
Cardiovascular Involvement in Tuberculosis: From Pathophysiology to Diagnosis and Complications—A Narrative Review
 , , , ,
, , , ,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Mycobacterium tuberculosis—An Old but “Still Standing” Enemy
2. Materials and Methods
3. Tuberculosis—Much More than a Pulmonary Disease
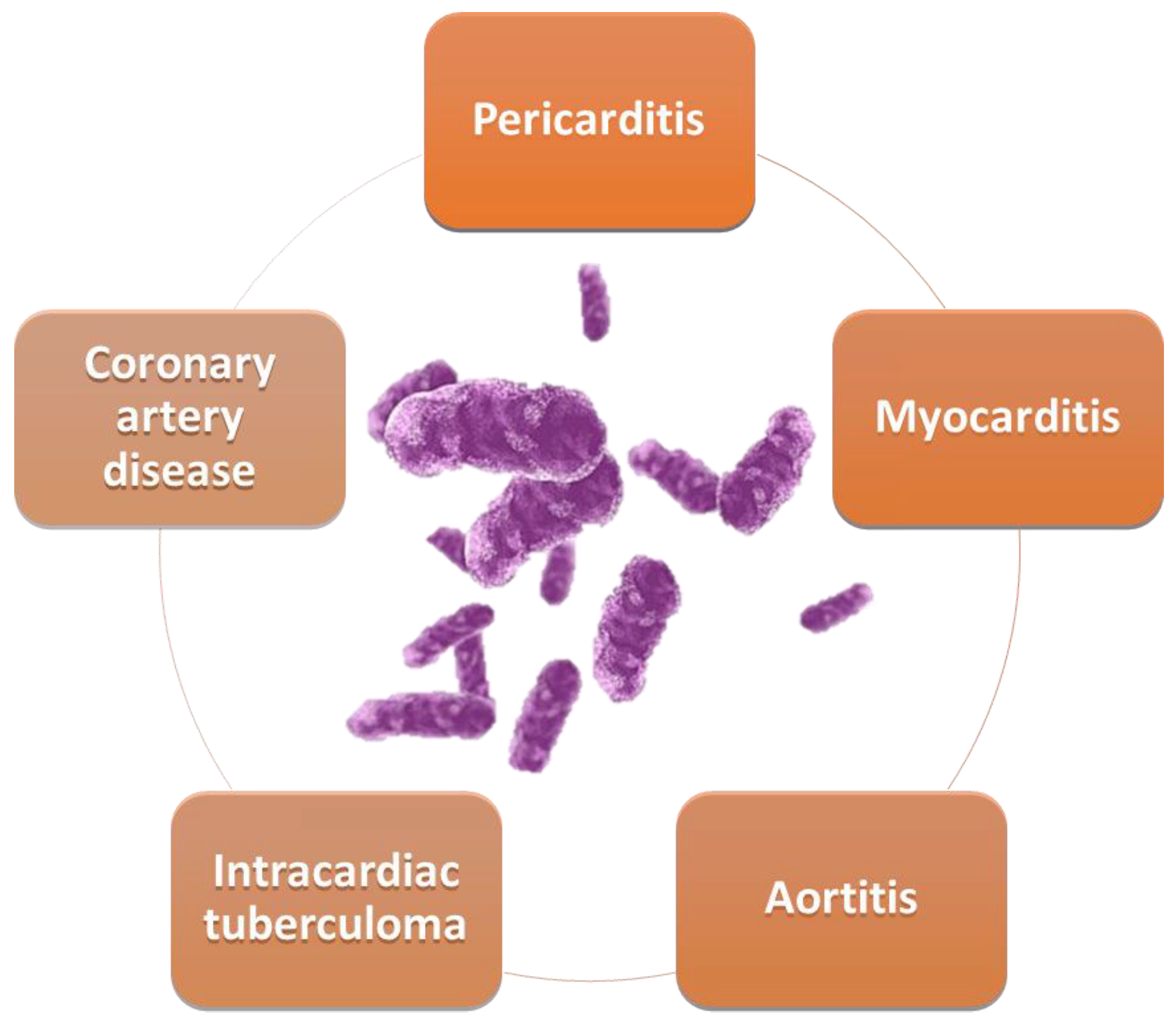
4. Cardiovascular Involvement in TB
4.1. Tuberculous Myocarditis
4.2. Coronary Artery Disease and Tuberculosis
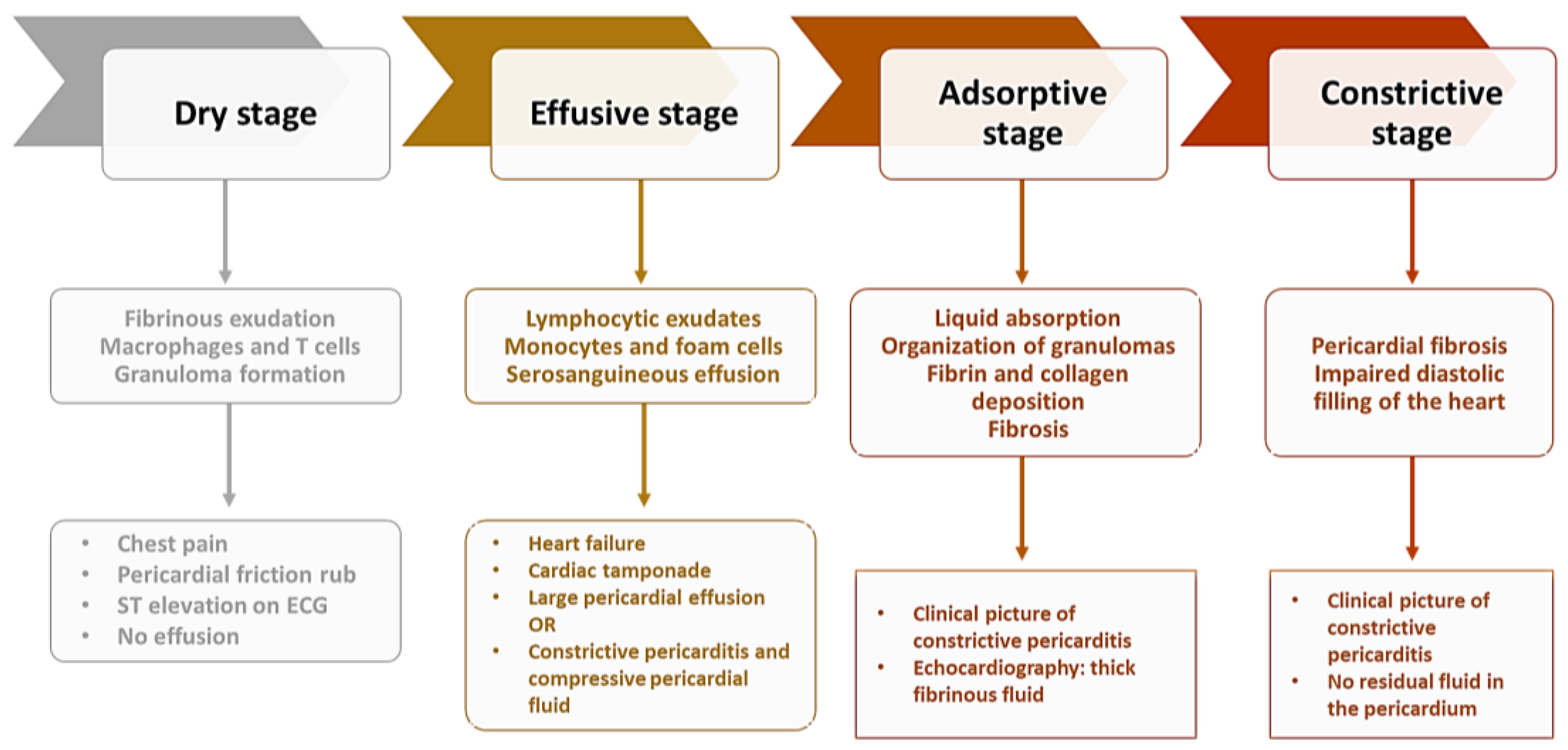
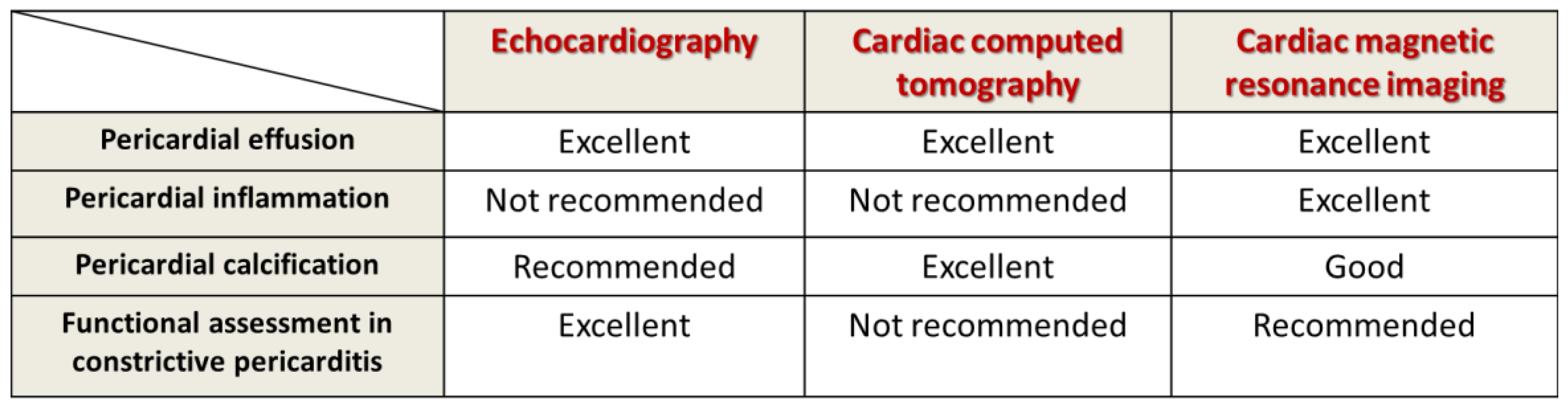
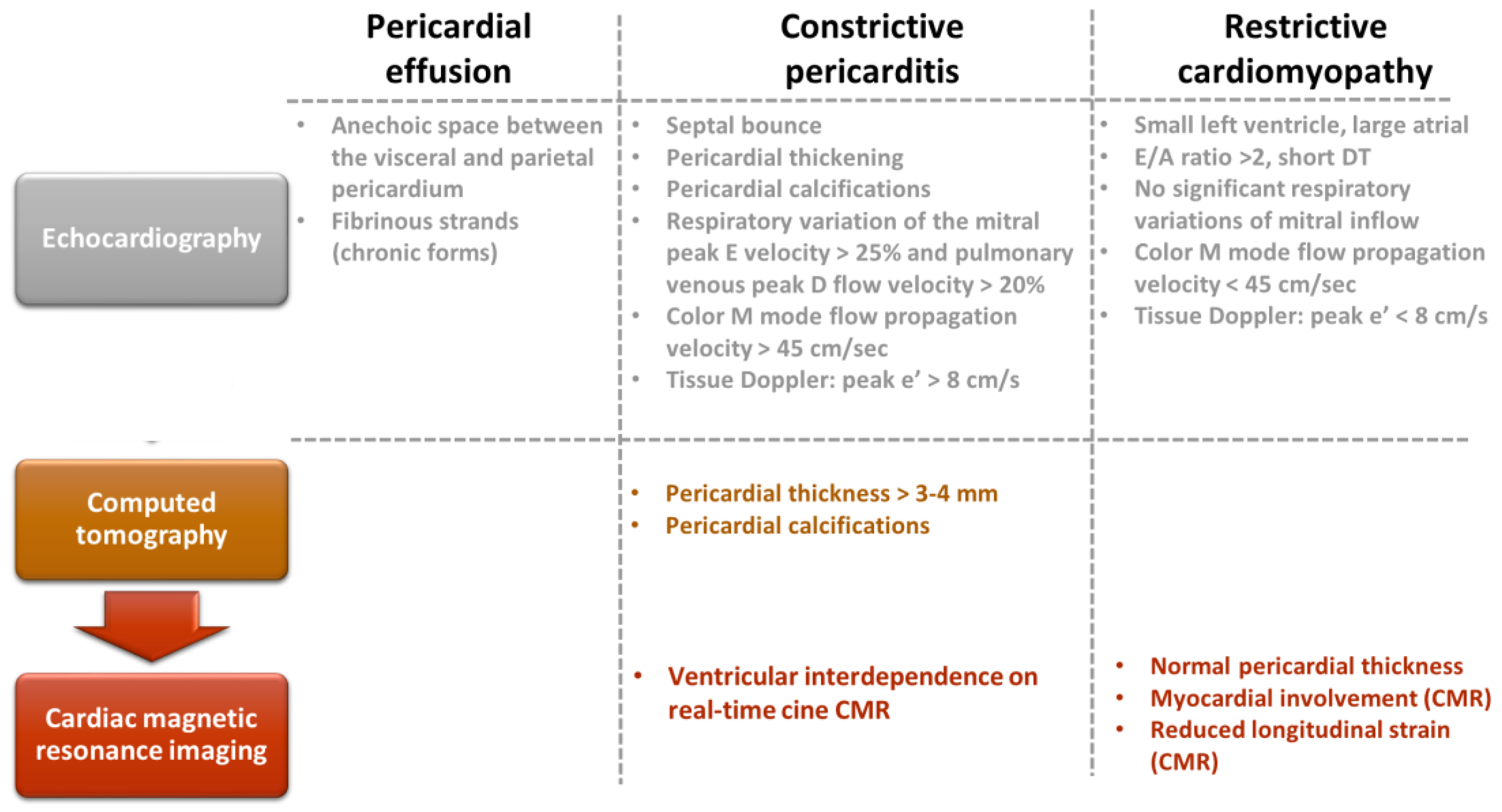
4.3. Tuberculous Pericarditis
4.4. Aortic Involvement
4.5. Intracardiac Tuberculoma and Papillary Muscle Enlargement
4.6. Cardiotoxic Effect of Antituberculosis Medication
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- 2.2 TB Mortality. Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2021/disease-burden/mortality (accessed on 27 November 2022).
- 2.2 TB Mortality. Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2022/tb-disease-burden/2-2-tb-mortality (accessed on 27 November 2022).
- 2.1 TB Incidence. Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2022/tb-disease-burden/2-1-tb-incidence (accessed on 27 November 2022).
- Global Tuberculosis Report. 2021. Available online: https://www.who.int/publications-detail-redirect/9789240037021 (accessed on 29 November 2022).
- Hayman, J. Mycobacterium Ulcerans: An Infection From Jurassic Time? The Lancet 1984, 324, 1015–1016. [Google Scholar] [CrossRef]
- Simpson, D.P. Cassell’s Latin Dictionary; Macmillan: New York, NY, USA, 1977. [Google Scholar]
- Brothwell, D. Diseases in Antiquity: A Survey of the Diseases, Injuries, and Surgery of Early Populations, 1st, ed.; Charles C Thomas Pub, Ltd.: Springfield, IL, USA, 1967; ISBN 978-0-398-00233-6. [Google Scholar]
- Morse, D.; Brothwell, D.R.; Ucko, P.J. Tuberculosis in Ancient Egypt. Am. Rev. Respir. Dis. 1964, 90, 524–541. [Google Scholar] [CrossRef]
- Cave, A.J.E.; Demonstrator, A. The Evidence for the Incidence of Tuberculosis in Ancient Egypt. Br. J. Tuberc. 1939, 33, 142–152. [Google Scholar] [CrossRef]
- Strong, J. Strong’s Exhaustive Concordance of the Bible; Hendrickson Publishers: Peabody, MA, USA, 2009; ISBN 978-1-59856-378-8. [Google Scholar]
- Daniel, V.S.; Daniel, T.M. Old Testament Biblical References to Tuberculosis. Clin. Infect. Dis. 1999, 29, 1557–1558. [Google Scholar] [CrossRef] [Green Version]
- Murray, J.F.; Rieder, H.L.; Finley-Croswhite, A. The King’s Evil and the Royal Touch: The Medical History of Scrofula. Int. J. Tuberc. Lung Dis. 2016, 20, 713–716. [Google Scholar] [CrossRef]
- López-López, J.P.; Posada-Martínez, E.L.; Saldarriaga, C.; Wyss, F.; Ponte-Negretti, C.I.; Alexander, B.; Miranda-Arboleda, A.F.; Martínez-Sellés, M.; Baranchuk, A. The Neglected Tropical Diseases, Other Infectious Diseases Affecting the Heart (the NET-Heart Project) Tuberculosis and the Heart. J. Am. Heart Assoc. 2021, 10, e019435. [Google Scholar] [CrossRef]
- Mutyaba, A.K.; Ntsekhe, M. Tuberculosis and the Heart. Cardiol. Clin. 2017, 35, 135–144. [Google Scholar] [CrossRef]
