

A Cross-Sectional Study of the Dermatological Manifestations of Patients with Fabry Disease and the Assessment of Angiokeratomas with Multimodal Imaging
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Dermoscopy
2.3. Multispectral Imaging
2.4. Non-Linear Optical Microscopy
3. Results
3.1. Diagnosis and Treatment
3.2. Extracutaneous Manifestations
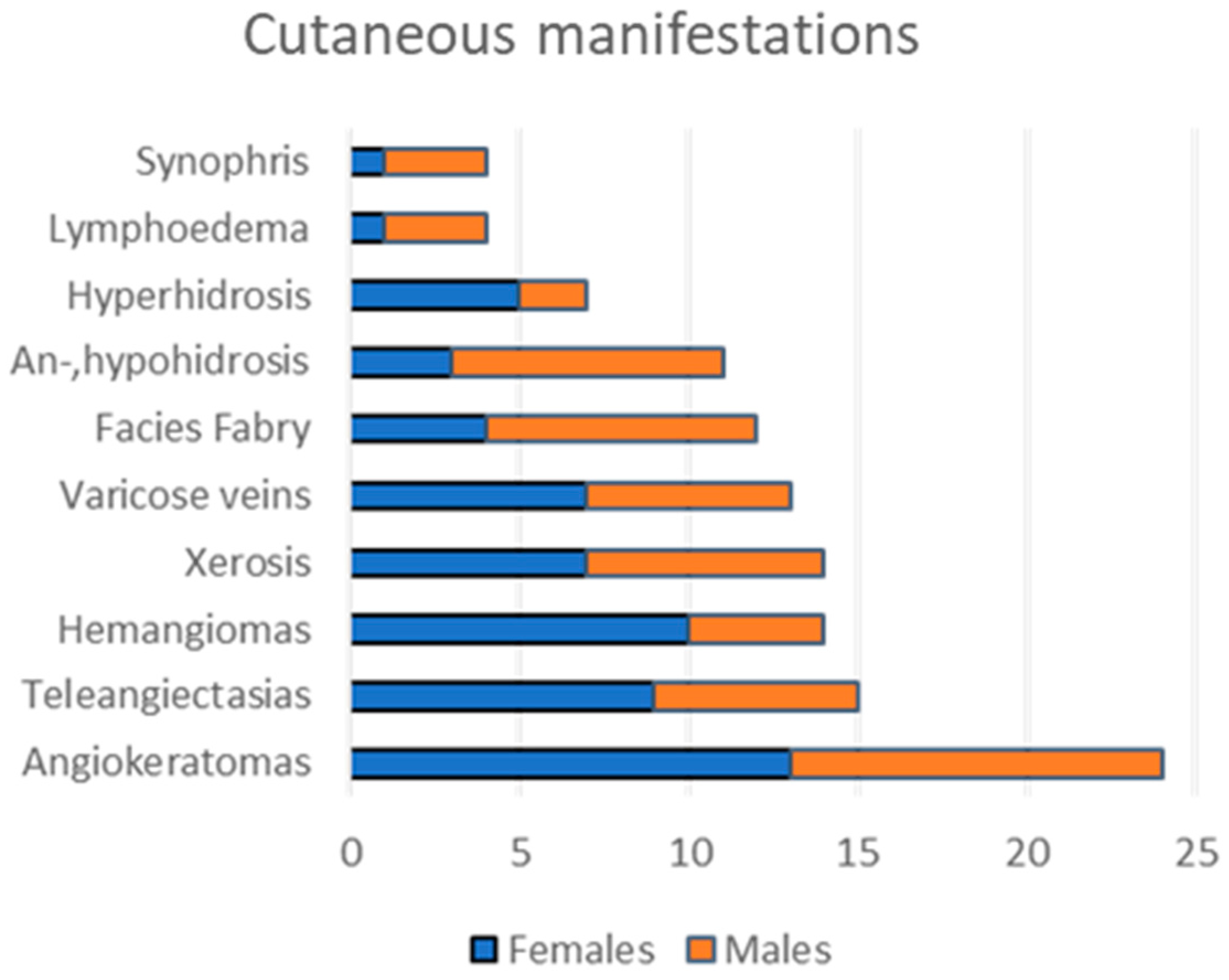
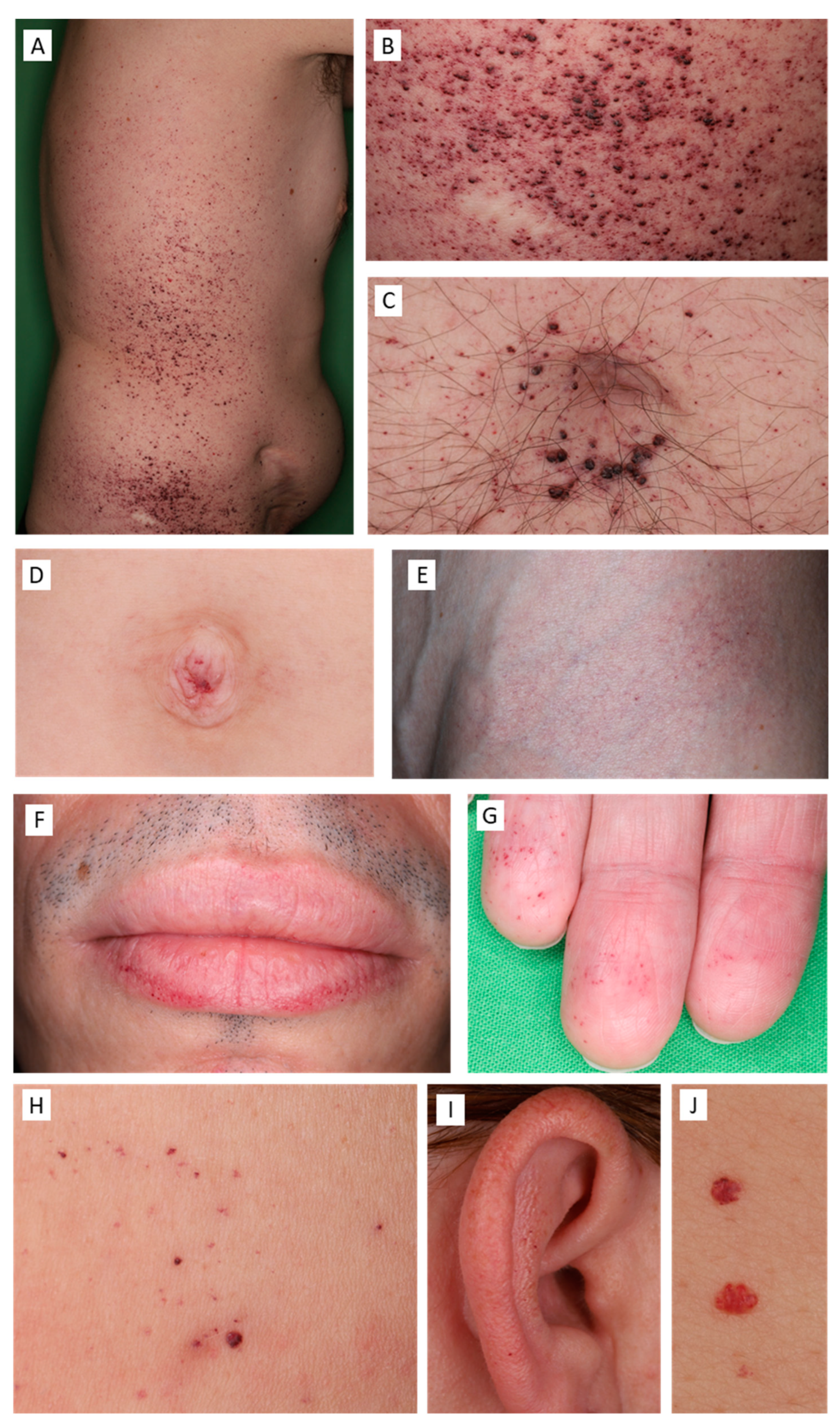
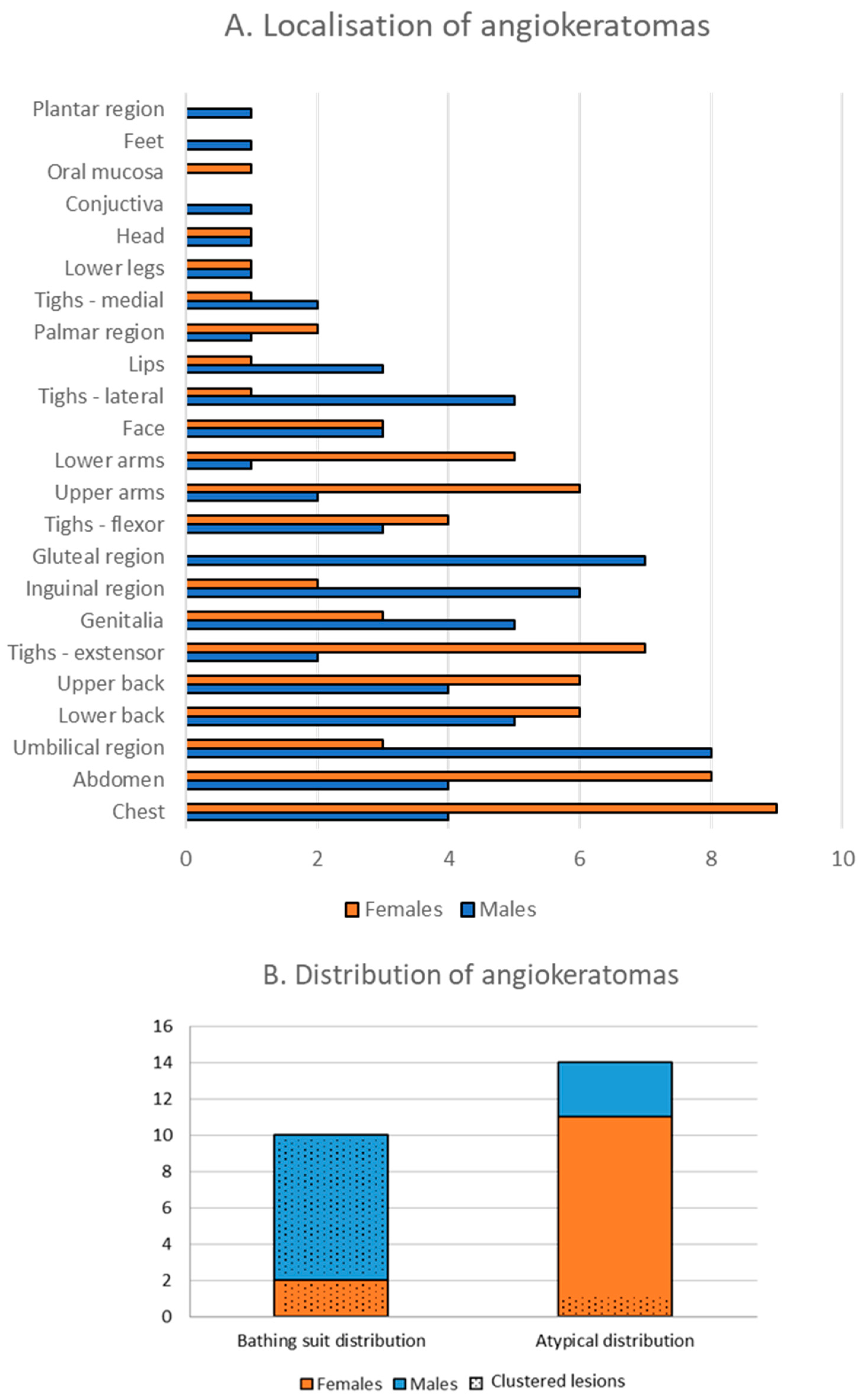
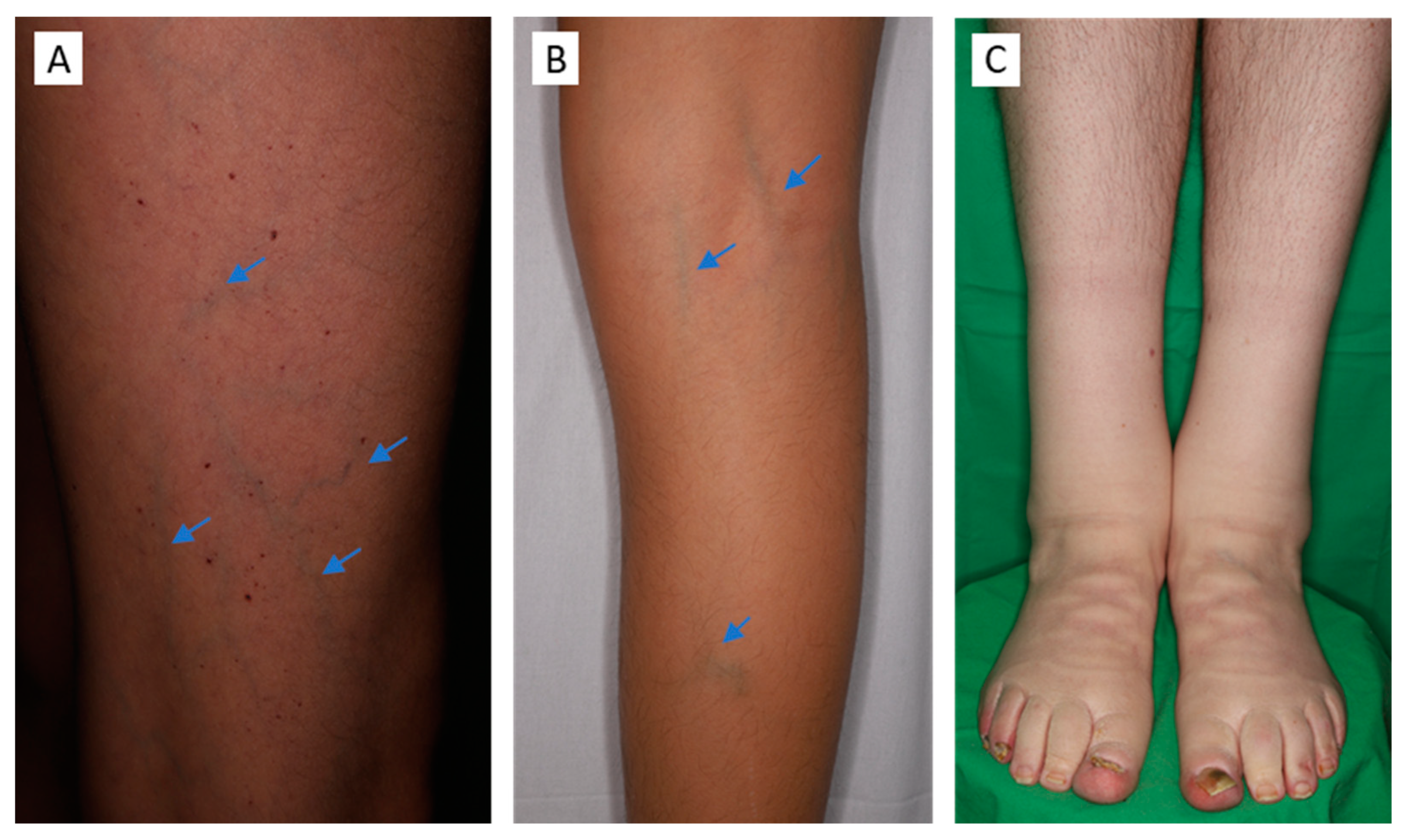
3.3. Cutaneous Findings
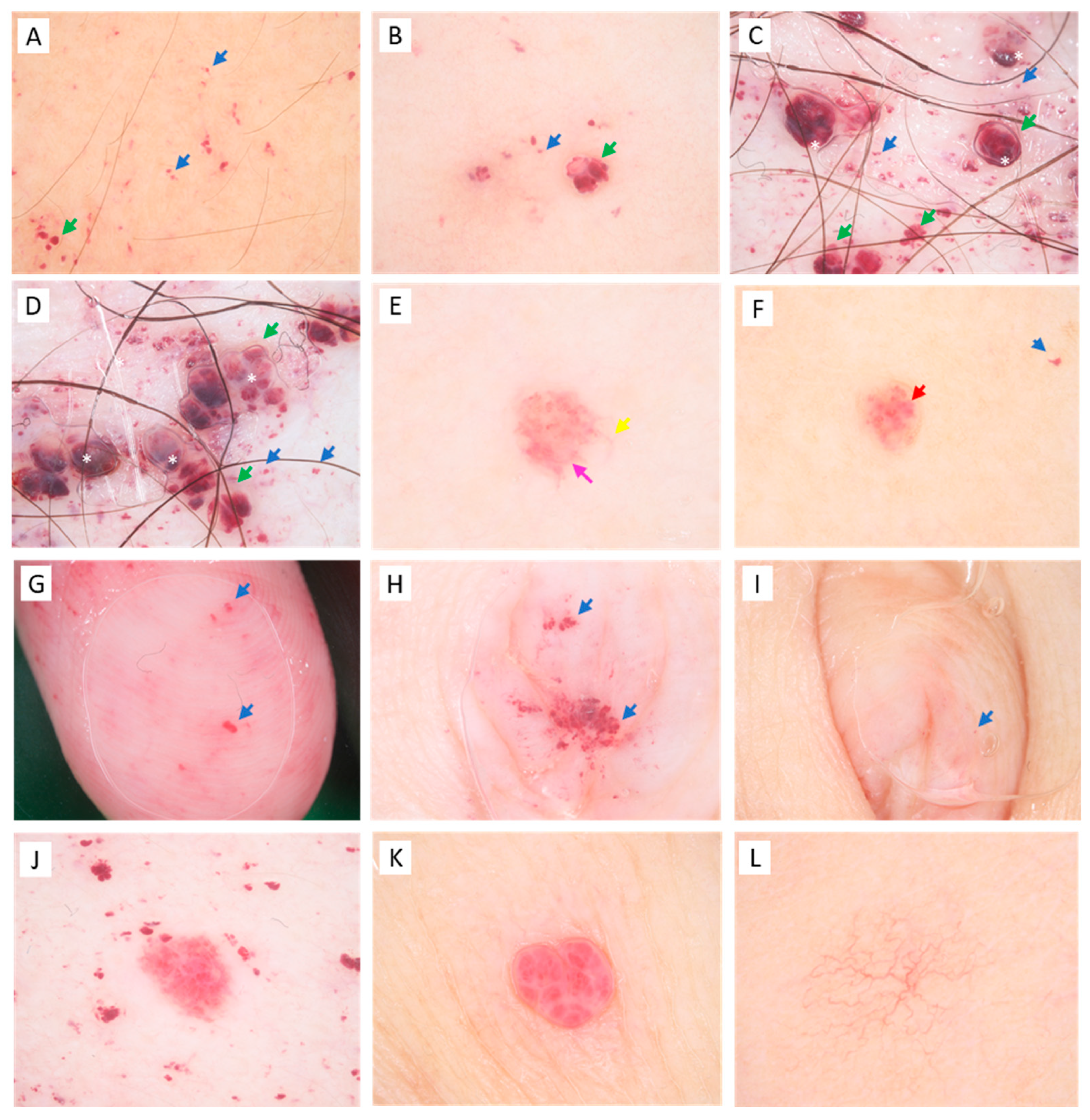
3.4. Dermoscopic Features
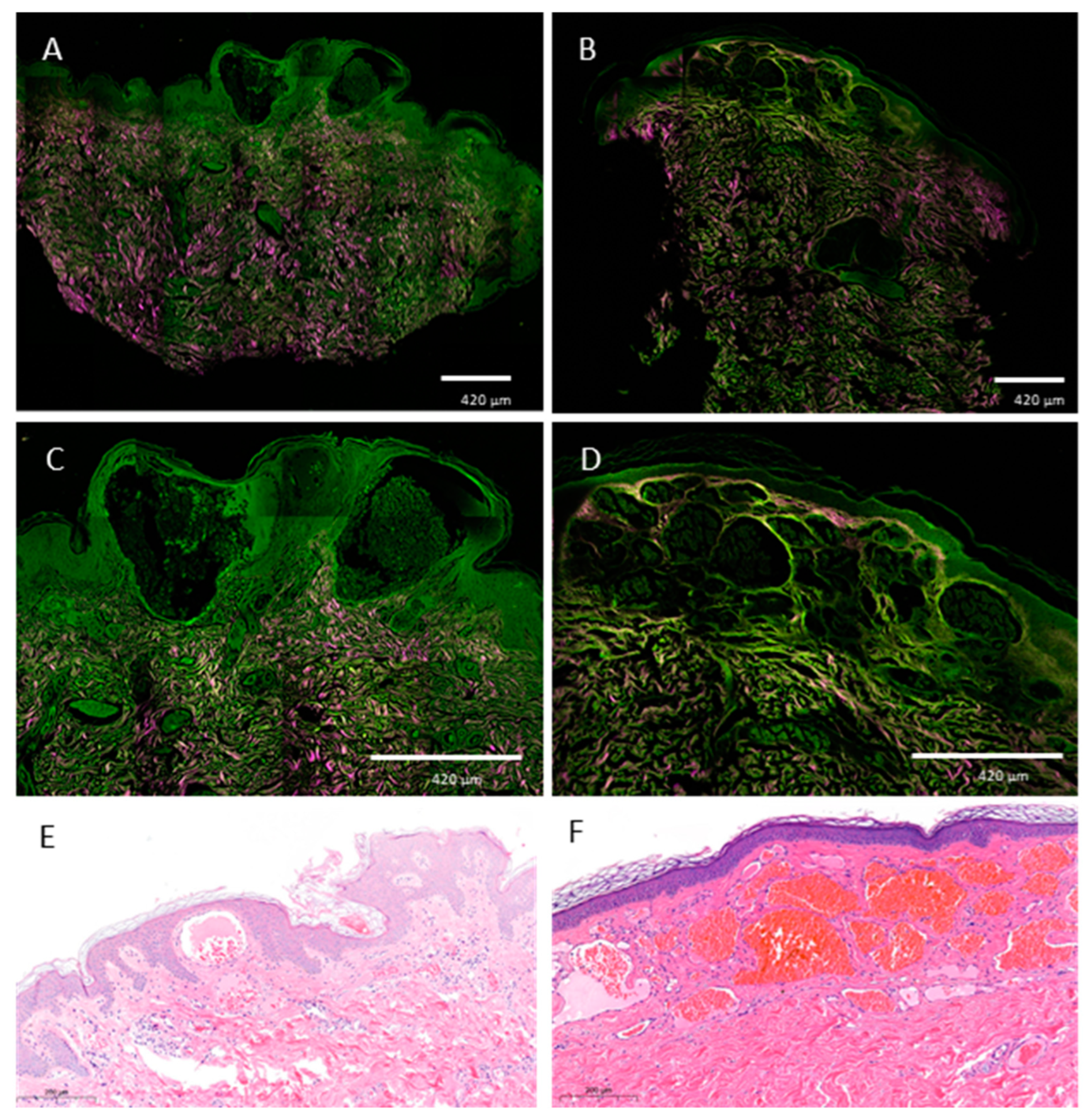
3.5. Non-Linear Microscopic Imaging
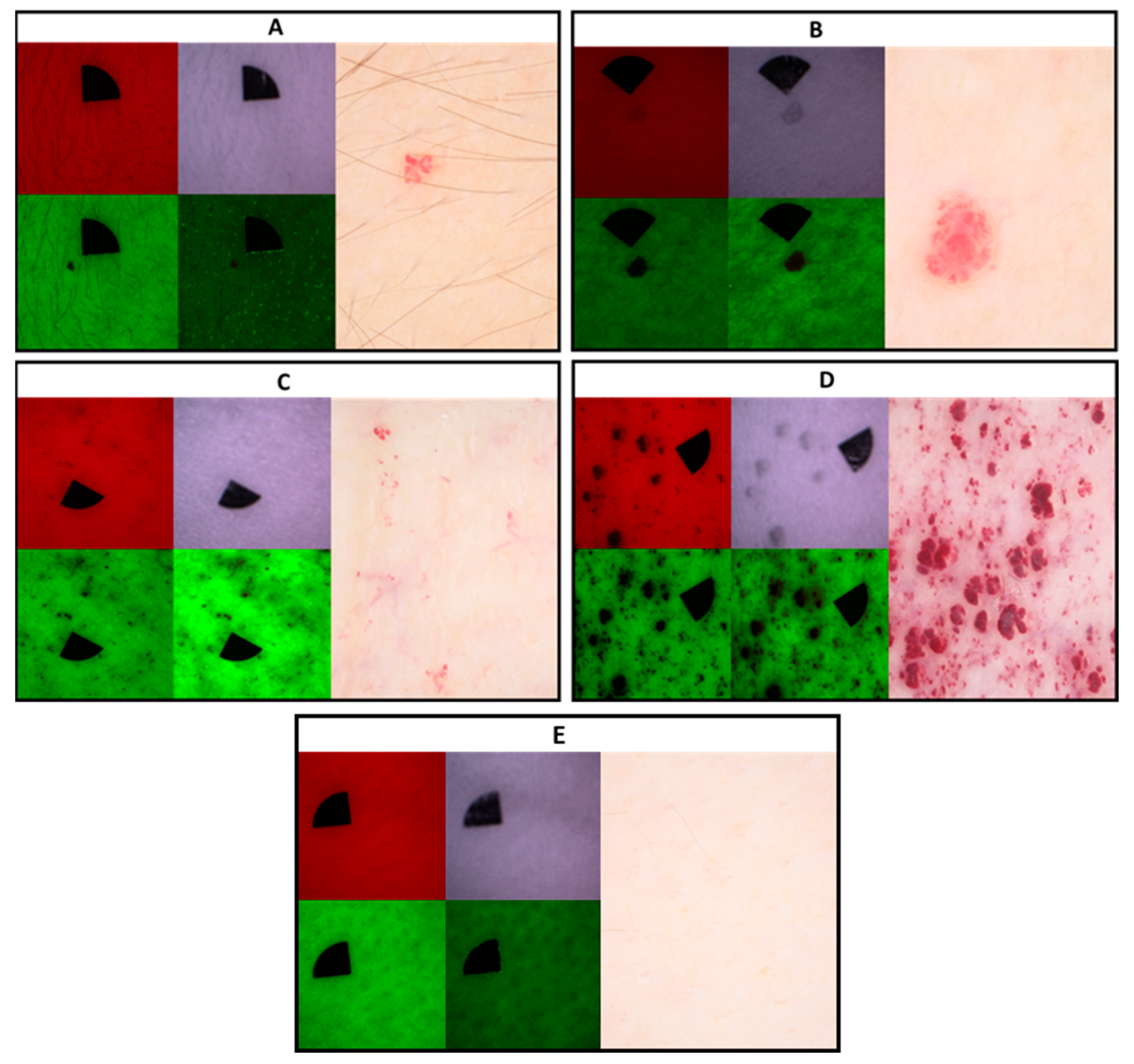
3.6. Multispectral LED Imaging
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Spada, M.; Pagliardini, S.; Yasuda, M.; Tukel, T.; Thiagarajan, G.; Sakuraba, H.; Ponzone, A.; Desnick, R.J. High incidence of later-onset fabry disease revealed by newborn screening. Am. J. Hum. Genet. 2006, 79, 31–40. [Google Scholar] [CrossRef] [Green Version]
- Miller, J.J.; Kanack, A.J.; Dahms, N.M. Progress in the understanding and treatment of Fabry disease. Biochim. Biophys. Acta Gen. Subj. 2020, 1864, 129437. [Google Scholar] [CrossRef] [PubMed]
- Errichetti, E.; Zalaudek, I.; Kittler, H.; Apalla, Z.; Argenziano, G.; Bakos, R.; Blum, A.; Braun, R.P.; Ioannides, D.; Lacarrubba, F.; et al. Standardization of dermoscopic terminology and basic dermoscopic parameters to evaluate in general dermatology (non-neoplastic dermatoses): An expert consensus on behalf of the International Dermoscopy Society. Br. J. Dermatol. 2020, 182, 454–467. [Google Scholar] [CrossRef] [PubMed]
