Association between Gingival Biotype and Facial Typology through Cephalometric Evaluation and Three-Dimensional Facial Scanning


 ,
,  and
and
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Periodontal Assessment and Clinical Procedure
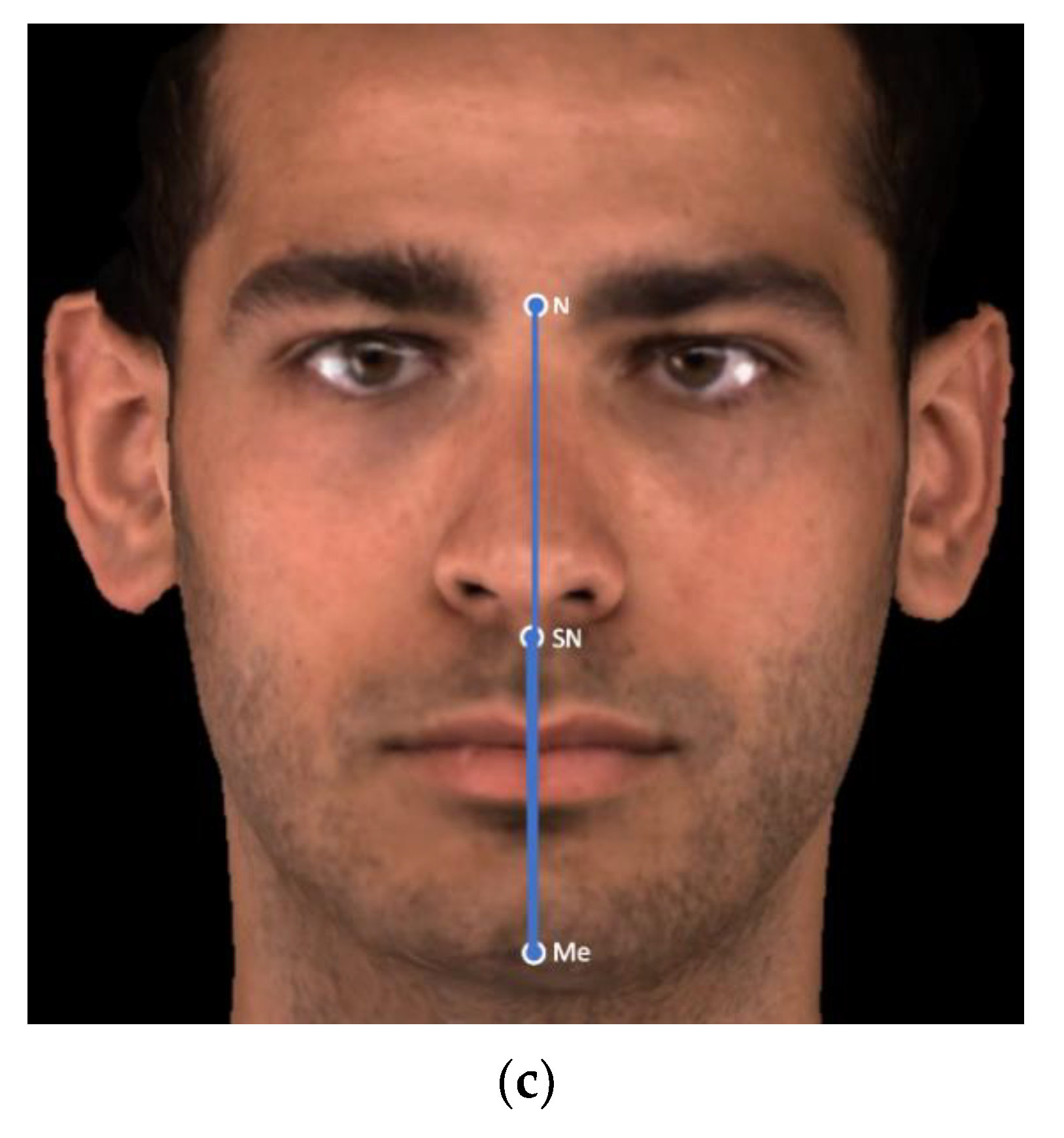
2.3. D Facial Scans Acquisition Process
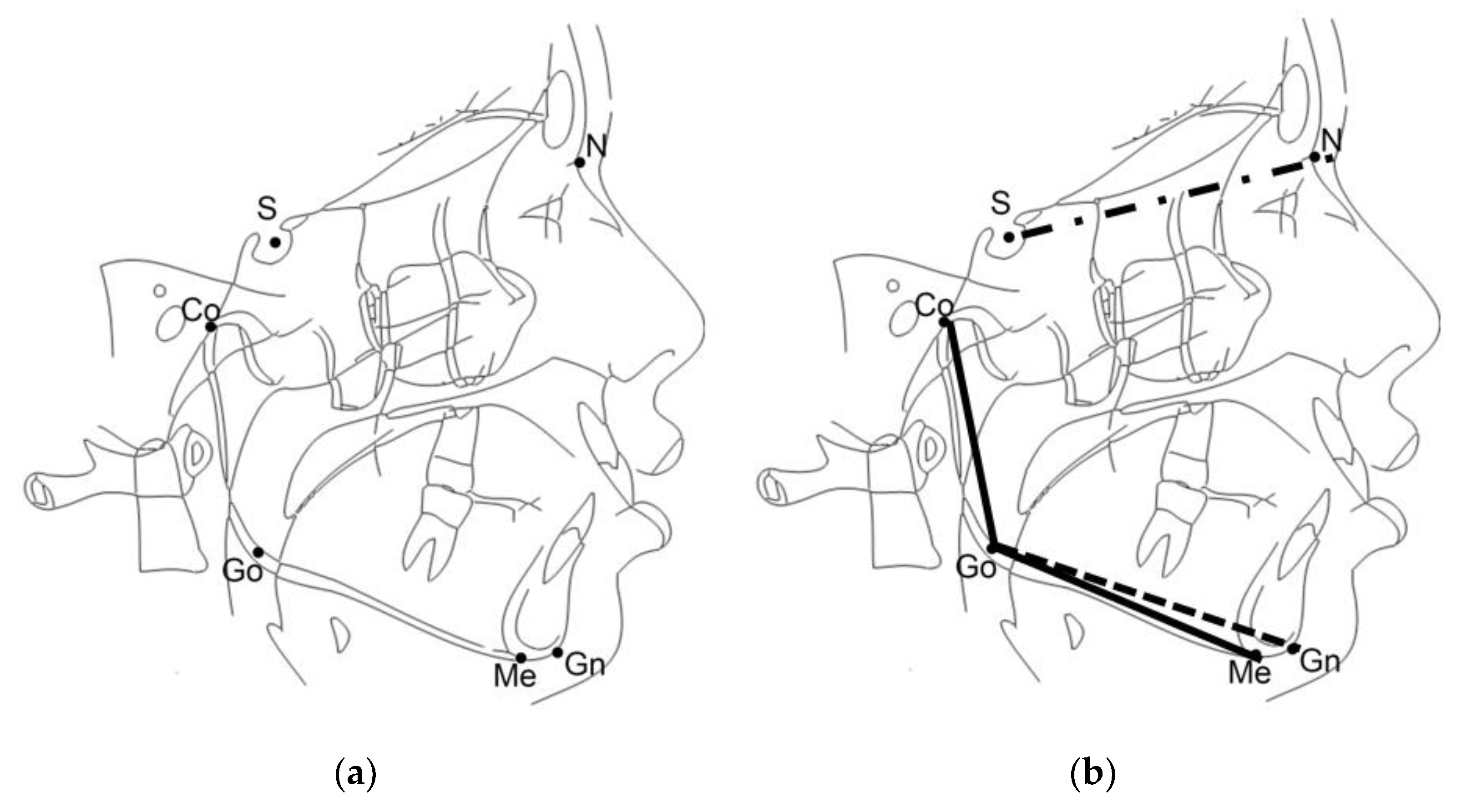
2.4. Facial Typology Assessment with Two-Dimensional and Three-Dimensional Cephalometric Evaluation
2.5. Sample Size
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- There is no association between facial typology (evaluated with SN^GoGn and CoGoMe) and gingival biotype.
- When the ratio of SNMe/NMe is decreased, it represents a protective factor and a minor risk of finding a thin gingival biotype.
