
Syphilitic Gummata in the Central Nervous System: A Narrative Review and Case Report about a Noteworthy Clinical Manifestation

 ,
,
Abstract
:1. Introduction
2. Case Presentation
3. Review
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Search Criteria
References
- Church, B.; Wall, E.; Webb, J.R.; Cameron, C.E. Interaction of treponema pallidum, the syphilis spirochete, with human platelets. PLoS ONE 2019, 14, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Margos, G.; Gofton, A.; Wibberg, D.; Dangel, A.; Marosevic, D.; Loh, S.M.; Oskam, C.; Fingerle, V. The genus Borrelia reloaded. PLoS ONE 2018, 13, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Pónyai, K.; Ostorházi, E.; Marschalkó, M.; Kárpáti, S.; Rozgonyi, F. Syphilis: Today. Rev. Med. Microbiol. 2010, 21, 84–95. [Google Scholar] [CrossRef]
- Ojcius, D.; Peeling, R.W.; Mabey, D.C.W. In the news/focus: Syphilis. Nat. Rev. Microbiol. 2004, 2, 448–449. [Google Scholar] [CrossRef]
- CDC Syphilis & MSM (Men who have Sex with Men). CDC Fact Sheet. STD Facts 2019, 1–2, 1. [Google Scholar]
- Marra, C.M.; González-Scarano, F.; Jeanne, M. Neurosyphilis—UpToDate. Available online: https://www.uptodate.com/contents/neurosyphilis?search=neurosyphilis&source=search_result&selectedTitle=1~70&usage_type=default&display_rank=1 (accessed on 4 March 2020).
- Ropper, A.H. Neurosyphilis. N. Engl. J. Med. 2019, 381, 1358–1363. [Google Scholar] [CrossRef]
- Tien, R.D.; Gean-Marton, A.D.; Mark, A.S. Neurosyphilis in HIV carriers: MR findings in six patients. Am. J. Roentgenol. 1992, 158, 1325–1328. [Google Scholar] [CrossRef]
- Thibodeau, R.; Goel, A.; Jafroodifar, A.; Klumpp, M.; Mirchia, K.; Swarnkar, A. Cerebral syphilitic gumma presenting with intracranial gumma and pathologic vertebrae fractures. Radiol. Case Rep. 2021, 16, 916–922. [Google Scholar] [CrossRef]
- Weng, C.; Huang, K.; Jiang, T.; Zhou, G.; Wu, T. Cerebral syphilitic gumma masquerading as cerebral metastatic tumors: Case report. Neurosurg. Focus 2019, 47. [Google Scholar] [CrossRef]
- Tawfik, S.; Khong, P.; Dower, A.; Huynh, W. Syphilitic gumma presenting as myelopathy. J. Clin. Neurosci. 2019, 10–11. [Google Scholar] [CrossRef]
- Shen, S.; Yang, R.; Wang, L.; Tang, L.; Liu, B. Multiple intracranial and spinal cord syphilitic gummas in a human immunodeficiency virus-negative man with untreated syphilis: A case report. Medicine 2019, 98, e16887. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, R.; Tanaka, N.; Okazaki, T.; Yonezawa, T. Multiple cerebral syphilitic gummas mimicking brain tumor in a non-HIV-infected patient: A case report. J. Infect. Chemother. 2019, 25, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.H.; Shi, Q.X.; Xu, M.M.; Chen, C.Z.; Yang, M.L.; Li, J.J.; Chen, Y.F.; Lin, Z.Q.; Lin, Y.Y. Spinal cord syphilitic gumma presenting with brown-Séquard syndrome: A case report and literature review. Ann. Clin. Lab. Sci. 2019, 49, 265–270. [Google Scholar] [PubMed]
- Shao, X.; Qiang, D.; Liu, Y.; Yuan, Q.; Tao, J.; Ji, B. Diagnosis and Treatment of Cerebral Syphilitic Gumma: A Report of Three Cases. Front. Neurosci. 2018, 12, 1–6. [Google Scholar] [CrossRef]
- Kuroi, Y.; Tani, S.; Shibuya, M.; Kasuya, H. Teaching NeuroImages: Cerebral syphilitic gumma with numerous spirochetes in immunohistochemical staining. Neurology 2018, 90, e818–e819. [Google Scholar] [CrossRef]
- Koizumi, Y.; Watabe, T.; Ota, Y.; Nakayama, S.I.; Asai, N.; Hagihara, M.; Yamagishi, Y.; Suematsu, H.; Tsuzuki, T.; Takayasu, M.; et al. Cerebral Syphilitic Gumma Can Arise Within Months of Reinfection: A Case of Histologically Proven Treponema pallidum Strain Type 14b/f Infection with Human Immunodeficiency Virus Positivity. Sex. Transm. Dis. 2018, 45, e1–e4. [Google Scholar] [CrossRef]
- Kodama, T.; Sato, H.; Osa, M.; Fujikura, Y.; Kawana, A. Cerebral syphilitic gumma in immunocompetent man, Japan. Emerg. Infect. Dis. 2018, 24, 395–396. [Google Scholar] [CrossRef] [Green Version]
- Kikuchi, Y.; Hiwatashi, A.; Togao, O.; Yamashita, K.; Momosaka, D.; Honda, H. Cerebral syphilitic gumma mimicking glioma: Utility of CT perfusion. Diagn. Interv. Imaging 2018, 99, 755–757. [Google Scholar] [CrossRef]
- Yin, R.; Wang, L.; Zhang, T.; Zhao, B. Syphilis of the lumbar spine: A case report and review of the literature. Medicine 2017, 96, e9098. [Google Scholar] [CrossRef]
- Xia, D.Y.; Zhu, M.F.; Liu, C.G.; Dai, Y.; Li, Z.B.; Jiang, X.C.; Xu, S.S. Cerebral Syphilitic Gumma Misdiagnosed as a Malignant Brain Tumor. J. Craniofac. Surg. 2017, 28, e170–e172. [Google Scholar] [CrossRef]
- Shi, F.; Jiang, H.; Shi, Z.; Liu, H.; Zhang, Q. Cerebral syphilitic gumma: Case report of a brainstem mass lesion and brief review of the literature. Jpn. J. Infect. Dis. 2017, 70, 595–596. [Google Scholar] [CrossRef]
- Rasool, N.; Stefater, J.A.; Eliott, D.; Cestari, D.M. Isolated presumed optic nerve gumma, a rare presentation of neurosyphilis. Am. J. Ophthalmol. Case Rep. 2017, 6, 7–10. [Google Scholar] [CrossRef]
- Zhang, L.; Zhou, Y.; Chen, J.; Yan, W.; Kong, Q.; Chen, P.; Sang, H. A case of a cerebral syphilitic gumma developed in a few months mimicking a brain tumor in a human immunodeficiency virus-negative patient. Br. J. Neurosurg. 2016, 31, 481–483. [Google Scholar] [CrossRef]
- Yang, C.; Li, G.; Fang, J.; Liu, H.; Yang, B.; Xu, Y. Spinal Intramedullary Syphilitic Gumma: An Unusual Presentation of Neurosyphilis. World Neurosurg. 2016, 95, e17–e23. [Google Scholar] [CrossRef]
