
Disproportionate Vertebral Bodies and Their Impact on Lumbar Disc Herniation


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
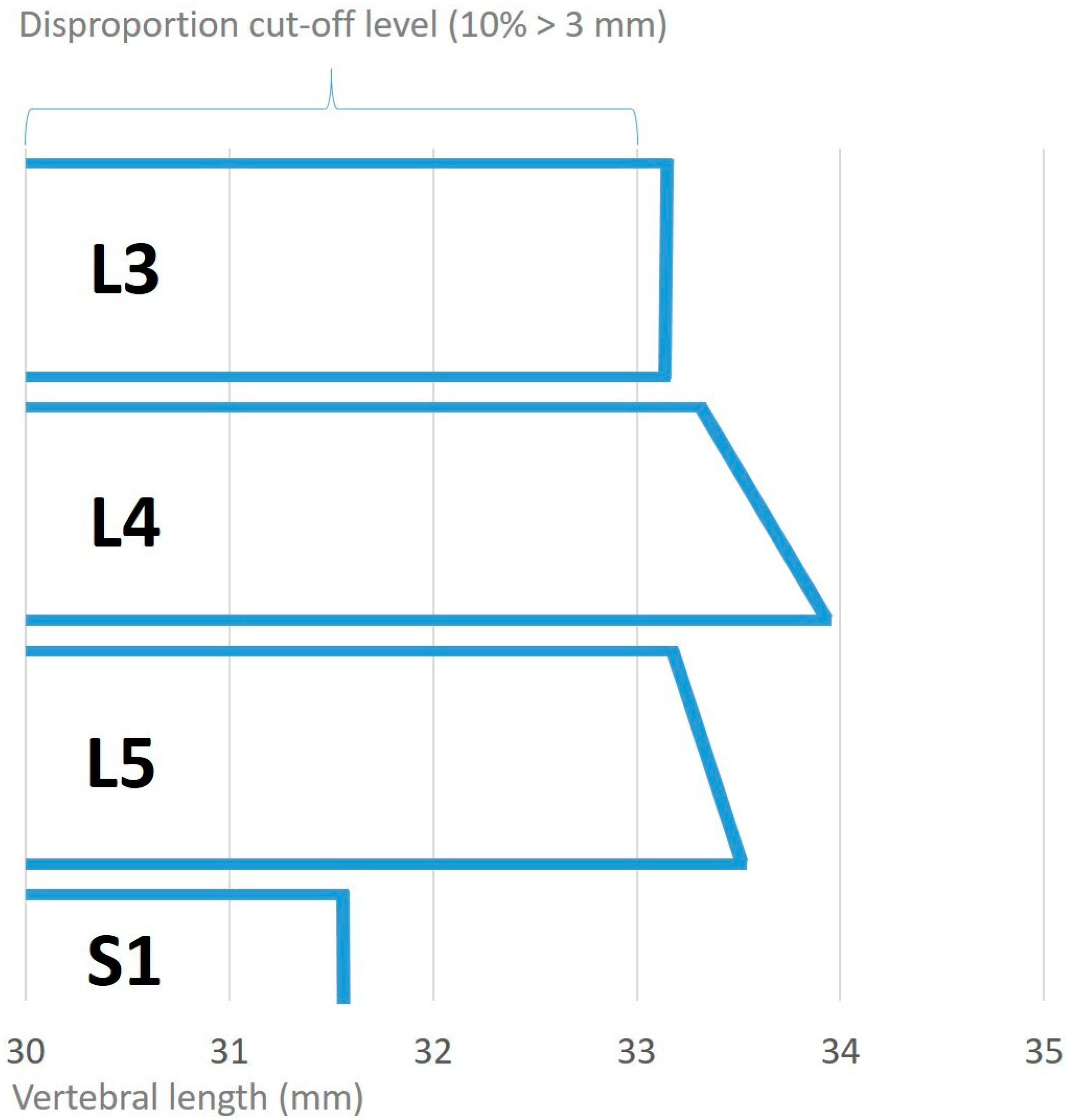
2.2. Definition of DH
2.3. Inclusion and Exclusion Criteria
2.4. Indications for Surgery
2.5. Image Acquisition
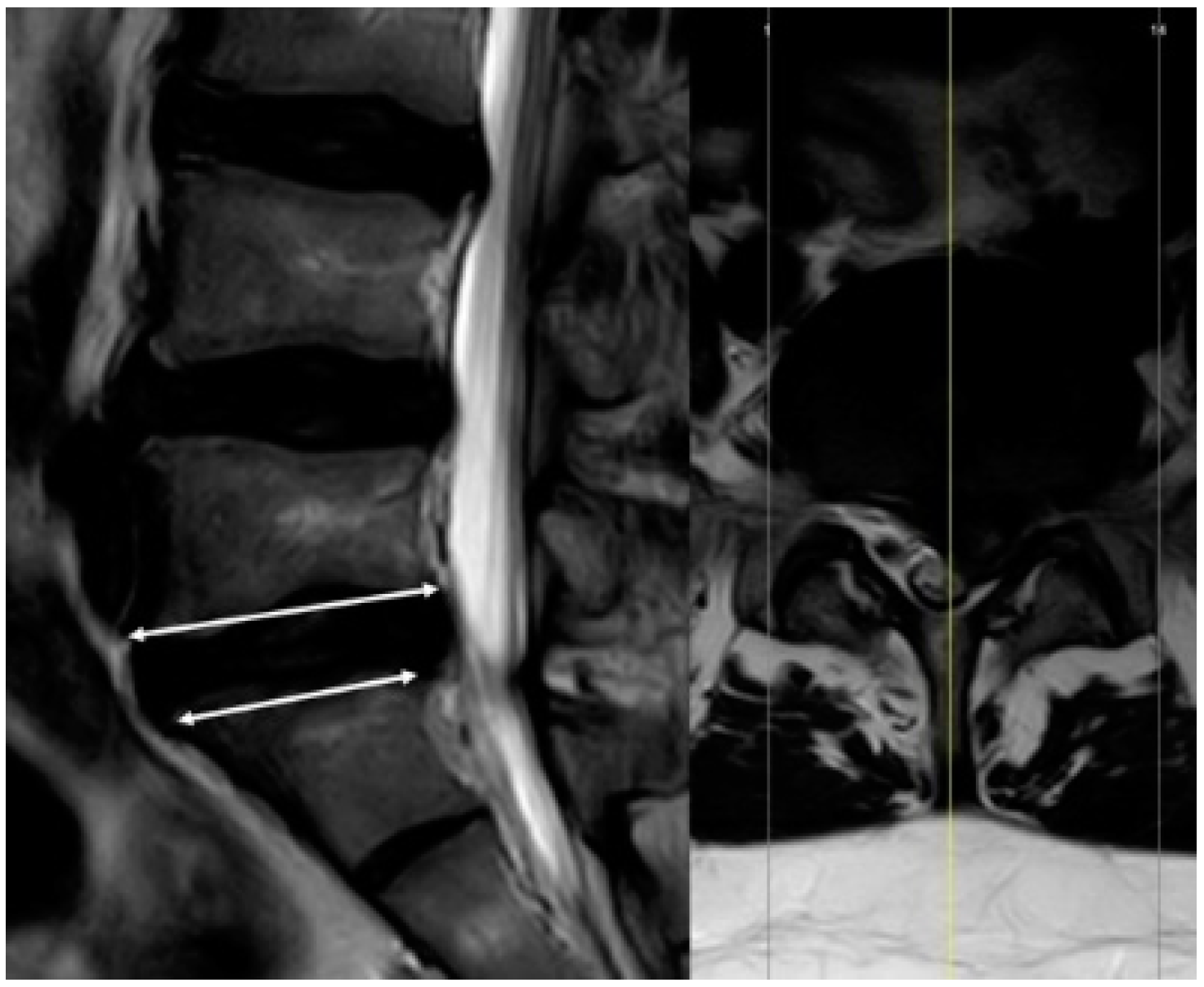
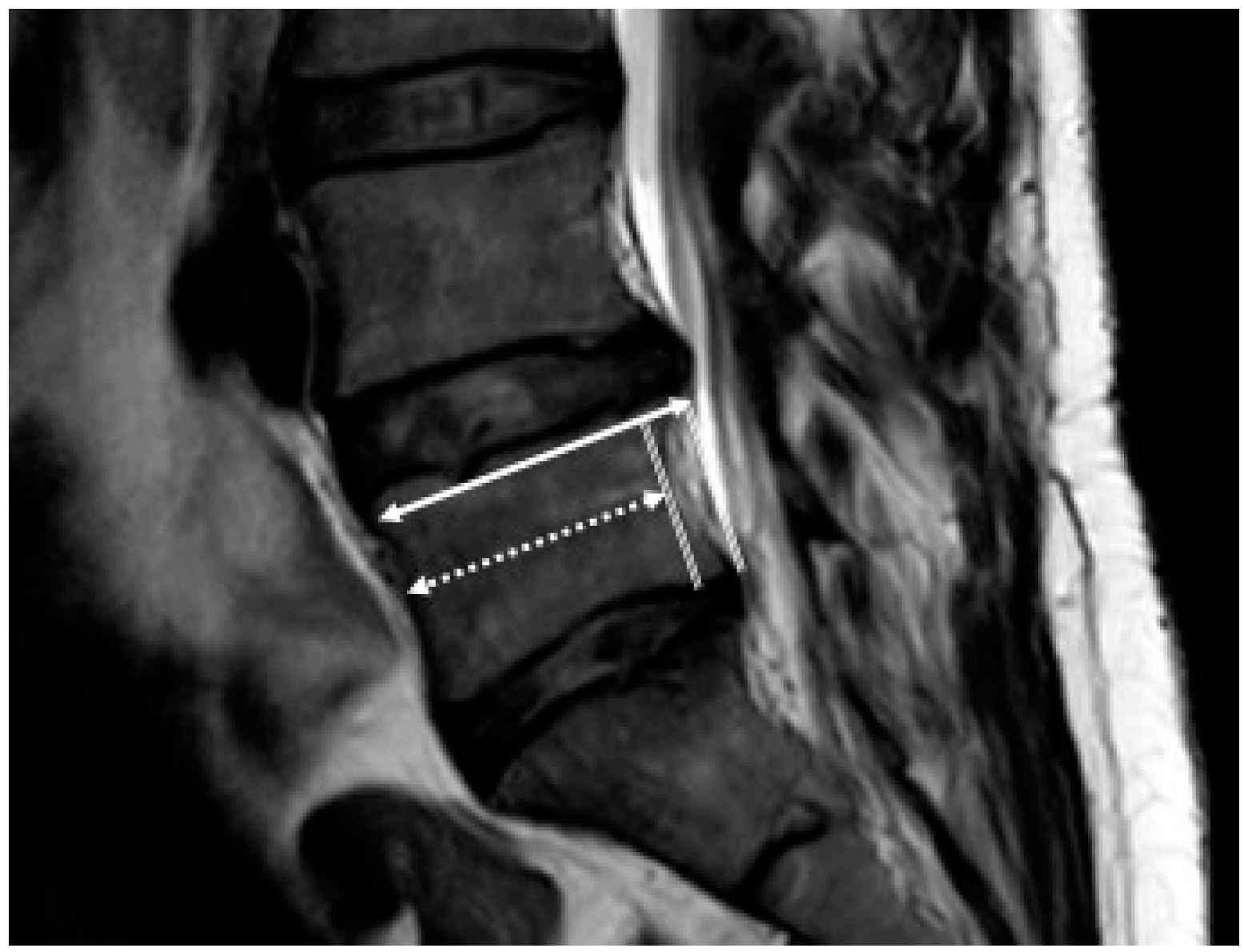
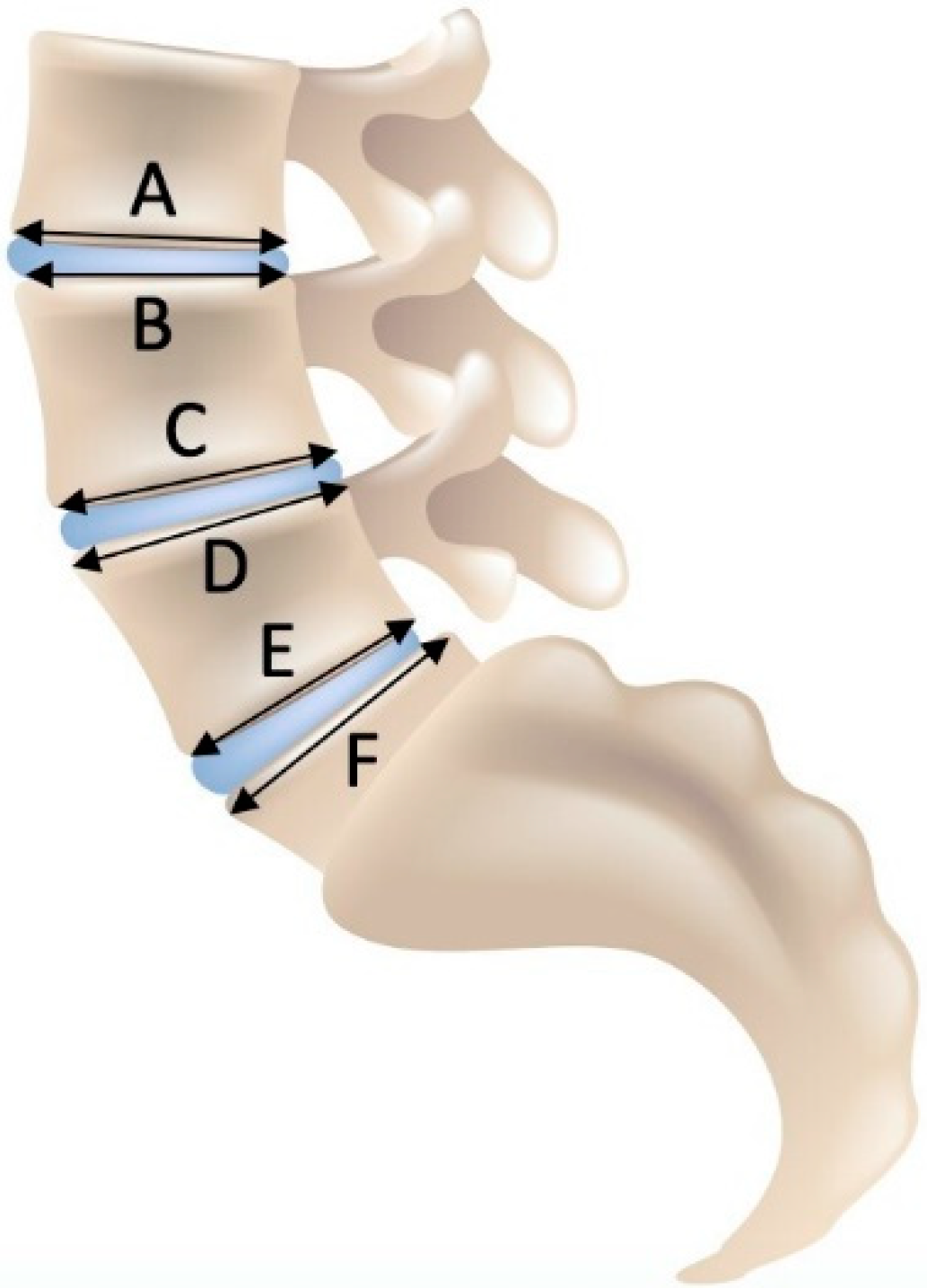
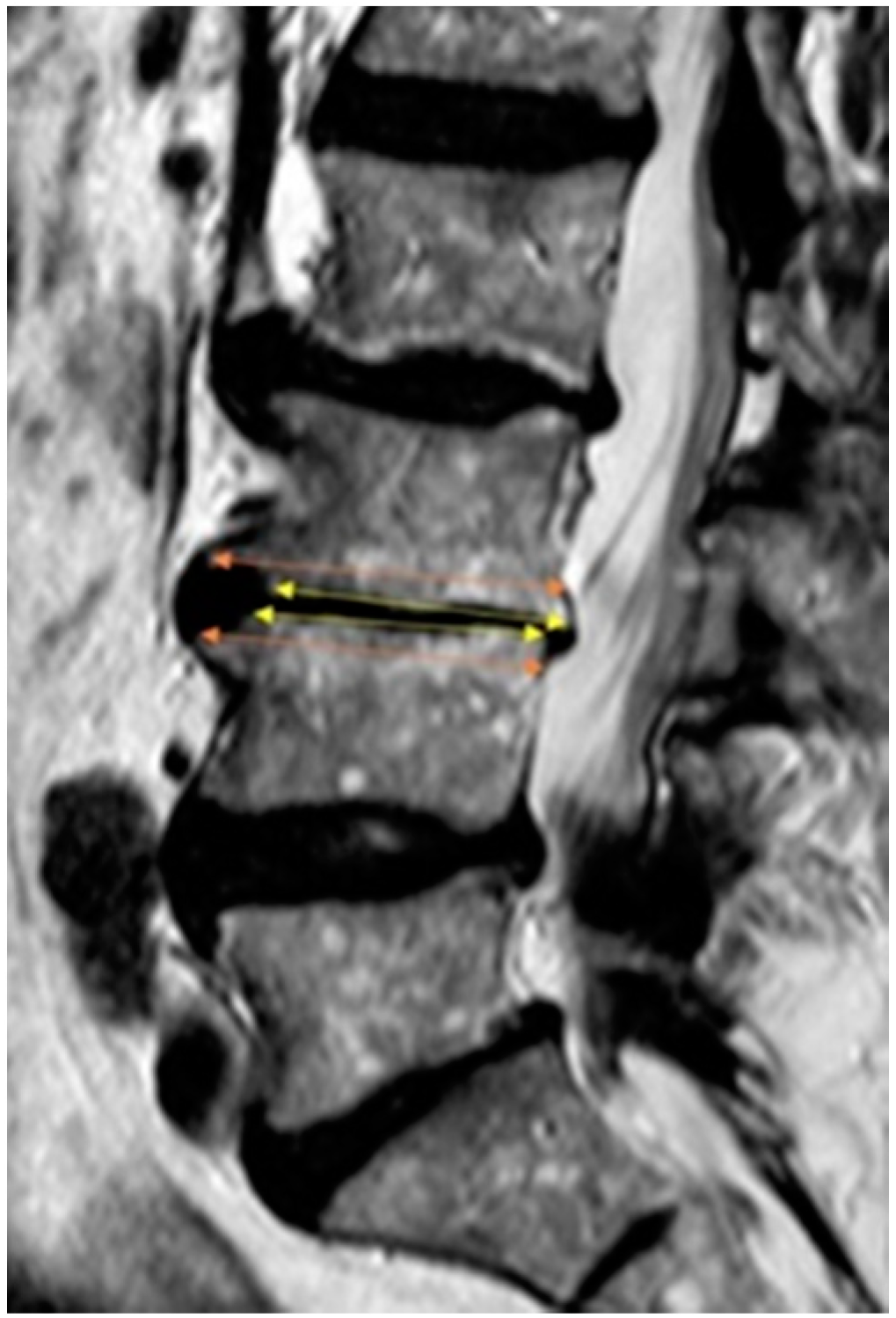
2.6. Measurement
2.7. Theory/Calculations
2.8. Statistical Analysis
3. Results
3.1. Study Population
3.2. Anatomical Results
3.3. Segmental Distribution of DH in the Study Population (67 Discectomies)
3.4. Segmental Distribution of Disproportionate Motion Segments
3.5. Disproportion as a Risk Factor for DH
3.6. Logistic Regression Correlation and ROC Curve between DP and DH
3.7. Disc Sequestration (DS)
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maniadakis, N.; Gray, A. The Economic Burden of Back Pain in the UK. Pain 2000, 84, 95–103. [Google Scholar] [CrossRef]
- Woolf, A.D.; Pfleger, B. Burden of Major Musculoskeletal Conditions. Bull. World Health Organ. 2003, 81, 646–656. [Google Scholar] [PubMed]
