
Evolution of Diagnostic Methods for Helicobacter pylori Infections: From Traditional Tests to High Technology, Advanced Sensitivity and Discrimination Tools

 ,
, 
Abstract
:1. Introduction
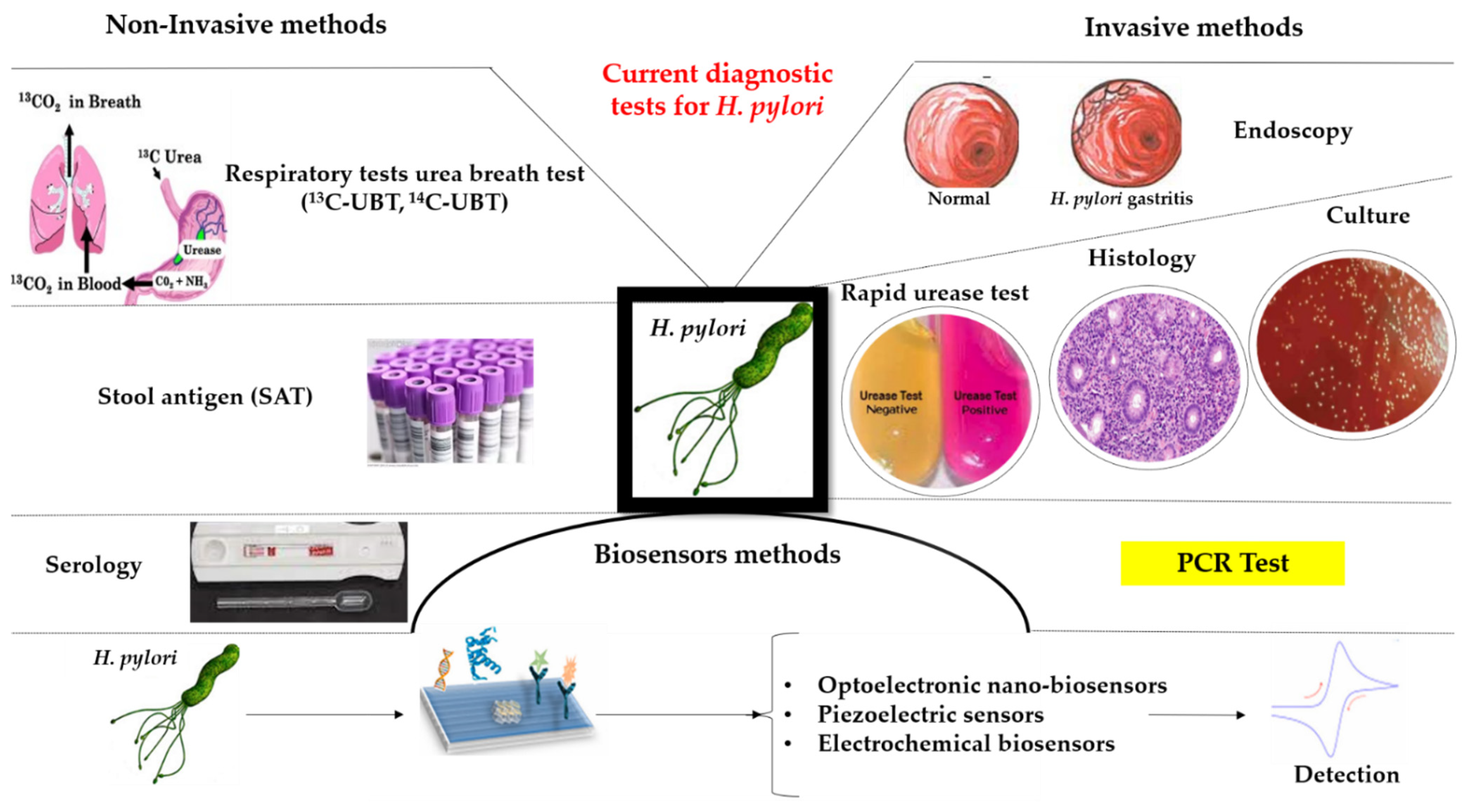
2. Current Diagnostic Methods
2.1. Non-Invasive Tests
2.1.1. Urea Breath Tests (UBT)
2.1.2. Stool Antigen Test (SAT)
2.1.3. Serology
2.2. Invasive Methods
2.2.1. Endoscopy
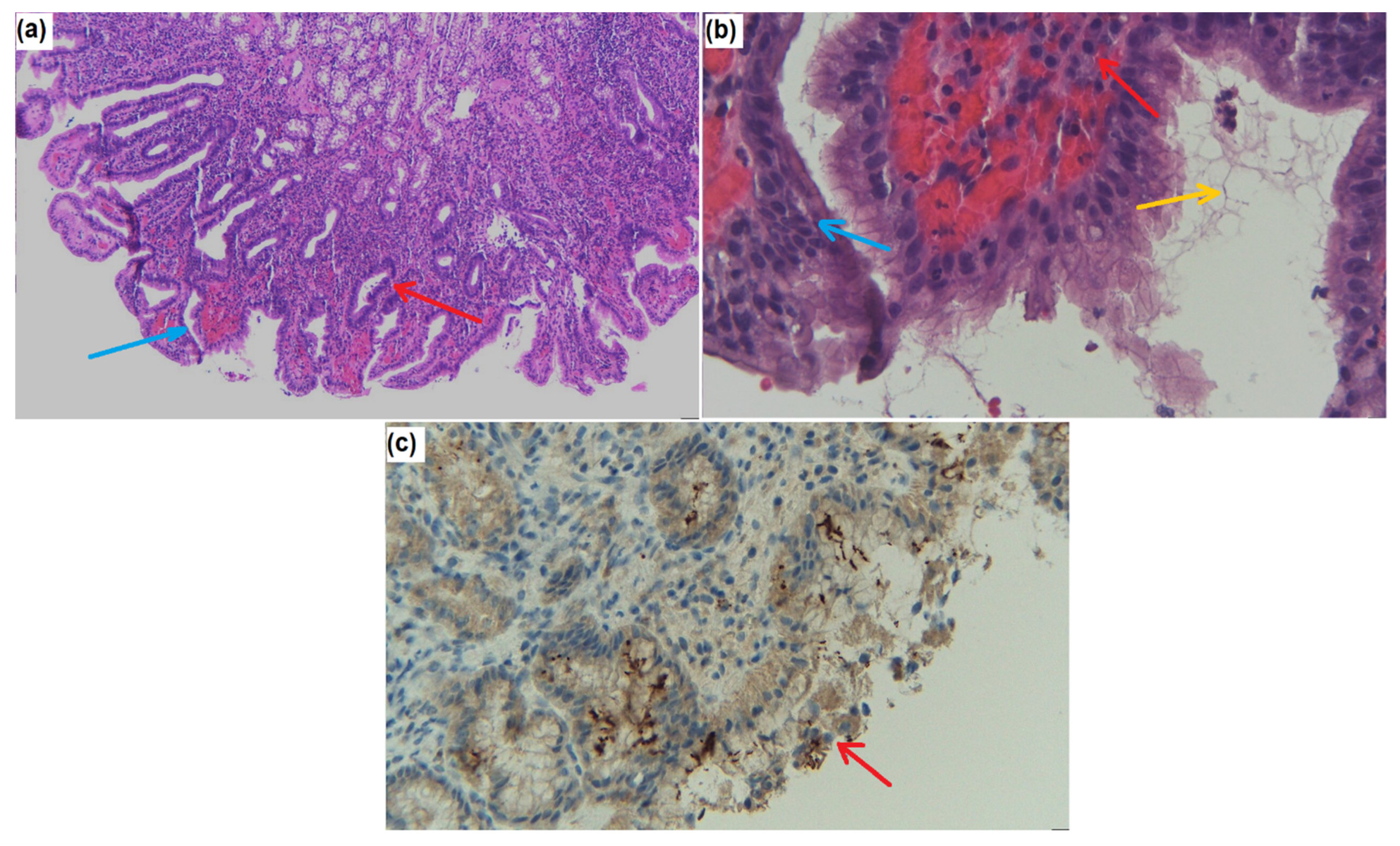
2.2.2. Histology
2.2.3. Rapid Urease Test (RUT)
2.2.4. Culture
2.2.5. Molecular Testing
2.3. Advantages and Disadvantages of the Current Available Diagnostic Tests
3. Matrix-Assisted Laser Desorption/Ionization–TIME-of-Flight—Mass Spectrometry (MALDI-TOF MS)
4. Biosensors
4.1. Optoelectronic Nano-Biosensors for H. pylori Detection
4.2. Piezoelectric Sensors
4.3. Electrochemical Biosensors
5. Point of Care (POC) Diagnostic-Nano Sensors
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Marshall, B.J.; Warren, J.R. Unidentified Curved Bacilli in the Stomach of Patients with Gastritis and Peptic Ulceration. Lancet 1984, 1, 1311–1315. [Google Scholar] [CrossRef]
- Malnick, S.D.H.; Melzer, E.; Attali, M.; Duek, G.; Yahav, J. Helicobacter pylori: Friend or Foe? World J. Gastroenterol. 2014, 20, 8979–8985. [Google Scholar] [CrossRef] [PubMed]
- Hooi, J.K.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; Wong, V.W.S.; Wu, J.C.Y.; et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamani, M.; Ebrahimtabar, F.; Zamani, V.; Miller, W.; Alizadeh-Navaei, R.; Shokri-Shirvani, J.; Derakhshan, M. Systematic Review with Meta-Analysis: The Worldwide Prevalence of Helicobacter pylori Infection. Aliment. Pharmacol. Ther. 2018, 47, 868–876. [Google Scholar] [CrossRef] [Green Version]
- IARC Working Group. Schistosomes, Liver Flukes and Helicobacter pylori. In IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; International Agency for Research on Cancer: Lyon, France, 1994; Volume 61, pp. 1–241. [Google Scholar]
- Mladenova, I. Clinical Relevance of Helicobacter pylori Infection. J. Clin. Med. 2021, 10, 3473. [Google Scholar] [CrossRef]
- Ford, A.C.; Forman, D.; Hunt, R.H.; Yuan, Y.; Moayyedi, P. Helicobacter pylori Eradication Therapy to Prevent Gastric Cancer in Healthy Asymptomatic Infected Individuals: Systematic. Review and Meta-Analysis of Randomised Controlled Trials. BMJ 2014, 348, g3174. [Google Scholar] [CrossRef] [Green Version]
- Díaz, P.; Valenzuela Valderrama, M.; Bravo, J.; Quest, A.F.G. Helicobacter pylori and Gastric Cancer: Adaptive Cellular Mechanisms Involved in Disease Progression. Front. Microbiol. 2018, 9, 5. [Google Scholar] [CrossRef] [Green Version]
- Cardos, I.A.; Zaha, D.C.; Sindhu, R.K.; Cavalu, S. Revisiting Therapeutic Strategies for H. Pylori Treatment in the Context of Antibiotic Resistance: Focus on Alternative and Complementary Therapies. Molecules 2021, 26, 6078. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori Infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [Green Version]
- Chey, W.D.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am. J. Gastroenterol. 2017, 112, 212–239. [Google Scholar] [CrossRef]
- Alipour, M. Molecular Mechanism of Helicobacter Pylori-Induced Gastric Cancer. J. Gastrointest. Cancer 2021, 52, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Xue, H.; Lin, B.; Ni, P.; Xu, H.; Huang, G. Interleukin-1B and Interleukin-1 RN Polymorphisms and Gastric Carcinoma Risk: A Meta-Analysis. J. Gastroenterol. Hepatol. 2010, 25, 1604–1617. [Google Scholar] [CrossRef] [PubMed]
- Baj, J.; Forma, A.; Sitarz, M.; Portincasa, P.; Garruti, G.; Krasowska, D.; Maciejewski, R. Helicobacter pylori Virulence Factors-Mechanisms of Bacterial Pathogenicity in the Gastric Microenvironment. Cells 2020, 10, 27. [Google Scholar] [CrossRef] [PubMed]
- Ansari, S.; Yamaoka, Y. Helicobacter pylori BabA in Adaptation for Gastric Colonization. World J. Gastroenterol. 2017, 23, 4158–4169. [Google Scholar] [CrossRef]
- Raza, Y.; Ahmed, A.; Khan, A.; Chishti, A.A.; Akhter, S.S.; Mubarak, M.; Bernstein, C.; Zaitlin, B.; Kazmi, S.U. Helicobacter pylori Severely Reduces Expression of DNA Repair Proteins PMS2 and ERCC1 in Gastritis and Gastric Cancer. DNA Repair 2020, 89, 102836. [Google Scholar] [CrossRef]
- Aziz, Z.W.; Saleem, S.H.; Al-Nuaimy, H.A. Helicobacter pylori in Gastric Biopsy: A Histochemical and Immunohistochemical Assessment. Ann. Coll. Med. Mosul 2020, 41, 139–147. [Google Scholar] [CrossRef]
- Denic, M.; Touati, E.; De Reuse, H. Review: Pathogenesis of Helicobacter pylori Infection. Helicobacter 2020, 25 (Suppl. 1), e12736. [Google Scholar] [CrossRef]
