
Effects of Cardiac Contractility Modulation Therapy on Right Ventricular Function: An Echocardiographic Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
- -
- HFrEF with a left ventricular ejection fraction < 40%;
- -
- NYHA class II–III;
- -
- QRS duration < 120 ms.
- -
- The following exclusion criteria were used:
- -
- Acute coronary syndrome in the previous three month;
- -
- Non-optimal medical therapy with disease modifier drugs for HFrEF.
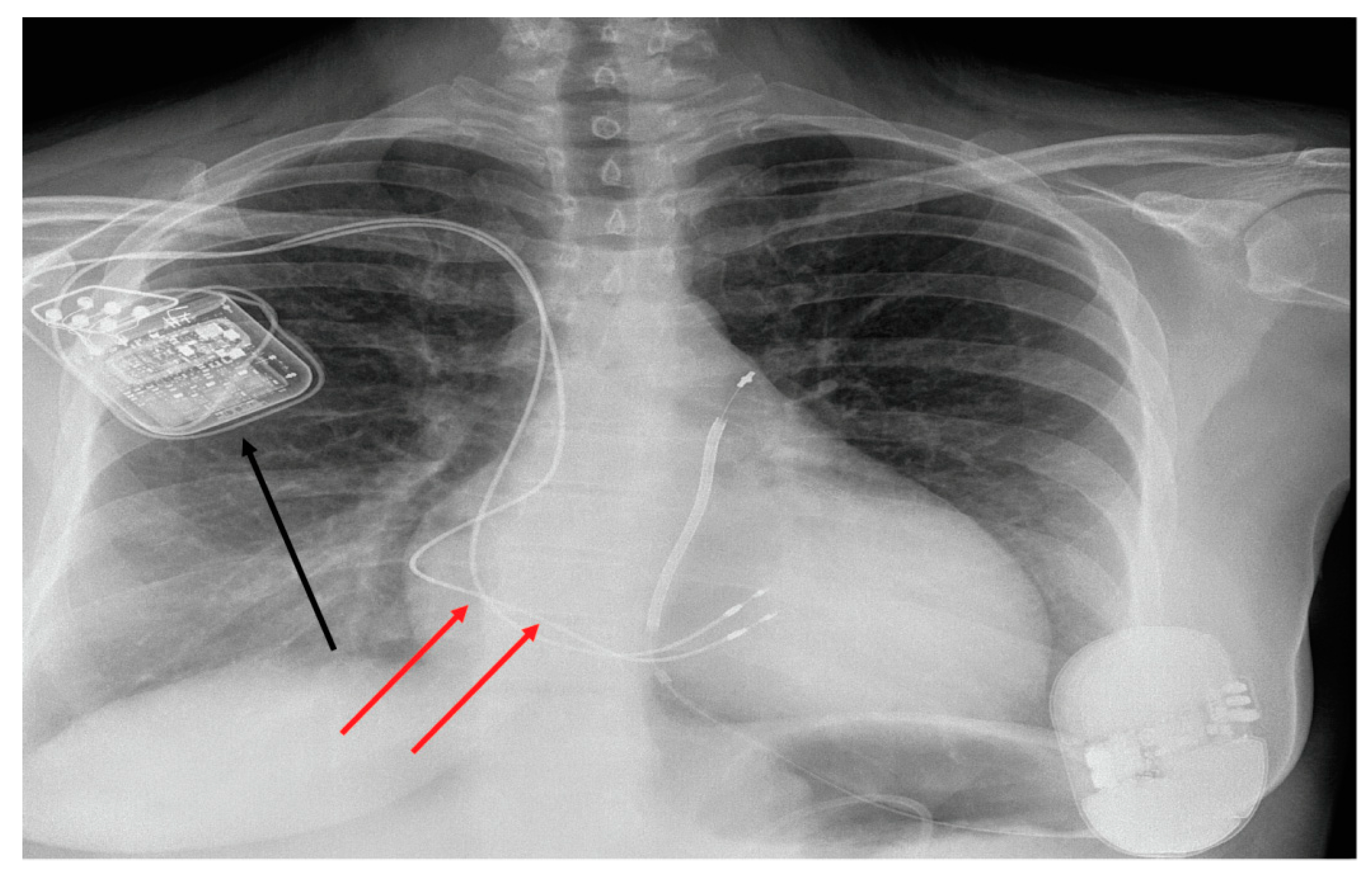
2.2. Optimizer Smart Implant
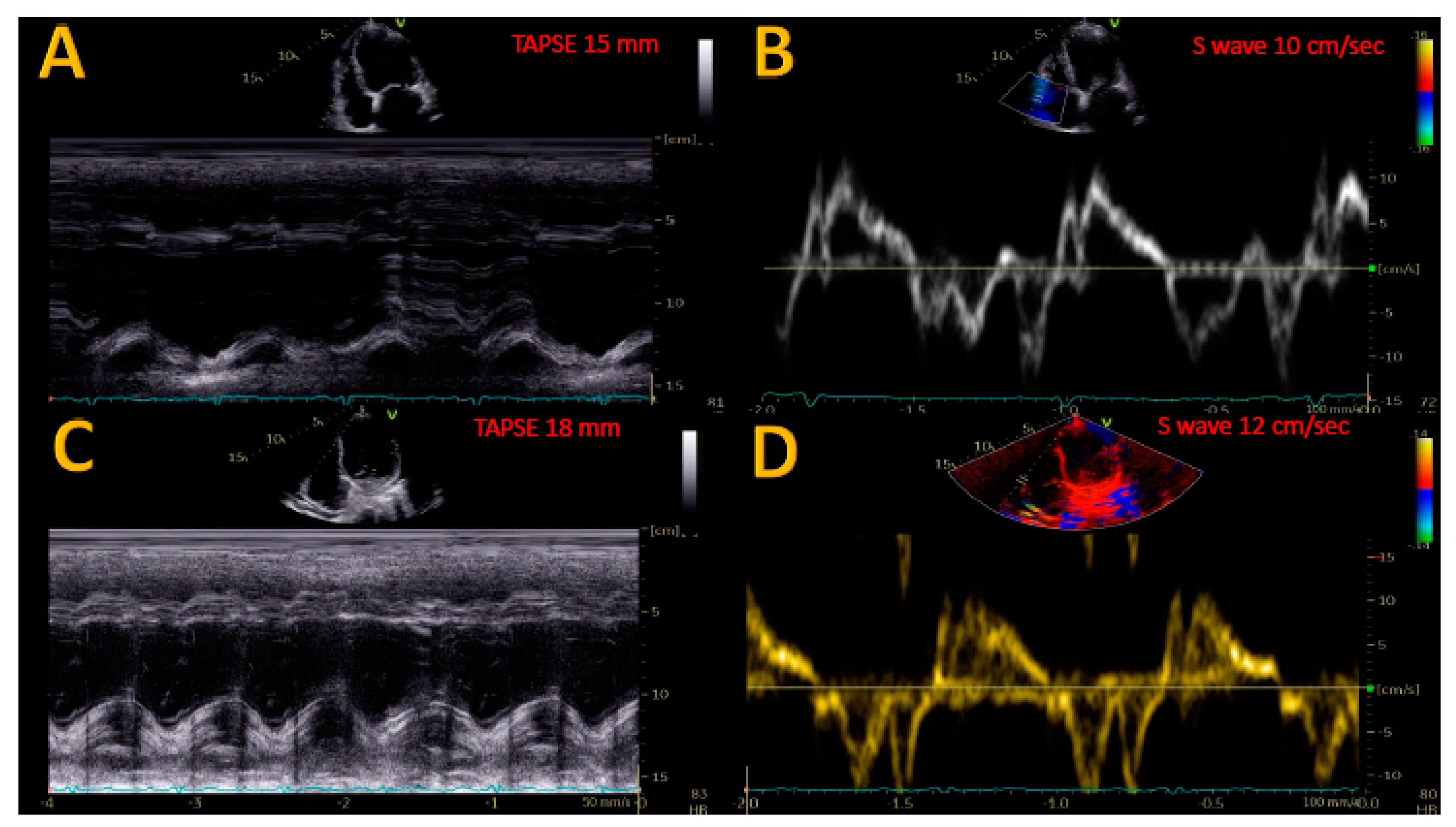
2.3. Echocardiographic Evaluation
2.4. Statistical Analysis
3. Results
3.1. Effects of CCM on RV Reverse Remodeling and Contractility Index
3.2. Effects of CCM on PASP
3.3. Effects of CCM on RV-PA Coupling
4. Discussion
4.1. Improvement of RV Reverse Remodeling Systolic Function after CCM
4.2. Improvement of PASP after CCM
4.3. Improvement of RV-PA Coupling after CCM
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Savarese, G.; Lund, L.H. Global Public Health Burden of Heart Failure. Card. Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics-2018 Update: A Report from the American Heart Association. Circulation 2018, 137, e67–e492, Erratum in Circulation 2018, 137, e493. [Google Scholar] [CrossRef]
- Komajda, M.; Böhm, M.; Borer, J.S.; Ford, I.; Tavazzi, L.; Pannaux, M.; Swedberg, K. Incremental benefit of drug therapies for chronic heart failure with reduced ejection fraction: A network meta-analysis. Eur. J. Heart Fail. 2018, 20, 1315–1322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moskovitch, J.; Voskoboinik, A. Cardiac resynchronization therapy: A comprehensive review. Minerva Medica 2019, 110, 121–138. [Google Scholar] [CrossRef] [PubMed]
- Abraham, W.T. Cardiac Resynchronization Therapy and Cardiac Contractility Modulation in Patients with Advanced Heart Failure. Heart Fail. Clin. 2021, 17, 599–606. [Google Scholar] [CrossRef]
- Campbell, C.M.; Kahwash, R.; Abraham, W.T. Optimizer Smart in the treatment of moderate-to-severe chronic heart failure. Future Cardiol. 2020, 16, 13–25. [Google Scholar] [CrossRef]