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A Systematic Review of The Global Prevalence of Low Back Pain. Arthritis Rheum. 2012, 64, 2028–2037. [Google Scholar] [CrossRef]
- Leven, D.; Passias, P.G.; Errico, T.J.; Lafage, V.; Bianco, K.; Lee, A.; Lurie, J.D.; Tosteson, T.D.; Zhao, W.; Spratt, K.F. Risk Factors for Reoperation in Patients Treated Surgically for Intervertebral Disc Herniation: A Subanalysis of Eight-Year SPORT Data. J. Bone Jt. Surg. Am. 2015, 97, 1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordon, J.; Konstantinou, K.; O’Dowd, J. Herniated Lumbar Disc. BMJ Clin. Evid. 2009, 2009, 1118. [Google Scholar]
- Kushchayev, S.V.; Glushko, T.; Jarraya, M.; Schuleri, K.H.; Preul, M.C.; Brooks, M.L.; Teytelboym, O.M. ABCs of The Degenerative Spine. Insights Imaging 2018, 9, 253–274. [Google Scholar] [CrossRef] [Green Version]
- Modic, M.T.; Ross, J.S. Lumbar Degenerative Disk Disease. Radiology 2007, 245, 43–61. [Google Scholar] [CrossRef] [PubMed]
- Vergroesen, P.P.; Kingma, I.; Emanuel, K.S.; Hoogendoorn, R.J.; Welting, T.J.; van Royen, B.J.; van Dieën, J.H.; Smit, T.H. Mechanics and Biology in Intervertebral Disc Degeneration: A Vicious Circle. Osteoarthr. Cartil. 2015, 23, 1057–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefanakis, M.; Luo, J.; Pollintine, P.; Dolan, P.; Adams, M.A. ISSLS Prize Winner: Mechanical Influences in Progressive Intervertebral Disc Degeneration. Spine 2014, 39, 1365–1372. [Google Scholar] [CrossRef]
