green Version]
- Selthofer-Relatić, K.; Belovari, T.; Bijelić, N.; Kibel, A.; Rajc, J. Presence of Intramyocardial Fat Tissue in the Right Atrium and Right Ventricle-Postmortem Human Analysis. Acta Clin. Croat. 2018, 57, 122–129. [Google Scholar] [CrossRef]
- McKenna, W.J.; Thiene, G.; Nava, A.; Fontaliran, F.; Blomstrom-Lundqvist, C.; Fontaine, G.; Camerini, F. Diagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Task Force of the Working Group Myocardial and Pericardial Disease of the European Society of Cardiology and of the Scientific Council on Cardiomyopathies of the International Society and Federation of Cardiology. Br. Heart J. 1994, 71, 215–218. [Google Scholar]
- Tansey, D.K.; Aly, Z.; Sheppard, M.N. Fat in the right ventricle of the normal heart. Histopathology 2003, 46, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Imada, M.; Funabashi, N.; Asano, M.; Uehara, M.; Hori, Y.; Ueda, M.; Komuro, I. Epidemiology of fat replacement of the right ventricular myocardium determined by multislice computed tomography using a logistic regression model. Int. J. Cardiol. 2007, 119, 410–413. [Google Scholar] [CrossRef]
- Naneix, A.L.; Périer, M.C.; Beganton, F.; Jouven, X.; Lorin de la Grandmaison, G. Sudden adult death: An autopsy series of 534 cases with gender and control comparison. J. Forensic Leg. Med. 2015, 32, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Tandri, H.; Bomma, C.; Calkins, H.; Bluemke, D.A. Magnetic resonance and computed tomography imaging of arrhythmogenic right ventricular dysplasia. J. Magn. Reson. Imaging 2004, 19, 848–858. [Google Scholar] [CrossRef]
- Elgendy, A. Arrhythmogenic Right Ventricular Cardiomyopathy. 2018. Available online: https://radiopaedia.org/cases/arrhythmogenic-right-ventricular-cardiomyopathy-4 (accessed on 1 July 2021).
- Thiene, G.; Corrado, D.; Basso, C. Arrhythmogenic right ventricular cardiomyopathy/dysplasia. Orphanet J. Rare Dis. 2007, 2, 45. [Google Scholar] [CrossRef] [PubMed]
- Rastegar, N.; Burt, J.R.; Corona-Villalobos, C.P.; Te Riele, A.S.; James, C.A.; Murray, B.; Calkins, H.; Tandri, H.; Bluemke, D.A.; Zimmerman, S.L.; et al. Cardiac MR findings and potential diagnostic pitfalls in patients evaluated for arrhythmogenic right ventricular cardiomyopathy. Radiographics 2014, 34, 1553–1570. [Google Scholar] [CrossRef] [Green Version]
- El Ghannudi, S.; Nghiem, A.; Germain, P.; Jeung, M.Y.; Gangi, A.; Roy, C. Left ventricular involvement in arrhythmogenic right ventricular cardiomyopathy—A cardiac magnetic resonance imaging study. Clin. Med. Insights Cardiol. 2015, 8 (Suppl. 4), 27–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, M.T.; Yang, Z.G.; Diao, K.Y.; Jiang, L.; Zhang, Y.; Liu, X.; Gao, Y.; Hu, B.Y.; Huang, S.; Guo, Y.K. Left Ventricular Involvement in Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy Predicts Adverse Clinical Outcomes: A Cardiovascular Magnetic Resonance Feature Tracking Study. Sci. Rep. 2019, 9, 14235. [Google Scholar] [CrossRef]
- Berte, B.; Denis, A.; Amraoui, S.; Yamashita, S.; Komatsu, Y.; Pillois, X.; Sacher, F.; Mahida, S.; Wielandts, J.Y.; Sellal, J.M.; et al. Characterization of the Left-Sided Substrate in Arrhythmogenic Right Ventricular Cardiomyopathy. Circ. Arrhythm Electrophysiol. 2015, 8, 1403–1412. [Google Scholar] [CrossRef] [Green Version]
- Mattesi, G.; Cipriani, A.; Bauce, B.; Rigato, I.; Zorzi, A.; Corrado, D. Arrhythmogenic Left Ventricular Cardiomyopathy: Genotype-Phenotype Correlations and New Diagnostic Criteria. J. Clin. Med. 2021, 10, 2212. [Google Scholar] [CrossRef] [PubMed]
