
A Deep Feature Fusion of Improved Suspected Keratoconus Detection with Deep Learning
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
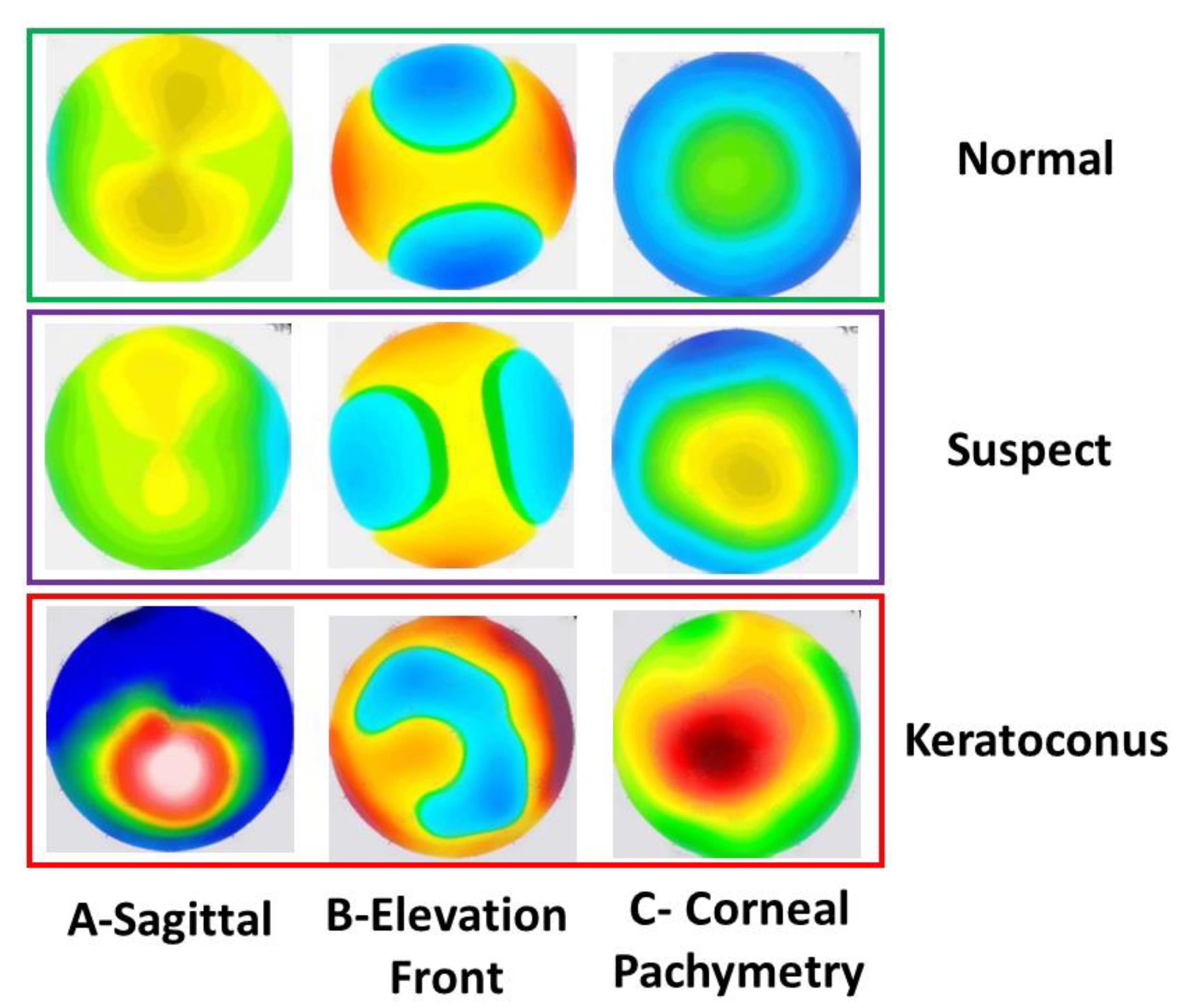
2.1. Datasets
2.2. Image Dataset Preprocessing Pipeline
