
“Bezoar Egg”—A Rare Cause of Small Bowel Obstruction

 , , , , ,
, , , , ,
Abstract
:Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, P.Y.; Wang, X.; Zhang, L.; Li, H.F.; Chen, L.; Wang, X.; Wang, B. Bezoar-induced small bowel obstruction: Clinical characteristics and diagnostic value of multi-slice spiral computed tomography. World J. Gastroenterol. 2015, 21, 9774–9784. [Google Scholar] [CrossRef] [PubMed]
- Abou Azar, S.; Wehbe, M.R.; Jamali, S.; Hallal, A. Small Bowel Obstruction Secondary to a Metamucil Bezoar: Case Report and Review of the Literature. Case Rep. Surg. 2017, 2017, 2702896. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Yang, X.; Zheng, Y.; Wu, Y. Clinical characteristics and indications for surgery for bezoar-induced small bowel obstruction. J. Int. Med. Res. 2021, 49, 300060520979377. [Google Scholar] [CrossRef] [PubMed]
- Shah, D.; Desai, A.B. Isolated ileal bezoar causing small bowel obstruction. BMJ Case Rep. 2012, 2012, bcr0120125656. [Google Scholar] [CrossRef] [PubMed]
- Aydin, I.; Sengul, I.; Sengul, D. Phytobezoar: An Unusual Condition Leading to Small Bowel Obstruction. Cureus 2022, 14, e23885. [Google Scholar] [CrossRef] [PubMed]
- Kang, W.R.; Park, S.Y.; You, H.S.; Kim, D.H.; Park, C.H.; Choi, S.K.; Kim, H.S. A Single-center 12-year Experience of Patients with Gastrointestinal Bezoars. Korean J. Gastroenterol. 2023, 81, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Campos, P.; Almeida, J.; Ferreira da Silva, M.J. Adrenal Crisis Secondary to Small Bowel Obstruction Caused by a Bezoar. Cureus 2022, 14, e21498. [Google Scholar] [CrossRef] [PubMed]
