

Immature Sacrococcygeal Teratoma: A Case Report and Extensive Review of the Literature
 ,
,  ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Case Report

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Exam | Age | Imagistic Findings |
|---|---|---|
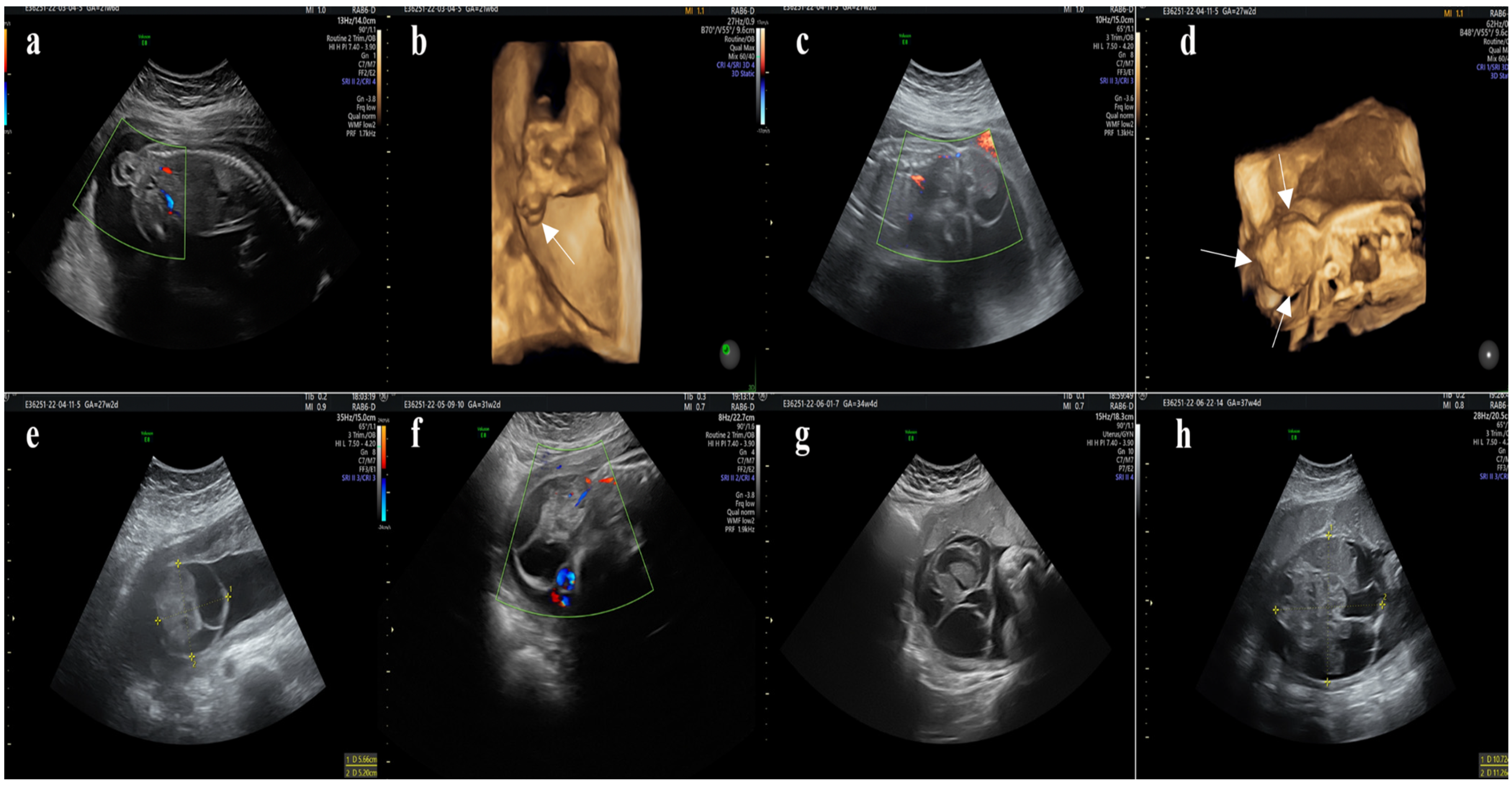
| Abdominal ultrasound | 21st week |
|
| Abdominal ultrasound | 29th week |
|
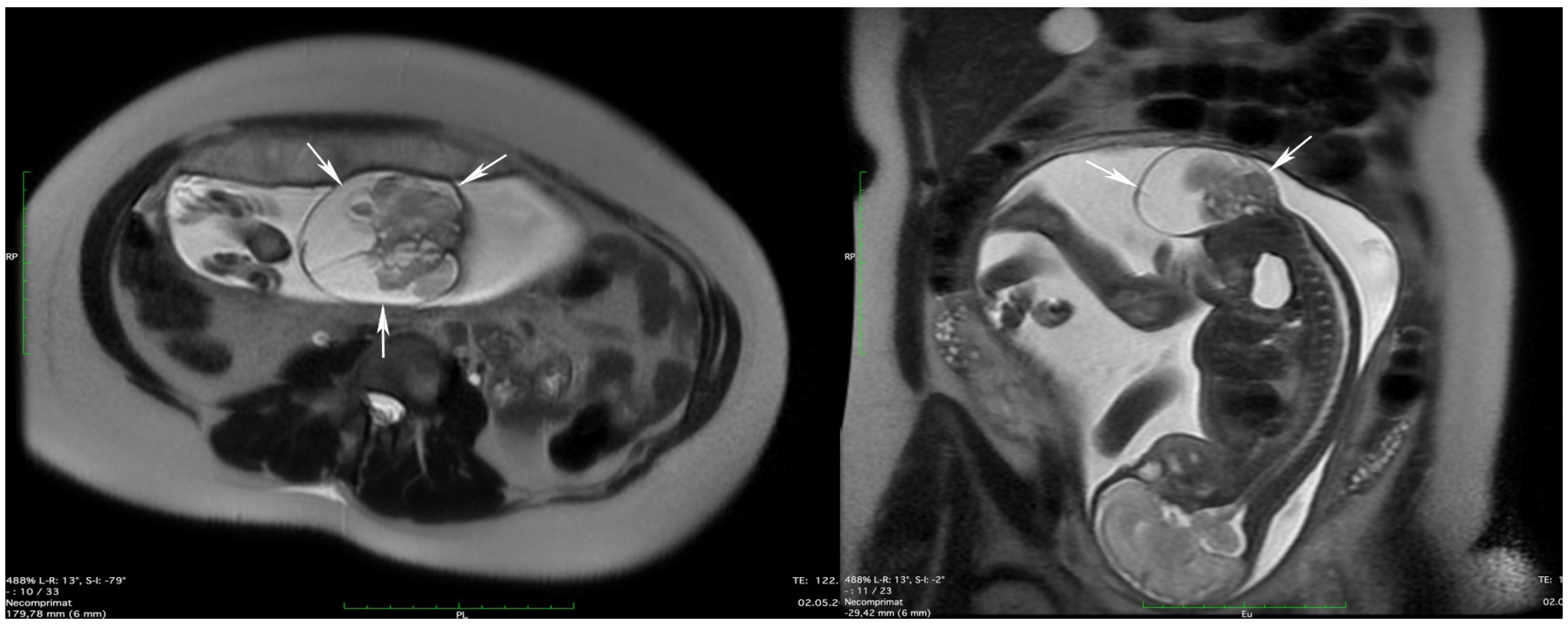
| Fetal MRI | 30th week |
|


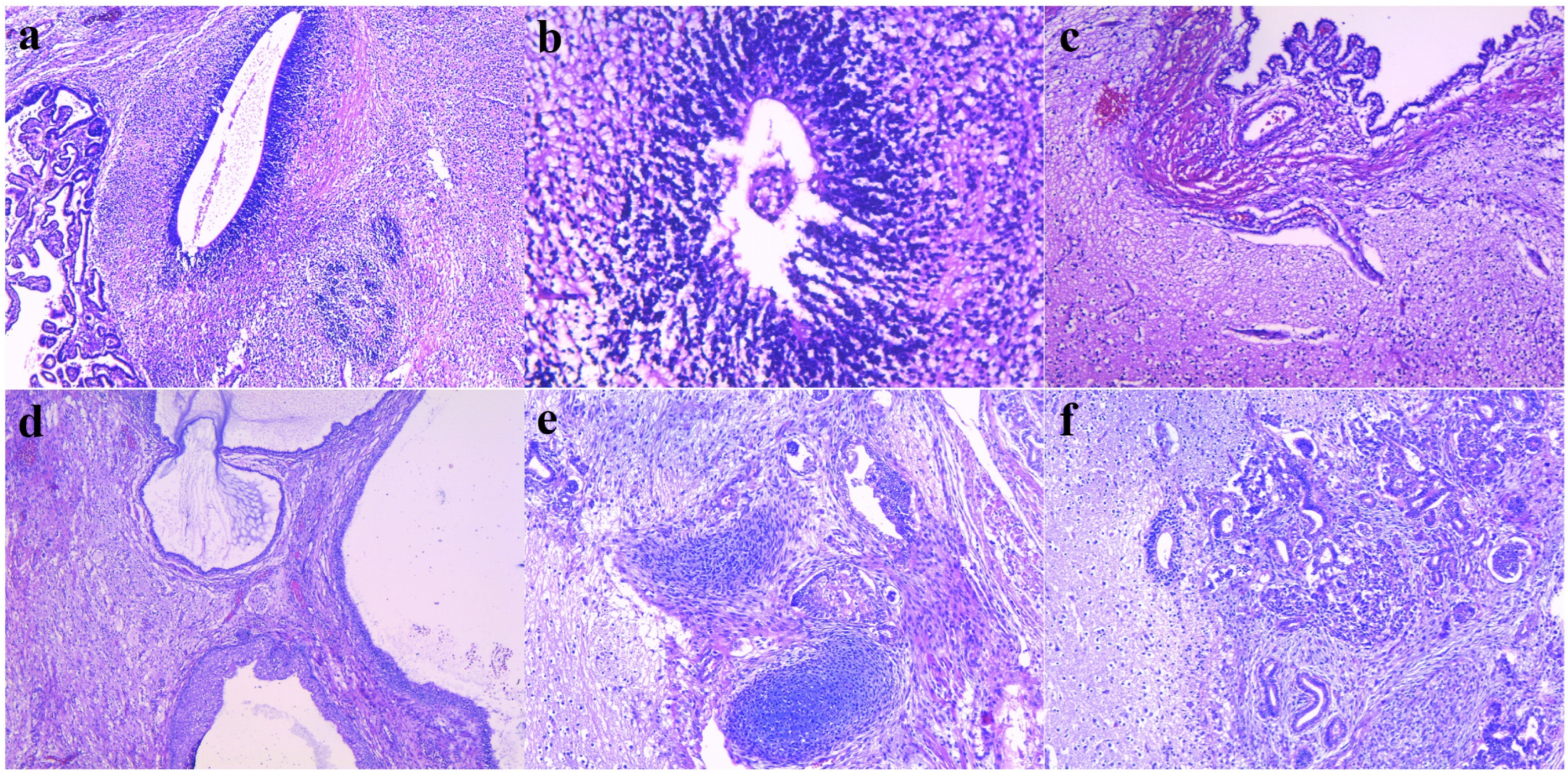
| Type of Exam | Histological Finding |
| Histopathological exam | Specimens:
|

3. Review of the Literature
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Simonini, C.; Strizek, B.; Berg, C.; Gembruch, U.; Mueller, A.; Heydweiller, A.; Geipel, A. Fetal Teratomas—A Retrospective Observational Single-Center Study. Prenat. Diagn. 2021, 41, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Santos-Ramos, R.; Duenhoelter, J.H. Diagnosis of Congenital Fetal Abnormalities by Sonography. Obstet. Gynecol. 1975, 45, 279–283. [Google Scholar] [PubMed]
- Swamy, R.; Embleton, N.; Hale, J. Sacrococcygeal Teratoma over Two Decades: Birth Prevalence, Prenatal Diagnosis and Clinical Outcomes. Prenat. Diagn. 2008, 28, 1048–1051. [Google Scholar] [CrossRef] [PubMed]
- Pauniaho, S.-L.; Heikinheimo, O.; Vettenranta, K.; Salonen, J.; Stefanovic, V.; Ritvanen, A.; Rintala, R.; Heikinheimo, M. High Prevalence of Sacrococcygeal Teratoma in Finland—A Nationwide Population-Based Study. Acta Paediatr. 2013, 102, e251–e256. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.-Q.; Yan, J.-Y.; Xu, R.-L.; Wang, X.-C.; Chen, X.; Huang, K.-H. A Clinical Analysis of the Diagnosis and Treatment of Fetal Sacrococcygeal Teratomas. Cancer Manag. Res. 2020, 12, 13185–13193. [Google Scholar] [CrossRef] [PubMed]
- Tuladhar, R.; Patole, S.K.; Whitehall, J.S. Sacrococcygeal Teratoma in the Perinatal Period. Postgrad. Med. J. 2000, 76, 754–759. [Google Scholar] [CrossRef]
- Ashley, D.J. Origin of Teratomas. Cancer 1973, 32, 390–394. [Google Scholar] [CrossRef]
- Moore, S.W.; Satgé, D.; Sasco, A.J.; Zimmermann, A.; Plaschkes, J. The Epidemiology of Neonatal Tumours. Report of an International Working Group. Pediatr. Surg. Int. 2003, 19, 509–519. [Google Scholar] [CrossRef]
- Peiró, J.L.; Sbragia, L.; Scorletti, F.; Lim, F.Y.; Shaaban, A. Management of Fetal Teratomas. Pediatr. Surg. Int. 2016, 32, 635–647. [Google Scholar] [CrossRef]
- Hambraeus, M.; Karlsson, J.; Kasselaki, I.; Hagerling, C.; Hagander, L.; Gisselsson, D. Differential Activation of Immune Effector Processes in Mature Compared to Immature Sacrococcygeal Teratomas. Fetal Pediatr. Pathol. 2022, 41, 413–425. [Google Scholar] [CrossRef]