- Lawo, T.; Borggrefe, M.; Butter, C.; Hindricks, G.; Schmidinger, H.; Mika, Y.; Burkhoff, D.; Pappone, C.; Sabbah, H.N. Electrical Signals Applied during the Absolute Refractory Period: An Investigational Treatment for Advanced Heart Failure in Patients with Normal QRS Duration. J. Am. Coll. Cardiol. 2005, 46, 2229–2236. [Google Scholar] [CrossRef] [Green Version]
- Butter, C.; Rastogi, S.; Minden, H.-H.; Meyhöfer, J.; Burkhoff, D.; Sabbah, H.N. Cardiac Contractility Modulation Electrical Signals Improve Myocardial Gene Expression in Patients with Heart Failure. J. Am. Coll. Cardiol. 2008, 51, 1784–1789. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.; Dang, Y.; Li, Y.; Hao, Q.; Li, R.; Qi, X. Cardiac Contractility Modulation Attenuate Myocardial Fibrosis by Inhibiting TGF-β1/Smad3 Signaling Pathway in a Rabbit Model of Chronic Heart Failure. Cell. Physiol. Biochem. 2016, 39, 294–302. [Google Scholar] [CrossRef]
- Lyon, A.R.; Samara, M.A.; Feldman, D.S. Cardiac contractility modulation therapy in advanced systolic heart failure. Nat. Rev. Cardiol. 2013, 10, 584–598, Erratum in Nat. Rev. Cardiol. 2014, 11, 188. [Google Scholar] [CrossRef]
- Cappannoli, L.; Scacciavillani, R.; Rocco, E.; Perna, F.; Narducci, M.L.; Vaccarella, M.; D’Amario, D.; Pelargonio, G.; Massetti, M.; Crea, F.; et al. Cardiac contractility modulation for patient with refractory heart failure: An updated evidence-based review. Heart Fail. Rev. 2021, 26, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1321–1360. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–271, Erratum in Eur. Heart J. Cardiovasc. Imaging 2016, 17, 412. [Google Scholar] [CrossRef] [PubMed]
- Jones, N.; Burns, A.T.; Prior, D.L. Echocardiographic Assessment of the Right Ventricle–State of the Art. Heart Lung Circ. 2019, 28, 1339–1350. [Google Scholar] [CrossRef] [Green Version]
- Santamore, W.P.; Dell’Italia, L.J. Ventricular interdependence: Significant left ventricular contributions to right ventricular systolic function. Prog. Cardiovasc. Dis. 1998, 40, 289–308. [Google Scholar] [CrossRef]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the Echocardiographic Assessment of the Right Heart in Adults: A Report from the American Society of Echocardiography: Endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713. [Google Scholar] [CrossRef]
