
Performance of Immunodiagnostic Tests for Typhoid Fever: A Systematic Review and Meta-Analysis

 ,
,  ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Characteristics of Studies
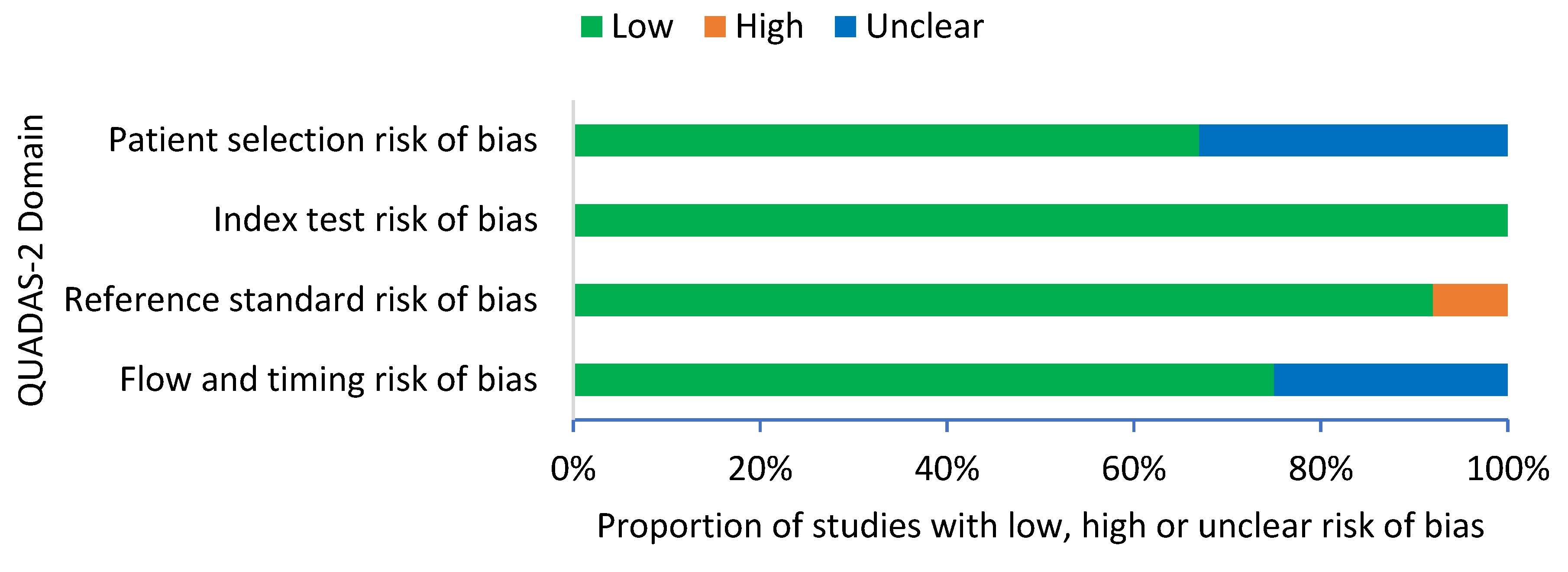
2.2. Methodological Risk of Bias
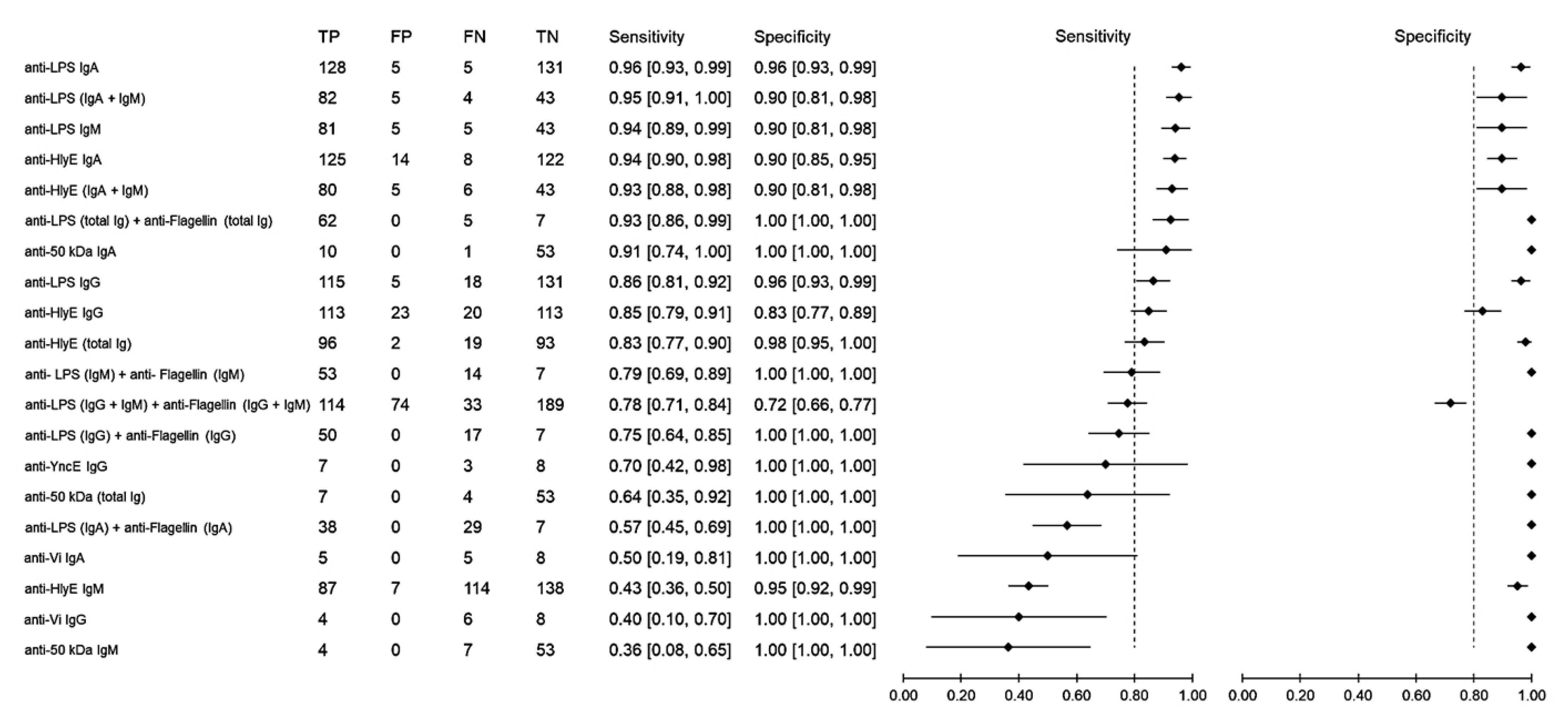
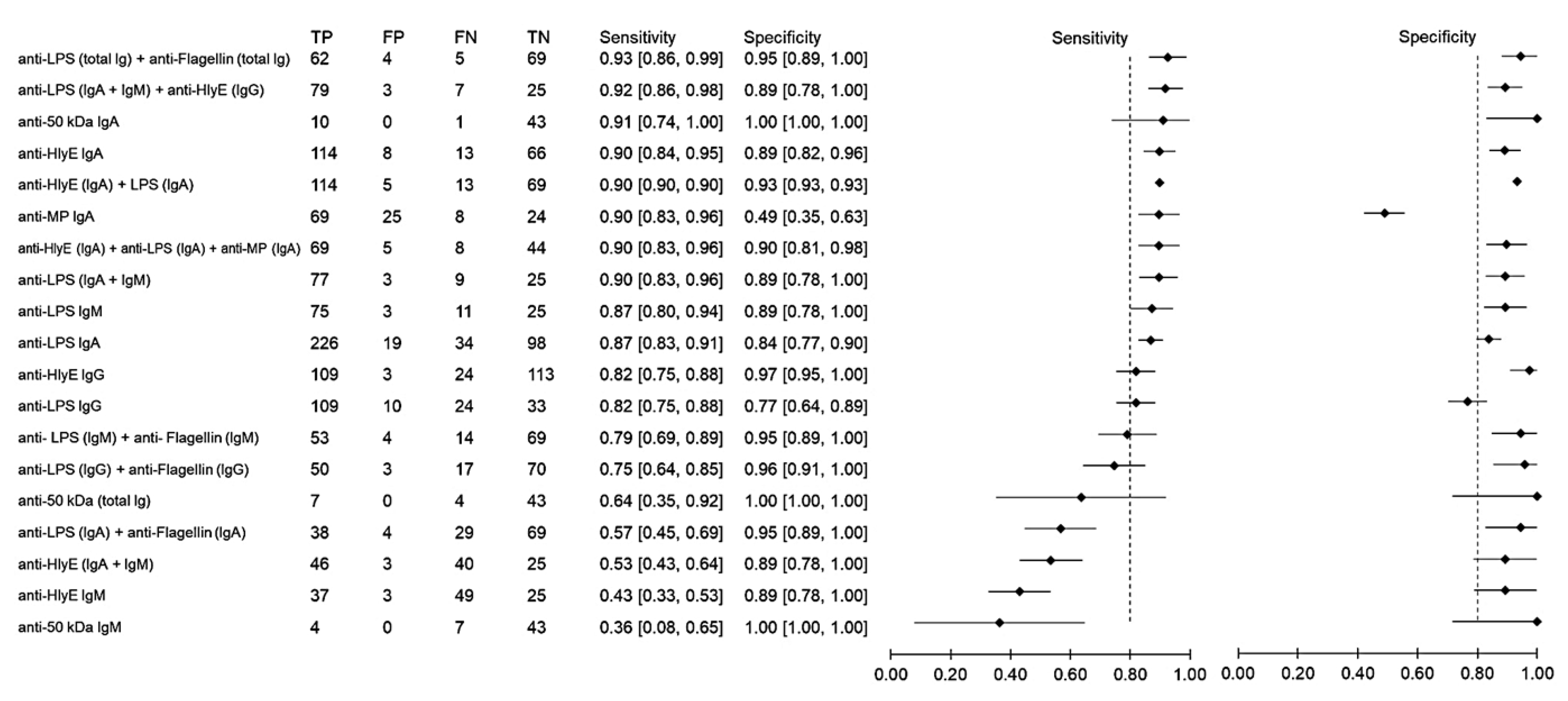
2.3. Performances of the Immunodiagnostic Assays
3. Discussion
4. Methods
4.1. Search Strategy
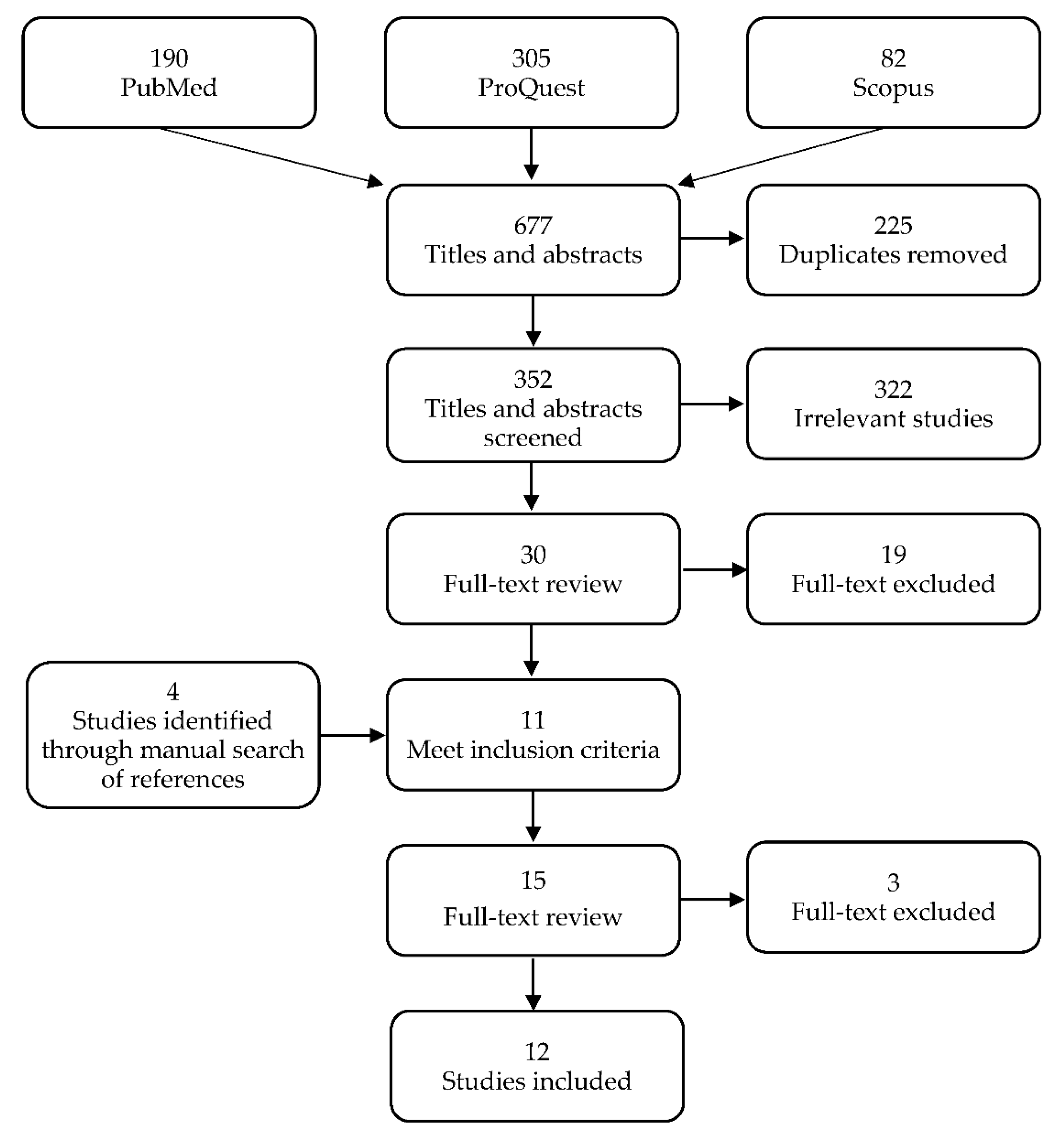
4.2. Selection of Studies
4.3. Data Analysis
4.4. Assessment of the Risk of Bias
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stanaway, J.D.; Reiner, R.C.; Blacker, B.F.; Goldberg, E.M.; Khalil, I.A.; Troeger, C.E.; Andrews, J.R.; Bhutta, Z.A.; Crump, J.A.; Im, J.; et al. The global burden of typhoid and paratyphoid fevers: A systematic analysis for the global burden of disease study 2017. Lancet Infect. Dis. 2019, 19, 369–381. [Google Scholar] [CrossRef] [Green Version]
- Als, D.; Radhakrishnan, A.; Arora, P.; Gaffey, M.F.; Campisi, S.; Velummailum, R.; Zareef, F.; Bhutta, Z.A. Global trends in typhoidal salmonellosis: A systematic review. Am. J. Trop. Med. Hyg. 2018, 99, 10–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muhammad, E.N.; Abdul Mutalip, M.H.; Hasim, M.H.; Paiwai, F.; Pan, S.; Mahmud, M.A.F.; Yeop, N.; Tee, G.H.; Senin, A.A.; Aris, T. The burden of typhoid fever in Klang Valley, Malaysia, 2011–2015. BMC Infect. Dis. 2020, 20, 843. [Google Scholar] [CrossRef]
- Gunn, J.S.; Marshall, J.M.; Baker, S.; Dongol, S.; Charles, R.C.; Ryan, E.T. Salmonella chronic carriage: Epidemiology, diagnosis, and gallbladder persistence. Trends Microbiol. 2014, 22, 648–655. [Google Scholar] [CrossRef] [Green Version]
- Contini, S. Typhoid intestinal perforation in developing countries: Still unavoidable deaths? World J. Gastroenterol. 2017, 23, 1925–1931. [Google Scholar] [CrossRef] [PubMed]
- Dougan, G.; Baker, S. Salmonella enterica serovar Typhi and the pathogenesis of typhoid fever. Annu. Rev. Microbiol. 2014, 68, 317–336. [Google Scholar] [CrossRef]
- Katiyar, A.; Sharma, P.; Dahiya, S.; Singh, H.; Kapil, A.; Kaur, P. Genomic profiling of antimicrobial resistance genes in clinical isolates of Salmonella Typhi from patients infected with typhoid fever in India. Sci. Rep. 2020, 10, 8299. [Google Scholar] [CrossRef]
- Godbole, G.; McCann, N.; Jones, S.M.; Dallman, T.J.; Brown, M. Ceftriaxone-resistant Salmonella Typhi in a traveller returning from a mass gathering in Iraq. Lancet Infect. Dis. 2019, 19, 467. [Google Scholar] [CrossRef] [Green Version]
