
Selective Segmental Pulmonary Angiography: Anatomical, Technical and Safety Aspects of a Must-Learn Technique in Times of Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Pulmonary Arteries’ Anatomy
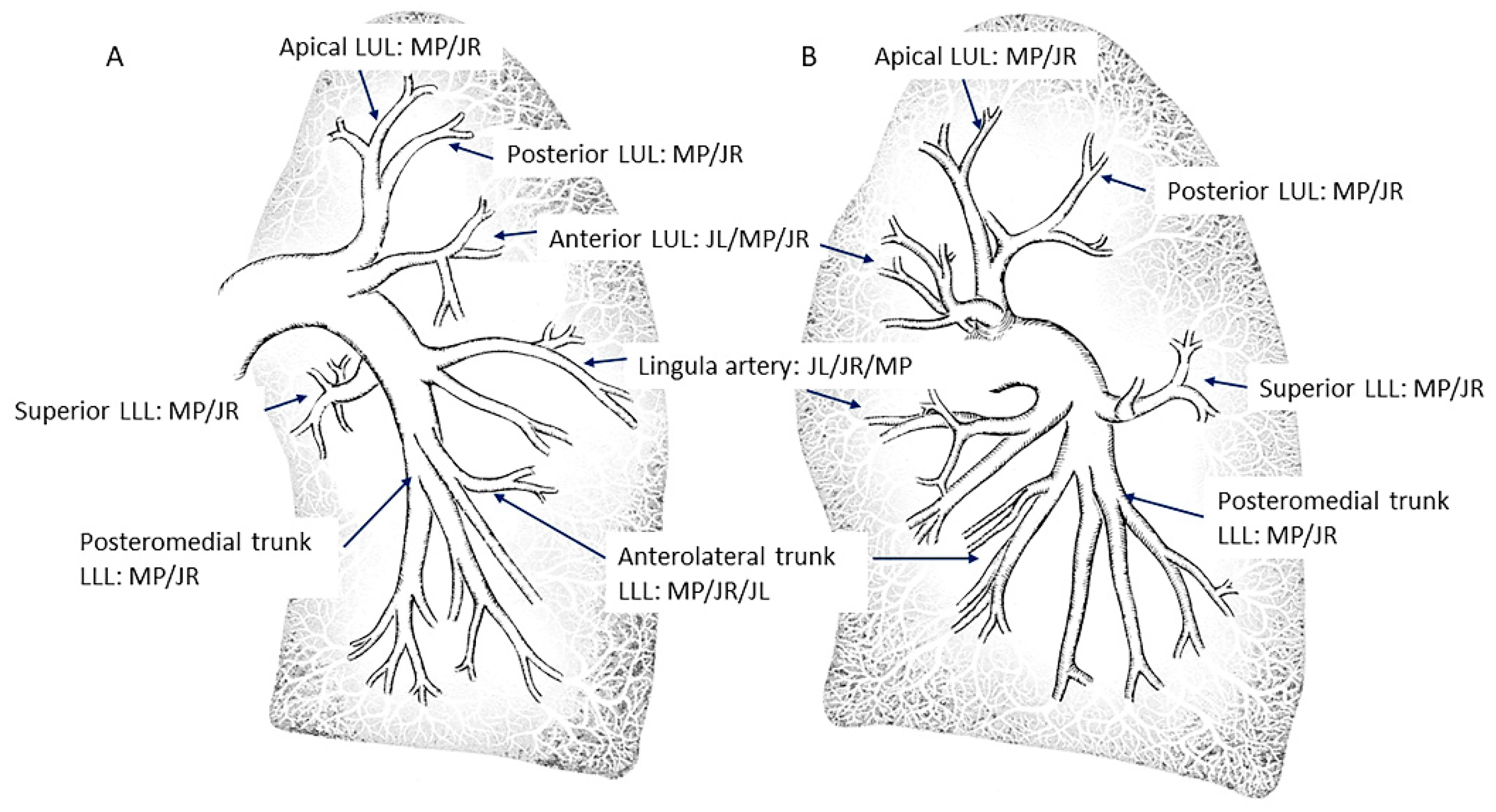
2.1. Lobar and Segmental Arteries of the Upper Lobes
2.2. Lobar and Segmental Arteries of the Lingula and the Middle Lobe
2.3. Lobar and Segmental Arteries of the Lower Lobes
3. Angiographic Projections
4. Procedure
5. Venous Access
6. Catheter Selection and Positioning
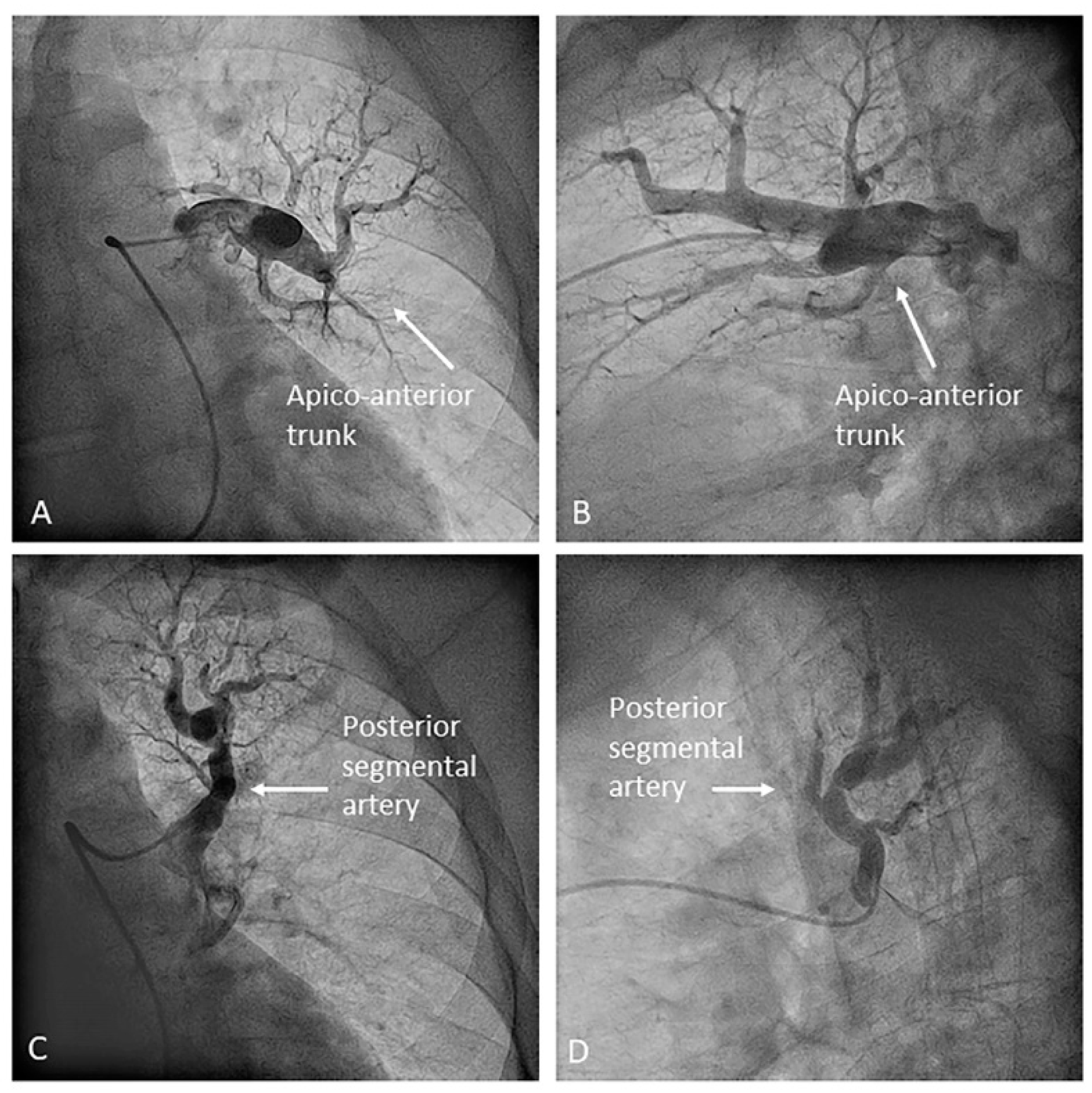
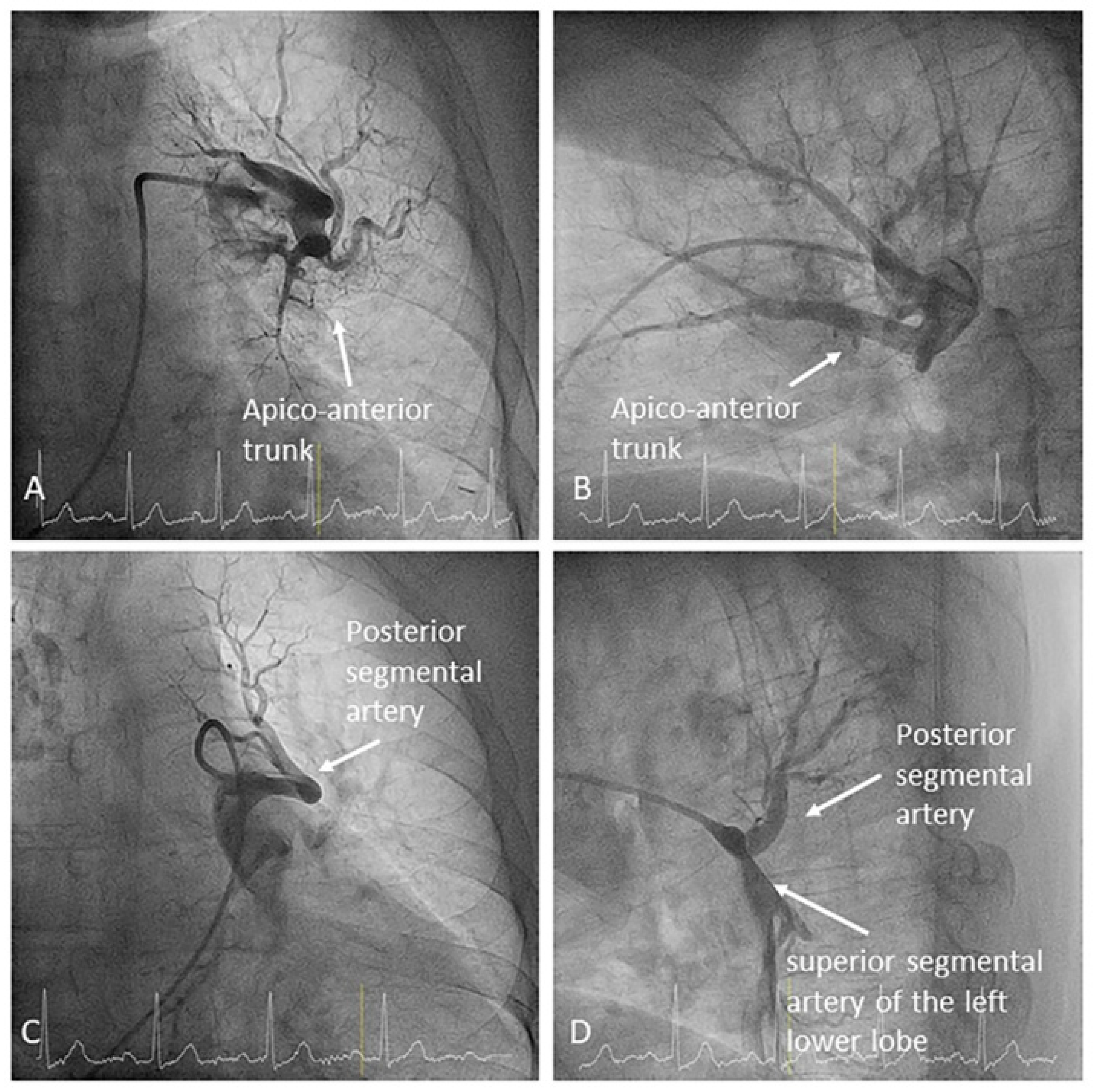
- Left upper lobe. The apico-posterior trunk (A1/2) is easily cannulated in the AP view. We should rotate the MP-A2 catheter counterclockwise in the proximal segment of the LPA to make the tip face upwards (Figure 23). The apical and posterior segmental arteries (A1 and A2) are well visualized by filming in the AP and lateral views. The anterior segmental artery (A3) is engaged more easily with the Judkins left catheter (JL) 3.5 or 4. Position the JL below the aortic arc in the AP view with the distal tip facing the left lateral chest wall. Rotate the catheter counterclockwise and withdraw it slightly. The distal tip of the catheter will climb 2–3 cm, engaging the anterior segmental branch (A3) (Figure 24). Film this branch in the cranial RAO and lateral views.