- Kind, T.; Mauritz, G.-J.; Marcus, J.T.; van de Veerdonk, M.; Westerhof, N.; Vonk-Noordegraaf, A. Right ventricular ejection fraction is better reflected by transverse rather than longitudinal wall motion in pulmonary hypertension. J. Cardiovasc. Magn. Reson. 2010, 12, 35. [Google Scholar] [CrossRef] [Green Version]
- Dandel, M.; Hetzer, R. Echocardiographic strain and strain rate imaging–Clinical applications. Int. J. Cardiol. 2009, 132, 11–24. [Google Scholar] [CrossRef]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600, Erratum in Eur. Heart J. Cardiovasc. Imaging 2018, 19, 830–833. [Google Scholar] [CrossRef]
- Yu, C.-M.; Chan, J.Y.-S.; Zhang, Q.; Yip, G.W.; Lam, Y.-Y.; Chan, A.; Burkhoff, D.; Lee, A.; Fung, J.W.-H. Impact of Cardiac Contractility Modulation on Left Ventricular Global and Regional Function and Remodeling. JACC Cardiovasc. Imaging 2009, 2, 1341–1349. [Google Scholar] [CrossRef] [Green Version]
- Roubertie, F.; Eschalier, R.; Zemmoura, A.; Thambo, J.-B.; Rooryck, C.; Labrousse, L.; Ploux, S.; Ritter, P.; Haïssaguerre, M.; Dos Santos, P.; et al. Cardiac Contractility Modulation in a Model of Repaired Tetralogy of Fallot: A Sheep Model. Pediatr. Cardiol. 2016, 37, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Sanz, J.; Sánchez-Quintana, D.; Bossone, E.; Bogaard, H.J.; Naeije, R. Anatomy, Function, and Dysfunction of the Right Ventricle. J. Am. Coll. Cardiol. 2019, 73, 1463–1482. [Google Scholar] [CrossRef] [PubMed]
- Haddad, F.; Hunt, S.A.; Rosenthal, D.; Murphy, D.J. Right Ventricular Function in Cardiovascular Disease, Part I. Circulation 2008, 117, 1436–1448. [Google Scholar] [CrossRef] [PubMed]
- Yücel, G.; Fastner, C.; Hetjens, S.; Toepel, M.; Schmiel, G.; Yazdani, B.; Husain-Syed, F.; Liebe, V.; Rudic, B.; Akin, I.; et al. Impact of baseline left ventricular ejection fraction on long-term outcomes in cardiac contractility modulation therapy. Pacing Clin. Electrophysiol. 2022, 45, 639–648. [Google Scholar] [CrossRef] [PubMed]
