
Challenges in the Diagnosis of Cutaneous Mastocytosis
 , , , and
, , , and
Abstract
:1. Introduction
2. Challenges in the Use of the Nomenclature for Cutaneous Mastocytosis
3. Clinical Diagnosis of Cutaneous Mastocytosis
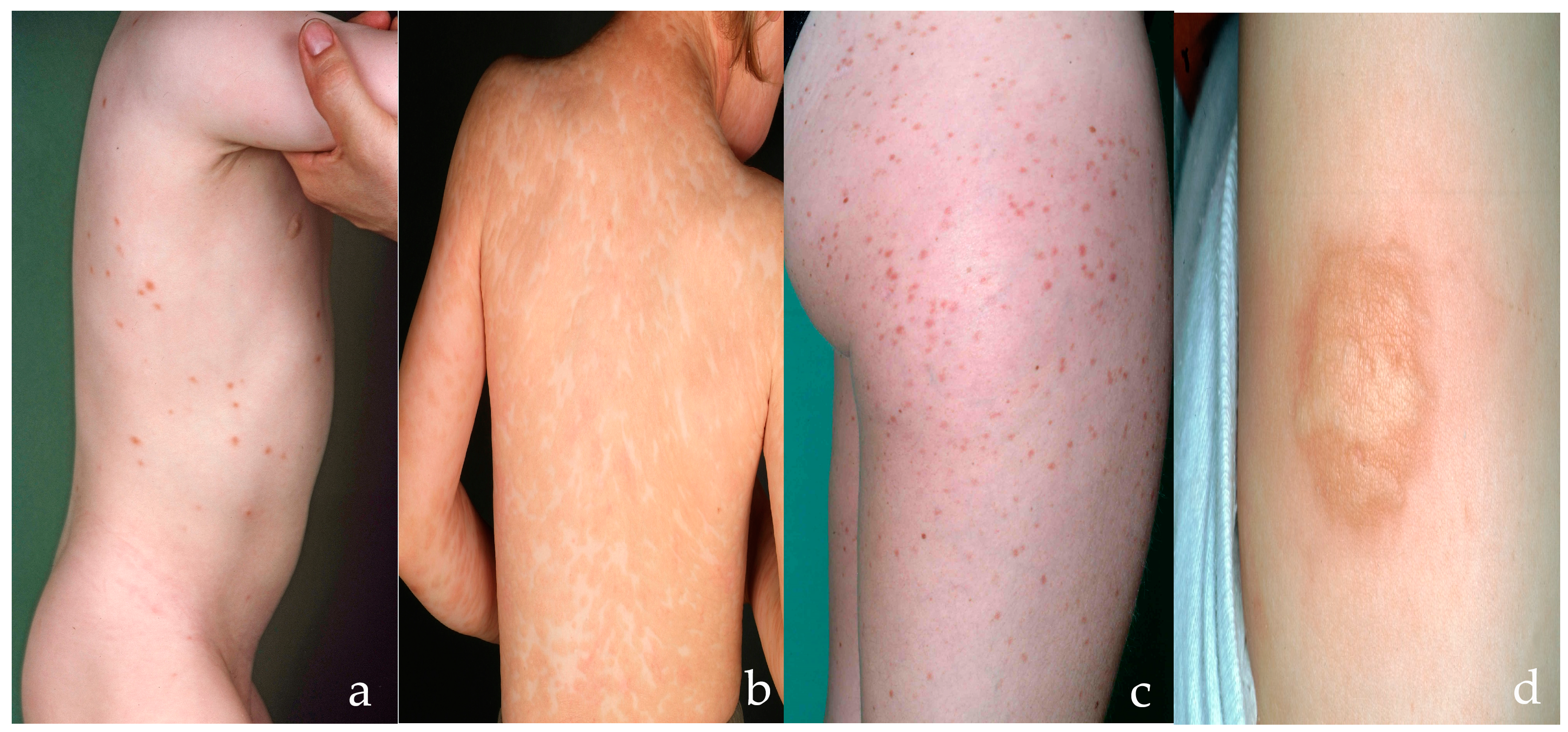
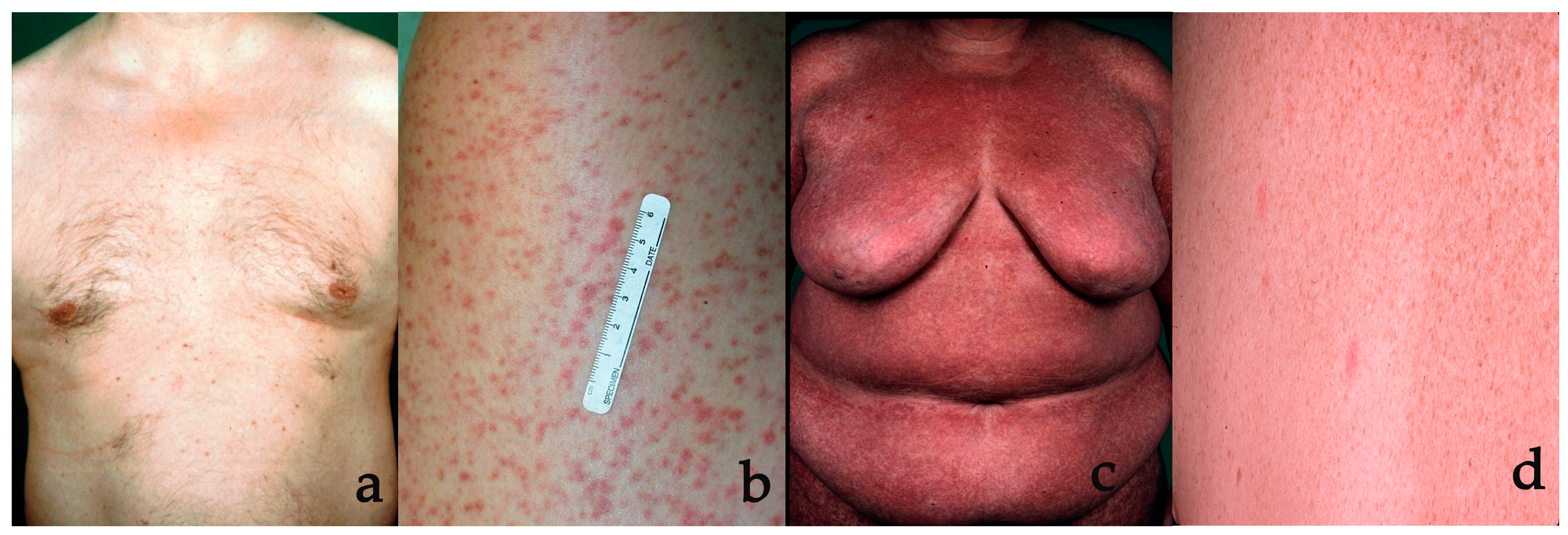
3.1. Typical Clinical Presentations
3.2. Darier’s Sign
3.3. Less Typical Clinical Presentations
3.4. Differential Diagnoses
4. Confirmation of the Diagnosis of Cutaneous Mastocytosis
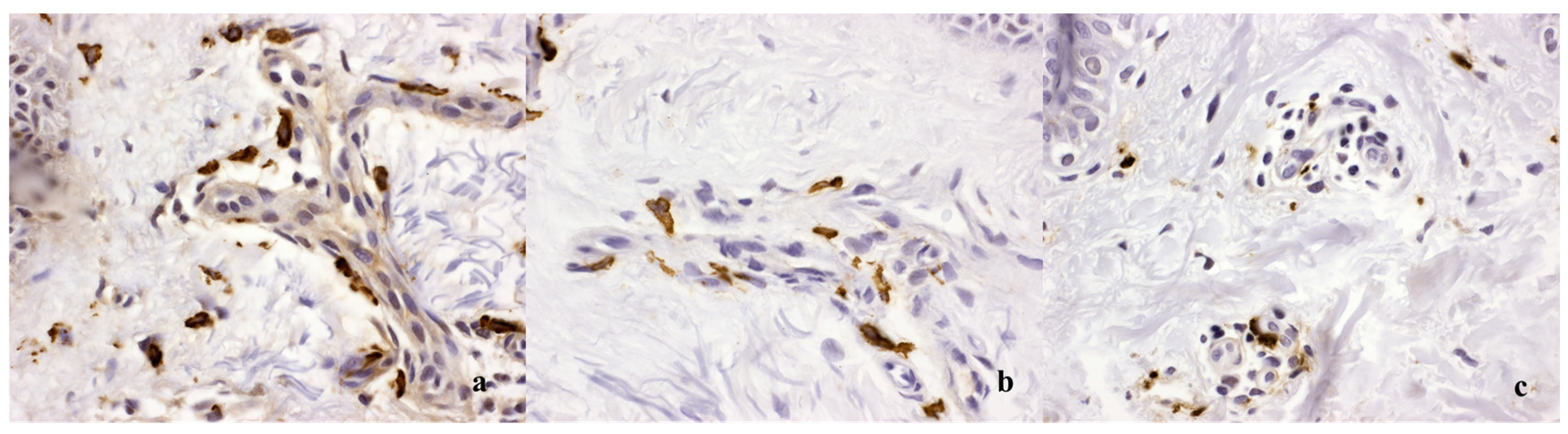
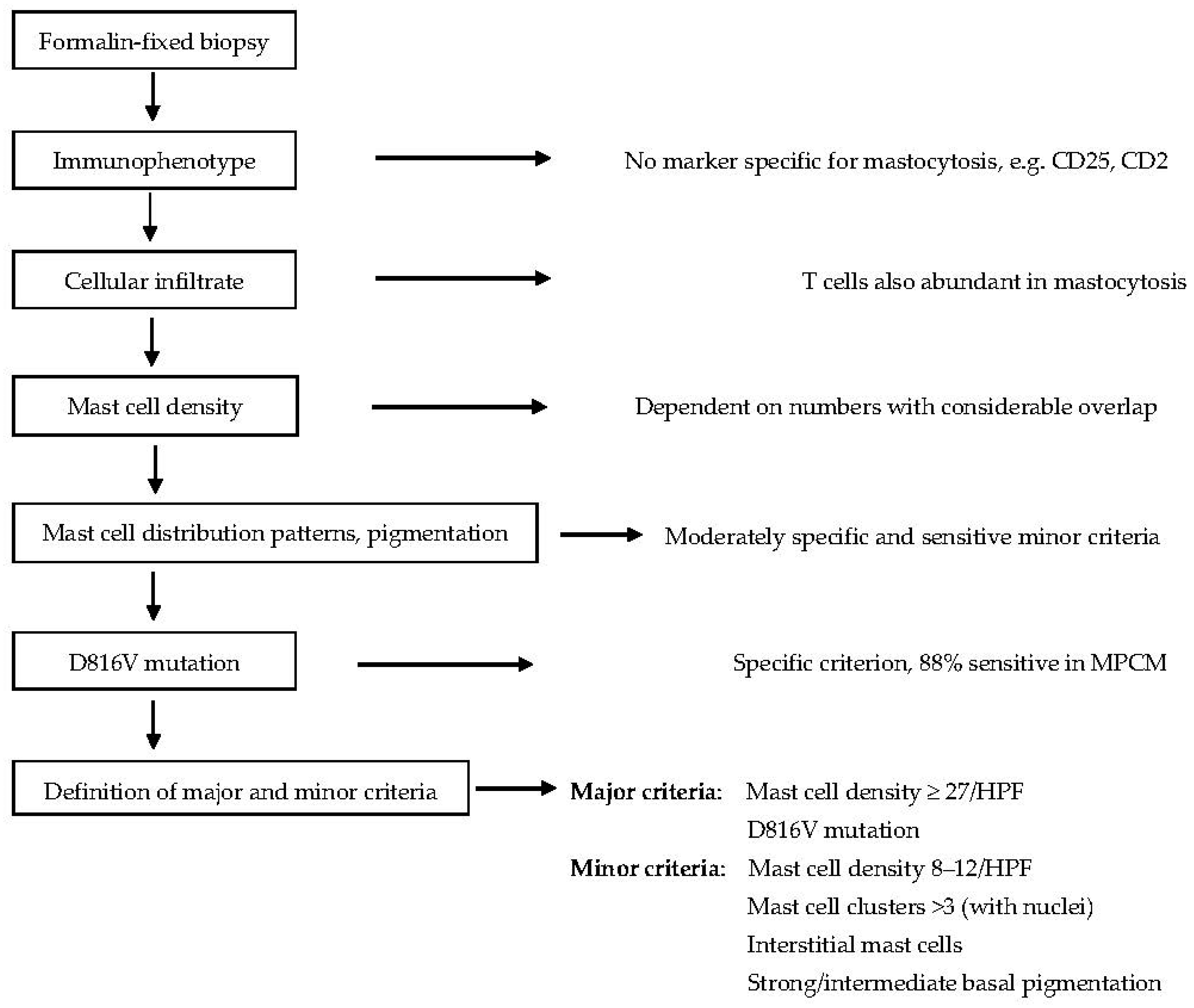
4.1. Dermatohistopathology
4.2. KIT Mutation Analysis
5. Prediction of Evolution or Resolution of Disease
6. Further Assessments in Patients with Cutaneous Mastocytosis
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMB | Bone marrow biopsy |
| CLM | Cutaneous lesions of mastocytosis |
| CM | Cutaneous Mastocytosis |
| DCM | Diffuse cutaneous mastocytosis |
| ISM | Indolent systemic mastocytosis |
| MIS | Mastocytosis in the Skin |
| MPCM | Maculopapular cutaneous mastocytosis |
| MC | Mast cell |
| HPF | High power field (defined as 0.196 mm2) |
| SM | Systemic mastocytosis |
References
- Arber, D.A.; Orazi, A.; Hasserjian, R.P.; Borowitz, M.J.; Calvo, K.R.; Kvasnicka, H.M.; Wang, S.A.; Bagg, A.; Barbui, T.; Branford, S.; et al. International Consensus Classification of Myeloid Neoplasms and Acute Leukemias: Integrating morphologic, clinical, and genomic data. Blood 2022, 140, 1200–1228. [Google Scholar] [CrossRef] [PubMed]
- Khoury, J.D.; Solary, E.; Abla, O.; Akkari, Y.; Alaggio, R.; Apperley, J.F.; Bejar, R.; Berti, E.; Busque, L.; Chan, J.K.C.; et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia 2022, 36, 1703–1719. [Google Scholar] [CrossRef] [PubMed]
- Brockow, K. Urticaria pigmentosa. Immunol. Allergy Clin. N. Am. 2004, 24, 287–316. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, K.; Escribano, L.; Grattan, C.; Brockow, K.; Carter, M.C.; Alvarez-Twose, I.; Matito, A.; Broesby-Olsen, S.; Siebenhaar, F.; Lange, M.; et al. Cutaneous manifestations in patients with mastocytosis: Consensus report of the European Competence Network on Mastocytosis; the American Academy of Allergy, Asthma & Immunology; and the European Academy of Allergology and Clinical Immunology. J. Allergy Clin. Immunol. 2016, 137, 35–45. [Google Scholar] [PubMed]
- Brockow, K. Epidemiology, prognosis, and risk factors in mastocytosis. Immunol. Allergy Clin. N. Am. 2014, 34, 283–295. [Google Scholar] [CrossRef] [PubMed]
