
Clinical Phenotypes of COVID-19 Associated Mucormycosis (CAM): A Comprehensive Review
by
 , ,
, ,
Maria Panagiota Almyroudi
1, 
Karolina Akinosoglou
2,
Jordi Rello
3,
Stijn Blot
4,5 and
George Dimopoulos
6,* 1
Department of Emergency Medicine, University Hospital Attikon, Medical School, National and Kapodistrian University of Athens, 12462 Athens, Greece
2
Department of Internal Medicine and Infectious Diseases, University General Hospital of Patras, School of Medicine University of Patras, 26504 Rio, Greece
3
Vall d’Hebron Institute of Research, Barcelona, Spain & Clinical Research, CHU Nîmes, 30900 Nîmes, France
4
Department of Internal Medicine and Pediatrics, Ghent University, 9000 Ghent, Belgium
5
UQ Centre for Clinical Research, Faculty of Medicine, The University of Queensland, Brisbane 4029, Australia
6
3rd Department of Critical Care, EVGENIDIO Hospital, Medical School, National and Kapodistrian University of Athens, 11528 Athens, Greece
*
Author to whom correspondence should be addressed.
Diagnostics 2022, 12(12), 3092; https://doi.org/10.3390/diagnostics12123092
Submission received: 10 November 2022
/
Revised: 2 December 2022
/
Accepted: 6 December 2022
/
Published: 8 December 2022
(This article belongs to the Special Issue Emerging and Re-emerging Infectious Diseases: Diagnosis and Management)
Abstract
:A mucormycosis surge was reported during the COVID-19 pandemic in India. A literature search until 14 July 2022, with the aim of updating COVID-19-associated mucormycosis (CAM), identified 663 studies and 88 met inclusion criteria (8727 patients). India reported 8388 patients, Egypt 208 and Europe 40. Rhino-orbito-cerebral mucormycosis (ROCM) was identified among 8082 (98.3%) patients, followed by 98 (1.2%) with pulmonary. In India, 82.6% of patients had diabetes mellitus, with 82% receiving corticosteroids. In Europe, 75% presented pulmonary CAM, 32.5% had diabetes and 40% were immunocompromised. CAM was identified at a median of 17.4 days (IQR 7.5 days) post COVID-19 diagnosis, and PCR was performed in five studies. Rhino-orbital invasion is clinically obvious, while cerebral involvement presents with cavernous sinus thrombosis, meningitis and cerebrovascular disease. Symptoms of pulmonary CAM usually overlap with severe COVID-19 pneumonia. High-dose liposomal Amphotericin B (and early surgical debridement in ROCM) are the mainstay of therapy. The median mortality rate was estimated to be 21.4% (IQR 31.9%), increased by the presence of pulmonary (80% (IQR 50%) or cerebral involvement (50% (IQR 63.9%). In summary, different CAM clinical phenotypes need to be distinguished, influenced by geographical presentation. Opportunities exist for diagnosis and therapy optimization, based on earlier high-dose antifungal therapy, early source control, strict glycemic control and restriction of steroids to COVID-19 patients with oxygen requirements.
1. Introduction
Mucormycosis is a rare infection caused the members of the order Mucorales. Its prevalence ranges from 0.005 to 1.7 per million people worldwide, while in India, it reaches 14 cases per 100,000 inhabitants [1,2]. During the COVID-19 pandemic, a surge in mucormycosis cases has been observed, especially in India, where the Government of India portal reported 47,508 cases from 5 May 2021 to 3 August 2021 [3]. Characteristically, Samir Joshi et al. reported 160 cases of COVID-19-associated mucormycosis (CAM) from April to May 2021 in the Ear, Nose, Throat Department of BJGMC-SGH hospital in India, compared with 3–8 cases of mucormycosis detected each year from 2016 to 2020 [4].
Invasive fungal infections may complicate COVID-19, as immunological alterations, intense inflammatory response and lung damage favor fungal growth [5]. Aspergillosis is most often reported, but mucormycosis has also emerged and been associated with COVID-19. The most common fungi isolated are Mucor and Rhizopus, followed by Cunninghamella sp., Saksenaea sp., Lichtheimia sp., Apophysomyces sp., Rhizomucor sp. and Cokeromyces sp. [5]. They are ubiquitous in nature and the spores are transmitted mainly by inhalation, leading to sinus or lung infection, by ingestion or by direct inoculation following trauma. They cause invasive disease in vulnerable patients with predisposing medical conditions and risk factors including immunosuppression, diabetes mellitus (DM), corticosteroid treatment, hematologic malignancies, hematopoietic cell transplantation, solid organ transplantation and iron overload [6,7]. Different types of mucormycosis are recognized, with rhino-orbito-cerebral mucormycosis (ROCM) and the pulmonary form being the most common clinical presentations [6].
The fungus usually first infects the nasal mucosa and the palate and subsequently spreads to paranasal sinuses and to the retro-orbital space through the ethmoid sinus [8]. It spreads through direct regional extension and vascular and perineural invasion, while angioinvasion results in thrombi formation, tissue infarction and necrosis. Immune dysregulation with impaired phagocytosis, endothelial dysfunction, hyperglycemia, hypoxia, acidosis and hyperferritinemia, seen with COVID-19, create favorable conditions for fungal growth [5]. Mucorales spores escape phagocytosis and transform into hyphae, enabling tissue invasion [5]. Neutrophil dysfunction, in the context of COVID-19, DM and steroid use, plays an important role in the pathogenesis of CAM. As macrophage function and polymorphonuclear chemotaxis is impaired in diabetics, spores escape phagocytosis, germinate, enlarge and convert to hyphae which invade the tissues and vessels [2]. Additionally, in an acidic environment, as in diabetic ketoacidosis, the binding capacity of transferrin is reduced and free iron is released into the circulation. Iron is then absorbed in a solubilized form by Mucorales spores. Elevated ferritin levels are commonly found in COVID-19 patients, reflecting high iron levels, which act as a substrate for fungal overgrowth [2].
The aim of this review is to present the current data in the literature concerning the incidence, risk factors, pathophysiology, diagnosis, outcome and treatment of CAM.
2. Methods
The literature was explored using the search string “((COVID *) OR (SARS-CoV2) OR (SARS-CoV-2)) AND (mucor *)” in Pubmed (EMBASE). Observational trials, interventional trials and case series (the latter consisting of ≥5 CAM patients) until 14 July 2022 were considered for inclusion. Only studies written in English, with available full article and using the diagnostic criteria for mucormycosis proposed by the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium [6] were included. In addition, studies including patients with invasive fungal infections in general, and not mucormycosis specifically, and studies including mucormycosis cases not associated with COVID-19 and not separately with CAM cases were excluded. Sixteen studies were excluded due to unavailable–insufficient information [9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24]. Four studies were excluded as they included patients with non-microbiologically confirmed SARS-CoV-2 infection [25,26,27,28]. Figure 1 reports a PRISMA flow-chart detailing the selected studies and exclusion criteria.
The quality of the included articles was assessed by means of the Quality Assessment Tool for Case Series Studies by the National Heart, Lung and Blood Institute (NHLBI). Two authors independently screened the literature search results and executed data extraction (MPA, GD). In each study, data regarding the type of the study, the country of origin, the setting of actualization, the number of CAM patients, the reported CAM incidence, the interval between COVID-19 and CAM diagnosis, the type of infection, the comorbidities and risk factors for CAM, the performance of PCR and the identification of species and the outcome were sought and registered when they were mentioned. The median mortality rate and median interval between COVID-19 diagnosis and CAM diagnosis were calculated according to the formula p = (n + 1)/2 where n is the size of the data set and p is the position of the median value. The PRISMA 2020 checklist is detailed in Appendix A.
3. Incidence of CAM
The literature search revealed 662 studies, of which, ultimately, 88 studies were included in the review. Overall, only 13/88 studies were prospective. According to the Quality Assessment Tool for Case Series Studies by the National Heart, Lung and Blood Institute (NHLBI), 32 studies were rated as good quality studies, 42 as fair quality studies and 14 as poor quality studies (Table 1).
A total of 8727 cases of CAM are reported in the 88 qualified studies (Table 1), the majority of them from India (n = 8388, 96.1%), 208 patients (2.4%) were from Egypt and 40 patients (0.46%) from Europe (France and Germany) (Figure 2). CAM cases have also been reported in USA [41], Pakistan [70], Iran [84], Oman [113], Syria [115], Iraq [116], Latin America [117] and Turkey [7].
The incidence of CAM largely remains unknown, as 12 studies out of 88 have mentioned CAM incidence (Table 2). In India, CAM incidence (September 2020–June 2021) ranged from 0.27% to 3.36% among hospitalized and microbiologically confirmed COVID-19 patients and the rhino-orbital-cerebral form represented the majority of cases (Table 2) [32,44,61,80,82,102]. Among seven centers in India, the prevalence of CAM was estimated to be 0.27% in general wards (28/10,517 COVID-19 patients) and 1.6% (25/1579) in ICUs [102]. However, Casalini et al., reported an average incidence of 8.6% among hospitalized COVID-19 patients in a review including 12 observational studies and 3126 cases of CAM [118]. A higher incidence was estimated among kidney transplant COVID-19 patients in India in two studies (4.4% and 10.8%) [40,42] Notably, during a 6-month period of the pandemic, 61 kidney transplant patients were diagnosed with CAM, in contrast with only 11 patients who had been diagnosed with mucormycosis during the previous year [42].
Similar characteristics are observed in Egypt. Sahar Farghly Youssif et al. reported an incidence of CAM of 7.6% among 433 patients with confirmed COVID-19 infection [107]. ROCM was identified in 207/208 (99.5%) CAM patients with only 1/208 (0.5%) having lung involvement.
On the other hand, in Europe, the reported incidence is much lower, but still, COVID-19 patients seem to be more affected, and interestingly, the pulmonary form is the most prevalent clinical presentation (Table 2). In France, among 473,353 COVID-19 patients hospitalized from March 2020 to June 2021, only 17 cases were considered as CAM nationwide (0.0036%) [57]. In two German tertiary centers, the CAM prevalence from January 2020 to June 2021 was 0.67% and 0.58%, respectively, while it was much lower in non-COVID-19 patients (0.0047% and 0.001%, respectively). In the same centers, in the ICUs, the prevalence of CAM was 1.47% and 1.78%, while in non-COVID-19 patients the prevalence of mucormycosis was 0.015% and 0.005% [76].
In the ICU, the prevalence of mucormycosis was estimated at 0.3–0.8% of COVID-19 admissions, based on data from four centers in France, Germany, Mexico and Turkey [7], while in a national, observational cohort study in 18 ICUs across France, among 509 COVID-19 mechanically ventilated patients who were systematically screened for respiratory fungal infections, 6 (1%) were diagnosed with invasive mucormycosis [119]. Analogously, in another German study, among 100 COVID-19 ICU patients whose respiratory specimens were checked routinely for Mucorales via culture and PCR, only one PCR in the bronchoalveolar lavage (BAL) came out positive for Mucorales (1%) [120]. However, a cluster of cases was detected in a French ICU, during a two month period, which was possibly linked to construction work that was undertaken near the ICU [62].
4. Risk Factors
Generally, 82.4% (6824/8279) of CAM patients were either diabetics or developed hyperglycemia during COVID-19 illness. In India, Egypt and Europe, 82.6%, 84.6% and 32.5% of patients had DM, respectively (Table 2). Poorly controlled DM is the strongest risk factor for mucormycosis described in the literature. In a case control study, the level of hyperglycemia was associated with the risk of CAM development, with the highest risk reported for patients with blood glucose >400 mg/dL [36]. Among 26 patients with CAM, the mean HbA1c was 9.3% (8–10.7%) [33], while diabetic ketoacidosis was noticed in 40% (27/67) of patients with CAM [32]. Except for preexisting DM, hyperglycemia that develops during COVID-19 illness, induced by the virus infection (viral-mediated islet cell destruction) or attributed to steroid treatment, contributes, respectively, to CAM emergence.
Corticosteroids have been established as the standard therapy for severe COVID-19, which increases the risk of secondary infections [121]. Overall, 81.6% (5777/7058) of patients with CAM had received steroids, 82% of Indian cases, 81.6% of Egyptian and 82.5% of European (Table 2). In many cases, steroid administration was considered as inappropriate, as they were given even in mild COVID-19 disease [33]. Finally, in a large Indian study, among 2826 patients with CAM, only 2% (n = 47) were neither diabetic, nor had they received corticosteroids [83], underlining the determinant role of these risk factors. Immunosuppression, hematological malignancies and solid organ or bone marrow transplantation are also well-known risk factors for invasive fungal infections. Forty percent of CAM patients in Europe were immunosuppressed, while 7/73 (9.6%) of patients with COVID-19-associated pulmonary mucormycosis had hematological malignancy. Danion et al. [57] described 17 cases of CAM in France, where, in contrast to Indian reports, fewer patients were diabetics (47%) and a higher proportion had hematological malignancies (41%) [57]. Other comorbidities identified in the literature are hypertension, chronic kidney disease, liver disease and ischemic heart disease (Table S1).
Ultimately, whether COVID-19 independently predisposes patients to mucormycosis infection needs to be studied further. In a prospective cohort study, among 540 proven cases of mucormycosis from March to May 2021, 89.4% of patients had a history of previous COVID-19 infection [31]. Two hundred and eighty-eight/2801 (10.3%) of CAM patients had been submitted to invasive or non-invasive mechanical ventilation during hospitalization for COVID-19 according to data contained in 32 studies (Table 2). However, the severity of COVID-19 pneumonia does not seem to determine the development of COVID-19-associated ROCM. In a prospective observational study from India, 7.9% of 101 patients with post-COVID-19 ROCM were asymptomatic, 36% had mild disease, 40% had moderate disease and only 15.8% had severe disease [58]. Vare et al. emphasized that 22% of cases did not receive any supplemental oxygen [32], while according to CT criteria, the average severity of COVID-19 pneumonia complicated by ROCM was described as moderate [49]. The emergence of ROCM in non-severe COVID-19 is either associated with the determinant role of DM in the pathogenesis of CAM or may be related to the early death of critically ill patients before symptoms of mucormycosis develop. However, pulmonary mucormycosis is more often described in ICU patients, reflecting a possible association with severe COVID-19 pneumonia (Table S3).
In multivariable analysis, in a case control study, risk factors that were independently associated with CAM were diabetes, glucose levels >200 mg/dL during the course of COVID-19, steroid use, mild and moderate (vs. severe) COVID-19 and repeated swab tests [36]. Additionally, in two studies, ferritin levels were significantly higher in patients with CAM compared to COVID-19 patients without mucormycosis [36,40] Zinc consumption is another risk factor discussed in the literature. Zinc was widely used as a nutrient supplement during the second wave of the pandemic in India and was significantly associated with CAM in a case–control study [60]. However, the relationship between zinc exposure and CAM remains controversial, as another study revealed opposite results, with zinc supplementation being more frequently used among COVID-19 patients without mucormycosis (79.9% vs. 53.8%, p < 0.001) [36].