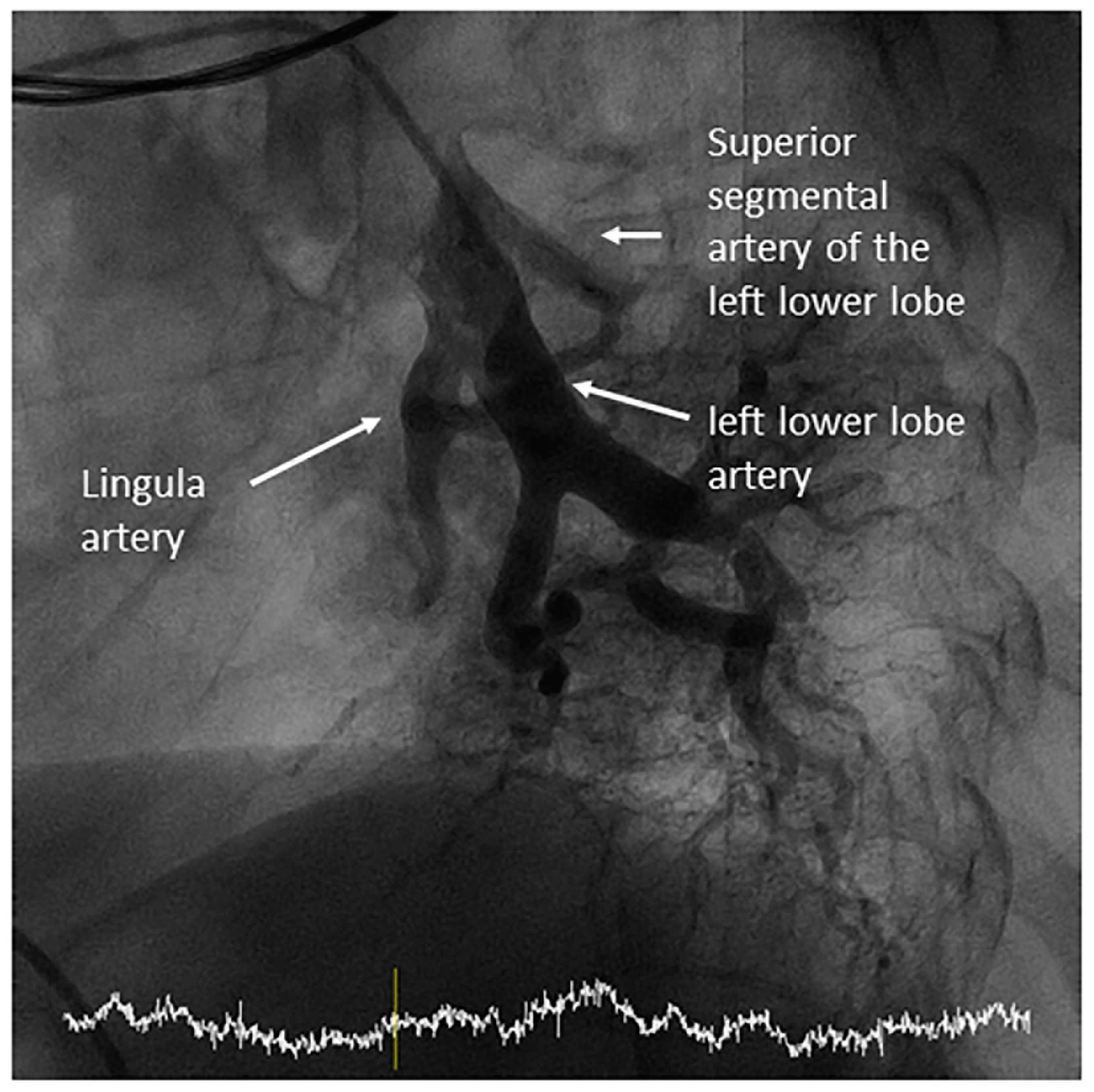
- Lingula. The lingula artery is easily cannulated in the AP view with the JL 3.5/4 catheter (depending on the PA dilatation). The maneuver and position in the AP view is the same as described for the anterior segmental artery of the left upper lobe (A3), though somewhat lower (Figure 25). Amplatz left 1 or 2 is also a good