- Qamar, F.N.; Yousafzai, M.T.; Khalid, M.; Kazi, A.M.; Lohana, H.; Karim, S.; Khan, A.; Hotwani, A.; Qureshi, S.; Kabir, F.; et al. Outbreak investigation of ceftriaxone-resistant Salmonella enterica serotype Typhi and its risk factors among the general population in Hyderabad, Pakistan: A matched case-control study. Lancet Infect. Dis. 2018, 18, 1368–1376. [Google Scholar] [CrossRef]
- Castonguay-Vanier, J.; Davong, V.; Bouthasavong, L.; Sengdetka, D.; Simmalavong, M.; Seupsavith, A.; Dance, D.A.B.; Baker, S.; Phuong, T.L.T.; Vongsouvath, M.; et al. Evaluation of a simple blood culture amplification and antigen detection method for diagnosis of Salmonella enterica serovar Typhi bacteremia. J. Clin. Microbiol. 2013, 51, 142–148. [Google Scholar] [CrossRef] [Green Version]
- Baker, S.; Favorov, M.; Dougan, G. Searching for the elusive typhoid diagnostic. BMC Infect. Dis. 2010, 10, 45. [Google Scholar] [CrossRef] [Green Version]
- Adhikari, A.; Rauniyar, R.; Raut, P.P.; Manandhar, K.D.; Gupta, B.P. Evaluation of sensitivity and specificity of ELISA against widal test for typhoid diagnosis in endemic population of Kathmandu. BMC Infect. Dis. 2015, 15, 523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdullah, J.; Saffie, N.; Sjasri, F.A.R.; Husin, A.; Abdul-Rahman, Z.; Ismail, A.; Aziah, I.; Mohamed, M. Rapid detection of Salmonella Typhi by loop-mediated isothermal amplification (LAMP) method. Braz. J. Microbiol. 2014, 45, 1385–1391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, S.; Rajendran, K.; Dutta, P.; Saha, T.K.; Dutta, S. Validation of a new serology-based dipstick test for rapid diagnosis of typhoid fever. Diagn. Microbiol. Infect. Dis. 2013, 76, 5–9. [Google Scholar] [CrossRef]
- Andrews, J.R.; Khanam, F.; Rahman, N.; Hossain, M.; Bogoch, I.I.; Vaidya, K.; Kelly, M.; Calderwood, S.B.; Bhuiyan, T.R.; Ryan, E.T.; et al. Plasma immunoglobulin A responses against 2 Salmonella Typhi antigens identify patients with typhoid fever. Clin. Infect. Dis. 2019, 68, 949–955. [Google Scholar] [CrossRef] [Green Version]
- Franklin, F.; Chong, C.W.; Chua, L.H.; Anthony, A.A.; Liew, M.W.O.; Aziah, I.; Ong, E.B.B. Evaluation of Salmonella Typhi antigen YncE alongside HlyE for the detection of typhoid fever and its carriers. Med. Microbiol. Immunol. 2020, 209, 593–601. [Google Scholar] [CrossRef]