Author Contributions
Funding
Conflicts of Interest
References
- Liu, P.; Liu, Y.; Wang, J.; Guo, Y.; Zhang, Y.; Xiao, S. Detection of fusobacterium nucleatum and fada adhesin gene in patients with orthodontic gingivitis and non-orthodontic periodontal inflammation. PLoS ONE 2014, 9, e85280. [Google Scholar] [CrossRef] [PubMed]
- Bollen, A.; Cunha-cruz, J.; Bakko, W.; Huang, G.J.; Hujoel, P.P. The Effects of Orthodontic Therapy on Periodontal Health: A Systematic Review of Controlled Evidence. J. Am. Dent. Assoc. 2008, 139, 413–422. [Google Scholar] [CrossRef] [PubMed]
- Tanner, A.C.R.; Sonis, A.L.; Lif Holgerson, P.; Starr, J.R.; Nunez, Y.; Kressirer, C.A.; Paster, B.J.; Johansson, I. White-spot lesions and gingivitis microbiotas in orthodontic patients. J. Dent. Res. 2012, 91, 853–858. [Google Scholar] [CrossRef] [PubMed]
- Renkema, A.M.; Navratilova, Z.; Mazurova, K.; Katsaros, C.; Fudalej, P.S. Gingival labial recessions and the post-treatment proclination of mandibular incisors. Eur. J. Orthod. 2015, 37, 508–513. [Google Scholar] [CrossRef]
- Renkema, A.M.; Fudalej, P.S.; Renkema, A.A.P.; Abbas, F.; Bronkhorst, E.; Katsaros, C. Gingival labial recessions in orthodontically treated and untreated individuals: A case-Control study. J. Clin. Periodontol. 2013, 40, 631–637. [Google Scholar] [CrossRef]
- Morris, J.W.; Campbell, P.M.; Tadlock, L.P.; Boley, J.; Buschang, P.H. Prevalence of gingival recession after orthodontic tooth movements. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 851–859. [Google Scholar] [CrossRef]
- Kim, D.M.; Neiva, R. Periodontal Soft Tissue Non–Root Coverage Procedures: A Systematic Review From the AAP Regeneration Workshop. J. Periodontol. 2015, 86, S56–S72. [Google Scholar] [CrossRef]
- Joss-Vassalli, I.; Grebenstein, C.; Topouzelis, N.; Sculean, A.; Katsaros, C. Orthodontic therapy and gingival recession: A systematic review. Orthod. C. Res. 2010, 13, 127–141. [Google Scholar] [CrossRef]
- Kois, J.C. Predictable single-tooth peri-implant esthetics: Five diagnostic keys. Compend. Contin. Educ. Dent. 2004, 25, 895–896. [Google Scholar]
- Ahmad, I. Anterior dental aesthetics: Gingival perspective. Br. Dent. J. 2005, 199, 195–202. [Google Scholar] [CrossRef]
- Grover, V.; Bhardwaj, A.; Mohindra, K.; Malhotra, R. Analysis of the gingival biotype based on the measurement of the dentopapillary complex. J. Indian Soc. Periodontol. 2014, 18, 43. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 89, S173–S182. [Google Scholar] [CrossRef] [PubMed]
- Vandana, K.L.; Savitha, B. Thickness of gingiva in association with age, gender and dental arch location. J. Clin. Periodontol. 2005, 32, 828–830. [Google Scholar] [CrossRef] [PubMed]
- Seibert, J.; Lindhe, J. Aestetics and periodontal therapy. In Textbook of Clinical Periodontology, 2nd ed.; Munksgaard: Copenhagen, Denmark, 1989; pp. 477–514. [Google Scholar]
- Olsson, M.; Lindhe, J. Periodontal characteristics in individuals with varying form of the upper central incisors. J. Clin. Periodontol. 1991, 18, 78–82. [Google Scholar] [CrossRef]
- Fields, H.; Proffit, W.; Nixon, W.; Phillips, C.; Stanek, E. Facial pattern differences in long-faced children and adults. Am. J. Orthod. 1984, 85, 217–223. [Google Scholar] [CrossRef]
- Cangialosi, T.J. Additional criteria for sample division suggested. Am. J. Orthod. Dentofac. Orthop. 1989, 96, A24. [Google Scholar] [CrossRef]