- Fagoonee, S.; Pellicano, R. Helicobacter Pylori: Molecular Basis for Colonization and Survival in Gastric Environment and Resistance to Antibiotics. A Short Review. Infect. Dis. 2019, 51, 399–408. [Google Scholar] [CrossRef]
- Posselt, G.; Backert, S.; Wessler, S. The Functional Interplay of Helicobacter pylori Factors with Gastric Epithelial Cells Induces a Multi-Step Process in Pathogenesis. Cell Commun. Signal. CCS 2013, 11, 77. [Google Scholar] [CrossRef] [Green Version]
- Ilver, D.; Arnqvist, A.; Ogren, J.; Frick, I.-M.; Kersulyte, D.; Incecik, E.; Berg, D.; Covacci, A.; Engstrand, L.; Borén, T. Helicobacter pylori Adhesin Binding Fucosylated Histo-Blood Group Antigens Revealed by Retagging. Science 1998, 279, 373–377. [Google Scholar] [CrossRef]
- Whitmire, J.M.; Merrell, D.S. Helicobacter pylori Genetic Polymorphisms in Gastric Disease Development. Adv. Exp. Med. Biol. 2019, 1149, 173–194. [Google Scholar] [CrossRef] [PubMed]
- Enroth, H.; Kraaz, W.; Engstrand, L.; Nyrén, O.; Rohan, T. Helicobacter pylori Strain Types and Risk of Gastric Cancer: A Case-Control Study. Cancer Epidemiol. Biomarkers Prev. 2000, 9, 981–985. [Google Scholar] [PubMed]
- Burucoa, C.; Axon, A. Epidemiology of Helicobacter pylori Infection. Helicobacter 2017, 22 (Suppl. 1), 1–5. [Google Scholar] [CrossRef] [PubMed]
- Leja, M.; Grinberga-Derica, I.; Bilgilier, C.; Steininger, C. Review: Epidemiology of Helicobacter pylori Infection. Helicobacter 2019, 24 (Suppl. 1), e12635. [Google Scholar] [CrossRef] [Green Version]
- Yucel, O. Prevention of Helicobacter pylori Infection in Childhood. World J. Gastroenterol. 2014, 20, 10348–10354. [Google Scholar] [CrossRef]
- Zhu, R.; Chen, K.; Zheng, Y.-Y.; Zhang, H.-W.; Wang, J.-S.; Xia, Y.-J.; Dai, W.-Q.; Wang, F.; Shen, M.; Cheng, P.; et al. Meta-Analysis of the Efficacy of Probiotics in Helicobacter pylori Eradication Therapy. World J. Gastroenterol. 2014, 20, 18013–18021. [Google Scholar] [CrossRef] [PubMed]
- Ferwana, M.; Abdulmajeed, I.; Alhajiahmed, A.; Madani, W.; Firwana, B.; Hasan, R.; Altayar, O.; Limburg, P.J.; Murad, M.H.; Knawy, B. Accuracy of Urea Breath Test in Helicobacter pylori Infection: Meta-Analysis. World J. Gastroenterol. 2015, 21, 1305–1314. [Google Scholar] [CrossRef]
- Graham, D.Y.; Miftahussurur, M. Helicobacter pylori Urease for Diagnosis of Helicobacter pylori Infection: A Mini Review. J. Adv. Res. 2018, 13, 51–57. [Google Scholar] [CrossRef]
- Zhou, Q.; Li, L.; Ai, Y.; Pan, Z.; Guo, M.; Han, J. Diagnostic Accuracy of the 14C-Urea Breath Test in Helicobacter pylori Infections: A Meta-Analysis. Wien. Klin Wochenschr. 2017, 129, 38–45. [Google Scholar] [CrossRef]
- Honar, N.; Minazadeh, A.; Shakibazad, N.; Haghighat, M.; Saki, F.; Javaherizadeh, H. Diagnostic Accuracy Of Urea Breath Test For Helicobacter pylori Infection In Children With Dyspepsia In Comparison To Histopathology. Arch. Gastroenterol. 2016, 53, 108–112. [Google Scholar] [CrossRef] [Green Version]
- Ling, D. Carbon-13 Urea Breath Test for Helicobacter pylori Infection in Patients with Uninvestigated Ulcer-like Dyspepsia: An Evidence-Based Analysis. Ont. Health Technol. Assess. Ser. 2013, 13, 1–30. [Google Scholar]
- Best, L.M.; Takwoingi, Y.; Siddique, S.; Selladurai, A.; Gandhi, A.; Low, B.; Yaghoobi, M.; Gurusamy, K.S. Non-Invasive Diagnostic Tests for Helicobacter pylori Infection. Cochrane Database Syst. Rev. 2018, 3, CD012080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimoyama, T. Stool Antigen Tests for the Management of Helicobacter pylori Infection. World J. Gastroenterol. 2013, 19, 8188–8191. [Google Scholar] [CrossRef] [PubMed]
- Kodama, M.; Murakami, K.; Okimoto, T.; Fukuda, Y.; Shimoyama, T.; Okuda, M.; Kato, C.; Kobayashi, I.; Fujioka, T. Influence of Proton Pump Inhibitor Treatment on Helicobacter pylori Stool Antigen Test. World J. Gastroenterol. 2012, 18, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Leal, Y.A.; Cedillo-Rivera, R.; Simón, J.A.; Velázquez, J.R.; Flores, L.L.; Torres, J. Utility of Stool Sample-Based Tests for the Diagnosis of Helicobacter pylori Infection in Children. J. Pediatr. Gastroenterol. Nutr. 2011, 52, 718–728. [Google Scholar] [CrossRef]
- Lopes, A.I.; Vale, F.F.; Oleastro, M. Helicobacter pylori Infection—Recent Developments in Diagnosis. World J. Gastroenterol. 2014, 20, 9299–9313. [Google Scholar] [CrossRef] [Green Version]
- Burucoa, C.; Delchier, J.-C.; Courillon-Mallet, A.; de Korwin, J.-D.; Mégraud, F.; Zerbib, F.; Raymond, J.; Fauchère, J.-L. Comparative Evaluation of 29 Commercial Helicobacter pylori Serological Kits. Helicobacter 2013, 18, 169–179. [Google Scholar] [CrossRef]
