
Deep Segmentation Networks for Segmenting Kidneys and Detecting Kidney Stones in Unenhanced Abdominal CT Images


Abstract
:1. Introduction
2. Related Work
3. Materials and Methods
3.1. Data Acquisition and Annotations
3.1.1. Data Acquisition
3.1.2. Data Processing
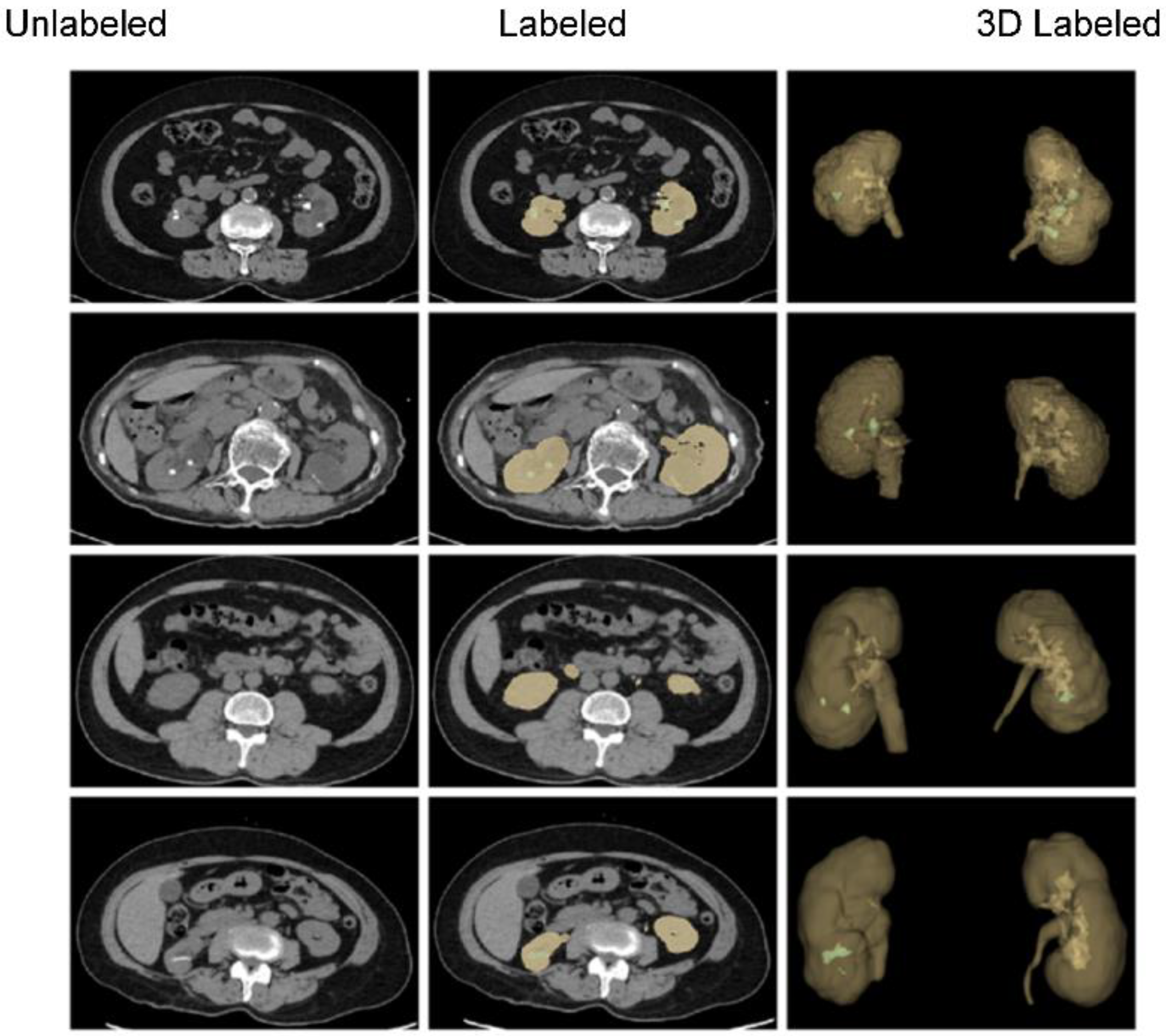
3.1.3. Data Annotations
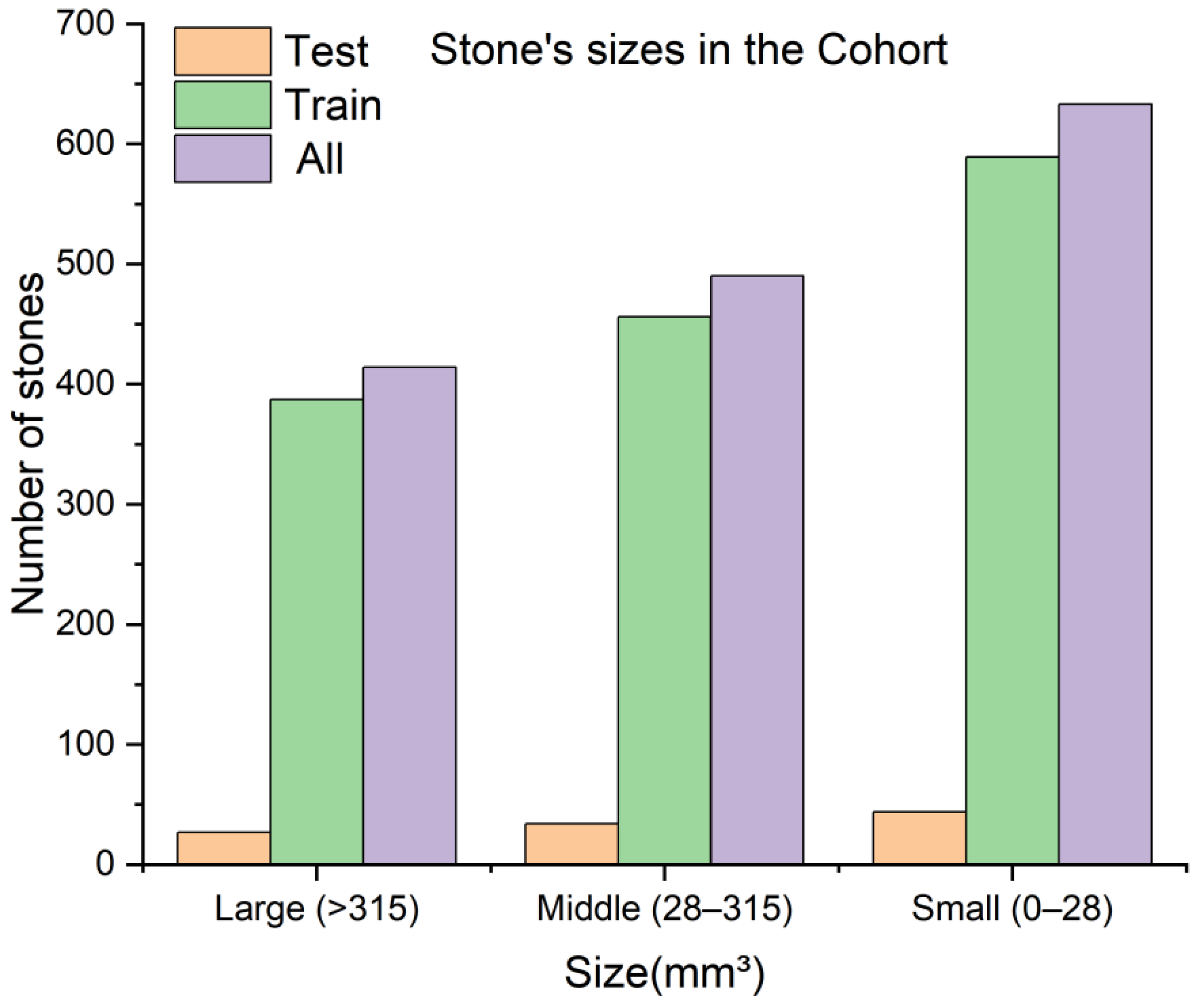
3.1.4. Data Split and Preparation
3.1.5. Data Augmentation
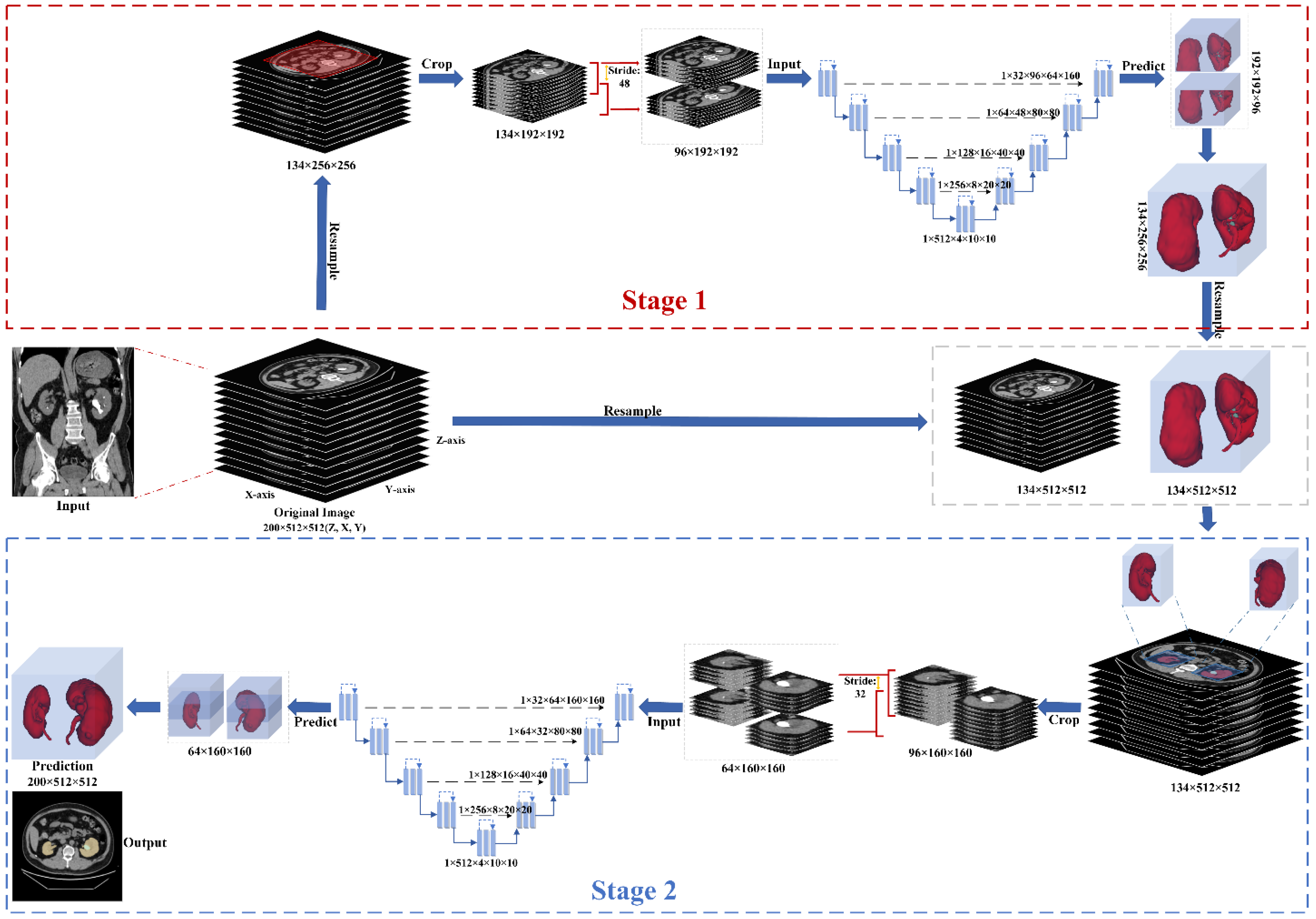
3.2. Proposed Two-Stage Training Scheme
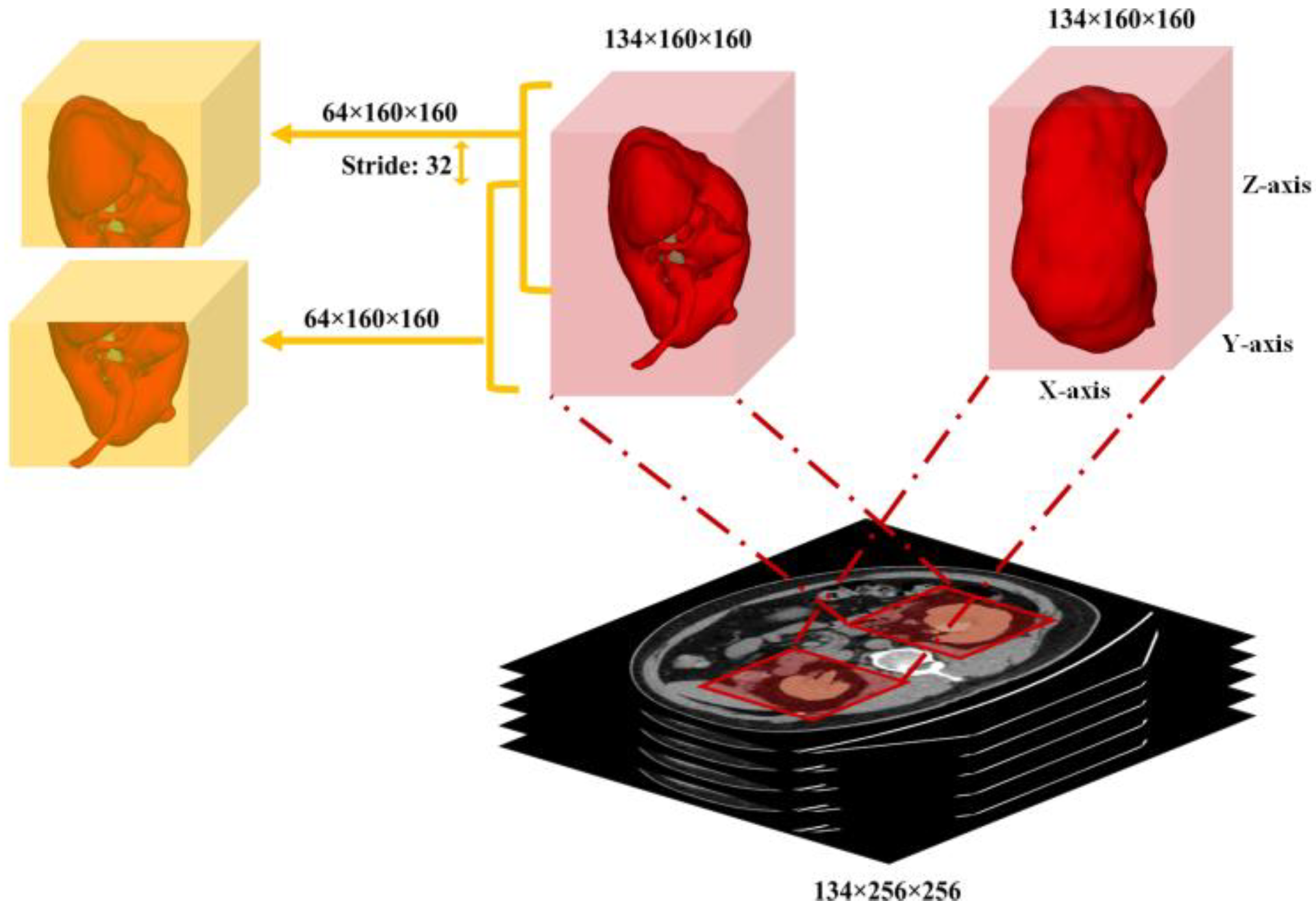
3.2.1. Preprocessing
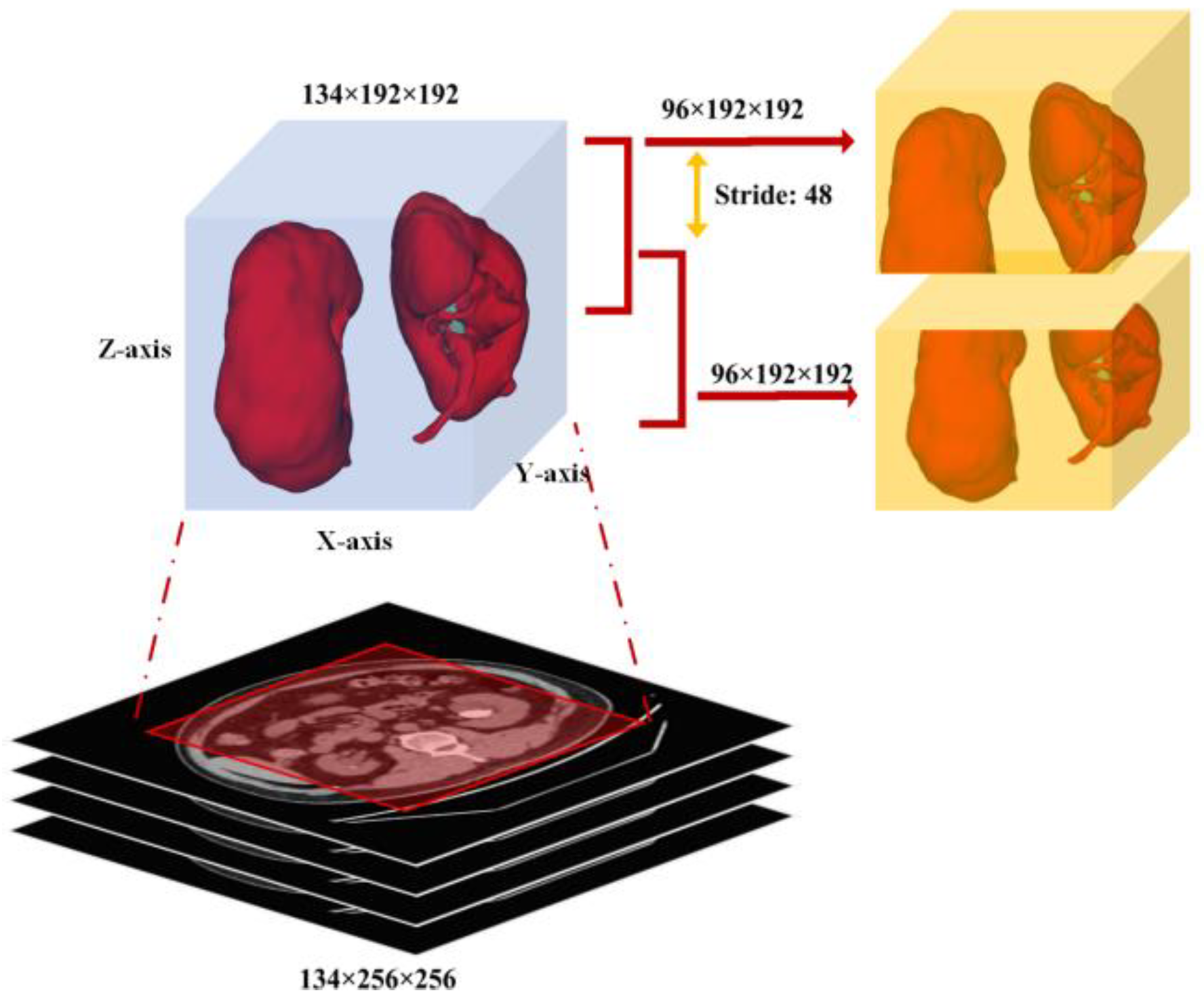
3.2.2. Coarse Kidney Segmentation (Stage 1)
3.2.3. Fine Kidney and Kidney Stone Segmentation (Stage 2)
3.3. Adopted Segmentation Networks
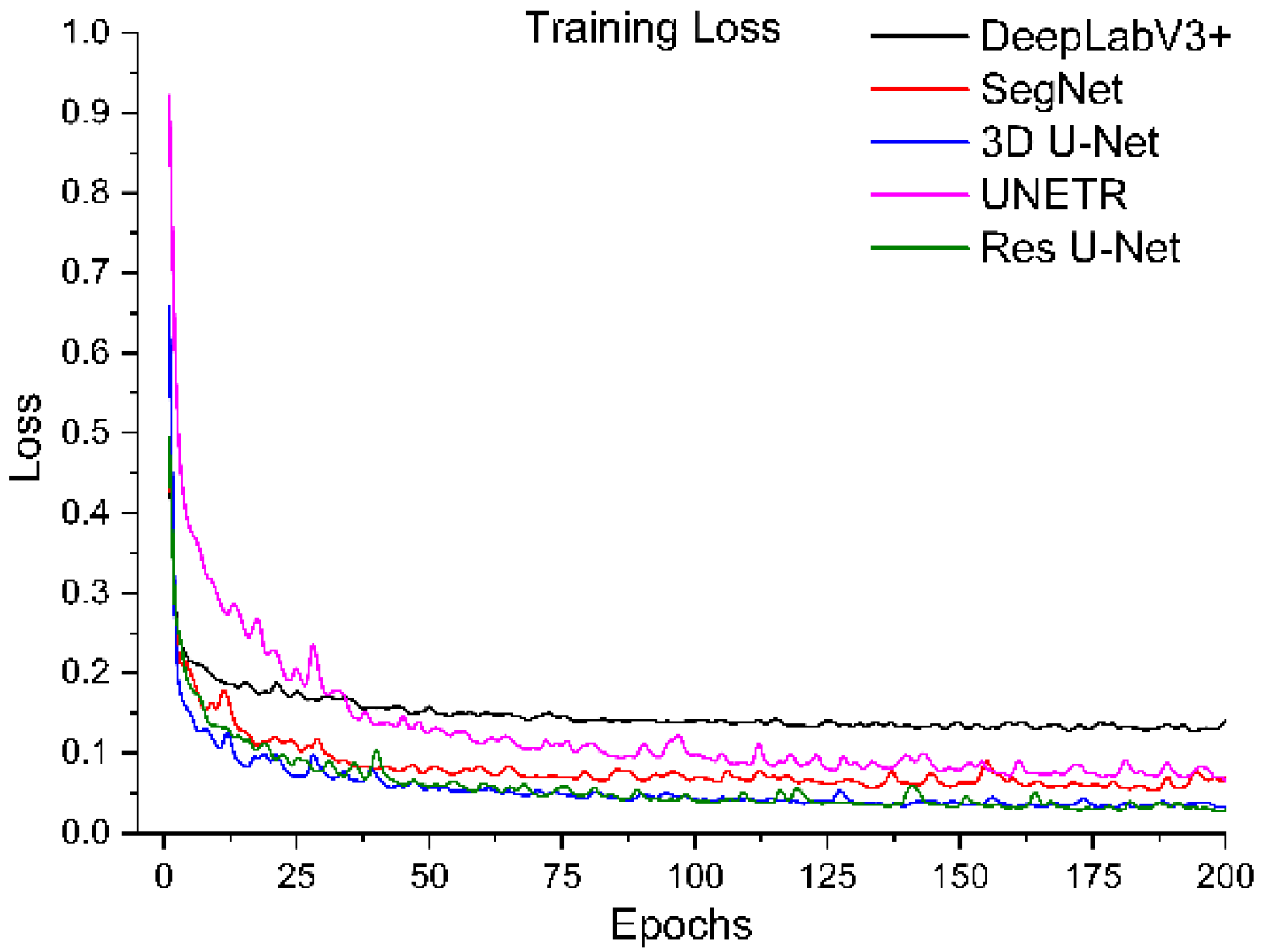
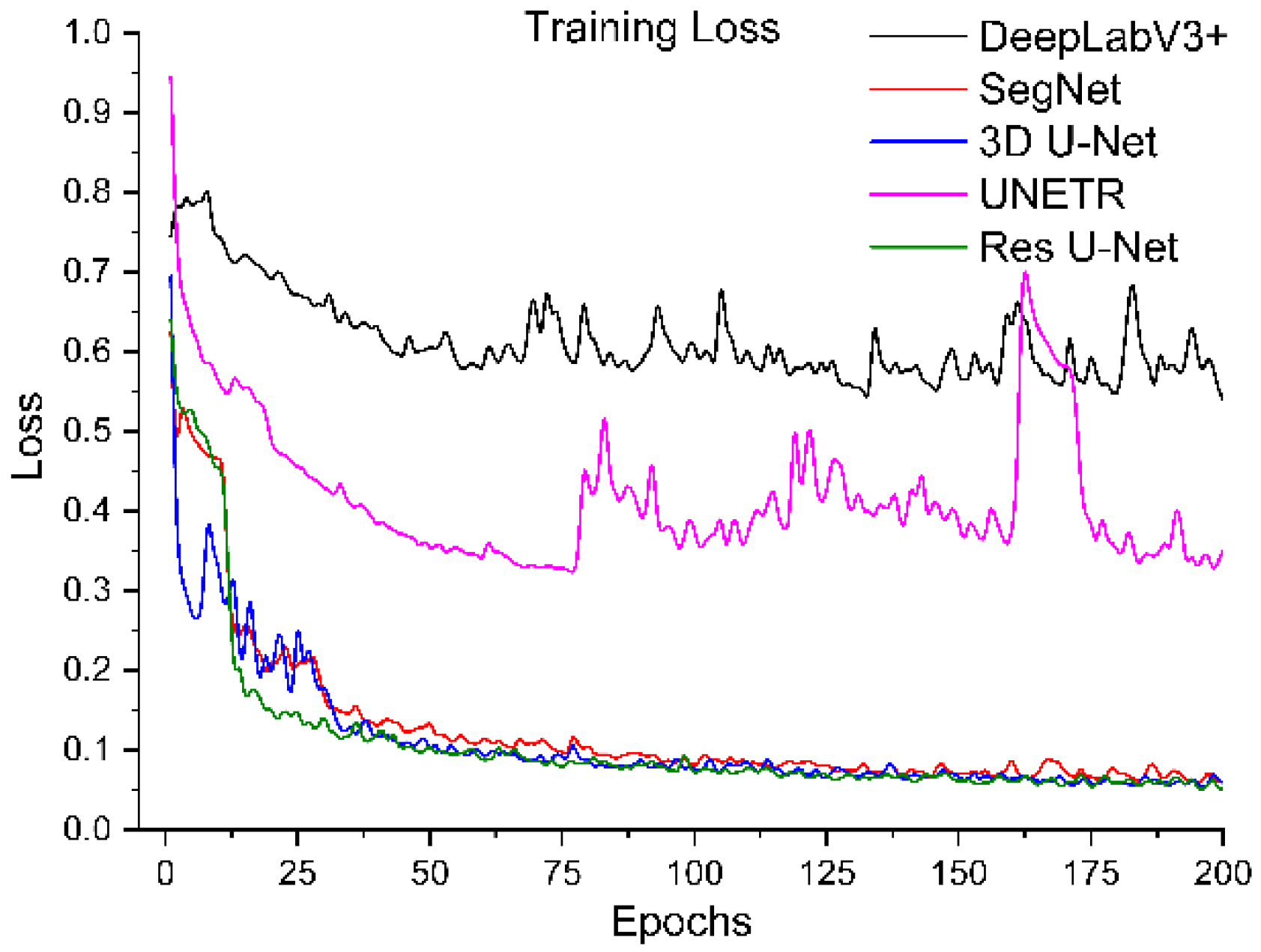
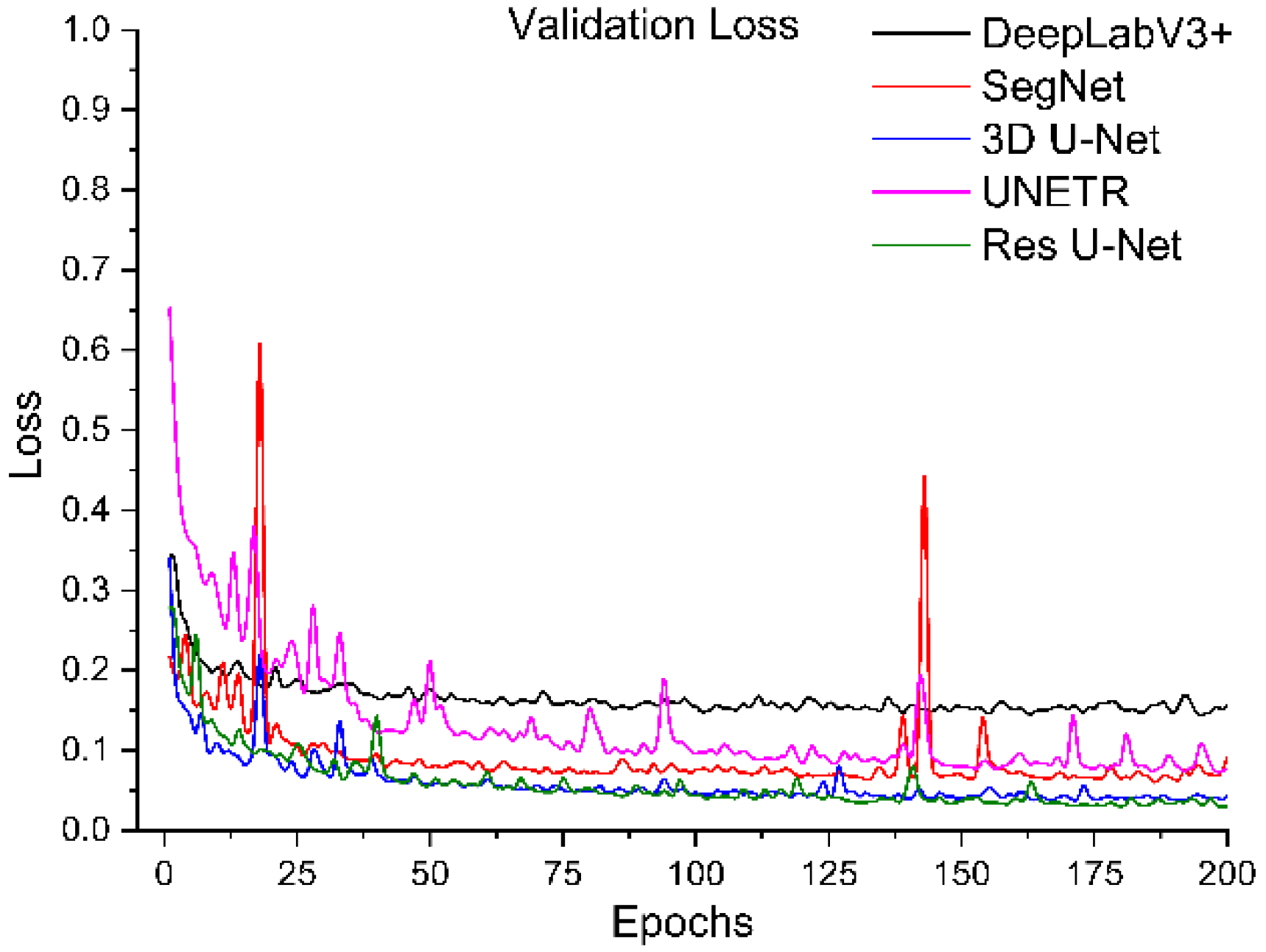
3.4. Segmentation Network Training with Proposed Training Scheme
4. Results and Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yoruk, U.; Hargreaves, B.A.; Vasanawala, S.S. Automatic renal segmentation for MR urography using 3D-GrabCut and random forests. Magn. Reson. Med. 2017, 79, 1696–1707. [Google Scholar] [CrossRef] [PubMed]
- Zisman, A.L.; Evan, A.P.; Coe, F.L.; Worcester, E.M. Do kidney stone formers have a kidney disease? Kidney Int. 2015, 88, 1240–1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, S.R.; Pearle, M.S.; Robertson, W.G.; Gambaro, G.; Canales, B.K.; Doizi, S.; Traxer, O.; Tiselius, H.-H. Kidney stones. Nat. Rev. Dis. Primers 2016, 2, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Parakh, A.; Lee, H.; Lee, J.H.; Eisner, B.H.; Sahani, D.V.; Do, S. Urinary Stone Detection on CT Images Using Deep Convolutional Neural Networks: Evaluation of Model Performance and Generalization. Radiol. Artif. Intell. 2019, 1, e180066. [Google Scholar] [CrossRef]