- Russo, F.; Ambrosio, L.; Ngo, K.; Vadalà, G.; Denaro, V.; Fan, Y.; Sowa, G.; Kang, J.D.; Vo, N. The Role of Type I Diabetes in Intervertebral Disc Degeneration. Spine 2019, 44, 1177. [Google Scholar] [CrossRef]
- Urban, J.P.; Smith, S.; Fairbank, J.C. Nutrition of The Intervertebral Disc. Spine 2004, 29, 2700–2709. [Google Scholar] [CrossRef] [PubMed]
- Urban, J.P.; Roberts, S. Degeneration of The Intervertebral Disc. Arthritis Res. Ther. 2003, 5, 120–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadjipavlou, A.G.; Tzermiadianos, M.N.; Bogduk, N.; Zindrick, M.R. The Pathophysiology of Disc Degeneration: A Critical Review. J. Bone Jt. Surg. Br. 2008, 90, 1261–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanna, R.M.; Shetty, A.P.; Rajasekaran, S. Patterns of Lumbar Disc Degeneration Are Different in Degenerative Disc Disease and Disc Prolapse Magnetic Resonance Imaging Analysis of 224 Patients. Spine J. 2014, 14, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Steffens, D.; Hancock, M.J.; Maher, C.G.; Williams, C.; Jensen, T.S.; Latimer, J. Does Magnetic Resonance Imaging Predict Future Low Back Pain? A Systematic Review. Eur. J. Pain 2014, 18, 755–765. [Google Scholar] [CrossRef]