- Sugano, K.; Tack, J.; Kuipers, E.; Graham, D.; El-Omar, E.; Miura, S.; Haruma, K.; Asaka, M.; Uemura, N.; Malfertheiner, P. Kyoto Global Consensus Report on Helicobacter pylori Gastritis. Gut 2015, 64, 9252. [Google Scholar] [CrossRef] [Green Version]
- McNicholl, A.G.; Forné, M.; Barrio, J.; De la Coba, C.; González, B.; Rivera, R.; Esteve, M.; Fernandez-Bañares, F.; Madrigal, B.; Gras-Miralles, B.; et al. Accuracy of GastroPanel for the Diagnosis of Atrophic Gastritis. Eur. J. Gastroenterol. Hepatol. 2014, 26, 941–948. [Google Scholar] [CrossRef] [Green Version]
- Nishikawa, Y.; Ikeda, Y.; Murakami, H.; Hori, S.-I.; Hino, K.; Sasaki, C.; Nishikawa, M. Classification of Atrophic Mucosal Patterns on Blue LASER Imaging for Endoscopic Diagnosis of Helicobacter Pylori-Related Gastritis: A Retrospective, Observational Study. PLoS ONE 2018, 13, e0193197. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Wang, F.; Zhou, Y.; Xia, G.-L.; Dong, L.; He, W.-H.; Xiao, B. Blue Laser Magnifying Endoscopy in the Diagnosis of Chronic Gastritis. Exp. Ther. Med. 2019, 18, 1993–2000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, J.R.; Sami, S.S.; Reddiar, D.; Mannath, J.; Ortiz-Fernández-Sordo, J.; Beg, S.; Scott, R.; Thiagarajan, P.; Ahmad, S.; Parra-Blanco, A.; et al. Narrow Band Imaging and Serology in the Assessment of Premalignant Gastric Pathology. Scand. J. Gastroenterol. 2018, 53, 1611–1618. [Google Scholar] [CrossRef]
- Wang, Y.-K.; Kuo, F.-C.; Liu, C.-J.; Wu, M.-C.; Shih, H.-Y.; Wang, S.S.W.; Wu, J.-Y.; Kuo, C.-H.; Huang, Y.-K.; Wu, D.-C. Diagnosis of Helicobacter pylori Infection: Current Options and Developments. World J. Gastroenterol. 2015, 21, 11221–11235. [Google Scholar] [CrossRef] [PubMed]
- Shukla, S.; Pujani, M.; Agarwal, A.; Pujani, M.; Rohtagi, A. Correlation of Serology with Morphological Changes in Gastric Biopsy in Helicobacter pylori Infection and Evaluation of Immunohistochemistry for H. pylori Identification. Saudi J. Gastroenterol. 2012, 18, 369–374. [Google Scholar] [CrossRef]
- Pity, I.S.; Baizeed, A.M. Identification of Helicobacter pylori in Gastric Biopsies of Patients with Chronic Gastritis: Histopathological and Immunohistochemical Study. Duhok Med. J. 2011, 5, 69–77. [Google Scholar]
- Ibrahim, A.; Morais, S.; Ferro, A.; Lunet, N.; Peleteiro, B. Sex-Differences in the Prevalence of Helicobacter pylori Infection in Pediatric and Adult Populations: Systematic Review and Meta-Analysis of 244 Studies. Dig. Liver Dis. 2017, 49, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Pranjal Sharma, R.; Kalpana Kumari, M.K. Histological Identification of Helicobacter pylori: Comparison of Staining Methods. Int. J. Med. Res. Rev. 2015, 3, 1167–1173. [Google Scholar] [CrossRef]
- Benoit, A.; Hoyeau, N.; Fléjou, J.-F. Diagnosis of Helicobacter pylori infection on gastric biopsies: Standard stain, special stain or immunohistochemistry? Ann. Pathol. 2018, 38, 363–369. [Google Scholar] [CrossRef]
- Snead, D.R.J.; Tsang, Y.-W.; Meskiri, A.; Kimani, P.K.; Crossman, R.; Rajpoot, N.M.; Blessing, E.; Chen, K.; Gopalakrishnan, K.; Matthews, P.; et al. Validation of Digital Pathology Imaging for Primary Histopathological Diagnosis. Histopathology 2016, 68, 1063–1072. [Google Scholar] [CrossRef] [Green Version]
- Glickman, J.N.; Noffsinger, A.; Nevin, D.T.; Ray, M.; Lash, R.H.; Genta, R.M. Helicobacter Infections with Rare Bacteria or Minimal Gastritis: Expecting the Unexpected. Dig. Liver Dis. 2015, 47, 549–555. [Google Scholar] [CrossRef]
- Cerqueira, L.; Fernandes, R.M.; Ferreira, R.M.; Oleastro, M.; Carneiro, F.; Brandão, C.; Pimentel-Nunes, P.; Dinis-Ribeiro, M.; Figueiredo, C.; Keevil, C.W.; et al. Validation of a Fluorescence In Situ Hybridization Method Using Peptide Nucleic Acid Probes for Detection of Helicobacter pylori Clarithromycin Resistance in Gastric Biopsy Specimens. J. Clin. Microbiol. 2013, 51, 1887–1893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godbole, G.; Mégraud, F.; Bessède, E. Review: Diagnosis of Helicobacter pylori Infection. Helicobacter 2020, 25 (Suppl. 1), e12735. [Google Scholar] [CrossRef]
- Dore, M.P.; Pes, G.M. What Is New in Helicobacter pylori Diagnosis. An Overview. J. Clin. Med. 2021, 10, 2091. [Google Scholar] [CrossRef] [PubMed]
- Mégraud, F.; Bessède, E.; Lehours, P. Current Methods Used for the Diagnosis of Helicobacter pylori Infection. Available online: https://www.eurekaselect.com/120887/chapter (accessed on 29 November 2021).
- Lee, T.-H.; Lin, C.-C.; Chung, C.-S.; Lin, C.-K.; Liang, C.-C.; Tsai, K.-C. Increasing Biopsy Number and Sampling from Gastric Body Improve the Sensitivity of Rapid Urease Test in Patients with Peptic Ulcer Bleeding. Dig. Dis. Sci. 2015, 60, 454–457. [Google Scholar] [CrossRef]