Especially in India, the high prevalence of CAM is attributed to regional environmental factors, especially climatological conditions (hot and humid), to high incidence of uncontrolled DM and possibly to poor healthcare system conditions, as transmission of fungal spores through water used for oxygen humidifiers is speculated [8,118]. In a multi-centre study, including 11 hospitals in India, Mucorales contamination of 11.1% of air-conditioning vents was found, mainly with Rhizopus spp. [122]. CAM was also associated with prolonged use of cloth masks (4–6 h, p = 0.002; >6 h, p < 0.0001) and surgical masks (>6 h, p = 0.002) [36].
5. Clinical Presentation
CAM was diagnosed after a median of 17.4 days (Q1:14.4, Q3:21.8, IQR 7.5 days) post COVID-19 diagnosis (Table S1) but simultaneous manifestation with acute COVID-19 is also reported. Mucormycosis may be associated with neuroinflammation of the acute phase or be integrated in the post-COVID-19 syndrome [123]. However, the long period that is mediated between COVID-19 positivity and CAM diagnosis may actually reflect a delay in diagnosis, that may be associated with a higher mortality [33].
Mucormycosis most commonly affects the head and neck region. ROCM is the commonest form globally and was also the most frequent form associated with COVID-19. ROCM was diagnosed in 8082/8218 (98.3%) CAM patients and pulmonary infection in 98/8218 (1.2%), of whom 30.6% were in Europe. (Table 2). Mucormycosis of the gastrointestinal tract was found in 5/8218 (0.06%) CAM patients, cutaneous in 11/8218 (0.13%), disseminated in 11/8218 (0.13%) and renal in 1/8218 (0.01%) (Table 2). In Europe 3/40 (7.5%) of CAM patients had ROCM, 30/40 (75%) had pulmonary mucormycosis, 4/40 (10%) mucormycosis of the gastrointestinal tract and 3/40 (7.5%) disseminated (Figure 3).
Clinical manifestations of head and neck mucormycosis include headache, loosening of teeth, black necrotic turbinate, facial pain, facial palsy, peri-orbital or facial swelling, skin induration and blackish discoloration [35]. Symptoms attributed to nasal and oral cavity invasion include epistaxis, bloody nasal discharge and palate destruction. Orbital extension may lead to destruction of the ophthalmic artery and optic nerves resulting in ptosis of the eyelid, proptosis, vision disturbances and blindness. In a large retrospective study from India, 519/2716 (19%) patients with CAM presented with vision loss [83]. Cavernous sinus involvement occurs due to extension from the orbit and manifests as diplopia and ophthalmoplegia [8].
Cerebral involvement was noted in 1400/7388 (18.9%) patients with COVID-19 associated ROCM, reported in 72 studies (Table 2). Cerebral involvement may manifest as cavernous sinus thrombosis, fungal abscess, meningitis and cerebrovascular disease [73]. Rahul Kulkarni et al. noted that 45/49 (91.8%) of patients with cerebral involvement presented with ischemic stroke, which concerned large artery infracts, followed by intracranial hemorrhage in 3/49 (6.1%) and sub-arachnoid hemorrhage in 1/49 (2.0%) [44].
Ninety-eight patients with pulmonary mucormycosis are described in the literature (57 in India, 30 in Europe, 6 in Pakistan, 3 in USA, 1 in Egypt and 1 in Mexico) (Table S3). Ten studies contained data on ventilatory support, with invasive or non-invasive mechanical ventilation reported in 26/45 (57.8%) of patients with COVID-19-associated pulmonary mucormycosis. In 7 studies where CAPA was sought, 19/43 (44.2%) patients with pulmonary mucormycosis were found with positive microbiological testing for Aspergillus. Symptoms of pulmonary mucormycosis in non-ventilated patients include fever, dyspnea, cough, chest pain and hemoptysis [124]. Pruthi et al. reported five cases of pulmonary mucormycosis associated with COVID-19 that were complicated by pulmonary artery pseudoaneurysm [39]. In mechanically ventilated patients, identification of an agent of mucormycosis from respiratory specimens in combination with compatible radiographic findings support the diagnosis.
Symptoms of mucormycosis of the gastrointestinal tract are non-specific and consist of abdominal pain and distension, diarrhea and gastrointestinal bleed [124], while disseminated mucormycosis may affect any organ, but mainly the brain and lungs, and is a result of bloodstream invasion in severely immunocompromised patients [124].
6. Diagnosis
Early recognition of CAM is crucial, as delay in therapy is associated with higher mortality [42]. A high index of suspicion should be maintained when clinical symptoms and radiological features appear in a patient with predisposing factors. According to criteria proposed by the European Confederation of Medical Mycology and the Mycoses Study Group Education and Research Consortium [6], the diagnosis of mucormycosis is based on clinical and imaging characteristics and confirmed with direct microscopy, histopathologic analysis and culture of samples obtained with biopsy.
Diagnosis is challenging, as appropriate specimens are obtained through invasive procedures and specific stains are needed to identify Mucorales. Direct microscopy with potassium hydroxide (KOH) mount is usually used for the rapid diagnosis of mucormycosis, as results are delayed with culture and histopathology. Direct microscopy reveals wide, non-septate, ribbon-like hyaline hyphae, with irregular right-angled branching that are characteristic of Mucorales [125]. Ιnfarcts, angioinvasion and perineural invasion are usually present in the histological analysis. Preceding antifungal therapy may alter morphological characteristics of the fungus, while specimens’ processing must be carefully undertaken to keep hyphae intact [2]. Even when fungal hyphae are recognized in histopathological analysis, cultures may be negative in 50% of cases, due to the fragility of fungal hyphae [125]. Characteristically, among 2175 patients with CAM, direct microscopy with KOH/calcofluor white was performed in 89% (1931), and culture in 19% (432), of cases [83].
Molecular techniques are promising, as rapid detection is needed and cultures are time-consuming and may be false-negative [124]. However, results should be cautiously evaluated due to ubiquitous nature of Mucorales. PCR was performed in five studies in the literature (two French, two from India and one from Egypt) and concerned 174 patients, of which 31 were positive (Table S4). In the French study [57], PCR was positive in 15/17 (88%) patients with CAM in serum (n = 14), BAL (n = 7), tissues (n = 3) and peritoneal fluid (n = 1) [57]. It is of interest that, in another French study [62], Mucorales was detected with PCR in respiratory samples of 10 COVID-19 patients, of which 80% simultaneously tested positive for Aspergillus. This cluster of cases was possibly attributed to environmental exposure, due to construction work near the hospital [62].
Few studies in the literature report on the species isolated, reflecting the difficulties encountered with culture-based identification and the infrequent use of PCR. Rhizopus sp. were the most common species isolated (Table S3). In a study including 203 cases of mucormycosis with positive cultures during the second wave of the pandemic in India, Rhizopus oryzae, followed by R. microspores, were most frequently identified [126].
Mixed infections with Aspergillus and Candida are detected both in pulmonary and rhino-orbital-cerebral form. Eighteen studies in the literature (12 from India, 3 from Europe, 2 from Pakistan and 1 from Egypt) refer to Aspergillus possible co-infection, with Aspergillus being isolated in 89/863 (10.3%) CAM patients (Table S4). Danion et al., reported 5 mixed fungal infections with Aspergillus in 17 (29%) CAM cases, of which 2 exhibited pulmonary involvement, 1 ROCM, 1 disseminated and 1 GI disease. All patients were mechanically ventilated and COVID-19-associated pulmonary aspergillosis (CAPA) was diagnosed at a median of 2 days before CAM. Four out of five patients with CAM and CAPA received L-Amphotericin B (one was diagnosed after death) and 5/5 died [57]. In Toulouse, France, eight cases of concomitant infection with Mucor and Aspergillus were detected in the ICU and were attributed to construction work that was undertaken near the hospital. All patients had pulmonary involvement, 3/8 were treated with L-Amphotericin B, 4/8 with a combination of L-Amphotericin B and Posaconazole and/or isavuconazole and 1/8 with isavuconazole. Four out of eight (50%) patients died [62]. Aspergillus fumigatus, Aspergillus niger and Aspergillus nidulans have been isolated [70], while mixed mold infections with Candida are also described in the literature [66,67]. Nidhya Ganesan et al. reported that among 60 biopsy samples from suspected rhino-maxillary/rhino-orbital mucormycosis post COVID-19, mucorales was isolated in 58 (96.67%) samples, aspergillus along with mucorales in 12 (20%) and a combination of mucorales and candida in 8 (13.33%) [24].
Neither 1,3-beta-D-glucan assay and galactomannan are positive in mucormycosis but can aid in the diagnosis of invasive pulmonary aspergillosis, which is recognized as a severe superinfection of COVID-19 pneumonia resulting in higher mortality. A positive serum or BAL galactomannan in a patient with compatible clinical presentation and imaging findings is indicative of invasive aspergillosis [127]. BAL galactomannan was measured in the study of R.H. Mehta et al. and was found positive (≥1) in 4/5 cases of COVID-19-associated pulmonary mucormycosis. In two cases, Aspergillus fumigatus was isolated in fungal culture, while in three cases, Aspergillus was identified in histopathological analysis [89]. Ultimately, mixed infection should be actively searched and isavuconazole is a potential empirical choice if mixed infection is suspected.
7. Imaging
CT and MRI imaging contribute to diagnosis and determine disease extension. Imaging evaluation in CAM is similar to mucormycosis not complicating COVID-19. Radiological findings include signs of sinusitis (thickened mucosa, opacification of the paranasal sinuses, air fluid levels), orbital invasion, cavernous sinus thrombosis and infiltration, internal carotid artery infiltration, cerebritis, cerebral infraction, thrombosis of the surface veins and dural venous sinuses, mycotic aneurysms, subarachnoid hemorrhage and abscess formation [8]. Bone destruction may be detected, as 79% of 96 patients with ROCM exhibited bony erosions [49]. The “black turbinate sign” on MRI is characterized by lack of contrast enhancement as a result of turbinate necrosis but can also be found in other circumstances [8]. CT and MRI-scan imaging are necessary for disease staging [35]. In pulmonary CAM, imaging findings recorded in CT were a reversed halo sign (8% of patients), consolidation (83%), cavitation (33%) and nodules (6%) [57]. Other CT findings include the halo sign, pleural effusion and wedge-shaped infiltrates [125].
8. Treatment
High-dose liposomal amphotericin B is the first line treatment for mucormycosis [6]. It is well established that antifungals are insufficient alone in treating ROCM and surgical debridement is needed, as the removal of necrotic tissues is necessary to allow antifungal penetration and is associated with better prognosis [128]. Lipid formulation of amphotericin B is preferred over Amphotericin B deoxycholate due to less nephrotoxicity and better CNS penetration. The starting dose of liposomal amphotericin B is in the range of 5–7.5 mg/kg/day and 10 mg/kg/day for brain involvement. Resistance of certain strains to amphotericin B is noted, with amphotericin B being ineffective against Cunninghamella bertholletiae and Apophysomyces elegans [124]. In India, due to shortages of liposomal amphotericin B, amphotericin B deoxycholate was also administered [83].
Isavuconazole and posaconazole are indicated as rescue therapy or in cases with preexisting renal failure [6]. However, due to deficiency of liposomal amphotericin B in India during the second wave of the COVID-19 pandemic, isavuconazole and posaconazole were also used as first line agents. Specifically, Soni et al. used oral posaconazole for mild cases of mucormycosis, along with surgical debridement [34]. With posaconazole DR tablets, increased bioavailability is achieved, while the drug can also be infused intravenously. Posaconazole suspension is not supported due to variable bioavailability, while steady state is achieved earlier with DR tablet formulation. Trough levels of posaconazole should be monitored and levels >1.0 μg/mL are pursued [129]. In a study by Atul Patel et al., 24.1% of patients (7/29) had a posaconazole trough level <1.2 μg/mL. They arbitrarily used 1.2 μg/mL as a cut off level, as posaconazole was used off label as a primary treatment for invasive mucormycosis due to shortage of amphotericin B. Antifungal therapy was changed to amphotericin B when subtherapeutic levels were detected [3]. Isavuconazole exhibits less hepatotoxicity and drug interactions, while therapeutic drug monitoring is not required and is not approved for prophylaxis. In immunocompromised patients or refractory cases, a combination of liposomal amphotericin B with echinocandins or posaconazole or isavuconazole may prove beneficial [124].
Other antifungals against mucormycosis were also tested during the pandemic and the recent surge of CAM due to unavailability of first-line agents. Specifically, Gupta et al. reported that susceptibility of Mucorales to itraconazole and terbinafine was species dependent, as 97.7% of R. oryzae and 36.5% of R. microsporus had MIC ≤ 2 µg/mL for itraconazole, while 85.2% of R. microsporus had MIC ≤ 2 µg/mL for terbinafine [126]. The use of iron chelators is under debate in the literature. Deferiprone and Deferasirox have in vitro activity against Mucorales [125], but have not been found to be beneficial for mucormycosis treatment [2]. No data were found in the literature concerning hyperbaric oxygen therapy. Patients with orbital involvement and intact vision can be managed with complementary transcutaneous retrobulbar amphotericin B (TRAMB) injections. A satisfactory response was noticed especially in patients without necrosis, as 40% of them showed improvement of visual acuity and/or ocular movement [31].
Early initiation of antifungal therapy and surgical removal of operable lesions are the mainstay of management for mucormycosis [39]. Surgical debridement of necrotic tissues is required among ROCM infections and multiple sessions may be needed to treat residual and recurrent disease [128].
In summary, management is based on three pillars: high-dose antifungal therapy, early source control when feasible and optimized management of associated conditions. Therefore, both strict glycemic control and restricted use of corticosteroids among COVID-19 patients requiring supplementary oxygen administration are essential to reverse predisposing factors [124].
9. Outcome
Median all-cause mortality rate was estimated to be 21.4% (Q1:14.3, Q3:46.2, IQR 31.9%). The median mortality among CAM patients with cerebral involvement was 50% (Q1:25, Q3:88.9, IQR 63.9%) and among CAM patients with pulmonary involvement, 80% (Q1:50, Q3:100, IQR 50%) (Table 2, Tables S5 and S6). When data were searched for the contribution of cerebral and pulmonary involvement to mortality rate, 142/237 (59.9%) patients who died (from 24 studies) were found with intracranial disease and 43/101 (42.6%) patients who died (from 13 studies) were found with pulmonary involvement (Tables S5 and S6). The median mortality rate in India was 18.2% (Q1:12.3, Q3:30.3, IQR 18), in Europe, 53.8%, and in the rest of the world, 39.8% (Q1:18.8, Q3:63.4, IQR 44.6).