- Lee, H.; Tajmir, S.; Lee, J.; Zissen, M.; Yeshiwas, B.A.; Alkasab, T.K.; Choy, G.; Do, S. Fully Automated Deep Learning System for Bone Age Assessment. J. Digit. Imaging 2017, 30, 427–441. [Google Scholar] [CrossRef] [Green Version]
- Prevedello, L.M.; Erdal, B.S.; Ryu, J.L.; Little, K.J.; Demirer, M.; Qian, S.; White, R.D. Automated Critical Test Findings Identification and Online Notification System Using Artificial Intelligence in Imaging. Radiology 2017, 285, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Levin, S.; Toerper, M.; Hamrock, E.; Hinson, J.S.; Barnes, S.; Gardner, H.; Dugas, A.; Linton, B.; Kirsch, T.; Kelen, G. Machine-Learning-Based Electronic Triage More Accurately Differentiates Patients with Respect to Clinical Outcomes Compared With the Emergency Severity Index. Ann. Emerg. Med. 2018, 71, 565–574.e2. [Google Scholar] [CrossRef]
- Berlyand, Y.; Raja, A.S.; Dorner, S.C.; Prabhakar, A.M.; Sonis, J.D.; Gottumukkala, R.V.; Succi, M.D.; Yun, B.J. How artificial intelligence could transform emergency department operations. Am. J. Emerg. Med. 2018, 36, 1515–1517. [Google Scholar] [CrossRef]
- Onthoni, D.D.; Sheng, T.-W.; Sahoo, P.K.; Wang, L.-J.; Gupta, P. Deep Learning Assisted Localization of Polycystic Kidney on Contrast-Enhanced CT Images. Diagnostics 2020, 10, 1113. [Google Scholar] [CrossRef]
- Cuingnet, R.; Prevost, D.; Lesage, L.; Cohen, D.; Mory, B.; Ardon, R. Automatic detection and segmentation of kidneys in 3D CT images using random forests. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Nice, France, 1–5 October 2012; pp. 66–74. [Google Scholar]
- Thong, W.; Kadoury, S.; Piché, N.; Pal, C.J. Convolutional networks for kidney segmentation in contrast-enhanced CT scans. Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 2018, 6, 277–282. [Google Scholar] [CrossRef]