- Dechant, F.-X.; Dechant, R.; Kandulski, A.; Selgrad, M.; Weber, F.; Reischl, U.; Wilczek, W.; Mueller, M.; Weigand, K. Accuracy of Different Rapid Urease Tests in Comparison with Histopathology in Patients with Endoscopic Signs of Gastritis. Digestion 2020, 101, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Dolak, W.; Bilgilier, C.; Stadlmann, A.; Leiner, J.; Püspök, A.; Plieschnegger, W.; Siebert, F.; Wewalka, F.; Schöfl, R.; Huber-Schönauer, U.; et al. A Multicenter Prospective Study on the Diagnostic Performance of a New Liquid Rapid Urease Test for the Diagnosis of Helicobacter pylori Infection. Gut Pathog. 2017, 9, 78. [Google Scholar] [CrossRef] [Green Version]
- Kuhns, L.G.; Benoit, S.L.; Bayyareddy, K.; Johnson, D.; Orlando, R.; Evans, A.L.; Waldrop, G.L.; Maier, R.J. Carbon Fixation Driven by Molecular Hydrogen Results in Chemolithoautotrophically Enhanced Growth of Helicobacter pylori. J. Bacteriol. 2016, 198, 1423–1428. [Google Scholar] [CrossRef] [Green Version]
- Peretz, A.; Paritsky, M.; Pastukh, N.; Koifman, A.; Brodsky, D.; Glyatman, T.; On, A. Improvement and Optimization of the Classical Gastric Biopsy Culture Technique for Helicobacter pylori Diagnosis Using Trypsin. J. Med. Microbiol. 2015, 64, 642–645. [Google Scholar] [CrossRef] [Green Version]
- Hortelano, I.; Moreno, Y.; Vesga, F.J.; Ferrús, M.A. Evaluation of Different Culture Media for Detection and Quantification of H. pylori in Environmental and Clinical Samples. Int. Microbiol. 2020, 23, 481–487. [Google Scholar] [CrossRef]
- Leszczyńska, K.; Namiot, A.; Namiot, Z.; Leszczyńska, J.K.; Jakoniuk, P.; Chilewicz, M.; Namiot, D.B.; Kemona, A.; Milewski, R.; Bucki, R. Patient Factors Affecting Culture of Helicobacter pylori Isolated from Gastric Mucosal Specimens. Adv. Med. Sci. 2010, 55, 161–166. [Google Scholar] [CrossRef]
- Mégraud, F.; Lehours, P. Helicobacter pylori Detection and Antimicrobial Susceptibility Testing. Clin. Microbiol. Rev. 2007, 20, 280–322. [Google Scholar] [CrossRef] [Green Version]
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of Antibiotic Resistance in Helicobacter pylori: A Systematic Review and Meta-Analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382.e17. [Google Scholar] [CrossRef] [Green Version]
- Pichon, M.; Pichard, B.; Barrioz, T.; Plouzeau, C.; Croquet, V.; Fotsing, G.; Chéron, A.; Vuillemin, É.; Wangermez, M.; Haineaux, P.-A.; et al. Diagnostic Accuracy of a Noninvasive Test for Detection of Helicobacter pylori and Resistance to Clarithromycin in Stool by the Amplidiag H. pylori + ClariR Real-Time PCR Assay. J. Clin. Microbiol. 2020, 58, e01787-19. [Google Scholar] [CrossRef] [PubMed]
- Kovacheva-Slavova, M.; Valkov, H.; Angelov, T.; Tropcheva, R.; Vladimirov, B. Screening for Helicobacter pylori Infection and Clarithromycin Resistance Using Real-Time Polymerase Chain Reaction. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5042–5046. [Google Scholar] [CrossRef] [PubMed]
- Gong, R.-J.; Xu, C.-X.; Li, H.; Liu, X.-M. Polymerase Chain Reaction-Based Tests for Detecting Helicobacter pylori Clarithromycin Resistance in Stool Samples: A Meta-Analysis. World J. Clin. Cases 2021, 9, 133–147. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.; Vaghasiya, J.; Pancholi, S.S.; Paul, A. Therapeutic Potential Of Secoisolariciresinol Diglucoside: A Plant Lignan. Int. J. Pharm. Sci. Drug Res. 2012, 4, 15–18. [Google Scholar]
- Roth, D.E.; Taylor, D.N.; Gilman, R.H.; Meza, R.; Katz, U.; Bautista, C.; Cabrera, L.; Velapatiño, B.; Lebron, C.; Razúri, M.; et al. Posttreatment Follow-up of Helicobacter pylori Infection Using a Stool Antigen Immunoassay. Clin. Diagn. Lab. Immunol. 2001, 8, 718–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menoni, S.M.F.; Bonon, S.H.A.; Zeitune, J.M.R.; Costa, S.C.B. PCR-Based Detection and Genotyping of Helicobacter pylori in Endoscopic Biopsy Samples from Brazilian Patients. Gastroenterol. Res. Pract. 2013, 2013, e951034. [Google Scholar] [CrossRef] [Green Version]
- Mishra, S.; Singh, V.; Rao, G.R.K.; Dixit, V.K.; Gulati, A.K.; Nath, G. Prevalence of Helicobacter pylori in Asymptomatic Subjects-a Nested PCR Based Study. Infect. Genet. Evol. 2008, 8, 815–819. [Google Scholar] [CrossRef]
- Lottspeich, C.; Schwarzer, A.; Panthel, K.; Koletzko, S.; Rüssmann, H. Evaluation of the Novel Helicobacter pylori ClariRes Real-Time PCR Assay for Detection and Clarithromycin Susceptibility Testing of H. Pylori in Stool Specimens from Symptomatic Children. J. Clin. Microbiol 2007, 45, 1718–1722. [Google Scholar] [CrossRef] [Green Version]
