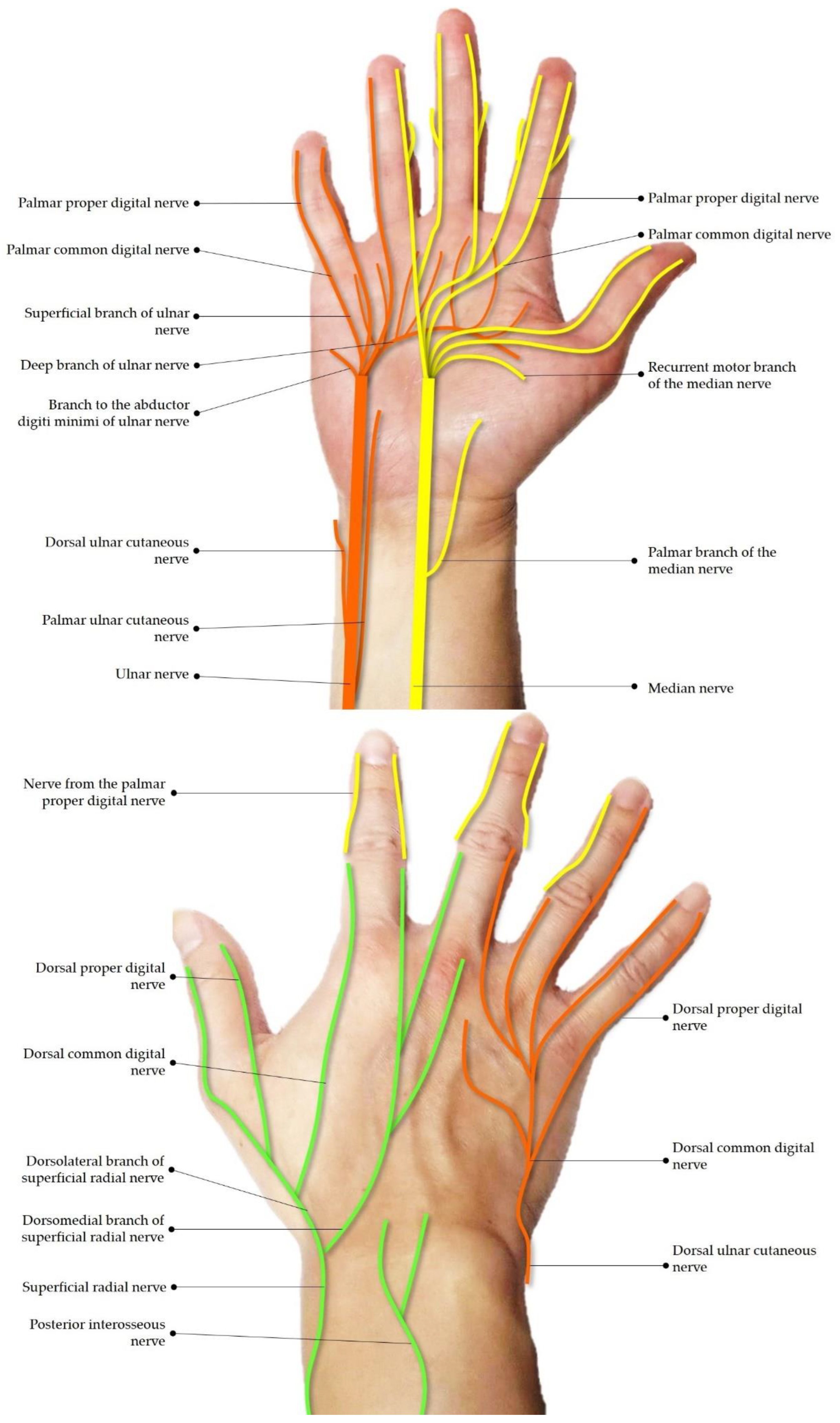
Figure 1.
Schematic drawing of the innervation of the wrist and hand.
Figure 1.
Schematic drawing of the innervation of the wrist and hand.
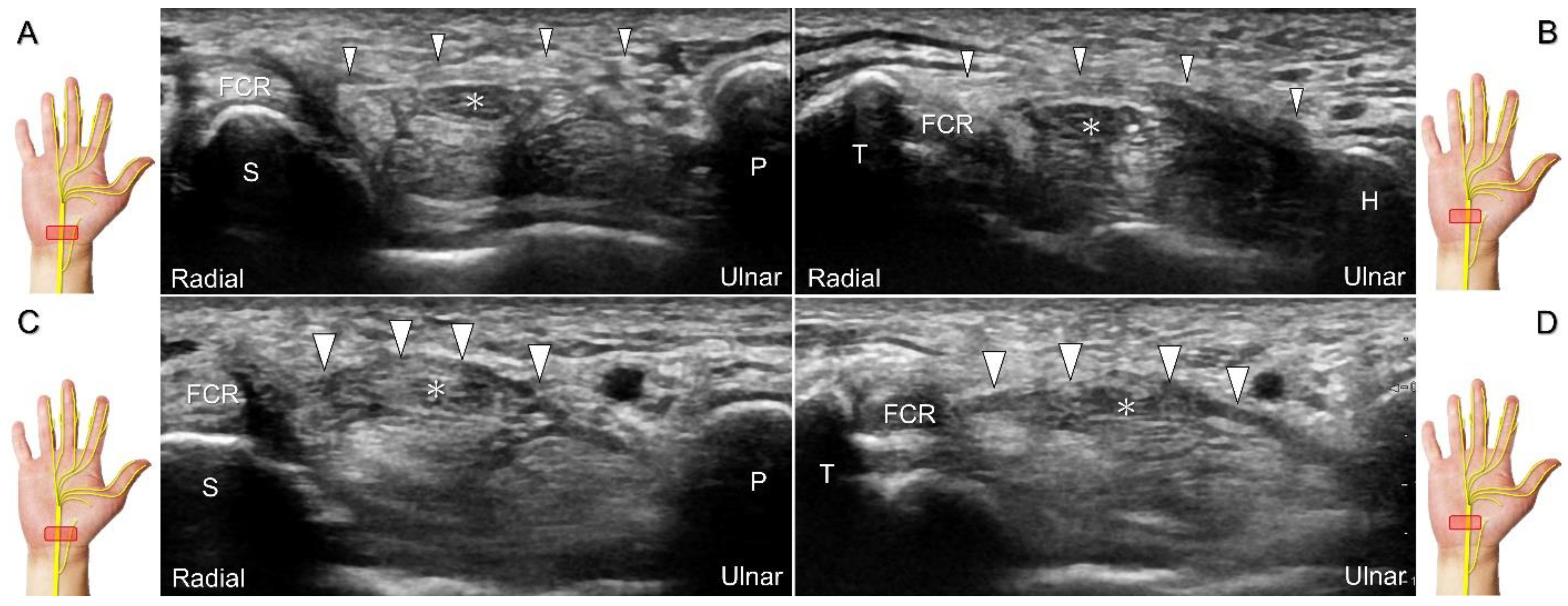
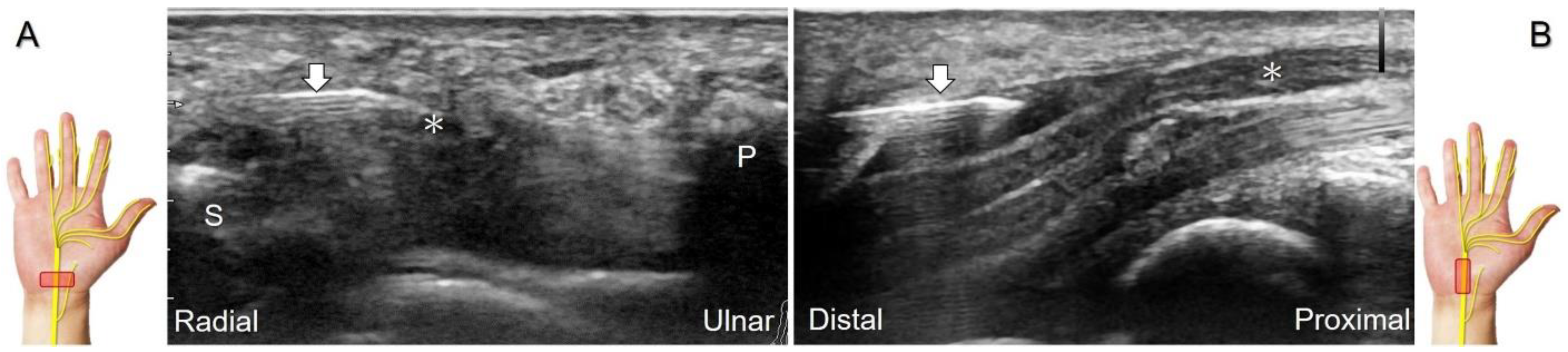
Figure 2.
Sonographic/normal imaging of the median nerve from the inlet (A) to the outlet (B) of the carpal tunnel. Hypertrophy of the flexor retinaculum at both the inlet (C) and outlet (D) of the carpal tunnel. Asterisk: median nerve; small white arrowheads: normal flexor retinaculum; large arrowheads: hypertrophy of the flexor retinaculum. FCR: flexor carpi radialis; S: scaphoid; P: pisiform; T: trapezium; H: hook of the hamate.
Figure 2.
Sonographic/normal imaging of the median nerve from the inlet (A) to the outlet (B) of the carpal tunnel. Hypertrophy of the flexor retinaculum at both the inlet (C) and outlet (D) of the carpal tunnel. Asterisk: median nerve; small white arrowheads: normal flexor retinaculum; large arrowheads: hypertrophy of the flexor retinaculum. FCR: flexor carpi radialis; S: scaphoid; P: pisiform; T: trapezium; H: hook of the hamate.
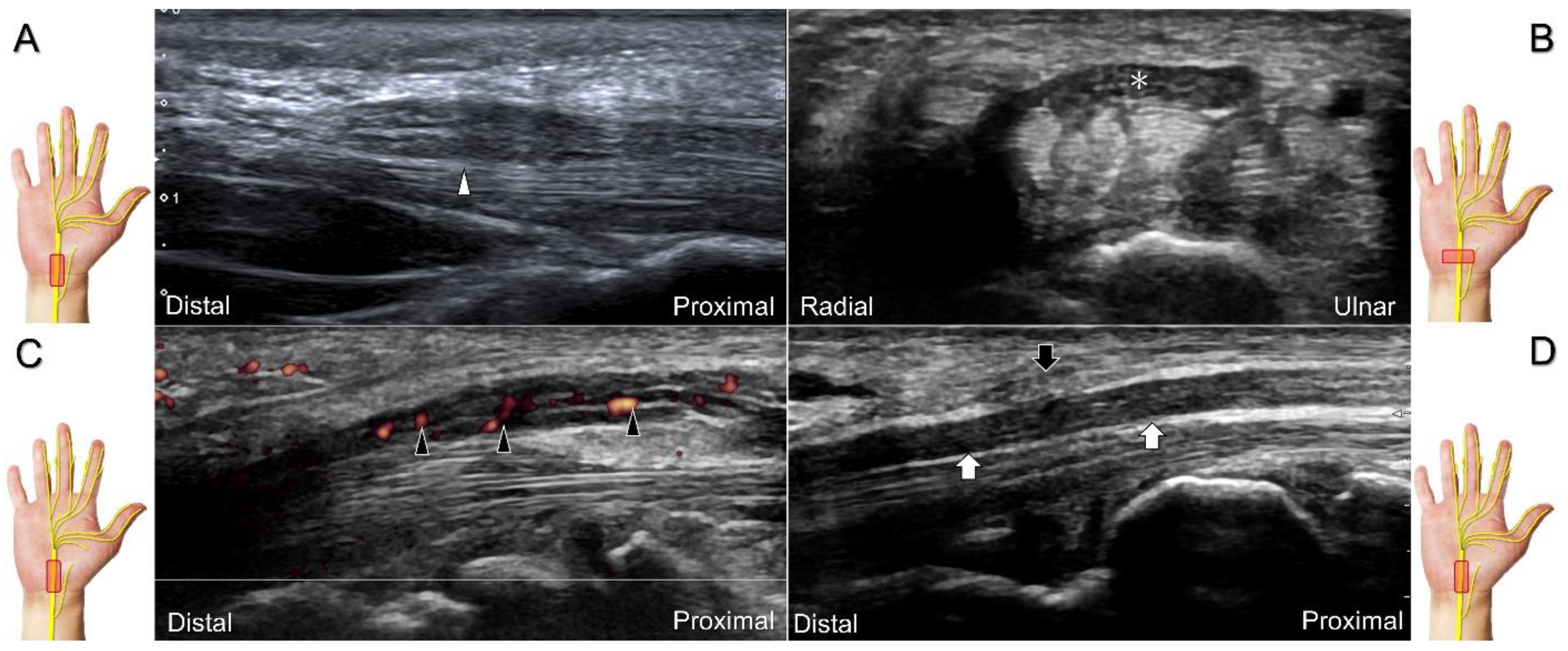
Figure 3.
Sonographic images of patients with carpal tunnel syndrome, showing focal swelling proximal to the compression site (A), flattening at the compression site (B), intraneural hypervascularity (C), and loss of the trimline pattern (D). White arrowhead: focal swelling of the median nerve; asterisk: flattening of the median nerve; black arrowheads: intraneural hypervascularity of the median nerve; white arrows: loss of the trimline pattern of the median nerve; black arrow: thickened flexor retinaculum.
Figure 3.
Sonographic images of patients with carpal tunnel syndrome, showing focal swelling proximal to the compression site (A), flattening at the compression site (B), intraneural hypervascularity (C), and loss of the trimline pattern (D). White arrowhead: focal swelling of the median nerve; asterisk: flattening of the median nerve; black arrowheads: intraneural hypervascularity of the median nerve; white arrows: loss of the trimline pattern of the median nerve; black arrow: thickened flexor retinaculum.
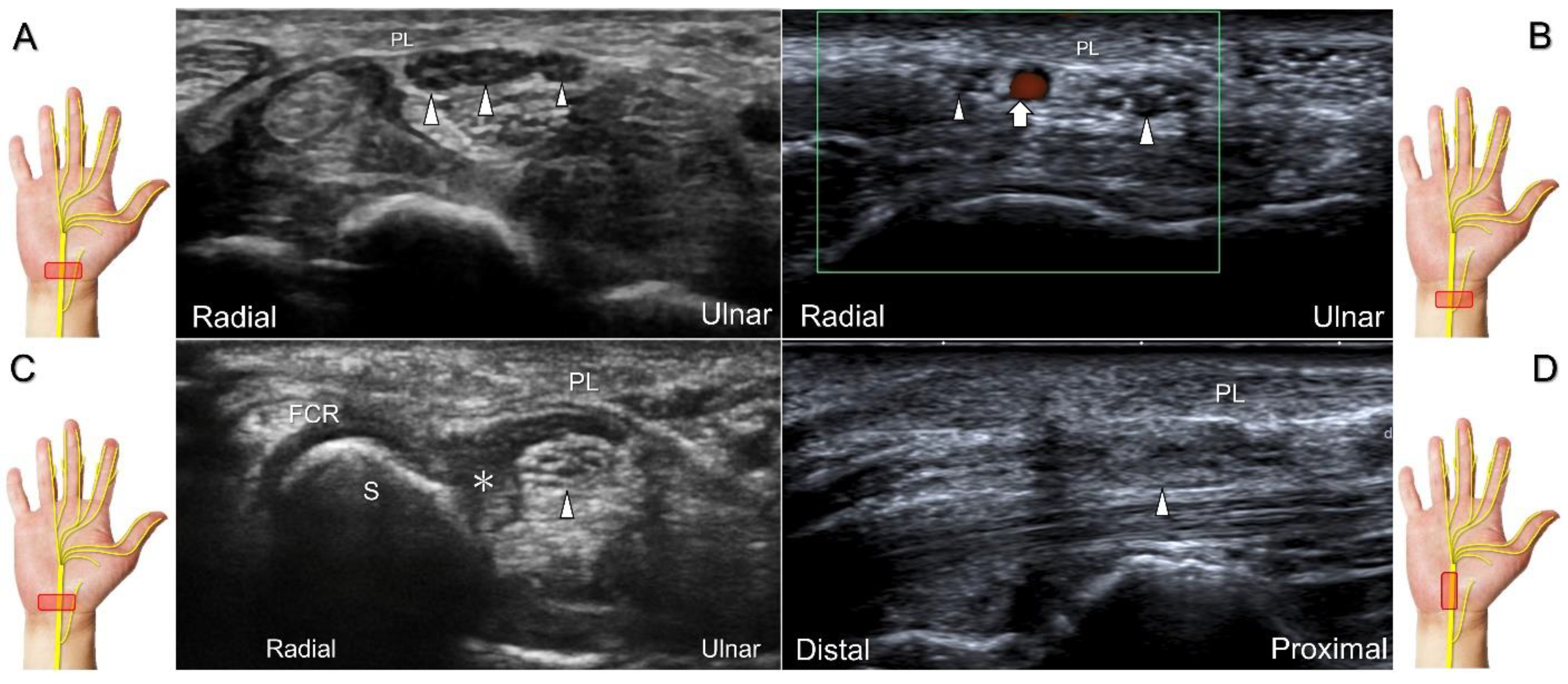
Figure 4.
Sonographic images show a bifid median nerve (A), a persistent median artery with a bifid median nerve (B), accessory flexor digitorum superficialis muscle (C), and laceration of the palmaris longus (PL) tendon with the compression of the median nerve (D). White arrowheads: median nerve; white arrow: persistent median artery; asterisk: accessory flexor digitorum superficialis muscle. FCR: flexor carpi radialis tendon; S: scaphoid.
Figure 4.
Sonographic images show a bifid median nerve (A), a persistent median artery with a bifid median nerve (B), accessory flexor digitorum superficialis muscle (C), and laceration of the palmaris longus (PL) tendon with the compression of the median nerve (D). White arrowheads: median nerve; white arrow: persistent median artery; asterisk: accessory flexor digitorum superficialis muscle. FCR: flexor carpi radialis tendon; S: scaphoid.