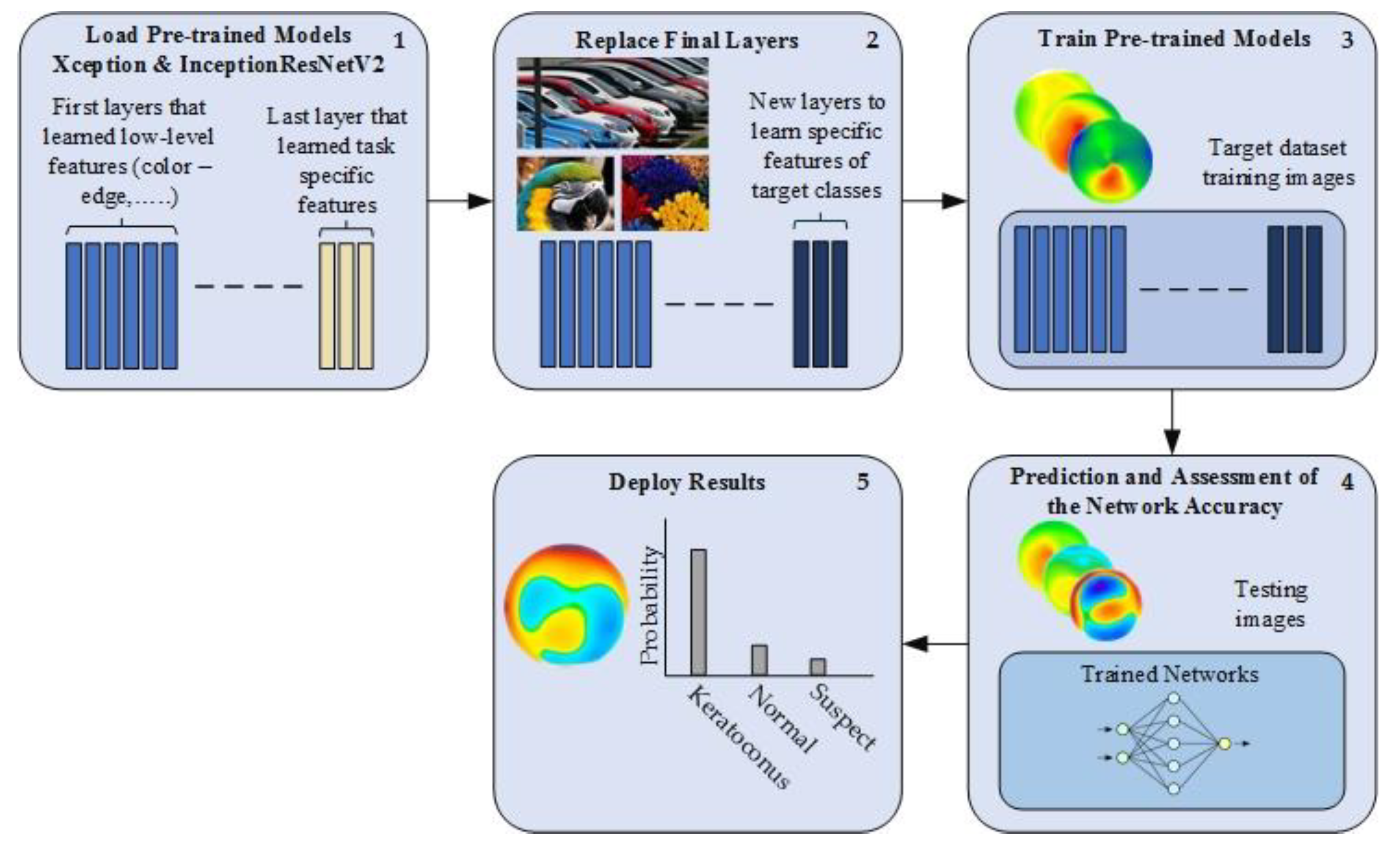
2.3. Deep Transfer Learning
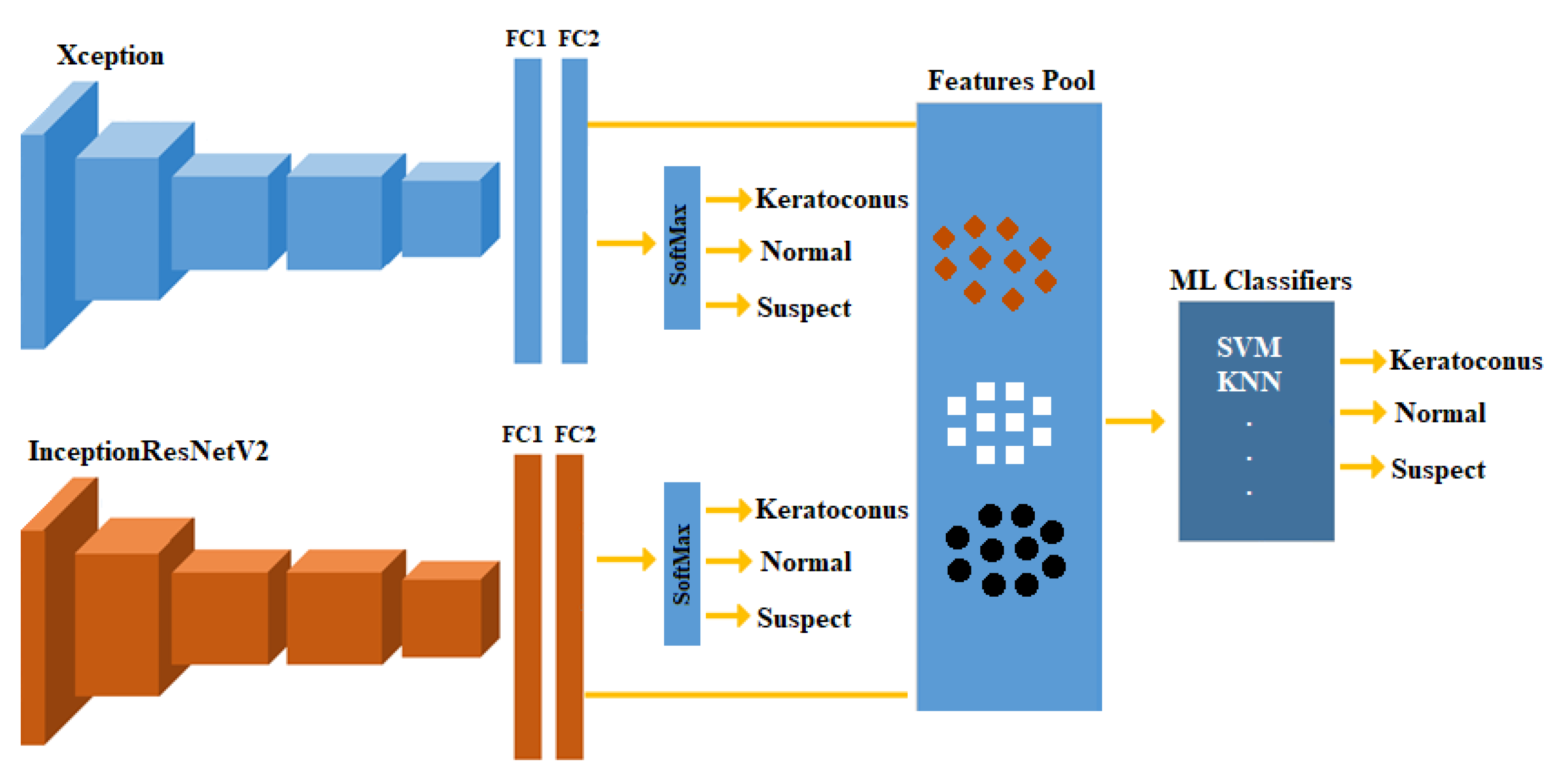
2.4. Feature Fusion and ML Classifiers
2.5. Training the DL Models
- Scenario 1 (S1—2-class): training the models with two classes of normal and KCN.