- Berry, J.L.; Moran, J.M.; Berg, W.S.; Steffee, A.D. A Morphometric Study of Human Lumbar and Selected Thoracic Vertebrae. Spine 1987, 12, 362–367. [Google Scholar] [CrossRef]
- Wang, T.M.; Shih, C. Morphometric Variations of The Lumbar Vertebrae Between Chinese and Indian Adults. Cells Tissues Organs 1992, 144, 23–29. [Google Scholar] [CrossRef]
- Davies, K.M.; Recker, R.R.; Heaney, R.P. Normal Vertebral Dimensions and Normal Variation in Serial Measurements of Vertebrae. J. Bone Min. Res. 1989, 4, 341–349. [Google Scholar] [CrossRef]
- Williams, P.L.; Bannister, L.H.; Berry, M.M.; Collins, P.; Dyson, M.; Dussek, J.E.; Ferguson, M.W. Gray’s Anatomy: The Anatomical Basis of Medicine and Surgery, 38th ed.; Churchill Livingstone: New York, NY, USA, 1995. [Google Scholar]
- Kim, S.K.; Lee, S.R.; Moon, W.J.; Park, D.W.; Hahm, C.K. Regional Disc Change in Segmental Hypoplasia of The Lumbosacral Vertebral Bodies: MR Findings. J. Korean Radiol. Soc. 2000, 43, 25–30. [Google Scholar] [CrossRef] [Green Version]