- Schuch, A.; Brockow, K. Mastocytosis and Anaphylaxis. Immunol. Allergy Clin. N. Am. 2017, 37, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Zuberbier, T.; Aberer, W.; Asero, R.; Abdul Latiff, A.H.; Baker, D.; Ballmer-Weber, B.; Church, M.K.; Ensina, L.F.; Giménez-Arnau, A.; Godse, K.; et al. The EAACI/GA(2)LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of urticaria. Allergy 2018, 73, 1393–1414. [Google Scholar] [CrossRef] [PubMed]
- Valent, P.; Akin, C.; Hartmann, K.; Alvarez-Twose, I.; Brockow, K.; Hermine, O.; Niedoszytko, M.; Schwaab, J.; Lyons, J.J.; Carter, M.C.; et al. Updated Diagnostic Criteria and Classification of Mast Cell Disorders: A Consensus Proposal. Hemasphere 2021, 5, e646. [Google Scholar] [CrossRef]
- Sotlar, K.; George, T.I.; Kluin, P.; Reiter, A.; Schwaab, J.; Panse, J.; Brockow, K.; Hartmann, K.; Sperr, W.R.; Kristensen, T.; et al. Standards of Pathology in the Diagnosis of Systemic Mastocytosis: Recommendations of the EU-US Cooperative Group. J. Allergy Clin. Immunol. Pract. 2022, 10, 1986–1998. [Google Scholar] [CrossRef]
- Valent, P.; Akin, C.; Escribano, L.; Fodinger, M.; Hartmann, K.; Brockow, K.; Castells, M.; Sperr, W.R.; Kluin-Nelemans, H.C.; Hamdy, N.A.T.; et al. Standards and standardization in mastocytosis: Consensus statements on diagnostics, treatment recommendations and response criteria. Eur. J. Clin. Investig. 2007, 37, 435–453. [Google Scholar] [CrossRef]
- Brockow, K.; Akin, C.; Huber, M.; Metcalfe, D. Assessment of the extent of cutaneous involvement in children and adults with mastocytosis: Relationship to symptomatology, tryptase levels, and bone marrow pathology. J. Am. Acad. Dermatol. 2003, 48, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Brockow, K. Unsatisfactory agreement using current classification of maculopapular cutaneous mastocytosis. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 1917–1918. [Google Scholar] [CrossRef]
- Torrelo, A.; Vergara-de-la-Campa, L.; Azana, J.M.; Greenberger, S.; Lam, J.M.; Lawley, L.P.; Morren, M.-A.; Schaffer, J.V.; García-Doval, I.; Matito, A.; et al. Interobserver variability in the classification of childhood maculopapular cutaneous mastocytosis. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 2079–2084. [Google Scholar] [CrossRef] [PubMed]
- Brockow, K.; Metcalfe, D.D. Mastocytosis. Chem. Immunol. Allergy 2010, 95, 110–124. [Google Scholar] [PubMed]
- Ludolph-Hauser, D.; Schopf, P.; Rueff, F.; Przybilla, B. Okkulte kutane Mastozytose. Hautarzt 2001, 52, 390–393. [Google Scholar] [CrossRef]