- Visco, V.; Esposito, C.; Manzo, M.; Fiorentino, A.; Galasso, G.; Vecchione, C.; Ciccarelli, M. A Multistep Approach to Deal with Advanced Heart Failure: A Case Report on the Positive Effect of Cardiac Contractility Modulation Therapy on Pulmonary Pressure Measured by CardioMEMS. Front. Cardiovasc. Med. 2022, 9, 874433. [Google Scholar] [CrossRef]
- Guazzi, M.; Bandera, F.; Pelissero, G.; Castelvecchio, S.; Menicanti, L.; Ghio, S.; Temporelli, P.L.; Arena, R. Tricuspid annular plane systolic excursion and pulmonary arterial systolic pressure relationship in heart failure: An index of right ventricular contractile function and prognosis. Am. J. Physiol. Circ. Physiol. 2013, 305, H1373–H1381. [Google Scholar] [CrossRef]
- Guazzi, M.; Dixon, D.; Labate, V.; Beussink-Nelson, L.; Bandera, F.; Cuttica, M.J.; Shah, S.J. RV Contractile Function and its Coupling to Pulmonary Circulation in Heart Failure with Preserved Ejection Fraction. JACC Cardiovasc. Imaging 2017, 10, 1211–1221. [Google Scholar] [CrossRef]
- Amsallem, M.; Boulate, D.; Aymami, M.; Guihaire, J.; Selej, M.; Huo, J.; Denault, A.Y.; McConnell, M.V.; Schnittger, I.; Fadel, E.; et al. Load Adaptability in Patients with Pulmonary Arterial Hypertension. Am. J. Cardiol. 2017, 120, 874–882. [Google Scholar] [CrossRef]
- Topilsky, Y.; Oh, J.K.; Shah, D.K.; Boilson, B.A.; Schirger, J.A.; Kushwaha, S.S.; Pereira, N.L.; Park, S.J. Echocardiographic Predictors of Adverse Outcomes After Continuous Left Ventricular Assist Device Implantation. JACC Cardiovasc. Imaging 2011, 4, 211–222. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overall Population (21) |
|---|---|
| Age (mean ± SD) | 65 ± 12.5 years |
| Female sex (n, %) | 3 (14.2%) |
| Ischemic (n, %) | 12 (57%) |
| Hypertension (n, %) | 10 (47%) |
| Diabetes (n, %) | 7 (33%) |
| COPD (n, %) | 6 (28 %) |
| NYHA class III (n, %) | 13 (62%) |
| NYHA class IV (n, %) | 8 (38%) |
| ICD-DR (n, %) | 16 (71%) |
| S-ICD | 2 (9%) |
| CRT-D | 3 (14%) |
| SBP (mean ± SD) | 108 ± 18 mmHg |
| DBP (mean ± SD) | 65 ± 9 mmHg |
| NT-pro BNP (mean ± SD) | 2665 ± 1298 pg/mL |
| Atrial fibrillation | 7 (33%) |
| LVEDV (mean ± SD) | 224.2 ± 69.8 mL |
| LVESV(mean ± SD) | 154.8 ± 53.6 mL |
| LVEF (mean ± SD) | 30.2 ± 6.1% |
| LAVi | 47.2 ± 7.9 mL/m2 |
| Loop diuretic (n, %) | 14 (66%) |