- Mitra, R.; Bhan, S.; Nath, G.; Kumar, N.; Ali, Z. Development of a novel rapid immunodiagnostic kit based on flagellar 40 kDa antigen epitope for the detection of typhoid fever in Indian patients. Sci. World J. 2013, 2013, 363652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fadeel, M.A.; House, B.L.; Wasfy, M.M.; Klena, J.D.; Habashy, E.E.; Said, M.M.; Maksoud, M.A.; Rahman, B.A.; Pimentel, G. Evaluation of a newly developed ELISA against widal, TUBEX-TF and Typhidot for typhoid fever surveillance. J. Infect. Dev. Ctries 2011, 5, 169–175. [Google Scholar] [CrossRef]
- Zaka-ur-Rab, Z.; Abqari, S.; Shahab, T.; Islam, N.; Shukla, I. Evaluation of salivary anti-Salmonella typhi lipopolysaccharide IgA ELISA for serodiagnosis of typhoid fever in children. Arch. Dis. Child. 2012, 97, 236–238. [Google Scholar] [CrossRef]
- Charles, R.C.; Sultana, T.; Alam, M.M.; Yu, Y.; Wu-Freeman, Y.; Bufano, M.K.; Rollins, S.M.; Tsai, L.; Harris, J.B.; LaRocque, R.C.; et al. Identification of immunogenic Salmonella enterica serotype Typhi antigens expressed in chronic biliary carriers of S. Typhi in Kathmandu, Nepal. PLoS Negl. Trop. Dis. 2013, 7, e2335. [Google Scholar] [CrossRef] [Green Version]
- Ong, E.B.; Ignatius, J.; Anthony, A.A.; Aziah, I.; Ismail, A.; Lim, T.S. Multi-isotype antibody responses against the multimeric Salmonella Typhi recombinant hemolysin E antigen. Microbiol. Immunol. 2015, 59, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Davies, D.H.; Jain, A.; Nakajima, R.; Liang, L.; Jasinskis, A.; Supnet, M.; Felgner, P.L.; Teng, A.; Pablo, J.; Molina, D.M.; et al. Serodiagnosis of acute typhoid fever in Nigerian pediatric cases by detection of serum IgA and IgG against hemolysin E and Lipopolysaccharide. Am. J. Trop. Med. Hyg. 2016, 95, 431–439. [Google Scholar] [CrossRef] [Green Version]
- Felgner, J.; Jain, A.; Nakajima, R.; Liang, L.; Jasinskas, A.; Gotuzzo, E.; Vinetz, J.M.; Miyajima, F.; Pirmohamed, M.; Hassan-Hanga, F.; et al. Development of ELISAs for diagnosis of acute typhoid fever in Nigerian children. PLoS Negl. Trop. Dis. 2017, 11, e0005679. [Google Scholar] [CrossRef] [Green Version]
- Mohd Redhuan, N.E.; Chin, K.L.; Adnan, A.S.; Ismail, A.; Balaram, P.; Phua, K.K. Salivary anti-50 kDa antibodies as a useful biomarker for diagnosis of typhoid fever. J. Clin. Diagnostic. Res. 2017, 11, 10–13. [Google Scholar]