- Hadi, S.; Memduh, D.; Ahmet, K.B. The role of magnetic resonance imaging in diagnosis of arrhythmogenic right ventricle dysplasia. Namık Kemal Med. J. 2019, 7, 110–117. [Google Scholar]
- Luijkx, T.; Velthuis, B.K.; Prakken, N.H.; Cox, M.G.; Bots, M.L.; Mali, W.P.T.M.; Cramer, M.J. Impact of revised Task Force Criteria: Distinguishing the athlete’s heart from ARVC/D using cardiac magnetic resonance imaging. Eur. J. Prev. Cardiol. 2012, 19, 885–891. [Google Scholar] [CrossRef]
- Tavano, A.; Maurel, B.; Gaubert, J.Y.; Varoquaux, A.; Cassagneau, P.; Vidal, V.; Bartoli, J.M.; Moulin, G.; Jacquier, A. MR imaging of arrhythmogenic right ventricular dysplasia: What the radiologist needs to know. Diagn. Interv. Imaging 2015, 96, 449–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sievers, B.; Addo, M.; Franken, U.; Trappe, H.J. Right Ventricular Wall Motion Abnormalities Found in Healthy Subjects by Cardiovascular Magnetic Resonance Imaging and Characterized with a New Segmental Model. J. Cardiovasc. Magn. Reason. 2004, 3, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Lahtinen, A.M.; Lehtonen, E.; Marjamaa, A.; Kaartinen, M.; Heliö, T.; Porthan, K.; Oikarinen, L.; Toivonen, L.; Swan, H.; Jula, A.; et al. Population-prevalent desmosomal mutations predisposing to arrhythmogenic right ventricular cardiomyopathy. Heart Rhythm. 2011, 8, 1214–1221. [Google Scholar] [CrossRef]
- DeWitt, E.S.; Chandler, S.F.; Hylind, R.J.; Beausejour Ladouceur, V.; Blume, E.D.; Van Der Pluym, C.; Powell, A.J.; Fynn-Thompson, F.; Roberts, A.E.; Sanders, S.P.; et al. Phenotypic Manifestations of Arrhythmogenic Cardiomyopathy in Children and Adolescents. J. Am. Coll. Cardiol. 2019, 74, 346–358. [Google Scholar] [CrossRef] [PubMed]
- Ohno, S.; Nagaoka, I.; Fukuyama, M.; Kimura, H.; Itoh, H.; Makiyama, T.; Shimizu, A.; Horie, M. Age-dependent clinical and genetic characteristics in Japanese patients with arrhythmogenic right ventricular cardiomyopathy/dysplasia. Circ. J. 2013, 77, 1534–1542. [Google Scholar] [CrossRef] [Green Version]
- Pawel, B.R.; de Chadarévian, J.P.; Wolk, J.H.; Donner, R.M.; Vogel, R.L.; Braverman, P. Sudden death in childhood due to right ventricular dysplasia: Report of two cases. Pediatr. Pathol. 1994, 14, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Marcus, F.I.; Fontaine, G.H.; Frank, R.; Gallagher, J.J.; Reiter, M.J. Long-term follow-up in patients with arrhythmogenic right ventricular disease. Eur. Heart J. 1989, 10 (Suppl. D), 68–73. [Google Scholar] [CrossRef]
- Blomström-Lundqvist, C.; Sabel, K.G.; Olsson, S.B. A long term follow up of 15 patients with arrhythmogenic right ventricular dysplasia. Br. Heart J. 1987, 58, 477–488. [Google Scholar] [CrossRef] [Green Version]
- Daliento, L.; Terrini, P.; Nava, A.; Rizzoti, G.; Angelini, A.; Buja, G.; Scognamiglio, R.; Thiene, G. Arrhythmogenic right ventricular cardiomiyopathy in young versus adult patients. Similarities and differences. J. Am. Cardiol. 1995, 25, 655–664. [Google Scholar]
- Thiene, G.; Nava, A.; Corrado, D.; Rossi, L.; Pennelli, N. Right ventricular cardiomyopathy and sudden death in young people. N. Engl. J. Med. 1988, 318, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Buja, G.; Nava, A.; Daliento, L.; Scognamiglio, R.; Miorelli, M.; Canciani, B.; Alampi, G.; Thiene, G. Right ventricular cardiomyopathy in identical and nonidentical young twins. Am. Heart J. 1993, 126, 1187–1193. [Google Scholar] [CrossRef]