| Beta-Blockers (n, %) | 21 (100%) |
| ARNI (n %) | 21 (100%) |
| MRA (n, %) | 16 (76%) |
| Drugs | Baseline Dose (Mean ± SD) | Follow-Up Dose (Mean ± SD) | p-Value |
|---|---|---|---|
| Bisoprolol | 7.8 ± 1.9 mg | 7.3 ± 2.1 mg | 0.163 |
| Carvedilol | 40.8 ± 9.8 mg | 43.3 ± 11.4 mg | 0.098 |
| Sacubitril/valsartan | 95.4 ± 58.7 mg | 103.8 ± 62.5 mg | 0.087 |
| Eplerenone | 22.8 ± 12.6 mg | 20.5 ± 10.2 | 0.34 |
| Variable | Baseline | 6 Months Follow Up | p-Value |
|---|---|---|---|
| LVEDV (mL) | 224.2 ± 69.8 | 198.3 ± 45.7 | <0.05 |
| LVESV (mL) | 154.8 ± 53.6 | 122.6 ± 66.3 | <0.05 |
| LVEF (%) | 30.2 ± 6.1 | 35.4 ± 7.3 | <0.05 |
| TAPSE (mm) | 16.6 ± 4.2 | 18.5 ± 3.6 | <0.05 |
| S wave (cm/s) | 10.1 ± 1.8 | 11.3 ± 1.4 | <0.05 |
| PASP (mmHg) | 34.2 ± 9.6 | 28.1 ± 6.9 | <0.05 |
| RVFWLS (%) | −13.7 ± 2.5 | −15.1 ± 2.8 | <0.05 |
| TAPSE/PASP (mm/mmHg) | 0.52 ± 0.22 | 0.66 ± 0.21 | <0.05 |
| RVOT PLAX (mm) | 28.2 ± 3.1 | 27.1 ± 4.2 | 0.062 |
| RVD 1 | 26.8 ± 5.3 | 25.7 ± 4.1 | <0.05 |
| RVD 2 | 28.1 ± 4.3 | 26.2 ± 3.2 | <0.05 |
| TI mild (n, %) | 16 (76%) | 18 (85%) | NA |
| TI moderate (n, %) | 3 (14%) | 2 (9%) | NA |
| TI severe (n, %) | 2 (10%) | 1 (4%) | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Contaldi, C.; De Vivo, S.; Martucci, M.L.; D’Onofrio, A.; Ammendola, E.; Nigro, G.; Errigo, V.; Pacileo, G.; Masarone, D. Effects of Cardiac Contractility Modulation Therapy on Right Ventricular Function: An Echocardiographic Study. Appl. Sci. 2022, 12, 7917. https://doi.org/10.3390/app12157917
Contaldi C, De Vivo S, Martucci ML, D’Onofrio A, Ammendola E, Nigro G, Errigo V, Pacileo G, Masarone D. Effects of Cardiac Contractility Modulation Therapy on Right Ventricular Function: An Echocardiographic Study. Applied Sciences. 2022; 12(15):7917. https://doi.org/10.3390/app12157917
Chicago/Turabian StyleContaldi, Carla, Stefano De Vivo, Maria L. Martucci, Antonio D’Onofrio, Ernesto Ammendola, Gerardo Nigro, Vittoria Errigo, Giuseppe Pacileo, and Daniele Masarone. 2022. "Effects of Cardiac Contractility Modulation Therapy on Right Ventricular Function: An Echocardiographic Study" Applied Sciences 12, no. 15: 7917. https://doi.org/10.3390/app12157917