- Wittmann, J.; Karg, E.; Turi, S.; Legnini, E.; Wittmann, G.; Giese, A.K.; Lukas, J.; Gölnitz, U.; Klingenhäger, M.; Bodamer, O.; et al. Newborn screening for lysosomal storage disorders in hungary. JIMD Rep. 2012, 6, 117–125. [Google Scholar]
- Chan, B.; Adam, D.N. A Review of Fabry Disease. Ski. Ther. Lett. 2018, 23, 4–6. [Google Scholar]
- Arends, M.; Hollak, C.E.M.; Biegstraaten, M. Quality of life in patients with Fabry disease: A systematic review of the literature. Orphanet J. Rare Dis. 2015, 10, 77. [Google Scholar] [CrossRef] [Green Version]
- van der Veen, S.J.; Hollak, C.E.M.; van Kuilenburg, A.B.P.; Langeveld, M. Developments in the treatment of Fabry disease. J. Inherit. Metab. Dis. 2020, 43, 908–921. [Google Scholar] [CrossRef] [Green Version]
- Dutra-Clarke, M.; Tapia, D.; Curtin, E.; Rünger, D.; Lee, G.K.; Lakatos, A.; Alandy-Dy, Z.; Freedkin, L.; Hall, K.; Ercelen, N.; et al. Variable clinical features of patients with Fabry disease and outcome of enzyme replacement therapy. Mol. Genet. Metab. Rep. 2020, 26, 100700. [Google Scholar] [CrossRef]
- Lenders, M.; Brand, E. Fabry Disease: The Current Treatment Landscape. Drugs 2021, 81, 635–645. [Google Scholar] [CrossRef]
- Germain, D.P. Fabry disease. Orphanet J. Rare Dis. 2010, 5, 30. [Google Scholar] [CrossRef] [Green Version]