- Groeneweg, J.A.; Bhonsale, A.; James, C.A.; Te Riele, A.S.; Dooijes, D.; Tichnell, C.; Murray, B.; Wiesfeld, A.C.; Sawant, A.C.; Kassamali, B.; et al. Clinical Presentation, Long-Term Follow-Up, and Outcomes of 1001 Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy Patients and Family Members. Circ. Cardiovasc. Genet. 2015, 8, 437–446. [Google Scholar] [CrossRef]
- Pilichou, K.; Thiene, G.; Bauce, B.; Rigato, I.; Lazzarini, E.; Migliore, F.; Marra, M.P.; Rizzo, S.; Zorzi, A.; Daliento, L.; et al. Arrhythmogenic cardiomyopathy. Orphanet J. Rare Dis. 2016, 11, 33. [Google Scholar] [CrossRef] [Green Version]
- Barskiy, V. Arrhythmogenic Right Ventricular Cardiomyopathy. 2019. Available online: https://radiopaedia.org/cases/arrhythmogenic-right-ventricular-cardiomyopathy-3 (accessed on 1 July 2021).
- Marcus, F.I.; Zareba, W.; Calkins, H.; Towbin, J.A.; Basso, C.; Bluemke, D.A.; Estes, N.A., 3rd; Picard, M.H.; Sanborn, D.; Thiene, G.; et al. Arrhythmogenic right ventricular cardiomyopathy/dysplasia clinical presentation and diagnostic evaluation: Results from the North American Multidisciplinary Study. Heart Rhythm. 2009, 6, 984–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scalco, A.; Liboni, C.; Angioni, R.; Di Bona, A.; Albiero, M.; Bertoldi, N.; Fadini, G.P.; Thiene, G.; Chelko, S.P.; Basso, C.; et al. Arrhythmogenic Cardiomyopathy Is a Multicellular Disease Affecting Cardiac and Bone Marrow Mesenchymal Stromal Cells. J. Clin. Med. 2021, 10, 1871. [Google Scholar] [CrossRef] [PubMed]
- Grosse-Wortmann, L.; Etoom, Y.; Govindapillai, S.; McCrindle, B.; Manlhiot, C.; Yoo, S.-J. MRI in childhood Arrhythmogenic Right Ventricular Cardiomyopathy and proposed modification of the Task Force Criteria for children. J. Cardiovasc. Magn. Reson. 2012, 14, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Staab, W.; Lauerer, P.; Fasshauer, M.; Krause, U.J.; Sohns, J.S.; Schuster, A.; Unterberg-Buchwald, C.; Paul, T.; Lotz, J.; Steinmetz, M. Cardiac magnetic resonance imaging in pediatric patients ≤ 18 years with suspected arrhythmogenic right ventricular cardiomyopathy (ARVC): A correlation to genetics. J. Cardiovasc. Magn. Reson. 2015, 17 (Suppl. 1), 269. [Google Scholar] [CrossRef] [Green Version]
- Deshpande, S.R.; Herman, H.K.; Quigley, P.C.; Shinnick, J.K.; Cundiff, C.A.; Caltharp, S.; Shehata, B.M. Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia (ARVC/D): Review of 16 Pediatric Cases and a Proposal of Modified Pediatric Criteria. Pediatr. Cardiol. 2016, 37, 646–655. [Google Scholar] [CrossRef]
- Martins, D.; Ovaert, C.; Khraiche, D.; Boddaert, N.; Bonnet, D.; Raimondi, F. Myocardial inflammation detected by cardiac MRI in arrhythmogenic right ventricular cardiomyopathy: A paediatric case series. Int. J. Cardiol. 2018, 271, 81–86. [Google Scholar] [CrossRef]
- Sabel, K.G.; Blomström-Lundqvist, C.; Olsson, S.B.; Eneström, S. Arrhythmogenic right ventricular dysplasia in brother and sister: Is it related to myocarditis? Pediatr. Cardiol. 1990, 11, 113–116. [Google Scholar] [CrossRef]
- Que, D.; Yang, P.; Song, X.; Liu, L. Traditional vs. genetic pathogenesis of arrhythmogenic right ventricular cardiomyopathy. Europace 2015, 17, 1770–1776. [Google Scholar] [CrossRef]