- Tsuboi, M.; Nishijima, T.; Teruya, K.; Kikuchi, Y.; Gatanaga, H.; Oka, S. Cerebral syphilitic gumma within 5 months of syphilis in HIV-infected patient. Emerg. Infect. Dis. 2016, 22, 1846–1848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faropoulos, K.; Zolota, V.; Gatzounis, G. Occipital lobe gumma: A case report and review of the literature. Acta Neurochir. 2017, 159, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Sprenger, K.; Furrer, H. Chameleons everywhere. BMJ Case Rep. 2014, 2014, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, Y.K.; Kim, M.J.; Chae, Y.S.; Kang, S.H. Cerebral syphilitic gumma mimicking a brain tumor in the relapse of secondary syphilis in a human immunodeficiency virus-negative patient. J. Korean Neurosurg. Soc. 2013, 53, 197–200. [Google Scholar] [CrossRef]
- Huo, K.; Liu, L. Horizontal gaze palsy with progressive myoclonic epilepsy: Rare presentation of Gaucher’s disease. Neurol. India 2013, 61, 177–178. [Google Scholar] [CrossRef]
- Ventura, N.; Cannelas, R.; Bizzo, B.; Gasparetto, E.L. Intracranial syphilitic gumma mimicking a brain stem glioma. Am. J. Neuroradiol. 2012, 33, 110–111. [Google Scholar] [CrossRef] [Green Version]
- Noel, C.B.; Moeketsi, K.; Kies, B. Cavernous sinus syndrome, an atypical presentation of tertiary syphilis: Case report and review of the literature. Clin. Neurol. Neurosurg. 2011, 113, 65–67. [Google Scholar] [CrossRef]
- Li, J.C.; Mahta, A.; Kim, R.Y.; Saria, M.; Kesari, S. Cerebral syphilitic gumma: A case report and review of the literature. Neurol. Sci. 2012, 33, 1179–1181. [Google Scholar] [CrossRef]
- Lee, C.W.; Lim, M.J.; Son, D.; Lee, J.S.; Cheong, M.H.; Park, I.S.; Lim, M.K.; Kim, E.; Ha, Y. A case of cerebral gumma presenting as brain tumor in a human immunodeficiency virus (HIV)-negative patient. Yonsei Med. J. 2009, 50, 284–288. [Google Scholar] [CrossRef]
- Fargen, K.M.; Alvernia, J.E.; Lin, C.S.; Melgar, M. Cerebral syphilitic gummata: A case presentation and analysis of 156 reported cases. Neurosurgery 2009, 64, 568–575. [Google Scholar] [CrossRef]
- Weinert, L.S.; Scheffel, R.S.; Zoratto, G.; Samios, V.; Jeffmann, M.W.; Dora, J.M.; Goldani, L.Z. Cerebral syphilitic gumma in HIV-infected patients: Case report and review. Int. J. STD AIDS 2008, 19, 62–64. [Google Scholar] [CrossRef]
- Morshed, M.G.; Lee, M.K.; Maguire, J.; Zwimpfer, T.; Willoughby, B.; Clement, J.; Crawford, R.I.; Barberie, J.; Gul, S.; Jones, H. Neurosyphilitic gumma in a homosexual man with HIV infection confirmed by polymerase chain reaction. Int. J. STD AIDS 2008, 19, 568–569. [Google Scholar] [CrossRef]
- Darwish, B.S.; Fowler, A.; Ong, M.; Swaminothan, A.; Abraszko, R. Intracranial syphilitic gumma resembling malignant brain tumour. J. Clin. Neurosci. 2008, 15, 308–310. [Google Scholar] [CrossRef]
- Soares-Fernandez, J.; Ribeiro, M.; Mare, R.; Magalhaes, Z.; Lourenco, E.; Rocha, J. Diffusion-Weighted Magnetic Resonance Imaging Findings in a Patient with Cerebral Syphilitic Gumma. J. Comput. Assist. Tomogr. 2007, 31, 592–594. [Google Scholar] [CrossRef]
- Gyori, E.; Lew, E.O. Unsuspected central nervous system gummas in a case of “cerebral infarctg” associated with cocaine use. Am. J. Forensic Med. Pathol. 2007, 28, 208–211. [Google Scholar] [CrossRef]
- Régal, L.; Demaerel, P.; Dubois, B. Cerebral syphilitic gumma in a human immunodeficiency virus-positive patient. Arch. Neurol. 2005, 62, 1310–1311. [Google Scholar] [CrossRef]
- Ances, B.; Danish, S.; Kolson, D.; Judy, K.; Liebeskind, D. Cerebral Gumma Micking Glioblastoma Multiforme. Neurocrit. Care 2005, 2, 300–302. [Google Scholar] [CrossRef]
- Lana-Peixoto, M.; Teixeira, A.J.; Tzelikis, P.; Campos, W.; Curi, A.; Orefice, F. Asymptomatic Intracranial Gumma in a Patient with Syphilitic Uveitis and Human Immunodeficiency Infection. Scand. J. Infect. Dis. 2003, 35, 341–343. [Google Scholar] [CrossRef]
- Charach, G.; Groskopf, I.; Turner, D.; Barilan, M.; Kugel, C.; Weintraub, M. Syphilitic Gumma and Tubercolosis: An Unusual Combination in AIDS. Case Commun. 2008, 10, 1–2. [Google Scholar]
- Takeshima, H.; Kaku, T.; Ushio, Y. Cerebral Gumma showing spontaneous regression on magnetic resonance imaging study. Neurol. Med. Chir. 1999, 39, 242–245. [Google Scholar] [CrossRef] [Green Version]
- Suarez, J.; Mlakar, D.; Snodgrass, S. Cerebral Syphilitic Gumma in an HIV-Negative Patient Presenting as Prolonged Focal Motor Status Epilepticus. N. Engl. J. Med. 1996, 335, 1159–1160. [Google Scholar] [CrossRef]
- Uemura, K.; Yamada, T.; Tsukada, A.; Enomoto, T.; Yoshii, Y.; Nose, T. Cerebral Gumma Mimicking Resonance Glioblastoma Images on Magnetic. Neurol. Med. Chir. 1995, 35, 462–466. [Google Scholar] [CrossRef] [Green Version]
- Inoue, R.; Katayama, S.; Kusakabe, T.; Mori, T.; Hori, S. Cerebral Gumma Showing Linear Dural Enhancement on Magnetic Resonance Imaging. Neurol. Med. Chir. 1995, 35, 813–817. [Google Scholar] [CrossRef] [Green Version]
- Horowitz, H.; Valsamis, M.; Wicher, V.; Abbruscato, F.; Larsen, S.; Wormser, G.; Wicher, K. Brief Report: Cerebral Syphilitic Gumma Confirmed by The Polymerase Chain Reaction in a Man with Human Immunodeficiency Virus Infection. N. Engl. J. Med. 1994, 331, 1488–1491. [Google Scholar] [CrossRef]
- Herrold, J.M. A Syphilitic Cerebral Gumma Manifesting as a Brain-Stem Mass Lesion That Responded to Corticosteroid Monotherapy. Mayo Clin. Proc. 1994, 69, 960–961. [Google Scholar] [CrossRef]
- Berger, J.R.; Waskin, H.; Pall, L.; Hensley, G.; Ihmedian, I.; Post, M.J.D. Syphilitic cerebral gumma with HIV infection. Neurology 1992, 42, 1282–1287. [Google Scholar] [CrossRef]
- Wang, A.M.; Barriger, T.K.; Wesolowski, D.P. Intracranial gumma mimicking a tuber cinereum tumor. Comput. Med. Imaging Graph. 1991, 15, 57–60. [Google Scholar] [CrossRef]
- Standaert, D.G.; Galetta, S.L.; Atlas, S.W. Meningovascular syphilis with a gumma of the midbrain. J. Clin. Neuroophthalmol. 1991, 11, 139–143. [Google Scholar] [PubMed]