- Frank, D.F.; Miller, J.E. Hypoplasia of The Lumbar Vertebral Body Simulating Spondylolisthesis. Radiology 1979, 133, 59–60. [Google Scholar] [CrossRef]
- Oura, P.; Nurkkala, M.; Auvinen, J.; Niinimäki, J.; Karppinen, J.; Junno, J.A. The Association of Body Size, Shape and Composition with Vertebral Size in Midlife–The Northern Finland Birth Cohort 1966 Study. Sci. Rep. 2019, 9, 1–8. [Google Scholar] [CrossRef]
- Abdel-Salam, A.; Eyres, K.S.; Cleary, J. Management of The Herniated Lumbar Disc: The Outcome After Chemonucleolysis, Surgical Disc Excision and Conservative Treatments. Eur. Spine J. 1992, 1, 89–95. [Google Scholar] [CrossRef]
- www.spine.org. Available online: https://www.spine.org/Portals/0/Assets/Downloads/ResearchClinicalCare/Guidelines/LumbarDiscHerniation.pdf (accessed on 13 April 2016).
- Vanhoutte, E.K.; Faber, C.G.; Van Nes, S.I.; Jacobs, B.C.; Van Doorn, P.A.; Van Koningsveld, R.; Cornblath, D.R.; Van Der Kooi, A.J.; Cats, E.A.; Van Den Berg, L.H. Modifying the Medical Research Council Grading System through Rasch Analyses. Brain 2012, 135, 1639–1649. [Google Scholar] [CrossRef] [Green Version]