- Valent, P.; Horny, H.P.; Escribano, L.; Longley, B.J.; Li, C.Y.; Schwartz, L.B.; Marone, G.; Nuñez, R.; Akin, C.; Sotlar, K.; et al. Diagnostic criteria and classification of mastocytosis: A consensus proposal. Leuk. Res. 2001, 25, 603–625. [Google Scholar] [CrossRef]
- Parks, A.; Camisa, C. Reddish-brown macules with telangiectasia and pruritus. Urticaria pigmentosa-telangiectasia macularis eruptiva perstans (TMEP) variant, with systemic mastocytosis. Arch. Dermatol. 1988, 124, 429–430, 432–433. [Google Scholar] [CrossRef]
- Williams, K.W.; Metcalfe, D.D.; Prussin, C.; Carter, M.C.; Komarow, H.D. Telangiectasia macularis eruptiva perstans or highly vascularized urticaria pigmentosa? J. Allergy Clin. Immunol. Pract. 2014, 2, 813–815. [Google Scholar] [CrossRef]
- Zink, A.; Bohner, A.; Schuch, A.; Biedermann, T.; Brockow, K. Systemic mastocytosis with generalised skin involvement. Lancet 2017, 389, 940. [Google Scholar] [CrossRef]
- Husak, R.; Blume-Peytavi, U.; Pfrommer, C.; Geilen, C.C.; Goerdt, S.; Orfanos, C.E. Nodular and bullous cutaneous mastocytosis of the xanthelasmoid type: Case report. Br. J. Dermatol. 2001, 144, 355–358. [Google Scholar] [CrossRef]
- Griffiths, W.A.; Daneshbod, K. Pseudoxanthomatous mastocytosis. Br. J. Dermatol. 1975, 93, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Brockow, K.; Ring, J.; Alvarez-Twose, I.; Orfao, A.; Escribano, L. Extensive blistering is a predictor for severe complications in children with mastocytosis. Allergy 2012, 67, 1323–1324. [Google Scholar] [CrossRef] [PubMed]
- Eichenfield, L.F.; Honig, P.J. Blistering disorders in childhood. Pediatr. Clin. N. Am. 1991, 38, 959–976. [Google Scholar] [CrossRef] [PubMed]
- Cosulich, M.T.; Norton, S.A. Dermatographic fixed-drug eruption: Another cause of pseudo-Darier’s sign. Skinmed 2013, 11, 368–369. [Google Scholar] [PubMed]
- Viglizzo, G.; Nemelka, O.; Nozza, P.; Occella, C.; Rongioletti, F. Congenital smooth muscle hamartoma presenting with an unusual pseudo-Darier’s sign. Clin. Exp. Dermatol. 2006, 31, 148–149. [Google Scholar] [CrossRef] [PubMed]
- Aberer, E.; Sperr, W.R.; Bretterklieber, A.; Avian, A.; Hadzijusufovic, E.; Kluin-Nelemans, H.C.; Oude Elberink, H.; van Anrooij, B.; Niedoszytko, M.; Lange, M.; et al. Clinical Impact of Skin Lesions in Mastocytosis: A Multicenter Study of the European Competence Network on Mastocytosis. J. Investig. Dermatol. 2021, 141, 1719–1727. [Google Scholar] [CrossRef]