- Orteu, C.H.; Jansen, T.; Lidove, O.; Jaussaud, R.; Hughes, D.A.; Pintos-Morell, G.; Ramaswami, U.; Parini, R.; Sunder-Plassman, G.; Beck, M.; et al. Fabry disease and the skin: Data from FOS, the Fabry outcome survey. Br. J. Dermatol. 2007, 157, 331–337. [Google Scholar] [CrossRef]
- Happle, R. Capillary malformations: A classification using specific names for specific skin disorders. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 2295–2305. [Google Scholar] [CrossRef] [PubMed]
- Merzel Šabović, E.K.; Žerjav Tanšek, M.; Grošelj, U.; Dragoš, V. Angiokeratomas and treatment with enzyme replacement therapy in a patient with Fabry disease. Acta Dermatovenerol. Alp. Pannonica Adriat. 2020, 29, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Cuestas, D.; Perafan, A.; Forero, Y.; Bonilla, J.; Velandia, A.; Gutierrez, A.; Motta, A.; Herrera, H.; Rolon, M. Angiokeratomas, not everything is Fabry disease. Int. J. Dermatol. 2019, 58, 713–721. [Google Scholar] [CrossRef]
- Zaballos, P.; Daufi, C.; Puig, S.; Argenziano, G.; Moreno-Ramirez, D.; Cabo, H.; Marghoob, A.A.; Llambrich, A.; Zalaudek, I.; Malvehy, J. Dermoscopy of solitary angiokeratomas: A morphological study. Arch. Dermatol. 2007, 143, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, V.; Russo, T.; Moscarella, E.; Brancaccio, G.; Alfano, R.; Argenziano, G. Dermatoscopy of Vascular Lesions. Dermatol. Clin. 2018, 36, 389–395. [Google Scholar] [CrossRef]
- Luna, P.C.; Boggio, P.; Larralde, M. Dermatologic Aspects of Fabry Disease. J. Inborn Errors Metab. Screen. 