- Sharma, T.; Sharma, C.; Sankhyan, A.; Bedi, S.P.; Bhatnagar, S.; Khanna, N.; Gautam, V.; Sethi, S.; Vrati, S.; Tiwari, A. Serodiagnostic evaluation of recombinant CdtB of S. Typhi as a potential candidate for acute typhoid. Immunol. Res. 2018, 66, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Nodoushani, A.; Khanam, F.; DeCruz, A.T.; Lambotte, P.; Scott, R.; Bogoch, I.I.; Vaidya, K.; Calderwood, S.B.; Bhuiyan, T.R.; et al. Evaluation of a rapid point-of-care multiplex immunochromatographic assay for the diagnosis of enteric fever. Clin. Sci. Epidemiol. 2020, 5, 1–8. [Google Scholar] [CrossRef]
- Maheshwari, V.; Kaore, N.M.; Ramnani, V.K.; Sarda, S. A comparative evaluation of different diagnostic modalities in the diagnosis of typhoid fever using a composite reference standard: A tertiary hospital-based study in Central India. J. Clin. Diagnostic. Res. 2016, 10, DC01–DC04. [Google Scholar] [CrossRef]
- Wijedoru, L.; Mallett, S.; Parry, C.M. Rapid diagnostic tests for typhoid and paratyphoid (enteric) fever. Cochrane Database Syst. Rev. 2017, 2017, CD008892. [Google Scholar] [CrossRef] [Green Version]
- Herath, H.M.T.U. Early diagnosis of typhoid fever by the detection of salivary IgA. J. Clin. Pathol. 2003, 56, 694–698. [Google Scholar] [CrossRef] [Green Version]
- Choo, K.E.; Davis, T.M.; Ismail, A.; Ong, K.H. Longevity of antibody responses to a Salmonella typhi-specific outer membrane protein: Interpretation of a dot enzyme immunosorbent assay in an area of high typhoid fever endemicity. Am. J. Trop. Med. Hyg. 1997, 57, 656–659. [Google Scholar] [CrossRef]
- Ismail, A. New Advances in the Diagnosis of Typhoid and Detection of Typhoid Carriers. Malays. J. Med. Sci. 2000, 7, 3–8. [Google Scholar]
- Strid, M.A.; Dalby, T.; Mølbak, K.; Krogfelt, K.A. Kinetics of the Human Antibody Response against Salmonella enterica Serovars Enteritidis and Typhimurium Determined by Lipopolysaccharide Enzyme-Linked Immunosorbent Assay. Clin. Vaccine Immunol. 2007, 14, 741–747. [Google Scholar] [CrossRef] [Green Version]
- Bhatti, A.B.; Ali, F.; Satti, S.A. Cross-reactivity of rapid Salmonella Typhi IgM immunoassay in dengue fever without co-existing infection. Cureus J. Med. Sci. 2015, 7, e396. [Google Scholar] [CrossRef] [Green Version]
- Dunn, M.R.; Jimenez, R.M.; Chaput, J.C. Analysis of aptamer discovery and technology. Nat. Rev. Chem. 2017, 1, 0076. [Google Scholar] [CrossRef]
- Kintz, E.; Heiss, C.; Black, I.; Donohue, N.; Brown, N.; Davies, M.R.; Azadi, P.; Baker, S.; Kaye, P.M.; Woude, M.V.D. Salmonella enterica Serovar Typhi lipopolysaccharide O-antigen modification impact on serum resistance and antibody recognition. Infect. Immun. 2017, 85, e01021-16. [Google Scholar] [CrossRef] [Green Version]