- Wilms, G.; Maldague, B.; Parizel, P.; Meylaerts, L.; Vanneste, D.; Peluso, J. Hypoplasia of L5 and Wedging and Pseudospondylolisthesis in Patients with Spondylolysis: Study With MR Imaging. AJNR Am. J. Neuroradiol. 2009, 4, 674–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niggemann, P.; Kuchta, J.; Grosskurth, D.; Beyer, H.K.; Hoeffer, J.; Delank, K.S. Spondylolysis and Isthmic Spondylolisthesis: Impact of Vertebral Hypoplasia on The Use of The Meyerding Classification. Br. J. Radiol. 2012, 85, 358–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masharawi, Y.; Salame, K.; Mirovsky, Y.; Peleg, S.; Dar, G.; Steinberg, N.; Hershkovitz, I. Vertebral Body Shape Variation in The Thoracic and Lumbar Spine: Characterization of Its Asymmetry and Wedging. Clin. Anat. 2008, 21, 46–54. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | n | % | |
|---|---|---|---|
| All Patients | 67 | 100 | |
| Sex | Female | 36 | 50.7 |
| Male | 31 | 49.3 | |
| Age (years) | median (range) | 49 (18–87) | |
| Body Height (cm) | median (range) | 172 (153–191) | |
| Body Weight (kg) | median (range) | 74 (50–155) | |
| Body Mass Index (BMI) | median (range) | 25 (18.8–49.5) | |
| Smoker | 24 | 35.8 | |
| Diabetes | 2 | 3.0 | |
| Vertebral Endplate Level | n | Minimum (mm) | Maximum (mm) | Mean (mm) | Median (mm) | SD | p-Value |
|---|---|---|---|---|---|---|---|