2016, 4, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Eng, C.M.; Banikazemi, M.; Gordon, R.E.; Goldman, M.; Phelps, R.; Kim, L.; Gass, A.; Winston, J.; Dikman, S.; Fallon, J.T.; et al. A phase 1/2 clinical trial of enzyme replacement in fabry disease: Pharmacokinetic, substrate clearance, and safety studies. Am. J. Hum. Genet. 2001, 68, 711–722. [Google Scholar] [CrossRef] [Green Version]
- Reisin, R.; Perrin, A.; García-Pavía, P. Time delays in the diagnosis and treatment of Fabry disease. Int. J. Clin. Pract. 2017, 71, e12914. [Google Scholar] [CrossRef]
- Bozsányi, S.; Varga, N.N.; Farkas, K.; Bánvölgyi, A.; Lőrincz, K.; Lihacova, I.; Lihachev, A.; Plorina, E.V.; Bartha, Á.; Jobbágy, A.; et al. Multispectral Imaging Algorithm Predicts Breslow Thickness of Melanoma. J. Clin. Med. 2021, 11, 189. [Google Scholar] [CrossRef]
- Bozsányi, S.; Farkas, K.; Bánvölgyi, A.; Lőrincz, K.; Fésűs, L.; Anker, P.; Zakariás, S.; Jobbágy, A.; Lihacova, I.; Lihachev, A.; et al. Quantitative Multispectral Imaging Differentiates Melanoma from Seborrheic Keratosis. Diagnostics 2021, 11, 1315. [Google Scholar] [CrossRef]
- Krolopp, Á.; Fésűs, L.; Szipőcs, G.; Wikonkál, N.; Szipőcs, R. Fiber coupled, 20 MHz Repetition Rate, sub ps Ti:sapphire Laser for in vivo Nonlinear Microscopy of the Skin. In Proceedings of the Biophotonics Congress 2021, Washington, DC, USA, 12 April 2021; p. DF2A.5. [Google Scholar]
- Anker, P.; Fésűs, L.; Kiss, N.; Noll, J.; Becker, K.; Kuroli, E.; Mayer, B.; Bozsányi, S.; Lőrincz, K.; Lihacova, I.; et al. Visualization of Keratin with Diffuse Reflectance and Autofluorescence Imaging and Nonlinear Optical Microscopy in a Rare Keratinopathic Ichthyosis. Sensors 2021, 21, 1105. [Google Scholar] [CrossRef] [PubMed]