- Fuchs, D.; Kilbertus, A.; Kofler, K.; von Bubnoff, N.; Shoumariyeh, K.; Zanotti, R.; Bonadonna, P.; Scaffidi, L.; Doubek, M.; Elberink, H.O.; et al. Scoring the Risk of Having Systemic Mastocytosis in Adult Patients with Mastocytosis in the Skin. J. Allergy Clin. Immunol. Pract. 2021, 9, 1705–1712.e4. [Google Scholar] [CrossRef] [PubMed]
- Gebhard, J.; Horny, H.P.; Kristensen, T.; Broesby-Olsen, S.; Zink, A.; Biedermann, T.; Brockow, K. Validation of dermatopathological criteria to diagnose cutaneous lesions of mastocytosis: Importance of KIT D816V mutation analysis. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1367–1375. [Google Scholar] [CrossRef]
- Irani, A.A.; Garriga, M.M.; Metcalfe, D.D.; Schwartz, L.B. Mast cells in cutaneous mastocytosis: Accumulation of the MCTC type. Clin. Exp. Allergy 1990, 20, 53–58. [Google Scholar] [CrossRef]
- Brockow, K.; Akin, C.; Huber, M.; Scott, L.M.; Schwartz, L.B.; Metcalfe, D.D. Levels of mast cell growth factors in plasma and in suction skin blister fluid in adults with mastocytosis: Correlation with dermal mast cell numbers and mast cell tryptase. J. Allergy Clin. Immunol. 2002, 109, 82–88. [Google Scholar] [CrossRef]
- Horny, H.P.; Valent, P. Histopathological and immunohistochemical aspects of mastocytosis. Int. Arch. Allergy Immunol. 2002, 127, 115–117. [Google Scholar] [CrossRef] [PubMed]
- Mihm, M.C.; Clark, W.H.; Reed, R.J.; Caruso, M.G. Mast cell infiltrates of the skin and the mastocytosis syndrome. Hum. Pathol. 1973, 4, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, T.; Broesby-Olsen, S.; Vestergaard, H.; Bindslev-Jensen, C.; Moller, M.B. KIT D816V mutation-positive cell fractions in lesional skin biopsies from adults with systemic mastocytosis. Dermatology 2013, 226, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, T.; Vestergaard, H.; Bindslev-Jensen, C.; Moller, M.B.; Broesby-Olsen, S. Sensitive KIT D816V mutation analysis of blood as a diagnostic test in mastocytosis. Am. J. Hematol. 2014, 89, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.C.; Bai, Y.; Ruiz-Esteves, K.N.; Scott, L.M.; Cantave, D.; Bolan, H.; Eisch, R.; Sun, X.; Hahn, J.; Maric, I.; et al. Detection of KIT D816V in peripheral blood of children with manifestations of cutaneous mastocytosis suggests systemic disease. Br. J. Haematol. 2018, 183, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Uzzaman, A.; Maric, I.; Noel, P.; Kettelhut, B.V.; Metcalfe, D.D.; Carter, M.C. Pediatric-onset mastocytosis: A long term clinical follow-up and correlation with bone marrow histopathology. Pediatr. Blood Cancer 2009, 53, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Lange, M.; Hartmann, K.; Carter, M.C.; Siebenhaar, F.; Alvarez-Twose, I.; Torrado, I.; Brockow, K.; Renke, J.; Irga-Jaworska, N.; Plata-Nazar, K.; et al. Molecular Background, Clinical Features and Management of Pediatric Mastocytosis: Status 2021. Int. J. Mol. Sci. 2021, 22, 2586. [Google Scholar] [CrossRef]