- Hao, S.; Zhou, Y.; Guo, Y. A Brief Survey on Semantic Segmentation with Deep Learning. Neurocomputing 2020, 406, 302–321. [Google Scholar] [CrossRef]
- Lateef, F.; Ruichek, Y. Survey on semantic segmentation using deep learning techniques. Neurocomputing 2019, 338, 321–348. [Google Scholar] [CrossRef]
- Simpson, A.L.; Antonelli, M.; Bakas, S.; Bilello, M.; Farahani, K.; van Ginneken, B.; Kopp-Schneider, A.; Landman, B.A.; Litjens, G.; Menze, B.; et al. large annotated medical image dataset for the development and evaluation of segmentation algorithms. arXiv 2019, arXiv:1902.09063. [Google Scholar]
- Greenspan, H.; van Ginneken, B.; Summers, R.M. Guest Editorial Deep Learning in Medical Imaging: Overview and Future Promise of an Exciting New Technique. IEEE Trans. Med. Imaging 2016, 35, 1153–1159. [Google Scholar] [CrossRef]
- Xia, K.-J.; Yin, H.-S.; Zhang, Y.-D. Deep Semantic Segmentation of Kidney and Space-Occupying Lesion Area Based on SCNN and ResNet Models Combined with SIFT-Flow Algorithm. J. Med. Syst. 2019, 43, 1–12. [Google Scholar] [CrossRef]
- Bae, K.; Park, B.; Sun, H.; Wang, J.; Tao, C.; Chapman, A.B.; Torres, V.E.; Grantham, J.J.; Mrug, M.; Bennet, W.M.; et al. Segmentation of individual renal cysts from MR images in patients with autosomal dominant polycystic kidney disease. Clin. J. Am. Soc. Nephrol. 2013, 8, 1089–1097. [Google Scholar] [CrossRef] [Green Version]
- Fu, X.; Liu, H.; Bi, X.; Gong, X. Deep-Learning-Based CT Imaging in the Quantitative Evaluation of Chronic Kidney Diseases. J. Health Eng. 2021, 2021, 3774423. [Google Scholar] [CrossRef]
- Xiang, D.; Bagci, U.; Jin, C.; Shi, F.; Zhu, W.; Yao, J.; Sonka, M.; Chen, X. CorteXpert: A model-based method for automatic renal cortex segmentation. Med. Image Anal. 2017, 42, 257–273. [Google Scholar] [CrossRef]