- Uchiyama, M.; Iwafuchi, M.; Naitoh, M.; Yagi, M.; Iinuma, Y.; Kanada, S.; Takeda, M. Sacrococcygeal Teratoma: A Series of 19 Cases with Long-Term Follow-Up. Eur. J. Pediatr. Surg. 1999, 9, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Izant, R.J.; Filston, H.C. Sacrococcygeal Teratomas. Analysis of Forty-Three Cases. Am. J. Surg. 1975, 130, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Bedabrata, M.; Chhanda, D.; Moumita, S.; Kumar, S.A.; Madhumita, M.; Biswanath, M. An Epidemiological Review of Sacrococcygeal Teratoma over Five Years in a Tertiary Care Hospital. Indian J. Med. Paediatr. Oncol. 2018, 39, 4–7. [Google Scholar] [CrossRef]
- Isserman, R.S.; Nelson, O.; Tran, K.M.; Cai, L.; Polansky, M.; Rosenbloom, J.M.; Goebel, T.K.; Lin, E.E. Risk Factors for Perioperative Mortality and Transfusion in Sacrococcygeal Teratoma Resections. Paediatr. Anaesth. 2017, 27, 726–732. [Google Scholar] [CrossRef]
- Altman, R.P.; Randolph, J.G.; Lilly, J.R. Sacrococcygeal Teratoma: American Academy of Pediatrics Surgical Section Survey-1973. J. Pediatr. Surg. 1974, 9, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Mlčochová, G.; Kučerová, L.; Rousková, B.; Rygl, M.; Prosová, B.; Matěcha, J.; Černý, M.; Hercíková, L.; Sochůrek, J.; Fait, T. Sacrococcygeal Teratoma. Ceska Gynekol. 2019, 84, 140–144. [Google Scholar] [PubMed]
- Busch, C.; Oppitz, M.; Wehrmann, M.; Schweizer, P.; Drews, U. Immunohistochemical Localization of Nanog and Oct4 in Stem Cell Compartments of Human Sacrococcygeal Teratomas. Histopathology 2008, 52, 717–730. [Google Scholar] [CrossRef]
- De Backer, A.; Madern, G.C.; Hakvoort-Cammel, F.G.A.J.; Haentjens, P.; Oosterhuis, J.W.; Hazebroek, F.W.J. Study of the Factors Associated with Recurrence in Children with Sacrococcygeal Teratoma. J. Pediatr. Surg. 2006, 41, 173–181. [Google Scholar] [CrossRef]
- Rescorla, F.J.; Sawin, R.S.; Coran, A.G.; Dillon, P.W.; Azizkhan, R.G. Long-Term Outcome for Infants and Children with Sacrococcygeal Teratoma: A Report from the Childrens Cancer Group. J. Pediatr. Surg. 1998, 33, 171–176. [Google Scholar] [CrossRef]
- Dhaiban, M.; Cross, K.; Giuliani, S. Sacrococcygeal Teratoma: Long-Term Outcome in Paediatric Population. Arch. Dis. Child. 2021, 106 (Suppl. S3), A40–A41. [Google Scholar] [CrossRef]
- Yoneda, A.; Usui, N.; Taguchi, T.; Kitano, Y.; Sago, H.; Kanamori, Y.; Nakamura, T.; Nosaka, S.; Oba, M.S. Impact of the Histological Type on the Prognosis of Patients with Prenatally Diagnosed Sacrococcygeal Teratomas: The Results of a Nationwide Japanese Survey. Pediatr. Surg. Int. 2013, 29, 1119–1125. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Crussi, F.; Winkler, R.F.; Mirkin, D.L. Sacrococcygeal Teratomas in Infants and Children: Relationship of Histology and Prognosis in 40 Cases. Arch. Pathol. Lab. Med. 1978, 102, 420–425. [Google Scholar] [PubMed]