Mortality rates vary in the literature. This is likely the result of the different forms of the disease, the challenging diagnosis, especially for pulmonary mucormycosis, and the association with either mild, moderate or severe COVID-19, which also affects mortality. In Europe, mortality ranges from 53.8% to 88% (Table 2). Data on mucormycosis-related mortality are lacking in the literature. In a national survey in Germany, including 13 patients with CAM from 6 tertiary care hospitals, all-cause mortality was 53.8% and mucormycosis-attributable mortality was 15.3% [76].
Delay in identification of CAM may be an important prognostic factor [128], as in studies where both mortality rates and the time period between COVID-19 and CAM diagnosis were recorded, median mortality was 33.7% (Q1:16.7, Q3:51, IQR 34.3%) when CAM diagnosis was performed after 15 days from COVID-19 diagnosis and 23.4% (Q1:15.5, Q3:50, IQR 34.5%) when it was performed ≤15 days post COVID-19 diagnosis.
In multivariate regression analysis in a study including 73 consecutive CAM patients, history of mechanical ventilation due to COVID-19 was associated with a 9-fold increased risk of death (p = 0.003) [45]. Other factors significantly associated with mortality were older age (>40 years), intracranial involvement, Hb1AC >9.1%, (n = 540) [31] advanced stage of ROCM, qSOFA ≥ 2 (n = 105) [58], chronic kidney disease, renal dysfunction during hospital stay, orbital involvement and tocilizumab use (n = 84) [54].
10. Limitations
The limitations of our review are the small number of prospective studies included (11/88) and the lack of studies comparing characteristics and outcomes of CAM patients with COVID-19 patients without mucormycosis. A high risk of bias was noted due to missing information on the incidence of CAM and heterogeneity in mortality rates was observed among studies mainly due to the different forms of mucormycosis included and diverse mortality endpoints used.
11. Conclusions
Our literature review suggests that COVID-19 may be complicated by secondary invasive fungal infections, including mucormycosis. Important geographical differences were identified and need to be taken into consideration. CAM was mainly reported in India, with an incidence of 0.27% to 3.36% among hospitalized COVID-19 patients. In India, near all reports were ROCM in patients with uncontrolled DM and history of corticosteroids intake. On the other hand, the most prevalent presentation in Europe was as pulmonary mucormycosis, particularly among hematologically immunocompromised patients with severe COVID-19. Patients with kidney transplant also seem to be exposed to a higher risk. Based on our findings, CAM was diagnosed a median of 17.4 days (IQR 7.5 days) post COVID-19. Since rapid diagnosis is crucial, molecular diagnostic techniques have to be generalized. Concomitant Aspergillus isolates were identified in 19/43 (44.2%) pulmonary mucormycosis reports and 89/863 (10.3%) CAM cases. Reported all-cause mortality was estimated to have a median of 21.4% (IQR 31.9%) (in ROCM with cerebral involvement 50% (IQR 63.9%), while in pulmonary, it was 80% (IQR 50%) and in India, it was 18.2% (IQR 18), while in Europe, it was 53.8%. When two weeks was used as the threshold for the diagnosis of CAM, median mortality was 23.4% (IQR 34.5%) vs. 33.7% (IQR 34.3%) after two weeks. Altogether, these studies revealed that an optimization of therapy is crucial, based on earlier high-dose antifungal therapy administration, early source control with repeated debridement when feasible, strict glycemic control and restriction of steroid therapy to COVID-19 patients with additional oxygen requirements.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/diagnostics12123092/s1, Table S1: Interval between CAM diagnosis and COVID-19 diagnosis and other comorbidities described; Table S2: Cases of pulmonary mucormycosis associated with COVID-19; Table S3: Studies containing data on PCR and species identification; Table S4: Concomitant Aspergillus isolation; Table S5: Outcome, Table S6: Percentage of deaths with cerebral and pulmonary involvement.
Funding
This review received no external funding.
Acknowledgments
We are indebted to K Esharwara Vandana, Department of Microbiology, Kasturba Medical college, Manipal Academy of Higher Education, India, for critical review of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
| Section and Topic | Item # | Checklist Item | Location Where Item is Reported |
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | Pages 1,2 |
| ABSTRACT | |||
| Abstract | 2 | See the PRISMA 2020 for Abstracts checklist. | Page 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | Pages 1,2 |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | Pages 1,2 |
| METHODS | |||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | Pages 2,3 |
| Information sources | 6 | Specify all databases, registers, websites, organizations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | Pages 2,3 |
| Search strategy | 7 | Present the full search strategies for all databases, registers and websites, including any filters and limits used. | Pages 2,3 |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently and, if applicable, details of automation tools used in the process. | Pages 2,3 |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators and, if applicable, details of automation tools used in the process. | Pages 2,3 |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points, analyses) and if not, the methods used to decide which results to collect. | Page 3 |
| 10b | List and define all other variables for which data were sought (e.g., participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. | Page 3 | |
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently and, if applicable, details of automation tools used in the process. | Page 3 |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g., risk ratio, mean difference) used in the synthesis or presentation of results. | NA |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis (e.g., tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). | Tables |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics or data conversions. | NA | |
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | Tables | |
| 13d | Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used. | NA | |
| 13e | Describe any methods used to explore possible causes of heterogeneity among study results (e.g., subgroup analysis, meta-regression). | NA | |
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | NA | |
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | Page 3 |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | NA |
| RESULTS | |||
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | Figure 1 |
| 16b | Cite studies that might appear to meet the inclusion criteria, but which were excluded and explain why they were excluded. | Pages 2,3 | |
| Study characteristics | 17 | Cite each included study and present its characteristics. | Table 1 |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | Table 1 |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g., confidence/credible interval), ideally using structured tables or plots. | Tables |
| Results of syntheses | 20a | For each synthesis, briefly summarize the characteristics and risk of bias among contributing studies. | Table 1 |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was performed, present, for each, the summary estimate and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | Pages 3–10 | |
| 20c | Present results of all investigations of possible causes of heterogeneity among study results. | Heterogeneity observed in mortality rates, causes page 10 | |
| 20d | Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. | NA | |
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | NA |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | NA |
| DISCUSSION | |||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | Pages 3–10 |
| 23b | Discuss any limitations of the evidence included in the review. | Page 10 | |
| 23c | Discuss any limitations of the review processes used. | NA | |
| 23d | Discuss implications of the results for practice, policy and future research. | Page 10 | |
| OTHER INFORMATION | |||
| Registration and protocol | 24a | Provide registration information for the review, including register name and registration number, or state that the review was not registered. | NA |
| 24b | Indicate where the review protocol can be accessed, or state that a protocol was not prepared. | NA | |
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | NA | |
| Support | 25 | Describe sources of financial or non-financial support for the review and the role of the funders or sponsors in the review. | No financial support to report |
| Competing interests | 26 | Declare any competing interests of review authors. | Page 25 |
| Availability of data, code and other materials | 27 | Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; any other materials used in the review. | All data available |
References
- Prakash, H.; Chakrabarti, A. Epidemiology of Mucormycosis in India. Microorganisms 2021, 93, 523. [Google Scholar] [CrossRef] [PubMed]
- Fathima, A.S.; Mounika, V.L.; Kumar, V.U.; Gupta, A.K.; Garapati, P.; Ravichandiran; Dhingra, S.; Murtia, K. Mucormycosis: A triple burden in patients with diabetes during COVID-19 Pandemic. Health Sci. Rev. 2021, 1, 100005. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Patel, K.; Patel, K.; Shah, K.; Chakrabarti, A. Therapeutic drug monitoring of posaconazole delayed release tablet while managing COVID-19-associated mucormycosis in a real-life setting. Mycoses 2021, 65, 312–316. [Google Scholar] [CrossRef]
- Joshi, S.; Telang, R.; Tambe, M.; Havaldar, R.; Sane, M.; Shaikh, A.; Roy, C.; Yathati, K.; Sonawale, S.; Borkar, R.; et al. Outbreak of Mucormycosis in Coronavirus Disease Patients, Pune, India. Emerg. Infect. Dis. 2022, 28, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Dogra, S.; Arora, A.; Aggarwal, A.; Passi, G.; Sharma, A.; Singh, G.; Barnwal, R.P. Mucormycosis Amid COVID-19 Crisis: Pathogenesis, Diagnosis, and Novel Treatment Strategies to Combat the Spread. Front. Microbiol. 2022, 12, 794176. [Google Scholar] [CrossRef] [PubMed]
- Cornely, O.A.; Alastruey-Izquierdo, A.; Arenz, D.; Chen, S.C.A.; Dannaoui, E.; Hochhegger, B.; Hoenigl, M.; Jensen, H.E.; Lagrou, K.; Lewis, R.E.; et al. Global guideline for the diagnosis and management of mucormycosis: An initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect. Dis. 2019, 19, e405–e421. [Google Scholar] [CrossRef]