- Patrianakos, A.P.; Protonotarios, N.; Nyktari, E.; Pagonidis, K.; Tsatsopoulou, A.; Parthenakis, F.; Vardas, P. Arrhythmogenic right ventricular cardiomyopathy/dysplasia and troponin release. Myocarditis or the “hot phase” of the disease? Int. J. Cardiol. 2012, 157, e26–e28. [Google Scholar] [CrossRef]
- Tanawuttiwat, T.; Sager, S.J.; Hare, J.M.; Myerburg, R.J. Myocarditis and ARVC/D: Variants or mimics? Heart Rhythm. 2013, 10, 1544–1548. [Google Scholar] [CrossRef]
- Scheel, P.J., 3rd; Murray, B.; Tichnell, C.; James, C.A.; Tandri, H.; Calkins, H.; Chelko, S.P.; Gilotra, N.A. Arrhythmogenic Right Ventricular Cardiomyopathy Presenting as Clinical Myocarditis in Women. Am. J. Cardiol. 2021, 145, 128–134. [Google Scholar] [CrossRef]
- Bomma, C.; Rutberg, J.; Tandri, H.; Nasir, K.; Roguin, A.; Tichnell, C.; Rodriguez, R.; James, C.; Kasper, E.; Spevak, P.; et al. Misdiagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy. J. Cardiovasc. Electrophysiol. 2004, 15, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Costa, S.; Gasperetti, A.; Medeiros-Domingo, A.; Akdis, D.; Brunckhorst, C.; Saguner, A.M.; Duru, F. Familial Arrhythmogenic Cardiomyopathy: Clinical Determinants of Phenotype Discordance and the Impact of Endurance Sports. J. Clin. Med. 2020, 9, 3781. [Google Scholar] [CrossRef]
- Amadu, A.M.; Baritussio, A.; Dastidar, A.G.; De Garate, E.; Rodrigues, J.C.L.; Biglino, G.; Lyen, S.; Diab, I.; Duncan, E.; Nisbet, A.; et al. Arrhythmogenic right ventricular cardiomyopathy (ARVC) mimics: The knot unravelled by cardiovascular MRI. Clin. Radiol. 2019, 74, 228–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scharhag, J.; Schneider, G.; Urhausen, A.; Rochette, V.; Kramann, B.; Kindermann, W. Athlete’s heart: Right and left ventricular mass and function in male endurance athletes and untrained individuals determined by magnetic resonance imaging. J. Am. Coll. Cardiol. 2002, 10, 1856–1863. [Google Scholar] [CrossRef] [Green Version]
- Ng, A.C.T.; Strudwick, M.; van der Geest, R.J.; Ng, A.C.C.; Gillinder, L.; Goo, S.Y.; Cowin, G.; Delgado, V.; Wang, W.Y.S.; Bax, J.J. Impact of Epicardial Adipose Tissue, Left Ventricular Myocardial Fat Content, and Interstitial Fibrosis on Myocardial Contractile Function. Circ. Cardiovasc. Imaging 2018, 11, e007372. [Google Scholar] [CrossRef] [Green Version]
- Cannavale, G.; Francone, M.; Galea, N.; Vullo, F.; Molisso, A.; Carbone, I.; Catalano, C. Fatty Images of the Heart: Spectrum of Normal and Pathological Findings by Computed Tomography and Cardiac Magnetic Resonance Imaging. BioMed Res. Int. 2018, 2018, 5610347. [Google Scholar] [CrossRef]
- IMMER, F.; Romanens, M.; Saner, H. Visualising fatty deposits in familial arrhythmogenic right ventricular cardiomyopathy by magnetic resonance imaging. Heart 2000, 84, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ichikawa, Y.; Kitagawa, K.; Chino, S.; Ishida, M.; Matsuoka, K.; Tanigawa, T.; Nakamura, T.; Hirano, T.; Takeda, K.; Sakuma, H. Adipose tissue detected by multislice computed tomography in patients after myocardial infarction. JACC Cardiovasc. Imaging 2009, 2, 548–555. [Google Scholar] [CrossRef] [Green Version]
- Kaminaga, T.; Naitou, H.; Hamada, S.; Takamiya, M. Detection of myocardial fatty components with ultrafast CT. Nippon Igaku Hoshasen Gakkai zasshi. Nippon Acta Radiol. 1993, 53, 28–34. [Google Scholar]
- Lutokhina, Y.; Blagova, O.; Varionchik, N.; Alexandrova, S.; Gagarina, N.; Kogan, E.; Sedov, V.; Shestak, A.; Zaklyazminskaya, E.; Nedostup, A. Three Myocardial Diseases in One Heart: Arrhythmogenic Right Ventricular Cardiomyopathy, Left Ventricular Noncompaction and Myocarditis. Cardiogenetics 2021, 11, 18–27. [Google Scholar] [CrossRef]