- Smith, J.L.; Byrne, S.F.; Cambron, C.R. Syphiloma/gumma of the optic nerve and human immunodeficiency virus seropositivity. J. Clin. Neuroophthalmol. 1990, 10, 175–184. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| # of Case | Location | Sex | MSM | Age | HIV | Year of Report | Country | Ref. |
|---|---|---|---|---|---|---|---|---|
| 1 | Frontal lobe; thoracic vertebrae | f | 37 | no | 2021 | U.S. | [9] | |
| 2 | Frontal lobe | m | 45 | 2019 | China | [10] | ||
| 3 | Thoracic medullary Th10; cauda equina at the 3/4 lumbar level | m | “In his 30s” | no | 2019 | Australia | [11] | |
| 4 | Multiple loci cerebellar and medullary | m | 22 | no | 2019 | China | [12] | |
| 5 | Frontal and temporal lobe | m | 47 | no | 2019 | Japan | [13] | |
| 6 | Thoracal intra-/extramedullary T8 level | f | 45 | no | 2019 | China | [14] | |
| 7 | Frontal lobe | m | 37 | 2018 | China | [15] | ||
| 8 | Frontal lobe | m | 62 | 2018 | China | [15] | ||
| 9 | Frontal lobe | m | 66 | 2018 | China | [15] | ||
| 10 | Temporal lobe | m | 62 | no | 2018 | Japan | [16] | |
| 11 | Temporal lobe | m | no | 44 | yes | 2018 | Japan | [17] |
| 12 | Temporal | m | 36 | no | 2018 | Japan | [18] | |
| 13 | Frontal lobe | f | 50 | 2018 | Japan | [19] | ||
| 14 | Medullary L4 | m | 61 | 2017 | China | [20] | ||
| 15 | Frontal lobe | m | 62 | 2017 | China | [21] | ||
| 16 | Brain stem | m | no | 41 | no | 2017 | China | [22] |
| 17 | Optic nerve | m | 36 | yes | 2016 | U.S. | [23] | |
| 18 | Parietal lobe | m | 56 | no | 2016 | China | [24] | |
| 19 | Intramedullary C5 level | f | 65 | no | 2016 | China | [25] | |
| 20 | Frontal lobe | m | 21 | yes | 2016 | Japan | [26] | |
| 21 | Occipital lobe | m | 53 | 2016 | Greece | [27] | ||
| 22 | Frontal lobe | m | yes | 51 | no | 2016 | Germany | This case |
| 23 | Parietal lobe | m | 40 | yes | 2014 | Switzerland | [28] | |
| 24 | Frontal lobe | f | 59 | no | 2013 | South Korea | [29] | |
| 25 | Parietal | m | 38 | no | 2013 | China | [30] | |
| 26 | Pons | m | 26 | yes | 2012 | Brazil | [31] | |
| 27 | Cavernous sinus | f | 62 | no | 2011 | South Africa | [32] | |
| 28 | Basal ganglia; temporal lobe | m | 45 | no | 2011 | China | [33] | |
| 29 | Cerebrum | f | 40 | no | 2009 | South Korea | [34] | |
| 30 | Occipital lobe | m | yes | 61 | no | 2008 | U.S. | [35] |
| 31 | Frontal lobe | m | 20 | yes | 2008 | Brazil | [36] | |
| 32 | Frontal lobe | m | yes | 46 | yes | 2008 | Canada | [37] |
| 33 | Temporal lobe | m | no | 43 | no | 2008 | Australia | [38] |
| 34 | Parietal lobe | m | 42 | yes | 2007 | Portugal | [39] | |
| 35 | Parietotemporal | m | no | 54 | 2007 | U.S. | [40] | |
| 36 | Frontal lobe | m | yes | 42 | yes | 2005 | Belgium | [41] |
| 37 | Corpus callosum | m | 42 | no | 2005 | U.S. | [42] | |
| 38 | Pons and middle cerebellar peduncle | m | no | 51 | yes | 2003 | Brazil | [43] |
| 39 | Temporo-parietal | m | 42 | yes | 2002 | Israel | [44] | |
| 40 | Temporo-occipital | m | 75 | 1999 | Japan | [45] | ||
| 41 | Frontal lobe | m | 47 | no | 1996 | U.S. | [46] | |
| 42 | Optic tract, temporal lobe | f | 39 | no | 1995 | Japan | [47] | |
| 43 | Cerebellar, temporal lobe | m | 51 | 1995 | Japan | [48] | ||
| 44 | Parieto-occipital, cerebellum | m | 29 | yes | 1994 | U.S. | [49] | |
| 45 | Pontomesencephalic region; choroidal fissure | m | 69 | no | 1994 | U.S. | [50] | |
| 46 | “Cerebral” | m | yes | 1992 | U.S. | [51] | ||
| 47 | “Cerebral” | m | yes | 1992 | U.S. | [51] | ||
| 48 | Tuber cinereum | m | 37 | 1991 | U.S. | [52] | ||
| 49 | Midbrain and thalamus | m | 27 | 1991 | U.S. | [53] | ||
| 50 | Optic nerve | m | 68 | 1990 | U.S. | [54] |
| # of Case | Clinical Appearance | Surgery | Treatment | Outcome | Ref. |
|---|---|---|---|---|---|
| 1 | Seizures, left-sided weakness, urinary incontinence, mild photophobia, ataxia, and headache. | Yes | Benzathine penicillin G daily; dexamethasone. | [9] | |
| 2 | Headache and left-sided weakness. | Yes | 14-day course of IV penicillin (2.5 million U administered every 4 h) followed by a three-week course of IM of benzathine penicillin (2.4 million U administered once per week). | Myodynamia of the left limbs gradually improved. | [10] |
| 3 | Rapidly progressive right lower limb monoparesis associated with sphincter and erectile dysfunction; impaired sensation in the right leg, with reduced anal tone and saddle anesthesia. | Yes | IV benzylpenicillin. | Near complete neurological recovery after three months. | [11] |
| 4 | Progressive right lower limb weakness with tremor, and headache. | No | IV penicillin G at 24 million units daily divided into six doses was given for a total of 21 days, along with three weekly IM of benzathine penicillin G (BPG, 2.4 million units); oral prednisolone (40 mg) was also prescribed 24 h before the start of penicillin for three days. | Complete neurological recovery after three weeks. | [12] |
| 5 | Generalized tonic-clonic seizures; syphilitic roseola was observed on the skin in the hypogastric region. | no | Amoxicillin per os 1500 mg/day followed by penicillin G IV 24 × 106 U for 14 days. | Completely recovered. | [13] |
| 6 | Revealed muscle strength of grade 3/5 in right lower extremities and loss of superficial sensation of grade 3/10 below the umbilicus on the left side; grade 3 ankle and knee hyperreflexia on the right side; positive Babinski sign and Chaddock sign. | yes | Penicillin G (IV 19.6 million U/day, and 4.9 million U QID) for 14 days, then IM benzathine penicillin G (2.4 million U QW) for 21 days. | Completely recovered after three months. | [14] |
| 7 | Dizziness for ~15 days. | no | 14-day IV penicillin (2.4 million U every 4 h) followed by three weeks of IM benzathine penicillin (2.4 million U, once per week). | Complete recovery after four months. | [15] |