- Von Rhein, C.; Hunfeld, K.; Ludwig, A. Serologic evidence for effective production of cytolysin A in Salmonella enterica serovars Typhi and Paratyphi A during human infection. Infect. Immun. 2006, 74, 6505–6508. [Google Scholar] [CrossRef] [Green Version]
- Liang, L.; Juarez, S.; Nga, T.V.T.; Dunstan, S.; Nakajima-Sasaki, R.; Huw Davies, D.; McSorley, S.; Baker, S.; Felgner, P.L. Immune profiling with a Salmonella Typhi antigen microarray identifies new diagnostic biomarkers of human typhoid. Sci. Rep. 2013, 3, 1043. [Google Scholar] [CrossRef]
- Chin, K.L.; Redhuan, N.E.M.; Balaram, P.; Phua, K.K.; Ong, E.B.B. Detection of salivary IgA antibodies against the HlyE antigen as a diagnosis of typhoid fever. J. Clin. Diagnostic. Res. 2016, 10, DM01–DM03. [Google Scholar] [CrossRef] [PubMed]
- Von Rhein, C.; Bauer, S.; López Sanjurjo, E.J.; Benz, R.; Goebel, W.; Ludwig, A. ClyA cytolysin from Salmonella: Distribution within the genus, regulation of expression by SlyA, and pore-forming characteristics. Int. J. Med. Microbiol. 2009, 299, 21–35. [Google Scholar] [CrossRef]
- Singh, A.; Verma, H.N.; Arora, K. Surface plasmon resonance-based label-free detection of Salmonella using DNA self-assembly. Appl. Biochem. Biotechnol. 2014, 175, 1330–1343. [Google Scholar] [CrossRef] [PubMed]
- Shephard, M.; Shephard, A.; Matthews, S.; Andrewartha, K. The benefits and challenges of point-of-care testing in rural and remote primary care settings in Australia. Arch. Pathol. Lab. Med. 2020, 144, 1372–1380. [Google Scholar] [CrossRef]
- Tran Vu Thieu, N.; Trinh Van, T.; Tran Tuan, A.; Klemm, E.J.; Nguyen Ngoc Minh, C.; Voong Vinh, P.; Pham Thanh, D.; Ho Ngoc Dan, T.; Pham Duc, T.; Langat, P.; et al. An evaluation of purified Salmonella Typhi protein antigens for the serological diagnosis of acute typhoid fever. J. Infect. 2017, 75, 104–114. [Google Scholar] [CrossRef] [Green Version]
- Darton, T.C.; Baker, S.; Randall, A.; Dongol, S.; Karkey, A.; Voysey, M.; Carter, M.J.; Jones, C.; Trappl, K.; Pablo, J.; et al. Identification of novel serodiagnostic signatures of typhoid fever using a Salmonella proteome array. Front. Microbiol. 2017, 8, 1794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naveen Kumar, C.; Ponniah, M.; Srikumar, R.; Vijayakumar, R.; Chidambaram, R.; Jayalakshmi, G.; Prabhakar Reddy, E.; Manoharan, A.; Sai Ravi Kiran, B. Incidence of dengue fever in febrile patients and co-infection with typhoid fever in South India. Ann. Med. Health Sci. Res. 2017, 7, 111–113. [Google Scholar]