- Hoenigl, M.; Seidel, D.; Carvalho, A.; Rudramurthy, S.M.; Arastehfar, A.; Gangneux, J.-P.; Nasir, N.; Bonifaz, A.; Araiza, J.; Klimko, N.; et al. The emergence of COVID-19 associated mucormycosis: A review of cases from 18 countries. Lancet Microbe 2022, 3, e543–e552. [Google Scholar] [CrossRef]
- Pai, V.; Sansi, R.; Kharche, R.; Bandili, S.C.; Pai, B. Rhino-orbito-cerebral Mucormycosis: Pictorial Review. Insights Imaging 2021, 12, 167. [Google Scholar] [CrossRef]
- Ramamurthy, L.B.; Bhandari, R.; Kanakpur, S.; Thejaswini, P. Outcome of transcutaneous retrobulbar injection of liposomal amphotericin B in post-COVID-19 rhino-orbito-cerebral mucormycosis: Our experience. Indian J. Ophthalmol. 2022, 70, 1019. [Google Scholar] [CrossRef]
- Bhadania, S.; Bhalodiya, N.; Sethi, Y.; Kaka, N.; Mishra, S.; Patel, N.; Wasim, A.U.; Joshi, S.S.; Shah, K. Hyperferritinemia and the Extent of Mucormycosis in COVID-19 Patients. Cureus 2021, 13, 20569. [Google Scholar] [CrossRef]
- Murthy, R.; Gote, Y.S.; Bagchi, A. Localized surgical debridement for the management of orbital mucormycosis. Indian J. Ophthalmol. 2022, 70, 649–652. [Google Scholar] [CrossRef] [PubMed]
- Shenoy, V.; Bajpai, S.; Kasargod, S.K. Intraoperative Scoring Assessment as a Prognostic Tool in Covid-19 Associated Mucormycosis: A Short-Term Observational Study. Indian J. Otolaryngol. Head Neck Surg. 2022, 74, 3521–3525. [Google Scholar] [CrossRef] [PubMed]
- Popli, H.; Gupta, A.; Singh, V.; Agarwal, V.; Akilan, R.; Kumar, A. Are Low Serum Vitamin D Levels a Risk Factor for Advent of COVID-19 Associated Rhinocerebral Mucormycosis: A Preliminary Case Control Study. Indian J. Otolaryngol. Head Neck Surg. 2022, 74, 3529–3533. [Google Scholar] [CrossRef]
- Bhat, V.K.; Bongale, K.R.; Basti, S.P.; Gadag, R.P.; Kizhakkilottu, N.; Sebastian, E.; Gopalegowda, M.K.; Thammaiah, P. Risk factors for palatal and orbital involvement in mucormycosis epidemic-Report of a center in India. Am. J. Otolaryngol. 2021, 43, 103371. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.; Arora, R.; Shah, S.; Chhabra, M.; Kumar, J.; Khurana, N.; Gupta, S.; Khanam, S.; Kumar, S.; Singh, S.; et al. Clinico-Radiological-Pathological Correlation of Visual Loss in COVID-Associated Rhino-Orbito-Cerebral Mucormycosis. Ophthalmic. Plast Reconstr. Surg. 2021, 38, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, D.; Ahirwal, R.; Dubey, S.; Gurjar, P.; Pandey, A.; Beena, S.; Koneru, G. COVID Induced Functional Exhaustion and Persistently Reduced Lymphocytes as Vital Contributing Factors for Post-COVID Rhino-orbital and Cerebral Mucormycosis in Patients with Diabetes: Report from the Indian Sub-continent. Head Neck Pathol. 2021, 16, 645–650. [Google Scholar] [CrossRef]
- Hooli, S.A.; Gadre, V.N.; Bage, S.; Gilvarkar, M.D. The aftermath of COVID-19 pandemic: Rhino-orbital mucormycosis. Indian J. Anaesth. 2021, 65, 548–553. [Google Scholar] [CrossRef] [PubMed]
- Mulakaluri, A.; Subramanian, S.; Rao, P.S.; Lengade, P. The perioperative anaesthetic management and outcomes of COVID-19 associated mucormycosis patients. Indian J. Anaesth. 2022, 66, 379–383. [Google Scholar] [CrossRef]
- Sajjan, A.; Nimbal, A.V.; Shahapur, R.; Bagoji, I.B.; Chiniwar, V.A.; Chillalashetti, S.K. Post-Covid-19 Rhino-Cerebral Mucormycosis: An Observational Study During the Second Wave. Maedica 2022, 171, 103–106. [Google Scholar] [CrossRef]
- Lakshmi, I.S.; Kumari, B.S.; Jyothi, C.; Devojee, M.; Malini, K.P.; Sunethri, P.; Somalwar, S.B.; Kavitha, T. Histopathological Study of Mucormycosis in Post COVID-19 Patients and Factors Affecting it in a Tertiary Care Hospital. Int. J. Surg. Pathol. 2022. [Google Scholar] [CrossRef]
- Chandwani, N.; Dabhekar, S.; Selvi, K.; Mohamed, R.N.; Abullais, S.S.; Moothedath, M.; Jadhav, G.; Chandwani, J.; Karobari, M.I.; Pawar, A.M. Oral Tissue Involvement and Probable Factors in Post-COVID-19 Mucormycosis Patients: A Cross-Sectional Study. Healthcare 2022, 10, 912. [Google Scholar] [CrossRef] [PubMed]
- Khichar, S.; Samantaray, S.; Kumar, D.; Mobarsa, V.; Jain, V.; Sharma, V.; Soni, K.; Choudhary, B.; Goyal, A.; Meena, D.S.; et al. New-onset hyperglycaemia and prolonged systemic corticosteroids therapy in mild COVID-19 patients as major risk factors for invasive mucormycosis: A preliminary study. Curr. Med. Mycol. 2021, 73, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Misra, S.; Rastogi, S.; Malviya, D.; Gupta, R.; Yadav, S.K.; Alam, S. Perioperative anesthetic concerns in postcovid mucormycosis patients posted for surgical intervention: An observational Study. Saudi J. Anaesth. 2022, 16, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, N.; Sivanandam, S. Histomorphological features of mucormycosis with rise and fall of COVID-19 pandemic. Pathol. Res. Pract. 2022, 236. [Google Scholar] [CrossRef] [PubMed]
- Pal, P.; Singh, B.; Singla, S.; Kaur, R. Mucormycosis in COVID-19 pandemic and its neurovascular spread. Eur. Arch. Otorhinolaryngol. 2021, 279, 2965–2972. [Google Scholar] [CrossRef] [PubMed]
- Dubey, S.; Mukherjee, D.; Sarkar, P.; Mukhopadhyay, P.; Barman, D.; Bandopadhyay, M.; Pandit, A.; Sengupta, A.; Das, S.; Ghosh, S.; et al. COVID-19 associated rhino-orbital-cerebral mucormycosis: An observational study from Eastern India, with special emphasis on neurological spectrum. Diabetes Metab. Syndr. 2021, 15, 102267. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.K.; Kapre, M.; Gupta, H.; Vaidya, G.K.; Jani, S.; Meshram, S.; Singh, S.; Kapre, V.; Ravi, R.; Tambe, V.; et al. Risk Based Decision Algorithms for Management of COVID-19 Associated Rhino-orbital Mucormycosis. Indian J. Otolaryngol. Head Neck Surg. 2021, 74, 3447–3454. [Google Scholar] [CrossRef]
- Kumar, A.; Verma, M.; Hakim, A.; Sharma, S.; Meena, R.; Bhansali, S. Epidemiology of Mucormycosis Cases During the Second Wave of COVID-19 in a Tertiary Care Institute in Western Rajasthan, India. Cureus 2022, 14, e22973. [Google Scholar] [CrossRef]
- Ahmed, W.M.S.; Elsherbini, A.M.; Elsherbiny, N.M.; El-Sherbiny, M.; Ramzy, N.I.; Arafa, F.A. Maxillary Mucormycosis Osteomyelitis in Post COVID-19 Patients: A Series of Fourteen Cases. Diagnostics 2021, 11, 2050. [Google Scholar] [CrossRef]
- Murthy, R.; Bagchi, A.; Gote, Y.S. Role of medial orbital wall decompression in COVID-19-associated rhino-orbital mucormycosis management. Indian J. Ophthalmol. 2021, 69, 3795–3796. [Google Scholar] [CrossRef]
- Walia, S.; Bhaisare, V.; Rawat, P.; Kori, N.; Sharma, M.; Gupta, N.; Urdhwareshwar, S.; Thakur, S.; Arya, N. COVID-19-associated mucormycosis: Preliminary report from a tertiary eye care centre. Indian J. Ophthalmol. 2021, 69, 3685–3689. [Google Scholar] [CrossRef] [PubMed]
- Vare, A.A.; Yellambkar, S.; Farheen, A.; Nandedkar, V.; Bhombe, S.S.; Shah, R. Incidence, cumulative mortality and factors affecting the outcome of COVID-19-associated mucormycosis from Western India. Indian J. Ophthalmol. 2021, 69, 3678–3683. [Google Scholar] [CrossRef] [PubMed]
- Fouad, Y.A.; Bakre, H.M.; Nassar, M.A.; Gad, M.O.A.; Shaat, A.A.K. Characteristics and Outcomes of a Series of COVID-Associated Mucormycosis Patients in Two Different Settings in Egypt Through the Third Pandemic Wave. Clin. Ophthalmol. 2021, 15, 4795–4800. [Google Scholar] [CrossRef]
- Soni, K.; Das, A.; Sharma, V.; Goyal, A.; Choudhury, B.; Chugh, A.; Kumar, D.; Yadav, T.; Jain, V.; Agarwal, A.; et al. Sanje Surgical & medical management of ROCM (Rhino-orbito-cerebral mucormycosis) epidemic in COVID-19 era and its outcomes—A tertiary care center experience. J. Mycol. Med. 2021, 32, 101238. [Google Scholar] [CrossRef] [PubMed]
- Metwally, M.I.; Mobashir, M.; Sweed, A.H.; Mahmoud, S.M.; Hassan, A.G.; ElKashishy, K.; Eesa, M.; Elnashar, I.; Elmalt, A.; Elsayed, A.I.; et al. Post COVID-19 Head and Neck Mucormycosis: MR Imaging Spectrum and Staging. Acad. Radiol. 2021, 29, 674–684. [Google Scholar] [CrossRef]
- Arora, U.; Priyadarshi, M.; Katiyar, V.; Soneja, M.; Garg, P.; Gupta, I.; Bharadiya, V.; Berry, P.; Ghosh, T.; Patel, L.; et al. Risk factors for Coronavirus disease-associated mucormycosis. J. Infect. 2021, 84, 383–390. [Google Scholar] [CrossRef]
- Jindal, G.; Sethi, A.; Bhargarva, K.; Sethi, S.; Mittal, A.; Singh, U.; Singh, S.; Shrivastava, A. Imaging findings in invasive rhino-orbito-cerebral mucormycosis in post-COVID-19 patients. Bayl. Univ. Med. Cent. Proc. 2021, 351, 32–34. [Google Scholar] [CrossRef]
- Syed-Abdul, S.; Babu, A.S.; Bellamkonda, R.S.; Itumalla, R.; Acharyulu, G.; Krishnamurthy, S.; Ramana, Y.V.S.; Mogilicharla, N.; Malwade, S.; Li, Y.-C. Using artificial intelligence-based models to predict the risk of mucormycosis among COVID-19 survivors: An experience from a public hospital in India. J. Infect. 2021, 84, 351–354. [Google Scholar] [CrossRef]
- Pruthi, H.; Muthu, V.; Bhujade, H.; Sharma, A.; Baloji, A.; Ratnakara, R.G.; Bal, A.; Singh, H.; Sandhu, M.S.; Negi, S.; et al. Pulmonary Artery Pseudoaneurysm in COVID-19-Associated Pulmonary Mucormycosis: Case Series and Systematic Review of the Literature. Mycopathologia 2021, 187, 31–37. [Google Scholar] [CrossRef]
- Bansal, S.B.; Rana, A.; Babras, M.; Yadav, D.; Jha, P.; Jain, M.; Sethi, S.K. Risk factors and outcomes of COVID associated mucormycosis in kidney transplant recipients. Transpl. Infect. Dis. 2021, 24, e13777. [Google Scholar] [CrossRef]
- Dulski, T.M.; DeLong, M.; Garner, K.; Patil, N.; Cima, M.J.; Rothfeldt, L.; Gulley, T.; Porter, A.; Vyas, K.S.; Liverett, H.K.; et al. Notes from the Field: COVID-19-Associated Mucormycosis—Arkansas, July–September 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1750–1751. [Google Scholar] [CrossRef] [PubMed]
- Meshram, H.S.; Kute, V.B.; Yadav, D.K.; Godara, S.; Dalal, S.; Guleria, S.; Bhalla, A.K.; Pathak, V.; Anandh, U.; Bansal, S.; et al. Impact of COVID-19-associated Mucormycosis in Kidney Transplant Recipients: A Multicenter Cohort Study. Transplant. Direct. 2021, 8, e1255. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, S.K.; Kaur, U.; Talda, D.; Pandey, A.; Jaiswal, S.; Kanakan, A.; Singh, A.; Chakrabarti, S.S. Case Report: Rhino-orbital Mucormycosis Related to COVID-19: A Case Series Exploring Risk Factors. Am. J. Trop. Med. Hyg. 2022, 106, 566–570. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, R.; Pujari, S.S.; Gupta, D.; Ojha, P.; Dhamne, M.; Bolegave, V.; Dhonde, P.; Soni, A.; Adwani, S.; Diwan, A.; et al. Cerebrovascular Involvement in Mucormycosis in COVID-19 Pandemic. J. Stroke Cerebrovasc. Dis. 2021, 31, 106231. [Google Scholar] [CrossRef]
- Choksi, T.; Agrawal, A.; Date, P.; Rathod, D.; Gharat, A.; Ingole, A.; Chaudhari, B.; Pawar, N. Cumulative Mortality and Factors Associated with Outcomes of Mucormycosis after COVID-19 at a Multispecialty Tertiary Care Center in India. JAMA Ophthalmol. 2022, 140, 66–72. [Google Scholar] [CrossRef]