- Lihachev, A.; Derjabo, A.; Ferulova, I.; Lange, M.; Lihacova, I.; Spigulis, J. Autofluorescence imaging of basal cell carcinoma by smartphone RGB camera. J. Biomed. Opt. 2015, 20, 120502. [Google Scholar] [CrossRef]
- Lihachev, A.; Lihacova, I.; Plorina, E.V.; Lange, M.; Derjabo, A.; Spigulis, J. Differentiation of seborrheic keratosis from basal cell carcinoma, nevi and melanoma by RGB autofluorescence imaging. Biomed. Opt. Express 2018, 9, 1852–1858. [Google Scholar] [CrossRef] [Green Version]
- Kumar, P. Synophrys: Epidemiological Study. Int. J. Trichology 2017, 9, 105–107. [Google Scholar] [CrossRef] [Green Version]
- Galimberti, C.; Madeo, A.; Di Rocco, M.; Fiumara, A. Mucopolysaccharidoses: Early diagnostic signs in infants and children. Ital. J. Pediatr. 2018, 44, 133. [Google Scholar] [CrossRef]
- Okada, J.; Hossain, M.A.; Wu, C.; Miyajima, T.; Yanagisawa, H.; Akiyama, K.; Eto, Y. Ten-year-long enzyme replacement therapy shows a poor effect in alleviating giant leg ulcers in a male with Fabry disease. Mol. Genet. Metab. Rep. 2018, 14, 68–72. [Google Scholar] [CrossRef]
- Śnit, M.; Przyłudzka, M.; Grzeszczak, W. Fabry disease—A genetically conditioned extremely rare disease with a very unusual course. Intractable Rare Dis. Res. 2022, 11, 34–36. [Google Scholar] [CrossRef] [PubMed]
- Effraimidis, G.; Rasmussen, Å.K.; Bundgaard, H.; Sørensen, S.S.; Feldt-Rasmussen, U. Is the alpha-galactosidase A variant p.Asp313Tyr (p.D313Y) pathogenic for Fabry disease? A systematic review. J. Inherit. Metab. Dis. 2020, 43, 922–933. [Google Scholar] [CrossRef]