| upper L3 | 67 | 25.8 | 46.6 | 33.2 | 33.3 | 3.3 | 0.9875 |
| lower L3 | 67 | 25.1 | 42.9 | 33.2 | 33.2 | 3.4 | 0.2279 |
| upper L4 | 67 | 27.2 | 41.8 | 33.3 | 33.3 | 3.1 | 0.0034 |
| lower L4 | 67 | 27.1 | 44.7 | 34.0 | 34.4 | 3.4 | 0.0146 |
| upper L5 | 67 | 27.1 | 41.1 | 33.2 | 33.1 | 3.3 | 0.2365 |
| lower L5 | 67 | 26.4 | 41.2 | 33.5 | 33.6 | 3.5 | <0.0001 |
| upper S1 | 67 | 24.6 | 39.9 | 31.6 | 31.1 | 3.5 | n/a |
| L3/4 | DH+ | DH− | PPV | OR | ±SE | p-Value |
|---|---|---|---|---|---|---|
| Disproportion + | 0 | 3 | 0.00 | n/a | n/a | 1.000 |
| Disproportion − | 6 | 58 | ||||
| L4/5 | DH+ | DH− | PPV | OR | ±SE | p-Value |
| Disproportion + | 4 | 4 | 0.50 | 1.68 | 0.76 | 0.489 |
| Disproportion − | 22 | 37 | ||||
| L5/S1 | DH+ | DH− | PPV | OR | ±SE | p-Value |
| Disproportion + | 10 | 2 | 0.83 | 6.00 | 0.82 | 0.017 |
| Disproportion − | 25 | 30 | ||||
| L3-S1 (pooled) | DH+ | DH− | PPV | OR | ±SE | p-Value |
| Disproportion + | 14 | 9 | 0.61 | 3.67 | 0.46 | 0.003 |
| Disproportion − | 53 | 125 |
| Variable | Coefficient c1–8 | Std. Error | Odds Ratio | 95% CI | p |
|---|---|---|---|---|---|
| Age (A) | 0.01 | 0.01 | 1.01 | 0.99 to 1.03 | 0.520 |
| Weight (W) | 0.04 | 0.10 | 1.04 | 0.85 to 1.28 | 0.721 |