- Di Leo, G.; Di Terlizzi, F.; Flor, N.; Morganti, A.; Sardanelli, F. Measurement of renal volume using respiratory-gated MRI in subjects without known kidney disease: Intraobserver, interobserver, and interstudy reproducibility. Eur. J. Radiol. 2011, 80, e212–e216. [Google Scholar] [CrossRef]
- Bae, K.T.; Commean, P.K.; Lee, J. Volumetric Measurement of Renal Cysts and Parenchyma Using MRI: Phantoms and Patients with Polycystic Kidney Disease. J. Comput. Assist. Tomogr. 2000, 24, 614–619. [Google Scholar] [CrossRef]
- Daniel, A.J.; Buchanan, C.E.; Allcock, T.; Scerri, D.; Cox, E.F.; Prestwich, B.L.; Francis, S.T. Automated renal segmentation in healthy and chronic kidney disease subjects using a convolutional neural network. Magn. Reson. Med. 2021, 86, 1125–1136. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, D.K.; Xi, Y.; Kapur, P.; Madhuranthakam, A.J.; Lewis, M.A.; Udayakumar, D.; Rasmussen, R.; Yuan, Q.; Bagrodia, A.; Margulis, V.; et al. Magnetic Resonance Imaging Radiomics Analyses for Prediction of High-Grade Histology and Necrosis in Clear Cell Renal Cell Carcinoma: Preliminary Experience. Clin. Genitourin. Cancer 2021, 19, 12–21.e1. [Google Scholar] [CrossRef] [PubMed]
- Souza, J.C.; Diniz, J.O.B.; Ferreira, J.L.; da Silva, G.L.F.; Silva, A.C.; de Paiva, A.C. An automatic method for lung segmentation and reconstruction in chest X-ray using deep neural networks. Comput. Methods Programs Biomed. 2019, 177, 285–296. [Google Scholar] [CrossRef] [PubMed]
- Hatt, M.; Laurent, B.; Ouahabi, A.; Fayad, H.; Tan, S.; Li, L.; Lu, W.; Jaouen, V.; Tauber, C.; Czakon, J.; et al. The first MICCAI challenge on PET tumor segmentation. Med. Image Anal. 2018, 44, 177–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goyal, M.; Oakley, A.; Bansal, P.; Dancey, D.; Yap, M.H. Skin Lesion Segmentation in Dermoscopic Images with Ensemble Deep Learning Methods. IEEE Access 2019, 8, 4171–4181. [Google Scholar] [CrossRef]