Figure 5.
Comparative ultrasonography (long-axis view) between healthy (A) vs. affected (B) sides shows a schwannoma (black arrowhead) with increased intraneural vascularity.
Figure 5.
Comparative ultrasonography (long-axis view) between healthy (A) vs. affected (B) sides shows a schwannoma (black arrowhead) with increased intraneural vascularity.
Figure 6.
Ultrasound-guided hydrodissection of the median nerve under short-axis (A) or long-axis (B) imaging. Asterisk: median nerve; arrows: needle. S: scaphoid; P: pisiform.
Figure 6.
Ultrasound-guided hydrodissection of the median nerve under short-axis (A) or long-axis (B) imaging. Asterisk: median nerve; arrows: needle. S: scaphoid; P: pisiform.
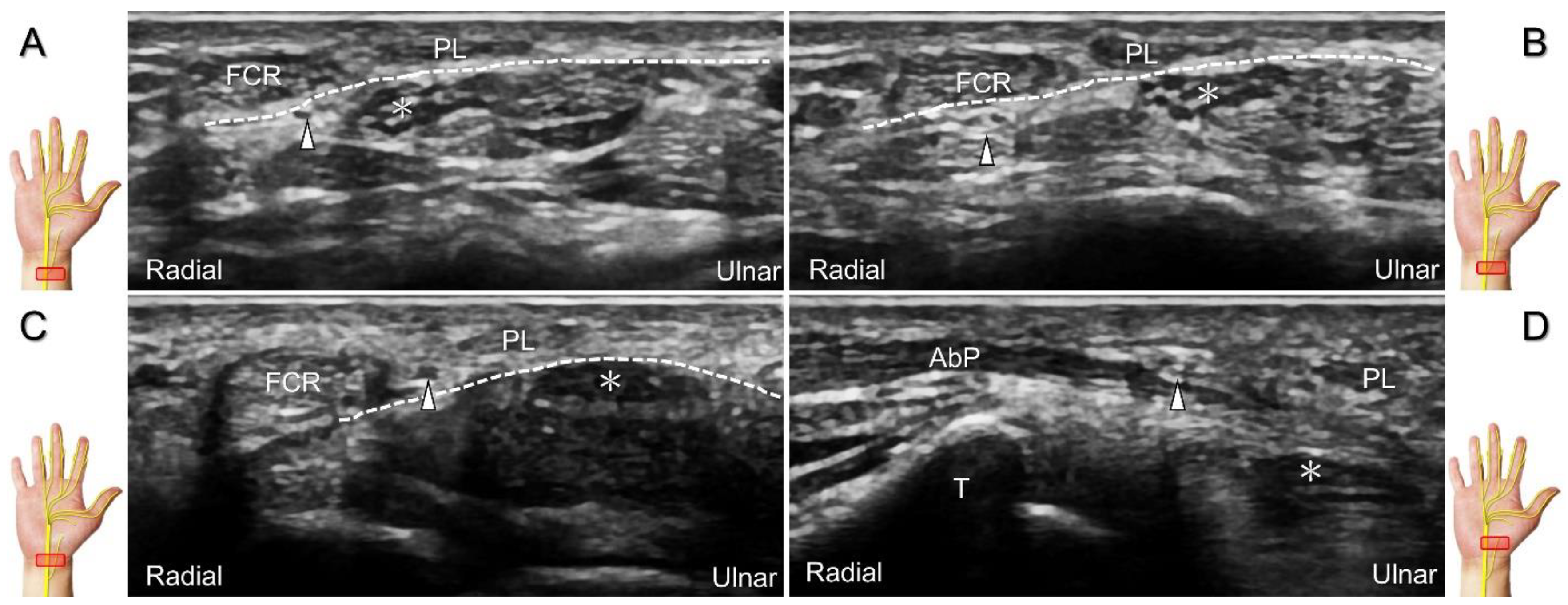
Figure 7.
Sonographic imaging of the palmar cutaneous branch of the median nerve (A) shows its emerging from the radial aspect of the median nerve (B), penetrating the antebrachial fascia (C), and arriving at the superficial site of the abductor pollicis brevis muscle (D). Asterisk: median nerve; arrowhead: palmar cutaneous branch of the median nerve; dashed line, antebrachial fascia; FCR: flexor carpi radialis tendon; T: trapezium; PL: palmaris longus tendon; AbP: abductor pollicis brevis muscle.
Figure 7.
Sonographic imaging of the palmar cutaneous branch of the median nerve (A) shows its emerging from the radial aspect of the median nerve (B), penetrating the antebrachial fascia (C), and arriving at the superficial site of the abductor pollicis brevis muscle (D). Asterisk: median nerve; arrowhead: palmar cutaneous branch of the median nerve; dashed line, antebrachial fascia; FCR: flexor carpi radialis tendon; T: trapezium; PL: palmaris longus tendon; AbP: abductor pollicis brevis muscle.
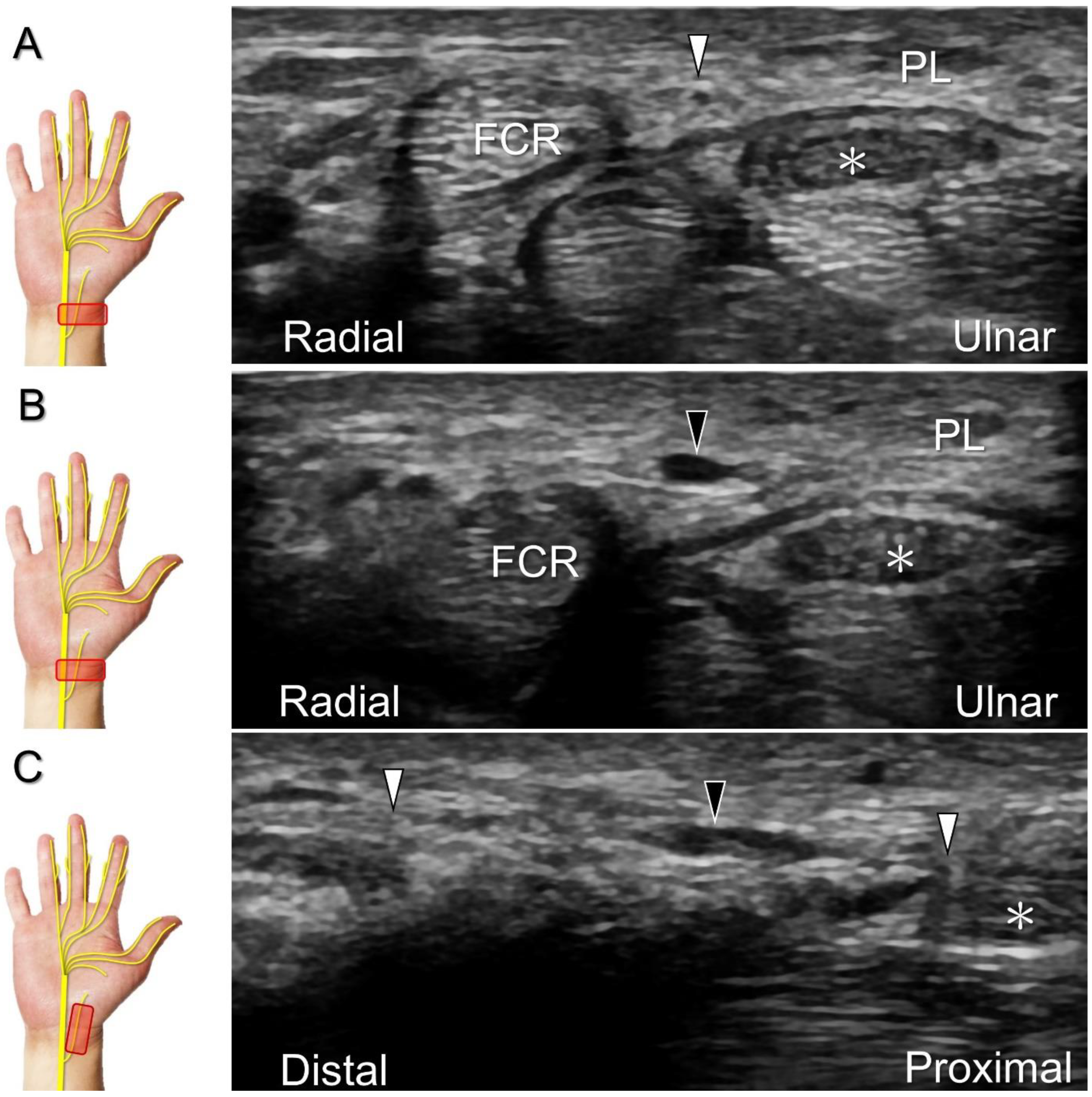
Figure 8.
Compared with the normal proximal segment (A), a neuroma originating from the palmar cutaneous branch of the median nerve is seen in short-axis (B) and long-axis (C) imaging. Asterisk: median nerve; white arrowheads: palmar cutaneous branch of the median nerve; black arrowhead: neuroma. FCR: flexor carpi radialis tendon; PL: palmaris longus tendon.
Figure 8.
Compared with the normal proximal segment (A), a neuroma originating from the palmar cutaneous branch of the median nerve is seen in short-axis (B) and long-axis (C) imaging. Asterisk: median nerve; white arrowheads: palmar cutaneous branch of the median nerve; black arrowhead: neuroma. FCR: flexor carpi radialis tendon; PL: palmaris longus tendon.
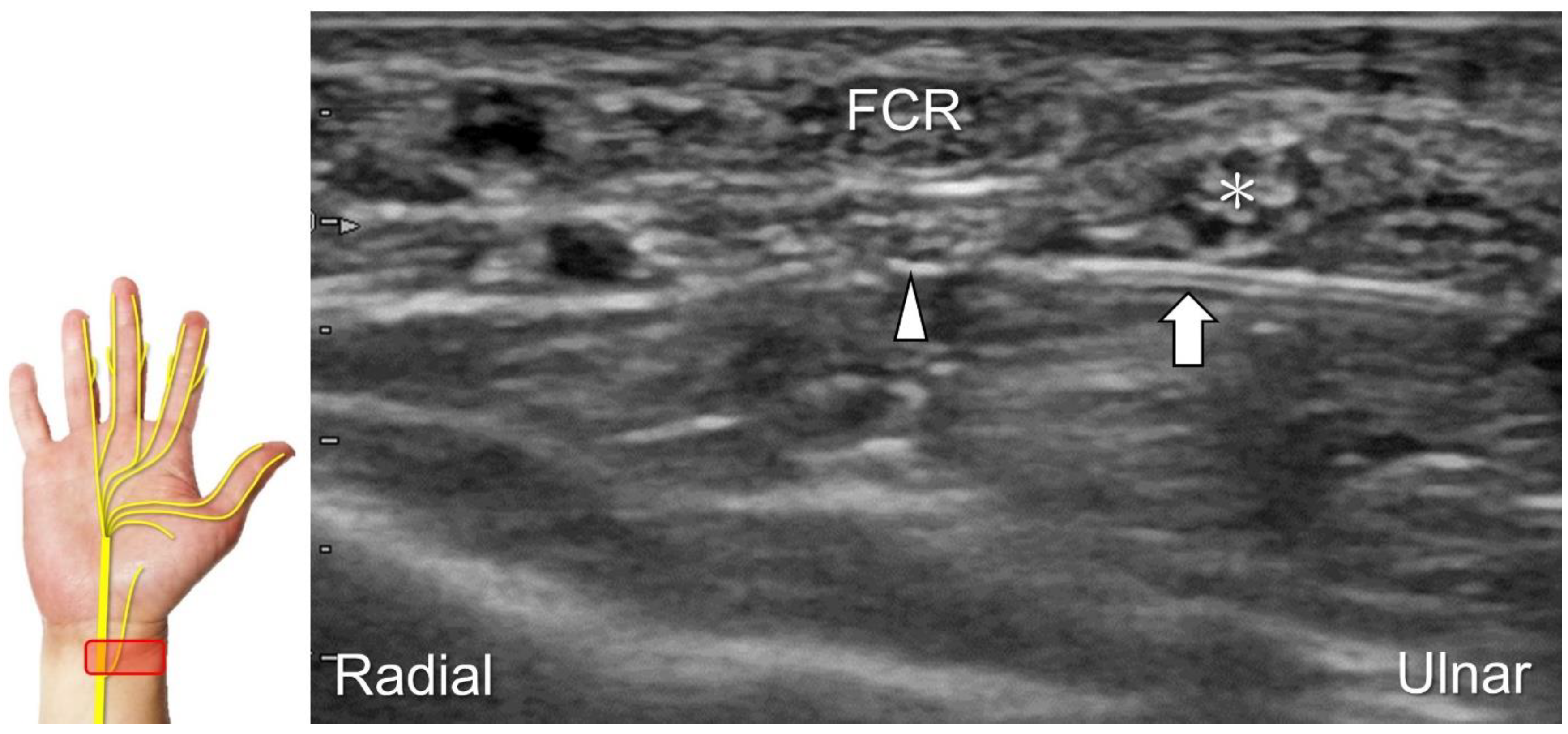
Figure 9.
Ultrasound-guided hydrodissection (short-axis view) for the palmar cutaneous branch of the median nerve. Asterisk: median nerve; arrowhead: palmar cutaneous branch of the median nerve; arrow: needle. FCR: flexor carpi radialis tendon.
Figure 9.
Ultrasound-guided hydrodissection (short-axis view) for the palmar cutaneous branch of the median nerve. Asterisk: median nerve; arrowhead: palmar cutaneous branch of the median nerve; arrow: needle. FCR: flexor carpi radialis tendon.
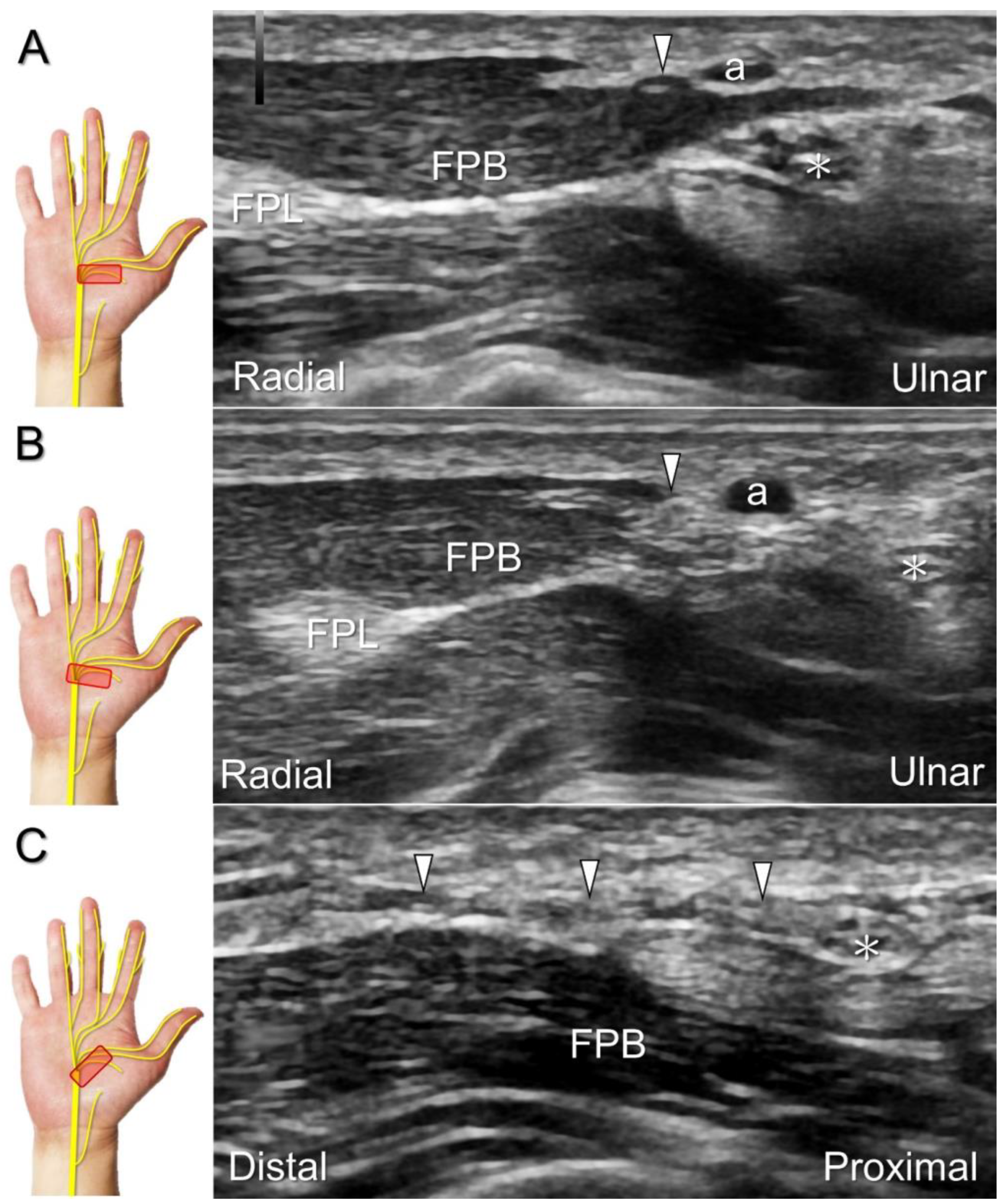
Figure 10.
Sonographic imaging for the recurrent motor branch of the median nerve. Tracking back from the surface of the thenar muscle (A) toward the division site from the main trunk in short-axis (B) and long-axis (C) imaging. Asterisk: median nerve; white arrowheads: recurrent motor branch of the median nerve; a: artery; FPL: flexor pollicis longus tendon; FPB: flexor pollicis brevis muscle.
Figure 10.