- Opdebeeck, H.; Bell, W. The short face syndrome. Am. J. Orthod. 1978, 73, 499–511. [Google Scholar] [CrossRef]
- Schudy, F.F. The Rotation of The Mandible Resulting From Growth: Its Implications In Orthodontic Treatment. Angle Orthod. 1964, 34, 75–93. [Google Scholar]
- Matarese, G.; Isola, G.; Ramaglia, L.; Dalessandri, D.; Lucchese, A.; Alibrandi, A.; Fabiano, F.; Cordasco, G. Periodontal biotype: Characteristc, prevalence and dimension related to dental malocclusion. Minerva Stomatol. 2016, 65, 231–238. [Google Scholar]
- Al-Zo’ubia, I.A.; Hammadb, M.M.; Abu Alhaijac, E.S.J. Periodontal parameters in different dentofacial vertical patterns. Angle Orthod. 2008, 78, 1006–1014. [Google Scholar] [CrossRef]
- Hornera, K.A.; Behrents, R.G.; Beom Kim, K.; Buschangd, P.H. Cortical bone and ridge thickness of hyperdivergent and hypodivergent adults. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Esfahanizadeh, N.; Daneshparvar, N.; Askarpour, F.; Akhoundi, N.; Panjnoush, M. Correlation Between Bone and Soft Tissue Thickness in Maxillary Anterior Teeth. J. Dent. (Tehran) 2016, 13, 302–308. [Google Scholar]
- Sadek, M.M.; Sabet, N.E.; Hassan, I.T. Alveolar bone mapping in subjects with different vertical facial dimensions. Eur. J. Orthod. 2014, 37, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Björk, A. Prediction of mandibular growth rotation. Am. J. Orthod. 1969, 55, 585–599. [Google Scholar] [CrossRef]
- Kaya, Y.; Alkan, Ö.; Alkan, E.A.; Keskin, S. Gingival thicknesses of maxillary and mandibular anterior regions in subjects with different craniofacial morphologies. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Baik, H.S.; Kim, S.Y. Facial soft-tissue changes in skeletal Class III orthognathic surgery patients analyzed with 3-dimensional laser scanning. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Kau, C.H.; Richmond, S.; Incrapera, A.; English, J.; Xia, J.J. Three-dimensional surface acquisition systems for the study of facial morphology and their application to maxillofacial surgery. Int. J. Med. Robot. Comput. Assist. Surg. 2007, 3, 97–110. [Google Scholar] [CrossRef]
- Staderini, E.; Patini, R.; De Luca, M.; Gallenzi, P. Three-dimensional stereophotogrammetric analysis of nasolabial soft tissue effects of rapid maxillary expansion: A systematic review of clinical trials. Acta Otorhinolaryngol. Ital. 2018, 38, 399–408. [Google Scholar]
- Antoun, J.S.; Lawrence, C.; Leow, A.; Rongo, R.; Dias, G.; Farella, M. A three-dimensional evaluation of Māori and New Zealand European faces. Aust. Orthod. J. 2014, 30, 169. [Google Scholar]
- Aynechi, N.; Larson, B.E.; Leon-Salazar, V.; Beiraghi, S. Accuracy and precision of a 3D anthropometric facial analysis with and without landmark labeling before image acquisition. Angle Orthod. 2011, 81, 245–252. [Google Scholar] [CrossRef]
- Plooij, J.M.; Swennen, G.R.J.; Rangel, F.A.; Maal, T.J.J.; Schutyser, F.A.C.; Bronkhorst, E.M.; Kuijpers-Jagtman, A.M.; Bergé, S.J. Evaluation of reproducibility and reliability of 3D soft tissue analysis using 3D stereophotogrammetry. Int. J. Oral Maxillofac. Surg. 2009, 38, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Toma, A.M.; Zhurov, A.; Playle, R.; Ong, E.; Richmond, S. Reproducibility of facial soft tissue landmarks on 3D laser-scanned facial images. Orthod. Craniofac. Res. 2009, 12, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Rongo, R.; Antoun, J.S.; Lim, Y.X.; Dias, G.; Valletta, R.; Farella, M. Three-dimensional evaluation of the relationship between jaw divergence and facial soft tissue dimensions. Angle Orthod. 2014, 84, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Young, N.M.; Sherathiya, K.; Gutierrez, L.; Nguyen, E.; Bekmezian, S.; Huang, J.C.; Hallgrimsson, B.; Lee, J.S.; Marcucio, R.S. Facial surface morphology predicts variation in internal skeletal shape. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 501–508. [Google Scholar] [CrossRef]