- van Heurn, L.J.; Coumans, A.B.C.; Derikx, J.P.M.; Bekker, M.N.; Bilardo, K.M.; Duin, L.K.; Knapen, M.F.C.M.; Pajkrt, E.; Sikkel, E.; van Heurn, L.W.E.; et al. Factors Associated with Poor Outcome in Fetuses Prenatally Diagnosed with Sacrococcygeal Teratoma. Prenat. Diagn. 2021, 41, 1430–1438. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, N.; Durrani, Z. Management of Sacrococcygeal Teratoma of the Fetus. J. Coll. Physicians Surg. Pak. 2004, 14, 506–507. [Google Scholar] [PubMed]
- Zvizdic, Z.; Jonuzi, A.; Milisic, E.; Hadzimehmedagic, A.; Vranic, S. A Long-Term Outcome of the Patients with Sacrococcygeal Teratoma: A Bosnian Cohort. Turk. Arch. Pediatr. 2023, 58, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Valdiserri, R.O.; Yunis, E.J. Sacrococcygeal Teratomas: A Review of 68 Cases. Cancer 1981, 48, 217–221. [Google Scholar] [CrossRef]
- Tapper, D.; Lack, E.E. Teratomas in Infancy and Childhood. A 54-Year Experience at the Children’s Hospital Medical Center. Ann. Surg. 1983, 198, 398–410. [Google Scholar] [CrossRef]
- Khanna, S.S. Sacrococcygeal Tumours in Children. J. Postgrad. Med. 1987, 33, 109. [Google Scholar]
- Sheth, S.; Nussbaum, A.R.; Sanders, R.C.; Hamper, U.M.; Davidson, A.J. Prenatal Diagnosis of Sacrococcygeal Teratoma: Sonographic-Pathologic Correlation. Radiology 1988, 169, 131–136. [Google Scholar] [CrossRef]
- Johnston, P.W. The Diagnostic Value of Alpha-Fetoprotein in an Infant with Sacrococcygeal Teratoma. J. Pediatr. Surg. 1988, 23, 862–863. [Google Scholar] [CrossRef]
- Havránek, P.; Hedlund, H.; Rubenson, A.; Güth, D.; Husberg, M.; Frykberg, T.; Larsson, L.T. Sacrococcygeal Teratoma in Sweden between 1978 and 1989: Long-Term Functional Results. J. Pediatr. Surg. 1992, 27, 916–918. [Google Scholar] [CrossRef] [PubMed]
- Kirkinen, P.; Partanen, K.; Merikanto, J.; Ryynänen, M.; Haring, P.; Heinonen, K. Ultrasonic and Magnetic Resonance Imaging of Fetal Sacrococcygeal Teratoma. Acta Obstet. Gynecol. Scand. 1997, 76, 917–922. [Google Scholar] [CrossRef] [PubMed]
- Graf, J.L.; Housely, H.T.; Albanese, C.T.; Adzick, N.S.; Harrison, M.R. A Surprising Histological Evolution of Preterm Sacrococcygeal Teratoma. J. Pediatr. Surg. 1998, 33, 177–179. [Google Scholar] [CrossRef] [PubMed]