Sonographic imaging for the recurrent motor branch of the median nerve. Tracking back from the surface of the thenar muscle (A) toward the division site from the main trunk in short-axis (B) and long-axis (C) imaging. Asterisk: median nerve; white arrowheads: recurrent motor branch of the median nerve; a: artery; FPL: flexor pollicis longus tendon; FPB: flexor pollicis brevis muscle.
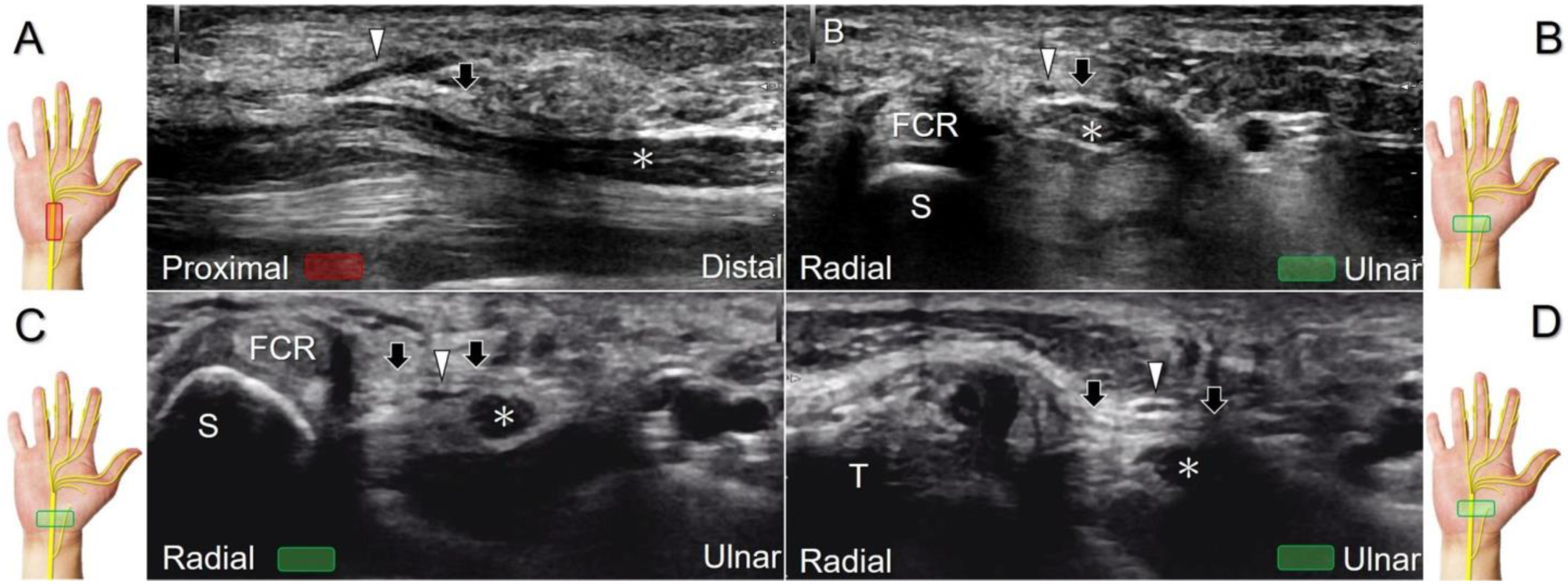
Figure 11.
Sonographic imaging of the preligamentous type of recurrent motor branch of the median nerve. It divides from the median nerve proximal to the carpal tunnel as seen in the long-axis view (A), and resides superficial to the flexor retinaculum, as seen in the short-axis view (B), whereas the transligamentous type of recurrent motor branch accompanies the median nerve into the carpal tunnel (C), penetrating the retinaculum at the outlet of the carpal tunnel (D). Asterisk: median nerve; arrowheads: recurrent motor branch of the median nerve; arrows: flexor retinaculum. FCR: flexor carpi radialis tendon.
Figure 11.
Sonographic imaging of the preligamentous type of recurrent motor branch of the median nerve. It divides from the median nerve proximal to the carpal tunnel as seen in the long-axis view (A), and resides superficial to the flexor retinaculum, as seen in the short-axis view (B), whereas the transligamentous type of recurrent motor branch accompanies the median nerve into the carpal tunnel (C), penetrating the retinaculum at the outlet of the carpal tunnel (D). Asterisk: median nerve; arrowheads: recurrent motor branch of the median nerve; arrows: flexor retinaculum. FCR: flexor carpi radialis tendon.
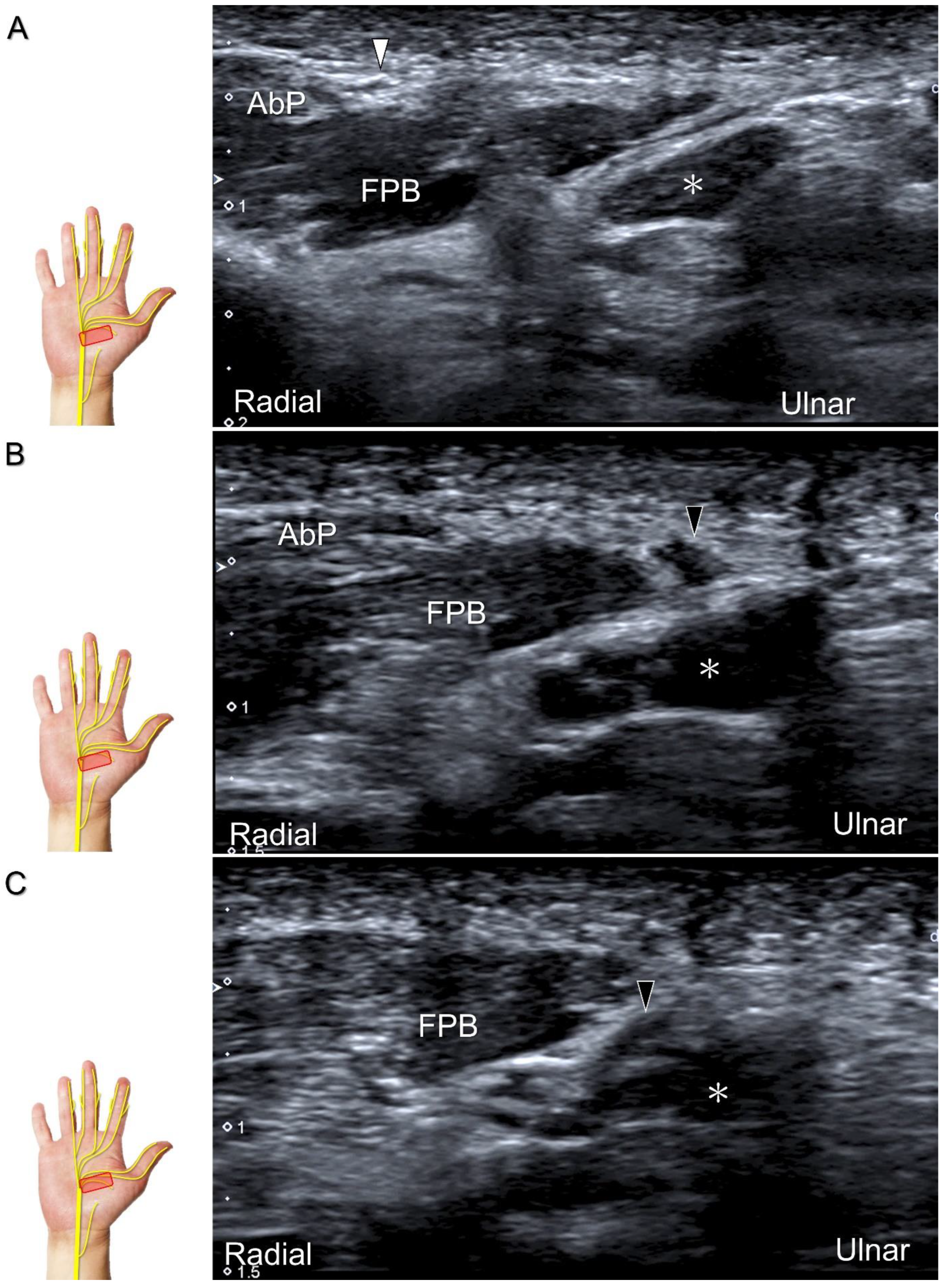
Figure 12.
Sonographic imaging (short-axis view) shows the segment (A) distal to the neuroma of the recurrent motor branch of the median nerve (B) and the proximal segment (C). Asterisk: median nerve; white arrowhead: recurrent motor branch of the median nerve; black arrowheads: neuroma. FPB: flexor pollicis brevis muscle; AbP: abductor pollicis brevis muscle.
Figure 12.
Sonographic imaging (short-axis view) shows the segment (A) distal to the neuroma of the recurrent motor branch of the median nerve (B) and the proximal segment (C). Asterisk: median nerve; white arrowhead: recurrent motor branch of the median nerve; black arrowheads: neuroma. FPB: flexor pollicis brevis muscle; AbP: abductor pollicis brevis muscle.
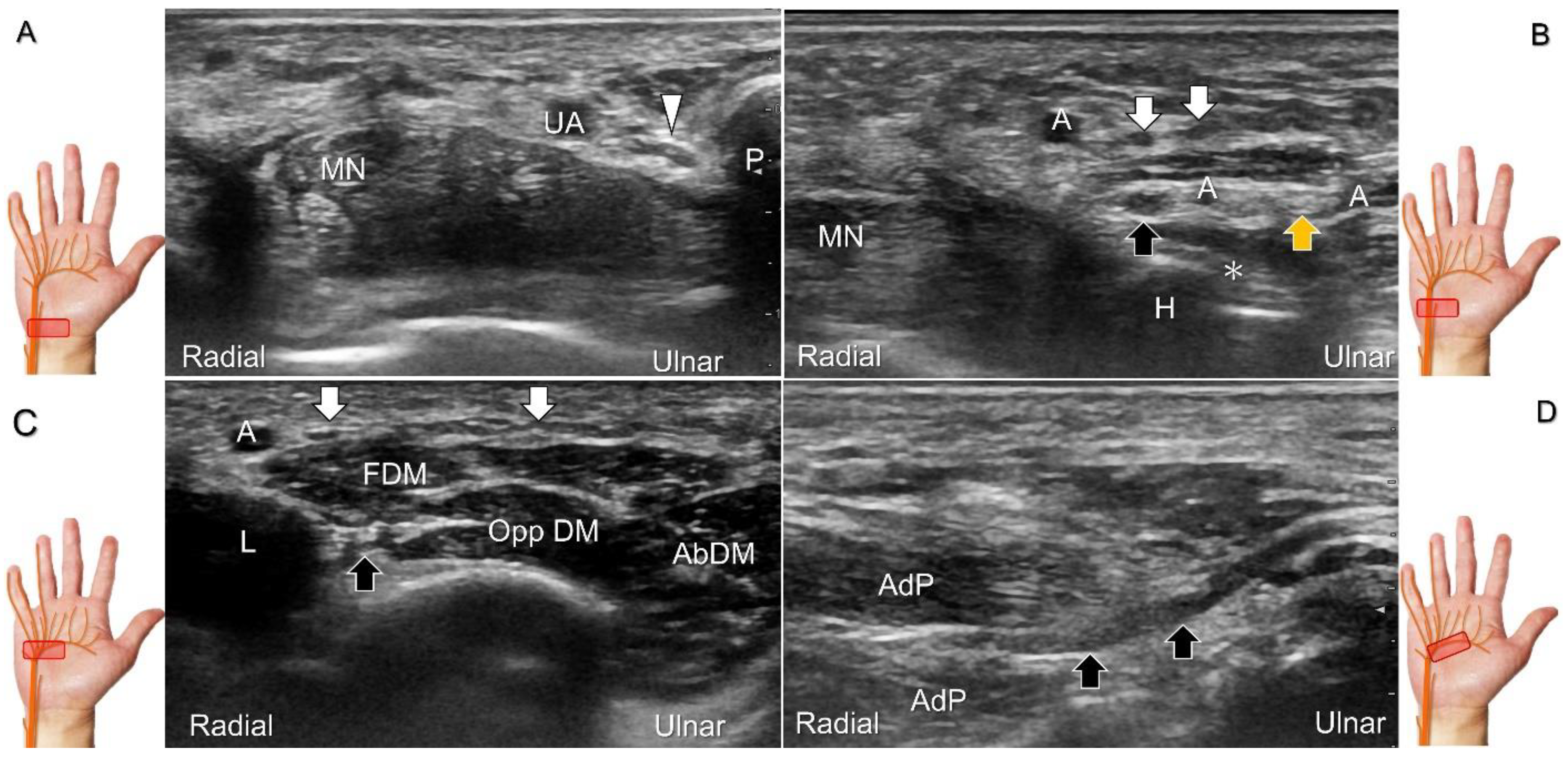
Figure 13.
Sonographic imaging (short-axis view) shows the ulnar nerve within the Guyon’s canal (A), separation of branches beside the pisohamate hiatus (B), deep branch of the ulnar nerve located between the hypothenar muscles distal to the hook of the hamate (C). Long-axis view (through pivoting the transducer) shows the segment of the deep branch within the adductor pollicis muscle (D). Arrowhead: ulnar nerve; white arrows: superficial branch of the ulnar nerve; black arrows: deep branch of the ulnar nerve; orange arrow: branch of the ulnar nerve to the abductor digiti minimi; *: pisohamate ligment MN: median nerve; UA: ulnar artery; P: pisiform; H: hook of hamate; A: artery; L: lumbrical muscle; FDM: flexor digiti minimi brevis muscle; Opp DM: opponens digiti minimi muscle; AbDM: abductor digiti minimi muscle; AdP: adductor pollicis muscle.
Figure 13.
Sonographic imaging (short-axis view) shows the ulnar nerve within the Guyon’s canal (A), separation of branches beside the pisohamate hiatus (B), deep branch of the ulnar nerve located between the hypothenar muscles distal to the hook of the hamate (C). Long-axis view (through pivoting the transducer) shows the segment of the deep branch within the adductor pollicis muscle (D). Arrowhead: ulnar nerve; white arrows: superficial branch of the ulnar nerve; black arrows: deep branch of the ulnar nerve; orange arrow: branch of the ulnar nerve to the abductor digiti minimi; *: pisohamate ligment MN: median nerve; UA: ulnar artery; P: pisiform; H: hook of hamate; A: artery; L: lumbrical muscle; FDM: flexor digiti minimi brevis muscle; Opp DM: opponens digiti minimi muscle; AbDM: abductor digiti minimi muscle; AdP: adductor pollicis muscle.
Figure 14.
Sonographic images depict a fibrolipomatous hamartoma (arrowheads) in the short- (A) and long-axis (B) views.
Figure 14.
Sonographic images depict a fibrolipomatous hamartoma (arrowheads) in the short- (A) and long-axis (B) views.
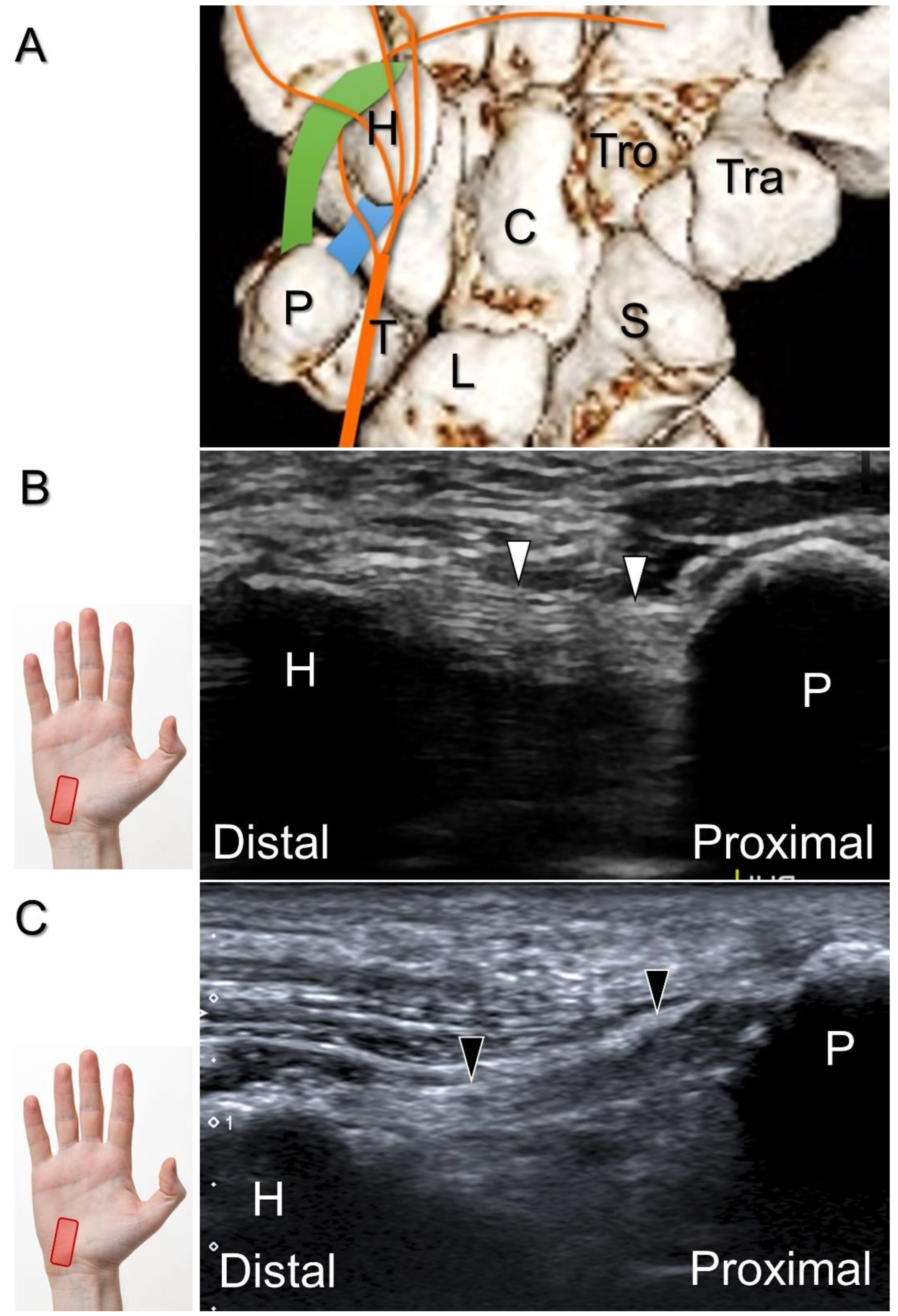
Figure 15.