- Pohl, D.; Keller, P.M.; Bordier, V.; Wagner, K. Review of Current Diagnostic Methods and Advances in Helicobacter pylori Diagnostics in the Era of next Generation Sequencing. World J. Gastroenterol. 2019, 25, 4629–4660. [Google Scholar] [CrossRef] [PubMed]
- Šeligová, B.; Lukáč, Ľ.; Bábelová, M.; Vávrová, S.; Sulo, P. Diagnostic Reliability of Nested PCR Depends on the Primer Design and Threshold Abundance of Helicobacter pylori in Biopsy, Stool, and Saliva Samples. Helicobacter 2020, 25, e12680. [Google Scholar] [CrossRef] [PubMed]
- Wieser, A.; Schneider, L.; Jung, J.; Schubert, S. MALDI-TOF MS in Microbiological Diagnostics-Identification of Microorganisms and beyond (Mini Review). Appl. Microbiol. Biotechnol. 2012, 93, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Berlamont, H.; De Witte, C.; De Bruyckere, S.; Fox, J.G.; Backert, S.; Smet, A.; Boyen, F.; Haesebrouck, F. Differentiation of Gastric Helicobacter Species Using MALDI-TOF Mass Spectrometry. Pathogens 2021, 10, 366. [Google Scholar] [CrossRef]
- Singhal, N.; Kumar, M.; Kanaujia, P.K.; Virdi, J.S. MALDI-TOF Mass Spectrometry: An Emerging Technology for Microbial Identification and Diagnosis. Front. Microbiol. 2015, 6, 791. [Google Scholar] [CrossRef] [Green Version]
- Carroll, K.C.; Patel, R. Systems for Identification of Bacteria and Fungi. In Manual of Clinical Microbiology; John Wiley & Sons Ltd.: London, UK, 2015; pp. 29–43. ISBN 978-1-68367-280-7. [Google Scholar]
- Sauer, S.; Freiwald, A.; Maier, T.; Kube, M.; Reinhardt, R.; Kostrzewa, M.; Geider, K. Classification and Identification of Bacteria by Mass Spectrometry and Computational Analysis. PLoS ONE 2008, 3, e2843. [Google Scholar] [CrossRef] [Green Version]
- Clark, C.M.; Costa, M.S.; Sanchez, L.M.; Murphy, B.T. Coupling MALDI-TOF Mass Spectrometry Protein and Specialized Metabolite Analyses to Rapidly Discriminate Bacterial Function. Proc. Natl. Acad. Sci. USA 2018, 115, 4981–4986. [Google Scholar] [CrossRef] [Green Version]
- Ilina, E.N.; Borovskaya, A.D.; Serebryakova, M.V.; Chelysheva, V.V.; Momynaliev, K.T.; Maier, T.; Kostrzewa, M.; Govorun, V.M. Application of Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry for the Study of Helicobacter Pylori. Rapid Commun. Mass Spectrom. 2010, 24, 328–334. [Google Scholar] [CrossRef]
- Troncoso, C.; Pavez, M.; Cerda, A.; Oporto, M.; Villarroel, D.; Hofmann, E.; Rios, E.; Sierralta, A.; Copelli, L.; Barrientos, L. MALDI-TOF MS and 16S RNA Identification of Culturable Gastric Microbiota: Variability Associated with the Presence of Helicobacter pylori. Microorganisms 2020, 8, 1763. [Google Scholar] [CrossRef]
- Taniguchi, T.; Sekiya, A.; Higa, M.; Saeki, Y.; Umeki, K.; Okayama, A.; Hayashi, T.; Misawa, N. Rapid Identification and Subtyping of Helicobacter Cinaedi Strains by Intact-Cell Mass Spectrometry Profiling with the Use of Matrix-Assisted Laser Desorption Ionization–Time of Flight Mass Spectrometry. J. Clin. Microbiol. 2014, 52, 95–102. [Google Scholar] [CrossRef] [Green Version]
- Tsuchida, S.; Umemura, H.; Nakayama, T. Current Status of Matrix-Assisted Laser Desorption/Ionization-Time-of-Flight Mass Spectrometry (MALDI-TOF MS) in Clinical Diagnostic Microbiology. Molecules 2020, 25, 4775. [Google Scholar] [CrossRef]
- Faron, M.L.; Buchan, B.W.; Ledeboer, N.A. Matrix-Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry for Use with Positive Blood Cultures: Methodology, Performance, and Optimization. J. Clin. Microbiol. 2017, 55, 3328–3338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishop, B.; Geffen, Y.; Plaut, A.; Kassis, O.; Bitterman, R.; Paul, M.; Neuberger, A. The Use of Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry for Rapid Bacterial Identification in Patients with Smear-Positive Bacterial Meningitis. Clin. Microbiol. Infect. 2018, 24, 171–174. [Google Scholar] [CrossRef] [Green Version]
- Matos, R.; De Witte, C.; Smet, A.; Berlamont, H.; De Bruyckere, S.; Amorim, I.; Gärtner, F.; Haesebrouck, F. Antimicrobial Susceptibility Pattern of Helicobacter Heilmannii and Helicobacter Ailurogastricus Isolates. Microorganisms 2020, 8, 957. [Google Scholar] [CrossRef] [PubMed]
- Balážová, T.; Makovcová, J.; Šedo, O.; Slaný, M.; Faldyna, M.; Zdráhal, Z. The Influence of Culture Conditions on the Identification of Mycobacterium Species by MALDI-TOF MS Profiling. FEMS Microbiol. Lett. 2014, 353, 77–84. [Google Scholar] [CrossRef] [Green Version]
- Fritea, L.; Banica, F.; Costea, T.O.; Moldovan, L.; Iovan, C.; Cavalu, S. A Gold Nanoparticles-Graphene Based Electrochemical Sensor for Sensitive Determination of Nitrazepam. J. Electroanal. Chem. 2018, 830, 63–71. [Google Scholar] [CrossRef]