| 8 | Speech arrest for 10 h, clear consciousness. | yes | Complete recovery after six months. | [15] | |
| 9 | Decreasing right eye vision and headache since ~50 days ago. | yes | [15] | ||
| 10 | Headache. | yes | [16] | ||
| 11 | Severe headache, nausea, and vomiting. | yes | 14 days of IV ceftriaxone 2 g every 24 h. | Completely recovered. | [17] |
| 12 | Hearing loss in right ear and right-side facial paralysis since two weeks ago. | no | “2015 U.K. national guidelines”. | After two weeks: facial nerve palsy improved markedly; hearing loss improved gradually. | [18] |
| 13 | Headache, right-sided hearing loss, tinnitus, and vertigo since three months ago. | no | IV penicillin G. | [19] | |
| 14 | Worsening pain and numbness in both lower legs for four weeks, started one year ago. | yes | [20] | ||
| 15 | Speech disturbance and a mild headache since 10 days ago. | yes | Penicillin G IV daily (24 million units for 14 days), followed by IM benzathine penicillin G (2.4 million units three-weekly). | “Improving gradually”. | [21] |
| 16 | Headache, swallowing difficulties, and dysarthria for four months, and vomiting for a month and a half; progressive right facial and neck numbness for two years; dysarthria; right Babinski sign positive. | no | IV penicillin G (24 million units per day). | Complete recovery after two months. | [22] |
| 17 | Decreased vision, left eye. | no | 14 days of IV penicillin. | Vision improved. | [23] |
| 18 | Mild headache; twitch and right limb sustained shaking. | yes | IV penicillin G (24 million units per day for 12 days), followed by IM benzathine penicillin G (2.4 million units three-weekly). | [24] | |
| 19 | Paresthesia in both upper extremities and weakness; two-month history of neck–shoulder–back pain. | yes | IV penicillin G (24 million units/day) for 14 days. | After 29 months: pain completely relieved; sensorimotor dysfunctions partially improved; sensory disturbance remained; muscle strength legs improved. | [25] |
| 20 | 2 h loss of consciousness; prior: uncomfortable feeling at the back of his head and neck and eye fatigue that lasted for one week. | no | IV benzylpenicillin (24 million units/day) for 14 consecutive days. | Complete recovery after two months. | [26] |
| 21 | Rapidly deteriorating gait disorder. | yes | “Per os penicillin”. | Complete recovery. | [27] |
| 22 | One-month history of vertigo and blurry vision; two episodes of tinnitus. | yes | IV penicillin G (24 million units per day, 3–4 million units every 4 h) for 10 days. | Complete recovery after four months. | This case |
| 23 | Persistent fatigue, excessive sweating and pain in the right thorax, slight paresthesia of the right hand, and headaches. | yes | IV penicillin G (6 × 4 Mio U/day) for 14 days. | [28] | |
| 24 | Speech disturbance/dysarthria. | yes | Ceftriaxone IV daily dose of 2 g for 14 days. | Completely recovered after 15 months. | [29] |
| 25 | Headache and emesis for 15 days. | yes | “Symptoms are improving gradually”. | [30] | |
| 26 | Four-month history of fever, weight loss, dizziness, diarrhea, tremors, and paresthesia, disorientation, pyramidal and extrapyramidal symptoms, and multiple cutaneous non-pruriginous cicatricial lesions affecting the chest and inferior limbs. | no | IV crystalline penicillin (24 × 106 units/day) for 14 days. | “Significant clinical improvement”. | [31] |
| 27 | Two-week history of painful ophthalmoplegia and a complete left ptosis, signs of cavernous sinus syndrome, with left sided III, IV, V1, V2, and VI cranial nerve palsies. | no | IV crystalline penicillin G (24 million units per day) for two weeks, followed by 2.4 million units of IM penicillin administered weekly for three weeks (total 7.2 million units). | Cranial nerves: After three weeks, full recovery in III, IV, V1, and V2, and partial recovery in cranial nerve VI. | [32] |
| 28 | Eight-day history of right-sided vision loss, slurred speech, incoordination of his right arm and leg, and imbalance ad admission. | yes | IV penicillin G 14 days, followed by three-weekly IM shots of benzathine penicillin G (2.4 million units). | One-month follow-up: gait and use of right hand improved dramatically; right-sided visual loss persisted. | [33] |
| 29 | Three- to four-month history of headache. | yes | IV penicillin G daily (24 × 106 U) for 10 days. | Complete recovery. | [34] |
| 30 | Two-month history of progressively worsening altered mental status and intermittent seizures characterized by the déjà vu phenomena; left homonymous hemianopsia. | yes | [35] | ||
| 31 | Single episode of a tonic-clonic seizure. | yes | IV crystalline penicillin G (24 million units) daily for 14 days. | [36] | |
| 32 | Eight-week history of left frontal headaches. | no | “Intravenous penicillin”. | No further symptoms. | [37] |
| 33 | Two-month history of worsening generalized headaches, nausea, and peculiar speech. | yes | “Intravenous penicillin”. | Full clinical recovery. | [38] |
| 34 | Generalized seizure. | no | IV penicillin G; after 10 days, the patient refused further treatment. | After two-month asymptomatic period, follow-up MRI: residual focal contrast enhancement, marked reduction of perilesional edema, and normal signal on diffusion weighted imaging (DWI). | [39] |
| 35 | “Altered mental status,” rhabdomyolysis, and hypernatremia; confused, disoriented, and agitated; “speech was incoherent, his mood anxious, and his affect inappropriate”. | no | The patient died eight days after admission; the diagnosis of neurosyphilitic gumma was made post-mortem. | [40] | |
| 36 | Fever, headache for two and a half months, and hearing loss since one week before | no | IV penicillin G and ampicillin for three weeks | Complete recovery after three weeks | [41] |