- Michira, B.N.; Alkizim, F.O.; Matheka, D.M. Patterns and Clinical Manifestations of Tuberculous Myocarditis: A Systematic Review of Cases. Pan Afr. Med. J. 2015, 21, 118. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Wang, J.; Liu, J.; Zhang, Z.; He, J.; Wang, Y. A Case Report and Review of Literature: Tuberculous Pericarditis with Pericardial Effusion as the Only Clinical Manifestation. Front. Cardiovasc. Med. 2022, 9, 1020672. [Google Scholar] [CrossRef] [PubMed]
- Prakasha, S.R.; Suresh, G.; D’sa, I.P.; Shetty, S.S.; Kumar, S.G. Mapping the Pattern and Trends of Extrapulmonary Tuberculosis. J. Glob. Infect. Dis. 2013, 5, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.K.; Mohan, A.; Kohli, M. Extrapulmonary Tuberculosis. Expert Rev. Respir. Med. 2021, 15, 931–948. [Google Scholar] [CrossRef] [PubMed]
- Cherian, J.J.; Lobo, I.; Sukhlecha, A.; Chawan, U.; Kshirsagar, N.A.; Nair, B.L.; Sawardekar, L. Treatment Outcome of Extrapulmonary Tuberculosis under Revised National Tuberculosis Control Programme. Indian J. Tuberc. 2017, 64, 104–108. [Google Scholar] [CrossRef]
- Pottenger, F.M. The Effect of Tuberculosis on the Heart. Arch. Intern. Med. 1909, IV, 306–322. [Google Scholar] [CrossRef] [Green Version]
- Ohene, S.-A.; Bakker, M.I.; Ojo, J.; Toonstra, A.; Awudi, D.; Klatser, P. Extra-Pulmonary Tuberculosis: A Retrospective Study of Patients in Accra, Ghana. PLoS ONE 2019, 14, e0209650. [Google Scholar] [CrossRef]
- Amini, M.; Zayeri, F.; Salehi, M. Trend Analysis of Cardiovascular Disease Mortality, Incidence, and Mortality-to-Incidence Ratio: Results from Global Burden of Disease Study 2017. BMC Public Health 2021, 21, 401. [Google Scholar] [CrossRef]
- Huaman, M.A.; Kryscio, R.J.; Fichtenbaum, C.J.; Henson, D.; Salt, E.; Sterling, T.R.; Garvy, B.A. Tuberculosis and Risk of Acute Myocardial Infarction: A Propensity Score-Matched Analysis. Epidemiol. Infect. 2017, 145, 1363–1367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adefuye, M.A.; Manjunatha, N.; Ganduri, V.; Rajasekaran, K.; Duraiyarasan, S.; Adefuye, B.O. Tuberculosis and Cardiovascular Complications: An Overview. Cureus 2022, 14, e28268. [Google Scholar] [CrossRef] [PubMed]
- Tran, D.-M.T.; Lekhak, N.; Gutierrez, K.; Moonie, S. Risk Factors Associated with Cardiovascular Disease among Adult Nevadans. PLoS ONE 2021, 16, e0247105. [Google Scholar] [CrossRef]
- Epstein, S.E.; Zhu, J.; Najafi, A.H.; Burnett, M.S. Insights Into the Role of Infection in Atherogenesis and in Plaque Rupture. Circulation 2009, 119, 3133–3141. [Google Scholar] [CrossRef] [Green Version]
- Wongtrakul, W.; Charoenngam, N.; Ungprasert, P. Tuberculosis and Risk of Coronary Heart Disease: A Systematic Review and Meta-Analysis. Indian J. Tuberc. 2020, 67, 182–188. [Google Scholar] [CrossRef]
- Hasanain, A.F.A.; El-Maghraby, K.M.; Zayed, A.A.H.; Nafee, A.M.A.; Abdel-Aal, S.M.; Bakkar, S.M. Latent Tuberculosis Infection among Patients with Coronary Artery Stenosis: A Case–Control Study. Int. J. Mycobacteriology 2018, 7, 143. [Google Scholar] [CrossRef]
- Huaman, M.A.; De Cecco, C.N.; Bittencourt, M.S.; Ticona, E.; Kityo, C.; Ballena, I.; Nalukwago, S.; Nazzinda, R.; Ticona, C.; Azañero, R.; et al. Latent Tuberculosis Infection and Subclinical Coronary Atherosclerosis in Peru and Uganda. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, e3384–e3390. [Google Scholar] [CrossRef]