- Carter, M.C.; Clayton, S.T.; Komarow, H.D.; Brittain, E.H.; Scott, L.M.; Cantave, D.; Gaskins, D.M.; Maric, I.; Metcalfe, D.D. Assessment of clinical findings, tryptase levels, and bone marrow histopathology in the management of pediatric mastocytosis. J. Allergy Clin. Immunol. 2015, 136, 1673–1679.e3. [Google Scholar] [CrossRef]
- Wiechers, T.; Rabenhorst, A.; Schick, T.; Preussner, L.M.; Forster, A.; Valent, P.; Horny, H.-P.; Sotlar, K.; Hartmann, K. Large maculopapular cutaneous lesions are associated with favorable outcome in childhood-onset mastocytosis. J. Allergy Clin. Immunol. 2015, 136, 1581–1590.e3. [Google Scholar] [CrossRef]
- Metcalfe, D.D. Classification and diagnosis of mastocytosis: Current status. J. Investig. Dermatol. 1991, 96, 2S–4S. [Google Scholar] [CrossRef]
- Brockow, K.; Scott, L.M.; Worobec, A.S.; Kirshenbaum, A.; Akin, C.; Huber, M.M.; Metcalfe, D. Regression of urticaria pigmentosa in adult patients with systemic mastocytosis: Correlation with clinical patterns of disease. Arch. Dermatol. 2002, 138, 785–790. [Google Scholar] [CrossRef]
- Escribano, L.; Alvarez-Twose, I.; Sanchez-Munoz, L.; Garcia-Montero, A.; Nunez, R.; Almeida, J.; Jara-Acevedo, M.; Teodósio, C.; García-Cosío, M.; Bellas, C.; et al. Prognosis in adult indolent systemic mastocytosis: A long-term study of the Spanish Network on Mastocytosis in a series of 145 patients. J. Allergy Clin. Immunol. 2009, 124, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Valent, P.; Hartmann, K.; Schwaab, J.; Alvarez-Twose, I.; Brockow, K.; Bonadonna, P.; Hermine, O.; Niedoszytko, M.; Carter, M.C.; Hoermann, G.; et al. Personalized Management Strategies in Mast Cell Disorders: ECNM-AIM User’s Guide for Daily Clinical Practice. J. Allergy Clin. Immunol. Pract. 2022, 10, 1999–2012.e6. [Google Scholar] [CrossRef]
- Broesby-Olsen, S.; Farkas, D.K.; Vestergaard, H.; Hermann, A.P.; Moller, M.B.; Mortz, C.G.; Kristensen, T.K.; Bindslev-Jensen, C.; Sørensen, H.T.; Frederiksen, H. Risk of solid cancer, cardiovascular disease, anaphylaxis, osteoporosis and fractures in patients with systemic mastocytosis: A nationwide population-based study. Am. J. Hematol. 2016, 91, 1069–1075. [Google Scholar] [CrossRef] [PubMed]