| 37 | Frequent falling, visual hallucinations, headaches, diminished appetite, and prominent weight loss over a period of several months; cachectic and minimally interactive; prominent abulia, psychomotor retardation, and tremulousness of bilateral upper extremities; diminished proprioception with a shuffling gait | yes | Patient died during hospital stay | [42] | |
| 38 | Three-month history of progressive visual decline in the right eye | no | IV penicillin (24 million units/day) for 21 days | Lost to follow-up | [43] |
| 39 | Grand mal seizure; ataxia | yes | Treatment for tuberculosis | Died after three weeks; post-mortem diagnosis of syphilis | [44] |
| 40 | 10-day history of headache | yes | IV penicillin G: Skin eruption; switch to oral erythromycin for 28 days | Recovery | [45] |
| 41 | Generalized seizure | no | IV phenytoin and high-dose penicillin G for 21 days | Recovery | [46] |
| 42 | Visual impairment worsening rapidly over one week; left upper quadrantanopsia, diplopia, slight hemiparesis, and hypesthesia on the left side; bilateral optic atrophy | yes | IV penicillin G (24 × 106 U/day IV) plus probenecid for 14 days, followed by procaine penicillin G (2.4 × 106 U/week IM) | Rigidity in left upper extremity resolved; left upper homonymous quadrantanopsia remained | [47] |
| 43 | Four-month history of headache; diplopia for three months; vertigo; cerebellar ataxia; abducens nerve paresis | yes | IV penicillin G (12 × 106 U/day) for 10 days (total 120 × 106 U) | Cerebellar ataxia gradually improved; right abducens nerve paresis remained unchanged | [48] |
| 44 | Three years before: history of right-sided weakness for six months, changes in mental status for three months, one seizure one week before admission, problems with swallowing for one week; at admission: disorientation, tremoulus, and poor memory | no | Cefotaxime 2 g IV every 6 h for 11 days, followed by IV penicillin G (12 × 106 U/day) for 10 days; subsequently, amphotericin B and ceftazidime (because of progressive neurological deterioration) | None of the lesions resolved with treatment; four days before death, occlusive hydrocephalus | [49] |
| 45 | Intermittent diplopia, slurred speech, right-sided weakness, and gait unsteadiness; after therapy (five months later): Mild worsening of the right-sided hemiparesis | no | Allergy to penicillin: two-week IV ceftriaxone (1 g/day), followed by 30 days of oral doxycycline (100 mg twice a day); second treatment five months after initial treatment: skin tests for penicillin allergy; subsequently, 21 days of IV penicillin (4 million U every 4 h) | Five months after initial therapy: Mild worsening of hemiparesis; at follow-up six months after last therapy (penicillin): Remained neurologically stable; findings on a repeated lumbar puncture were normal | [50] |
| 46 | Seizure disorder | yes | “High-dose” IV penicillin | [51] | |
| 47 | Seizure disorder | no | “High-dose” IV penicillin | [51] | |
| 48 | Headache for three months; mild ataxia, intermittent low-grade fever, skin rashes, cervical lymph node enlargement, conjunctivitis, and progressively decreased libido | Initial diagnosis sarcoidosis: prednisone; after second lumbar puncture and diagnosis of syphilis: IV penicillin G (24 million units per day) for 10 days. | Three months after therapy: Neurological examination was normal; left hemi-ataxia resolved | [52] | |
| 49 | Dorsal midbrain syndrome, cognitive dysfunction, and a left peripheral seventh nerve palsy | no | “Intravenous penicillin” | [53] | |
| 50 | Right eye vision suddenly became “totally black,” cleared totally within 10–12 s; edema of the right optic nerve with dilated vessels on its surface and a bit of hemorrhage around the papilla; less than one month later: transient obscurations in the right eye, floaters in the left eye, photophobic, and persistent blurring left eye | no | IV penicillin G (20 million U/day) for 10 days | Transient obscurations stopped completely during hospital stay; after five months: right optic disc appeared notably improved; blind spot sizes within normal limits in both eyes; iritis and vitritis of left eye improved | [54] |
| # of Case | Histology | CSF | Neuroimaging | Ref. |
|---|---|---|---|---|
| 1 | Focal chronic dural inflammation and a reactive neocortex with chronic inflammation and rare spirochetes. | MRI: cerebral edema of the frontoparietal lobes; nodular contrast enhancement (T1). | [9] | |
| 2 | Large quantity of inflammatory cell infiltration containing lymphocytes, neutrophils, and necrosis. | Routine examination, biochemical indexes: normal; TPPA: positive. | Edema around the lesion in MRI and CT. CT: low-density lesion; homogeneous enhancement with contrast. MRI: isointensity on T1; long T2 nodular signal shadow; somewhat higher T2-FLAIR signal; high signal in diffusion-weighted imaging. | [10] |
| 3 | Initial Warthin–Starry staining for spirochetes, Ziehl–Neelsen staining for atypical bacteria, and periodic acid-Schiff staining for fungi were negative; retrospective immunoperoxidase stains returned positive and revealed scattered spirochetes. | MRI: lobulated contrast enhancing intramedullary mass at level T10. | [11] | |
| 4 | White blood cells: 84 cells/mL; total protein level: 2.08 g/L; glucose level: 2.95 mmol/L; TRUST: positive (1:4). | MRI: multiple dural-based enhancing masses; irregular ring-enhancing lesion, central hypointense surrounding edema; enhanced nodules: homogeneous-enhancing or ring-enhancing. | [12] | |
| 5 | Cell count: 199/mL; glucose: 61 mg/dL; protein: 116 mg/dL; positive TPHA and FTA-ABS—immunoglobulin G. | MRI: multiple mass lesions, enhanced and adjacent to the dura, left cerebral hemisphere. | [13] | |