- Uzunoglu, M.Y.; Altintoprak, F.; Dikicier, E.; Zengin, I. Treatment results of small bowel perforations due to unusual causes. Pak. J. Med. Sci. 2018, 34, 974–979. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.W.W.; Prabhakaran, S.; Bell, S.; Chin, M.; Carne, P.; Warrier, S.K.; Skinner, S.; Kong, J.C. Non-operative management for small bowel obstruction in a virgin abdomen: A systematic review. ANZ J. Surg. 2021, 91, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Hua, Y.; Meng, H.; Dong, L.; Zhang, L.; Jiang, X.; Chen, L. The value of MSCT in evaluating the passability of bezoar by conservative treatment for bezoars-induced small bowel obstruction. Abdom. Radiol. 2023, 48, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Delabrousse, E.; Lubrano, J.; Sailley, N.; Aubry, S.; Mantion, G.A.; Kastler, B.A. Small-bowel bezoar versus small-bowel feces: CT evaluation. AJR Am. J. Roentgenol. 2008, 191, 1465–1468. [Google Scholar] [CrossRef] [PubMed]
- Soon, Y.Q.A.; Low, H.M.; Huey, C.W.T.; Wansaicheong, G.K. Clinics in diagnostic imaging (198). Small bowel obstruction secondary to a bezoar. Singap. Med. J. 2019, 60, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Qu, L.; Li, J.; Wang, B. MR Imaging Features of Intestinal Phytobezoar. J. Gastrointest. Surg. 2017, 21, 1954–1956. [Google Scholar] [CrossRef] [PubMed]