- Onyido, A.E.; Ifeadi, C.P.; Umeanaeto, P.U.; Irikannu, K.C.; Aribodor, D.N.; Ezeanya, L.C.; Ugha, C.N.; Obiechina, I.O. Co-Infection of malaria and typhoid fever in Ekwulumili Community Anambra State, Southeastern Nigeria. N. Y. Sci. J. 2014, 7, 18–27. [Google Scholar]
- Parry, C.M.; Wijedoru, L.; Arjyal, A.; Baker, S. The utility of diagnostic tests for enteric fever in endemic locations. Expert Rev. Anti-Infect. Ther. 2011, 9, 711–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thriemer, K.; Ley, B.; Menten, J.; Jacobs, J.; Van Den Ende, J. A systematic review and meta-analysis of the performance of two point of care typhoid fever tests, tubex TF and typhidot, in endemic countries. PLoS ONE 2013, 8, e81263. [Google Scholar]
- Bujang, M.A.; Adnan, T.H. Requirements for minimum sample size for sensitivity and specificity analysis. J. Clin. Diagnostic. Res. 2016, 10, YE01–YE06. [Google Scholar] [CrossRef] [PubMed]
- Storey, H.L.; Huang, Y.; Crudder, C.; Golden, A.; De Los Santos, T.; Hawkins, K. A meta-Analysis of typhoid diagnostic accuracy studies: A recommendation to adopt a standardized composite reference. PLoS ONE 2015, 10, e0142364. [Google Scholar]
- Amalina, Z.N.; Khalid, M.F.; Rahman, S.F.; Ahmad, M.N.; Najib, M.A.; Ismail, A.; Aziah, I. Nucleic acid-based lateral flow biosensor for Salmonella Typhi and Salmonella Paratyphi: A detection in stool samples of suspected carriers. Diagnostics 2021, 11, 700. [Google Scholar] [CrossRef]
- Maude, R.R.; de Jong, H.K.; Wijedoru, L.; Fukushima, M.; Ghose, A.; Samad, R.; Hossain, M.A.; Karim, M.R.; Faiz, M.A.; Parry, C.M.; et al. The diagnostic accuracy of three rapid diagnostic tests for typhoid fever at Chittagong Medical College Hospital, Chittagong, Bangladesh. Trop. Med. Int. Health 2015, 20, 1376–1384. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Biomarker | Sample | Sensitivity and Specificity | No of Samples | Ref. | |
|---|---|---|---|---|---|---|
| 1 | ELISA | Anti-LPS (IgG, IgM and IgA) anti-flagellin (IgG, IgM and IgA) | Serum | Total Ig: 93% and 95% IgG: 75% and 55% IgM: 79% and 95% IgA: 57% and 96% | Positive S. Typhi blood culture (n = 67), Widal positive (98), febrile controls (n = 216) and healthy controls (n = 7). | [18] |
| 2 | ELISA | Anti-LPS IgA | Saliva | 89.2% and 100% | Positive S. Typhi blood culture (n = 37), febrile controls (n = 30) and healthy controls (n = 30). | [19] |