Illustration of the pisohamate hiatus formed by the arch of hypothenar muscles and the pisohamate ligament (A). Compared with the normal ligament (B), long-axis imaging displays sprain and swelling of the pisohamate ligament (C). Blue area: pisohamate ligament; green area: fibrous arch of the flexor digiti minimi brevis muscle; white arrows: normal pisohamate ligament; black arrows: swollen pisohamate ligament; H: hamate; P: pisiform; T: triquetrum; L: lunate; C: capitate; Tro: trapezoid; Tra: trapezium; S: scaphoid.
Figure 15.
Illustration of the pisohamate hiatus formed by the arch of hypothenar muscles and the pisohamate ligament (A). Compared with the normal ligament (B), long-axis imaging displays sprain and swelling of the pisohamate ligament (C). Blue area: pisohamate ligament; green area: fibrous arch of the flexor digiti minimi brevis muscle; white arrows: normal pisohamate ligament; black arrows: swollen pisohamate ligament; H: hamate; P: pisiform; T: triquetrum; L: lunate; C: capitate; Tro: trapezoid; Tra: trapezium; S: scaphoid.
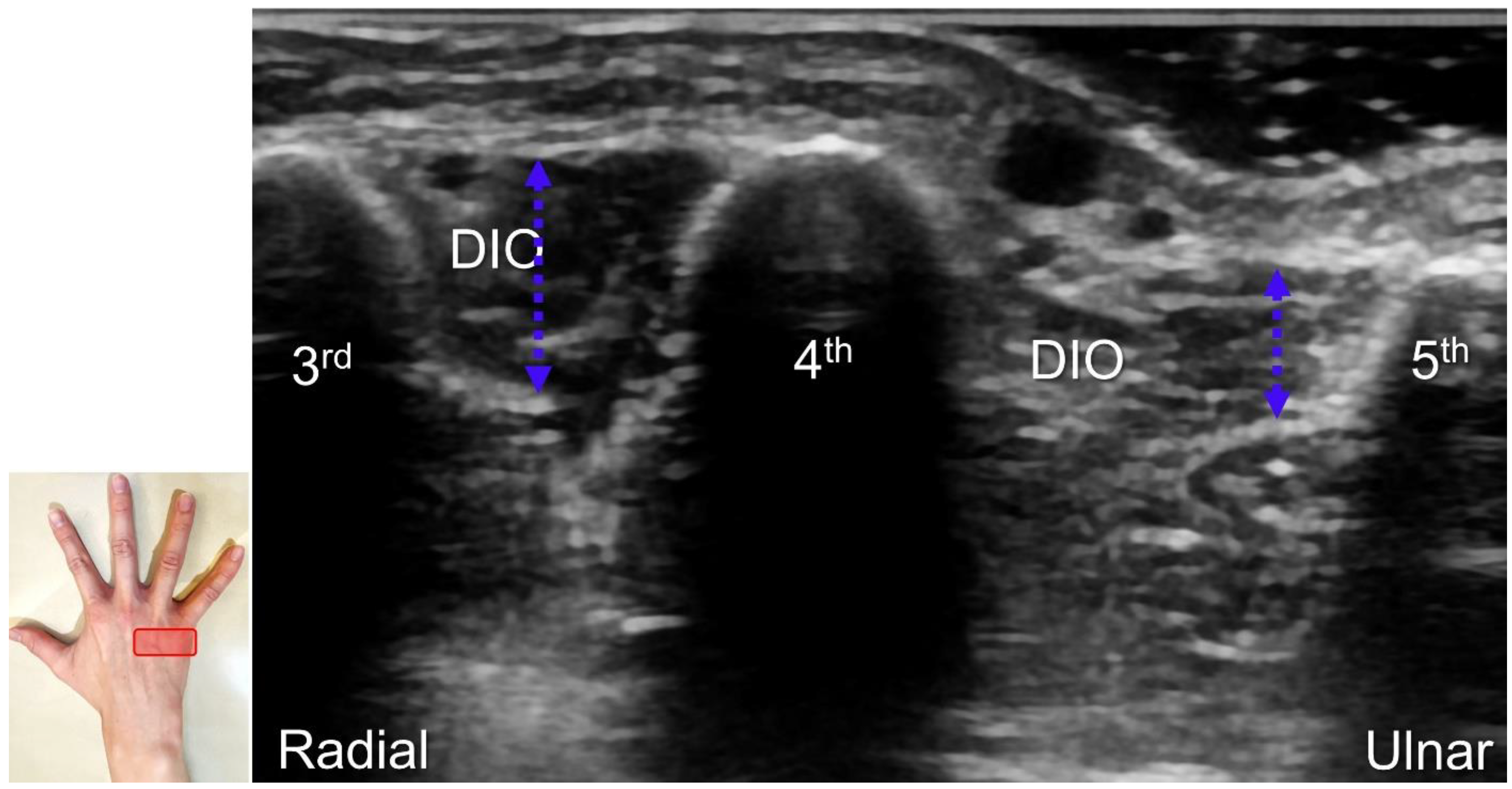
Figure 16.
As opposed to the normal third dorsal interossei (DIO) muscle, atrophy in the fourth DIO muscle indicates injury to the terminal branch of the deep branch of the ulnar nerve. Blue double dashed arrows: muscle thickness.
Figure 16.
As opposed to the normal third dorsal interossei (DIO) muscle, atrophy in the fourth DIO muscle indicates injury to the terminal branch of the deep branch of the ulnar nerve. Blue double dashed arrows: muscle thickness.
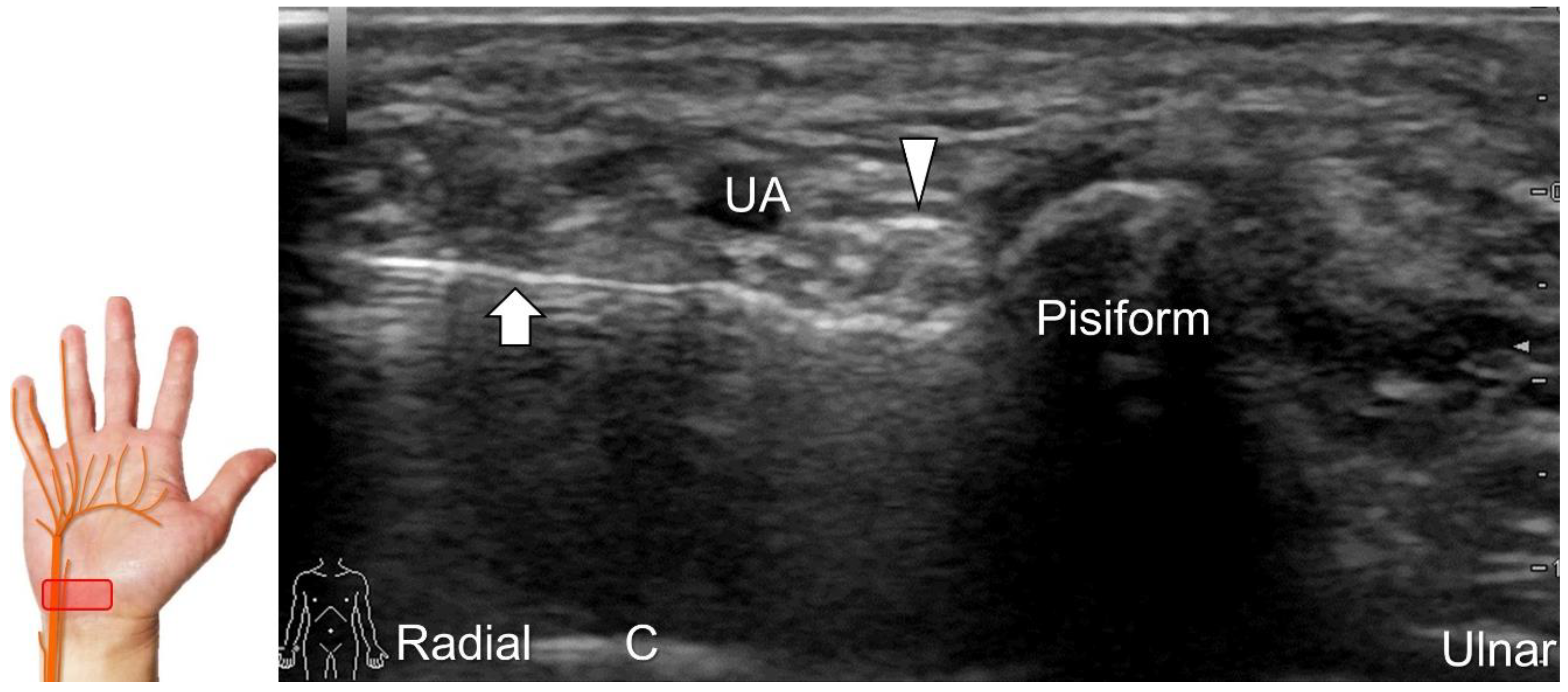
Figure 17.
Ultrasound-guided injection of the ulnar nerve in short-axis view. Arrowhead: ulnar nerve; arrow: needle. UA: ulnar artery; C: capitate.
Figure 17.
Ultrasound-guided injection of the ulnar nerve in short-axis view. Arrowhead: ulnar nerve; arrow: needle. UA: ulnar artery; C: capitate.
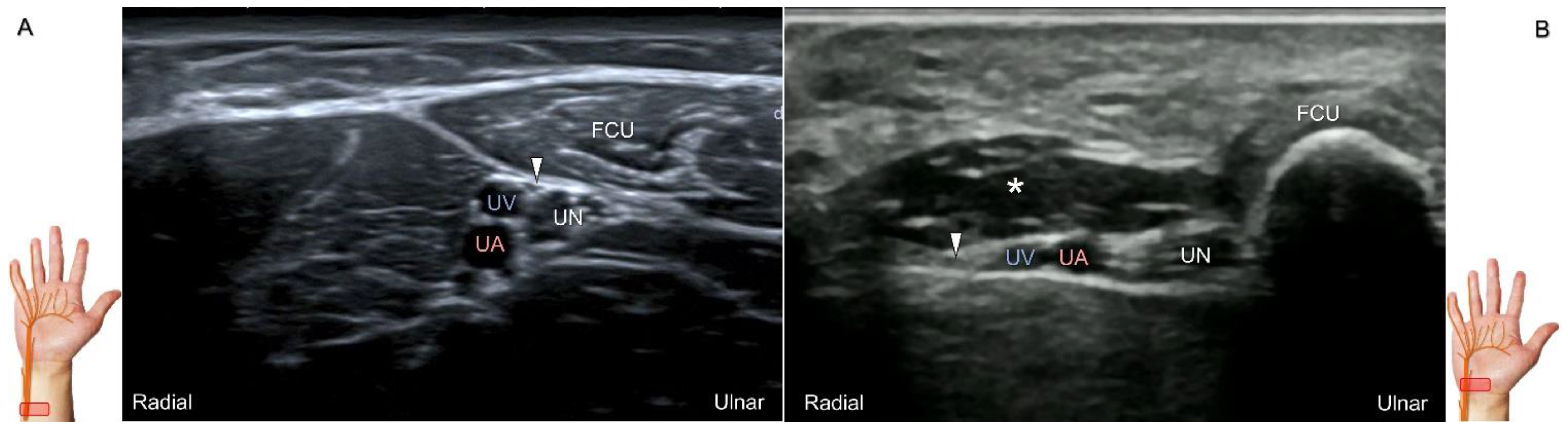
Figure 18.
Sonographic imaging (short-axis view) of the palmar ulnar cutaneous nerve (A) and its entrapment in the presence of an accessory abductor digiti minimi muscle (B). Arrowhead: palmar ulnar cutaneous nerve; asterisk: accessory abductor digiti minimi muscle. UN: ulnar nerve; UA: ulnar artery; UV: ulnar vein; FCU: flexor carpi ulnaris tendon.
Figure 18.
Sonographic imaging (short-axis view) of the palmar ulnar cutaneous nerve (A) and its entrapment in the presence of an accessory abductor digiti minimi muscle (B). Arrowhead: palmar ulnar cutaneous nerve; asterisk: accessory abductor digiti minimi muscle. UN: ulnar nerve; UA: ulnar artery; UV: ulnar vein; FCU: flexor carpi ulnaris tendon.
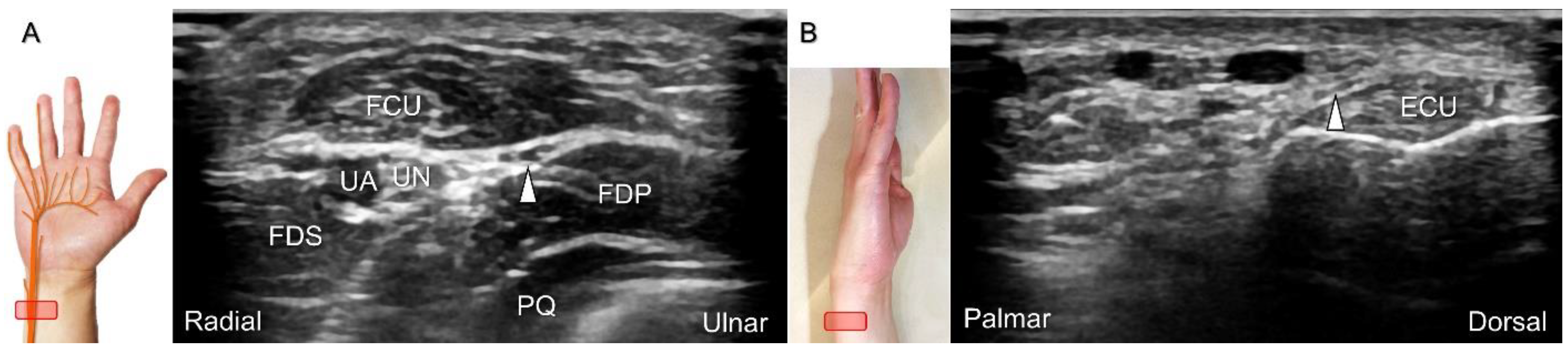
Figure 19.
Sonographic imaging of the dorsal ulnar cutaneous nerve as it branches from the ulnar aspect of the ulnar nerve underneath the flexor carpi ulnaris (FCU) muscle (A). The nerve wraps around the distal ulna to reach the dorsal wrist (B). Arrowhead: dorsal ulnar cutaneous nerve. UN: ulnar nerve; UA: ulnar artery; FDS: flexor digitorum superficialis muscle; FDP: flexor digitorum profundus muscle; PQ; pronator quadratus muscle; ECU: extensor carpi ulnaris tendon.
Figure 19.
Sonographic imaging of the dorsal ulnar cutaneous nerve as it branches from the ulnar aspect of the ulnar nerve underneath the flexor carpi ulnaris (FCU) muscle (A). The nerve wraps around the distal ulna to reach the dorsal wrist (B). Arrowhead: dorsal ulnar cutaneous nerve. UN: ulnar nerve; UA: ulnar artery; FDS: flexor digitorum superficialis muscle; FDP: flexor digitorum profundus muscle; PQ; pronator quadratus muscle; ECU: extensor carpi ulnaris tendon.