choice for catheterization of the lingula branches. In addition, this catheter gives extra support when performing BPA of these branches. The two lingula segmental arteries are well displayed in the lateral and in the cranial RAO/cranial AP views.
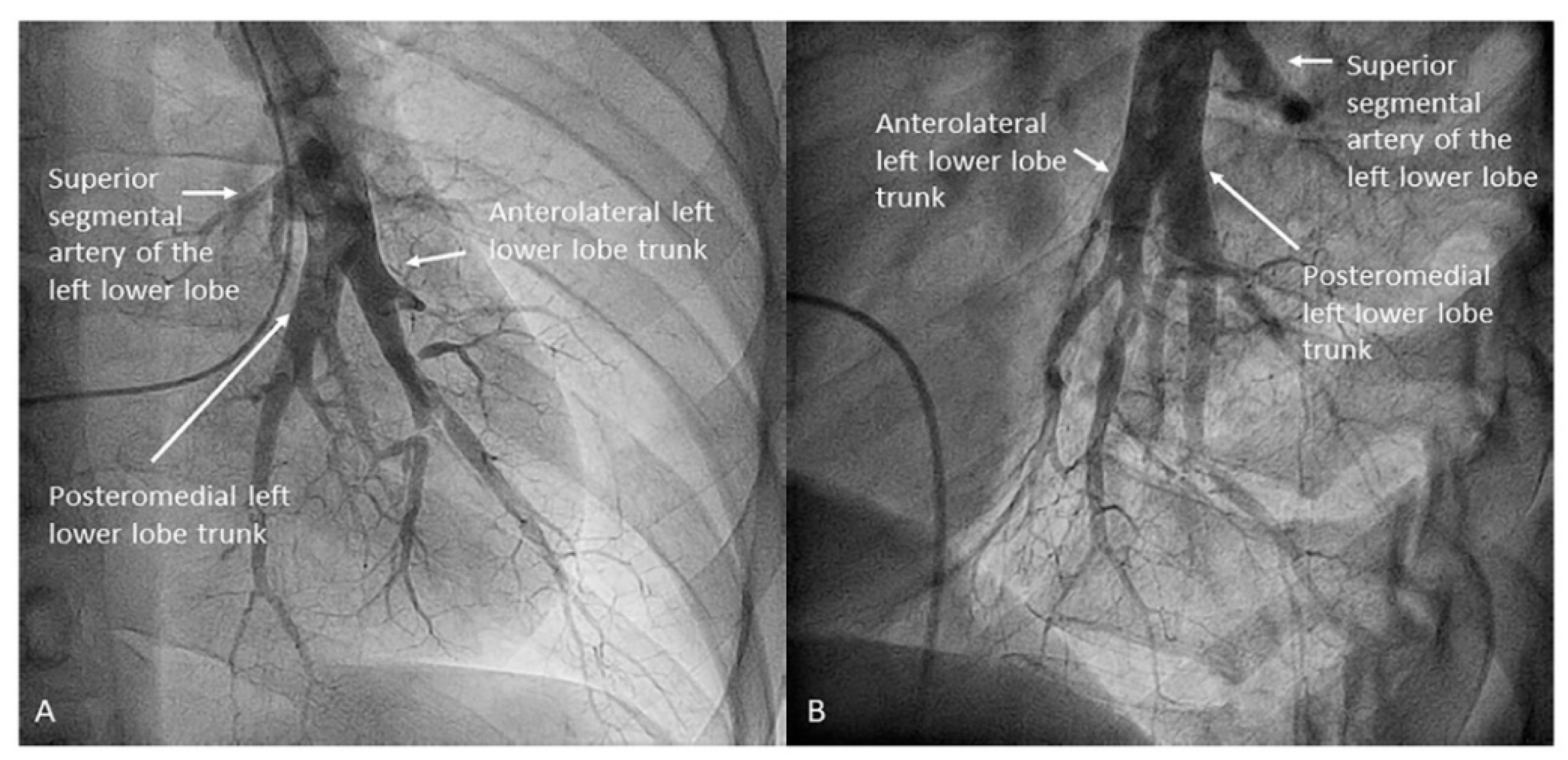
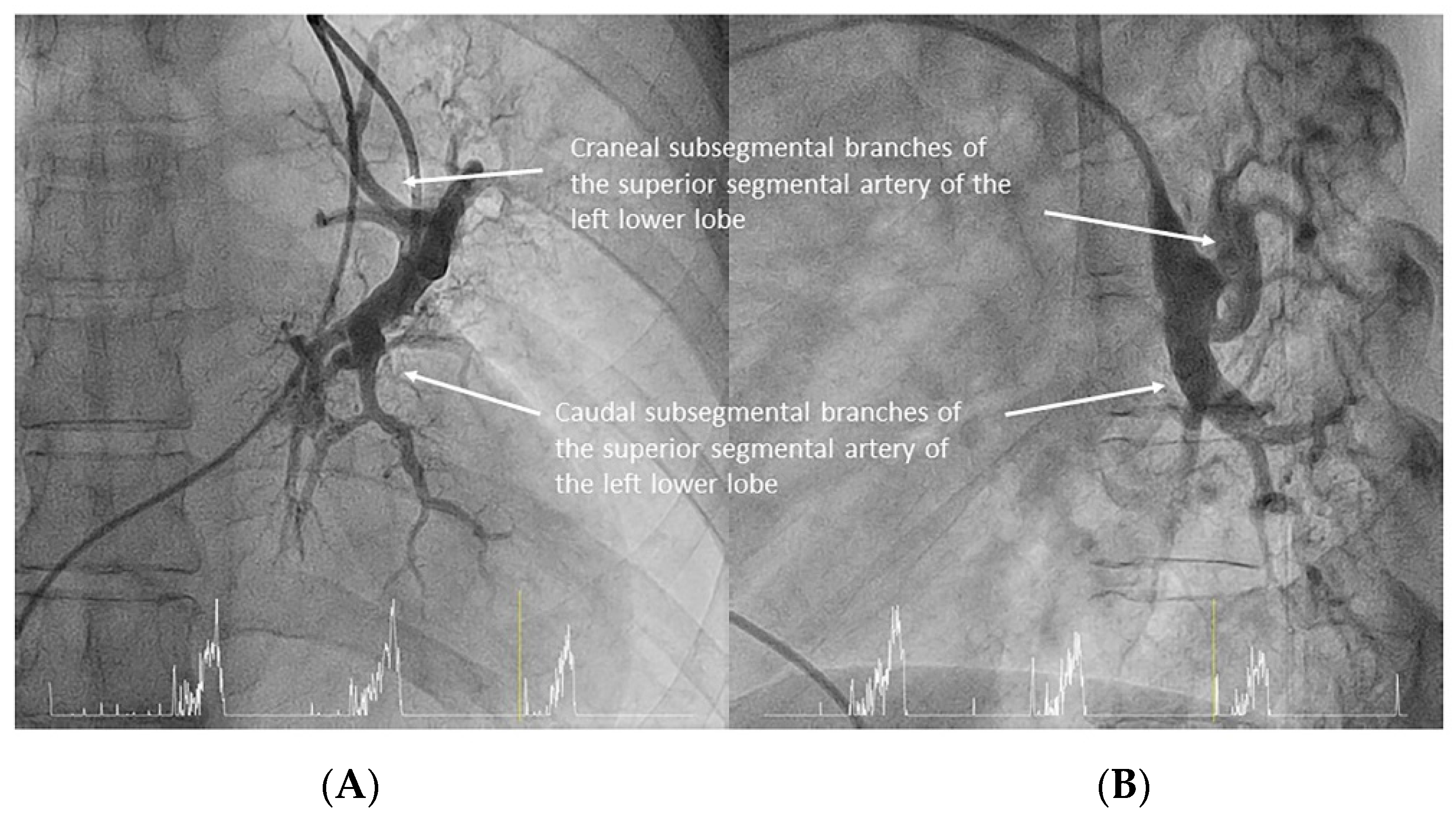
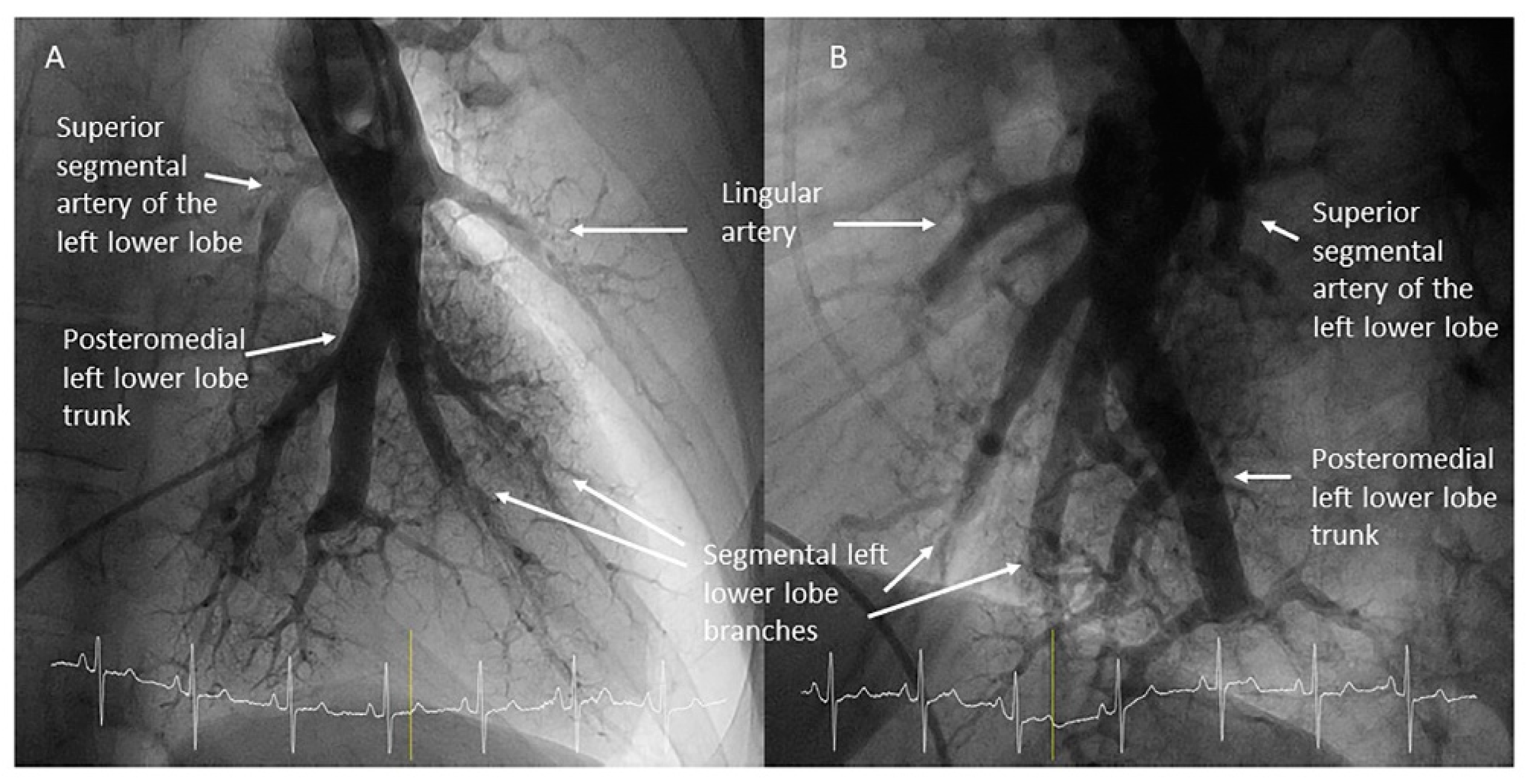