- Scenario 2 (S2—3-class): training the models with three classes of normal, suspect, and KCN.
2.6. Performance Evaluation
3. Results
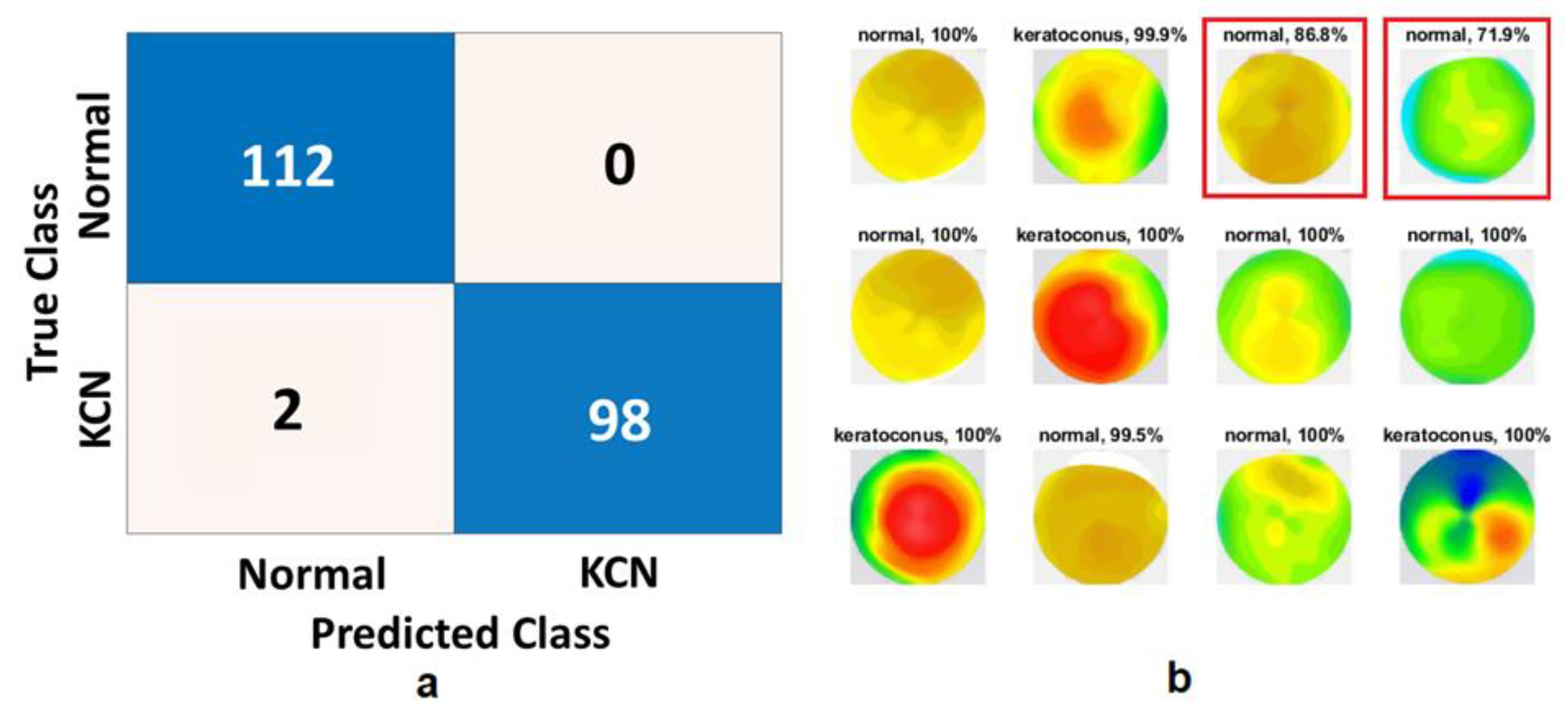
3.1. Scenario 1: 2-Class Problem (Normal and KCN)
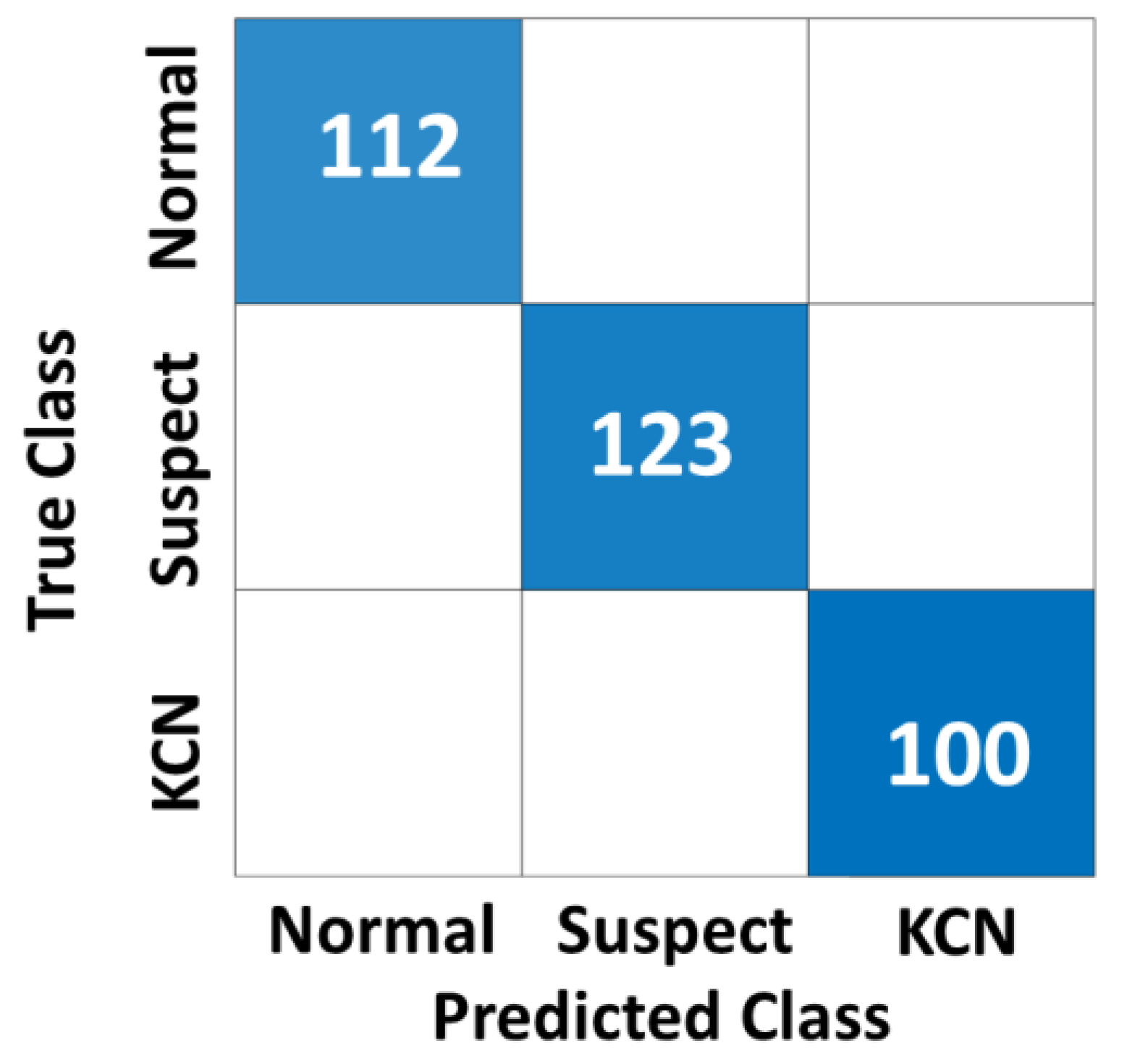
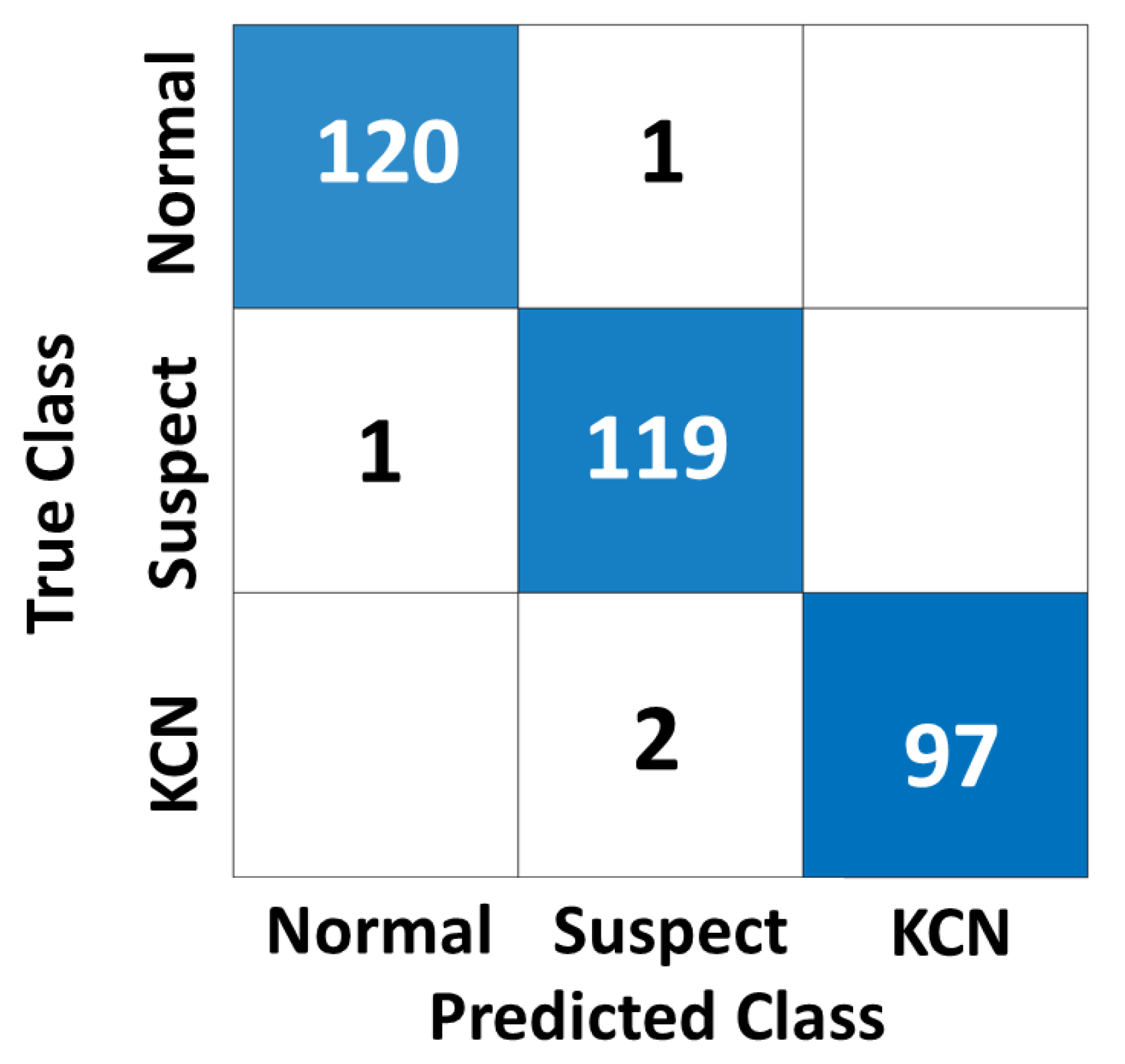
3.2. Scenario 2: 3-Class Problem (Normal, Suspect, and KCN)
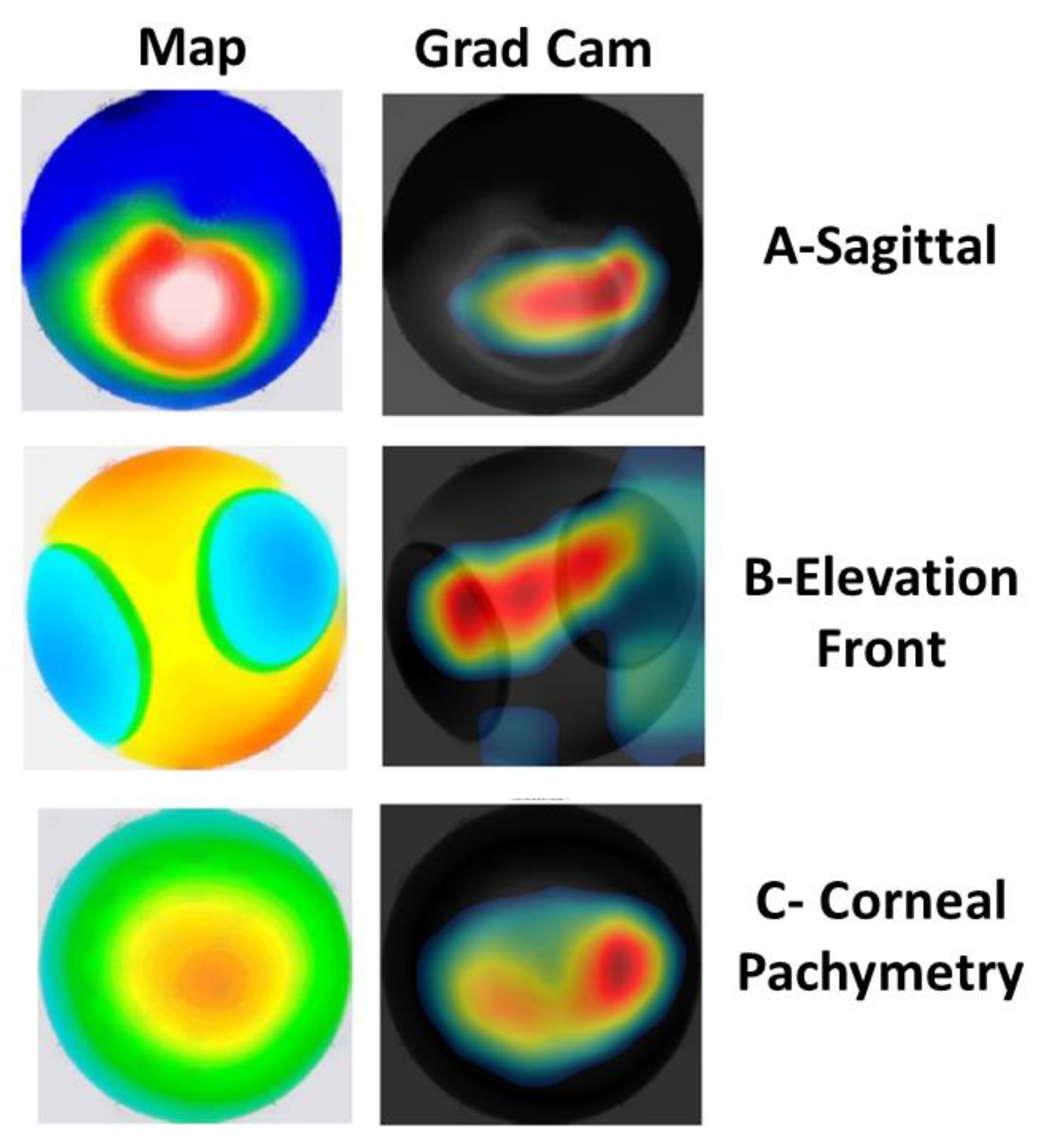
3.3. Visualization of the CAMs
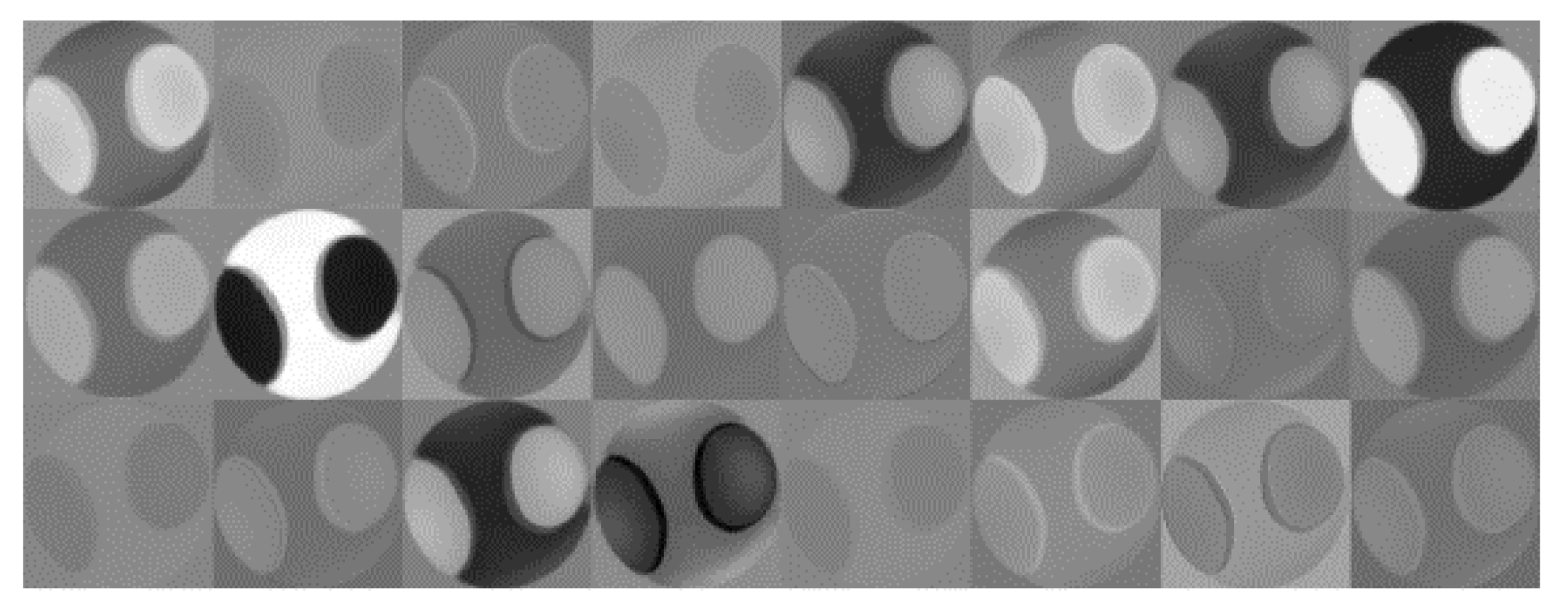
3.4. Features Extracted by the Xception Model
3.5. Validating the Models Based on an Independent Dataset from Iraq
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yousefi, S.; Yousefi, E.; Takahashi, H.; Hayashi, T.; Tampo, H.; Inoda, S.; Arai, Y.; Asbell, P. Keratoconus severity identification using unsupervised machine learning. PLoS ONE 2018, 13, e0205998. [Google Scholar] [CrossRef] [PubMed]
- Al-Timemy, A.H.; Ghaeb, N.H.; Mosa, Z.M.; Escudero, J. Deep Transfer Learning for Improved Detection of Keratoconus using Corneal Topographic Maps. Cognit. Comput. 2021, 14, 1627–1642. [Google Scholar] [CrossRef]
- Al-Timemy, A.; Al-Zubaidi, L.; Ghaeb, N.; Takahashi, H.; Lavric, A.; Mosa, Z.; Hazarbassanov, R.M.; Alyasseri, Z.A.A.; Yousefi, S. A device-agnostic deep learning model for detecting keratoconus based on anterior elevation corneal maps. Investig. Ophthalmol. Vis. Sci. 2022, 63, 2101-F0090. [Google Scholar]
- Alyasseri, Z.A.A.; Al-Timemy, A.H.; Abasi, A.K.; Lavric, A.; Mohammed, H.J.; Takahashi, H.; Milhomens Filho, J.A.; Campos, M.; Hazarbassanov, R.M.; Yousefi, S. A Hybrid Artificial Intelligence Model for Detecting Keratoconus. Appl. Sci. 2022, 12, 12979. [Google Scholar] [CrossRef]
- Lavric, A.; Popa, V.; Takahashi, H.; Yousefi, S. Detecting Keratoconus From Corneal Imaging Data Using Machine Learning. IEEE Access 2020, 8, 149113–149121. [Google Scholar] [CrossRef]