- Marina, N.M.; Cushing, B.; Giller, R.; Cohen, L.; Lauer, S.J.; Ablin, A.; Weetman, R.; Cullen, J.; Rogers, P.; Vinocur, C.; et al. Complete Surgical Excision Is Effective Treatment for Children with Immature Teratomas with or without Malignant Elements: A Pediatric Oncology Group/Children’s Cancer Group Intergroup Study. J. Clin. Oncol. 1999, 17, 2137–2143. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, M.E.; Thompson, K.; Wojcik, E.M.; Martinez, R.; Husain, A.N. Congenital Sacrococcygeal Teratomas: Effect of Gestational Age on Size, Morphologic Pattern, Ploidy, P53, and Ret Expression. Pediatr. Dev. Pathol. 2000, 3, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Perrelli, L.; D’Urzo, C.; Manzoni, C.; Pintus, C.; De Santis, M.; Masini, L.; Noia, G. Sacrococcygeal Teratoma. Outcome and Management. An Analysis of 17 Cases. J. Perinat. Med. 2002, 30, 179–184. [Google Scholar] [CrossRef]
- Huddart, S.N.; Mann, J.R.; Robinson, K.; Raafat, F.; Imeson, J.; Gornall, P.; Sokal, M.; Gray, E.; McKeever, P.; Oakhill, A.; et al. Sacrococcygeal Teratomas: The UK Children’s Cancer Study Group’s Experience. I. Neonatal. Pediatr. Surg. Int. 2003, 19, 47–51. [Google Scholar] [CrossRef]
- Isaacs, H. Perinatal (Fetal and Neonatal) Germ Cell Tumors. J. Pediatr. Surg. 2004, 39, 1003–1013. [Google Scholar] [CrossRef]
- Heerema-McKenney, A.; Harrison, M.R.; Bratton, B.; Farrell, J.; Zaloudek, C. Congenital Teratoma: A Clinicopathologic Study of 22 Fetal and Neonatal Tumors. Am. J. Surg. Pathol. 2005, 29, 29–38. [Google Scholar] [CrossRef]
- Gabra, H.O.; Jesudason, E.C.; McDowell, H.P.; Pizer, B.L.; Losty, P.D. Sacrococcygeal Teratoma—A 25-Year Experience in a UK Regional Center. J. Pediatr. Surg. 2006, 41, 1513–1516. [Google Scholar] [CrossRef]
- Mann, J.R.; Gray, E.S.; Thornton, C.; Raafat, F.; Robinson, K.; Collins, G.S.; Gornall, P.; Huddart, S.N.; Hale, J.P.; Oakhill, A.; et al. Mature and Immature Extracranial Teratomas in Children: The UK Children’s Cancer Study Group Experience. J. Clin. Oncol. 2008, 26, 3590–3597. [Google Scholar] [CrossRef] [PubMed]
- Okada, T.; Sasaki, F.; Cho, K.; Honda, S.; Naito, S.; Hirokata, G.; Todo, S. Management and Outcome in Prenatally Diagnosed Sacrococcygeal Teratomas. Pediatr. Int. 2008, 50, 576–580. [Google Scholar] [CrossRef] [PubMed]
- Chirdan, L.B.; Uba, A.F.; Pam, S.D.; Edino, S.T.; Mandong, B.M.; Chirdan, O.O. Sacrococcygeal Teratoma: Clinical Characteristics and Long-Term Outcome in Nigerian Children. Ann. Afr. Med. 2009, 8, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Chou, M.-M.; Chen, Y.-F.; Chen, W.-C.; Chen, H.-C.; Ho, E.S.-C. Prenatal Ultrasonographic Characterization of a Giant Fetal Sacrococcygeal Immature Teratoma with Four-Dimensional Ultrasound. Taiwan J. Obstet. Gynecol. 2011, 50, 385–387. [Google Scholar] [CrossRef] [PubMed]