- Akkus, Z.; Galimzianova, A.; Hoogi, A.; Rubin, D.L.; Erickson, B.J. Deep Learning for Brain MRI Segmentation: State of the Art and Future Directions. J. Digit. Imaging 2017, 30, 449–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yap, M.H.; Goyal, M.; Osman, F.; Martí, R.; Denton, E.; Juette, A.; Zwiggelaar, R. Breast ultrasound region of interest detection and lesion localisation. Artif. Intell. Med. 2020, 107, 101880. [Google Scholar] [CrossRef]
- Goyal, M.; Guo, J.; Hinojosa, L.; Hulsey, K.; Pedrosa, I. Automated kidney segmentation by mask R-CNN in T2-weighted magnetic resonance imaging. arXiv 2022, arXiv:2108.12506. [Google Scholar] [CrossRef]
- He, K.; Gkioxari, G.; Dollár, P.; Girshick, R. Mask r-cnn. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 29 October 2017; pp. 2961–2969. [Google Scholar]
- Kline, T.L.; Edwards, M.E.; Fetzer, J.; Gregory, A.V.; Annam, D.; Metzger, A.J.; Erickson, B.J. Automatic semantic segmentation of kidney cysts in MR images of patients affected by autosomal-dominant polycystic kidney disease. Abdom. Radiol. 2021, 46, 1053–1061. [Google Scholar] [CrossRef]
- Xiong, X.; Guo, Y.; Wang, Y.; Zhang, D.; Ye, Z.; Zhang, S.; Xin, X. Kidney tumor segmentation in ultrasound images using adaptive sub-regional evolution level set models. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi= J. Biomed. Eng. = Shengwu Yixue Gongchengxue Zazhi 2019, 36, 945–956. [Google Scholar]