| 3 | IC-LFT | Anti-LPS (IgG IgM) and anti-flagellin (IgG IgM) | Serum | 68.8% and 71.1% | Positive S. Typhi blood culture (n = 80) and negative S. Typhi blood culture (n = 256). | [14] |
| 4 | ELISA | Anti-YncE (IgG) and anti-Vi (IgG and IgA) | Serum | YncE IgG: 70% and 100% Vi IgG: 40% and 100% Vi IgA: 50% and 97% | S. Typhi carriers (n = 10), acute typhoid fever cases (n = 8), Nepalese controls undergoing elective cholecystectomy with negative bile cultures (n = 8) and healthy Bangladeshis (n = 8). | [20] |
| 5 | ELISA | Anti-HlyE (IgG IgM and IgA) | Serum | 70% and 100% | Positive S. Typhi blood culture (n = 50), positive S. Paratyphi A blood culture (n = 6), other febrile infections (n = 19) and healthy individuals (n = 25). | [21] |
| 6 | LFT | Anti-HlyE (IgG IgA) and anti-LPS (IgG IgA) | Serum | HlyE IgG: 91.5% and 80.0% (against healthy) HlyE IgA: 94.4% and 90.0% (against healthy) HlyE IgG: 78.7% and 100% (against other febrile infections) HlyE IgA: 66.7% and 80% (against other febrile infections) LPS IgG: 89.3% and 100% (against healthy) LPS IgA: 94.4% and 90.0% (against healthy) LPS IgG: 82.1% and 60.0% (against other febrile infections) LPS IgA: 81.8% and 54.5% (against other febrile infections) | Positive S. Typhi blood culture (n = 47), other febrile infections (n = 15), febrile with no bacterial growth (n = 67), healthy U.S. adults (n = 11) and healthy Nigerian children (n = 10). | [22] |
| 7 | ELISA | Anti-HlyE (IgG IgA IgM) and anti-LPS (IgG IgA IgM) | Serum | HlyE IgG: 84% and 90% (against Nigerian febrile controls) LPS IgA and IgM: 90% and 90% (against Nigerian febrile controls) | Nigerian pediatric typhoid cases (n = 86), Nigerian febrile controls (n = 28) and Nigerian healthy controls (n = 48). | [23] |
| 8 | Dot-EIA | Anti-50 kDa (IgG IgA IgM) | Saliva, serum | 50 kDa IgGAM: 90.9% sensitivity and 85.4% (saliva) 50 kDa IgGAM: 100% and 100% (serum) | Positive S. Typhi blood culture (n = 11), non-typhoid fever patients (n = 43) and healthy (n = 53). | [24] |
| 9 | ELISA | Anti-CdtB IgM | Serum | 100% and 83.3% | Positive S. Typhi blood culture (n = 21) and healthy controls (n = 12). | [25] |
| 10 | ELISA | Anti-HlyE IgA, anti-MP IgA and anti-LPS IgA | Serum | HlyE: 90% and 87% LPS: 90% and 77% MP: 90% and 48% HlyE and anti-LPS: 90% and 92% HlyE, LPS and MP: 90% and 90% | Positive S. Typhi blood culture (n = 105), healthy controls (n = 84) and other febrile disease (n = 64). | [15] |