- Fritea, L.; Banica, F.; Costea, T.O.; Moldovan, L.; Dobjanschi, L.; Muresan, M.; Cavalu, S. Metal Nanoparticles and Carbon-Based Nanomaterials for Improved Performances of Electrochemical (Bio)Sensors with Biomedical Applications. Materials 2021, 14, 6319. [Google Scholar] [CrossRef] [PubMed]
- de la Escosura-Muñiz, A.; Parolo, C.; Merkoçi, A. Immunosensing Using Nanoparticles. Mater. Today 2010, 13, 24–34. [Google Scholar] [CrossRef]
- Shanehsaz, M.; Mohsenifar, A.; Hasannia, S.; Pirooznia, N.; Samaei, Y.; Shamsipur, M. Detection of Helicobacter pylori with a Nanobiosensor Based on Fluorescence Resonance Energy Transfer Using CdTe Quantum Dots. Microchim. Acta 2013, 180. [Google Scholar] [CrossRef]
- Liu, Z.; Tian, C.; Lu, L.; Su, X. A Novel Aptamer-Mediated CuInS2 Quantum Dots@graphene Oxide Nanocomposites-Based Fluorescence “Turn off–on” Nanosensor for Highly Sensitive and Selective Detection of Kanamycin. RSC Adv. 2016, 6, 10205–10214. [Google Scholar] [CrossRef]
- Zheng, Y.; Wang, K.; Zhang, J.; Qin, W.; Yan, X.; Shen, G.; Gao, G.; Pan, F.; Cui, D. Simultaneous Quantitative Detection of Helicobacter pylori Based on a Rapid and Sensitive Testing Platform Using Quantum Dots-Labeled Immunochromatiographic Test Strips. Nanoscale Res. Lett. 2016, 11, 62. [Google Scholar] [CrossRef] [Green Version]
- Shahrashoob, M.; Mohsenifar, A.; Tabatabaei, M.; Rahmani-Cherati, T.; Mobaraki, M.; Mota, A.; Shojaei, T.R. Detection of Helicobacter pylori Genome with an Optical Biosensor Based on Hybridization of Urease Gene with a Gold Nanoparticles-Labeled Probe. J. Appl. Spectrosc. 2016, 83, 322–329. [Google Scholar] [CrossRef]
- Gill, P.; Alvandi, A.-H.; Abdul-Tehrani, H.; Sadeghizadeh, M. Colorimetric Detection of Helicobacter pylori DNA Using Isothermal Helicase-Dependent Amplification and Gold Nanoparticle Probes. Diagn. Microbiol. Infect. Dis. 2008, 62, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Gu, L.; Ma, X.; Tian, X.; Fan, S.; Qin, M.; Lu, J.; Lyu, M.; Wang, S. Rapid Detection of Helicobacter pylori by the Naked Eye Using DNA Aptamers. ACS Omega 2021, 6, 3771–3779. [Google Scholar] [CrossRef] [PubMed]
- Yan, W.; Gu, L.; Ren, W.; Ma, X.; Qin, M.; Lyu, M.; Wang, S. Recognition of Helicobacter pylori by Protein-targeting Aptamers. Helicobacter 2019, 24, 2577. [Google Scholar] [CrossRef]
- Mannoor, M.S.; Tao, H.; Clayton, J.D.; Sengupta, A.; Kaplan, D.L.; Naik, R.R.; Verma, N.; Omenetto, F.G.; McAlpine, M.C. Graphene-Based Wireless Bacteria Detection on Tooth Enamel. Nat. Commun. 2012, 3, 763. [Google Scholar] [CrossRef]
- Su, X.; Li, S. Serological Determination of Helicobacter pylori Infection Using Sandwiched and Enzymatically Amplified Piezoelectric Biosensor. Anal. Chim. Acta 2001, 429, 27–36. [Google Scholar] [CrossRef]
- Kuchmenko, T.; Shuba, A.; Kuchmenko, D.; Umarkhanov, R. Development of a Method for Assessing Helicobacter pylori Activity Based on Exhaled Air Composition with the Use of an Array of Piezoelectric Chemical Sensors. J. Anal. Chem. 2020, 75, 553–562. [Google Scholar] [CrossRef]
- Peng, P. Fabrication of an Electrochemical Sensor for Helicobacter pylori in Excrement Based on a Gold Electrode. Int. J. Electrochem. Sci. 2017, 12, 9478–9487. [Google Scholar] [CrossRef]
- García, T.; Casero, E.; Revenga-Parra, M.; Martín-Benito, J.; Pariente, F.; Vázquez, L.; Lorenzo, E. Architectures Based on the Use of Gold Nanoparticles and Ruthenium Complexes as a New Route to Improve Genosensor Sensitivity. Biosens. Bioelectron. 2008, 24, 184–190. [Google Scholar] [CrossRef]
- Chen, L.-L.; Cui, H.-F.; Fan, S.-F.; Li, Z.-Y.; Han, S.-Y.; Ma, X.; Luo, S.-W.; Song, X.; Lv, Q.-Y. Detection of Helicobacter pylori in Dental Plaque Using a DNA Biosensor for Noninvasive Diagnosis. RSC Adv. 2018, 8, 21075–21083. [Google Scholar] [CrossRef] [Green Version]
- del Pozo, M.V.; Alonso, C.; Pariente, F.; Lorenzo, E. DNA Biosensor for Detection of Helicobacter pylori Using Phen-Dione as the Electrochemically Active Ligand in Osmium Complexes. Anal. Chem. 2005, 77, 2550–2557. [Google Scholar] [CrossRef] [PubMed]
- Revenga-Parra, M.; García, T.; Lorenzo, E.; Pariente, F. Comprehensive Study of Interactions between DNA and New Electroactive Schiff Base Ligands. Application to the Detection of Singly Mismatched Helicobacter pylori Sequences. Biosens. Bioelectron. 2007, 22, 2675–2681. [Google Scholar] [CrossRef]
- Wang, L.; Cui, K.; Wang, P.; Pei, M.; Guo, W. A Sensitive Electrochemical DNA Sensor for Detecting Helicobacter pylori Based on Accordion-like Ti3C2Tx: A Simple Strategy. Anal. Bioanal. Chem. 2021, 413, 4353–4362. [Google Scholar] [CrossRef] [PubMed]