- Will, S.; Martirosian, P.; Würslin, C.; Schick, F. Automated segmentation and volumetric analysis of renal cortex, medulla, and pelvis based on non-contrast-enhanced T1-and T2-weighted MR images. Magn. Reson. Mater. Phys. Biol. Med. 2014, 27, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Jiang, Y.; Tsui, H.-T. Segmentation of kidney from ultrasound images based on texture and shape priors. IEEE Trans. Med. Imaging 2005, 24, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Yang, X.; Chen, Y.; Tang, L. Ultrasound kidney segmentation with a global prior shape. J. Vis. Commun. Image Represent. 2013, 24, 937–943. [Google Scholar] [CrossRef]
- Yin, S.; Zhang, Z.; Li, H.; Peng, Q.; You, X.; Furth, S.L.; Tasian, G.E.; Fan, Y. Fully-Automatic Segmentation Of Kidneys In Clinical Ultrasound Images Using A Boundary Distance Regression Network. In Proceedings of the 16th International Symposium on Biomedical Imaging (ISBI 2019), Venice, Italy, 8–11 April 2019; pp. 1741–1744. [Google Scholar] [CrossRef]
- Torres, H.R.; Queiros, S.; Morais, P.; Oliveira, B.; Gomes-Fonseca, J.; Mota, P.; Lima, E.; D’Hooge, J.; Fonseca, J.C.; Vilaca, J.L. Kidney Segmentation in 3-D Ultrasound Images Using a Fast Phase-Based Approach. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2020, 68, 1521–1531. [Google Scholar] [CrossRef]
- Yin, S.; Peng, Q.; Li, H.; Zhang, Z.; You, X.; Fischer, K.; Furth, S.L.; Tasian, G.E.; Fan, Y. Automatic kidney segmentation in ultrasound images using subsequent boundary distance regression and pixelwise classification networks. Med. Image Anal. 2020, 60, 101602. [Google Scholar] [CrossRef]
- Goel, R.; Jain, A. Improved Detection of Kidney Stone in Ultrasound Images Using Segmentation Techniques. In Advances in Data and Information Sciences; Springer: Cham, Switzerland, 2020; pp. 623–641. [Google Scholar] [CrossRef]