| Height (H) | −0.03 | 0.10 | 0.97 | 0.81 to 1.18 | 0.787 |
| BMI (B) | −0.11 | 0.31 | 0.90 | 0.49 to 1.66 | 0.728 |
| Male sex (M) | −0.07 | 0.45 | 0.93 | 0.39 to 2.25 | 0.874 |
| Diabetes (D) | −0.61 | 1.41 | 0.54 | 0.03 to 8.65 | 0.665 |
| Smoking (S) | −0.03 | 0.36 | 0.97 | 0.48 to 1.94 | 0.925 |
| Disproportion (DP) | 1.41 | 0.48 | 4.11 | 1.60 to 10.54 | 0.003 |
| Constant b0 | 3.28 | 16.78 | 0.845 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Läubli, R.; Brugger, R.; Pirvu, T.; Hoppe, S.; Sieroń, D.; Szyluk, K.; Albers, C.E.; Christe, A. Disproportionate Vertebral Bodies and Their Impact on Lumbar Disc Herniation. J. Clin. Med. 2021, 10, 3174. https://doi.org/10.3390/jcm10143174
Läubli R, Brugger R, Pirvu T, Hoppe S, Sieroń D, Szyluk K, Albers CE, Christe A. Disproportionate Vertebral Bodies and Their Impact on Lumbar Disc Herniation. Journal of Clinical Medicine. 2021; 10(14):3174. https://doi.org/10.3390/jcm10143174
Chicago/Turabian StyleLäubli, Ralph, Robin Brugger, Tatiana Pirvu, Sven Hoppe, Dominik Sieroń, Karol Szyluk, Christoph E. Albers, and Andreas Christe. 2021. "Disproportionate Vertebral Bodies and Their Impact on Lumbar Disc Herniation" Journal of Clinical Medicine 10, no. 14: 3174. https://doi.org/10.3390/jcm10143174