- Batukan, C.; Ozgun, M.T.; Basbug, M. First Trimester Diagnosis of Sacrococcygeal Teratoma Using Two- and Three-Dimensional Ultrasound. J. Clin. Ultrasound 2011, 39, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Marković, I.; Stamenović, S.; Radovanović, Z.; Bosnjaković, P.; Ilić, D.; Stojanov, D. Ultrasound and Magnetic Resonance Imaging in Prenatal Diagnosis of Sacrococcygeal Teratoma—Case Report. Med. Pregl. 2013, 66, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Grammatikopoulou, I.; Kontomanolis, E.N.; Chatzaki, E.; Chouridou, E.; Pavlidis, P.; Papadopoulos, E.M.; Lambropoulou, M. Immature Malignant Sacrococcygeal Teratoma: Case Report and Review of the Literature. Clin. Exp. Obstet. Gynecol. 2013, 40, 437–439. [Google Scholar]
- Goto, S.; Suzumori, N.; Obayashi, S.; Ozaki, Y.; Sugiura-Ogasawara, M. Two Cases of Prenatally Diagnosed Sacrococcygeal Teratoma Type I with Different Clinical Features. Congenit. Anom. (Kyoto) 2013, 53, 92–94. [Google Scholar] [CrossRef]
- Van Mieghem, T.; Al-Ibrahim, A.; Deprest, J.; Lewi, L.; Langer, J.C.; Baud, D.; O’Brien, K.; Beecroft, R.; Chaturvedi, R.; Jaeggi, E.; et al. Minimally Invasive Therapy for Fetal Sacrococcygeal Teratoma: Case Series and Systematic Review of the Literature. Ultrasound Obstet. Gynecol. 2014, 43, 611–619. [Google Scholar] [CrossRef]
- Sarbu, I.; Socolov, D.; Socolov, R.; Miron, I.; Trandafirescu, M.; Diaconescu, S.; Ciongradi, C.I. Hydrocephalus Secondary to Chemotherapy in a Case of Prenatally Diagnosed Giant Immature Grade 3 Sacrococcygeal Teratoma. Medicine 2016, 95, e5244. [Google Scholar] [CrossRef]
- Emerson, R.E.; Kao, C.-S.; Eble, J.N.; Grignon, D.J.; Wang, M.; Zhang, S.; Wang, X.; Fan, R.; Masterson, T.A.; Roth, L.M.; et al. Evidence of a Dual Histogenetic Pathway of Sacrococcygeal Teratomas. Histopathology 2017, 70, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Ulm, B.; Muin, D.; Scharrer, A.; Prayer, D.; Dovjak, G.; Kasprian, G. Prenatal Ultrasound and Magnetic Resonance Evaluation and Fetal Outcome in High-risk Fetal Tumors: A Retrospective Single-center Cohort Study over 20 Years. Acta Obstet. Gynecol. Scand. 2020, 99, 1534–1545. [Google Scholar] [CrossRef] [PubMed]
- Marcu, M.L.; Bacalbaşa, N.; Candrea, E.; Stănică, C.D.; Massawi, T.; Chirilov, A.; Neacşu, A.; Pacu, I. Fetal Sacrococcygeal Immature Teratoma—Report of Two Cases and Review of the Literature. Rom. J. Morphol. Embryol. 2022, 63, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Tongsong, T.; Wanapirak, C.; Piyamongkol, W.; Sudasana, J. Prenatal Sonographic Features of Sacrococcygeal Teratoma. Int. J. Gynaecol. Obstet. 1999, 67, 95–101. [Google Scholar] [CrossRef]
- Merrow, A.C.; Hariharan, S. (Eds.) Sacrococcygeal Teratoma. In Imaging in Pediatrics; Elsevier: Amsterdam, The Netherlands, 2018; p. 333. [Google Scholar] [CrossRef]
- Themes, U.F.O. Sacrococcygeal Teratoma. Radiology Key. Available online: https://radiologykey.com/sacrococcygeal-teratoma/ (accessed on 8 January 2024).