- Chidambaram, V.; Ruelas Castillo, J.; Kumar, A.; Wei, J.; Wang, S.; Majella, M.G.; Gupte, A.; Wang, J.-Y.; Karakousis, P.C. The Association of Atherosclerotic Cardiovascular Disease and Statin Use with Inflammation and Treatment Outcomes in Tuberculosis. Sci. Rep. 2021, 11, 15283. [Google Scholar] [CrossRef]
- Pedroso, A.; Ferreira, I.; Chikura, T. Tuberculosis and Sarcoidosis Overlap: A Clinical Challenge From Diagnosis to Treatment. Cureus 2020, 12, e11662. [Google Scholar] [CrossRef]
- Carbonelli, C.; Giuffreda, E.; Palmiotti, A.; Loizzi, D.; Lococo, F.; Carpagnano, E.; Lacedonia, D.; Sollitto, F.; Foschino, M.P. Coexistent Sarcoidosis and Tuberculosis: A Case Report. Respiration 2017, 93, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Badar, F.; Azfar, S.F.; Ahmad, I.; Yasmeen, S.; Kirmani, S. Diagnostic Difficulties in Differentiating Sarcoidosis from Tuberculosis. Oman Med. J. 2011, 26, 210–211. [Google Scholar] [CrossRef] [PubMed]
- Das, K.M.; Mansoori, T.A.; Alattar, Y.H.; Gorkom, K.V.; Shamisi, A.; Melethil, A.P.; Alkoteesh, J.A. Tuberculosis of the Heart: A Diagnostic Challenge. Tomography 2022, 8, 1649–1665. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.V.; Toshniwal, S.; Gondhali, G.; Patil, D. Pulmonary Tuberculosis with Cardiac Dysfunction: An Ignored Combination! Electron. J. Gen. Med. 2023, 20, em437. [Google Scholar] [CrossRef] [PubMed]
- Awasthy, N.; Garg, R.; Goel, A.; Bhatia, M.; Radhakrishnan, S. Ventricular Arrhythmia: A Feature of Tubercular Myocarditis. Ann. Pediatr. Cardiol. 2019, 12, 53. [Google Scholar] [CrossRef]
- Choudhary, N.; Abera, H.; Naik, R.B. Tuberculosis Presenting With Acute Myocarditis and Systolic Heart Failure. Cureus 2021, 13, e13229. [Google Scholar] [CrossRef] [PubMed]
- Wallis, P.J.; Branfoot, A.C.; Emerson, P.A. Sudden Death Due to Myocardial Tuberculosis. Thorax 1984, 39, 155–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirsten, K.; Schaedel, C. Sudden Death Due to Myocardial Tuberculosis. Thorax 1985, 40, 799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- du Toit-Prinsloo, L.; Saayman, G. “Death at the Wheel” Due to Tuberculosis of the Myocardium: A Case Report. Cardiovasc. Pathol. 2016, 25, 271–274. [Google Scholar] [CrossRef] [Green Version]
- Maeder, M.; Ammann, P.; Rickli, H.; Schoch, O.D. Fever and Night Sweats in a 22-Year-Old Man with a Mediastinal Mass Involving the Heart. Chest 2003, 124, 2006–2009. [Google Scholar] [CrossRef] [Green Version]
- Raffali, M.A.; Muhammad, S.F.; Tiau Wei Jyung, P.; Farouk, D.; Zohdi, A.; Che Hassan, H.H. Disseminated Tuberculosis With Myocarditis and Intracardiac Thrombus in a Previously Young Healthy Woman. JACC Case Rep. 2021, 3, 1661–1666. [Google Scholar] [CrossRef]
- Al-Jahdali Tuberculous Myocarditis Is Not Always Fatal: Report of Three Confirmed Cases with Uneventful Outcome. Available online: https://www.ijmyco.org/article.asp?issn=2212-5531;year=2017;volume=6;issue=1;spage=111;epage=115;aulast=Al-Jahdali (accessed on 30 November 2022).