- Twa, M.D.; Parthasarathy, S.; Roberts, C.; Mahmoud, A.M.; Raasch, T.W.; Bullimore, M.A. Automated decision tree classification of corneal shape. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2005, 82, 1038. [Google Scholar] [CrossRef] [PubMed]
- Maeda, N.; Klyce, S.D.; Smolek, M.K. Neural Network Classification of Corneal Topography Preliminary Demonstration. Investig. Ophthalmol. Vis. Sci. 1995, 36, 1327–1335. [Google Scholar]
- Mosa, Z.M.; Ghaeb, N.H.; Ali, A.H. Detecting Keratoconus by Using SVM and Decision Tree Classifiers with the Aid of Image Processing. Baghdad Sci. J. 2019, 16, 4. [Google Scholar]
- Kamiya, K.; Ayatsuka, Y.; Kato, Y.; Shoji, N.; Mori, Y.; Miyata, K. Diagnosability of keratoconus using deep learning with Placido disk-based corneal topography. Front. Med. 2021, 8, 724902. [Google Scholar] [CrossRef]
- Reddy, J.C.; Bhamidipati, P.; Dwivedi, S.; Dhara, K.K.; Joshi, V.; Hasnat Ali, M.; Vaddavalli, P.K. KEDOP: Keratoconus early detection of progression using tomography images. Eur. J. Ophthalmol. 2022, 32, 2554–2564. [Google Scholar] [CrossRef]
- Alzubaidi, L.; Bai, J.; Al-Sabaawi, A.; Santamaría, J.; Albahri, A.S.; Al-dabbagh, B.S.N.; Fadhel, M.A.; Manoufali, M.; Zhang, J.; Al-Timemy, A.H. A survey on deep learning tools dealing with data scarcity: Definitions, challenges, solutions, tips, and applications. J. Big Data 2023, 10, 1–82. [Google Scholar]
- Albahri, A.S.; Duhaim, A.M.; Fadhel, M.A.; Alnoor, A.; Baqer, N.S.; Alzubaidi, L.; Albahri, O.S.; Alamoodi, A.H.; Bai, J.; Salhi, A. A systematic review of trustworthy and explainable artificial intelligence in healthcare: Assessment of quality, bias risk, and data fusion. Inf. Fusion 2023, 96, 156–191. [Google Scholar] [CrossRef]