- Benachi, A.; Durin, L.; Vasseur Maurer, S.; Aubry, M.-C.; Parat, S.; Herlicoviez, M.; Nihoul-Fekete, C.; Dumez, Y.; Dommergues, M. Prenatally Diagnosed Sacrococcygeal Teratoma: A Prognostic Classification. J. Pediatr. Surg. 2006, 41, 1517–1521. [Google Scholar] [CrossRef]
- Baumgarten, H.D.; Gebb, J.S.; Khalek, N.; Moldenhauer, J.S.; Johnson, M.P.; Peranteau, W.H.; Hedrick, H.L.; Adzick, N.S.; Flake, A.W. Preemptive Delivery and Immediate Resection for Fetuses with High-Risk Sacrococcygeal Teratomas. Fetal Diagn. Ther. 2019, 45, 137–144. [Google Scholar] [CrossRef]
- Coleman, A.; Kline-Fath, B.; Keswani, S.; Lim, F.-Y. Prenatal Solid Tumor Volume Index: Novel Prenatal Predictor of Adverse Outcome in Sacrococcygeal Teratoma. J. Surg. Res. 2013, 184, 330–336. [Google Scholar] [CrossRef]
- Sy, E.D.; Filly, R.A.; Cheong, M.-L.; Clifton, M.S.; Cortes, R.A.; Ohashi, S.; Takifuji, K.; Ventura, D.E.; Grethel, E.J.; Wagner, A.J.; et al. Prognostic Role of Tumor-Head Volume Ratio in Fetal Sacrococcygeal Teratoma. Fetal Diagn. Ther. 2009, 26, 75–80. [Google Scholar] [CrossRef]
- Hedrick, H.L.; Flake, A.W.; Crombleholme, T.M.; Howell, L.J.; Johnson, M.P.; Wilson, R.D.; Adzick, N.S. Sacrococcygeal Teratoma: Prenatal Assessment, Fetal Intervention, and Outcome. J. Pediatr. Surg. 2004, 39, 430–438; discussion 430–438. [Google Scholar] [CrossRef]
- Litwińska, M.; Litwińska, E.; Janiak, K.; Piaseczna-Piotrowska, A.; Szaflik, K. Percutaneous Intratumor Laser Ablation for Fetal Sacrococcygeal Teratoma. Fetal Diagn. Ther. 2020, 47, 138–144. [Google Scholar] [CrossRef]
- Ding, Y.; Yang, M.; Lv, M.; Jiang, Y.; Dong, T.; Zhao, B.; Luo, Q. The Ex-Utero Intrapartum Treatment (EXIT) Strategy for Fetal Giant Sacrococcygeal Teratoma with Cardiac Insufficiency: A Case Report and Review of the Literature. Front. Oncol. 2022, 12, 1035058. [Google Scholar] [CrossRef]
- Finamore, P.S.; Kontopoulos, E.; Price, M.; Giannina, G.; Smulian, J.C. Mirror Syndrome Associated with Sacrococcygeal Teratoma: A Case Report. J. Reprod. Med. 2007, 52, 225–227. [Google Scholar]
- Ferraro, S.; Panzeri, A.; Braga, F.; Panteghini, M. Serum α-Fetoprotein in Pediatric Oncology: Not a Children’s Tale. Clin. Chem. Lab. Med. (CCLM) 2019, 57, 783–797. [Google Scholar] [CrossRef] [PubMed]
- van Heurn, L.J.; Knipscheer, M.M.; Derikx, J.P.M.; van Heurn, L.W.E. Diagnostic Accuracy of Serum Alpha-Fetoprotein Levels in Diagnosing Recurrent Sacrococcygeal Teratoma: A Systematic Review. J. Pediatr. Surg. 2020, 55, 1732–1739. [Google Scholar] [CrossRef] [PubMed]
- Schneider, D.T.; Wessalowski, R.; Calaminus, G.; Pape, H.; Bamberg, M.; Engert, J.; Waag, K.; Gadner, H.; Göbel, U. Treatment of Recurrent Malignant Sacrococcygeal Germ Cell Tumors: Analysis of 22 Patients Registered in the German Protocols MAKEI 83/86, 89, and 96. J. Clin. Oncol. 2001, 19, 1951–1960. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.X.; Chen, L.; Zhang, Y.H.; Wen, H. Prenatal diagnosis and prognostic factors analysis of fetal sacrococcygeal teratoma. Zhonghua Fu Chan Ke Za Zhi 2022, 57, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Nasreen, S.; Rahman, M.Z.; Mosarrat, S.S.; Sharmin, T.; Rahman, M. Malignant Sacrococcygeal Teratoma with Yolk Sac Differentiation in a Child—A Case Presentation. Open J. Pathol. 2018, 8, 60–67. [Google Scholar] [CrossRef]
- Ein, S.H.; Mancer, K.; Adeyemi, S.D. Malignant Sacrococcygeal Teratoma—Endodermal Sinus, Yolk Sac Tumor—In Infants and Children: A 32-Year Review. J. Pediatr. Surg. 1985, 20, 473–477. [Google Scholar] [CrossRef]
- Padilla, B.E.; Vu, L.; Lee, H.; MacKenzie, T.; Bratton, B.; O’Day, M.; Derderian, S. Sacrococcygeal Teratoma: Late Recurrence Warrants Long-Term Surveillance. Pediatr. Surg. Int. 2017, 33, 1189–1194. [Google Scholar] [CrossRef]
- Göbel, U.; Schneider, D.T.; Calaminus, G.; Jürgens, H.; Spaar, H.J.; Sternschulte, W.; Waag, K.; Harms, D. Multimodal Treatment of Malignant Sacrococcygeal Germ Cell Tumors: A Prospective Analysis of 66 Patients of the German Cooperative Protocols MAKEI 83/86 and 89. J. Clin. Oncol. 2001, 19, 1943–1950. [Google Scholar] [CrossRef]
- 614_Extracranial_GCT_Guidance_updated_June_2018.Pdf. Available online: https://www.cclg.org.uk/write/MediaUploads/Member%20area/Treatment%20guidelines/614_Extracranial_GCT_Guidance_updated_June_2018.pdf (accessed on 10 January 2024).