- Germain, D.P.; Oliveira, J.P.; Bichet, D.G.; Yoo, H.W.; Hopkin, R.J.; Lemay, R.; Politei, J.; Wanner, C.; Wilcox, W.R.; Warnock, D.G. Use of a rare disease registry for establishing phenotypic classification of previously unassigned GLA variants: A consensus classification system by a multispecialty Fabry disease genotype-phenotype workgroup. J. Med. Genet. 2020, 57, 542–551. [Google Scholar] [CrossRef] [Green Version]
- Thurberg, B.L.; Randolph Byers, H.; Granter, S.R.; Phelps, R.G.; Gordon, R.E.; O’Callaghan, M. Monitoring the 3-Year Efficacy of Enzyme Replacement Therapy in Fabry Disease by Repeated Skin Biopsies. J. Investig. Dermatol. 2004, 122, 900–908. [Google Scholar] [CrossRef]
- Furujo, M.; Kubo, T.; Kobayashi, M.; Ohashi, T. Enzyme replacement therapy in two Japanese siblings with Fabry disease, and its effectiveness on angiokeratoma and neuropathic pain. Mol. Genet. Metab. 2013, 110, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Fei, W.; Shen, C.; Shen, X.; Sun, M.; Xu, N.; Li, Q.; Huang, C.; Zhang, T.; Ko, R.; et al. Dermoscopic Features Summarization and Comparison of Four Types of Cutaneous Vascular Anomalies. Front. Med. 2021, 8, 692060. [Google Scholar] [CrossRef]
- Farkas, K.; Bozsányi, S.; Plázár, D.; Bánvölgyi, A.; Fésűs, L.; Anker, P.; Zakariás, S.; Lihacova, I.; Lihachev, A.; Lange, M.; et al. Autofluorescence Imaging of the Skin Is an Objective Non-Invasive Technique for Diagnosing Pseudoxanthoma Elasticum. Diagnostics 2021, 11, 260. [Google Scholar] [CrossRef] [PubMed]