- Ly, S.Y.; Yoo, H.-S.; Choa, S.H. Diagnosis of Helicobacter pylori Bacterial Infections Using a Voltammetric Biosensor. J. Microbiol. Methods 2011, 87, 44–48. [Google Scholar] [CrossRef]
- Song, X.; Lv, M.-M.; Lv, Q.-Y.; Cui, H.-F.; Fu, J.; Huo, Y.-Y. A Novel Assay Strategy Based on Isothermal Amplification and Cascade Signal Amplified Electrochemical DNA Sensor for Sensitive Detection of Helicobacter pylori. Microchem. J. 2021, 166, 106243. [Google Scholar] [CrossRef]
- Hajihosseini, S.; Nasirizadeh, N.; Hejazi, M.S.; Yaghmaei, P. A Sensitive DNA Biosensor Fabricated from Gold Nanoparticles and Graphene Oxide on a Glassy Carbon Electrode. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 61, 506–515. [Google Scholar] [CrossRef]
- Hajihosseini, S.; Nasirizadeh, N.; Hejazi, M.S.; Yaghmaei, P. An Electrochemical DNA Biosensor Based on Oracet Blue as a Label for Detection of Helicobacter pylori. Int. J. Biol. Macromol. 2016, 91, 911–917. [Google Scholar] [CrossRef]
- Chauhan, N.; Gupta, S.; Avasthi, D.K.; Adelung, R.; Mishra, Y.K.; Jain, U. Zinc Oxide Tetrapods Based Biohybrid Interface for Voltammetric Sensing of Helicobacter pylori. ACS Appl. Mater. Interfaces 2018, 10, 30631–30639. [Google Scholar] [CrossRef]
- Jain, U.; Gupta, S.; Soni, S.; Khurana, M.P.; Chauhan, N. Triple-Nanostructuring-Based Noninvasive Electro-Immune Sensing of CagA Toxin for Helicobacter pylori Detection. Helicobacter 2020, 25, e12706. [Google Scholar] [CrossRef]
- Gupta, S.; Tiwari, A.; Jain, U.; Chauhan, N. Synergistic Effect of 2D Material Coated Pt Nanoparticles with PEDOT Polymer on Electrode Surface Interface for a Sensitive Label Free Helicobacter pylori CagA(Ag-Ab) Immunosensing. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 103, 109733. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Jain, U.; Murti, B.T.; Putri, A.D.; Tiwari, A.; Chauhan, N. Nanohybrid-Based Immunosensor Prepared for Helicobacter pylori BabA Antigen Detection through Immobilized Antibody Assembly with @ Pdnano/RGO/PEDOT Sensing Platform. Sci. Rep. 2020, 10, 21217. [Google Scholar] [CrossRef]
- Hubalek, J.; Hradecky, J.; Adam, V.; Krystofova, O.; Huska, D.; Masarik, M.; Trnkova, L.; Horna, A.; Klosova, K.; Adamek, M.; et al. Spectrometric and Voltammetric Analysis of Urease—Nickel Nanoelectrode as an Electrochemical Sensor. Sensors 2007, 7, 1238–1255. [Google Scholar] [CrossRef] [Green Version]
- Cinta-Pinzaru, S.; Cavalu, S.; Leopold, N.; Petry, R.; Kiefer, W. Raman and surface-enhanced Raman spectroscopy of tempyo spin labelled ovalbumin. J. Mol. Struct. 2001, 565, 225–229. [Google Scholar] [CrossRef]
- Gao, H.Y.; Shen, Q.J.; Zhao, X.R.; Yan, X.Q.; Pang, X.; Jin, W.J. Phosphorescent Co-Crystal Assembled by 1,4-Diiodotetrafluorobenzene with Carbazole Based on C–I⋯π Halogen Bonding. J. Mater. Chem. 2012, 22, 5336–5343. [Google Scholar] [CrossRef]
- Nosrati, R.; Golichenari, B.; Nezami, A.; Taghdisi, S.M.; Karimi, B.; Ramezani, M.; Abnous, K.; Shaegh, S.A.M. Helicobacter pylori Point-of-Care Diagnosis: Nano-Scale Biosensors and Microfluidic Systems. TrAC Trends Anal. Chem. 2017, 97, 428–444. [Google Scholar] [CrossRef]
- Zhao, Y.; Xu, D.; Tan, W. Aptamer-Functionalized Nano/Micro-Materials for Clinical Diagnosis: Isolation, Release and Bioanalysis of Circulating Tumor Cells. Integr. Biol. 2017, 9, 188–205. [Google Scholar] [CrossRef]
- Tade, R.S.; Nangare, S.N.; Patil, P.O. Fundamental Aspects of Graphene and Its Biosensing Applications. Funct. Compos. Struct. 2021, 3, 012001. [Google Scholar] [CrossRef]
- Vidic, J.; Manzano, M. Electrochemical Biosensors for Rapid Pathogen Detection. Curr. Opin. Electrochem. 2021, 29, 100750. [Google Scholar] [CrossRef]
- Alonso-Lomillo, M.A.; Domínguez-Renedo, O.; Arcos-Martínez, M.J. Screen-Printed Biosensors in Microbiology—A Review. Talanta 2010, 82, 1629–1636. [Google Scholar] [CrossRef]
- McConnell, E.M.; Morrison, D.; Rey Rincon, M.A.; Salena, B.J.; Li, Y. Selection and Applications of Synthetic Functional DNAs for Bacterial Detection. TrAC Trends Anal. Chem. 2020, 124, 115785. [Google Scholar] [CrossRef]
- Nicholson, B.D.; Abel, L.M.; Turner, P.J.; Price, C.P.; Heneghan, C.; Hayward, G.; Plüddemann, A. Point-of-Care Helicobacter pylori Testing: Primary Care Technology Update. Br. J. Gen. Pract. 2017, 67, 576–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkinson, N.S.S.; Braden, B. Helicobacter pylori Infection: Diagnostic Strategies in Primary Diagnosis and After Therapy. Dig. Dis. Sci. 2016, 61, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Tzianni, E.; Hrbac, J.; Christodoulou, D.; Prodromidis, M. A Portable Medical Diagnostic Device Utilizing Free-Standing Responsive Polymer Film-Based Biosensors and Low-Cost Transducer for Point-of-Care Applications. Sens. Actuat. B Chem. 2019, 304, 127356. [Google Scholar] [CrossRef]