- Kuo, B.-I.; Chang, W.-Y.; Liao, T.-S.; Liu, F.-Y.; Liu, H.-Y.; Chu, H.-S.; Chen, W.-L.; Hu, F.-R.; Yen, J.-Y.; Wang, I.-J. Keratoconus screening based on deep learning approach of corneal topography. Transl. Vis. Sci. Technol. 2020, 9, 53. [Google Scholar] [CrossRef] [PubMed]
- Abdelmotaal, H.; Mostafa, M.M.; Mostafa, A.N.R.; Mohamed, A.A.; Abdelazeem, K. Classification of color-coded Scheimpflug camera corneal tomography images using deep learning. Transl. Vis. Sci. Technol. 2020, 9, 30. [Google Scholar] [CrossRef] [PubMed]
- Zéboulon, P.; Debellemanière, G.; Bouvet, M.; Gatinel, D. Corneal topography raw data classification using a convolutional neural network. Am. J. Ophthalmol. 2020, 219, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Feng, R.; Xu, Z.; Zheng, X.; Hu, H.; Jin, X.; Chen, D.Z.; Yao, K.; Wu, J. KerNet: A novel deep learning approach for keratoconus and sub-clinical keratoconus detection based on raw data of the Pentacam HR system. IEEE J. Biomed. Heal. Informatics 2021, 25, 3898–3910. [Google Scholar] [CrossRef]
- Fassbind, B.; Langenbucher, A.; Streich, A. Automated cornea diagnosis using deep convolutional neural networks based on cornea topography maps. Sci. Rep. 2023, 13, 6566. [Google Scholar] [CrossRef]
- Kamiya, K.; Ayatsuka, Y.; Kato, Y.; Shoji, N.; Miyai, T.; Ishii, H.; Mori, Y.; Miyata, K. Prediction of keratoconus progression using deep learning of anterior segment optical coherence tomography maps. Ann. Transl. Med. 2021, 9, 1287. [Google Scholar] [CrossRef]
- Chen, X.; Zhao, J.; Iselin, K.C.; Borroni, D.; Romano, D.; Gokul, A.; McGhee, C.N.J.; Zhao, Y.; Sedaghat, M.-R.; Momeni-Moghaddam, H. Keratoconus detection of changes using deep learning of colour-coded maps. BMJ Open Ophthalmol. 2021, 6, e000824. [Google Scholar] [CrossRef]