- Kaszuba, A.; Slawinska, M.; Zolkiewicz, J.; Sobjanek, M.; Nowicki, R.J.; Lange, M. Mastocytosis and Skin Cancer: The Current State of Knowledge. Int. J. Mol. Sci. 2023, 24, 9840. [Google Scholar] [CrossRef]
- Hagglund, H.; Sander, B.; Gulen, T.; Lindelof, B.; Nilsson, G. Increased risk of malignant melanoma in patients with systemic mastocytosis? Acta Derm. Venereol. 2014, 94, 583–584. [Google Scholar] [CrossRef] [PubMed]
- Pyatilova, P.; Akin, C.; Alvarez-Twose, I.; Arock, M.; Bonadonna, P.; Brockow, K.; Butterfield, J.H.; Broesby-Olsen, S.; Carter, M.C.; Castells, M.; et al. Refined Treatment Response Criteria for Indolent Systemic Mastocytosis Proposed by the ECNM-AIM Consortium. J. Allergy Clin. Immunol. Pract. 2022, 10, 2015–2024. [Google Scholar] [CrossRef]
- Pulfer, S.; Ziehfreund, S.; Gebhard, J.; Hindelang, B.; Biedermann, T.; Brockow, K.; Zink, A. Health-Related Quality of Life and Influencing Factors in Adults with Nonadvanced Mastocytosis-A Cross-Sectional Study and Qualitative Approach. J. Allergy Clin. Immunol. Pract. 2021, 9, 3166–3175. [Google Scholar] [CrossRef]
- Barete, S.; Assous, N.; de Gennes, C.; Grandpeix, C.; Feger, F.; Palmerini, F.; Dubreuil, P.; Arock, M.; Roux, C.; Launay, J.M.; et al. Systemic mastocytosis and bone involvement in a cohort of 75 patients. Ann. Rheum. Dis. 2010, 69, 1838–1841. [Google Scholar] [CrossRef]
- Berezowska, S.; Flaig, M.J.; Rueff, F.; Walz, C.; Haferlach, T.; Krokowski, M.; Petat-Dutter, K.; Horny, H.-P.; Sotlar, K. Adult-onset mastocytosis in the skin is highly suggestive of systemic mastocytosis. Mod. Pathol. 2013, 27, 19–29. [Google Scholar] [CrossRef]
- Sperr, W.R.; Kundi, M.; Alvarez-Twose, I.; van Anrooij, B.; Oude Elberink, J.N.G.; Gorska, A.; Niedoszytko, M.; Gleixner, K.V.; Hadzijusufovic, E.; Zanotti, R.; et al. International prognostic scoring system for mastocytosis (IPSM): A retrospective cohort study. Lancet Haematol. 2019, 6, e638–e649. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subforms |
|---|
| Maculopapular cutaneous mastocytosis (synonym urticaria pigmentosa) (monomorphic and polymorphic variants) |
| Diffuse cutaneous mastocytosis |
| Cutaneous mastocytoma |
| Form of Mastocytosis | Abbreviation | Characteristics |
|---|---|---|
| Cutaneous mastocytosis - Maculopapular CM - Monomorphic - Polymorphic - Diffuse CM - Cutaneous mastocytoma - Isolated - Multilocalised | CM MPCM DCM - | Only the skin is involved. Disseminated lesions. Small uniform lesions, adult type. Larger variable lesions, childhood type. Diffuse indurated skin lesions. Solitary plaques or nodules. One lesion. Up to three lesions. |