- Gautam, M.P.; Sogunuru, G.; Subramanyam, G.; Viswanath, R.C. Tuberculous Myocarditis Presenting as a Refractory Ventricular Tachycardia of Biventricular Origin. J. Coll. Med. Sci.-Nepal 2011, 7, 60–66. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz, A.; Kindermann, I.; Kindermann, M.; Mahfoud, F.; Ukena, C.; Athanasiadis, A.; Hill, S.; Mahrholdt, H.; Voehringer, M.; Schieber, M.; et al. Comparative Evaluation of Left and Right Ventricular Endomyocardial Biopsy: Differences in Complication Rate and Diagnostic Performance. Circulation 2010, 122, 900–909. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, P.G.; Rokey, R.; Greenberg, S.; Pacifico, A. Resolution of Ventricular Tachycardia and Endocardial Tuberculoma Following Antituberculosis Therapy. Chest 1991, 100, 1467–1469. [Google Scholar] [CrossRef]
- Díaz-Peromingo, J.A.; Mariño-Callejo, A.I.; González-González, C.; García-Rodríguez, J.F.; Ameneiros-Lago, M.E.; Sesma-Sánchez, P. Tuberculous Myocarditis Presenting as Long QT Syndrome. Eur. J. Intern. Med. 2000, 11, 340–342. [Google Scholar] [CrossRef] [PubMed]
- Vennamaneni, V.; Chohan, F.; Rad, P.; Rodriguez, J.; Gupta, R.; Michel, G. Clinical Presentation of a Patient With Tuberculous Myocarditis: Case Report and Review of Literature. Cureus 2022, 14, e22715. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, O.P.; Mascarenhas, E.; Rananaware, M.M.; Gadgil, R.K. Tuberculoma of the Heart. Report of 9 Cases. Am. Heart J. 1973, 86, 334–340. [Google Scholar] [CrossRef]
- Alkhuja, S.; Miller, A. Tuberculosis and Sudden Death: A Case Report and Review. Heart Lung J. Crit. Care 2001, 30, 388–391. [Google Scholar] [CrossRef] [PubMed]
- Ren, M.; Zhang, C.; Zhang, X.; Zhong, J. Acute Tuberculous Myopericarditis Mimicking Acute Myocardial Infarction: A Case Report and Literature Review. Exp. Ther. Med. 2016, 11, 2373–2378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breton, G.; Leclerc, S.; Longuet, P.; Leport, C.; Vildé, J.-L.; Laissy, J.-P. Myocardial localisation of tuberculosis: The diagnostic value of cardiac MRI. Presse Medicale Paris Fr. 1983 2005, 34, 293–296. [Google Scholar] [CrossRef]
- Rajeshwari, K.; Gupta, S.; Dubey, A.; Gera, R. Asymptomatic Multiple Intracardiac Tuberculomas in a Child. Cardiol. J. 2012, 19, 518–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambatten, D.; Hammi, S.; Rhofir, Y.; Bourkadi, J.E. Myocardial tuberculoma: Unusual location of tuberculosis: A new observation and review of the literature. Pan Afr. Med. J. 2016, 24, 32. [Google Scholar] [CrossRef]
- Dixit, R.; Chowdhury, V.; Singh, S. Case Report: Myocardial Tuberculosis-MRI. Indian J. Radiol. Imaging 2009, 19, 57–59. [Google Scholar] [CrossRef]
- Amonkar, G.; Rupani, A.; Shah, V.; Parmar, H. Sudden Death in Tuberculous Myocarditis. Cardiovasc. Pathol. 2009, 18, 247–248. [Google Scholar] [CrossRef]
- Kumar, P.; Sharma, S.; Bisht, D.; Panwar, R. Tuberculous Dilated Cardiomyopathy with Myocarditis. Indian J. Pediatr. 2020, 87, 161. [Google Scholar] [CrossRef] [Green Version]
- Dada, M.A.; Lazarus, N.G.; Kharsany, A.B.; Sturm, A.W. Sudden Death Caused by Myocardial Tuberculosis: Case Report and Review of the Literature. Am. J. Forensic Med. Pathol. 2000, 21, 385–388. [Google Scholar] [CrossRef]
- Hitsumoto, T.; Ikeda, S.; Matsukage, S.; Hamada, M. Extensive Myocardial Calcinosis Due to Mycobacterium tuberculosis. Eur. Heart J. 2016, 37, 1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basham, C.A.; Smith, S.J.; Romanowski, K.; Johnston, J.C. Cardiovascular Morbidity and Mortality among Persons Diagnosed with Tuberculosis: A Systematic Review and Meta-Analysis. PLoS ONE 2020, 15, e0235821. [Google Scholar] [CrossRef] [PubMed]
- Huaman, M.A.; Ticona, E.; Miranda, G.; Kryscio, R.J.; Mugruza, R.; Aranda, E.; Rondan, P.L.; Henson, D.; Ticona, C.; Sterling, T.R.; et al. The Relationship Between Latent Tuberculosis Infection and Acute Myocardial Infarction. Clin. Infect. Dis. 2018, 66, 886–892. [Google Scholar] [CrossRef] [Green Version]
- Salindri, A.D.; Wang, J.-Y.; Lin, H.-H.; Magee, M.J. Post-Tuberculosis Incidence of Diabetes, Myocardial Infarction, and Stroke: Retrospective Cohort Analysis of Patients Formerly Treated for Tuberculosis in Taiwan, 2002-2013. Int. J. Infect. Dis. 2019, 84, 127–130. [Google Scholar] [CrossRef] [Green Version]
- Khoufi, E.A.A. Association between Latent Tuberculosis and Ischemic Heart Disease: A Hospital-Based Cross-Sectional Study from Saudi Arabia. Pan Afr. Med. J. 2021, 38, 362. [Google Scholar] [CrossRef]
- Rodríguez-Iturbe, B.; Johnson, R. Heat Shock Proteins and Cardiovascular Disease. Physiol. Int. 2018, 105, 19–37. [Google Scholar] [CrossRef]
- Sun, H.; Shen, J.; Liu, T.; Tan, Y.; Tian, D.; Luo, T.; Lai, W.; Dai, M.; Guo, Z. Heat Shock Protein 65 Promotes Atherosclerosis through Impairing the Properties of High Density Lipoprotein. Atherosclerosis 2014, 237, 853–861. [Google Scholar] [CrossRef]
- Huaman, M.A.; Deepe, G.S.; Fichtenbaum, C.J. Elevated Circulating Concentrations of Interferon-Gamma in Latent Tuberculosis Infection. Pathog. Immun. 2016, 1, 291–303. [Google Scholar] [CrossRef]
- Zak, D.E.; Penn-Nicholson, A.; Scriba, T.J.; Thompson, E.; Suliman, S.; Amon, L.M.; Mahomed, H.; Erasmus, M.; Whatney, W.; Hussey, G.D.; et al. A Prospective Blood RNA Signature for Tuberculosis Disease Risk. Lancet Lond. Engl. 2016, 387, 2312–2322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grundtman, C.; Jakic, B.; Buszko, M.; Onestingel, E.; Almanzar, G.; Demetz, E.; Dietrich, H.; Cappellano, G.; Wick, G. Mycobacterial Heat Shock Protein 65 (MbHSP65)-Induced Atherosclerosis: Preventive Oral Tolerization and Definition of Atheroprotective and Atherogenic MbHSP65 Peptides. Atherosclerosis 2015, 242, 303–310. [Google Scholar] [CrossRef]
- Chung, W.-S.; Lin, C.-L.; Hung, C.-T.; Chu, Y.-H.; Sung, F.-C.; Kao, C.-H.; Yeh, J.-J. Tuberculosis Increases the Subsequent Risk of Acute Coronary Syndrome: A Nationwide Population-Based Cohort Study. Int. J. Tuberc. Lung Dis. 2014, 18, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Van Eeden, S.; Leipsic, J.; Paul Man, S.F.; Sin, D.D. The Relationship between Lung Inflammation and Cardiovascular Disease. Am. J. Respir. Crit. Care Med. 2012, 186, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Sheu, J.-J.; Chiou, H.-Y.; Kang, J.-H.; Chen, Y.-H.; Lin, H.-C. Tuberculosis and the Risk of Ischemic Stroke: A 3-Year Follow-Up Study. Stroke 2010, 41, 244–249. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.-H.; Chien, W.-C.; Chung, C.-H.; Lin, F.-H.; Peng, C.-K.; Chian, C.-F.; Shen, C.-H. Tuberculosis Increases the Risk of Peripheral Arterial Disease: A Nationwide Population-Based Study: TB Increases the Risk of PAD. Respirology 2017, 22, 1670–1676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Jia, S.; Yao, Y.; Tang, X.-F.; Xu, N.; Jiang, L.; Gao, Z.; Chen, J.; Yang, Y.-J.; Gao, R.-L.; et al. Impact of High-Sensitivity C-Reactive Protein on Coronary Artery Disease Severity and Outcomes in Patients Undergoing Percutaneous Coronary Intervention. J. Cardiol. 2020, 75, 60–65. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Li, M.; Liu, L.; Dang, X.; Zhu, D.; Tian, G. Monocyte/Lymphocyte Ratio Is Related to the Severity of Coronary Artery Disease and Clinical Outcome in Patients with Non-ST-Elevation Myocardial Infarction. Medicine (Baltimore) 2019, 98, e16267. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, E.D.D.; Gil-Santana, L.; Ramalho, D.; Tonomura, E.; Silva, E.C.; Oliveira, M.M.; Andrade, B.B.; Kritski, A. For the Rede-TB Study group Associations between Systemic Inflammation, Mycobacterial Loads in Sputum and Radiological Improvement after Treatment Initiation in Pulmonary TB Patients from Brazil: A Prospective Cohort Study. BMC Infect. Dis. 2016, 16, 368. [Google Scholar] [CrossRef] [Green Version]