| 11 | ELISA | Anti-HlyE (IgG IgA IgM) and anti-YncE (IgG IgA IgM) | Serum | HlyE IgGAM: 83% and 98% | Acute typhoid cases (n = 115), healthy controls (n = 95), other febrile infections (n = 95) and food handlers (n = 117). | [16] |
| 12 | ELISA, DDP-LF | Anti-LPS IgA and anti-HlyE IgA | Serum | 92% and 94% (against all controls) 90% and 96% (against febrile endemic controls) | Positive S. Typhi blood culture (n = 30), positive S. Paratyphi A blood culture (n = 20), healthy endemic controls (n = 25) and febrile endemic controls (n = 25). | [26] |
| Domains | Criteria for Low Risk Assessment |
|---|---|
| Patient selection | Patient enrolment strategy is specified and free of bias. A case—control design and inappropriate exclusions are avoided. |
| Index test | The index test results are interpreted without knowledge of the results of the reference standard. The conduct or interpretation of the index test does not introduce bias. |
| Reference standard | The reference standard correctly classifies the target condition. The reference standard results are interpreted without knowledge of the results of the index test. The reference standard, its conduct, or its interpretation do not introduce bias. |
| Flow and timing | There is an appropriate interval between the index test(s) and reference standard. All patients receive the same reference standard. All patients included in the analysis and patient flow do not introduce bias. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Najib, M.A.; Mustaffa, K.M.F.; Ong, E.B.B.; Selvam, K.; Khalid, M.F.; Awang, M.S.; Zambry, N.S.; Manaf, A.A.; Bustami, Y.; Hamzah, H.H.; et al. Performance of Immunodiagnostic Tests for Typhoid Fever: A Systematic Review and Meta-Analysis. Pathogens 2021, 10, 1184. https://doi.org/10.3390/pathogens10091184
Najib MA, Mustaffa KMF, Ong EBB, Selvam K, Khalid MF, Awang MS, Zambry NS, Manaf AA, Bustami Y, Hamzah HH, et al. Performance of Immunodiagnostic Tests for Typhoid Fever: A Systematic Review and Meta-Analysis. Pathogens. 2021; 10(9):1184. https://doi.org/10.3390/pathogens10091184
Chicago/Turabian StyleNajib, Mohamad Ahmad, Khairul Mohd Fadzli Mustaffa, Eugene Boon Beng Ong, Kasturi Selvam, Muhammad Fazli Khalid, Mohd Syafiq Awang, Nor Syafirah Zambry, Asrulnizam Abd Manaf, Yazmin Bustami, Hairul Hisham Hamzah, and et al. 2021. "Performance of Immunodiagnostic Tests for Typhoid Fever: A Systematic Review and Meta-Analysis" Pathogens 10, no. 9: 1184. https://doi.org/10.3390/pathogens10091184