- Kumar, S.; Choudhary, R.; Pandey, V.P. “MuCovid-21” study: Mucormycosis at an Indian tertiary care centre during the COVID-19 pandemic. J. R. Coll. Physicians Edinb. 2021, 51, 352–358. [Google Scholar] [CrossRef]
- Mehta, R.; Nagarkar, N.M.; Ksbs, K.S.; Ty, S.S.; Arora, R.D.; Aggarwal, A. Facial Nerve Palsy in COVID-19-Associated Mucormycosis Patients: A Case Series. Cureus 2021, 13, e19208. [Google Scholar] [CrossRef]
- Panwar, P.; Gupta, A.; Kumar, A.; Gupta, B.; Navriya, S.C. Mucormycosis in COVID Diabetic Patients: A Horrifying Triad! Indian J. Crit. Care Med. 2021, 25, 1314–1317. [Google Scholar] [CrossRef]
- Patel, D.D.; Adke, S.; Badhe, P.V.; Lamture, S.; Marfatia, H.; Mhatre, P. COVID-19 associated Rhino-Orbito-Cerebral Mucormycosis: Imaging spectrum and Clinico-radiological correlation—A single Centre experience. Clin. Imaging 2021, 82, 172–178. [Google Scholar] [CrossRef]
- Vaid, N.; Mishra, P.; Gokhale, N.; Vaid, S.; Vaze, V.; Kothadiya, A.; Deka, T.; Agarwal, R. A Proposed Grading System and Experience of COVID-19 Associated Rhino Orbito Cerebral Mucormycosis from an Indian Tertiary Care Cente. Indian J. Otolaryngol. Head Neck Surg. 2021, 74, 3505–3512. [Google Scholar] [CrossRef]
- Goddanti, N.; Reddy, Y.M.; Kumar, M.K.; Rajesh, M.; Reddy, L.S. Role of COVID 19 Inflammatory Markers in Rhino-Orbito-Cerebral Mucormycosis: A Case Study in Predisposed Patients at a Designated Nodal Centre. Indian J. Otolaryngol. Head Neck Surg. 2021, 74, 3498–3504. [Google Scholar] [CrossRef] [PubMed]
- Yadav, T.; Tiwari, S.; Gupta, A.; Garg, P.K.; Khera, P.S.; Rajagopal, R.; Goyal, A.; Soni, K.; Chugh, A.; Jain, V.; et al. Magnetic Resonance Imaging in Coronavirus Disease—2019 Associated Rhino-Orbital-Cerebral Mucormycosis (CA-ROCM)—Imaging Analysis of 50 Consecutive Patients. Curr. Probl. Diagn. Radiol. 2022, 51, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Meshram, H.S.; Kute, V.B.; Chauhan, S.; Dave, R.; Patel, H.; Banerjee, S.; Desai, S.; Kumar, D.; Navadiya, V.; Mishra, V. Mucormycosis as SARS-CoV2 sequelae in kidney transplant recipients: A single-center experience from India. Int. Urol. Nephrol. 2021, 54, 1693–1703. [Google Scholar] [CrossRef] [PubMed]
- Zirpe, K.; Pote, P.; Deshmukh, A.; Gurav, S.K.; Tiwari, A.M.; Suryawanshi, P. A Retrospective Analysis of Risk Factors of COVID-19 Associated Mucormycosis and Mortality Predictors: A Single-Center Study. Cureus 2021, 13, e18718. [Google Scholar] [CrossRef] [PubMed]
- Alloush, T.K.; Mansour, O.; Alloush, A.T.; Roushd, T.; Hamid, E.; El-Shamy, M.; Shokri, H.M. Rhino-orbito-cerebral mucormycosis during the COVID-19 third wave in 2021: An Egyptian preliminary report from a single tertiary hospital. Neurol. Sci. 2021, 43, 799–809. [Google Scholar] [CrossRef]
- Pal, P.; Chatterjee, N.; Ghosh, S.; Ray, B.K.; Mukhopadhyay, P.; Bhunia, K.; Srivastava, S.R.; Adhikari, S.; Barman, D.; Banerjee, B.; et al. COVID Associated Mucormycosis: A Study on the Spectrum of Clinical, Biochemical and Radiological Findings in A Series of Ten Patients. J. Assoc. Physicians India 2021, 69, 11–12. [Google Scholar]
- Danion, F.; Letscher-Bru, V.; Guitard, J.; Sitbon, K.; Dellière, S.; Angoulvant, A.; Desoubeaux, G.; Botterel, F.; Bellanger, A.-P.; Gargala, G.; et al. Coronavirus Disease 2019-Associated Mucormycosis in France: A Rare but Deadly Complication. Open Forum Infect. Dis. 2021, 9, ofab566. [Google Scholar] [CrossRef]
- Nehara, H.R.; Kumawat, S.; Gupta, J.; Gupta, G.; Sirohi, P.; Ih, S.; Gupta, B. Coronavirus Disease, Diabetes and Glucocorticoid a Terrible Trio for Invasive Mucormycosis: An Observational Study from Northwest Rajasthan. J. Assoc. Physicians India 2022, 69, 11–12. [Google Scholar]
- Pandiar, D.; Ramani, P.; Krishnan, R.P.; Dinesh, Y. Histopathological analysis of soft tissue changes in gingival biopsied specimen from patients with underlying corona virus disease associated mucormycosis (CAM). Med. Oral Patol. Oral Cir. Bucal. 2022, 27, e216–e222. [Google Scholar] [CrossRef]
- Kumar, S.; Acharya, S.; Jain, S.; Shukla, S.; Talwar, D.; Shah, D.; Hulkoti, V.; Parveen, S.; Patel, M.; Patel, S. Role of Zinc and Clinicopathological Factors for COVID-19-Associated Mucormycosis (CAM) in a Rural Hospital of Central India: A Case-Control Study. Cureus 2022, 14, e22528. [Google Scholar] [CrossRef]
- Bilgic, A.; Kodjikian, L.; Sudhalkar, A.; Dwivedi, S.; Vasavada, V.; Shah, A.; Dziadzko, M.; Mathis, T. Risk Factors for COVID-19 Associated Mucormycosis: The Ophthalmologist’s Perspective. J. Fungi 2022, 8, 271. [Google Scholar] [CrossRef] [PubMed]
- Guemas, E.; Cassaing, S.; Malavaud, S.; Fillaux, J.; Chauvin, P.; Lelièvre, L.; Ruiz, S.; Riu, B.; Berry, A.; Iriart, X. A Clustered Case Series of Mucorales Detection in Respiratory Samples from COVID-19 Patients in Intensive Care, France, August to September 2021. J. Fungi 2022, 8, 258. [Google Scholar] [CrossRef] [PubMed]
- Gg, S.K.; Deepalam, S.; Siddiqui, A.; Adiga, C.P.; Kumar, S.; Shivalingappa, S.S.; Acharya, U.V.; Goolahally, L.N.; Sharma, S.; Andrew, D.; et al. Coronavirus Disease 2019 (COVID-19)-Associated Rhino-Orbito-Cerebral Mucormycosis: A Multi-Institutional Retrospective Study of Imaging Patterns. World Neurosurg. 2022, 162, e131–e140. [Google Scholar] [CrossRef]
- Mani, S.; Thirunavukkarasu, A. A clinico-pathological study of COVID-19 associated rhino-orbital-cerebral mucormycosis. Indian J. Ophthalmol. 2022, 70, 1013–1018. [Google Scholar] [CrossRef] [PubMed]
- Dravid, A.; Kashiva, R.; Khan, Z.; Bande, B.; Memon, D.; Kodre, A.; Mane, M.; Pawar, V.; Patil, D.; Kalyani, S.; et al. Epidemiology, clinical presentation and management of COVID-19 associated mucormycosis: A single centre experience from Pune, Western India. Mycoses 2022, 65, 526–540. [Google Scholar] [CrossRef] [PubMed]
- Naruka, S.; Rana, N.; Singh, N.; Kishore, A.; Nagpal, K. COVID-19 associated rhino-orbital-cerebral mucormycosis-an institutional series. Ear Nose Throat J. 2022. [Google Scholar] [CrossRef] [PubMed]
- Jain, K.; Surana, A.; Choudhary, T.S.; Vaidya, S.; Nandedkar, S.; Purohit, M. Clinical and histology features as predictor of severity of mucormycosis in post-COVID-19 patients: An experience from a rural tertiary setting in Central India. SAGE Open Med. 2022, 10. [Google Scholar] [CrossRef]
- Bhanuprasad, K.; Manesh, A.; Devasagayam, E.; Varghese, L.; Cherian, L.M.; Kurien, R.; Karthik, R.; Deodhar, D.; Vanjare, H.; Peter, J.; et al. Risk factors associated with the mucormycosis epidemic during the COVID-19 pandemic. Int. J. Infect. Dis. 2021, 111, 267–270. [Google Scholar] [CrossRef]
- Desai, E.J.; Pandya, A.; Upadhya, I.; Patel, T.; Banerjee, S.; Jain, V. Epidemiology, Clinical Features and Management of Rhino Orbital Mucormycosis in Post COVID 19 Patients. Indian J. Otolaryngol. Head Neck Surg. 2021, 74, 103–107. [Google Scholar] [CrossRef]
- Nasir, N.; Farooqi, J.; Mahmood, S.F.; Jabeen, K. COVID-19 associated mucormycosis: A life-threatening complication in patients admitted with severe to critical COVID-19 from Pakistan. Clin. Microbiol. Infect. 2021, 27, 1704–1707. [Google Scholar] [CrossRef]
- Gupta, S.; Ahuja, P. Risk Factors for Procurence of Mucormycosis and its Manifestations Post Covid-19: A Single Arm Retrospective Unicentric Clinical Study. Indian J. Otolaryngol. Head Neck Surg. 2021, 74, 3131–3138. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, P.; Shaikh, Z.; Mishra, A.; Preetam, C.; Parida, P.K.; Sarkar, S.; Samal, D.K.; Nayak, A.; Chadaram, S.; Das, K.K.; et al. Predisposing factors of rhino-orbital-cerebral mucormycosis in patients with COVID 19 infection. Indian J. Otolaryngol. Head Neck Surg. 2021, 74, 3151–3157. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.; Nagarkar, N.M.; Jindal, A.; Rao, K.N.; Nidhin, S.B.; Arora, R.D.; Sharma, A.; Wankhede, A.; Satpute, S.; Chakravarty, S.; et al. Multidisciplinary Management of COVID-Associated Mucormycosis Syndemic in India. Indian J. Surg. 2021, 84, 934–942. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Shabaan, A.A.; Issa, J.; Ibrahim, S.; Amer, H.; Mansy, Y.; Kassem, I.; Kassem, A.B.; Howaldt, H.; Klugar, M.; et al. COVID-19-Associated Mucormycosis (CAM): Case-Series and Global Analysis of Mortality Risk Factors. J. Fungi 2021, 7, 837. [Google Scholar] [CrossRef]
- Guzmán-Castro, S.; Chora-Hernandez, L.D.; Trujillo-Alonso, G.; Calvo-Villalobos, I.; Sanchez-Rangel, A.; Ferrer-Alpuin, E.; Ruiz-Jimenez, M.; Corzo-Leon, D.E. COVID-19-associated mucormycosis, diabetes and steroid therapy: Experience in a single centre in Western Mexico. Mycoses 2021, 65, 65–70. [Google Scholar] [CrossRef]
- Seidel, D.; Simon, M.; Sprute, R.; Lubnow, M.; Evert, K.; Speer, C.; Seeßle, J.; Khatamzas, E.; Merle, U.; Behrens, C.; et al. Results from a national survey on COVID-19-associated mucormycosis in Germany: 13 patients from six tertiary hospitals. Mycoses 2021, 65, 103–109. [Google Scholar] [CrossRef]
- Gupta, R.; Kesavadev, J.; Krishnan, G.; Agarwal, S.; Saboo, B.; Shah, M.; Mittal, A.; Durani, S.; Luthra, A.; Singhal, A.; et al. COVID-19 associated mucormycosis: A Descriptive Multisite Study from India. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102322. [Google Scholar] [CrossRef]
- Alfishawy, M.; Elbendary, A.; Younes, A.; Negm, A.; Hassan, W.S.; Osman, S.H.; Nassar, M.; Elanany, M.G. Diabetes mellitus and Coronavirus Disease (Covid-19) Associated Mucormycosis (CAM): A wake-up call from Egypt. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102195. [Google Scholar] [CrossRef]
- Dave, T.V.; Nair, A.G.; Hegde, R.; Vithalani, N.; Desai, S.; Adulkar, N.; Kamal, S.; Mittal, R.; Bradoo, R.A. Clinical Presentations, Management and Outcomes of Rhino-Orbital-Cerebral Mucormycosis (ROCM) Following COVID-19: A Multi-Centric Study. Ophthalmic Plast. Reconstr. Surg. 2021, 37, 488–495. [Google Scholar] [CrossRef]
- Selarka, L.; Sharma, S.; Saini, D.; Sharma, S.; Batra, A.; Waghmare, V.T.; Dileep, P.; Patel, S.; Shah, M.; Parikh, T.; et al. Mucormycosis and COVID-19: An epidemic within a pandemic in India. Mycoses 2021, 64, 1253–1260. [Google Scholar] [CrossRef]
- Fazeli, M.A.; Rezaei, L.; Javadirad, E.; Iranfar, K.; Khosravi, A.; Saman, J.A.; Poursabbagh, P.; Ghadami, M.R.; Parandin, M.M.; Dehghani, A.; et al. Increased incidence of rhino-orbital mucormycosis in an educational therapeutic hospital during the COVID-19 pandemic in western Iran: An observational study. Mycoses 2021, 64, 1366–1377. [Google Scholar] [CrossRef] [PubMed]
- Mishra, Y.; Prashar, M.; Sharma, D.; Akash; Kumar, V.P.; Tilak, T. Diabetes, COVID 19 and mucormycosis: Clinical spectrum and outcome in a tertiary care medical center in Western India. Diabetes Metab. Syndr. 2021, 15, 102196. [Google Scholar] [CrossRef] [PubMed]