- Lavric, A.; Valentin, P. KeratoDetect: Keratoconus Detection Algorithm Using Convolutional Neural Networks. Comput. Intell. Neurosci. 2019, 2019, 8162567. [Google Scholar] [CrossRef]
- Maile, H.; Li, J.-P.O.; Gore, D.; Leucci, M.; Mulholland, P.; Hau, S.; Szabo, A.; Moghul, I.; Balaskas, K.; Fujinami, K. Machine Learning Algorithms to Detect Subclinical Keratoconus: Systematic Review. JMIR Med. Inform. 2021, 9, e27363. [Google Scholar] [CrossRef] [PubMed]
- Fırat, M.; Çankaya, C.; Çınar, A.; Tuncer, T. Automatic detection of keratoconus on Pentacam images using feature selection based on deep learning. Int. J. Imaging Syst. Technol. 2022, 32, 1548–1560. [Google Scholar] [CrossRef]
- Al-Timemy, A.H.; Mosa, Z.M.; Alyasseri, Z.; Lavric, A.; Lui, M.M.; Hazarbassanov, R.M.; Yousefi, S. A Hybrid Deep Learning Construct for Detecting Keratoconus From Corneal Maps. Transl. Vis. Sci. Technol. 2021, 10, 16. [Google Scholar] [CrossRef] [PubMed]
- Chollet, F. Xception: Deep learning with depthwise separable convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1251–1258. [Google Scholar]
- Szegedy, C.; Ioffe, S.; Vanhoucke, V.; Alemi, A.A. Inception-v4, inception-resnet and the impact of residual connections on learning. In Proceedings of the Thirty-First AAAI Conference on Artificial Intelligence, San Francisco, CA, USA, 4–9 February 2017. [Google Scholar]
- Sinjab, M.M. Step by Step®: Reading Pentacam Topography: Basics and Case Study Series; Jaypee Brothers Medical Publishers: New Delhi, India, 2015; ISBN 9351523977. [Google Scholar]
- Alzubaidi, L.; Zhang, J.; Humaidi, A.J.; Al-Dujaili, A.; Duan, Y.; Al-Shamma, O.; Santamaría, J.; Fadhel, M.A.; Al-Amidie, M.; Farhan, L. Review of deep learning: Concepts, CNN architectures, challenges, applications, future directions. J. Big Data 2021, 8, 1–74. [Google Scholar] [CrossRef]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M. Imagenet large scale visual recognition challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef]