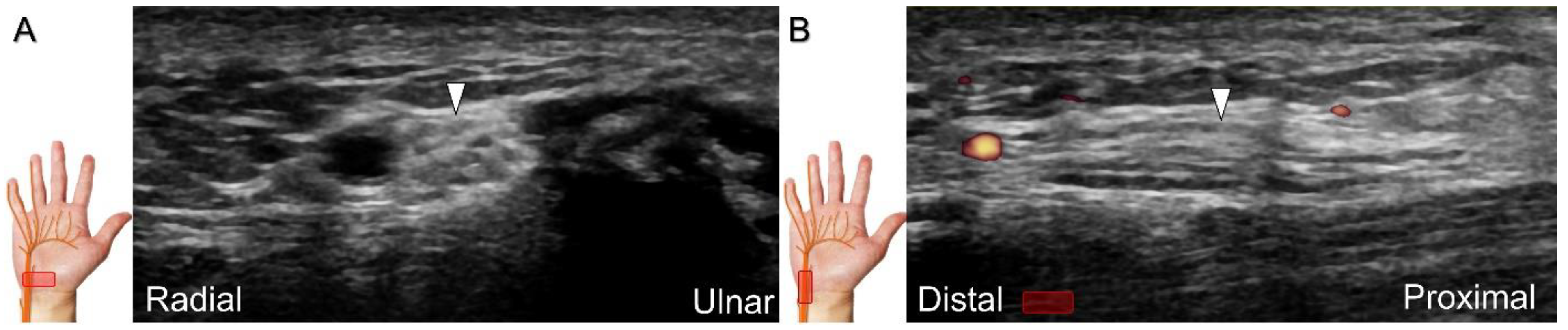
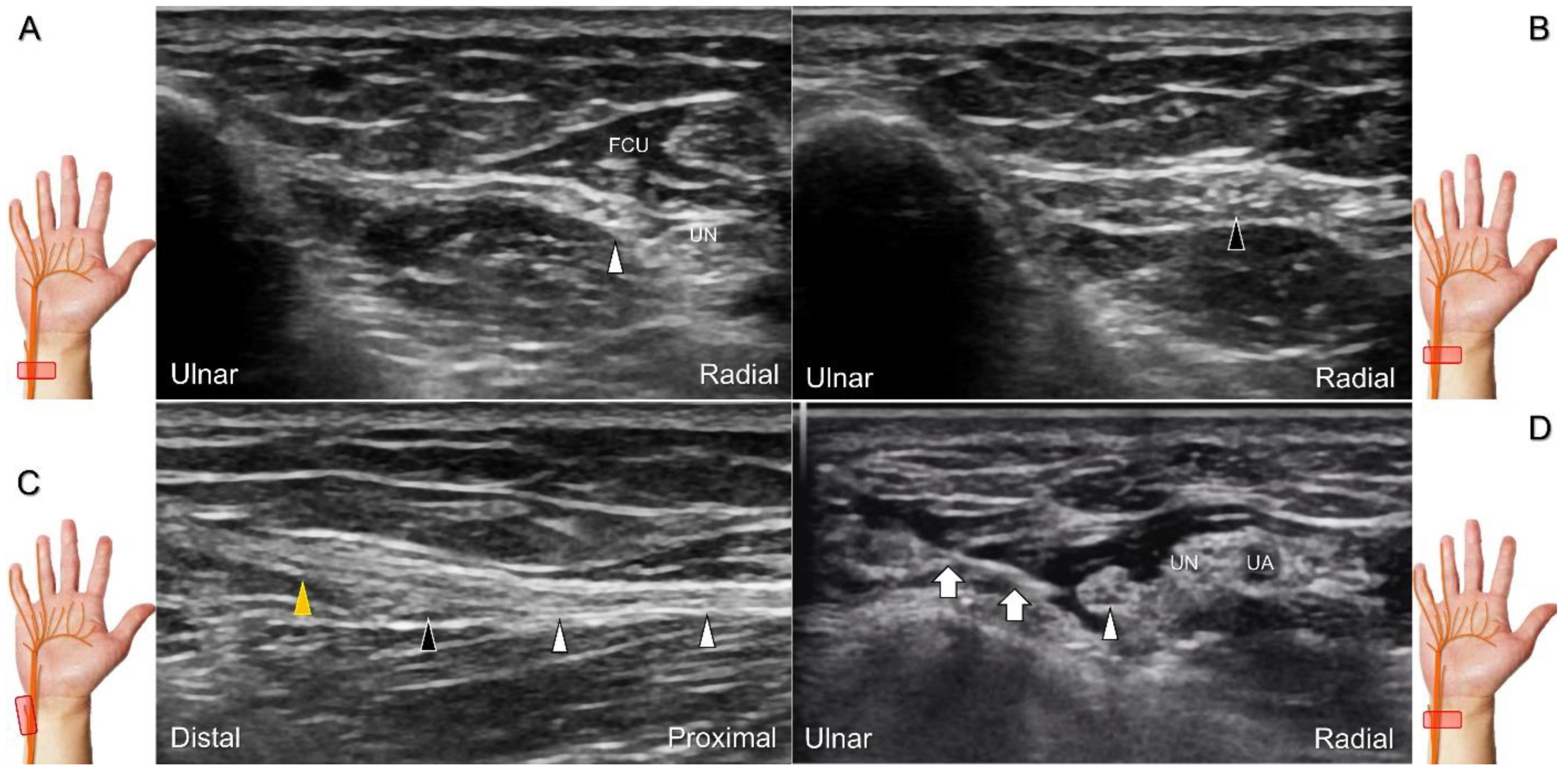
Figure 20.
Sonographic tracking (short-axis view) of the dorsal ulnar cutaneous nerve from its normal (A) to the swollen segment (B) proximal to the entrapment. The normal, swollen, and entrapped segments of the dorsal ulnar cutaneous nerve are seen in long-axis imaging (C). Ultrasound-guided hydrodissection of the nerve (D). White arrowheads: normal segment; black arrowheads: swollen segment; orange arrowhead: entrapped segment; white arrows: needle. FCU: flexor carpi ulnaris muscle; UN: ulnar nerve; UA: ulnar artery.
Figure 20.
Sonographic tracking (short-axis view) of the dorsal ulnar cutaneous nerve from its normal (A) to the swollen segment (B) proximal to the entrapment. The normal, swollen, and entrapped segments of the dorsal ulnar cutaneous nerve are seen in long-axis imaging (C). Ultrasound-guided hydrodissection of the nerve (D). White arrowheads: normal segment; black arrowheads: swollen segment; orange arrowhead: entrapped segment; white arrows: needle. FCU: flexor carpi ulnaris muscle; UN: ulnar nerve; UA: ulnar artery.
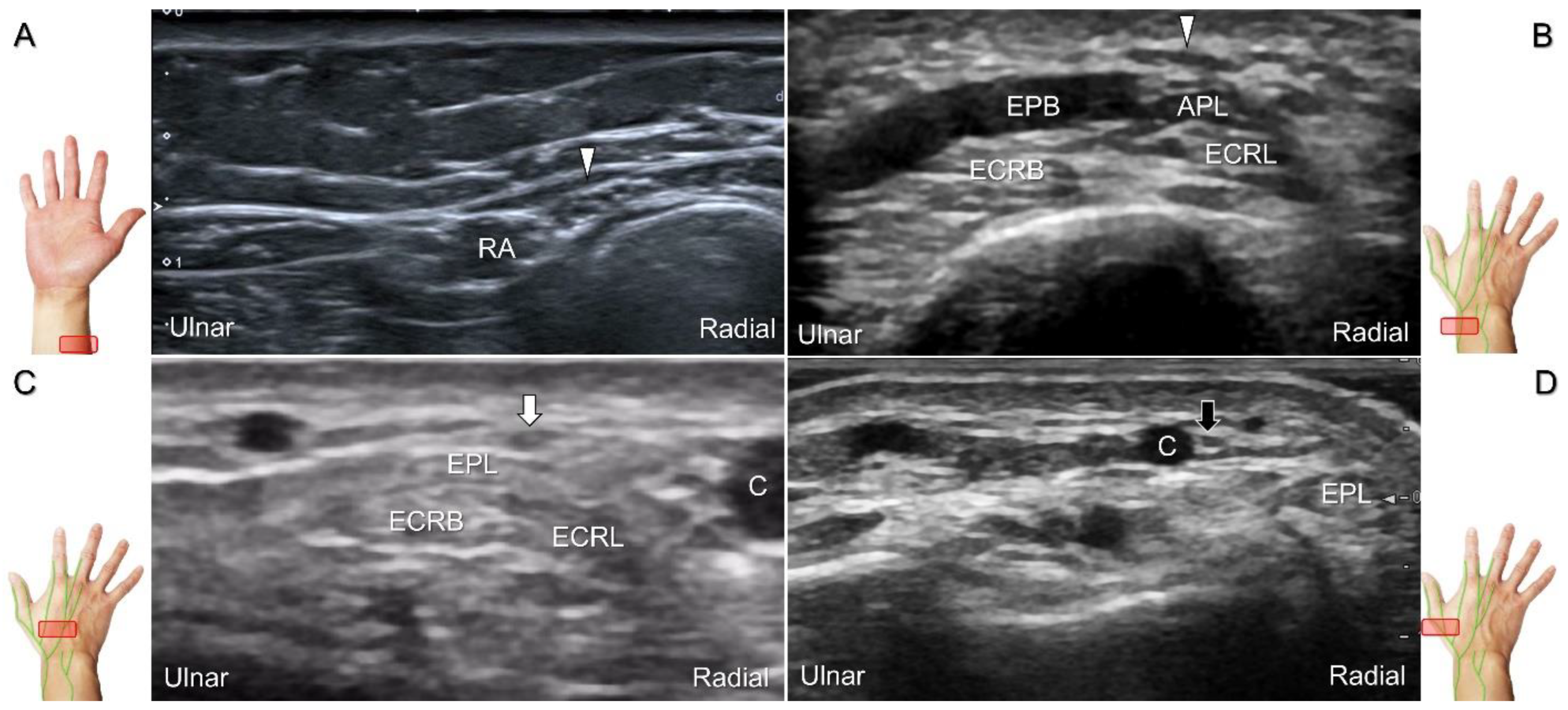
Figure 21.
Sonographic imaging (short-axis view) of the superficial radial nerve from the distal third of the supinated forearm (A). With the pronated forearm, the nerve is seen to travel above the proximal intersection junction (B), divide into the dorsomedial branch coursing above the distal intersection junction (C), and the dorsolateral branch running beside the extensor pollicis longus tendon (D). Arrowheads: superficial radial nerve; white arrow: dorsomedial branch; black arrow: dorsolateral branch. RA: radial artery; APL: abductor pollicis longus tendon; EPB: extensor pollicis brevis tendon; ECRL: extensor carpi radialis longus tendon; ECRB: extensor carpi radialis brevis tendon; EPL: extensor pollicis longus tendon; C: cephalic vein.
Figure 21.
Sonographic imaging (short-axis view) of the superficial radial nerve from the distal third of the supinated forearm (A). With the pronated forearm, the nerve is seen to travel above the proximal intersection junction (B), divide into the dorsomedial branch coursing above the distal intersection junction (C), and the dorsolateral branch running beside the extensor pollicis longus tendon (D). Arrowheads: superficial radial nerve; white arrow: dorsomedial branch; black arrow: dorsolateral branch. RA: radial artery; APL: abductor pollicis longus tendon; EPB: extensor pollicis brevis tendon; ECRL: extensor carpi radialis longus tendon; ECRB: extensor carpi radialis brevis tendon; EPL: extensor pollicis longus tendon; C: cephalic vein.
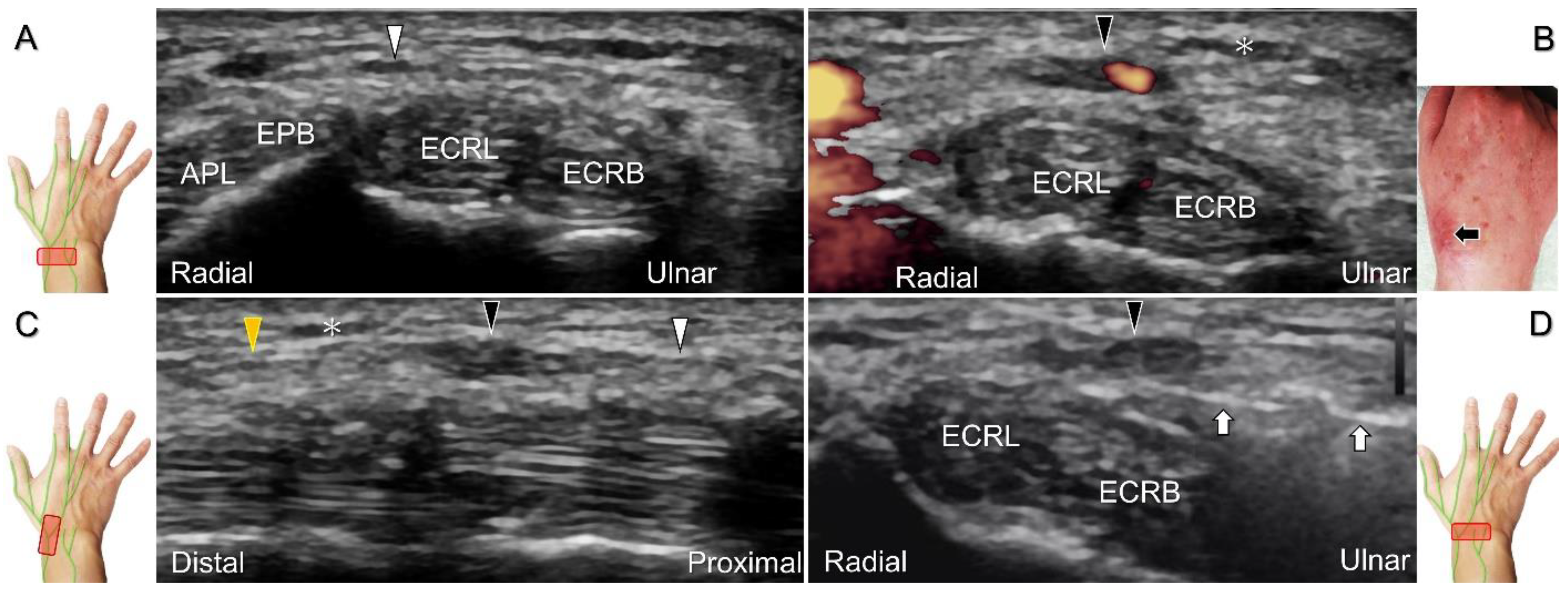
Figure 22.
Sonographic imaging (short-axis view) of the dorsolateral branch of the superficial radial nerve at normal (A), swollen (B), and compressed (C) segments. White arrowhead: normal segment; black arrowhead: swollen segment; orange arrowhead: entrapped segment. ECRL: extensor carpi radialis longus tendon; ECRB: extensor carpi radialis brevis tendon; EPL: extensor pollicis longus tendon.
Figure 22.
Sonographic imaging (short-axis view) of the dorsolateral branch of the superficial radial nerve at normal (A), swollen (B), and compressed (C) segments. White arrowhead: normal segment; black arrowhead: swollen segment; orange arrowhead: entrapped segment. ECRL: extensor carpi radialis longus tendon; ECRB: extensor carpi radialis brevis tendon; EPL: extensor pollicis longus tendon.
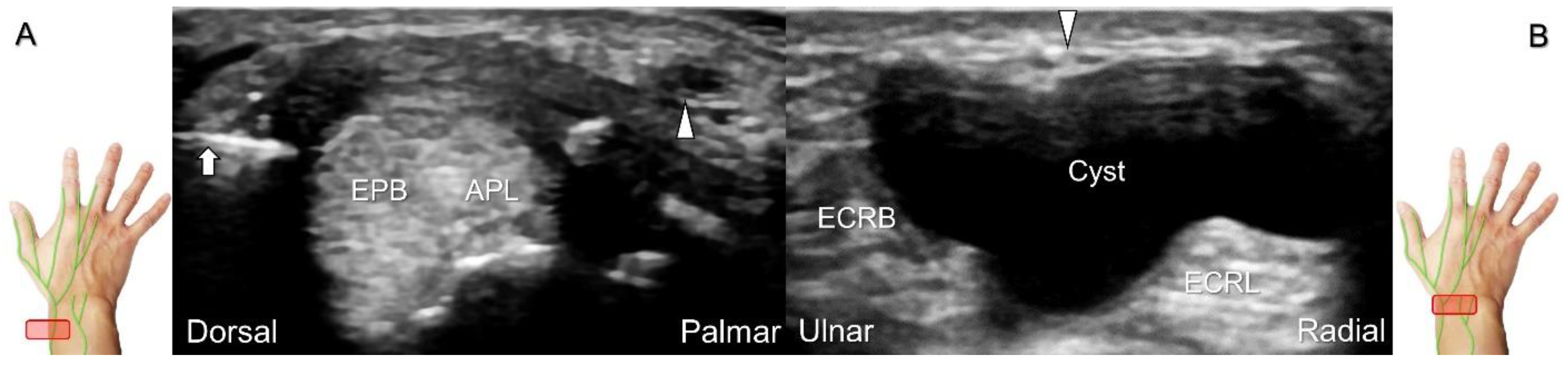
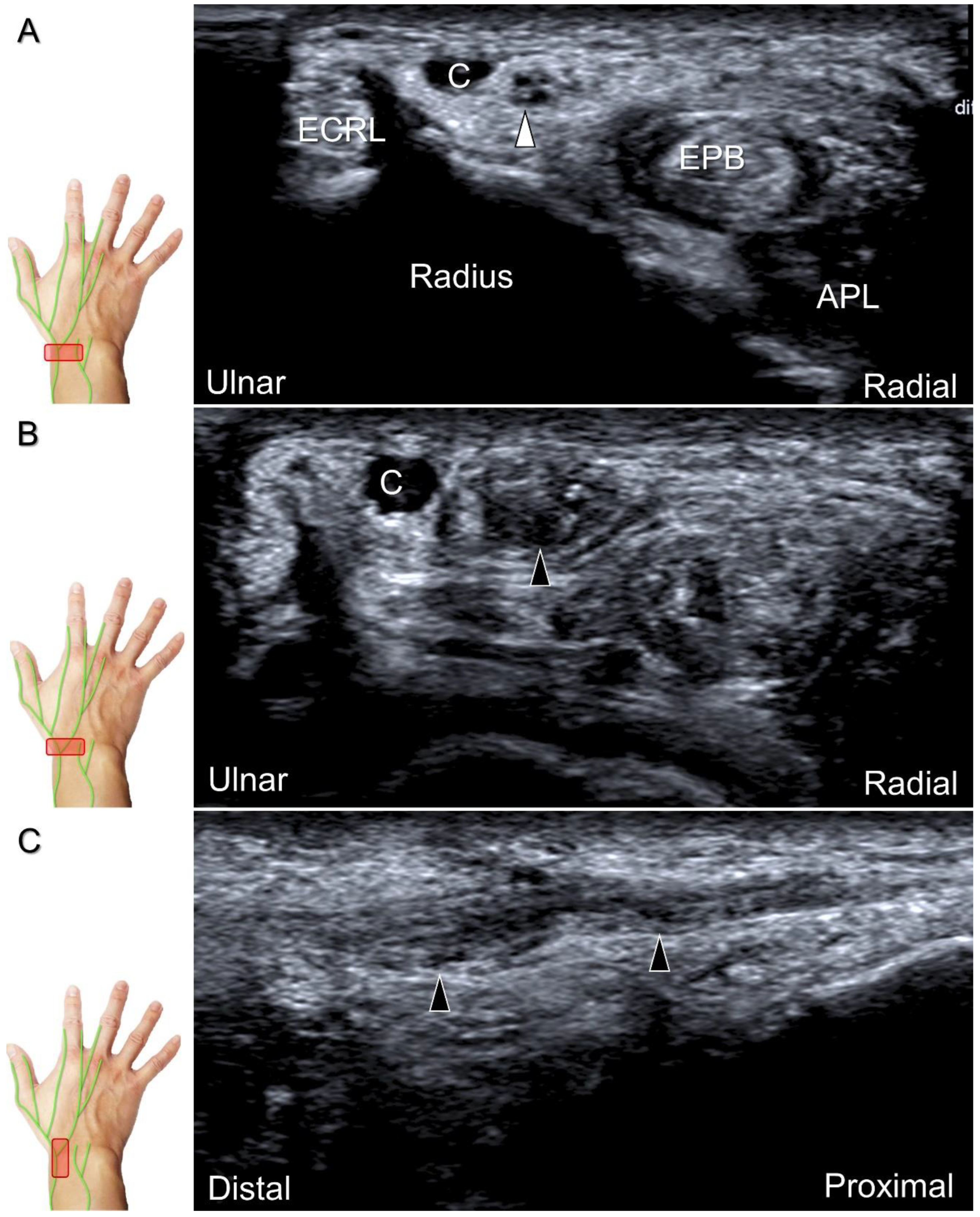
Figure 23.