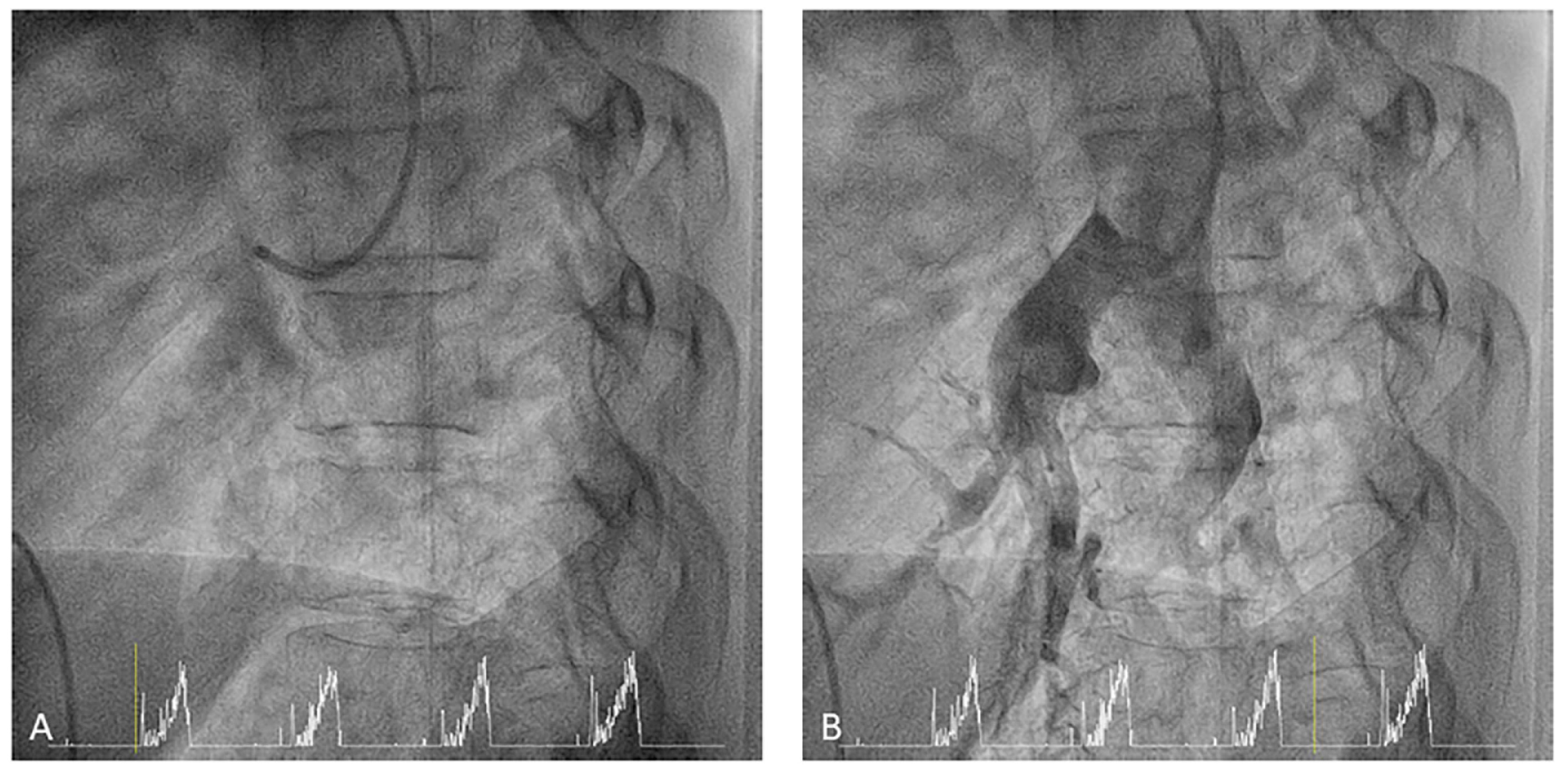
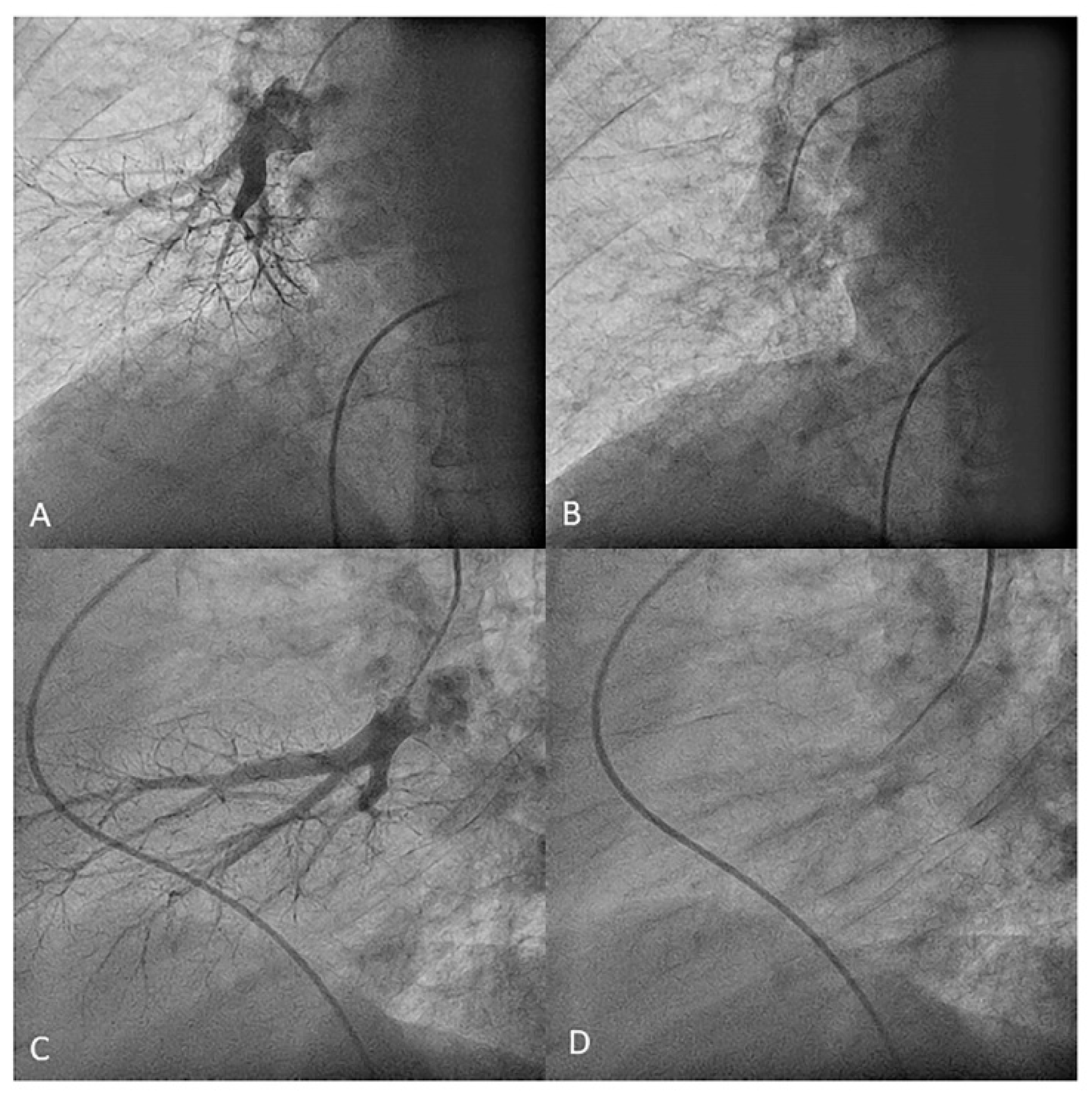
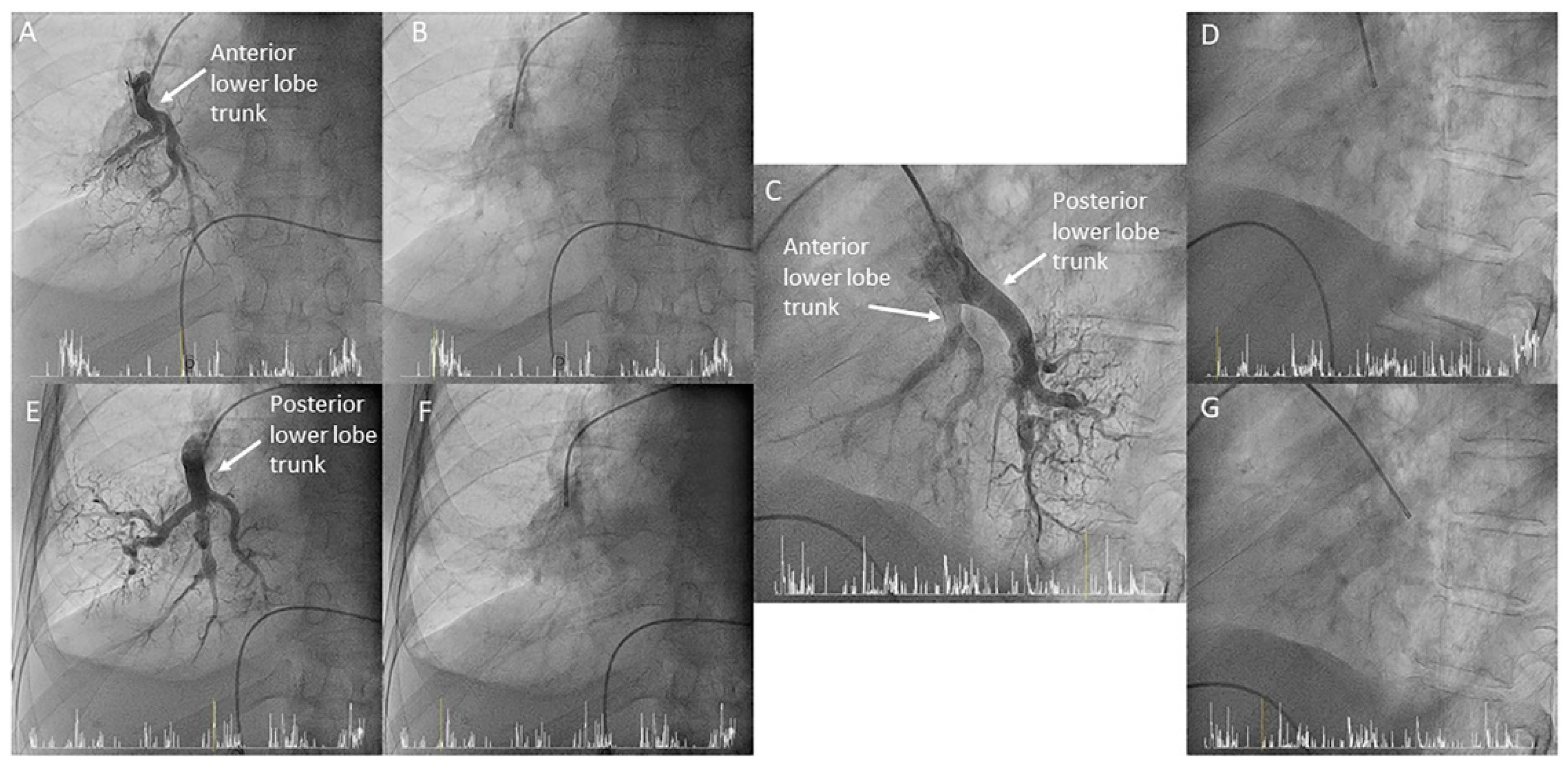
- Left lower lobe. The two trunks of the basal pyramid and the superior segmental artery (A6) are easily cannulated with the MP-A2 in the lateral projection (Figure 26). The anterolateral trunk (A8/9) sometimes requires the Judkins