- Kement, M.; Ozlem, N.; Colak, E.; Kesmer, S.; Gezen, C.; Vural, S. Synergistic effect of multiple predisposing risk factors on the development of bezoars. World J. Gastroenterol. 2012, 18, 960–964. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intraluminal Causes of SBO | Ultrasound | CT | MR |
|---|---|---|---|
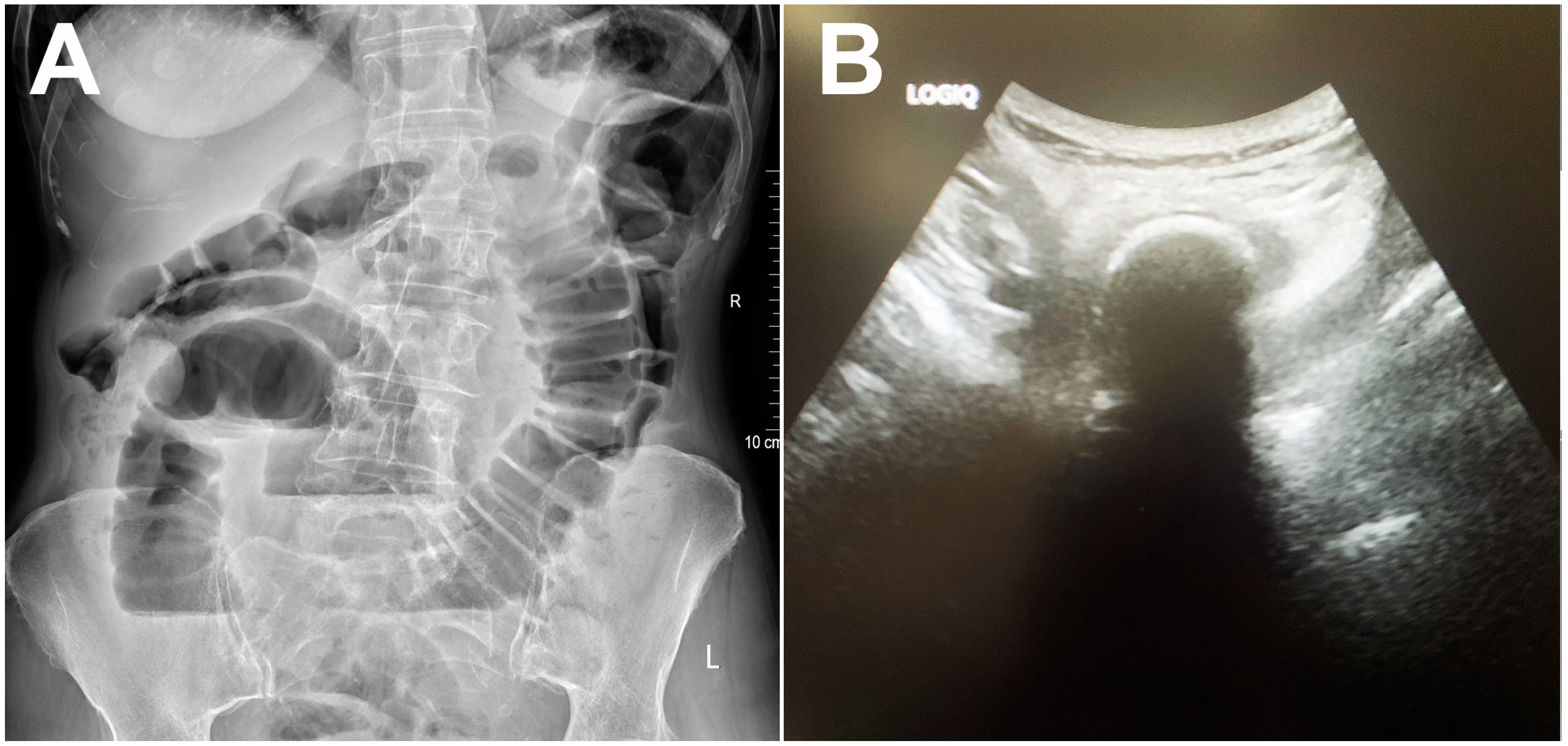
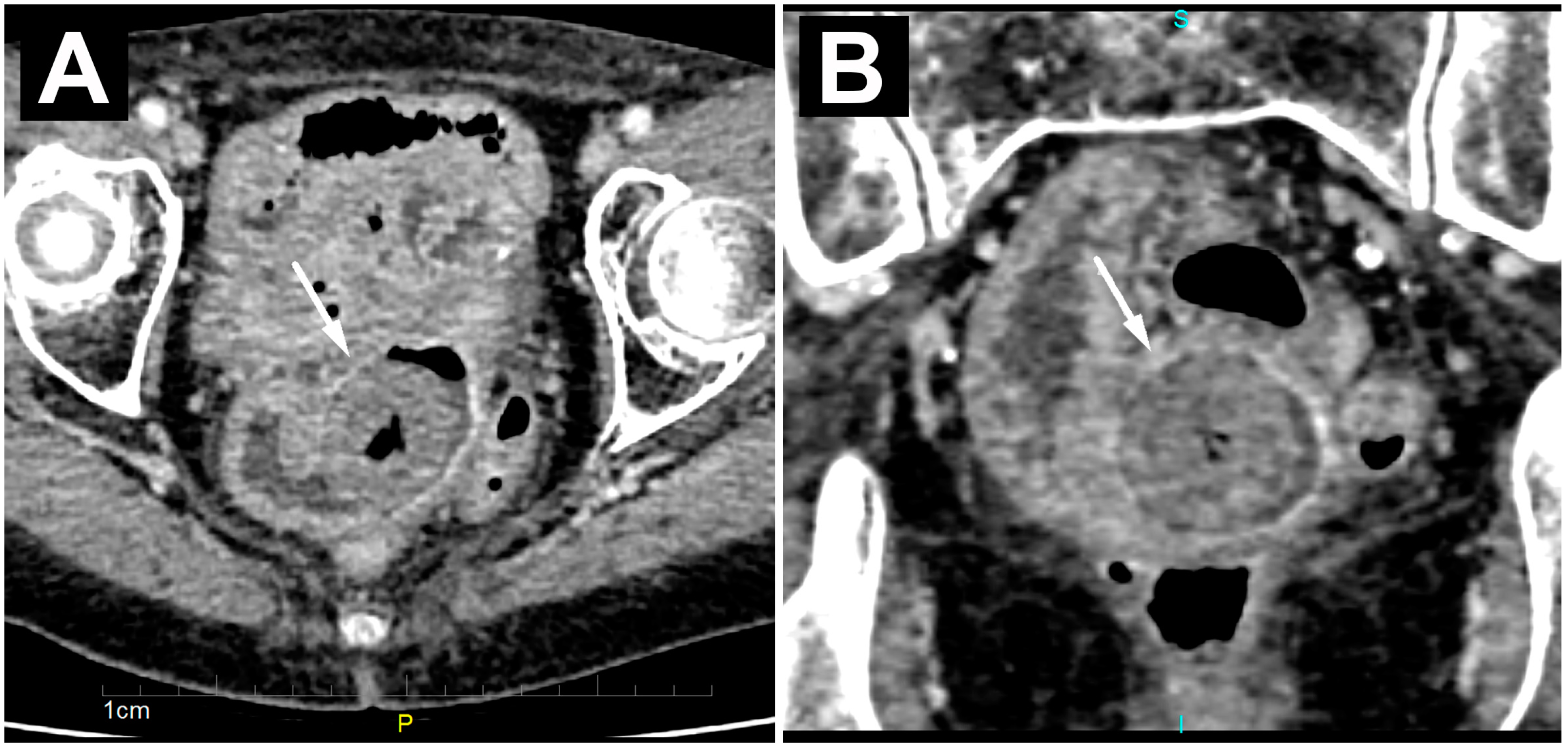
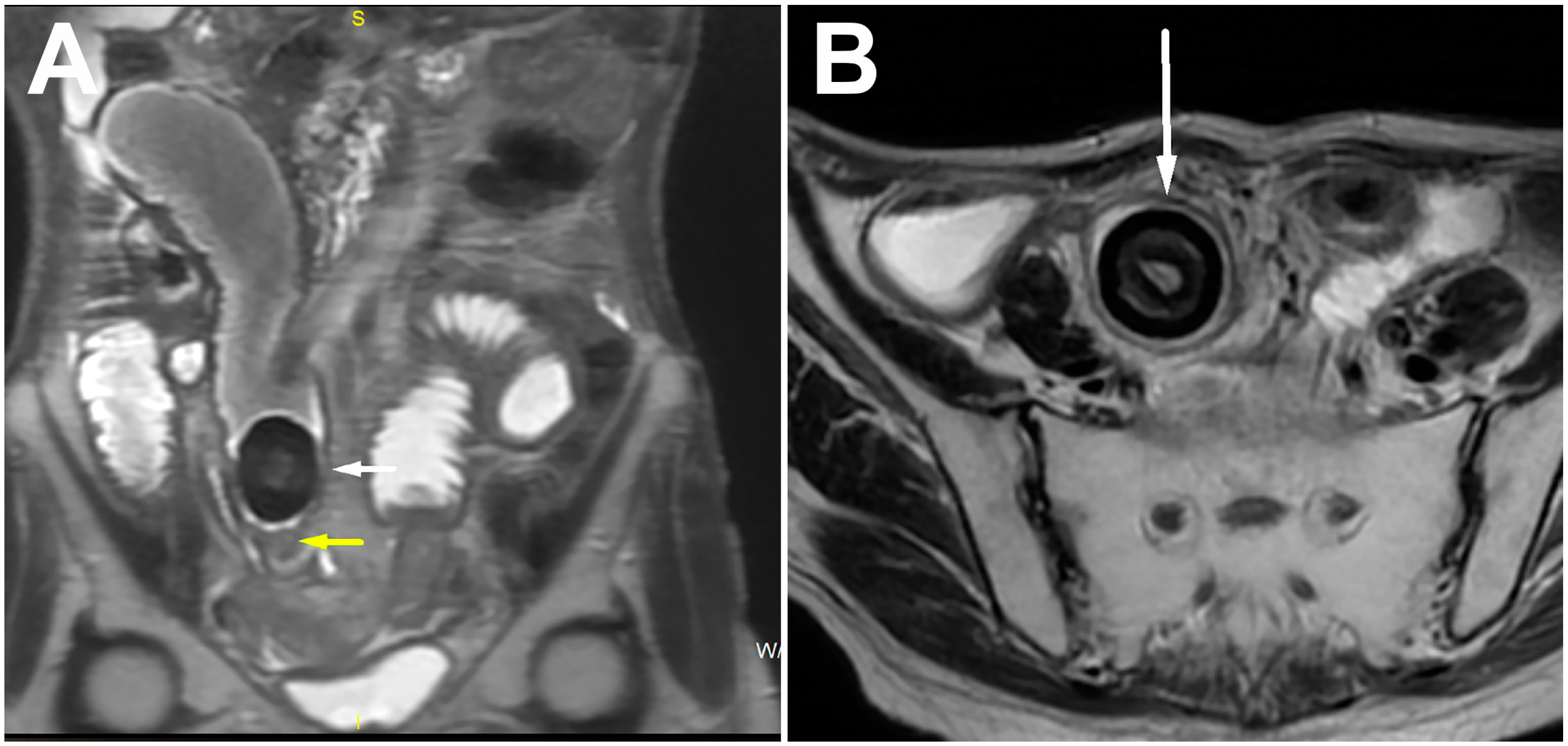
| Calcified bezoar (“Bezoar egg”) | Hyperechoic oval structure with posterior acoustic shadow within the bowel lumen | Oval, clearly demarcated mass with centrally placed gas | T1w and T2w hipointense oval mass with layered structure |
| Non-calcified bezoar (trichobezoar, phytobezoar, lactobezoar) | Arc-like surfaced intraluminal mass with posterior acoustic shadow | Oval or tubular masses with clear boundaries located inside the intestinal lumen, with mottled gas density | Oval mass with low T2w signal and a low to intermediate T1w signal intensity |
| Gallstone ileus | Hyperechoic oval structure with posterior acoustic shadow | Oval calcified or isodense intraluminal mass, presence of pneumobilia and cholecysto-enteric fistula | Oval mass with a homogenously low signal intensity on T1w and T2w |