- Wilson, D.; Moosa, M.-Y.S.; Cohen, T.; Cudahy, P.; Aldous, C.; Maartens, G. Evaluation of Tuberculosis Treatment Response With Serial C-Reactive Protein Measurements. Open Forum Infect. Dis. 2018, 5, ofy253. [Google Scholar] [CrossRef] [Green Version]
- Cubillos-Angulo, J.M.; Nogueira, B.M.F.; Arriaga, M.B.; Barreto-Duarte, B.; Araújo-Pereira, M.; Fernandes, C.D.; Vinhaes, C.L.; Villalva-Serra, K.; Nunes, V.M.; Miguez-Pinto, J.P.; et al. Host-Directed Therapies in Pulmonary Tuberculosis: Updates on Anti-Inflammatory Drugs. Front. Med. 2022, 9, 970408. [Google Scholar] [CrossRef] [PubMed]
- Jain, M.K.; Ridker, P.M. Anti-Inflammatory Effects of Statins: Clinical Evidence and Basic Mechanisms. Nat. Rev. Drug Discov. 2005, 4, 977–987. [Google Scholar] [CrossRef]
- Liberale, L.; Carbone, F.; Montecucco, F.; Sahebkar, A. Statins Reduce Vascular Inflammation in Atherogenesis: A Review of Underlying Molecular Mechanisms. Int. J. Biochem. Cell Biol. 2020, 122, 105735. [Google Scholar] [CrossRef] [PubMed]
- Montecucco, F.; Mach, F. Update on Statin-Mediated Anti-Inflammatory Activities in Atherosclerosis. Semin. Immunopathol. 2009, 31, 127–142. [Google Scholar] [CrossRef]
- Shahbaz, S.K.; Sadeghi, M.; Koushki, K.; Penson, P.E.; Sahebkar, A. Regulatory T Cells: Possible Mediators for the Anti-Inflammatory Action of Statins. Pharmacol. Res. 2019, 149, 104469. [Google Scholar] [CrossRef] [PubMed]
- Pinal-Fernandez, I.; Casal-Dominguez, M.; Mammen, A.L. Statins: Pros and Cons. Med. Clin. 2018, 150, 398–402. [Google Scholar] [CrossRef]
- Guerra-De-Blas, P.D.C.; Torres-González, P.; Bobadilla-Del-Valle, M.; Sada-Ovalle, I.; Ponce-De-León-Garduño, A.; Sifuentes-Osornio, J. Potential Effect of Statins on Mycobacterium Tuberculosis Infection. J. Immunol. Res. 2018, 2018, 7617023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tahir, F.; Bin Arif, T.; Ahmed, J.; Shah, S.R.; Khalid, M. Anti-Tuberculous Effects of Statin Therapy: A Review of Literature. Cureus 2020, 12, e7404. [Google Scholar] [CrossRef] [Green Version]
- Vrieling, F.; Wilson, L.; Rensen, P.C.N.; Walzl, G.; Ottenhoff, T.H.M.; Joosten, S.A. Oxidized Low-Density Lipoprotein (OxLDL) Supports Mycobacterium Tuberculosis Survival in Macrophages by Inducing Lysosomal Dysfunction. PLoS Pathog. 2019, 15, e1007724. [Google Scholar] [CrossRef] [Green Version]
- Shim, D.; Kim, H.; Shin, S.J. Mycobacterium Tuberculosis Infection-Driven Foamy Macrophages and Their Implications in Tuberculosis Control as Targets for Host-Directed Therapy. Front. Immunol. 2020, 11, 910. [Google Scholar] [CrossRef]
- Park, H.-E.; Lee, W.; Choi, S.; Jung, M.; Shin, M.-K.; Shin, S.J. Modulating Macrophage Function to Reinforce Host Innate Resistance against Mycobacterium Avium Complex Infection. Front. Immunol. 2022, 13, 931876. [Google Scholar] [CrossRef]
- Parihar, S.P.; Guler, R.; Khutlang, R.; Lang, D.M.; Hurdayal, R.; Mhlanga, M.M.; Suzuki, H.; Marais, A.D.; Brombacher, F. Statin Therapy Reduces the Mycobacterium Tuberculosis Burden in Human Macrophages and in Mice by Enhancing Autophagy and Phagosome Maturation. J. Infect. Dis. 2014, 209, 754–763. [Google Scholar] [CrossRef]
- Bruiners, N.; Dutta, N.K.; Guerrini, V.; Salamon, H.; Yamaguchi, K.D.; Karakousis, P.C.; Gennaro, M.L. The Anti-Tubercular Activity of Simvastatin Is Mediated by Cholesterol-Driven Autophagy via the AMPK-MTORC1-TFEB Axis. J. Lipid Res. 2020, 61, 1617–1628. [Google Scholar] [CrossRef]
- Dutta, N.K.; Bruiners, N.; Pinn, M.L.; Zimmerman, M.D.; Prideaux, B.; Dartois, V.; Gennaro, M.L.; Karakousis, P.C. Statin Adjunctive Therapy Shortens the Duration of TB Treatment in Mice. J. Antimicrob. Chemother. 2016, 71, 1570–1577. [Google Scholar] [CrossRef] [Green Version]
- Dutta, N.K.; Bruiners, N.; Zimmerman, M.D.; Tan, S.; Dartois, V.; Gennaro, M.L.; Karakousis, P.C. Adjunctive Host-Directed Therapy With Statins Improves Tuberculosis-Related Outcomes in Mice. J. Infect. Dis. 2020, 221, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Sheng, L.; Lou, L. Statin Use May Be Associated With Reduced Active Tuberculosis Infection: A Meta-Analysis of Observational Studies. Front. Med. 2020, 7, 121. [Google Scholar] [CrossRef]
- Guerra-De-Blas, P.D.C.; Bobadilla-Del-Valle, M.; Sada-Ovalle, I.; Estrada-García, I.; Torres-González, P.; López-Saavedra, A.; Guzmán-Beltrán, S.; Ponce-de-León, A.; Sifuentes-Osornio, J. Simvastatin Enhances the Immune Response Against Mycobacterium Tuberculosis. Front. Microbiol. 2019, 10, 2097. [Google Scholar] [CrossRef]
- Chidambaram, V.; Zhou, L.; Ruelas Castillo, J.; Kumar, A.; Ayeh, S.K.; Gupte, A.; Wang, J.-Y.; Karakousis, P.C. Higher Serum Cholesterol Levels Are Associated With Reduced Systemic Inflammation and Mortality During Tuberculosis Treatment Independent of Body Mass Index. Front. Cardiovasc. Med. 2021, 8, 696517. [Google Scholar] [CrossRef]
- Su, V.Y.-F.; Pan, S.-W.; Yen, Y.-F.; Feng, J.-Y.; Su, W.-J.; Chen, Y.-M. Statin Use and Impact on Tuberculosis Risk. Expert Rev. Anti Infect. Ther. 2021, 19, 1093–1098. [Google Scholar] [CrossRef]
- Meregildo-Rodriguez, E.D.; Chunga-Chévez, E.V.; Gianmarco, R.-A.L.; Vásquez-Tirado, G.A. Further Insights into to the Role of Statins against Active Tuberculosis: Systematic Review and Meta-Analysis. Infez. Med. 2022, 30, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Duan, H.; Liu, T.; Zhang, X.; Yu, A.; Cao, Y. Statin Use and Risk of Tuberculosis: A Systemic Review of Observational Studies. Int. J. Infect. Dis. 2020, 93, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-T.; Kuo, S.-C.; Chao, P.-W.; Chang, Y.-Y. Use of Lipid-Lowering Agents Is Not Associated with Improved Outcomes for Tuberculosis Patients on Standard-Course Therapy: A Population-Based Cohort Study. PLoS ONE 2019, 14, e0210479. [Google Scholar] [CrossRef] [PubMed]
- Vakamudi, S.; Ho, N.; Cremer, P.C. Pericardial Effusions: Causes, Diagnosis, and Management. Prog. Cardiovasc. Dis. 2017, 59, 380–388. [Google Scholar] [CrossRef]
- Ntsekhe, M.; Shey Wiysonge, C.; Commerford, P.J.; Mayosi, B.M. The Prevalence and Outcome of Effusive Constrictive Pericarditis: A Systematic Review of the Literature. Cardiovasc. J. Afr. 2012, 23, 281–285. [Google Scholar] [CrossRef] [Green Version]
- Mayosi, B.M.; Burgess, L.J.; Doubell, A.F. Tuberculous Pericarditis. Circulation 2005, 112, 3608–3616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reuter, H.; Burgess, L.J.; Carstens, M.E.; Doubell, A.F. Characterization of the Immunological Features of Tuberculous Pericardial Effusions in HIV Positive and HIV Negative Patients in Contrast with Non-Tuberculous Effusions. Tuberc. Edinb. Scotl. 2006, 86, 125–133. [Google Scholar] [CrossRef]
- Yu, G.; Zhong, F.; Shen, Y.; Zheng, H. Diagnostic Accuracy of the Xpert MTB/RIF Assay for Tuberculous Pericarditis: A Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0257220. [Google Scholar] [CrossRef]