- Honavar, S.; Sen, M.; Sengupta, S.; Rao, R.; Kim, U.; Sharma, M.; Sachdev, M.; Grover, A.; Surve, A.; Budharapu, A.; et al. Epidemiology, clinical profile, management, and outcome of COVID-19-associated rhino-orbital-cerebral mucormycosis in 2826 patients in India—Collaborative OPAI-IJO Study on Mucormycosis in COVID-19 (COSMIC), Report 1. Indian J. Ophthalmol. 2021, 69, 1670–1692. [Google Scholar] [CrossRef] [PubMed]
- Pakdel, F.; Ahmadikia, K.; Salehi, M.; Tabari, A.; Jafari, R.; Mehrparvar, G.; Rezaie, Y.; Rajaeih, S.; Alijani, N.; Barac, A.; et al. Mucormycosis in patients with COVID-19: A cross-sectional descriptive multicentre study from Iran. Mycoses 2021, 64, 1238–1252. [Google Scholar] [CrossRef] [PubMed]
- Reddy, Y.M.; Parida, S.; Reddy, S.B.; Yeduguri, S.; Pidaparthi, L.; Jaiswal, S.K.; Sadhvani, B.; Murthy, J.M.K. Decoding “guitar pick sign” in COVID-19-associated mucormycosis: A case series. Indian J. Ophthalmol. 2022, 70, 1425–1427. [Google Scholar] [CrossRef] [PubMed]
- Arora, R.; Goel, R.; Khanam, S.; Kumar, S.; Shah, S.; Singh, S.; Chhabra, M.; Meher, R.; Khurana, N.; Sagar, T.; et al. Rhino-Orbito-Cerebral-Mucormycosis During the COVID-19 Second Wave in 2021—A Preliminary Report from a Single Hospital. Clin. Ophthalmol. 2021, 15, 3505–3514. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.P.; Gupta, S.; Shah, C.K.; Sreevidya, S.R. Clinical Study of Surge of Mucormycosis in COVID-19 Pandemic: A Tertiary Care Center Study. Indian J. Otolaryngol. Head Neck Surg. 2021, 74, 3455–3462. [Google Scholar] [CrossRef]
- Gautam, M.; Soni, M.; Bhaisare, V.; Rawat, P.; Walia, S.; Kori, N. Complete and incomplete lower motor neuron facial palsy in post-COVID-19 mucormycosis. Indian J. Ophthalmol. 2022, 70, 1365–1370. [Google Scholar] [CrossRef]
- Mehta, R.M.; Bansal, S.; Kalpakkam, H. Critical COVID-19-associated pulmonary mucormycosis: The underreported life-threatening spectrum of the mucormycosis epidemic. Lung India 2022, 39, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Reddy, Y.M.; Yeduguri, S.; Reddy, N.V.S.; Parida, S.; Kamatham, S.N.; Pidaparthi, L.; Jaiswal, S.K.; Sadhvani, B.; Tourani, V.; Kumar, S.; et al. Pathogenetic factors fanning the flames of COVID-19 to cause rhino-orbito-cerebral mucormycosis: An observational study. J. Med. Mycol. 2022, 32, 101252. [Google Scholar] [CrossRef]
- Singh, S.P.; Rana, J.; Singh, V.K.; Singh, R.; Sachan, R.; Singh, S.; Jain, S. Rhino-orbital mucormycosis: Our experiences with clinical features and management in a tertiary care center. Rom. J. Ophthalmol. 2021, 65, 339–353. [Google Scholar] [CrossRef] [PubMed]
- Hada, M.; Gupta, P.; Bagarhatta, M.; Tripathy, K.; Harsh, A.; Khilnani, K.; Mendiratta, K.; Agarwal, S.; Chouhan, J.K.; Bhandari, S. Orbital magnetic resonance imaging profile and clinicoradiological correlation in COVID-19-associated rhino-orbital-cerebral mucormycosis: A single-center study of 270 patients from North India. Indian J. Ophthalmol. 2022, 70, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Kumar, H.M.; Sharma, P.; Rudramurthy, S.M.; Sehgal, I.S.; Prasad, K.T.; Pannu, A.K.; Das, R.; Panda, N.K.; Sharma, N.; Chakrabarti, A.; et al. Serum iron indices in COVID-19-associated mucormycosis: A case-control study. Mycoses 2021, 65, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, S.; Bhargava, S.; Samdhani, S.; Singh, S.N.; Sharma, B.B.; Agarwal, S.; Sharma, M.P.; Sharma, S.; Sharma, V.; Kakkar, S.; et al. COVID-19, Diabetes and Steroids: The Demonic Trident for Mucormycosis. Indian J. Otolaryngol. Head Neck Surg. 2021, 74, 3469–3472. [Google Scholar] [CrossRef]
- Chouhan, M.; Solanki, B.; Shakrawal, N. Rhino-orbital-cerebral mucormycosis: Fungal epidemic in a viral pandemic. J. Laryngol. Otol. 2021, 135, 981–986. [Google Scholar] [CrossRef]
- Singh, Y.; Ganesh, V.; Kumar, S.; Patel, N.; Aggarwala, R.; Soni, K.D.; Trikha, A. Coronavirus Disease-Associated Mucormycosis from a Tertiary Care Hospital in India: A Case Series. Cureus 2021, 13, e16152. [Google Scholar] [CrossRef]
- Desai, S.M.; Gujarathi-Saraf, A.; Agarwal, E.A. Imaging findings using a combined MRI/CT protocol to identify the “entire iceberg” in post-COVID-19 mucormycosis presenting clinically as only “the tip”. Clin. Radiol. 2021, 76, 784.e27–784.e33. [Google Scholar] [CrossRef]
- Kumari, A.; Rao, N.P.; Patnaik, U.; Malik, V.; Tevatia, M.S.; Thakur, S.; Jaydevan, J.; Saxena, P. Management outcomes of mucormycosis in COVID-19 patients: A preliminary report from a tertiary care hospital. Med. J. Armed Forces India 2021, 77 (Suppl. 2), S289–S295. [Google Scholar] [CrossRef]
- Mitra, S.; Janweja, M.; Sengupta, A. Post-COVID-19 rhino-orbito-cerebral mucormycosis: A new addition to challenges in pandemic control. Eur. Arch. Oto-Rhino-Laryngol. 2021, 279, 2417–2422. [Google Scholar] [CrossRef]
- Ramaswami, A.; Sahu, A.K.; Kumar, A.; Suresh, S.; Nair, A.; Gupta, D.; Chouhan, R.; Bhat, R.; Mathew, R.; Majeed, J.A.; et al. COVID-19-associated mucormycosis presenting to the Emergency Department-an observational study of 70 patients. Qjm Int. J. Med. 2021, 114, 464–470. [Google Scholar] [CrossRef]
- Joshi, A.R.; Muthe, M.M.; Patankar, S.H.; Athawale, A.; Achhapalia, Y. CT and MRI Findings of Invasive Mucormycosis in the Setting of COVID-19: Experience from a Single Center in India. Am. J. Roentgenol. 2021, 217, 1431–1432. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Agarwal, R.; Rudramurthy, S.M.; Shevkani, M.; Xess, I.; Sharma, R.; Savio, J.; Sethuraman, N.; Madan, S.; Shastri, P.; et al. Multicenter Epidemiologic Study of Coronavirus Disease-Associated Mucormycosis, India. Emerg. Infect. Dis. 2021, 27, 2349–2359. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Grover, M.; Bhargava, S.; Samdani, S.; Kataria, T. Post coronavirus disease mucormycosis: A deadly addition to the pandemic spectrum. J. Laryngol. Otol. 2021, 135, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Kant, R.; Totaganti, M.; Mohan, B.; Bairwa, M.; Panda, P.K.; Tyagi, A.; Prasad, A.; Bahurupi, Y. Clinical Characteristics of 100 Patients With COVID-19-Associated Mucormycosis From a Tertiary Care Center in North India. Cureus 2022, 14, e25652. [Google Scholar] [CrossRef] [PubMed]
- Eker, C.; Tarkan, O.; Surmelioglu, O.; Dagkiran, M.; Tanrisever, I.; Karakaya, S.P.Y.; Ulas, B.; Onan, E.; Uguz, A.H.; Ozdemir, S. Alternating pattern of rhino-orbital-cerebral mucormycosis with COVID-19 in diabetic patients. Eur. Arch. Otorhinolaryngol. 2022. [Google Scholar] [CrossRef]
- Pandit, A.K.; Tangri, P.; Misra, S.; Srivastava, M.V.P.; Bhatnagar, S.; Thakar, A.; Sikka, K.; Panda, S.; Vishnu, V.Y.; Singh, R.K.; et al. Mucormycosis in COVID-19 Patients: A Case-Control Study. Microorganisms 2022, 10, 1209. [Google Scholar] [CrossRef]
- Youssif, S.F.; Abdelrady, M.M.; Thabet, A.A.; Abdelhamed, M.A.; Gad, M.O.A.; Abu-Elfatth, A.M.; Saied, G.M.; Goda, I.; Algammal, A.M.; Batiha, G.E.-S.; et al. COVID-19 associated mucormycosis in Assiut University Hospitals: A multidisciplinary dilemma. Sci. Rep. 2022, 12, 10494. [Google Scholar] [CrossRef]
- Sekaran, A.; Patil, N.; Sabhapandit, S.; Sistla, S.K.; Reddy, D.N. Rhino-orbito-cerebral mucormycosis: An epidemic in a pandemic. IJID Reg. 2021, 2, 99–106. [Google Scholar] [CrossRef]
- Shabana, R.R.; Eldesouky, M.A.; Elbedewy, H.A. Exenterate or Not: A Simple Proposed Management Algorithm for Mucormycosis During the Era of COVID-19 in a Tertiary Eye Care Center in Egypt. Clin. Ophthalmol. 2022, 16, 1933–1940. [Google Scholar] [CrossRef]
- Patel, A.K.; Bakshi, H.; Shah, K.; Patel, S.; Patel, T.; Patel, K.; Patel, K.K. Risk factors for COVID-19 associated mucormycosis in India: A case control study. Med. Mycol. 2022, 60, myac044. [Google Scholar] [CrossRef]
- Martins, H.D.; Pares, A.R.; Martínez, A.T.; Guevara, R.A.P.; Inaoka, S.D.; Costa, D.F.; Leal, C.B.; Soares, C.D.; da Paz, A.R.; Perez, D.E.d.C.; et al. A case series of mucormycosis after covid infection in two hospitals. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, e757–e759. [Google Scholar] [CrossRef] [PubMed]
- Iqtadar, S.; Hashmat, M.; Chaudhry, M.N.A.; Mumtaz, S.U.; Abaidullah, S.; Pascual-Figal, D.A.; Khan, A. Unnecessary Use of Corticosteroids for managing early mild symptoms of COVID-19 may lead to Rhino-ortibal-cerebral mucormycosis in Patients with Diabetes—A case series from Lahore, Pakistan. Ther. Adv. Infect. Dis. 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Al Balushi, A.; Al Ajmi, A.; Al Sinani, Q.; Menon, V.; Al Berieki, Z.; Al Shezawi, A.; Al Azri, S.; Al Rashdi, A.; Al Jardani, A.; Al Baluki, T.; et al. COVID-19-Associated Mucormycosis: An Opportunistic Fungal Infection. A Case Series and Review. Int. J. Infect. Dis. 2022, 121, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Soman, R.; Chakraborty, S.; Joe, G. Posaconazole or isavuconazole as sole or predominant antifungal therapy for COVID-19-associated mucormycosis. A retrospective observational case series. Int. J. Infect. Dis. 2022, 120, 177–178. [Google Scholar] [CrossRef] [PubMed]
- Mohsen, A.Y.; Mohammad, J.G.; Al-Janabi, M.H. Mucormycosis (black fungus) infection and misuse of corticosteroids in COVID 19 patients in Syria. Ann. Med. Surg. 2022, 75, 103463. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, O.F.; Al-Neaimy, S.; Kakamad, F.H.; Ali, R.K.; Mikael, T.M.; Hamasaeed, A.G.; Mohammed, S.H.; Salih, R.Q.; Salh, A.M.; Hamasaeed, M.G. COVID-19 associated with pulmonary mucormycosis: A case series. Ann. Med. Surg. 2022, 76, 103434. [Google Scholar] [CrossRef]
- Rodriguez-Morales, A.J.; Mamani-García, C.S.; Nuñez-Lupaca, J.N.; León-Figueroa, D.A.; Olarte-Durand, M.; Yrene-Cubas, R.A.; Ticona, D.M.; Abanto-Urbano, S. COVID-19 and mucormycosis in Latin America—An emerging concern. Travel Med. Infect. Dis. 2021, 44, 102156. [Google Scholar] [CrossRef]
- Casalini, G.; Giacomelli, A.; Ridolfo, A.; Gervasoni, C.; Antinori, S. Invasive Fungal Infections Complicating COVID-19: A Narrative Review. J. Fungi 2021, 7, 921. [Google Scholar] [CrossRef]
- Gangneux, J.-P.; Dannaoui, E.; Fekkar, A.; Luyt, C.-E.; Botterel, F.; De Prost, N.; Tadié, J.-M.; Reizine, F.; Houzé, S.; Timsit, J.-F.; et al. Fungal infections in mechanically ventilated patients with COVID-19 during the first wave: The French multicentre MYCOVID study. Lancet Respir. Med. 2021, 10, 180–190. [Google Scholar] [CrossRef]
- Scharmann, U.; Herbstreit, F.; Steckel, N.K.; Dedy, J.; Buer, J.; Rath, P.-M.; Verhasselt, H.L. Prevalence of COVID-19 Associated Mucormycosis in a German Tertiary Care Hospital. J. Fungi 2022, 8, 307. [Google Scholar] [CrossRef]
- Bhimraj, A.; Morgan, R.L.; Shumaker, A.H.; Baden, L.; Cheng, V.C.C.; Edwards, K.M.; Gallagher, J.C.; Gandhi, R.T.; Muller, W.J.; Nakamura, M.M.; et al. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19. Clin. Infect. Dis. 2022. [Google Scholar] [CrossRef]