Sonographic imaging of the superficial radial nerve beside the first extensor compartment of the wrist (A), and a ganglion cyst over the second extensor compartment of the wrist (B). White arrowheads: superficial radial nerve; white arrow: needle. APL: abductor pollicis longus tendon; EPB: extensor pollicis brevis tendon; ECRL: extensor carpi radialis longus tendon; ECRB: extensor carpi radialis brevis tendon.
Figure 23.
Sonographic imaging of the superficial radial nerve beside the first extensor compartment of the wrist (A), and a ganglion cyst over the second extensor compartment of the wrist (B). White arrowheads: superficial radial nerve; white arrow: needle. APL: abductor pollicis longus tendon; EPB: extensor pollicis brevis tendon; ECRL: extensor carpi radialis longus tendon; ECRB: extensor carpi radialis brevis tendon.
Figure 24.
Sonographic imaging of the superficial radial nerve entrapment due to a post-surgical scar. Short-axis imaging at the normal (A) and the swollen (B) segment proximal to the entrapment. The normal, swollen, and entrapped segments of the nerve are seen in long-axis view (C). Ultrasound-guided hydrodissection of the nerve from the ulnar aspect (D). White arrowheads: normal segment; black arrowheads: swollen segment; orange arrowhead: entrapped segment; white arrows: needle; black arrow: scars on the skin; asterisk: scars in the subcutaneous tissue; APL: abductor pollicis longus tendon; EPB: extensor pollicis brevis tendon; ECRL: extensor carpi radialis longus tendon; ECRB: extensor carpi radialis brevis tendon.
Figure 24.
Sonographic imaging of the superficial radial nerve entrapment due to a post-surgical scar. Short-axis imaging at the normal (A) and the swollen (B) segment proximal to the entrapment. The normal, swollen, and entrapped segments of the nerve are seen in long-axis view (C). Ultrasound-guided hydrodissection of the nerve from the ulnar aspect (D). White arrowheads: normal segment; black arrowheads: swollen segment; orange arrowhead: entrapped segment; white arrows: needle; black arrow: scars on the skin; asterisk: scars in the subcutaneous tissue; APL: abductor pollicis longus tendon; EPB: extensor pollicis brevis tendon; ECRL: extensor carpi radialis longus tendon; ECRB: extensor carpi radialis brevis tendon.
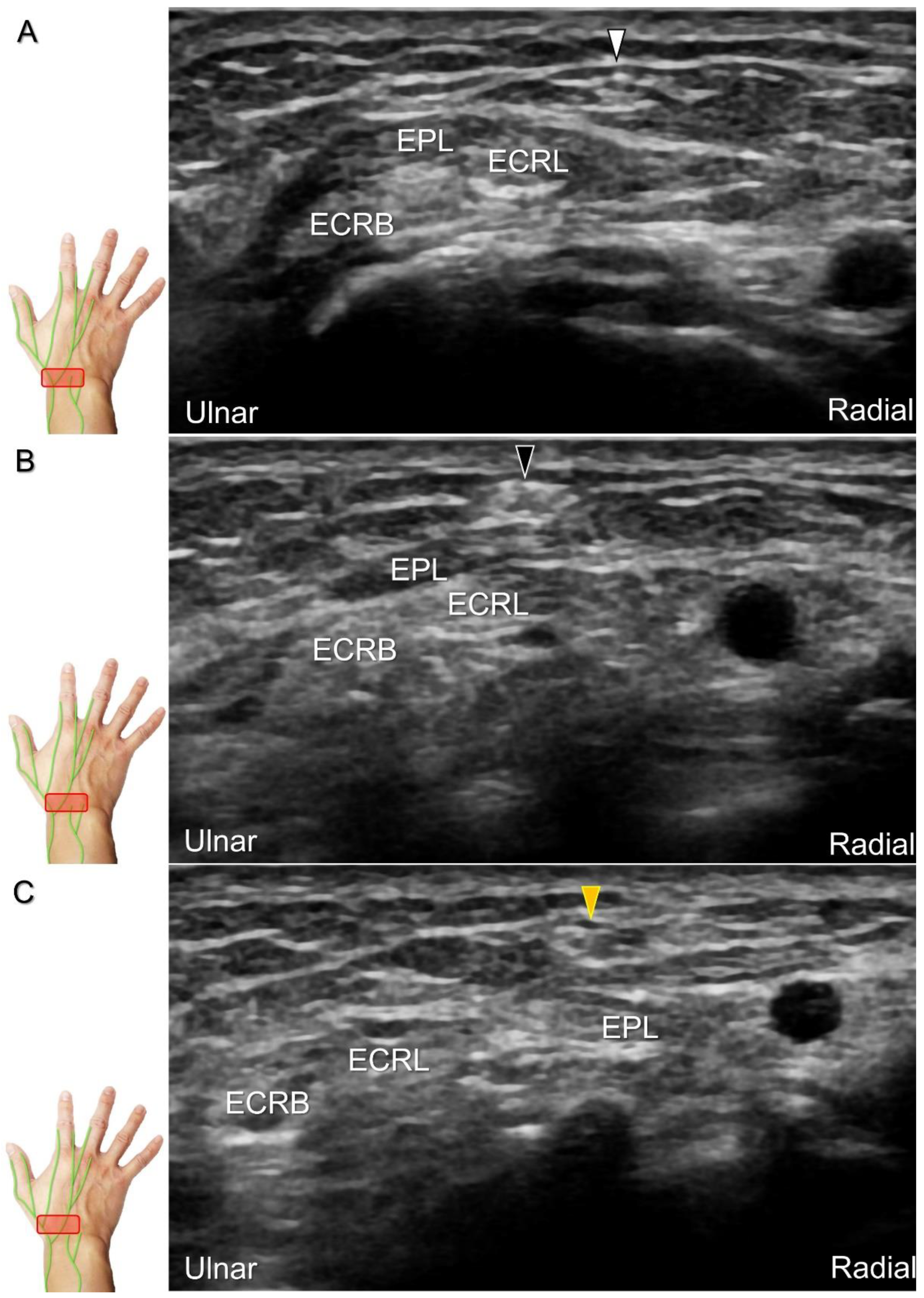
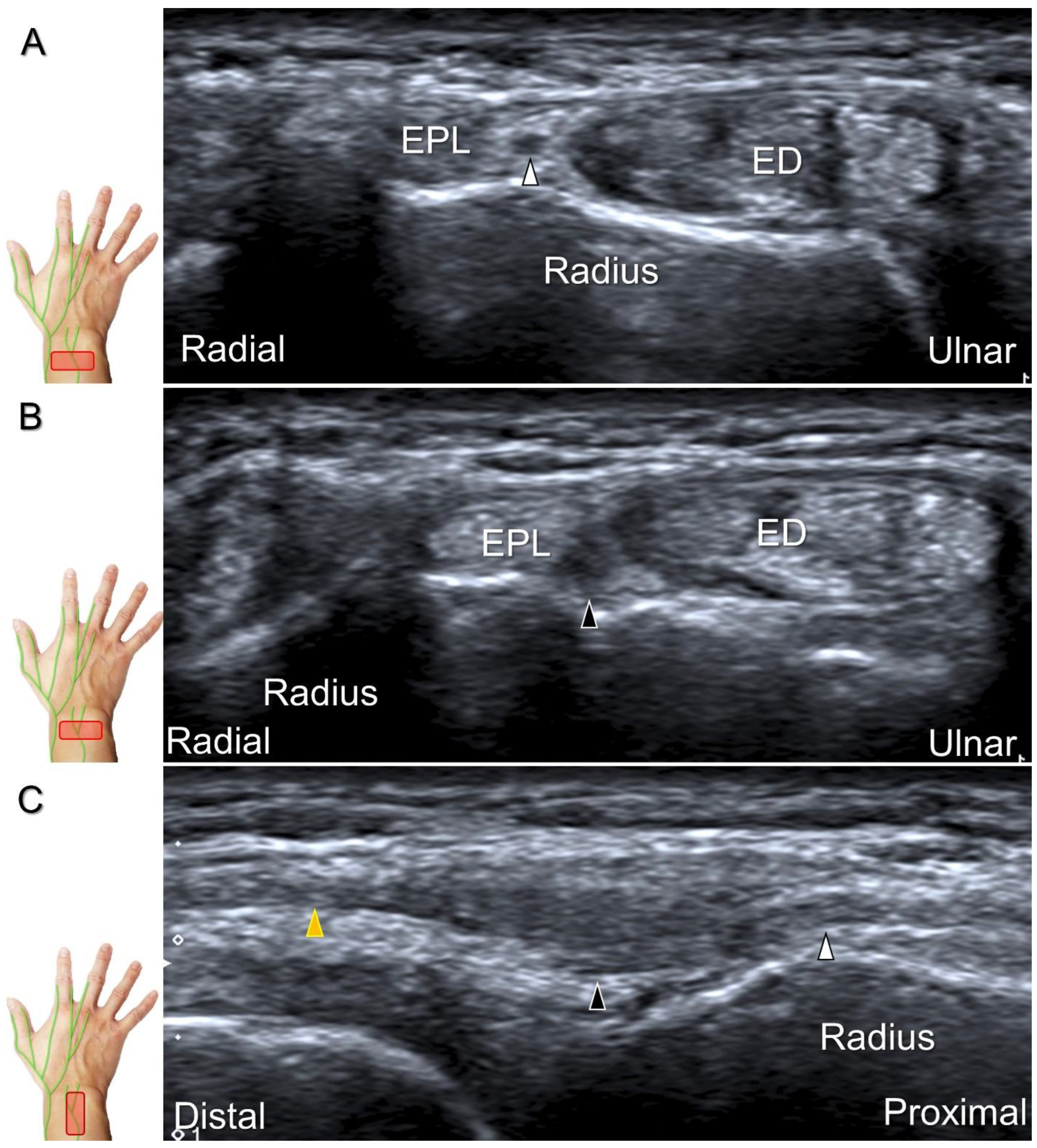
Figure 26.
Sonographic imaging (short-axis view) of the dorsal interosseus nerve from the normal (A) to the swollen (B) segment proximal to the entrapment site. Normal, swollen, and compressed segments of the nerve are seen in long-axis view (C). White arrowhead: normal segment; black arrowhead: swollen segment; yellow arrowhead: entrapped segment; EPL: extensor pollicis longus tendon; ED: extensor digitorum tendon.
Figure 26.
Sonographic imaging (short-axis view) of the dorsal interosseus nerve from the normal (A) to the swollen (B) segment proximal to the entrapment site. Normal, swollen, and compressed segments of the nerve are seen in long-axis view (C). White arrowhead: normal segment; black arrowhead: swollen segment; yellow arrowhead: entrapped segment; EPL: extensor pollicis longus tendon; ED: extensor digitorum tendon.
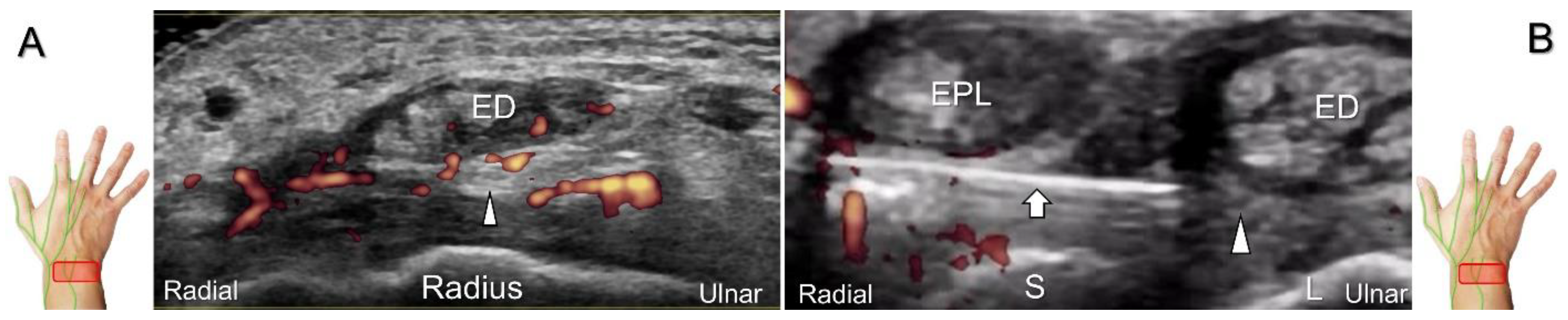
Figure 27.
Sonographic imaging (short-axis view) is performed to assess the posterior interosseus nerve entrapment due to synovitis in rheumatoid arthritis (A). Ultrasound-guided injection (B). Arrowheads: posterior interosseus nerve; arrow: needle; EPL: extensor pollicis longus tendon; ED: extensor digitorum communis tendon; S: scaphoid; L: lunate.
Figure 27.
Sonographic imaging (short-axis view) is performed to assess the posterior interosseus nerve entrapment due to synovitis in rheumatoid arthritis (A). Ultrasound-guided injection (B). Arrowheads: posterior interosseus nerve; arrow: needle; EPL: extensor pollicis longus tendon; ED: extensor digitorum communis tendon; S: scaphoid; L: lunate.
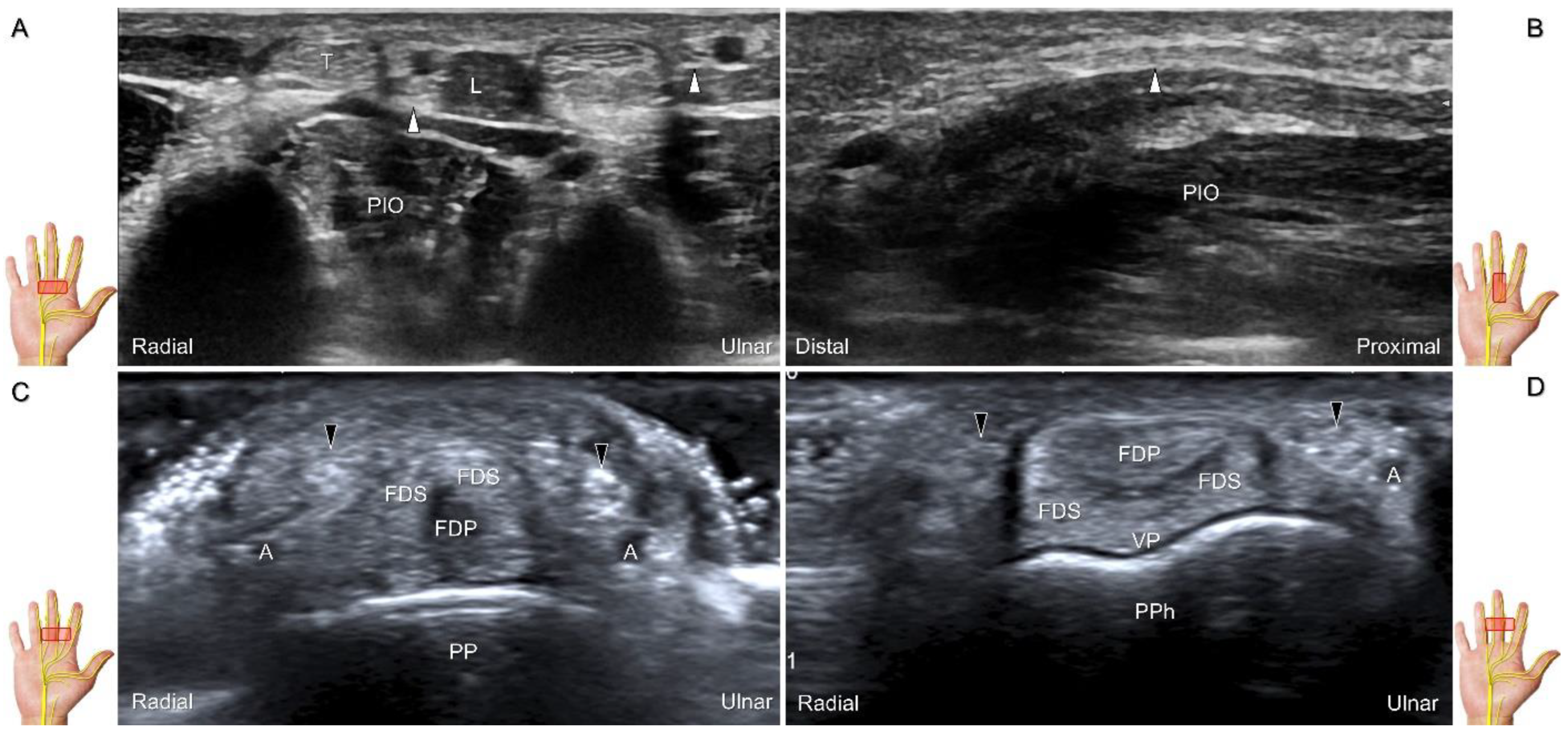
Figure 28.