| Systemic mastocytosis - Bone marrow mastocytosis - Indolent systemic mastocytosis - Smoldering systemic mastocytosis - Aggressive systemic mastocytosis - Systemic mastocytosis with an associated hematological neoplasm | SM BMM ISM SSM ASM SM-AHN | Extracutaneous organs are involved. SM is present only in the bone marrow. Benign form of SM. SM with high mast cell load. Aggressive form of SM. Additional hematological neoplasm. |
| - Mast cell leukemia | MCL | Circulating mast cells in blood. |
| - Well-differentiated systemic mastocytosis | WDSM | Morphologic variant that may occur in any SM type/subtype |
| Mast cell sarcoma | MCS | Malignant mast cells in tissue. |
| Criterion | Characteristics | Tissue |
|---|---|---|
| Major | Multifocal dense infiltrates of mast cells (≥15 mast cells in aggregates). | Bone marrow biopsies and/or in sections of other extracutaneous organ(s). |
| Minor criterion 1 | ≥25% of all mast cells are atypical or are spindle-shaped. | Atypical cells on bone marrow smears. Spindle-shaped mast cells in bone marrow or other extracutaneous organs. |
| Minor criterion 2 | KIT-activating point mutation(s) at codon 816 or in other critical regions of KIT. | Bone marrow, blood or another extracutaneous organ. |
| Minor criterion 3 | Mast cells express one or more of: CD2 and/or CD25 and/or CD30. | Bone marrow, blood, or another extracutaneous organ. |
| Minor criterion 4 | Baseline tryptase >20 ng/mL. In case of an unrelated myeloid neoplasm, an elevated tryptase does not count as an SM criterion. In case of a known hereditary alpha-tryptasemia (HαT), the tryptase level should be adjusted. | Serum |
| Differential Diagnosis | Similarity to CM | Different Aspects |
|---|---|---|
| Lentigines and pigmented nevi | Disseminated monomorphic small hyperpigmented lesions may mimic MPCM. | Hyperpigmentation without redness. Often solitary or regional. |
| Pityriasis lichenoides chronica | Multiple disseminated red small papules on trunk in children/young adults may mimic MPCM. | Very mild scaling, multiple often symmetrical lesions. |
| Lichen planus pigmentosus or exanthematicus | Multiple disseminated small hyperpigmented or erythematous macules and papules mimic MPCM. | Acute onset, severe itching. |
| Parapsoriasis en petites plaques | Disseminated red-brown pigmented small macules on lateral trunk. | Typically digital appearance, atrophic aspect, mild scaling. |
| Pityriasis versicolor | Hyperpigmented or erythematous macules on the trunk. | Scales after scratching, spores in microscopy, confluent lesions often on upper trunk. |