- Kiss, N.; Krolopp, Á.; Lőrincz, K.; Bánvölgyi, A.; Szipőcs, R.; Wikonkál, N. Stain-free Histopathology of Basal Cell Carcinoma by Dual Vibration Resonance Frequency CARS Microscopy. Pathol. Oncol. Res. 2018, 24, 927–930. [Google Scholar] [CrossRef] [PubMed]
- Kiss, N.; Fésűs, L.; Bozsányi, S.; Szeri, F.; Van Gils, M.; Szabó, V.; Nagy, A.I.; Hidvégi, B.; Szipőcs, R.; Martin, L.; et al. Nonlinear optical microscopy is a novel tool for the analysis of cutaneous alterations in pseudoxanthoma elasticum. Lasers Med. Sci. 2020, 35, 1821–1830. [Google Scholar] [CrossRef]
- Kiss, N.; Haluszka, D.; Lőrincz, K.; Kuroli, E.; Hársing, J.; Mayer, B.; Kárpáti, S.; Fekete, G.; Szipőcs, R.; Wikonkál, N.; et al. Ex vivo nonlinear microscopy imaging of Ehlers-Danlos syndrome-affected skin. Arch. Dermatol. Res. 2018, 310, 463–473. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 26) | Females (n = 14) | Males (n = 12) | |
|---|---|---|---|
| Mean age (years) | 37.0 ± 20.9 | 42.1 ± 19.9 | 31.1 ± 21.7 |
| Mean age at diagnosis (years) | 32.77 ± 19.4 | 37.07 ± 17.4 | 27.75 ± 21.1 |
| Mean age at the initiation of therapy (years) | 36.1 ± 18.3 | 43 ± 15.1 | 29.70 ± 19.4 |
| Therapy | |||
| Agalsidase-α | 10 (38%) | 5 (19%) | 5 (19%) |
| Agalsidase-β | 8 (31%) | 4 (15.5%) | 4 (15.5%) |
| Migalastat | 1 (4%) | 0 (0%) | 1 (4%) |
| None | 7 (27%) | 5 (19%) | 2 (8%) |
| Total (n = 26) | Females (n = 14) | Males (n = 12) | |
|---|---|---|---|
| Cardiovascular involvement | |||
| Cardiac involvement | 17 | 9 | 8 |
| Hypertension | 10 | 6 | 4 |
| Cerebrovascular involvement | |||