Sonographic imaging of the palmar common digital nerves in short-axis (A) and long-axis (B) views. Palmar proper digital nerves from the base (C) to the head of the proximal phalanx (D). White arrowheads: palmar common digital nerves; black arrowheads: palmar proper digital nerves. T: flexor tendon; L: lumbricalis muscle; PIO: palmar interosseous muscle; FDS: flexor digitorum superficialis tendon; FDP: flexor digitorum profundus tendon; A: artery; VP: volar plate; PP: proximal phalanx; PPh: head of the proximal phalanx.
Figure 28.
Sonographic imaging of the palmar common digital nerves in short-axis (A) and long-axis (B) views. Palmar proper digital nerves from the base (C) to the head of the proximal phalanx (D). White arrowheads: palmar common digital nerves; black arrowheads: palmar proper digital nerves. T: flexor tendon; L: lumbricalis muscle; PIO: palmar interosseous muscle; FDS: flexor digitorum superficialis tendon; FDP: flexor digitorum profundus tendon; A: artery; VP: volar plate; PP: proximal phalanx; PPh: head of the proximal phalanx.
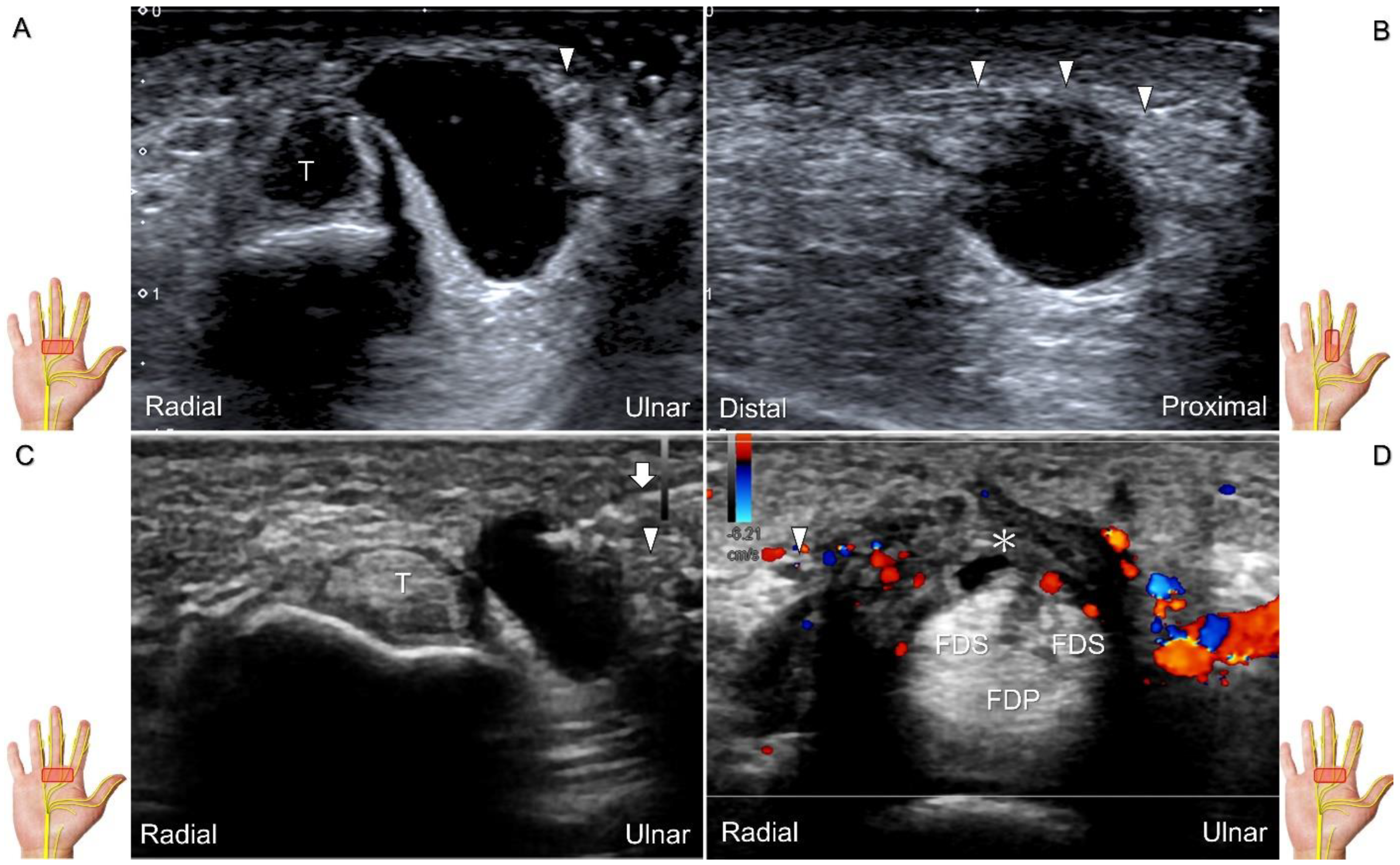
Figure 29.
Ultrasound images demonstrate the entrapment of the palmar common digital nerve due to a ganglion seen in short-axis (A) and long-axis (B) views. Ultrasound-guided aspiration (C). Nerve entrapment due to annular ligament tear (asterisk) following an iatrogenic injury (D). Arrowheads: palmar common digital nerve; Arrow: needle; T: flexor tendon; FDS: flexor digitorum superficialis tendon; FDP: flexor digitorum profundus tendon.
Figure 29.
Ultrasound images demonstrate the entrapment of the palmar common digital nerve due to a ganglion seen in short-axis (A) and long-axis (B) views. Ultrasound-guided aspiration (C). Nerve entrapment due to annular ligament tear (asterisk) following an iatrogenic injury (D). Arrowheads: palmar common digital nerve; Arrow: needle; T: flexor tendon; FDS: flexor digitorum superficialis tendon; FDP: flexor digitorum profundus tendon.
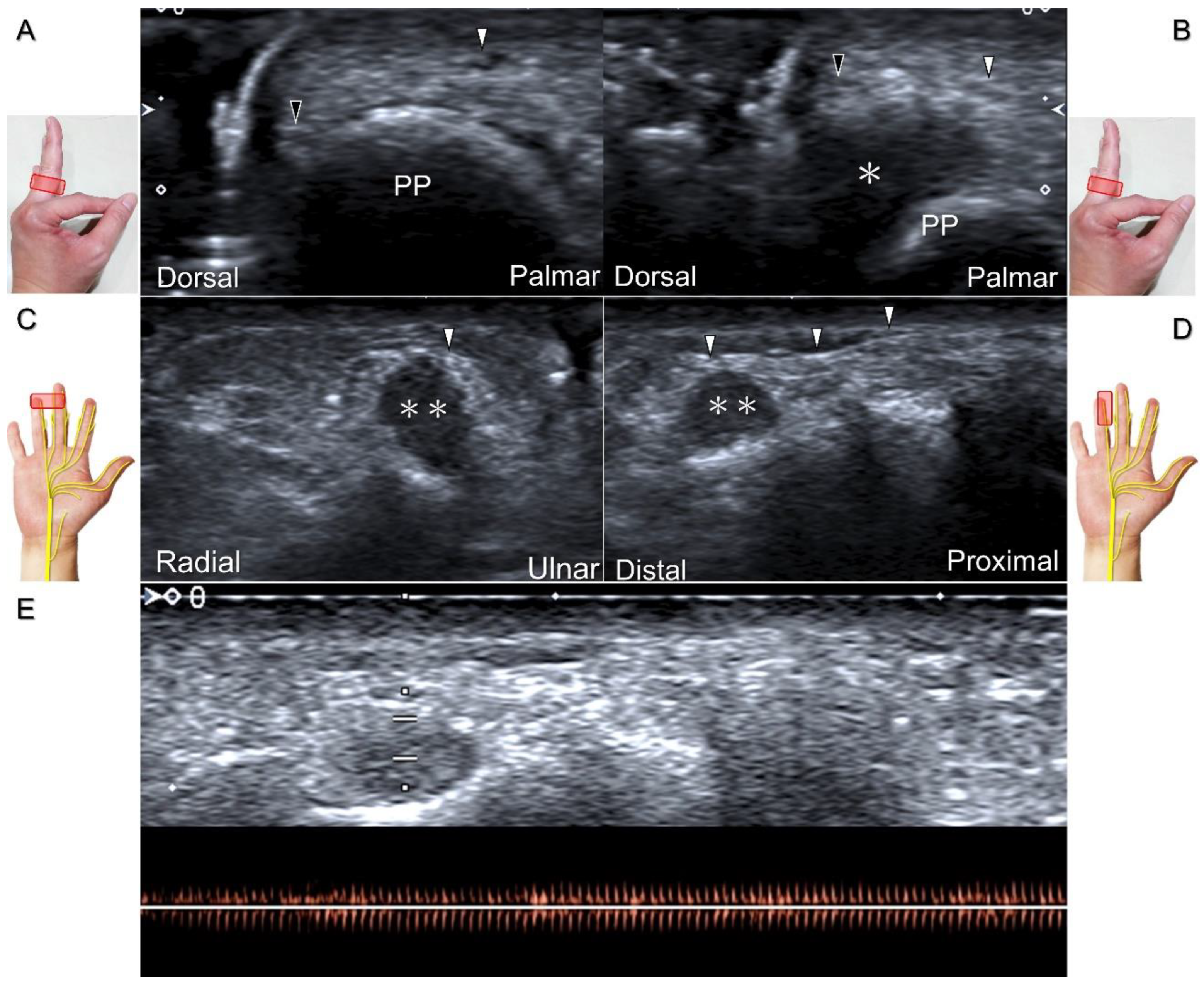
Figure 30.
In comparison to the healthy side (A), short-axis imaging (B) shows irritation of both the palmar and dorsal proper digital nerves due to a fibroma (asterisk). Short-axis (C) and long-axis (D) imaging demonstrates irritation of the palmar proper digital nerve due to a hemangioma. Spectral Doppler mode (E) confirms the hemangioma. White arrowhead: palmar proper digital nerve; black arrowhead: dorsal proper digital nerve; double asterisk: hemangioma; PP: proximal phalanx.
Figure 30.
In comparison to the healthy side (A), short-axis imaging (B) shows irritation of both the palmar and dorsal proper digital nerves due to a fibroma (asterisk). Short-axis (C) and long-axis (D) imaging demonstrates irritation of the palmar proper digital nerve due to a hemangioma. Spectral Doppler mode (E) confirms the hemangioma. White arrowhead: palmar proper digital nerve; black arrowhead: dorsal proper digital nerve; double asterisk: hemangioma; PP: proximal phalanx.
Figure 31.
Sonographic imaging of the neuroma of the palmar proper digital nerve in short-axis (A) and long-axis (B) views. White arrowheads: normal segments of the palmar proper digital nerve; black arrowhead: neuroma. FPL: flexor pollicis longus tendon.
Figure 31.
Sonographic imaging of the neuroma of the palmar proper digital nerve in short-axis (A) and long-axis (B) views. White arrowheads: normal segments of the palmar proper digital nerve; black arrowhead: neuroma. FPL: flexor pollicis longus tendon.
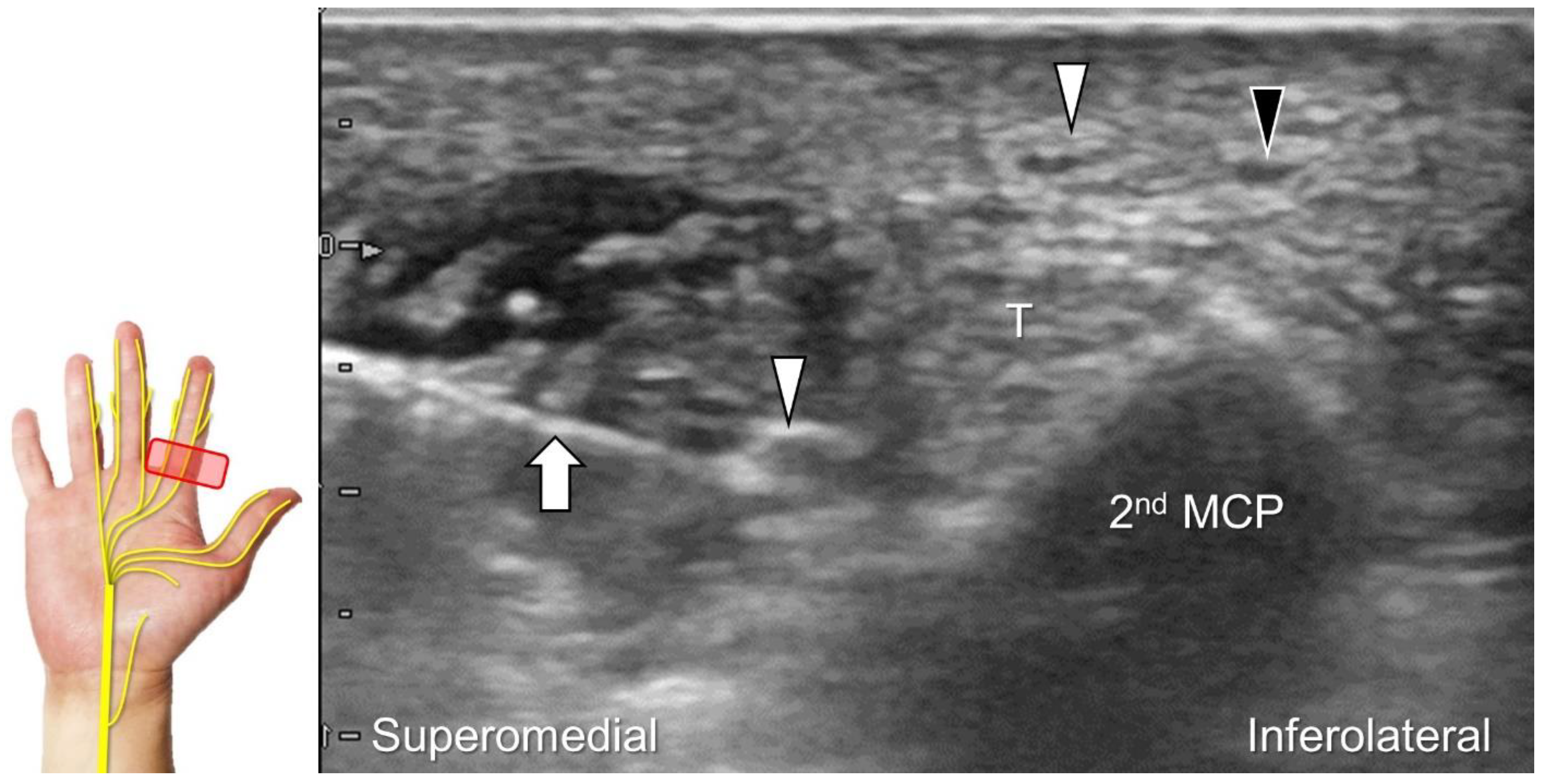
Figure 32.
In-plane ulnar to radial approach is used for injecting the palmar common digital nerve in short-axis view. White arrowheads: palmar common digital nerve; black arrowhead: common palmar digital artery; arrow: needle; T: flexor tendons; 2nd MCP: second metacarpal.
Figure 32.
In-plane ulnar to radial approach is used for injecting the palmar common digital nerve in short-axis view. White arrowheads: palmar common digital nerve; black arrowhead: common palmar digital artery; arrow: needle; T: flexor tendons; 2nd MCP: second metacarpal.