- Derikx, J.P.M.; De Backer, A.; van de Schoot, L.; Aronson, D.C.; de Langen, Z.J.; van den Hoonaard, T.L.; Bax, N.M.A.; van der Staak, F.; van Heurn, L.W.E. Long-Term Functional Sequelae of Sacrococcygeal Teratoma: A National Study in The Netherlands. J. Pediatr. Surg. 2007, 42, 1122–1126. [Google Scholar] [CrossRef] [PubMed]
- Elgendy, A.; AbouZeid, A.A.; El-Debeiky, M.; Mostafa, M.; Takrouney, M.H.; Abouheba, M.; Khairi, A.; Shehata, S.; Shehata, S.M. Management Strategy and Outcomes of Sacrococcygeal Teratoma—An Egyptian Multicenter Experience. World J. Surg. Oncol. 2023, 21, 294. [Google Scholar] [CrossRef] [PubMed]
- Partridge, E.A.; Canning, D.; Long, C.; Peranteau, W.H.; Hedrick, H.L.; Adzick, N.S.; Flake, A.W. Urologic and Anorectal Complications of Sacrococcygeal Teratomas: Prenatal and Postnatal Predictors. J. Pediatr. Surg. 2014, 49, 139–142; discussion 142–143. [Google Scholar] [CrossRef] [PubMed]
- Hambraeus, M.; Hagander, L.; Stenström, P.; Arnbjörnsson, E.; Börjesson, A. Long-Term Outcome of Sacrococcygeal Teratoma: A Controlled Cohort Study of Urinary Tract and Bowel Dysfunction and Predictors of Poor Outcome. J. Pediatr. 2018, 198, 131–136.e2. [Google Scholar] [CrossRef] [PubMed]
- Yadav, D.K.; Acharya, S.K.; Bagga, D.; Jain, V.; Dhua, A.; Goel, P. Sacrococcygeal Teratoma: Clinical Characteristics, Management, and Long-Term Outcomes in a Prospective Study from a Tertiary Care Center. J. Indian Assoc. Pediatr. Surg. 2020, 25, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Hambraeus, M.; Arnbjörnsson, E.; Börjesson, A.; Salvesen, K.; Hagander, L. Sacrococcygeal Teratoma: A Population-Based Study of Incidence and Prenatal Prognostic Factors. J. Pediatr. Surg. 2016, 51, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.D.; Hedrick, H.; Flake, A.W.; Johnson, M.P.; Bebbington, M.W.; Mann, S.; Rychik, J.; Liechty, K.; Adzick, N.S. Sacrococcygeal Teratomas: Prenatal Surveillance, Growth and Pregnancy Outcome. Fetal Diagn. Ther. 2009, 25, 15–20. [Google Scholar] [CrossRef]
- Rodriguez, M.A.; Cass, D.L.; Lazar, D.A.; Cassady, C.I.; Moise, K.J.; Johnson, A.; Mushin, O.P.; Hassan, S.F.; Belleza-Bascon, B.; Olutoye, O.O. Tumor Volume to Fetal Weight Ratio as an Early Prognostic Classification for Fetal Sacrococcygeal Teratoma. J. Pediatr. Surg. 2011, 46, 1182–1185. [Google Scholar] [CrossRef]
- Gebb, J.S.; Khalek, N.; Qamar, H.; Johnson, M.P.; Oliver, E.R.; Coleman, B.G.; Peranteau, W.H.; Hedrick, H.L.; Flake, A.W.; Adzick, N.S.; et al. High Tumor Volume to Fetal Weight Ratio Is Associated with Worse Fetal Outcomes and Increased Maternal Risk in Fetuses with Sacrococcygeal Teratoma. Fetal Diagn. Ther. 2019, 45, 94–101. [Google Scholar] [CrossRef]
- Shue, E.; Bolouri, M.; Jelin, E.B.; Vu, L.; Bratton, B.; Cedars, E.; Yoke, L.; Byrne, F.; Hirose, S.; Feldstein, V.; et al. Tumor Metrics and Morphology Predict Poor Prognosis in Prenatally Diagnosed Sacrococcygeal Teratoma: A 25-Year Experience at a Single Institution. J. Pediatr. Surg. 2013, 48, 1225–1231. [Google Scholar] [CrossRef]
- Drut, R. Immunohistochemical Localization of Nanog and Oct4 in Stem Cell Compartments of Human Sacrococcygeal Teratomas. Histopathology 2009, 54, 763. [Google Scholar] [CrossRef] [PubMed]
- Busch, C.; Bareiss, P.M.; Sinnberg, T.; Just, L.; Wehrmann, M.; Fuchs, J.; Garbe, C.; Drews, U. Isolation of Three Stem Cell Lines from Human Sacrococcygeal Teratomas. J. Pathol. 2009, 217, 589–596. [Google Scholar] [CrossRef] [PubMed]



| Grade | Percentage of Immature Tissue |
|---|---|
| 0 | 0% |
| I | <10% |
| II | 10–50% |
| III | >50% |
| Type of Exam | Age | Imagistic Findings | |
|---|---|---|---|
| Preoperative | Abdominal ultrasound | 1st day |
|
| Transfontanelar ultrasound + chest radiography | 1st day |
| |
| Radiography of lumbosacral spine | 1st day |
| |
| CT of the abdomen and pelvis | 2nd day |
| |
| Postoperative | Magnetic resonance imaging (MRI) | 7 months |
|
| Author | Year | Age at Presentation (wks) | Cases | Grade, Type of ISCT | Diagnostic Mode | Alpha-Fetoprotein (ng/mL) | Maximum Diameter of the ISCT (cm) | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Gonzalez- Crussi [22] | 1978 | 24.7 (18–38) 26.6 (20–38) | 2 5 3 | G1 G2 G3 | US | N/A | 11.9 (7.5–17) 12.4 (3.8–19.5) | Recurrences—10/18 (55%) |
| Valdiserri [26] | 1981 | N/A | 2 6 | G2 G3 | US | N/A | 11.3 (2–26) | NND G3—2; death 3 years after surgery G3—1; no recurrences—4 |
| Tapper [27] | 1983 | N/A | 5 8 6 | G1 G2 G3 | US | N/A | 11.6 | Recurrences of G1—1; G2—1; G3—2; favorable—12; post-op death—3 |