| 6 | Granulomatous inflammation with small areas of caseous necrosis, multinucleated giant cells infiltration, surrounded by large numbers of lymphocytes and small numbers of neutrophils; swelling and hyperplasia of some vascular endothelial cells with massive infiltration of lymphocytes and plasma cells around the blood vessels; immunohistochemistry: immunopositivity with glial fibrillary acidic protein, myelin basic protein, neurofilament protein, CD3, CD45RO, and CD68, but was negative for periodic acid-Schiff and CD56; acid-fast staining: negative; further Warthin–Starry staining confirmed spirochetes. | MRI: irregular nodule at T8 level intradural–extramedullary and intramedullary, slightly hyperintense (T1), heterogeneously hyperintense signal (T2), significantly and homogeneously enhanced with contrast. | [14] | |
| 7 | Protein: 97.3 mg/dL; white blood cells: 84 × 106/L; RPR: positive; TPPA: positive. | MRI: slightly abnormal lamellar and longer T1, T2 signal shadow; contrast enhancement: lesion patchy enhancement, adjacent meninges slightly thickened and enhanced. | [15] | |
| 8 | HE staining: necrotic with infiltration of inflammatory cells, glial proliferation in the periphery; GFAP staining: small amount of glial proliferation around necrotic foci; Ki67 staining: higher proliferative activity around the necrotic lesions; P53 staining: negative peripheral P53. | MRI: slightly long T1 and a long T2 nodular signal shadow left cerebral falx, slightly high T2- FLAIR and DWI signal; edema. CT: low-density-area left frontal lobe, ventricular compression. | [15] | |
| 9 | Argyrophilic staining: negative; HE staining: necrotic with infiltration of inflammatory cells, glial proliferation in the periphery; GFAP staining: small amount of glial proliferation around necrotic foci; Ki67 staining: higher proliferative activity around the necrotic lesions; P53 staining: negative peripheral P53. | TPPA: positive; RPR: positive. | MRI: irregular clumping, high-signal mixed with low-signal foci frontal lobe, unclear border, surrounded by a large, low-signal shadow, ventricle re-compressed. | [15] |
| 10 | Immunohistochemical staining revealed numerous spirochetes. | 2.2-fold higher RPR levels. | Contrast-enhanced T1-weighted, fluid-attenuated inversion recovery image reveal ring-enhanced lesion with substantial edema. | [16] |
| 11 | Nonspecific inflammatory granuloma with central necrosis; T. pallidum immunohistochemical stain: clearly stained as helical-shaped in the granuloma specimen (two different T. pallidum-specific PCR (targeting polA and TpN47) for homogenized specimens were positive; T. pallidum DNA was identified. | Cells: 12/mm3; glucose: 98 mg/dL; protein: 90 mg/dL; TPLA: negative; RPR: negative. | MRI: nodule with ring enhancement; high-intensity area in T2; SPECT: weak uptake both in early and late phase; high retention index of 0.86. | [17] |
| 12 | 142 cells/µL (96% lymphocytes); glucose: 60 mg/dL; total protein: 64 mg/dL; RPR titer: 1:2.4; Treponema pallidum latex agglutination titer: 1:53.4.; fluorescent treponemal antibody absorption: 2+ positive. | MRI: nodulus-enhanced temporal on T1, hyperintense on T2; enhanced vestibulo-cochlear nerve and facial nerve T1. | [18] | |
| 13 | Fluorescent treponemal antibody absorption: increased (1:514.5). | MRI: enhancing mass; iso to slightly hyperintense lesion (T1). CT: iso-attenuating lesion; mild enhancement, surrounding edema; hypointense with surrounding edema (T2*); hypointensity at cortex with surrounding hyperintensity (DWI; postcontrast T1: heterogeneous enhancement). CT perfusion: no increase in cerebral blood volume. | [19] | |
| 14 | Degenerative necrotic tissues and fibrous connective tissues with occasional perivascular infiltration by lymphocytes. | MRI: narrowing of the disc space at L4–5, mass behind vertebral body. CT: “Extensive wormy appearance”. | [20] | |
| 15 | Severe inflammation and putrescence formation with a large quantity of inflammatory cell infiltration (mainly of the lymphocytes and plasma cells). | RPR and Treponema pallidum particle agglutination test: positive; RPR titer: 1:8. | MRI: irregular-enhancing lesion with extensive edema. CT: lesion frontal lobe with severe edema. | [21] |
| 16 | 50 cells/µL (80% lymphocytes, 20% monocytes); total protein level: 0.29 g/L; chloride concentration: 126.1 mmol/L; RPR + VDRL: negative. | MRI: hyperintense gadolinium-enhanced T1-weighted regions in the brainstem. | [22] | |
| 17 | MRI: enhancement of the left optic nerve. | [23] | ||
| 18 | Severe inflammation; putrescence and abscess formation; large quantity of inflammatory cell infiltration (mainly of the plasma cells); Warthin–Starry staining: no spirochetes. | Protein level: 0.72 g/L; RPR: negative; TPPA: positive; Spirochetes: not detected. | MRI: mass lesion. | [24] |
| 19 | Granuloma with fibrous hyperplasia; large quantities of inflammatory cell infiltration; immunohistochemistry positive for GFAP, MBP, NF, CD3, and CD45RO; CD68 immunonegative: PAS and CD56; acid-fast staining: negative; Warthin–Starry staining: spirochete-positive. | VDRL: 1:16 dilution; TPPA assay: positive; very few cells; protein: 29 mg/dL; glucose: 57 mg/dL. | MRI: intramedullary nodule; isointense (T1); hyperintense with isointense center, perilesional oedema (T2); lesion enhanced after contrast. | [25] |
| 20 | Leukocyte count: 35 cells/mL (2 neutrophils/mL, 33 lymphocytes/mL); total protein level: 30 mg/dL; glucose: 59 mg/dL; RPR titer: 1:<1; TPHA titer: 1:160; fluorescent treponemal antibody absorption titer: 1:32. | CT: hypodense lesion. MRI: hypointense lesion by gadolinium-enhanced (T1), hyperintense (T2); extensive edema. | [26] | |