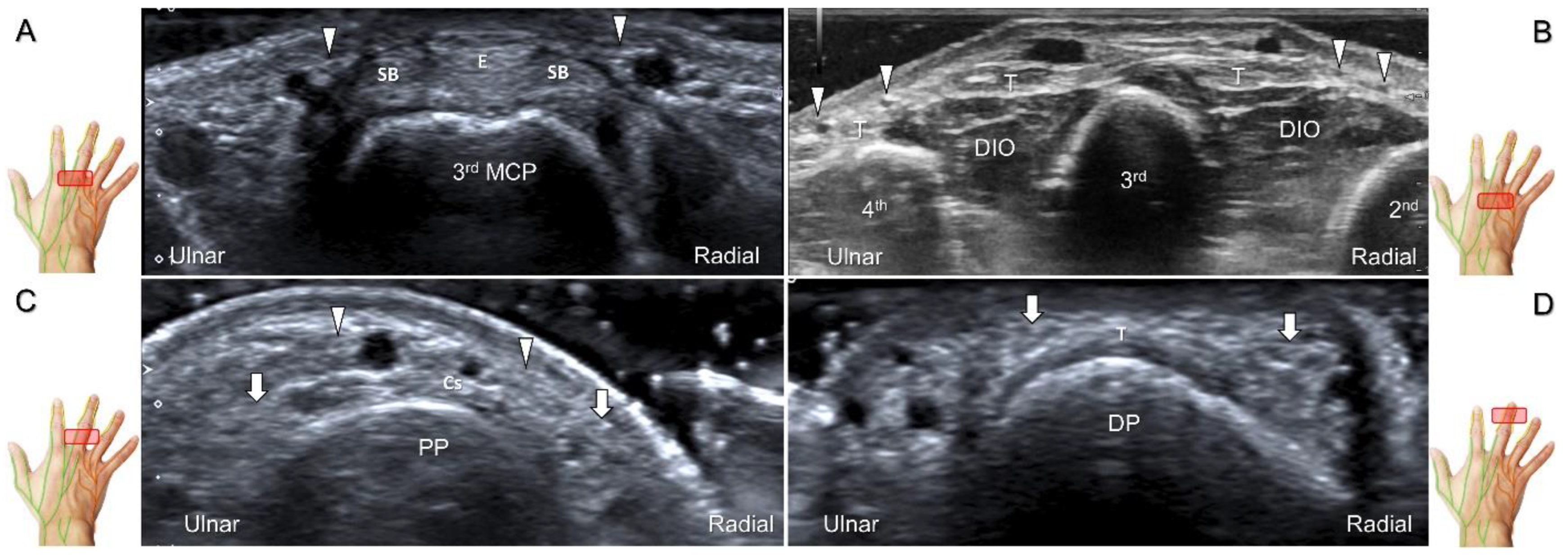
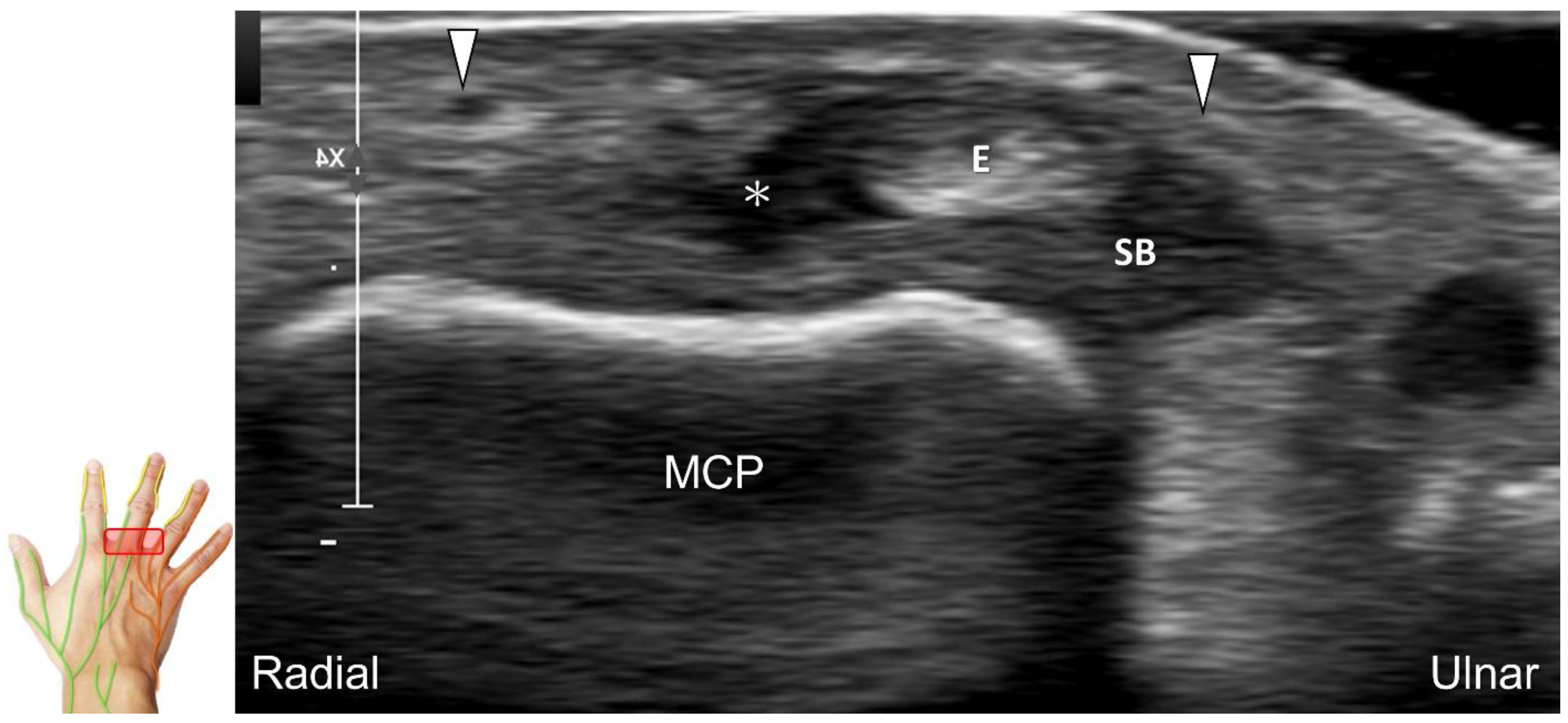
Figure 33.
Sonographic imaging of the dorsal common digital nerve on the metacarpal bone (A), toward the metacarpal head (B). Dorsal proper digital nerves on the proximal phalanx (C), and the terminal nerve originating from the palmar proper digital nerve on the distal phalanx of third finger (D). Arrowheads: dorsal common digital nerve; arrows: palmar proper digital nerve. MCP: metacarpal bone; SB: sagittal band; E: extensor tendon; Cs: central slip; PP: proximal phalanx; T: terminal band; DP: distal phalanx; DIO, dorsal interosseous muscle.
Figure 33.
Sonographic imaging of the dorsal common digital nerve on the metacarpal bone (A), toward the metacarpal head (B). Dorsal proper digital nerves on the proximal phalanx (C), and the terminal nerve originating from the palmar proper digital nerve on the distal phalanx of third finger (D). Arrowheads: dorsal common digital nerve; arrows: palmar proper digital nerve. MCP: metacarpal bone; SB: sagittal band; E: extensor tendon; Cs: central slip; PP: proximal phalanx; T: terminal band; DP: distal phalanx; DIO, dorsal interosseous muscle.
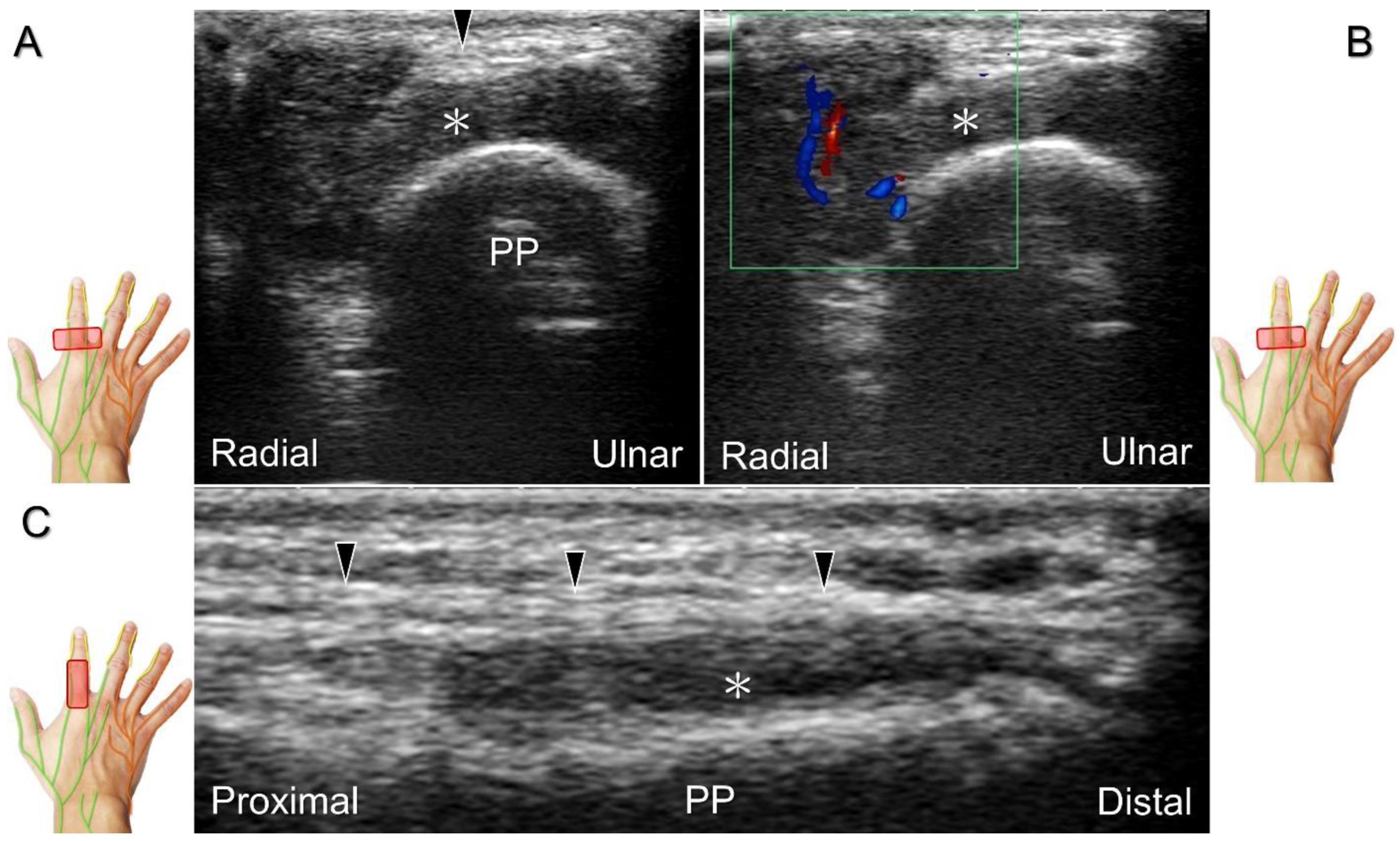
Figure 34.
In the short-axis view, the proper digital nerve is seen as irritated by a giant cell tumor (A) with increased vascular signals (B). The association between the proper digital nerve and the tumor is delineated in the long-axis view (C). Black arrowheads: proper digital nerve; PP: proximal phalanx; *: giant cell tumor.
Figure 34.
In the short-axis view, the proper digital nerve is seen as irritated by a giant cell tumor (A) with increased vascular signals (B). The association between the proper digital nerve and the tumor is delineated in the long-axis view (C). Black arrowheads: proper digital nerve; PP: proximal phalanx; *: giant cell tumor.
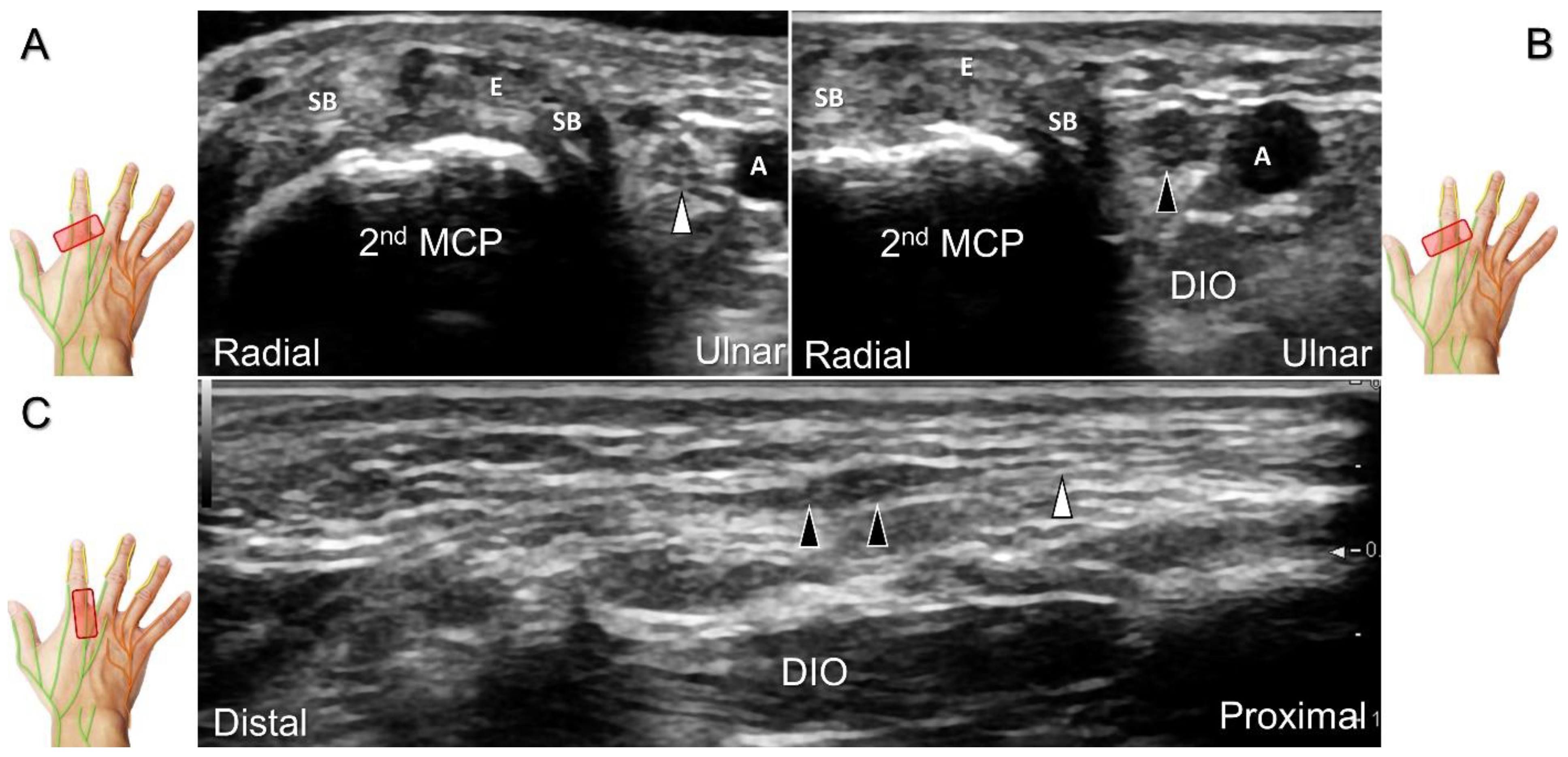
Figure 35.
Sonographic imaging reveals irritation of the ulnar aspect of the dorsal common digital nerve due to extensor tendon subluxation resulting from a tear in the sagittal band. Arrowheads: dorsal common digital nerve; asterisk: tear of the sagittal band. SB: sagittal band; E: extensor tendon; MCP: metacarpal bone.
Figure 35.
Sonographic imaging reveals irritation of the ulnar aspect of the dorsal common digital nerve due to extensor tendon subluxation resulting from a tear in the sagittal band. Arrowheads: dorsal common digital nerve; asterisk: tear of the sagittal band. SB: sagittal band; E: extensor tendon; MCP: metacarpal bone.
Figure 36.
Sonographic imaging (short-axis view) for a neuroma of the dorsal common digital nerve, proximal site (A) and the site of the lesion (B). Long-axis imaging of the nerve/neuroma (C). White arrowhead: normal dorsal common digital nerve; black arrowheads: neuroma. SB: sagittal band; E: extensor tendon; MCP: metacarpal bone; DIO: dorsal interosseous muscle; A: artery.
Figure 36.
Sonographic imaging (short-axis view) for a neuroma of the dorsal common digital nerve, proximal site (A) and the site of the lesion (B). Long-axis imaging of the nerve/neuroma (C). White arrowhead: normal dorsal common digital nerve; black arrowheads: neuroma. SB: sagittal band; E: extensor tendon; MCP: metacarpal bone; DIO: dorsal interosseous muscle; A: artery.
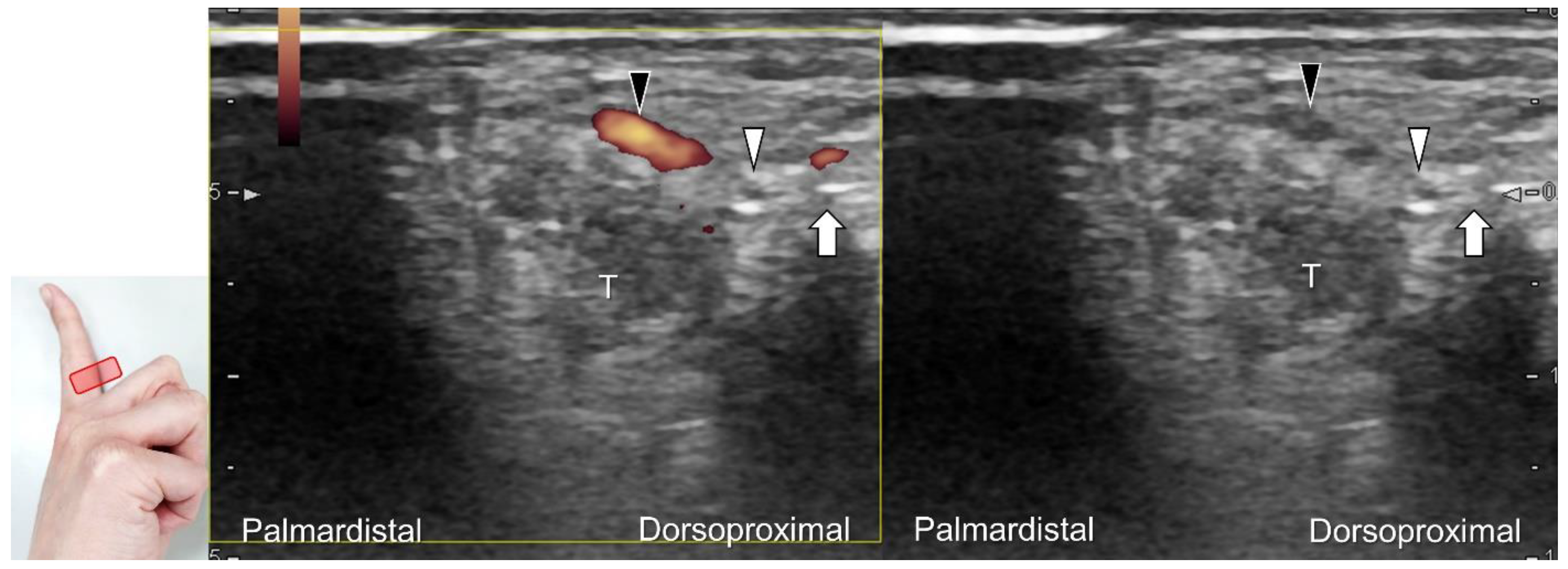
Figure 37.
Ultrasound-guided injection to the dorsal proper digital nerve in its short axis with the dual imaging mode (Doppler vs. B mode). White arrowhead: dorsal proper digital nerve; black arrowhead: dorsal proper digital artery; arrow: needle. T: flexor tendons.
Figure 37.
Ultrasound-guided injection to the dorsal proper digital nerve in its short axis with the dual imaging mode (Doppler vs. B mode). White arrowhead: dorsal proper digital nerve; black arrowhead: dorsal proper digital artery; arrow: needle. T: flexor tendons.

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




