| Multiple café au lait spots (CALMs) | Flat disseminated brown multilocular hyperpigmented birth marks. | Ovoid or jagged borders. The presence of ≥6 lesions >5–15 mm are neurofibromatosis criteria. |
| Neurofibromatosis | Single or multiple firm, skin-colored nodules or tumors (neurofibromas) +/− CALMs. | Peau-d’orange aspect of mastocytomas is absent. |
| Atrophodermia idiopathica | Disseminated larger multilocular hyperpigmented lesions often on the trunk beginning in childhood or early adults. | Superficial form of morphea with epidermal atrophy. |
| Ashy dermatosis (erythema chronicum perstans) | Disseminated larger confluent gray-brown macules, different sizes at trunk, extremities. | Hyperpigmentation without redness, often larger macules. |
| Postinflammatory hyperpigmentation | Solitary hyperpigmented macule(s). | No itch, history of previous inflammation. |
| Fixed drug eruption | First red macule, possible central blister, later hyperpigmentation. Multiple lesions possible. | Often solitary, history of drug intake. |
| Histiocytosis X (Abt-Letter-Siwe) | In early childhood, in sweat areas (breast, back, inguinal) small, disseminated papules. | Scales, crusts, severely ill patient. |
| Plane warts (Verrucae planae) | Multiple pale red-brown small papules. | Localized lesions, mostly face, aggregated. |
| Chronic urticaria | Multiple itching red lesions. | Acute development of lesions, locations change over time, severe itching. |
| Juvenile xanthogranuloma | Multiple yellow-red papules and nodules in childhood. | No itch, no confluence. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brockow, K.; Bent, R.K.; Schneider, S.; Spies, S.; Kranen, K.; Hindelang, B.; Kurgyis, Z.; Broesby-Olsen, S.; Biedermann, T.; Grattan, C.E. Challenges in the Diagnosis of Cutaneous Mastocytosis. Diagnostics 2024, 14, 161. https://doi.org/10.3390/diagnostics14020161
Brockow K, Bent RK, Schneider S, Spies S, Kranen K, Hindelang B, Kurgyis Z, Broesby-Olsen S, Biedermann T, Grattan CE. Challenges in the Diagnosis of Cutaneous Mastocytosis. Diagnostics. 2024; 14(2):161. https://doi.org/10.3390/diagnostics14020161
Chicago/Turabian StyleBrockow, Knut, Rebekka Karolin Bent, Simon Schneider, Sophie Spies, Katja Kranen, Benedikt Hindelang, Zsuzsanna Kurgyis, Sigurd Broesby-Olsen, Tilo Biedermann, and Clive E. Grattan. 2024. "Challenges in the Diagnosis of Cutaneous Mastocytosis" Diagnostics 14, no. 2: 161. https://doi.org/10.3390/diagnostics14020161