| Primary small bowel neoplasm (calcified polyp, calcified leiomyoma) | Oval soft tissue mass with posterior acoustic shadow | Intraluminal, completely or partially calcified mass that arises from the bowel wall | Low T1w signal intensity; heterogeneous to high T2w signal intensity with central area of enhancement representing a central vascular stalk and focal areas of signal void representing calcifications |
| Ingested foreign body | Variable shape and structure (depending on the type of ingested foreign body) with posterior acoustic shadow | High density, intraluminal variable shape and structure | Uniformly low signal intensity on T1w and T2w sequences |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milosevic, S.; Kovac, J.D.; Lazic, L.; Mitrovic, M.; Stosic, K.; Basaric, D.; Tadic, B.; Stojkovic, S.; Rasic, S.; Ivanovic, N.; et al. “Bezoar Egg”—A Rare Cause of Small Bowel Obstruction. Diagnostics 2024, 14, 360. https://doi.org/10.3390/diagnostics14040360
Milosevic S, Kovac JD, Lazic L, Mitrovic M, Stosic K, Basaric D, Tadic B, Stojkovic S, Rasic S, Ivanovic N, et al. “Bezoar Egg”—A Rare Cause of Small Bowel Obstruction. Diagnostics. 2024; 14(4):360. https://doi.org/10.3390/diagnostics14040360
Chicago/Turabian StyleMilosevic, Stefan, Jelena Djokic Kovac, Ljubica Lazic, Milica Mitrovic, Katarina Stosic, Dragan Basaric, Boris Tadic, Stefan Stojkovic, Slobodan Rasic, Nenad Ivanovic, and et al. 2024. "“Bezoar Egg”—A Rare Cause of Small Bowel Obstruction" Diagnostics 14, no. 4: 360. https://doi.org/10.3390/diagnostics14040360