- Spodick, D.H. Tuberculous Pericarditis. AMA Arch. Intern. Med. 1956, 98, 737–749. [Google Scholar] [CrossRef] [PubMed]
- Ntsekhe, M.; Mayosi, B.M. Tuberculous Pericarditis with and without HIV. Heart Fail. Rev. 2013, 18, 367–373. [Google Scholar] [CrossRef]
- Mayosi, B.M.; Wiysonge, C.S.; Ntsekhe, M.; Volmink, J.A.; Gumedze, F.; Maartens, G.; Aje, A.; Thomas, B.M.; Thomas, K.M.; Awotedu, A.A.; et al. Clinical Characteristics and Initial Management of Patients with Tuberculous Pericarditis in the HIV Era: The Investigation of the Management of Pericarditis in Africa (IMPI Africa) Registry. BMC Infect. Dis. 2006, 6, 2. [Google Scholar] [CrossRef] [Green Version]
- Schrire, V. Experience with Pericarditis at Groote Schuur Hospital, Cape Town: An Analysis of One Hundred and Sixty Cases Studied over a Six-Year Period. S. Afr. Med. J. Suid-Afr. Tydskr. Vir Geneeskd. 1959, 33, 810–817. [Google Scholar]
- Khorb, N.E.; Ouali, L.E.; Lahlou, I.; Ouaha, L.; Akoudad, H. La péricardite chronique constrictive. Moroc. J. Cardiol. 2012, 7, 16–20. [Google Scholar]
- Clare, G.C.; Troughton, R.W. Management of Constrictive Pericarditis in the 21st Century. Curr. Treat. Options Cardiovasc. Med. 2007, 9, 436–442. [Google Scholar] [CrossRef]
- Ghavidel, A.A.; Gholampour, M.; Kyavar, M.; Mirmesdagh, Y.; Tabatabaie, M.-B. Constrictive Pericarditis Treated by Surgery. Tex. Heart Inst. J. 2012, 39, 199–205. [Google Scholar] [PubMed]
- Conte, E.; Revaiah, P.C.; Tan, T.C. Pericardial Diseases: The Emerging Role for Cardiac Magnetic Resonance Imaging in the Diagnosis of Pericardial Diseases. Eur. Heart J. Case Rep. 2022, 6, ytac164. [Google Scholar] [CrossRef] [PubMed]
- Karima, T.; Nesrine, B.Z.; Hatem, L.; Skander, B.O.; Raouf, D.; Selim, C. Constrictive Pericarditis: 21 Years’ Experience and Review of Literature. Pan Afr. Med. J. 2021, 38, 141. [Google Scholar] [CrossRef] [PubMed]
- Yamani, N.; Abbasi, A.; Almas, T.; Mookadam, F.; Unzek, S. Diagnosis, Treatment, and Management of Pericardial Effusion- Review. Ann. Med. Surg. 2022, 80, 104142. [Google Scholar] [CrossRef]
- The EACVI Textbook of Echocardiography; Lancellotti, P.; Zamorano, J.L.; Habib, G.; Badano, L. (Eds.) Oxford University Press: Oxford, UK, 2016; Volume 1, ISBN 978-0-19-872601-2. [Google Scholar]
- Adler, Y.; Charron, P.; Imazio, M.; Badano, L.; Barón-Esquivias, G.; Bogaert, J.; Brucato, A.; Gueret, P.; Klingel, K.; Lionis, C.; et al. 2015 ESC Guidelines for the Diagnosis and Management of Pericardial Diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2015, 36, 2921–2964. [Google Scholar] [CrossRef] [PubMed]
- Di Gennaro, F.; Pisani, L.; Veronese, N.; Pizzol, D.; Lippolis, V.; Saracino, A.; Monno, L.; Huson, M.A.M.; Copetti, R.; Putoto, G.; et al. Potential Diagnostic Properties of Chest Ultrasound in Thoracic Tuberculosis-A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 2235. [Google Scholar] [CrossRef] [Green Version]
- Cocco, G.; Boccatonda, A.; Rossi, I.; D’Ardes, D.; Corvino, A.; Delli Pizzi, A.; Ucciferri, C.; Katia, F.; Jacopo, V. Early Detection of Pleuro-Pulmonary Tuberculosis by Bedside Lung Ultrasound: A Case Report and Review of Literature. Clin. Case Rep. 2022, 10, e05739. [Google Scholar] [CrossRef]
- Giannelli, F.; Cozzi, D.; Cavigli, E.; Campolmi, I.; Rinaldi, F.; Giachè, S.; Rogasi, P.G.; Miele, V.; Bartolucci, M. Lung Ultrasound (LUS) in Pulmonary Tuberculosis: Correlation with Chest CT and X-Ray Findings. J. Ultrasound 2022, 25, 625–634. [Google Scholar] [CrossRef]
- Isiguzo, G.; Du Bruyn, E.; Howlett, P.; Ntsekhe, M. Diagnosis and Management of Tuberculous Pericarditis: What Is New? Curr. Cardiol. Rep. 2020, 22, 2. [Google Scholar] [CrossRef]
- Noubiap, J.J.; Agbor, V.N.; Ndoadoumgue, A.L.; Nkeck, J.R.; Kamguia, A.; Nyaga, U.F.; Ntsekhe, M. Epidemiology of Pericardial Diseases in Africa: A Systematic Scoping Review. Heart Br. Card. Soc. 2019, 105, 180–188. [Google Scholar] [CrossRef]
- Ntsekhe, M.; Matthews, K.; Syed, F.F.; Deffur, A.; Badri, M.; Commerford, P.J.; Gersh, B.J.; Wilkinson, K.A.; Wilkinson, R.J.; Mayosi, B.M. Prevalence, Hemodynamics, and Cytokine Profile of Effusive-Constrictive Pericarditis in Patients with Tuberculous Pericardial Effusion. PLoS ONE 2013, 8, e77532. [Google Scholar] [CrossRef]
- Minardi, M.L.; Fato, I.; Di Gennaro, F.; Mosti, S.; Mastrobattista, A.; Cerva, C.; Libertone, R.; Saracino, A.; Goletti, D.; Girardi, E.; et al. Common and Rare Hematological Manifestations and Adverse Drug Events during Treatment of Active TB: A State of Art. Microorganisms 2021, 9, 1477. [Google Scholar] [CrossRef]
- Barzegari, S.; Afshari, M.; Movahednia, M.; Moosazadeh, M. Prevalence of Anemia among Patients with Tuberculosis: A Systematic Review and Meta-Analysis. Indian J. Tuberc. 2019, 66, 299–307. [Google Scholar] [CrossRef] [PubMed]
- De Vita, E.; Segala, F.V.; Amone, J.; Samuel, K.; Marotta, C.; Putoto, G.; Nassali, R.; Lochoro, P.; Bavaro, D.F.; Ictho, J.; et al. Subacute Cardiac Tamponade Due to Tuberculous Pericarditis Diagnosed by Urine Lipoarabinomannan Assay in a Immunocompetent Patient in Oyam District, Uganda: A Case Report. Int. J. Environ. Res. Public. Health 2022, 19, 15143. [Google Scholar] [CrossRef]
- Mathabire Rucker, S.C.; Cossa, L.; Harrison, R.E.; Mpunga, J.; Lobo, S.; Kisaka Kimupelenge, P.; Mandar Kol’Ampwe, F.; Amoros Quiles, I.; Molfino, L.; Szumilin, E.; et al. Feasibility of Using Determine TB-LAM to Diagnose Tuberculosis in HIV-Positive Patients in Programmatic Conditions: A Multisite Study. Glob. Health Action 2019, 12, 1672366. [Google Scholar] [CrossRef] [Green Version]
- Pandie, S.; Peter, J.G.; Kerbelker, Z.S.; Meldau, R.; Theron, G.; Govender, U.; Ntsekhe, M.; Dheda, K.; Mayosi, B.M. The Diagnostic Accuracy of Pericardial and Urinary Lipoarabinomannan (LAM) Assays in Patients with Suspected Tuberculous Pericarditis. Sci. Rep. 2016, 6, 32924. [Google Scholar] [CrossRef]
- Chatterjee, D.; Bozic, C.M.; McNeil, M.; Brennan, P.J. Structural Features of the Arabinan Component of the Lipoarabinomannan of Mycobacterium Tuberculosis. J. Biol. Chem. 1991, 266, 9652–9660. [Google Scholar] [CrossRef]
- Briken, V.; Porcelli, S.A.; Besra, G.S.; Kremer, L. Mycobacterial Lipoarabinomannan and Related Lipoglycans: From Biogenesis to Modulation of the Immune Response: The Mycobacterial Lipoarabinomannan and Related Molecules. Mol. Microbiol. 2004, 53, 391–403. [Google Scholar] [CrossRef] [PubMed]
- Mayosi, B.M.; Wiysonge, C.S.; Ntsekhe, M.; Gumedze, F.; Volmink, J.A.; Maartens, G.; Aje, A.; Thomas, B.M.; Thomas, K.M.; Awotedu, A.A.; et al. Mortality in Patients Treated for Tuberculous Pericarditis in Sub-Saharan Africa. S. Afr. Med. J. Suid-Afr. Tydskr. Vir Geneeskd. 2008, 98, 36–40. [Google Scholar]
- Syed, F.F.; Mayosi, B.M. A Modern Approach to Tuberculous Pericarditis. Prog. Cardiovasc. Dis. 2007, 50, 218–236. [Google Scholar] [CrossRef]
- Jung, I.Y.; Song, Y.G.; Choi, J.Y.; Kim, M.H.; Jeong, W.Y.; Oh, D.H.; Kim, Y.C.; Song, J.E.; Kim, E.J.; Lee, J.U.; et al. Predictive Factors for Unfavorable Outcomes of Tuberculous Pericarditis in Human Immunodeficiency Virus-Uninfected Patients in an Intermediate Tuberculosis Burden Country. BMC Infect. Dis. 2016, 16, 719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quale, J.M.; Lipschik, G.Y.; Heurich, A.E. Management of Tuberculous Pericarditis. Ann. Thorac. Surg. 1987, 43, 653–655. [Google Scholar] [CrossRef] [PubMed]