| Headaches | 4 | 1 | 3 |
| Tinnitus | 1 | 0 | 1 |
| Vertigo | 1 | 1 | 0 |
| Stroke | 4 | 3 | 1 |
| Hearing impariment | 5 | 2 | 3 |
| Renal involvement | 11 | 6 | 5 |
| Acroparesthaesia | 16 | 6 | 10 |
| Opthalmologic signs | |||
| Cornea verticillata | 18 | 9 | 9 |
| Other nonspecific signs | 14 | 8 | 6 |
| Gastrointestinal involvement | 11 | 4 | 7 |
| Pulmonary involvement | 4 | 3 | 1 |
| Fatigue | 13 | 7 | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anker, P.; Fésűs, L.; Kiss, N.; Lengyel, A.; Pinti, É.; Lihacova, I.; Lihachev, A.; Plorina, E.V.; Fekete, G.; Medvecz, M. A Cross-Sectional Study of the Dermatological Manifestations of Patients with Fabry Disease and the Assessment of Angiokeratomas with Multimodal Imaging. Diagnostics 2023, 13, 2368. https://doi.org/10.3390/diagnostics13142368
Anker P, Fésűs L, Kiss N, Lengyel A, Pinti É, Lihacova I, Lihachev A, Plorina EV, Fekete G, Medvecz M. A Cross-Sectional Study of the Dermatological Manifestations of Patients with Fabry Disease and the Assessment of Angiokeratomas with Multimodal Imaging. Diagnostics. 2023; 13(14):2368. https://doi.org/10.3390/diagnostics13142368
Chicago/Turabian StyleAnker, Pálma, Luca Fésűs, Norbert Kiss, Anna Lengyel, Éva Pinti, Ilze Lihacova, Alexey Lihachev, Emilija Vija Plorina, György Fekete, and Márta Medvecz. 2023. "A Cross-Sectional Study of the Dermatological Manifestations of Patients with Fabry Disease and the Assessment of Angiokeratomas with Multimodal Imaging" Diagnostics 13, no. 14: 2368. https://doi.org/10.3390/diagnostics13142368