- Li, F.P.; Xiao, Y.B.; Wang, W.F. A 23-year-old male with Uhl’s anomaly. J. Card. Surg. 2011, 26, 435–439. [Google Scholar] [CrossRef]
- Gerlis, L.M.; Schmidt-Ott, S.C.; Ho, S.Y.; Anderson, R.H. Dysplastic conditions of the right ventricular myocardium: Uhl’s anomaly vs. arrhythmogenic right ventricular dysplasia. Br. Heart J. 1993, 69, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Marcus, F.I. Is arrhythmogenic right ventricular dysplasia, Uhl’s anomaly and right ventricular outflow tract tachycardia a spectrum of the same disease? Cardiol. Rev. 1997, 5, 25–29. [Google Scholar] [CrossRef]
- Quarta, G.; Husain, S.I.; Flett, A.S.; Sado, D.M.; Chao, C.Y.; Tomé Esteban, M.T.; McKenna, W.J.; Pantazis, A.; Moon, J.C. Arrhythmogenic right ventricular cardiomyopathy mimics: Role of cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reason. 2013, 15, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritz, J.; Solaiyappan, M.; Tandri, H.; Bomma, C.; Genc, A.; Claussen, C.D.; Lima, J.A.; Bluemke, D.A. Right ventricle shape and contraction patterns and relation to magnetic resonance imaging findings. J. Comput. Assist. Tomogr. 2005, 29, 725–733. [Google Scholar] [CrossRef] [Green Version]
- Yared, K.; Johri, A.M.; Soni, A.V.; Johnson, M.; Alkasab, T.; Cury, R.C.; Hung, J.; Mamuya, W. Cardiac sarcoidosis imitating arrhythmogenic right ventricular dysplasia. Circulation 2008, 118, e113–e115. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.S.; Ko, S.M.; Song, M.G. Linear fat deposition in the middle later of the left ventricular myocardium: Computed tomographic fndings. Korean J. Radiol. 2010, 11, 571–573. [Google Scholar] [CrossRef] [Green Version]
- Grebenc, M.L.; de Christenson, M.L.R.; Burke, A.P.; Green, C.E.; Galvin, J.R. Primary cardiac and pericardial neoplasms: Radiologic-pathologic correlation. Radiographics 2000, 20, 1073–1103. [Google Scholar] [CrossRef] [Green Version]
- Araoz, P.A.; Eklund, H.E.; Welch, T.J.; Breen, J.F. CT and MR imaging of primary cardiac malignancies. Radiographics 1999, 19, 1421–1434. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.; Assis, F.; James, C.A.; Murray, B.; Tichnell, C.; Tandri, H.; Calkins, H. Misdiagnosis of ARVC leading to inappropriate ICD implant and subsequent ICD removal-lessons learned. J. Cardiovasc. Electrophysiol. 2019, 30, 2020–2026. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Type | Limitations |
|---|---|---|
| 1 | Epicardial fat | Epicardial adipose tissue is distributed in the antero-apical region of the right ventricle in 15% of the general population; furthermore, in obese patients, the percentage can increase to 50% which should be differentiated from the adipose tissue of ARVC [88]. |
| 2 | Moderator band | Contraction abnormalities observed near the insertion of the moderator band. Images can be misinterpreted as akinesia, dyskinesia, or hypokinesia of the ventricular wall. Sievers et al. showed in 29 healthy individuals that small contraction abnormalities occurred in 93% of the examined individuals near the moderator band [60]. |
| 3 | Short-axis images | Another limitation of cardiac MRI comes from the scarce analysis of short-axis images. The incidences are used for the correct assessment of the right ventricular size. If short-axis images are not used, there is a 20% chance that the radiologist will incorrectly measure right ventricular size and inadvertently assuming RV dilation [86]. |