- Trautner, B.W.; Darouiche, R.O. Tuberculous Pericarditis: Optimal Diagnosis and Management. Clin. Infect. Dis. 2001, 33, 954–961. [Google Scholar] [CrossRef]
- Esmail, H.; Macpherson, L.; Coussens, A.K.; Houben, R.M.G.J. Mind the Gap – Managing Tuberculosis across the Disease Spectrum. eBioMedicine 2022, 78, 103928. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for Treatment of Drug-Susceptible Tuberculosis and Patient Care; World Health Organization: Geneva, Switzerland, 2017; update; ISBN 978-92-4-155000-0. [Google Scholar]
- Naidoo, D.; Laurence, G.; Ponnusamy, S.; Sartorius, B. The Effects of HIV/AIDS on the Clinical Profile and Outcomes Post Pericardiectomy of Patients with Constrictive Pericarditis: A Retrospective Review. Cardiovasc. J. Afr. 2019, 30, 251–257. [Google Scholar] [CrossRef] [Green Version]
- Mayosi, B.M.; Ntsekhe, M.; Bosch, J.; Pandie, S.; Jung, H.; Gumedze, F.; Pogue, J.; Thabane, L.; Smieja, M.; Francis, V.; et al. Prednisolone and Mycobacterium Indicus Pranii in Tuberculous Pericarditis. N. Engl. J. Med. 2014, 371, 1121–1130. [Google Scholar] [CrossRef] [Green Version]
- Steigler, P.; Chhiba, M.; Francis, V.; Keyser, A.; Abrahams, D.; Hanekom, W.; Ntsekhe, M.; Scriba, T.J. T Cell Responses to Mycobacterium Indicus Pranii Immunotherapy and Adjunctive Glucocorticoid Therapy in Tuberculous Pericarditis. Vaccine X 2022, 11, 100177. [Google Scholar] [CrossRef]
- Yadav, S.; Shah, S.; Iqbal, Z.; Alharbi, M.G.; Kalra, H.S.; Suri, M.; Soni, N.; Okpaleke, N.; Hamid, P. Pericardiectomy for Constrictive Tuberculous Pericarditis: A Systematic Review and Meta-Analysis on the Etiology, Patients’ Characteristics, and the Outcomes. Cureus 2021, 13, e18252. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.K.; Lucas, S.B.; Fielding, K.L.; Lawn, S.D. Prevalence of Tuberculosis in Post-Mortem Studies of HIV-Infected Adults and Children in Resource-Limited Settings: A Systematic Review and Meta-Analysis. AIDS Lond. Engl. 2015, 29, 1987–2002. [Google Scholar] [CrossRef] [Green Version]
- Nelson, L.J.; Wells, C.D. Global Epidemiology of Childhood Tuberculosis. Int. J. Tuberc. Lung Dis. Off. J. Int. Union Tuberc. Lung Dis. 2004, 8, 636–647. [Google Scholar]
- Obihara, N.J.; Walters, E.; Lawrenson, J.; Garcia-Prats, A.J.; Hesseling, A.C.; Schaaf, H.S. Tuberculous Pericardial Effusions in Children. J. Pediatr. Infect. Dis. Soc. 2018, 7, 346–349. [Google Scholar] [CrossRef]
- Watch, V.; Aipit, J.; Kote-Yarong, T.; Rero, A.; Bolnga, J.W.; Lufele, E.; Laman, M. The Burden of Presumed Tuberculosis in Hospitalized Children in a Resource-Limited Setting in Papua New Guinea: A Prospective Observational Study. Int. Health 2017, 9, 374–378. [Google Scholar] [CrossRef]
- Aia, P.; Wangchuk, L.; Morishita, F.; Kisomb, J.; Yasi, R.; Kal, M.; Islam, T. Epidemiology of Tuberculosis in Papua New Guinea: Analysis of Case Notification and Treatment-Outcome Data, 2008-2016. West. Pac. Surveill. Response J. WPSAR 2018, 9, 9–19. [Google Scholar] [CrossRef]
- Castro, I.F.; Isorno-Porto, M.J.; Novo-Veleiro, I.; Casar-Cocheteux, C.; Barrera-López, L.; Andrade-Piña, A.H.; López-Rodríguez, M.; Reino, A.P. An Atypical Manifestation of Mycobacterium Tuberculosis Infection. Eur. J. Case Rep. Intern. Med. 2021, 8, 002598. [Google Scholar] [CrossRef]
- Long, R.; Guzman, R.; Greenberg, H.; Safneck, J.; Hershfield, E. Tuberculous Mycotic Aneurysm of the Aorta: Review of Published Medical and Surgical Experience. Chest 1999, 115, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Golzarian, J.; Cheng, J.; Giron, F.; Bilfinger, T.V. Tuberculous Pseudoaneurysm of the Descending Thoracic Aorta: Successful Treatment by Surgical Excision and Primary Repair. Tex. Heart Inst. J. 1999, 26, 232–235. [Google Scholar] [PubMed]
- Tran, H.V.; Ho, D.K.; Le, V.H.; Van Duong, H. Ruptured Tuberculous Aneurysms of the Abdominal Aorta: Two Case Series. Int. J. Surg. Case Rep. 2022, 92, 106860. [Google Scholar] [CrossRef]
- Canaud, L.; Marzelle, J.; Bassinet, L.; Carrié, A.-S.; Desgranges, P.; Becquemin, J.-P. Tuberculous Aneurysms of the Abdominal Aorta. J. Vasc. Surg. 2008, 48, 1012–1016. [Google Scholar] [CrossRef] [Green Version]
- Palaniswamy, C.; Kumar, U.; Selvaraj, D.R.; Pandey, B.; Handa, R.; Alappan, N.K.; Sharma, H. Tuberculous Mycotic Aneurysm of Aortic Root: An Unusual Cause of Cardiac Tamponade. Trop. Doct. 2009, 39, 112–113. [Google Scholar] [CrossRef]
- Pathirana, U.; Kularatne, S.; Karunaratne, S.; Ranasinghe, G.; Fernando, J. Ascending Aortic Aneurysm Caused by Mycobacterium Tuberculosis. BMC Res. Notes 2015, 8, 659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahabuddin, S.; Sami, S.A. Tuberculous Ascending Aortic Pseudoaneurysm. Interact. Cardiovasc. Thorac. Surg. 2013, 17, 742–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delaval, L.; Goulenok, T.; Achouh, P.; Saadoun, D.; Gaudric, J.; Pellenc, Q.; Kahn, J.-E.; Pasi, N.; van Gysel, D.; Bruneval, P.; et al. New Insights on Tuberculous Aortitis. J. Vasc. Surg. 2017, 66, 209–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, J.R.; Bruneval, P.; Angelini, A.; Bartoloni, G.; Basso, C.; Batoroeva, L.; Buja, L.M.; Butany, J.; d’Amati, G.; Fallon, J.T.; et al. Consensus Statement on Surgical Pathology of the Aorta from the Society for Cardiovascular Pathology and the Association for European Cardiovascular Pathology: I. Inflammatory Diseases. Cardiovasc. Pathol. 2015, 24, 267–278. [Google Scholar] [CrossRef]
- Soto, M.E.; Del Carmen Ávila-Casado, M.; Huesca-Gómez, C.; Alarcon, G.V.; Castrejon, V.; Soto, V.; Hernandez, S.; Espinola-Zavaleta, N.; Vallejo, M.; Reyes, P.A.; et al. Detection of IS6110 and HupB Gene Sequences of Mycobacterium Tuberculosis and Bovis in the Aortic Tissue of Patients with Takayasu’s Arteritis. BMC Infect. Dis. 2012, 12, 194. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, A.; Chag, M.; Sinha, N.; Naik, S. Takayasu’s Arteritis: Role of Mycobacterium Tuberculosis and Its 65 KDa Heat Shock Protein. Int. J. Cardiol. 1996, 55, 49–55. [Google Scholar] [CrossRef]
- Fama’, F.; Sindoni, A.; Donato, R.; Cascio, A.; Mondello, P.; Gaeta, R. Tuberculous Aortitis in an Human Immunodeficiency Virus–Positive Ivorian Migrant: A Case Report. Int. J. STD AIDS 2021, 32, 1361–1364. [Google Scholar] [CrossRef]
- Tsurutani, H.; Tomonaga, M.; Yamaguchi, T.; Sakai, H.; Soejima, Y.; Kadota, J.; Kohno, S. Hepatic Artery Pseudoaneurysms in a Patient Treated for Miliary Tuberculosis. Intern. Med. 2000, 39, 994–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hideaki, I.; Reiko, O. A Successfully Treated Case of Miliary Tuberculosis with Adult Respiratory Distress Syndrome and Tuberculous Aneurysm of Abdominal Aorta. Kekkaku (Tuberculosis) 1998, 73, 403–411. [Google Scholar] [CrossRef]
- Liu, W.C.; Kwak, B.K.; Kim, K.N.; Kim, S.Y.; Woo, J.J.; Chung, D.J.; Hong, J.H.; Kim, H.S.; Lee, C.J.; Shim, H.J. Tuberculous Aneurysm of the Abdominal Aorta: Endovascular Repair Using Stent Grafts in Two Cases. Korean J. Radiol. 2000, 1, 215–218. [Google Scholar] [CrossRef] [Green Version]
- Bukhary, Z.A.; Alrajhi, A.A. Tuberculous Aortitis. Ann. Saudi Med. 2006, 26, 56–58. [Google Scholar] [CrossRef] [Green Version]
- Tofeig, M. Tuberculous Aortitis | Radiology Reference Article | Radiopaedia. Available online: https://radiopaedia.org/articles/tuberculous-aortitis?utm_medium=email&utm_source=transaction (accessed on 30 November 2022).