- Biswal, M.; Gupta, P.; Kanaujia, R.; Kaur, K.; Kaur, H.; Vyas, A.; Hallur, V.; Behera, B.; Padaki, P.; Savio, J.; et al. Evaluation of hospital environment for presence of Mucorales during COVID-19-associated mucormycosis outbreak in India—A multi-centre study. J. Hosp. Infect. 2022, 122, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Leal-Buitrago, A.; Mondragon-Ángulo, D.; Cely-Aldana, N.A.; Ortega-Sierra, M.G.; Bolaño-Romero, M.P. Letter: Spectrum of hospitalized NeuroCOVID diagnoses from a tertiary care neurology centre in Eastern India. J. Clin. Neurosci. 2022, 96, 227–228. [Google Scholar] [CrossRef] [PubMed]
- Krishna, V.; Bansal, N.; Morjaria, J.; Kaul, S. COVID-19-Associated Pulmonary Mucormycosis. J. Fungi 2022, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- Samson, R.; Dharne, M. COVID-19 associated mucormycosis: Evolving technologies for early and rapid diagnosis. 3 Biotech. 2021, 12, 6. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Malhotra, H.S.; Saxena, P.; Singh, R.; Shukla, D.; Hasan, M.S.; Verma, V.; Banerjee, G.; Puri, B.; Dandu, H. Utility of itraconazole and terbinafine in mucormycosis: A proof-of-concept analysis. J. Investig. Med. 2022, 70, 914–918. [Google Scholar] [CrossRef]
- Dimopoulos, G.; Almyroudi, M.-P.; Myrianthefs, P.; Rello, J. COVID-19-Associated Pulmonary Aspergillosis (CAPA). J. Intensive Med. 2021, 1, 71–80. [Google Scholar] [CrossRef]
- Cag, Y.; Erdem, H.; Gunduz, M.; Komur, S.; Ankarali, H.; Ural, S.; Tasbakan, M.; Tattevin, P.; Tombak, A.; Ozturk-Engin, D.; et al. Survival in rhino-orbito-cerebral mucormycosis: An international, multicenter ID-IRI study. Eur. J. Intern. Med. 2022, 100, 56–61. [Google Scholar] [CrossRef]
- Khanna, P.; Kayarat, B. Posaconazole in the Prevention of COVID-19-associated Mucormycosis: A Concerning Contributor to the Rise in Antifungal Resistance. Indian J. Crit. Care Med. 2021, 25, 1209–1210. [Google Scholar] [CrossRef]
Figure 1.
PRISMA Flowchart of published studies related to COVID-19 associated mucormycosis.

Figure 2.
Geographical distribution of patients with COVID-19-associated mucormycosis (CAM) (n, %) reported in the 88 studies included.
Figure 2.
Geographical distribution of patients with COVID-19-associated mucormycosis (CAM) (n, %) reported in the 88 studies included.

Figure 3.
Clinical presentation of patients with CAM in total and in Europe.


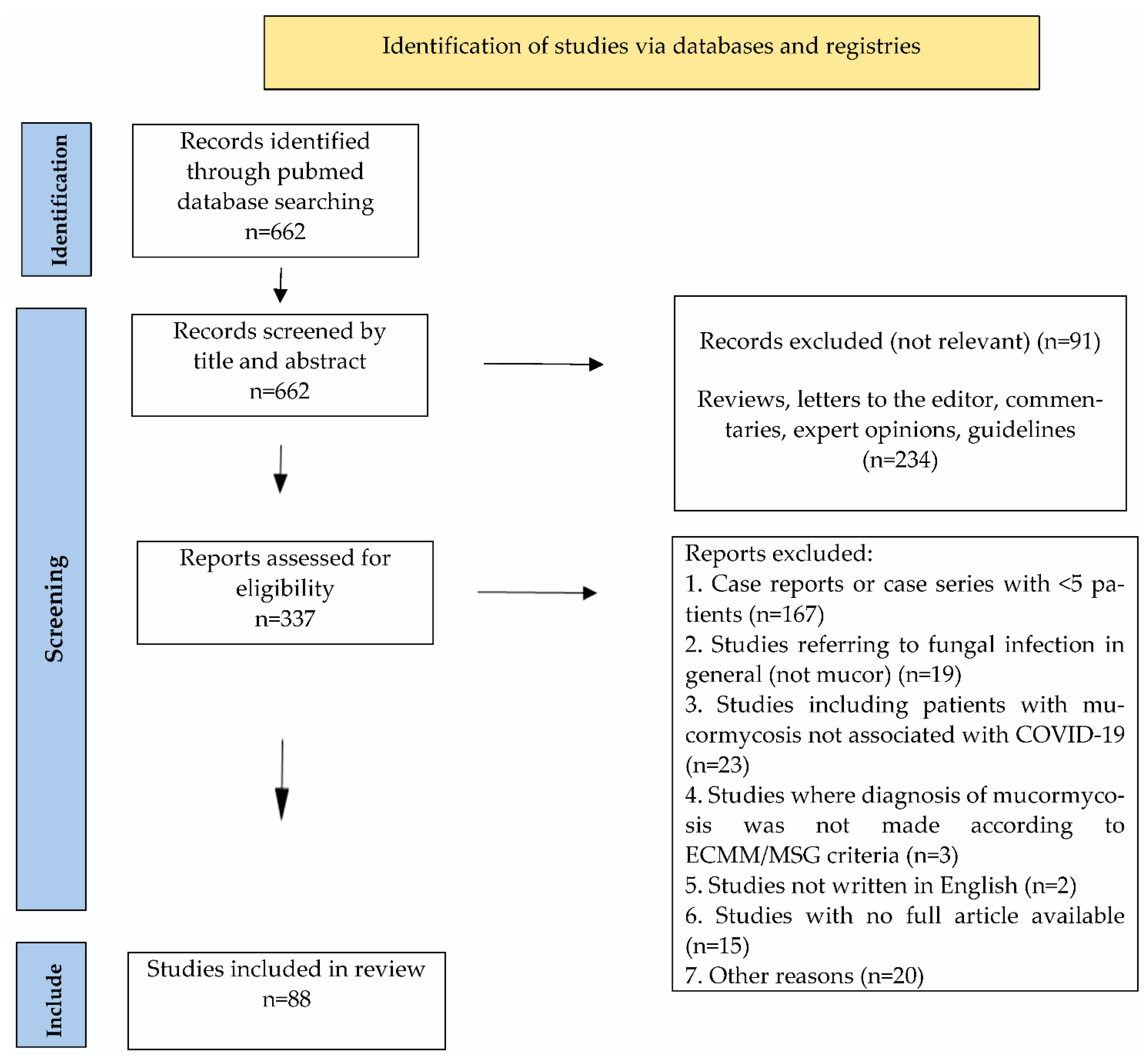{kind=link}
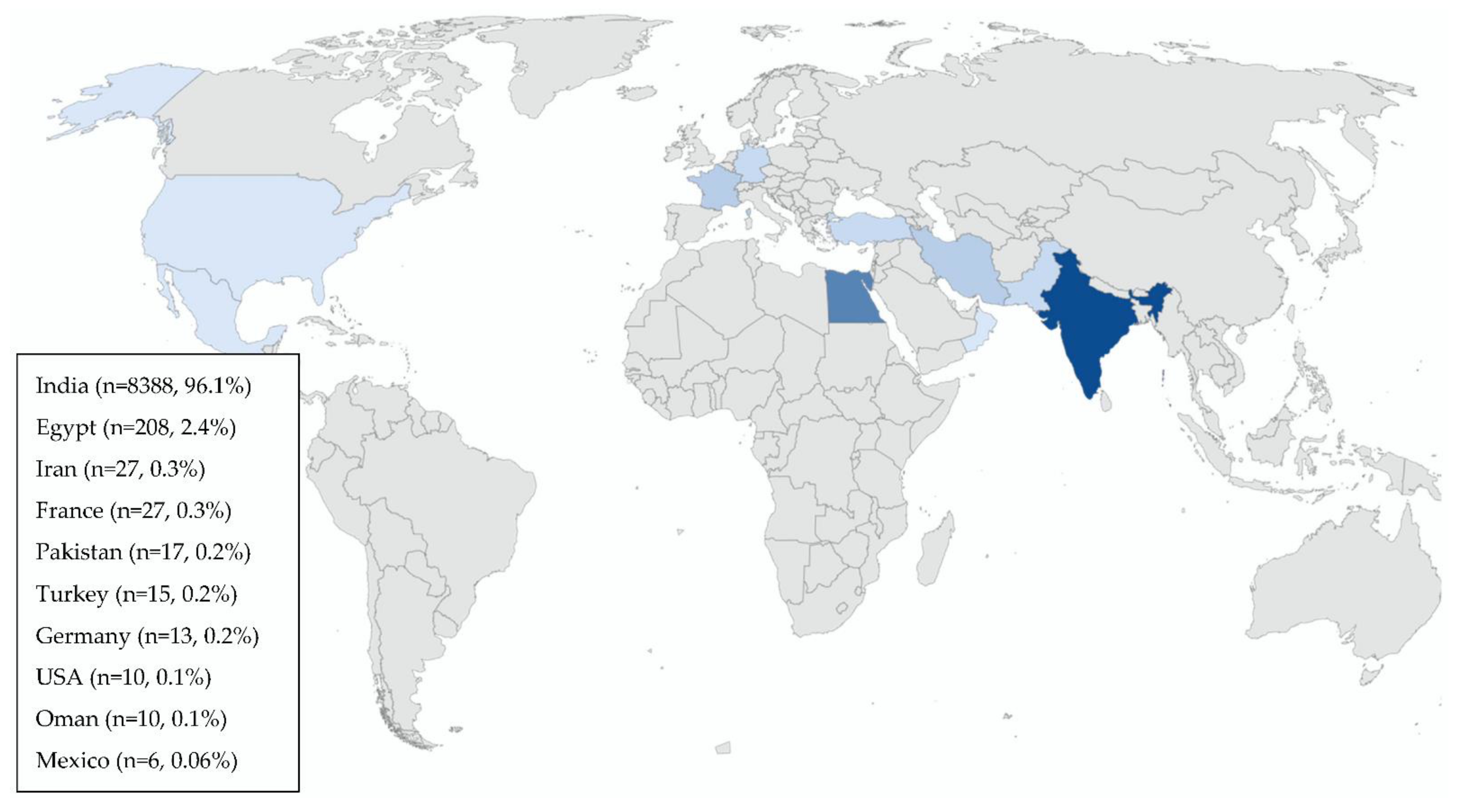{kind=link}
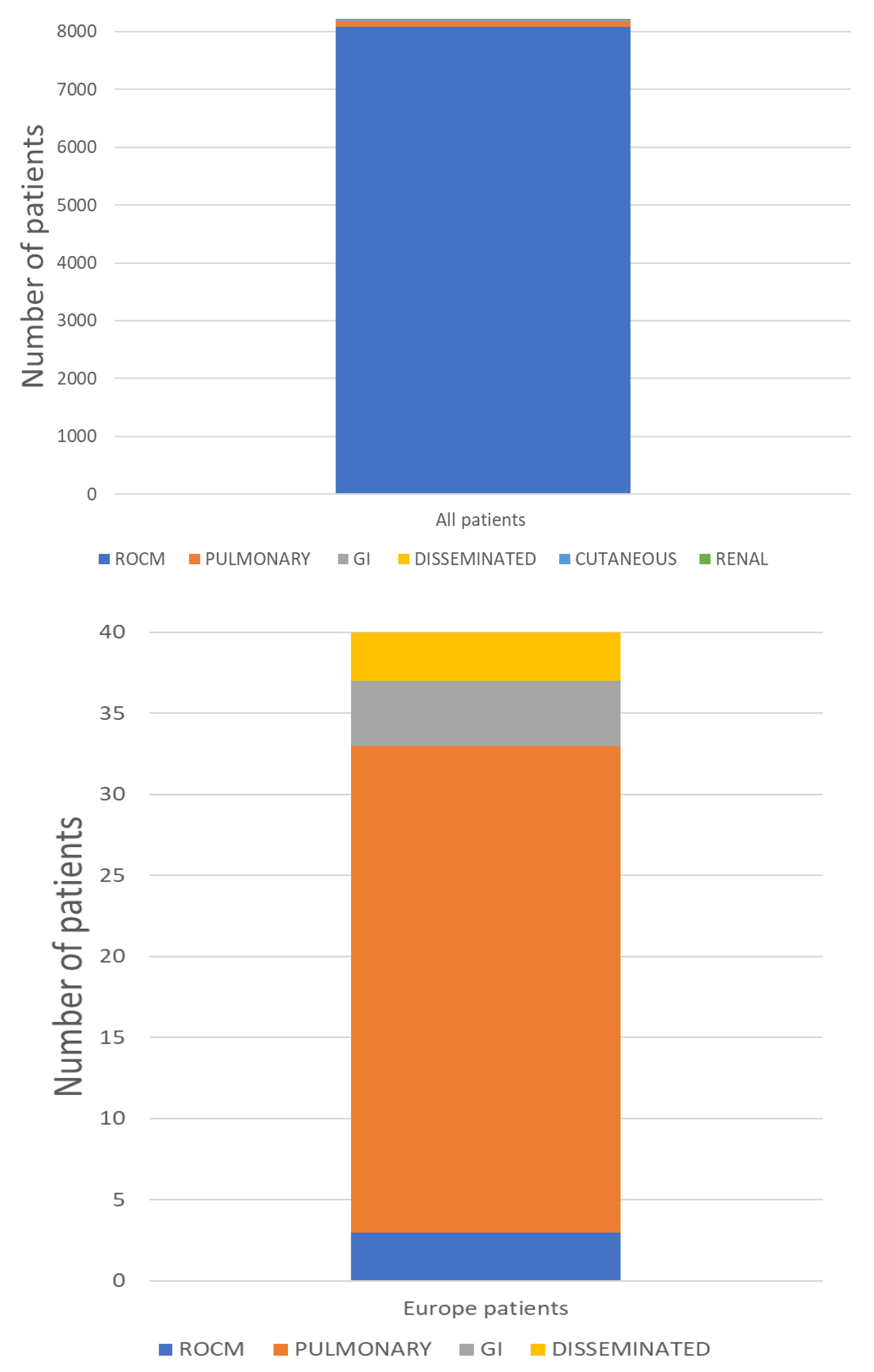{kind=link}
Table 1.
Studies’ characteristics.
| Study | Study Design | Country | CAM Patients (n) | Setting/Departments | Quality Rating * |
|---|---|---|---|---|---|
| Said Ahmed WM et al. [29] | Case series | Egypt | 14 | Oral and Maxillofacial Surgery | Fair |
| Murthy R et al. [30] | Case series | India | 111 | NA | Poor |
| Walia S et al. [31] | Prospective cohort study | India | 540 | Eye Care centre | Good |
| Vare AA et al. [32] | Retrospective | India | 67 | Hospital | Good |
| Fouad YA et al. [33] | Multicentric, retrospective case series | Egypt | 26 | Ophthalmological center | Good |
| Soni K et al. [34] | Retrospective | India | 145 | Tertiary care center | Good |
| Metwally MI et al. [35] | Cross section study | Egypt | 63 | Radiology department | Fair |
| Arora U et al. [36] | Retrospective case-control study | India | 152 | Tertiary care center | Good |
| Jindal G et al. [37] | Prospective observational | India | 15 | Radiology department | Fair |
| Syed-Abdul S et al. [38] | Retrospective | India | 214 | Tertiary care center | Fair |
| Patel A et al. [3] | Retrospective | India | 29 | Tertiary care center | Good |
| Pruthi H et al. [39] | Case series | India | 5 | Referral center | Poor |
| Bansal SB et al. [40] | Retrospective | India | 11 | Tertiary care center | Good |
| Dulski TM et al. [41] | MMWR/CDC | USA | 10 | 6 hospitals | Poor |
| Meshram HS et al. [42] | Retrospective cohort study | India | 61 | 18 transplant centers | Good |
| Aggarwal SK et al. [43] | Case series | India | 13 | Referral center | Fair |
| Kulkarni R et al. [44] | Retrospective, multi-centre study | India | 102 | 13 urban tertiary care centers | Good |
| Choksi T et al. [45] | Retrospective case–control study | India | 73 | Tertiary care center | Good |
| Kumar S et al. [46]. | Prospective | India | 287 | Tertiary care center | Good |
| Mehta R et al. [47] | Case series | India | 17 | Head and Neck Surgery | Poor |
| Panwar P et al. [48] | Case series | India | 7 | Tertiary care center | Fair |
| Patel DD et al. [49] | Cross-sectional study | India | 96 | Radiology department | Fair |
| Vaid N et al. [50] | Observational | India | 65 | Tertiary care center | Poor |
| Goddanti N et al. [51] | Retrospective cohort study | India | 300 | ENT center | Good |
| Yadav T et al. [52] | Retrospective | India | 50 | Tertiary care center | Fair |
| Meshram VB et al. [53] | Retrospective | India | 11 | Nephrology and transplantation | Good |
| Zirpe K et al. [54] | Retrospective, observational | India | 84 | Tertiary care center | Fair |
| Alloush TK et al. [55] | Retrospective case series | Egypt | 14 | Tertiary care center | Fair |
| Pal P et al. [56] | Retrospective observational | India | 10 | NA | Poor |
| Danion F et al. [57] | Retrospective nationwide study | France | 17 | 59 French mycology laboratories | Good |
| Nehara HR et al. [58] | Prospective observational | India | 105 | Tertiary care center | Fair |
| Pandiar D et al. [59] | Prospective observational | India | 12 | Outpatient center | Fair |
| Kumar S et al. [60] | Case–control study | India | 55 | Rural center | Good |
| Bilgic A et al. [61] | Retrospective cases series | India | 38 | 6 centers | Good |
| Guemas E et al. [62] | Retrospective | France | 10 | ICU | Good |
| Kumar SG et al. [63] | Retrospective | India | 101 | Tertiary care centre | Fair |
| Mani S et al. [64] | Retrospective observational | India | 89 | Tertiary care center | Fair |
| Dravid A et al. [65] | Retrospective cohort study | India | 59 | Tertiary care center | Good |
| Naruka S et al. [66] | Case series | India | 79 | Tertiary care center | Good |
| Jain K et al. [67] | Prospective | India | 95 | Tertiary care center | Fair |
| Bhanuprasad K et al. [68] | Prospective | India | 132 | Hospital | Good |
| Desai EJ et al. [69] | Observational | India | 100 | ENT department | Poor |
| Nasir \n et al. [70] | Observational | Pakistan | 10 | NA | Fair |
| Gupta\s et al. [71] | Observational retrospective | India | 56 | ENT department | Fair |
| Joshi S et al. [4] | Retrospective | India | 178 | ENT department | Fair |
| Pradhan P et al. [72] | Retrospective | India | 46 | Otorhinolaryngology department | Poor |
| Mehta RNM et al. [73] | Prospective interventional study | India | 215 | NA | Good |
| Riad A et al. [74] | Case series | Egypt | 7 | 4 hospitals | Fair |
| Guzmán-Castro S et al. [75] | Retrospective | Mexico | 6 | General hospital | Fair |
| Seidel D et al. [76] | Survey | Germany | 13 | 6 tertiary care centers | Good |
| Gupta R et al. [77] | Multicentric observational | India | 115 | Tertiary care centers | Fair |
| Alfishawy M et al. [78] | Case series | Egypt | 21 | NA | Fair |
| Dave TV et al. [79] | Multi-centric retrospective | India | 58 | 9 hospitals | Good |
| Selarka L et al. [80] | Prospective, observational, multi-centre | India | 47 | 3 tertiary care centers | Fair |
| Avatef Fazeli M et al. [81] | Observational retrospective | Iran | 12 | Educational therapeutic hospital | Good |
| Mishra Y et al. [82] | Descriptive study | India | 32 | COVID-19 Care Centre | Good |
| Sen M et al. [83] | Retrospective, observational | India | 2826 | 102 treatment centers | Fair |
| Pakdel F et al. [84] | Cross-sectional descriptive multicenter | Iran | 15 | 5 COVID-19 centers | Good |
| Y M. Reddy et al. [85] | Case series | India | 6 | Department of Neurology | Fair |
| R.Arora et al. [86] | Cross-sectional study | India | 60 | Hospital | Fair |
| D.P Gupta et al. [87] | Prospective cross-sectional study | India | 70 | ENT department | Poor |
| M.Gautam et al. [88] | Prospective cohort study | India | 30 | Department of ophthalmology | Fair |
| R.M.Mehta et al. [89] | Case series | India | 5 | Department of pulmonology and Critical Care Medicine | Fair |
| Y.M.Reddy et al. [90] | Retrospective cohort study | India | 31 | Tertiary care hospital | Fair |
| S.P.Singh et al. [91] | Case series | India | 6 | Tertiary care center | Fair |
| M.Hada et al. [92] | Cross-sectional study | India | 270 | Tertiary care center | Fair |
| M. Kumar H et al. [93] | Case–control study | India | 28 | Tertiary care hospital | Good |
| S. Bhandari et al. [94] | Prospective study | India | 235 | Tertiary care center | Poor |
| M Chouhan et al. [95] | Ambispective interventional study | India | 41 | Tertiary care center | Fair |
| Y. Singh et al. [96] | Case series | India | 13 | Tertiary care center | Fair |
| S M Desai et al. [97] | Retrospective study | India | 50 | Radiology department | Good |
| A. Kumari et al. [98] | Retrospective study | India | 20 | Tertiary care center | Fair |
| S. Mitra et al. [99] | Case series | India | 32 | ENT department | Poor |
| A Ramaswami et al. [100] | Retrospective study | India | 70 | Emergency department | Fair |
| A.R. Joshi et al. [101] | Retrospective study | India | 25 | Radiology department | Poor |
| A. Patel et al. [102] | Retrospective observational study | India | 187 | 16 healthcare centers | Good |
| S Sharma et al. [103] | Prospective observational study | India | 23 | Tertiary care centre | Fair |
| R. Kant et al. [104] | Case series | India | 100 | Tertiary care centre | Fair |
| C. Eker et al. [105] | Retrospective study | Turkey | 15 | Referral center for ENT care | Fair |
| A.K. Pandit et al. [106] | Case–control study | India | 61 | Tertiary care referral hospital | Good |
| S.F. Youssif et al. [107] | Retrospective cross-sectional | Egypt | 33 | Tertiary-care center | Good |
| A. Sekaran, et al. [108] | Retrospective study | India | 30 | Hospital | Fair |
| R. R. Shabana et al. [109] | Retrospective study | Egypt | 30 | Tertiary-care center | Fair |
| A. K Patel et al. [110] | Case–control study | India | 64 | Tertiary-care center | Good |
| H. D.D. Martins et al. [111] | Case series | Mexico, Brazil | 6 | Two referral services | Poor |
| S. Iqtadar et al. [112] | Case series | Pakistan | 7 | Hospital | Poor |
| A. Al Balushi et al. [113] | Case series | Oman | 10 | Secondary hospital | Fair |
| R. Soman et al. [114] | Case series | India | 28 | Hospital | Fair |
ENT: Ear, Nose and Throat, ICU: Intensive Care Unit, MMWR: Morbidity and Mortality Weekly Report. * According to the Quality Assessment Tool for Case Series Studies by the National Heart, Lung and Blood Institute (NHLBI).