| Khanna [28] | 1987 | 37 | 5 | Not graded | US | N/A | 13 | N/A |
| Sheth [29] | 1988 | 29 (20–35) | 7 | N/A | US | N/A | N/A | Recurrence at 11 m—1/7 (14.2%), elective abortion—1, IUD—2, NND—1 |
| Johnston [30] | 1988 | 35 | 1 | N/A | US | 191.5 | 20 | Favorable |
| Havranek [31] | 1992 | Birth | 1 1 | TI TII | US | N/A | 15 | Recurrences—2/4 (50%), Urine leakage—1 |
| Kirkinen [32] | 1997 | N/A | 4 | Not graded | US, MRI | N/A | 12.1 | NND—1, favorable—2, recurrence—1/4 (25%) |
| Rescorla [19] | 1998 | Birth | 24 | Not graded | US | N/A | N/A | Recurrence—1/24 (4%) |
| Graf [33] | 1998 | 26.6 (26–32) | 5 | G3 | US | N/A | N/A | NND—2, favorable—3 |
| Uchiyama [11] | 1999 | 30 | 5 (2 *) | Not graded | US | N/A | 14 | N/A |
| Marina [34] | 1999 | N/A | 2 3 | G2 G3 | US | N/A | N/A | Local recurrence—1, locoregional—1, favorable—3 |
| Herrmann [35] | 2000 | 25 (21–31) | 4 | Not graded | US | N/A | 13 (8.8–15) | IUD—2, NND—1, no recurrence—1 |
| Perelli [36] | 2002 | N/A | 3 | N/A | US | N/A | N/A | Recurrence—1/3 (33%) |
| Huddart [37] | 2003 | N/A | 16 | N/A | US | N/A | N/A | Recurrence—2/16 (12.5%) |
| Iqbal [24] | 2004 | 36 | 1 | N/A | US | N/A | N/A | Favorable |
| Isaacs [38] | 2004 | N/A | N/A | N/A | US | N/A | N/A | N/A |
| Heerema-McKenney [39] | 2005 | 26.6 (20–38) | 3 | G1 | US | N/A | 12.4 (3.8–19.5) | IUD—1; favorable—2 |
| 24.7 (18–38) | 11 | G3 | US | N/A | 11.9 (7.5–17) | NND—1, death 3 weeks after excision—1, re-excision after 3 weeks and 14 weeks—2, intraoperative death—1, IUD—1, favorable—4 | ||
| De Backer [18] | 2006 | N/A | 5 1 1 1 1 1 1 | TII TIII TII, G1 TI, G1, TIV, G1 TII, G2 | US | N/A | N/A | Recurrence—2/11(18%) local Local + liver—NND Tumor spill—NND Favorable—9 |
| Gabra [40] | 2006 | N/A | 1 | TIII | US | N/A | N/A | Neuropathic bladder, constipation, and soiling |
| Mann [41] | 2008 | 32 | N/A | N/A | US | N/A | N/A | NND—2, Recurrence—6/32 (18.7%), OS—93.8%, |
| Swamy [3] | 2008 | 28 | N/A | N/A | US | N/A | N/A | N/A |
| Okada [42] | 2008 | 29 | 1 | TIII | US | 69,822 | N/A | NND |
| Chirdan [43] | 2009 | 9 | N/A | N/A | US | N/A | N/A | N/A |
| Chou [44] | 2011 | 28 | 1 | G3 | US | 356.5 | 16 | NND |
| Batukan [45] | 2011 | 14 | 1 | TII | US | - | 3.3 | TOP at 14 weeks |
| Yoneda [21] | 2013 | 32.4 (22.7–38.8) | 33 | N/A | US | 281.3 | 14 | TOP—1, IUD—1, NND—8, favorable—23 |
| Marković [46] | 2013 | 20 | 1 | TI | US, MRI | N/A | 6.2 | NND |
| Grammatikopoulou [47] | 2013 | 23 | 1 | N/A | US, MRI | N/A | 10 | N/A |
| Goto [48] | 2013 | 27 | 1 | TI | US, MRI | 161,303 | 16 | Death first day after surgery |
| Mieghem [49] | 2014 | 26.3 | 1 1 | TII, G3 TI | US | N/A | 14 | NND Mild developmental delay and mild constipation |
| Sarbu [50] | 2016 | 39 | 1 | TI, G3 | US, MRI | N/A | 22 | Surgical wound dehiscence and sepsis, progressive active hydrocephaly secondary to chemotherapy |
| Emerson [51] | 2016 | N/A | 4 2 5 | G1 G2 G3 | US | N/A | N/A | N/A |
| Bedabrata [13] | 2018 | N/A | 1 3 | G1 G2 | US | N/A | N/A | N/A |
| Hambraeus [10] | 2020 | 30.8 (28.4–34) | 1 4 1 | G1 G2 G3 | US | N/A | 13.8 (6.5–20) | Favorable—6 |
| Ulm [52] | 2020 | 23.3 (19–35) | 1 3 2 | TI TII TIII | US, MRI | N/A | 305.2 cm3 (mean volume of the tumor) | TOP—1, NND—1, favorable—2, unfavorable—1, chemotherapy—1 |
| Zheng [5] | 2020 | 24.4 (22–29) | 2 5 | G2 G3 | US, MRI | N/A | 13.4 (9–20) | Favorable—7 |
| Marcu [53] | 2022 | 20 (18–22) | 1 1 | TI, G3 TII, G3 | US | N/A | 5.9 (3.3–8.5) | NND—2 |
| Zvizdic [25] | 2023 | 36.6 (34–38) | 1 2 | TI TII | US | 120,516.3 | 12 (5–16) | Favorable—1, recurrences—2 |
| Our case | 2023 | 38 | 1 | TI, G3 | US, MRI | 816 | 16 | Favorable |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varlas, V.N.; Cloțea, E.M.; Varlas, R.G.; Pop, A.; Peneș, O.; Crețoiu, D.; Dima, V.; Bălănescu, L. Immature Sacrococcygeal Teratoma: A Case Report and Extensive Review of the Literature. Diagnostics 2024, 14, 246. https://doi.org/10.3390/diagnostics14030246
Varlas VN, Cloțea EM, Varlas RG, Pop A, Peneș O, Crețoiu D, Dima V, Bălănescu L. Immature Sacrococcygeal Teratoma: A Case Report and Extensive Review of the Literature. Diagnostics. 2024; 14(3):246. https://doi.org/10.3390/diagnostics14030246
Chicago/Turabian StyleVarlas, Valentin Nicolae, Eliza Maria Cloțea, Roxana Georgiana Varlas, Anca Pop, Ovidiu Peneș, Dragoș Crețoiu, Vlad Dima, and Laura Bălănescu. 2024. "Immature Sacrococcygeal Teratoma: A Case Report and Extensive Review of the Literature" Diagnostics 14, no. 3: 246. https://doi.org/10.3390/diagnostics14030246