- Spiegel, M.; Hahn, D.A.; Daum, V.; Wasza, J.; Hornegger, J. Segmentation of kidneys using a new active shape model generation technique based on non-rigid image registration. Comput. Med Imaging Graph. 2009, 33, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Khalifa, F.; Elnakib, A.; Beache, G.M.; Gimel’Farb, G.; El-Ghar, M.A.; Ouseph, R.; Sokhadze, G.; Manning, S.; McClure, P.; El-Baz, A. 3D Kidney Segmentation from CT Images Using a Level Set Approach Guided by a Novel Stochastic Speed Function. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Cham, Switzerland, 2011; Volume 14, pp. 587–594. [Google Scholar] [CrossRef] [Green Version]
- Cha, K.; Hadjiiski, L.; Samala, R.; Chan, H.-P.; Caoili, E.M.; Cohan, R.H. Urinary bladder segmentation in CT urography using deep-learning convolutional neural network and level sets. Med. Phys. 2016, 43, 1882–1896. [Google Scholar] [CrossRef]
- Zhao, W.; Jiang, D.; Queralta, J.P.; Westerlund, T. MSS U-Net: 3D segmentation of kidneys and tumors from CT images with a multi-scale supervised U-Net. Inform. Med. Unlocked 2020, 19, 100357. [Google Scholar] [CrossRef]
- Taha, A.; Lo, P.; Li, J.; Zhao, T. Kid-net: Convolution networks for kidney vessels segmentation from ct-volumes. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Cham, Switzerland, 2018; pp. 463–471. [Google Scholar]
- Elton, D.C.; Turkbey, E.B.; Pickhardt, P.J.; Summers, R.M. A deep learning system for automated kidney stone detection and volumetric segmentation on noncontrast CT scans. Med. Phys. 2022, 49, 2545–2554. [Google Scholar] [CrossRef]
- Heller, N.; Sathianathen, N.; Kalapara, A.; Walczak, E.; Moore, K.; Kaluzniak, H.; Rosenberg, J.; Blake, P.; Rengel, Z.; Oestreich, M.; et al. The kits19 challenge data: 300 kidney tumor cases with clinical context, ct semantic segmentations, and surgical outcomes. arXiv 2019, arXiv:1904.00445. [Google Scholar]
- D Slicer Image Computing Platform. Available online: https://www.slicer.org/ (accessed on 29 June 2020).