- Saxena, K.; Chauhan, N.; Jain, U. Advances in Diagnosis of Helicobacter pylori through Biosensors: Point of Care Devices. Anal. Biochem 2021, 630, 114325. [Google Scholar] [CrossRef] [PubMed]
- Seo, S.E.; Tabei, F.; Park, S.J.; Askarian, B.; Kim, K.H.; Moallem, G.; Chong, J.W.; Kwon, O.S. Smartphone with Optical, Physical, and Electrochemical Nanobiosensors. J. Ind. Eng. Chem. 2019, 77, 1–11. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Current Diagnostic Methods | Advantages | Disadvantages |
|---|---|---|
| Noninvasive tests | ||
| Urea breath tests C13 and C14 (UBT) |
|
|
| Stool antigen test (SAT) |
|
|
| Serological tests antibody detection |
|
|
| Invasive tests (based on endoscopy) | ||
| Histology |
|
|
| Rapid urease test (RUT) |
|
|
| Culture |
|
|
| PCR |
|
|
| Innovative methods | ||
| MALDI-TOF-MS (Matrix-assisted laser desorption/ionization—time-of-flight—mass spectrometry) |
|
|
| Electrochemical method |
|
|
| Detection Technique | Biosensor Design | Detection Limit | Reference |
|---|---|---|---|
| Fluorescence/FRET (Fluorescence Resonance Energy Transfer) | CdTe Quantum Dots/NH2 and Tamra labeled oligonucleotide, hybridization with H. pylori urease gene | 4.5 × 10−9 M | [92] |
| CuInS2 Quantum dots/modified ssDNA/graphene oxide genosensor | 0.46 pmol·L−1 | [93] | |
| Fluorescence/Lateral flow immunochromatographic assay (LFIA) | Water-soluble Quantum dots-labeled urea-enzyme antibody | 5 mIU/mL | [94] |
| Autofluorescence | Self-assembled glass-immobilized DNA-labeled AuNPs, hybridization with cDNA | 5.10 × 10−10 M | [95] |
| Colorimetric detection | Thermophilic helicase-dependent isothermal amplification (tHDA) and AuNPs | 10 CFU mL−1 | [96] |
| Aptamer-binding fluorescence methods | HPA-2 DNA aptamer with high binding abilities to H. pylori cells | 88 CFU/mL | [97] |
| HP4 Aptamer with high affinity to H. pylori in physiological conditions | 26.48 ± 5.72 nmol/L | [98] | |
| Fluorescence microscopy, electronic detection, wireless | Graphene printed onto water-soluble silk, functionalized with antimicrobial peptides | ~100 H. pylori cells | [99] |
| Piezoelectric array | Sandwiched QCM, enzymatically amplified IgG in H. pylori | Not mentioned | [100] |
| Piezoelectric chemical sensors functionalized with sorbent films, measuring ammonia and carbon dioxide concentrations | Not mentioned | [101] | |
| Electrochemical | β-cyclodextrin (Au electrode) | 0.15 nM | [102] |
| AuNPs/Ruthenium complex (Au electrode) | 25 pM | [103] | |
| AuNPs/Ruthenium complex (Au electrode) | 12 fM | [104] | |
| Osmium complex (Au electrode) | 6 pM | [105] | |
| Schiff ligand (Au electrode) | 8 uM | [106] | |
| Ti3C2Tx + AuNPs (glassy carbon electrode) | 1.6 × 10−16 M | [107] | |
| MWCNTs + Bi (carbon paste electrode) | 0.06 ug/mL | [108] | |
| Au electrode | 34 aM (target DNA) 1.3 pg (HP DNA) | [109] | |
| GO + AuNPs (glassy carbon electrode) | 27 pM | [110] | |
| Au electrode | 0.17 nM | [111] | |
| ZnO tetrapods (Au screen printed electrode) | 0.2 ng/mL | [112] | |
| Polypirlindole carboxylic acid + MWCNTs + TiO2NPs (Au electrode) | 0.1 ng/mL | [113] | |
| rGO + PEDOT + PtNPs | 0.1 ng/mL | [114] | |
| PEDOT + rGO + PdNPs (Au electrode) | 0.2 ng/mL | [115] | |
| Ni nanopillars (Cu sheet fixed on Au pad) | 200 ng/mL (urease) | [116] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardos, A.I.; Maghiar, A.; Zaha, D.C.; Pop, O.; Fritea, L.; Miere, F.; Cavalu, S. Evolution of Diagnostic Methods for Helicobacter pylori Infections: From Traditional Tests to High Technology, Advanced Sensitivity and Discrimination Tools. Diagnostics 2022, 12, 508. https://doi.org/10.3390/diagnostics12020508
Cardos AI, Maghiar A, Zaha DC, Pop O, Fritea L, Miere F, Cavalu S. Evolution of Diagnostic Methods for Helicobacter pylori Infections: From Traditional Tests to High Technology, Advanced Sensitivity and Discrimination Tools. Diagnostics. 2022; 12(2):508. https://doi.org/10.3390/diagnostics12020508
Chicago/Turabian StyleCardos, Alexandra Ioana, Adriana Maghiar, Dana Carmen Zaha, Ovidiu Pop, Luminita Fritea, Florina Miere (Groza), and Simona Cavalu. 2022. "Evolution of Diagnostic Methods for Helicobacter pylori Infections: From Traditional Tests to High Technology, Advanced Sensitivity and Discrimination Tools" Diagnostics 12, no. 2: 508. https://doi.org/10.3390/diagnostics12020508