- Mungoli, N. Adaptive Ensemble Learning: Boosting Model Performance through Intelligent Feature Fusion in Deep Neural Networks. arXiv 2023, arXiv:2304.02653. [Google Scholar]
- Dhinakaran, P.; Shivanandappa, M.G.; Devnath, S. Keratoviz-A multistage keratoconus severity analysis and visualization using deep learning and class activated maps. Int. J. Electr. Comput. Eng. 2023, 13, 920–935. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Corneal Map | DL Model | Accuracy | Specificity | Sensitivity | Precision | F1-Score |
|---|---|---|---|---|---|---|
| Sag | Xception | 99.0 | 98.0 | 100 | 98.2 | 99.12 |
| Xception + SVM | 100 | 100 | 100 | 100 | 100 | |
| ElvF | Xception | 95.9 | 92.0 | 99.1 | 93.7 | 96.3 |
| Xception + SVM | 95.9 | 92.1 | 99.1 | 93.7 | 96.4 | |
| CorPac | Xception | 100 | 100 | 100 | 100 | 100 |
| Xception + SVM | 100 | 100 | 100 | 100 | 100 |
| DL Model | Accuracy | Specificity | Recall | Precision | F1-Score |
|---|---|---|---|---|---|
| Xception | 99.7 | 99.5 | 100 | 99.1 | 99.6 |
| InceptionResNetV2 | 97.0 | 95.3 | 100 | 92.4 | 96.0 |
| Feature Fusion + Decision Tree | 100 | 100 | 100 | 100 | 100 |
| DL Model | Accuracy | Specificity | Recall | Precision | F1-Score |
|---|---|---|---|---|---|
| Xception | 98.5 | 98.6 | 98.3 | 97.5 | 97.9 |
| InceptionResNetV2 | 97.0 | 95.9 | 99.1 | 92.9 | 95.9 |
| Feature Fusion+ SVM | 99.1 | 99.0 | 99.1 | 98.3 | 98.7 |
| Corneal Map | Accuracy | Specificity | Sensitivity | Precision | F1-Score | AUC |
|---|---|---|---|---|---|---|
| Sagittal | 89.2 | 90.3 | 87.8 | 88.7 | 88.3 | 0.91 |
| Elevation Front | 91.7 | 90.6 | 92.9 | 89.3 | 91.0 | 0.96 |
| Pachymetry | 87.7 | 84.3 | 92.9 | 79.8 | 85.8 | 0.92 |