| 21 | Necrotic area (star) with extensive peripheral granulomatous tissue (arrowhead). | Two lesions. MRI: low-signal (T1); ring-shaped enhancement and blurry borders (contrast enhanced); diffuse high-signal lesion (edema), low-signal, high-signal border (T2). CT: hypointense lesion, moderate edema. | [27] | |
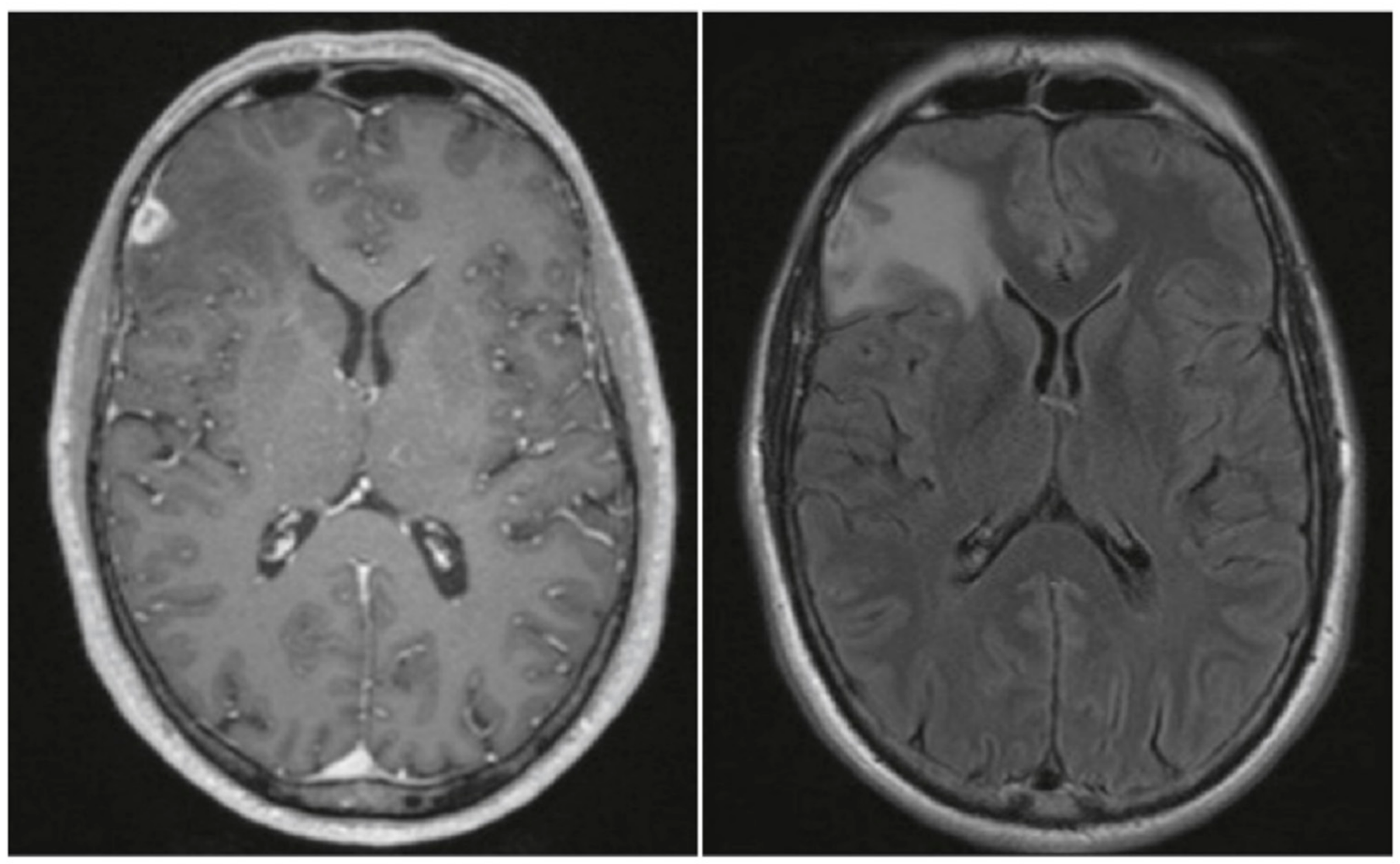
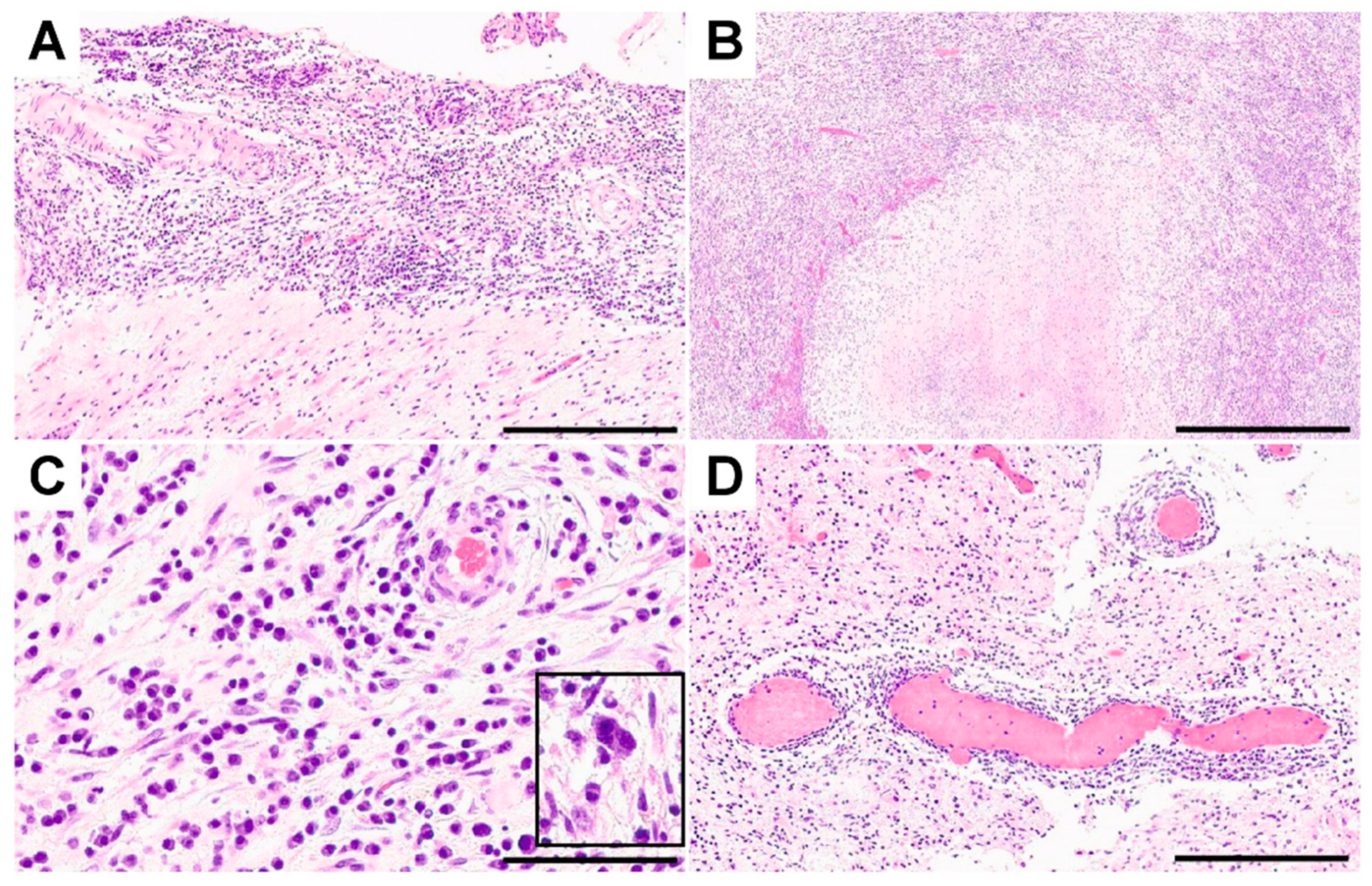
| 22 | Immunohistochemical stains: Toxoplasma spp.- and T. pallidum-negative; staining with antibodies to GFAP, p53, and IDH1-R132H negative. | Contrast-enhancing lesion with perifocal edema, contrast enhancement. | This case | |
| 23 | Epithelioid cell macrophages and plasma cells without evidence of a pathogen. | TPHA: CSF/serum index negative. | MRI: mass lesion. | [28] |
| 24 | Chronic inflammation; Warthin–Starry: no spirochetes; necrotic material infiltrated predominantly with plasma cells; peri-vascular region with fibrosis contained lymphocytes and plasma cells; parenchymal infiltration of lymphocytes and plasma cells in the gumma. | White cells: 0/dL; erythrocytes: 1/mm2; glucose: 74 mg/dL; protein: 16.8 mg/dL; VDRL test: negative; T. pallidum (PCR): negative; FTA-ABS IgG: reactive. | MRI: irregular-enhancing mass, central necrosis; edema. CT: mass-like lesion; severe swelling. | [29] |
| 25 | Vascular intimal hyperplasia and large quantities of inflammatory cell infiltration; Warthin–Starry stain: T. pallidum-positive. | Protein: 0.468 g/L; chloride: 133.2 mmol/L; glucose: “normal”; lactate: “normal”; “no demonstrable T. pallidum” | MRI: irregular nodulus; hypointense (T1); hyperintense (T2) with meningeal thickening; edema. Contrast: enhancing ring. | [30] |
| 26 | “Aseptic meningitis” (lymphocytic pleocytosis, elevated protein, and normal glucose levels) | MRI: Pontine lesion; isointense to gray matter (T1WI); hyperintense on (T2WI and flair); no contrast enhancement. | [31] | |
| 27 | VDRL: positive; FTA: positive; Ziehl–Neelsen stain: positive; protein: 0.37 g/L; glucose: 4.0 mmol/L; polymorphonuclear cells: 0 cells/mm3; lymphocytes: 8 cells/mm3; erythrocytes: 6 cells/mm3. | MRI: Left sphenoid wing dural-based enhancing mass. | [32] | |
| 28 | Non-monoclonal, perivascular inflammatory infiltrates; no viral inclusions, granuloma or inclusions. | White blood cells: 18; red blood cells: 350; VDRL: positive. | MRI: lesions with isointense signaling (T1); surrounding increased signal and mass effect (T2); CT (with contrast): homogeneously enhancing lesions. | [33] |
| 29 | Central portion of the mass: necrotic material infiltrated with eosinophils; peripheral portion: fibrotic0contained lymphocytes and plasma cells; Warthin–Starry staining: spirochete-positive. | Red blood cells: 0 cells/mm3; white blood cells: 3 cells/mm3; glucose: 65 mg/dL; protein level: 47.0 mg/dL; VDRL, FTA-ABS; IgG: positive. | MRI: mass with an ill-defined margin, accompanied with severe swelling; central portion hypointense, peripheral isointense (T1); central portion hyperintense, peripheral portion isointense (T2); enhancement peripheral portion; no enhancement in the central portion (T1 contrast); high-signal intensity in the central portion (DWI). | [34] |
| 30 | Atypical polymorphic inflammatory infiltrate with intralesional spirochetes; fluorescein immunostaining: consistent with syphilitic gumma. | Glucose, protein, and cell counts: “Normal”; VDRL: nonreactive. | MRI: Isodense lesion (T1); isointense, extensive perilesional edema (T2); enhanced uniformly in contrast. | [35] |
| 31 | Granulomatosis with inflammatory infiltration; reactional gliosis, especially in the perivascular space; Ziehl–Nielsen and Groccot staining: negative; T. pallidum: positive. | White blood cells: 2/mm3; protein: 26 mg/dL; glucose: 69 mg/dL; VDRL: negative. | MRI: lesion enhanced in contrast. | [36] |
| 32 | Intense lymphoproliferative infiltrates of plasma cells, T lymphocytes, and B-cell infiltrates; PCR: positive for T. pallidum; Warthin–Starry stain: positive spirochaetes. | VDRL: reactive. | CT: left frontal lobe mass. | [37] |
| 33 | Necrotizing inflammatory mass, intense granulation; layered appearance: outer layer of reactive glial tissue, middle layer of granulation tissue containing lymphocytes, neutrophils, and plasma cells, and inner layer of necrosis; PCR: T. pallidum positive. | Aseptic meningitis with mononuclear pleocytosis; elevated protein with a low glucose CSF/serum ratio; RPR: positive. | MRI and CT: irregularly enhancing lesion with a central hypointense area, extensive surrounding edema. | [38] |
| 34 | “Normal cytology, glucose, and protein levels”; polymerase chain reactions for herpes simplex, cytomegalovirus, HHV6, and enteroviruses: negative; anti-treponemal antibodies: positive; VDRL: positive. | MRI: cortical lesion, isointense (T1, T2, fluid-attenuated inversion); edema; nodular and meningeal enhancement (contrast); restricted diffusion modulus and meningeal-based tail (DWI). | [39] | |
| 35 | Syphilitic gumma on postmortem neuropathologic examination: well-defined, round, rubbery, gray-tan, 4 cm maximal diameter mass, with adjoining diffuse edema; diffuse thickening of leptomeninges and infiltration with lymphocytes and plasma cells peri-vascularly, and histiocytes within leptomeninges; Warthin–Starry and modified Steiner stain did not demonstrate treponemas. | CT: without contrast left middle cerebral artery infarct, with edema and mass effect. | [40] | |
| 36 | White blood cell count: 1010/µL (64% polymorphonuclear leukocytes); hypoglycorrhachia: 16 mg/dL; protein level: 0.17 g/dL; lactate level: 50 mg/dL; IgG index: 1.27; 16 oligoclonal bands; anti-treponemal antibodies: positive; VDRL: positive. | MRI: vasogenic edema; enhancement of gumma (contrast), edema. | [41] | |