- Kan, J.Y.K.; Rungcharassaeng, K.; Umezu, K.; Kois, J.C. Dimensions of Peri-Implant Mucosa: An Evaluation of Maxillary Anterior Single Implants in Humans. J. Periodontol. 2003, 74, 557–562. [Google Scholar] [CrossRef]
- Salti, L.; Holtfreter, B.; Pink, C.; Habes, M.; Biffar, R.; Kiliaridis, S.; Krey, K.F.; Bülow, R.; Völzke, H.; Kocher, T.; et al. Estimating effects of craniofacial morphology on gingival recession and clinical attachment loss. J. Clin. Periodontol. 2017, 44, 363–371. [Google Scholar] [CrossRef]
- Ronay, V.; Sahrmann, P.; Bindl, A.; Attin, T.; Schmidlin, P.R. Current status and perspectives of mucogingival soft tissue measurement methods. J. Esthet. Restor. Dent. 2011, 23, 146–156. [Google Scholar] [CrossRef]
- Eger, T.; Muller, H.-P.; Heinecke, A. Ultrasonic determination of gingival thickness subject variation and influence of tooth type and clinical features. J. Clin. Periodontol. 1996, 23, 839–845. [Google Scholar] [CrossRef]
- De Rouck, T.; Eghbali, R.; Collys, K.; De Bruyn, H.; Cosyn, J. The gingival biotype revisited: Transparency of the periodontal probe through the gingival margin as a method to discriminate thin from thick gingiva. J. Clin. Periodontol. 2009, 36, 428–433. [Google Scholar] [CrossRef]
- Cortellini, P.; Bissada, N.F. Mucogingival conditions in the natural dentition: Narrative review, case definitions, and diagnostic considerations. J. Clin. Periodontol. 2018, 45, S190–S198. [Google Scholar] [CrossRef] [Green Version]
- Müller, H.P.; Könönen, E. Variance components of gingival thickness. J. Periodontal Res. 2005, 40, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Paduano, S.; Rongo, R.; Bucci, R.; Aiello, D.; Carvelli, G.; Ingenito, A.; Cantile, T.; Ferrazzano, G.F. Is there an association between various aspects of oral health in Southern Italy children? An epidemiological study assessing dental decays, periodontal status, malocclusions and temporomandibular joint function. Eur. J. Paediatr. Dent. 2018, 19, 176–180. [Google Scholar] [PubMed]
- Asiri, S.N.; Tadlock, L.P.; Buschang, P.H. The prevalence of clinically meaningful malocclusion among US adults. Orthod. Craniofac. Res. 2019, 22, 321–328. [Google Scholar] [CrossRef]
- Jawad, Z.; Bates, C.; Hodge, T. Who needs orthodontic treatment? Who gets it? And who wants it? Br. Dent. J. 2015, 218, 99–103. [Google Scholar] [CrossRef]
- Alfuriji, S.; Alhazmi, N.; Alhamlan, N.; Al-Ehaideb, A.; Alruwaithi, M.; Alkatheeri, N.; Geevarghese, A. The effect of orthodontic therapy on periodontal health: A review of the literature. Int. J. Dent. 2014, 2014, 585048. [Google Scholar] [CrossRef]
- Maynard, J.G. The rationale for mucogingival therapy in the child and adolescent. Int. J. Periodontics Restor. Dent. 1987, 7, 36–51. [Google Scholar]
- Renkema, A.M.; Fudalej, P.S.; Renkema, A.; Kiekens, R.; Katsaros, C. Development of labial gingival recessions in orthodontically treated patients. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 206–212. [Google Scholar] [CrossRef]