| 4 | Adipose tissue | Adipose tissue infiltration of the right ventricular myocardium can be misinterpreted as arrhythmogenic dysplasia. False positive images of intramyocardic adipose tissue may be recorded by the radiologist. Furthermore, pericardial fat distributed on the surface of a thin myocardium may give a false image of adipose infiltration. The inter-individual reproducibility of adipose tissue images is poor, by virtue of (a) adipose tissue disposition at the epicardial and pericardial level in healthy individuals, and sometimes intramyocardial; (b) epicardial fat disposition at the level of the right atrioventricular groove—in cardiac MRI, this area is rather difficult to distinguish from the subtricuspid muscle zone, which might be affected by ARVC; (c) the right ventricular wall is thin, at 3–5 mm, and therefore the spatial resolution on cardiac MRI is poor, which can lead to diagnostic confusions [86,89,90]. |
| 5 | Athlete’s heart | Another possible source of error in athletic individuals is the enlargement of the right ventricle associated with intense and long duration physical activity. Large ventricular and RVOT diameters can be misinterpreted as ARVC, but the increase in the RA and RV size is symmetrical compared to the asymmetrical changes produced by ARVC [79,80,82,83]. |
| 6 | Viral myocarditis | Viral myocarditis can affect the regional contraction of the right ventricle; the decrease in contractility can be misinterpreted as being related to ARVC [32,58,87]. |
| 7 | Right ventricular myocardial infarction | In myocardial infarction, necrotic tissue is replaced by fibrous or adipose tissue (which is called “fibrous or adipose metaplasia”). Post-infarction lesions of the right ventricle resemble and should be differentiated from ARVC lesions, especially if infarction occurred > 6 months prior to cardiac MRI [91,92] |
| 8 | Dilated cardiomyopathy (DCM) | In dilated cardiomyopathy, in addition to areas of fibrosis, lymphocyte infiltration, and myocyte degeneration, myocardial fibro-adipose infiltration may be present. These fatty infiltrates may be present in 18–24% of DCM cases [92,93]. |
| 9 | Uhl’s anomaly | Uhl’s anomaly is a rare congenital disease without areas of fibro-fatty dysplasia. However, there is complete absence of the myocardium that causes the ventricular wall to be thin. Uhl’s disease is extremely rare and generally the diagnosis is made post-mortem. Echocardiography shows a dilated right ventricle, with thin walls 1–2 mm at all levels. In cardiac MRI, the ventricular wall is extremely thin, the myocardium of the free wall is missing, and the trabeculations at the apical level are minimal. Although there is no fibro-fatty infiltration, the systolic function is impaired. The differentiation in cardiac MRI between the two diseases is critical because Uhl’s disease progresses towards right heart failure, in contrast to ARVC, which leads to life-threatening ventricular arrhythmias. For Uhl’s disease, no primary prevention is available, but for ARVC, there is a primary prevention of sudden cardiac death by implanting an internal cardiac defibrillator [94,95,96,97]. |