- See, J. Aortic Aneurysm Secondary to TB Aortitis Due to TB-Induced Inflammation of the Vasa Vasorum: A Case Series. CHEST 2017, 152, A148. [Google Scholar] [CrossRef]
- de Kruijf, E.J.F.M.; van Rijn, A.B.B.; Koelma, I.A.; Kuijpers, T.J.A.; van ’t Wout, J.W. Tuberculous Aortitis with an Aortoduodenal Fistula Presenting as Recurrent Gastrointestinal Bleeding. Clin. Infect. Dis. 2000, 31, 841–842. [Google Scholar] [CrossRef] [Green Version]
- Hsu, Y.-C.; Luo, C.-Y.; Tsai, Y.-S. Tuberculous Aortitis Associated With Pleuritis and Spondylitis. Heart Lung Circ. 2018, 27, e84–e85. [Google Scholar] [CrossRef]
- Manika, K.; Efthymiou, C.; Damianidis, G.; Zioga, E.; Papadaki, E.; Lagoudi, K.; Kioumis, I. Miliary Tuberculosis in a Patient with Tuberculous Mycotic Aneurysm of the Abdominal Aorta: Case Report and Review of the Literature. Respir. Med. Case Rep. 2017, 21, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Chen, B.; Gu, Y.; Luo, T.; Yang, S.; Liang, W.; Wang, Z. Tuberculous Abdominal Aortic Pseudoaneurysm with Renal and Vertebral Tuberculosis: A Case and Literature Review. J. Infect. Dev. Ctries. 2014, 8, 1216–1221. [Google Scholar] [CrossRef] [Green Version]
- Azuma, S.; Fukuhara, S.; Yasuyoshi, Y. Endovascular Treatment of a Tuberculous Aneurysm of the Pararenal Abdominal Aorta Leading to an Aortoduodenal Fistula. J. Vasc. Surg. Cases Innov. Tech. 2022, 8, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Rob, C.G.; Eastcott, H.H.G. Aortic Aneurysm Due to Tuberculous Lymphadenitis. Br. Med. J. 1955, 1, 378–379. [Google Scholar] [CrossRef] [Green Version]
- Labrousse, L.; Montaudon, M.; Le Guyader, A.; Choukroun, E.; Laurent, F.; Deville, C. Endovascular Treatment of a Tuberculous Infected Aneurysm of the Descending Thoracic Aorta: A Word of Caution. J. Vasc. Surg. 2007, 46, 786–788. [Google Scholar] [CrossRef] [Green Version]
- Jagia, P.; Gulati, G.S.; Sharma, S.; Goyal, N.K.; Gaikwad, S.; Saxena, A. MRI Features of Tuberculoma of the Right Atrial Myocardium. Pediatr. Radiol. 2004, 34, 904–907. [Google Scholar] [CrossRef]
- Rose, A.G. Cardiac Tuberculosis. A Study of 19 Patients. Arch. Pathol. Lab. Med. 1987, 111, 422–426. [Google Scholar]
- Njovane, X. Intramyocardial Tuberculosis—A Rare Underdiagnosed Entity. S. Afr. Med. J. Suid-Afr. Tydskr. Vir Geneeskd. 2009, 99, 152–153. [Google Scholar]
- Licht, J.; Diefenbach, C.; Stang, A.; Hartmann, V.; Bolte, J.; Kirsten, D. Tuberculoma of the Myocardium: A Rare Case of Intra-Vitam Diagnosis. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2009, 98, 331–333. [Google Scholar] [CrossRef]
- Gulati, G.S.; Kothari, S.S. Diffuse Infiltrative Cardiac Tuberculosis. Ann. Pediatr. Cardiol. 2011, 4, 87–89. [Google Scholar] [CrossRef]
- Cantinotti, M.; De Gaudio, M.; de Martino, M.; Assanta, N.; Moschetti, R.; Veneruso, G.; Crocetti, M.; Murzi, B.; Chiappini, E.; Galli, L. Intracardiac Left Atrial Tuberculoma in an Eleven-Month-Old Infant: Case Report. BMC Infect. Dis. 2011, 11, 359. [Google Scholar] [CrossRef] [Green Version]
- Chang, B.C.; Ha, J.W.; Kim, J.T.; Chung, N.; Cho, S.H. Intracardiac Tuberculoma. Ann. Thorac. Surg. 1999, 67, 226–228. [Google Scholar] [CrossRef]
- Borrhomée, S.; Vergnat, M.; Roussin, R.; Hascoët, S. A Rare Case of Left Ventricular Pseudoaneurysm Due To Tuberculosis in a 13-Year-Old Boy. World J. Pediatr. Congenit. Heart Surg. 2019, 10, 370–372. [Google Scholar] [CrossRef] [PubMed]
- Säll, O.; Cha, S.-O.; Holmberg, H. Diagnostic Challenges in a Patient with Myocardial Tuberculoma: A Case Report. Int. J. Surg. Case Rep. 2016, 29, 201–203. [Google Scholar] [CrossRef] [Green Version]
- Hashmani, S.; Tipoo Sultan, F.A.; Masood, M.Q. Unusual Presentation of a Young Man with Disseminated Tuberculosis and Right Ventricular Mass. BMJ Case Rep. 2016, 2016, bcr2016216964. [Google Scholar] [CrossRef]
- Dooley, K.E.; Rosenkranz, S.L.; Conradie, F.; Moran, L.; Hafner, R.; von Groote-Bidlingmaier, F.; Lama, J.R.; Shenje, J.; Rios, J.D.L.; Comins, K.; et al. QT Effects of Bedaquiline, Delamanid, or Both in Patients with Rifampicin-Resistant Tuberculosis: A Phase 2, Open-Label, Randomised, Controlled Trial. Lancet Infect. Dis. 2021, 21, 975–983. [Google Scholar] [CrossRef]
- Polak, S.; Romero, K.; Berg, A.; Patel, N.; Jamei, M.; Hermann, D.; Hanna, D. Quantitative Approach for Cardiac Risk Assessment and Interpretation in Tuberculosis Drug Development. J. Pharmacokinet. Pharmacodyn. 2018, 45, 457–467. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marcu, D.T.M.; Adam, C.A.; Mitu, F.; Cumpat, C.; Aursulesei Onofrei, V.; Zabara, M.L.; Burlacu, A.; Crisan Dabija, R. Cardiovascular Involvement in Tuberculosis: From Pathophysiology to Diagnosis and Complications—A Narrative Review. Diagnostics 2023, 13, 432. https://doi.org/10.3390/diagnostics13030432
Marcu DTM, Adam CA, Mitu F, Cumpat C, Aursulesei Onofrei V, Zabara ML, Burlacu A, Crisan Dabija R. Cardiovascular Involvement in Tuberculosis: From Pathophysiology to Diagnosis and Complications—A Narrative Review. Diagnostics. 2023; 13(3):432. https://doi.org/10.3390/diagnostics13030432
Chicago/Turabian StyleMarcu, Dragos Traian Marius, Cristina Andreea Adam, Florin Mitu, Carmen Cumpat, Viviana Aursulesei Onofrei, Mihai Lucian Zabara, Alexandru Burlacu, and Radu Crisan Dabija. 2023. "Cardiovascular Involvement in Tuberculosis: From Pathophysiology to Diagnosis and Complications—A Narrative Review" Diagnostics 13, no. 3: 432. https://doi.org/10.3390/diagnostics13030432