- Holmesa, H.D.; Tennantb, M.; Goonewardenec, M.S. Augmentation of faciolingual gingival dimensions with free connective tissue grafts before labial orthodontic tooth movement: An experimental study with a canine model. Am. J. Orthod. Dentofac. Orthop. 2005, 127, 562–572. [Google Scholar] [CrossRef]
- Wennström, J.L.; Lindhe, J.; Sinclair, F.; Thilander, B. Some periodontal tissue reactions to orthodontic tooth movement in monkeys. J. Clin. Periodontol. 1987, 14, 121–129. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N | Median (IQR) |
|---|---|---|
| Age | 121 | 17.04 (13.7–22.1) |
| Frequency | Percentage (%) | |
| Gender | ||
| Male | 43 | 35.54 |
| Female | 78 | 63.64 |
| Upper Gingival Biotype | ||
| Thick | 105 | 86.78 |
| Thin | 16 | 13.22 |
| Lower Gingival Biotype | ||
| Thick | 63 | 52.07 |
| Thin | 58 | 47.93 |
| Facial Typology SN^GoGn | ||
| Brachyfacial | 33 | 27.27 |
| Mesofacial | 59 | 48.76 |
| Dolichofacial | 29 | 23.97 |
| Variables | Mean ± SD | P50 | P25 | P75 |
|---|---|---|---|---|
| SN^Go-Gn | 32.7° ± 8° | 32.7° | 28.1° | 36.3° |
| CoGoMe^ | 123.2° ± 6.6° | 122.8° | 118.7° | 127.4° |
| SNMe/SMe | 0.514 ± 0.042 | 0.51 | 0.497 | 0.530 |
| Facial Typology (N) | Upper Gingival Biotype | |||
| Thick | Thin | p value | ||
| Brachyfacial (33) | 29 (27.62%) | 4 (25.00%) | 0.83 | |
| Mesofacial (59) | 50 (47.62%) | 9 (56.25%) | ||
| Dolichofacial (29) | 26 (24.76%) | 3 (18.75%) | ||
| Total (121) | 105 (100%) | 16 (100%) | ||
| Lower Gingival Biotype | ||||
| Thick | Thin | p value | ||
| Brachyfacial (33) | 16 (25.40%) | 17 (29.31%) | 0.75 | |
| Mesofacial (59) | 33 (52.38%) | 26 (44.83%) | ||
| Dolichofacial (29) | 14 (22.22%) | 15 (25.86%) | ||
| Total (121) | 63 (100%) | 58 (100%) | ||
| Gingival Biotype | ||||
| Thick/Thick | Thick/Thin | Thin/Thin | p value | |
| Brachyfacial (33) | 16 (25.40%) | 13 (30.95%) | 4 (25%) | 0.77 |
| Mesofacial (59) | 33 (52.38%) | 17 (40.48%) | 9 (56.25%) | |
| Dolichofacial (29) | 14 (22.22%) | 12 (28.57%) | 3 (18.75%) | |
| Total (121) | 63 (100%) | 42 (100%) | 16 (100%) | |
| Model | Variable | p Value | Odds Ratio (OR) | 95% IC |
|---|---|---|---|---|
| Upper biotype (SNMe/NMe) | SNMe/NMe | 0.036 * | 0.843 | 0.719–0.989 |
| Lower biotype (SNMe/NMe) | SNMe/NMe | 0.049 * | 0.904 | 0.818–0.999 |
| Upper biotype (SNMe/NMe × Age) | SNMe/NMe | 0.034 * | 0.839 | 0.714–0.987 |
| Age | 0.620 | 0.985 | 0.927–1.046 | |
| Lower biotype (SNMe/NMe × Age) | SNMe/NMe | 0.048 * | 0.903 | 0.815–0.999 |
| Age | 0.207 | 0.976 | 0.939–1.014 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valletta, R.; Pango, A.; Tortora, G.; Rongo, R.; Simeon, V.; Spagnuolo, G.; D’Antò, V. Association between Gingival Biotype and Facial Typology through Cephalometric Evaluation and Three-Dimensional Facial Scanning. Appl. Sci. 2019, 9, 5057. https://doi.org/10.3390/app9235057
Valletta R, Pango A, Tortora G, Rongo R, Simeon V, Spagnuolo G, D’Antò V. Association between Gingival Biotype and Facial Typology through Cephalometric Evaluation and Three-Dimensional Facial Scanning. Applied Sciences. 2019; 9(23):5057. https://doi.org/10.3390/app9235057
Chicago/Turabian StyleValletta, Rosa, Ada Pango, Gregorio Tortora, Roberto Rongo, Vittorio Simeon, Gianrico Spagnuolo, and Vincenzo D’Antò. 2019. "Association between Gingival Biotype and Facial Typology through Cephalometric Evaluation and Three-Dimensional Facial Scanning" Applied Sciences 9, no. 23: 5057. https://doi.org/10.3390/app9235057