Table 2.
Incidence of CAM among hospitalized COVID-19 patients, type of infection, invasive or non-invasive mechanical ventilation, risk factors and all-cause mortality.
Table 2.
Incidence of CAM among hospitalized COVID-19 patients, type of infection, invasive or non-invasive mechanical ventilation, risk factors and all-cause mortality.
| Study | Incidence of CAM (%) | Type of Infection (%) | Cerebral Involvement /ROCM pts, n (%) | IMV or NIV n (%) | DM (% of CAM pts) | Steroids Intake (% of CAM pts) | All-Cause Mortality (%) |
|---|---|---|---|---|---|---|---|
| Said Ahmed WM et al. [29] | NA | Maxillary osteomyelitis | 0/14 (0%) | NA | 64.2% DM 35.7% with temporary post-COVID-19 hyperglycemia | NA | NA |
| Murthy R et al. [30] | NA | RO | 0/111 (0%) | NA | NA | NA | NA |
| Walia S et al. [31] | NA | SN (100%), O (51.85%), C (9.44%), Cu (1.85%), P (0.18%). | 51/529 (9.6%) | NA | 97.96% | 84.85% | 9.25% |
| Vare AA et al. [32] | 1.36% | ROCM | 3/67 (5%) | 18/67 (27%) | 90% | 84% | 34% |
| Fouad YA et al. [33] | NA | O | 0/26 (0%) | NA | 96.2% | 76.9% | 46,2% |
| Soni K et al. [34] | NA | ROCM | 29/145 (20%) | NA | 86.2% | 65% | 18% |
| Metwally MI et al. [35] | NA | Head and neck | 8/63 (12.7%) | NA | 80.9% | 82.5% | 17.5% |
| Arora U et al. [36] | NA | RS (29%), RO (47.3%), ROCM (14.5%), O (1.3%), RO/palatal (5.3%), Cu (0.6%), P (1.3%), D (0.6%) | 22/148 (14.9%) | NA | 92.1% | 65.8% | NA |
| Jindal G et al. [37] | NA | ROCM | 9/15 (60%) | NA | 100% | 80% | 6.6% |
| Syed-Abdul S et al. [38] | NA | NA | NA | NA | NA | NA | NA |
| Patel A et al. [3] | NA | RO (96.5%), P (3.4%) | 0/28 (0%) | NA | NA | NA | NA |
| Pruthi H et al. [39] | NA | P | NA | 0/5 (0%) | 100% | NA | 80% |
| Bansal SB et al. [40] | 10.8% | RO (91%), P (9%) | NA | 0/11 (0%) | 64%, 36% developed transient hyperglycemia | 100% | 18.2% |
| Dulski TM et al. [41] | NA | RO (10%), ROCM (30%), P (30%), D (20%), GI (10%) | 3/4 (75%) | 5/10 (50%) | 80% | 90% | 60% |
| Meshram HS et al. [42] | 4.4% | ROCM (91.8%), P (8.2%) | 11/42 (26.2%) | 0/61 (0%) | 24.6% | 44% | 26.2% |
| Aggarwal SK et al. [43] | NA | ROCM | 4/13 (30.8%) | NA | 92.3% | 92.3% | 15.4% |
| Kulkarni R et al. [44] | 2.1% (1 centre) | ROCM | 12/102 (11.8%) | NA | 81.6% | NA | 51%. |
| Choksi T et al. [45] | NA | ROCM | 6/73 (2%) | 17/73 (23.3%) | 74% | 98% | 36% |
| Kumar S et al. [46] | NA | ROCM | 60/287 (21%) | NA | 80% | NA | NA |
| Mehta R et al. [47] | NA | ROCM | 0/17 (0%) | NA | 100% | NA | NA |
| Panwar P et al. [48] | NA | ROCM | 0/7 (0%) | NA | 100% | 42.8% | 0% |
| Patel DD et al. [49] | NA | ROCM | 21/96 (21.9%) | 6/96 (6.3%) | 71.8% | 82.3% | NA |
| Vaid N et al. [50] | NA | ROCM | NA | NA | 33.8% | 100% | 10.7% |
| Goddanti N et al. [51] | NA | ROCM | NA | NA | 95.7% | 79% | NA |
| Yadav T et al. [52] | NA | ROCM | 25/50 (50%) | NA | 86% | 44% | NA |
| Meshram VB et al. [53] | NA | ROCM (90.9%), P (9%) | 3/10 (30%) | 0/11 (0%) | 54.5% | 100% | 27% |
| Zirpe K et al. [54] | NA | ROCM | 20/84 (23.8%) | NA | 64.3% | 83.3% | 15.5% |
| Alloush TK et al. [55] | NA | ROCM | 9/14 (64.2%) | 0/14 (0%) | 92.8% | NA | 21.4% |
| Pal P et al. [56] | NA | ROCM | 3/10 (30%) | ΝA | 70% | 80% | 30% |
| Danion F et al. [57] | NA | P(53%), GI (18%), ROCM (12%), D (18%) | NA | 13/17 (76.5%) | 47% | 76.5% | 88% |
| Nehara HR et al. [58] | NA | ROCM | 18/105 (17.1%) | NA | 78.1% | 66.3% | 19.05% |
| Pandiar D et al. [59] | NA | Oral | 0/12 (0%) | NA | 66,7% | NA | NA |
| Kumar S et al. [60] | NA | NA | NA | 0/55 (0%) | 83.6% | 98.2% | 16% |
| Bilgic A et al. [61] | 2.5% | ROCM | NA | 6/38 (16%) | 50% | 100% | 5% |
| Guemas E et al. [62] | 7.1% | P | NA | NA | 20% | 90% | 50% |
| Kumar SG et al. [63] | NA | ROCM | 44/101 (43.6%) | NA | 94% | 80.1% | 17.8% |
| Mani S et al. [64] | NA | ROCM | 4/89 (4.5%) | NA | 96% | 92% | 3.4% |
| Dravid A et al. [65] | NA | ROCM (98.3%), D (1.7%) | 26/58 (44.8%) | 3/59 (5.1%) | 89.8% | 100% | 25.4% |
| Naruka S et al. [66] | NA | ROCM | 9/79 (11.4%) | NA | 100% | NA | 18.18% |
| Jain K et al. [67] | NA | ROCM | 3/95 (3.2%) | NA | 77% | 100% | 5.2% |
| Bhanuprasad K et al. [68] | NA | ROCM | 39 (29.5%) | 3/132 (2.3%) | 97.7% | 55.3% | 9.8% |
| Desai EJ et al. [69] | NA | ROCM | 0/100 (0%) | NA | 80% | NA | 20% |
| Nasir\n et al. [70] | 0.35% | P (60%), ROCM (40%) | 4/4 (100%) | 3/10 (30%) | 70% | 80% | 70% |
| Gupta \s et al. [71] | NA | ROCM | 4/56 (7.1%) | NA | 85% | 66% | 16% |
| Joshi S et al. [4] | NA | ROCM | 22/178 (12.4%) | 5/178 (2.8%) | 74.2% | 52.8% | 15% |
| Pradhan P et al. [72] | NA | ROCM | 10/46 (21.7%) | NA | 95.65% | 89.1% | 19.5% |
| Mehta RNM et al. [73] | NA | ROCM | 33/215 (15.3%) | NA | 91% | 88% | 12.1% |
| Riad A et al. [74] | NA | ROCM | 7/7 (100%) | NA | 85.7% | 100% | 0% |
| Guzmán-Castro S et al. [75] | 0.04% | ROCM (83.3%), P(16.6%) | 5/5 (100%) | 2/6 (33.3%) | 83.3% | 100% | 83.3% |
| Seidel D et al. [76] | 2 centres: 0.67%, 0.58% ICU: 1.47%, 1.78% | P(84.6%), ROCM (7.7%), GI (7.7%) | 1/1 (100%) | 11/13 (84.6%) | 23.07% | 84.6% | 53.8% |
| Gupta R et al. [77] | NA | ROCM | 25/115 (21.7%) | 13/115 (11.3%) | 85.2% | 100% | 21.7% |
| Alfishawy M et al. [78] | NA | ROCM (95.2%), P (4.8%) | 5/20 (25%) | NA | 90% | 100% | 33.3% |
| Dave TV et al. [79] | NA | ROCM | 19/58 (33%) | NA | 74% | NA | 34% |
| Selarka L et al. [80] | 1.8% | ROCM | 9/47 (19.1%) | 20/47 (42.6%) | 76.6% | 100% | 23.4% |
| Avatef Fazeli M et al. [81] | NA | ROCM | 0/12 (0%) | 1/12 (8.3%) | 83.33% | 75% | 66.7% |
| Mishra Y et al. [82] | 3.36% | ROCM | 0/32 (0%) | NA | 87.5% | 93% | 12.5% |
| Sen M et al. [83] | NA | ROCM | 539/2826 (19.1%) | 114/1602 (7.1) | 78% | 87% | 14% |
| Pakdel F et al. [84] | NA | ROCM | 7/15 (46%) | 1/15 (6.7%) | 86% | 46.6% | 47% |
| Y M. Reddy et al. [85] | NA | RO | 0/6 (0%) | NA | 100% | 66.7% | 100% |
| R. Arora et al. [86] | NA | ROCM | 6/60 (10%) | NA | 98.3% | 63.3% | NA |
| D.P Gupta et al. [87] | NA | ROCM | NA | NA | 100% | NA | 5.7% |
| M.Gautam et al. [88] | NA | ROCM | NA | NA | 100% | 66.7% | 0% |
| R.M.Mehta et al. [89] | NA | P | NA | 4/5 (80%) | 80% | 100% | 80% |
| Y.M.Reddy et al. [90] | NA | ROCM | NA | NA | 100% | 80.6% | 35.5% |
| S.P.Singh et al. [91] | NA | RO | 0/6 (0%) | 0/6 (0%) | 100% | 66.7% | 16.7% |
| M.Hada et al. [92] | NA | ROCM | 54/270 (20%) | NA | 92.2% | 72% | NA |
| M. Kumar H et al. [93] | NA | ROCM (85.7%), P (14.3%) | 15/24 (62.5%) | 6/28 (21.4%) | 75% | 70.4% | 73.9% |
| S. Bhandari et al. [94] | NA | NA | NA | NA | 86.8% | 84.3% | NA |
| M Chouhan et al. [95] | NA | ROCM | 9/41 (21.9%) | NA | 97.6% | 87.8% | 9.8% |
| Y. Singh et al. [96] | NA | ROCM (92.3%), P (7.7%) | 2/12 (16.7%) | 10/13 (76.9%) | 61.5% | 84.6% | 69.2% |
| S M Desai et al. [97] | NA | ROCM | 3/50 (6%) | NA | 82% | 84% | 30% |
| A. Kumari et al. [98] | NA | ROCM | 4/20 (20%) | NA | 80% | 80% | 30% |
| S. Mitra et al. [99] | NA | ROCM | NA | NA | 100% | 78.1% | NA |
| A Ramaswami et al. [100] | NA | ROCM | 17/70 (24.3%) | NA | 70% | 70% | NA |
| A.R. Joshi et al. [101] | NA | ROCM | 7/25 (28%) | 12/25 (48%) | 88% | 100% | 56% |
| A. Patel et al. [102] | 7 centers: 0.27% (general wards) | ROCM (86.1%), P (8.6%), renal (0.5%), other (e.g., Cu, GI) (2.7%), D (2.1%) | 44/161 (27.3%) | NA | 60.4% | 78.1% | 44.1% |
| S Sharma et al. [103] | NA | ROCM | 2/23 (8.7%) | NA | 91.3% | 100% | NA |
| R. Kant et al. [104] | NA | ROCM (96%), P (4%) | 11/96 (11.5%) | NA | 95% | 81% | 13% |
| C. Eker et al. [105] | NA | ROCM | 9/15 (60%) | NA | 100% | NA | 33.3% |
| A.K. Pandit et al. [106] | NA | ROCM | 30/56 (53.6%) | NA | 85.7% | 53.6% | 30.6% |
| S.F. Youssif et al. [107] | 7.6% | ROCM | 32/33 (97%) | NA | 63.6% | NA | 90.9% |
| A. Sekaran, et al. [108] | NA | ROCM | 6/30 (20%) | 8/30 (26.7%) | 100% | 90% | 16.7% |
| R. R. Shabana et al. [109] | NA | ROCM | 4/30 (13.3%) | 1/30 (3.3%) | 90% | 66.6% | 20% |
| A. K Patel et al. [110] | NA | ROCM (92.2%), P (7.8%) | 5/59 (8.5%) | NA | 75% | 90.6% | 4.7% |
| H. D.D. Martins et al. [111] | NA | ROCM | 0/6 (0%) | NA | 83.3% | NA | 16.7% |
| S. Iqtadar et al. [112] | NA | ROCM | NA | 0/7 (0%) | 71.4% | 100% | 14.3% |
| A. Al Balushi et al. [113] | NA | ROCM | 3/10 (30%) | 6/10 (60%) | 100% | 30% | 60% |
| R. Soman et al. [114] | NA | ROCM (78.6%), P (21.4%) | 5/22 (22.7%) | NA | NA | NA | 25% |
C: Cerebral, Cu: Cutaneous, DM: Diabetes Mellitus, D: Disseminated, GI: gastrointestinal, IMV: Invasive Mechanical Ventilation, NA: Not Available, NIV: Non-invasive ventilation, O: Orbital, P: Pulmonary, RO: Rhino Orbital, ROCM: Rhino-Orbital-Cerebral Mucormycosis, RS: Rhino-sinus, SN: Sinonasal.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Almyroudi, M.P.; Akinosoglou, K.; Rello, J.; Blot, S.; Dimopoulos, G. Clinical Phenotypes of COVID-19 Associated Mucormycosis (CAM): A Comprehensive Review. Diagnostics 2022, 12, 3092. https://doi.org/10.3390/diagnostics12123092
AMA Style
Almyroudi MP, Akinosoglou K, Rello J, Blot S, Dimopoulos G. Clinical Phenotypes of COVID-19 Associated Mucormycosis (CAM): A Comprehensive Review. Diagnostics. 2022; 12(12):3092. https://doi.org/10.3390/diagnostics12123092
Chicago/Turabian StyleAlmyroudi, Maria Panagiota, Karolina Akinosoglou, Jordi Rello, Stijn Blot, and George Dimopoulos. 2022. "Clinical Phenotypes of COVID-19 Associated Mucormycosis (CAM): A Comprehensive Review" Diagnostics 12, no. 12: 3092. https://doi.org/10.3390/diagnostics12123092
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.