- Içek, A.; Abdulkadir, S.; Lienkamp, S.; Brox, T.; Ronneberger, O. 3D U-Net: Learning dense volumetric segmentation from sparse annotation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Athens, Greece, 17–21 October 2016; pp. 424–432. [Google Scholar]
- Zhang, Z.; Liu, Q.; Wang, Y. Road extraction by deep residual u-net. IEEE Geosci. Remote Sens. Lett. 2018, 15, 749–753. [Google Scholar] [CrossRef] [Green Version]
- Badrinarayanan, V.; Kendall, A.; Cipolla, R. Segnet: A deep convolutional encoder-decoder architecture for image segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 2481–2495. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-C.; Zhu, Y.; Papandreou, G.; Schroff, F.; Adam, F. Encoder-decoder with atrous separable convolution for semantic image segmentation. In Proceedings of the European Conference on Computer Vision (ECCV), Munich, Germany, 8–14 September 2018; pp. 801–818. [Google Scholar]
- Hatamizadeh, A.; Tang, Y.; Nath, V.; Tang, D.; Myronenko, A.; Landman, B.; Roth, H.R.; Xu, D. UNETR: Transformers for 3d medical image segmentation. In Proceedings of the IEEE/CVF Winter Conference on Applications of Computer Vision, 3–8 January 2022; pp. 574–584. [Google Scholar]
- Isensee, F.; Jaeger, P.F.; Kohl, S.A.; Petersen, J.; Maier-Hein, K.H. nnU-Net: A self-configuring method for deep learning-based biomedical image segmentation. Nat. Methods 2021, 18, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Chen, Z.; Hassan, H.; Xie, W.; Huang, B. A Cascaded 3D Segmentation Model for Renal Enhanced CT Images. In Kidney and Kidney Tumor Segmentation. KiTS 2021; Lecture Notes in Computer Science, vol 13168; Springer: Cham, Switzerland, 2022; pp. 123–168. [Google Scholar] [CrossRef]
- Xiao, C.; Hassan, H.; Huang, B. Contrast-Enhanced CT Renal Tumor Segmentation. In Kidney and Kidney Tumor Segmentation. KiTS 2021; Lecture Notes in Computer Science, vol 13168; Springer: Cham, Switzerland, 2022; pp. 116–122. [Google Scholar] [CrossRef]
- Chollet, F. Xception: Deep learning with depthwise separable convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21 July 2017; pp. 1251–1258. [Google Scholar]
- Loshchilov, I.; Hutter, F. Fixing weight decay regularization in adam. arXiv 2018, arXiv:1711.05101v3. [Google Scholar]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Network | Kidney (Mean ± Std) | Kidney Stone (Mean ± Std) | ||||
|---|---|---|---|---|---|---|
| Dice | Specificity | Sensitivity | Dice | Specificity | Sensitivity | |
| SegNet | 95.04 ± 1.18% | 99.96 ± 0.02% | 95.69 ± 0.94% | 75.59 ± 2.23% | 99.96 ± 0.01% | 73.43 ± 1.18% |
| DeepLabV3+ | 81.73 ± 2.43% | 99.89 ± 0.02% | 82.52 ± 2.50% | 33.36 ± 3.17% | 99.96 ± 0.01% | 35.61 ± 3.28% |
| 3D U-Net | 96.05 ± 1.68% | 99.98 ± 0.01% | 96.05 ± 0.18% | 80.04 ± 1.75% | 99.98 ± 0.01% | 80.21 ± 1.81% |
| UNETR | 93.35 ± 1.45% | 99.97 ± 0.01% | 93.09 ± 0.82% | 74.36 ± 0.80% | 99.96 ± 0.01% | 76.26 ± 2.78% |
| Res U-Net | 96.54 ± 1.06% | 99.99 ± 0.01% | 96.49 ± 0.08% | 80.59 ± 1.28% | 99.99 ± 0.01% | 79.73 ± 1.90% |
| Network | Kidney Stone Dice | Kidney Dice | Specificity | Sensitivity | Accuracy |
|---|---|---|---|---|---|
| SegNet | 75.42% | 95.50% | 99.96% | 97.50% | 99.94% |
| DeepLabV3+ | 41.09% | 65.56% | 99.75% | 70.91% | 99.59% |
| 3D U-Net | 77.63% | 96.70% | 99.97% | 97.20% | 99.96% |
| UNETR | 61.92% | 77.14% | 99.82% | 82.02% | 99.72% |
| Res U-Net | 79.83% | 95.81% | 99.97% | 96.61% | 99.95% |
| Network | Kidney Stone Dice (Mean ± Std) | ||
|---|---|---|---|
| Small | Middle | Large | |
| SegNet | 34.38 ± 1.67 | 74.76 ± 2.86 | 80.86 ± 4.51 |
| DeepLabV3+ | \ | 5.61 ± 2.48 | 47.42 ± 2.70 |
| 3D U-Net | 58.03 ± 1.42 | 81.56 ± 1.99 | 82.86 ± 3.52 |
| UNETR | 52.49 ± 2.13 | 76.54 ± 2.20 | 76.38 ± 1.85 |
| Res U-Net | 60.11 ± 0.84 | 76.08 ± 3.46 | 83.39 ± 2.33 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, D.; Xiao, C.; Liu, Y.; Chen, Z.; Hassan, H.; Su, L.; Liu, J.; Li, H.; Xie, W.; Zhong, W.; et al. Deep Segmentation Networks for Segmenting Kidneys and Detecting Kidney Stones in Unenhanced Abdominal CT Images. Diagnostics 2022, 12, 1788. https://doi.org/10.3390/diagnostics12081788
Li D, Xiao C, Liu Y, Chen Z, Hassan H, Su L, Liu J, Li H, Xie W, Zhong W, et al. Deep Segmentation Networks for Segmenting Kidneys and Detecting Kidney Stones in Unenhanced Abdominal CT Images. Diagnostics. 2022; 12(8):1788. https://doi.org/10.3390/diagnostics12081788
Chicago/Turabian StyleLi, Dan, Chuda Xiao, Yang Liu, Zhuo Chen, Haseeb Hassan, Liyilei Su, Jun Liu, Haoyu Li, Weiguo Xie, Wen Zhong, and et al. 2022. "Deep Segmentation Networks for Segmenting Kidneys and Detecting Kidney Stones in Unenhanced Abdominal CT Images" Diagnostics 12, no. 8: 1788. https://doi.org/10.3390/diagnostics12081788