| Study | Imaging Device | Number of Classes | Number of Maps | Network Used | Comments | Accuracy |
|---|---|---|---|---|---|---|
| Zéboulon et al. [15] | Orbscan | 2 | 3000 | CNN | No suspect | 98.3% |
| Al-Timemy et al. [2] | Pentcam | 2 | 534 | Ensemble of Alexnet | No suspect | 95–98.3% |
| Chen et al. [19] | Pentcam | 2 | 1926 | VGG16 | No suspect | 97.85% |
| Lavric and Valentin [20] | SyntEyes and SyntEyes KTC models/1 map | 3000 | KeratoDetect | No suspect synthetic maps | 99.3% | |
| Kuo et al. [13] | Tomy TMS-4 Topographer | 2 | 354 | VGG16 InceptionV3 ResNet152 | No suspect | 93.1% 93.1% 95.8% |
| Firat et al. [22] | Pentcam | 2 | 628 | ALexNet and SVM | No suspect | 98.53% |
| This study | Pentcam | 3 | 4113 | Fusion of Xception and InceptionResNetV2 | - | 97–100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Timemy, A.H.; Alzubaidi, L.; Mosa, Z.M.; Abdelmotaal, H.; Ghaeb, N.H.; Lavric, A.; Hazarbassanov, R.M.; Takahashi, H.; Gu, Y.; Yousefi, S. A Deep Feature Fusion of Improved Suspected Keratoconus Detection with Deep Learning. Diagnostics 2023, 13, 1689. https://doi.org/10.3390/diagnostics13101689
Al-Timemy AH, Alzubaidi L, Mosa ZM, Abdelmotaal H, Ghaeb NH, Lavric A, Hazarbassanov RM, Takahashi H, Gu Y, Yousefi S. A Deep Feature Fusion of Improved Suspected Keratoconus Detection with Deep Learning. Diagnostics. 2023; 13(10):1689. https://doi.org/10.3390/diagnostics13101689
Chicago/Turabian StyleAl-Timemy, Ali H., Laith Alzubaidi, Zahraa M. Mosa, Hazem Abdelmotaal, Nebras H. Ghaeb, Alexandru Lavric, Rossen M. Hazarbassanov, Hidenori Takahashi, Yuantong Gu, and Siamak Yousefi. 2023. "A Deep Feature Fusion of Improved Suspected Keratoconus Detection with Deep Learning" Diagnostics 13, no. 10: 1689. https://doi.org/10.3390/diagnostics13101689