| 37 | Necrotic areas with extensive mixed inflammation, consisting of lymphocytes, plasma cells, neutrophils, and focal collagen deposits; inflammation was also present in several midsized arteries, with extensive infiltration by macrophages and severe narrowing of the lumens. | MRI: heterogeneous enhancement of partially cystic midline butterfly-shaped intra- and extra-axial mass; edema; butterfly midline lesion with mild surrounding edema (postcontrast T1); necrotic regions within the lesion and surrounding inflammation and edema (FLAIR); no hyperintensity in the lesion (DWI). CT: heterogeneous perifalcine mass extending from the corpus callosum bilaterally into the subcortical regions of the frontal lobes with considerable mass effect. | [42] | |
| 38 | 26 cells/mm3 (94% lymphocytes); protein level: 106 mg/dL; glucose level: 65 mg/dL; VDRL and FTA-ABS: reactive. | MRI: contrast-enhancing lesions. | [43] | |
| 39 | Non-specific encephalitis. | Autopsy: rich lymphocytes and plasma cells around blood vessels at the border of the gummas. | CT: three-ringed space-occupying lesions, surrounding edema. | [44] |
| 40 | Granulomatous inflammation; necrosis, fibrosis, and infiltration of a large number of lymphocytes and plasma cells. | TPHA: positive. | MRI: hypointense lesion (T1, T2), and strongly enhanced (contrast). CT: irregular low-density, ring-like enhancement (contrast). | [45] |
| 41 | Protein level: 117 mg/dL; glucose level: 69 mg/dL; white blood cells: 11 per mm3 (82% lymphocytes and 18% polymorphonuclear cells); VDRL: positive. | MRI: “abnormal signal” (T2); multifocal contrast enhancement. | [46] | |
| 42 | Necrotic center, surrounded by a layer of granulation tissue infiltrated with proliferating fibroblasts, variable numbers of lymphocytes, macrophages, and histiocytes, and many newly formed small blood vessels; perivascular lymphocytes and histiocytes. | CT: Small ring-like enhanced mass with a surrounding low-density area. MRI: low-signal-intensity basal ganglia (T1); small ring-like enhancement in the vicinity of the right optic nerve (contrast); high-signal intensity surrounding the lesion (T2). | [47] | |
| 43 | Epithelioid granuloma; central caseating necrosis, plasma cell infiltration; destruction of the tunica media of small arteries embedded in the lesion. | TPHA: positive. | CT: ambiguous hypodense lesions; oval homogeneously contrast-enhanced mass lesion attached to the dura mater right temporal. MRI: low-intensity lesions in right cerebellar hemisphere, right middle cerebellar peduncle, and right temporal lobe (T1); and high intensity in T2, homogeneously enhanced (contrast). | [48] |
| 44 | Postmortem: lesions with rubbery greenish core, surrounded by darker area; necrosis with marked inflammatory exudate (lymphocytes and plasma); multinucleated giant cells; silver staining with modified Steiner stain: spirochetal forms; PCR of coded specimens: syphilis (confirmed with DNA hybridization). | Three years ago: white blood cells: 4/mm3 (lymphocytes); erythrocytes: 3/mm3; protein level: 140 mg/dL; glucose level: 40 mg/dL; VDRL: negative. Last admission: white blood cells: 12/mm3 (11 lymphocytes); erythrocytes: 0; glucose level: 50 mg/dL; protein level: 178 mg/dL; VDRL: positive. | CT: multiple ring-enhancing lesions, left frontal. | [49] |
| 45 | Protein level: 23 mg/dL; glucose level: 86 mg/dL; leukocytes: 28/mm3; erythrocytes: 2/mm3; VDRL: not recorded. Second CSF sampling after one month: protein level: 82 mg/dL; glucose level: 60 mg/dL; leukocytes: 38/mm3 (99% lymphocytes); VDRL: positive. Third lumbar puncture after five months (after therapy): protein level: 40 mg/dL; glucose level: 55 mg/dL; leukocytes: 13/mm3 (86% lymphocytes); VDRL: positive. | MRI: contrast-enhancing lesions (T1); edema. One month later: CT: substantial resolution of the lesions while the patient was receiving only corticosteroid therapy (contrast). Nine months later: MRI: after treatment with both antibiotics and corticosteroids, demonstrated resolution of the lesions, except for a subtle abnormality in the left midbrain (Tl + contrast). | [50] | |
| 46 | Lymphoplasmacytic infiltrate with extensive perivascular inflammation. | MRI: dural thickening in the area of the lesion. CT: isolated, peripherally located, contrast-enhancing lesion of the brain. | [51] | |
| 47 | CT: isolated, peripherally located, contrast-enhancing lesion of the brain. | [51] | ||
| 48 | “Increased lymphocytes, elevated protein, and decreased glucose.” Second lumbar puncture: FTA-ABS: positive. | MRI: mass; signal intensity isointense to cortex on (T1 + double spin echo); enhanced markedly (T1, contrast). CT: suprasellar enhancing mass. | [52] | |
| 49 | MRI: intense enhancement | [53] | ||
| 50 | Erythrocytes: 6; lymphocytes: 0; glucose level: 41; protein level: 83; culture: negative; VDRL: positive (units are not reported). | MRI: normal. | [54] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barthel, L.; Hetze, S.; Teuber-Hanselmann, S.; Chapot, V.; Sure, U. Syphilitic Gummata in the Central Nervous System: A Narrative Review and Case Report about a Noteworthy Clinical Manifestation. Microorganisms 2021, 9, 906. https://doi.org/10.3390/microorganisms9050906
Barthel L, Hetze S, Teuber-Hanselmann S, Chapot V, Sure U. Syphilitic Gummata in the Central Nervous System: A Narrative Review and Case Report about a Noteworthy Clinical Manifestation. Microorganisms. 2021; 9(5):906. https://doi.org/10.3390/microorganisms9050906
Chicago/Turabian StyleBarthel, Lennart, Susann Hetze, Sarah Teuber-Hanselmann, Valérie Chapot, and Ulrich Sure. 2021. "Syphilitic Gummata in the Central Nervous System: A Narrative Review and Case Report about a Noteworthy Clinical Manifestation" Microorganisms 9, no. 5: 906. https://doi.org/10.3390/microorganisms9050906