| 10 | Rib cage abnormalities | Another possible source of error is the structural change of the rib cage. In pectus excavatum, the position of the heart within the thorax changes and the heart becomes compressed between the sternum and the vertebral column, giving a false image of dilated right ventricle. In addition, the mediastinum may be shifted to the left and may mimic right ventricular dyskinesia, which can be interpreted as ARVC. |
| 11 | Box-shaped RV | Physiological changes of the right ventricle may mimic ARVC. In case of a box-shaped right ventricle, the anterior wall has an irregular trajectory, with a slight protrusion of the middle portion of the anterior wall, which can be confused with a dyskinetic RV [98]. |
| 12 | Sarcoidosis | Sarcoidosis is another source of confusion in that the areas affected by granulomas may be hypokinetic, become aneurysmal, or have delayed enhancement, thus mimicking ARVC [99]. |
| 13 | Lipomatous hypertrophy of the interatrial septum | Lipomatous hypertrophy of the interatrial septum is characterized by accumulation of adipose tissue inside the interatrial septum; the transverse diameter of the septum increases over 2 cm. This change must be differentiated from ARVC with concomitant atrial impairment. Nonetheless, in lipomatous hypertrophy, the oval fossa is spared, and contrast enhancement is never present [100]. |
| 14 | Hypertrophic cardiomyopathy | Hypertrophic cardiomyopathy. In this disease, 11% of patients may have deposits of adipose tissue inside the hypertrophied myocardium. However, the differentiation between the two diseases is straightforward because in ARVC, the myocardium is not thickened but is replaced with fat [100]. |
| 15 | Cardiac lipomas | Cardiac lipomas are the second most common benign tumors of the heart, after myxomas. Unlike ARVC, lipomas may be located intramyocardially; however, cardiac lipomas are well defined and sometimes encapsulated [101]. |
| 16 | Cardiac liposarcoma | Liposarcomas are a type of aggressive but very rare tumors that look inhomogeneous on cardiac MRI and generally affect the right chambers, starting with the right atrium and extending to the right ventricle. However, these tumors are destructive, affecting and destroying blood vessels and heart valves, a feature that helps in the differential with ARVC [102]. |
| 17 | Radiological experience | The radiologist interpreting images of suspected ARVC should have sufficient experience, considering the fact that in early stages of the disease the differential diagnosis must be made with other diseases that have similar characteristics [84,103]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cainap, S.-S.; Kovalenko, I.; Bonamano, E.; Crousen, N.; Tirpe, A.; Cismaru, A.; Iacob, D.; Lazea, C.; Negru, A.; Cismaru, G. Anatomical-MRI Correlations in Adults and Children with Arrhythmogenic Right Ventricular Cardiomyopathy. Diagnostics 2021, 11, 1388. https://doi.org/10.3390/diagnostics11081388
Cainap S-S, Kovalenko I, Bonamano E, Crousen N, Tirpe A, Cismaru A, Iacob D, Lazea C, Negru A, Cismaru G. Anatomical-MRI Correlations in Adults and Children with Arrhythmogenic Right Ventricular Cardiomyopathy. Diagnostics. 2021; 11(8):1388. https://doi.org/10.3390/diagnostics11081388
Chicago/Turabian StyleCainap, Simona-Sorana, Ilana Kovalenko, Edoardo Bonamano, Niclas Crousen, Alexandru Tirpe, Andrei Cismaru, Daniela Iacob, Cecilia Lazea, Alina Negru, and Gabriel Cismaru. 2021. "Anatomical-MRI Correlations in Adults and Children with Arrhythmogenic Right Ventricular Cardiomyopathy" Diagnostics 11, no. 8: 1388. https://doi.org/10.3390/diagnostics11081388