right (JR) 4 or the JL 3.5/4. We should sequentially film both trunks and the superior segmental artery (A6) in the lateral and AP view.
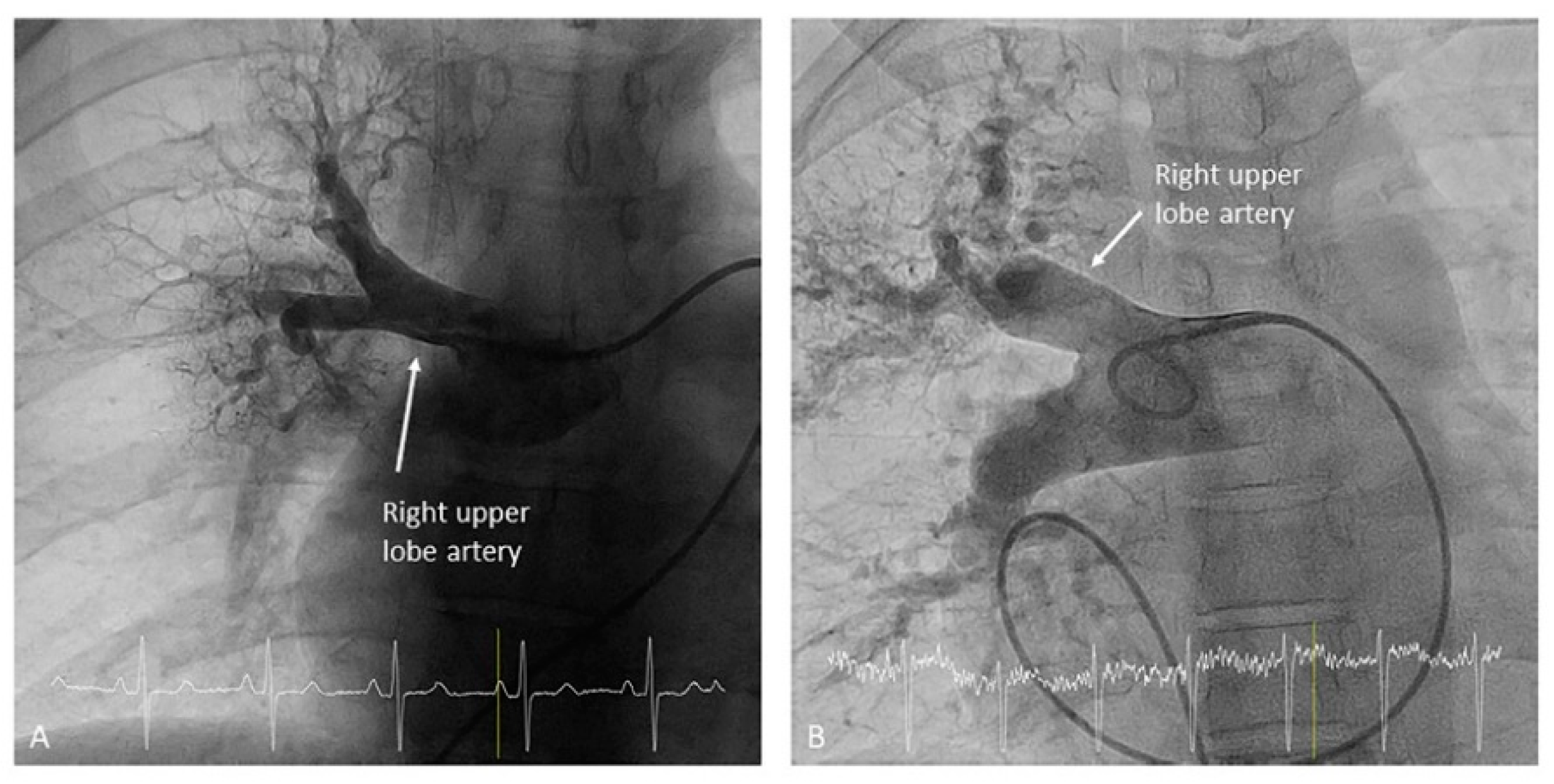
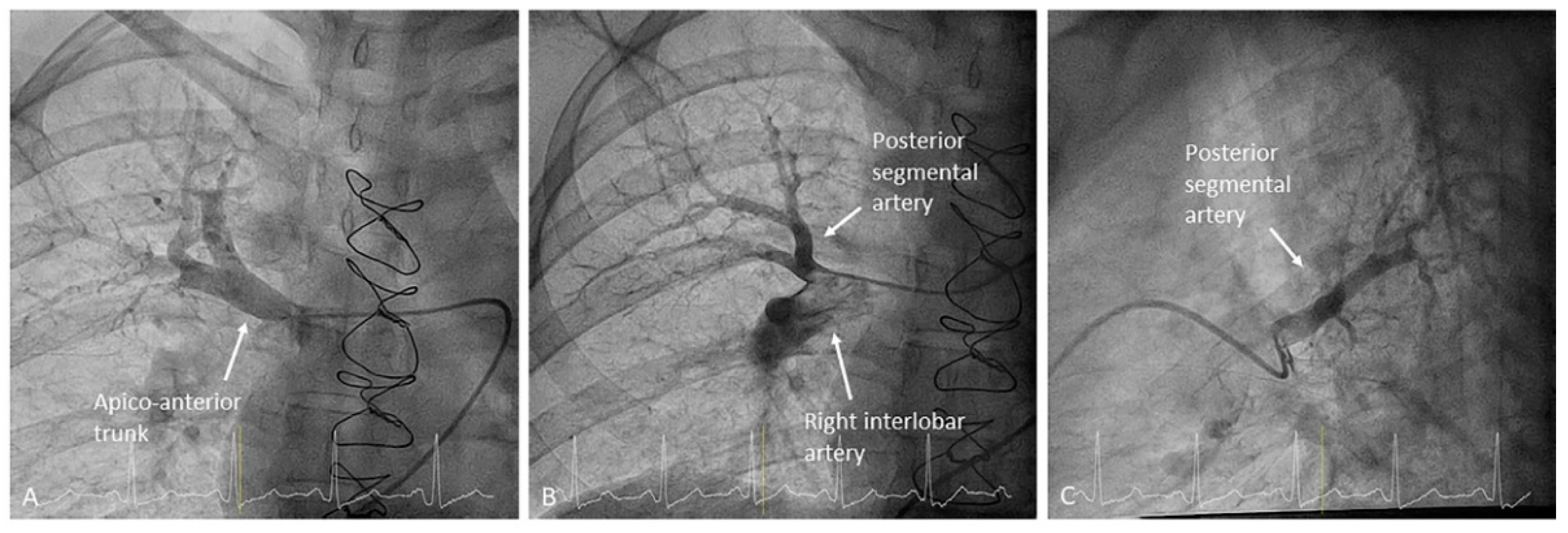
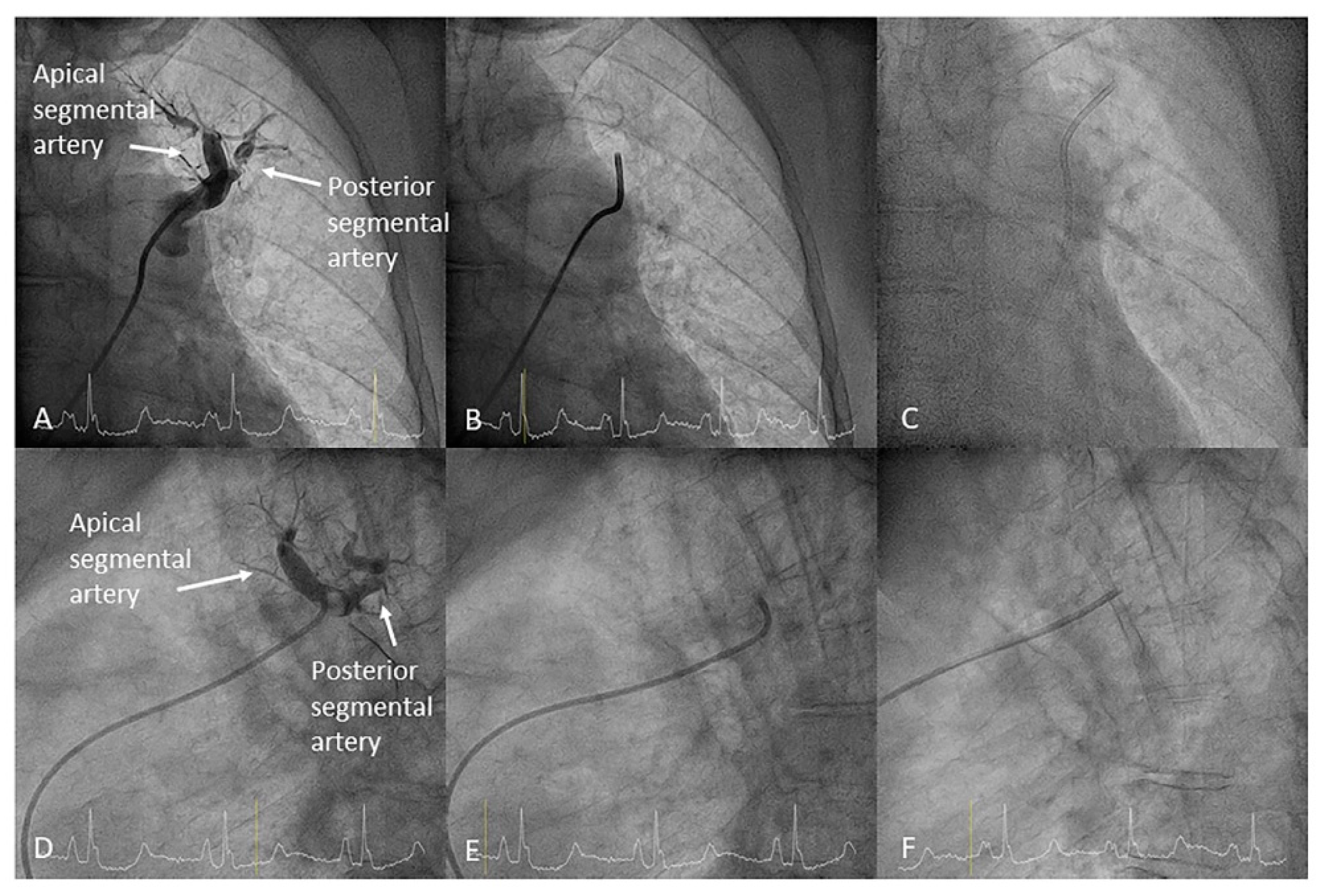
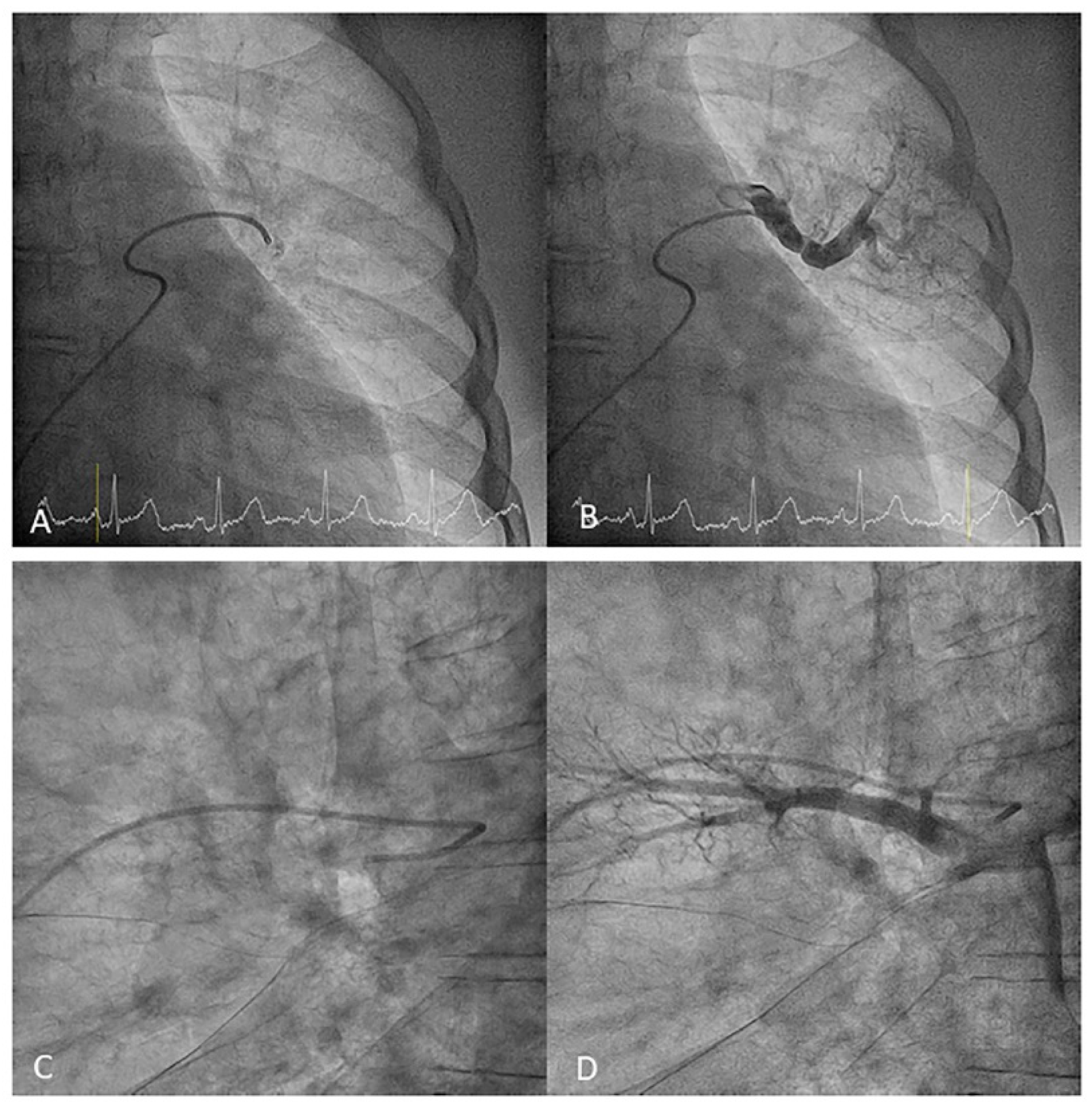
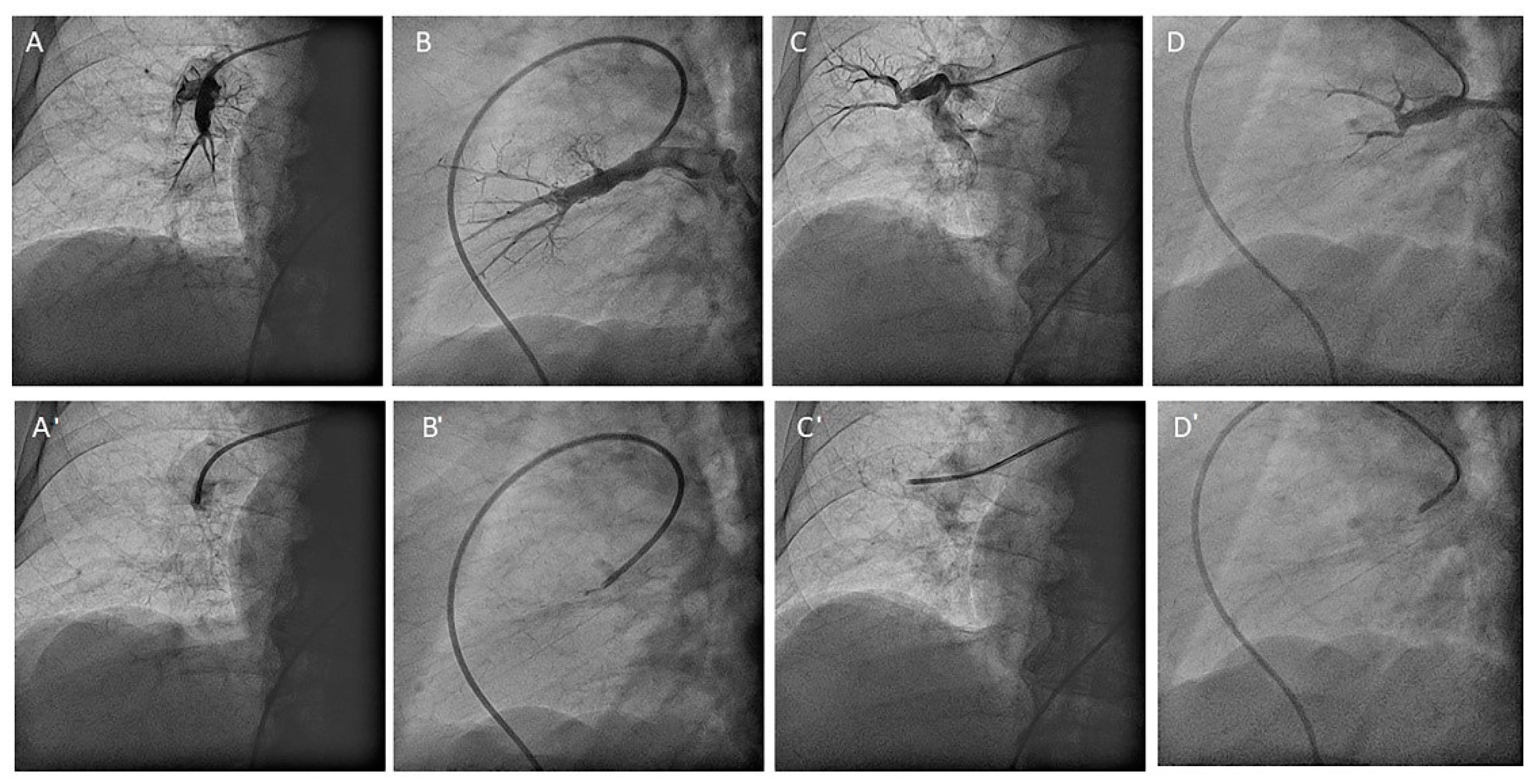
- Right upper lobe. The right upper lobar artery arises about 10 cm from the bifurcation. It is cannulated in the AP view with the tip of the MP-A2 facing upwards. The apico-posterior segmental artery (A1/2) is canalized just by advancing the MP distally once in the right upper lobe artery. The AP and lateral views display the apical (A1) and posterior branches (A2) (Figure 28). The anterior segmental artery (A3) is canalized in the lateral view, rotating the MP counterclockwise from its position in the apico-posterior artery (A1/2). With this maneuver, the tip of the catheter moves downwards, facing the sternum and engaging the anterior segmental artery (A3) (Figure 29). This branch should be filmed in lateral and cranial AP/cranial LAO view.
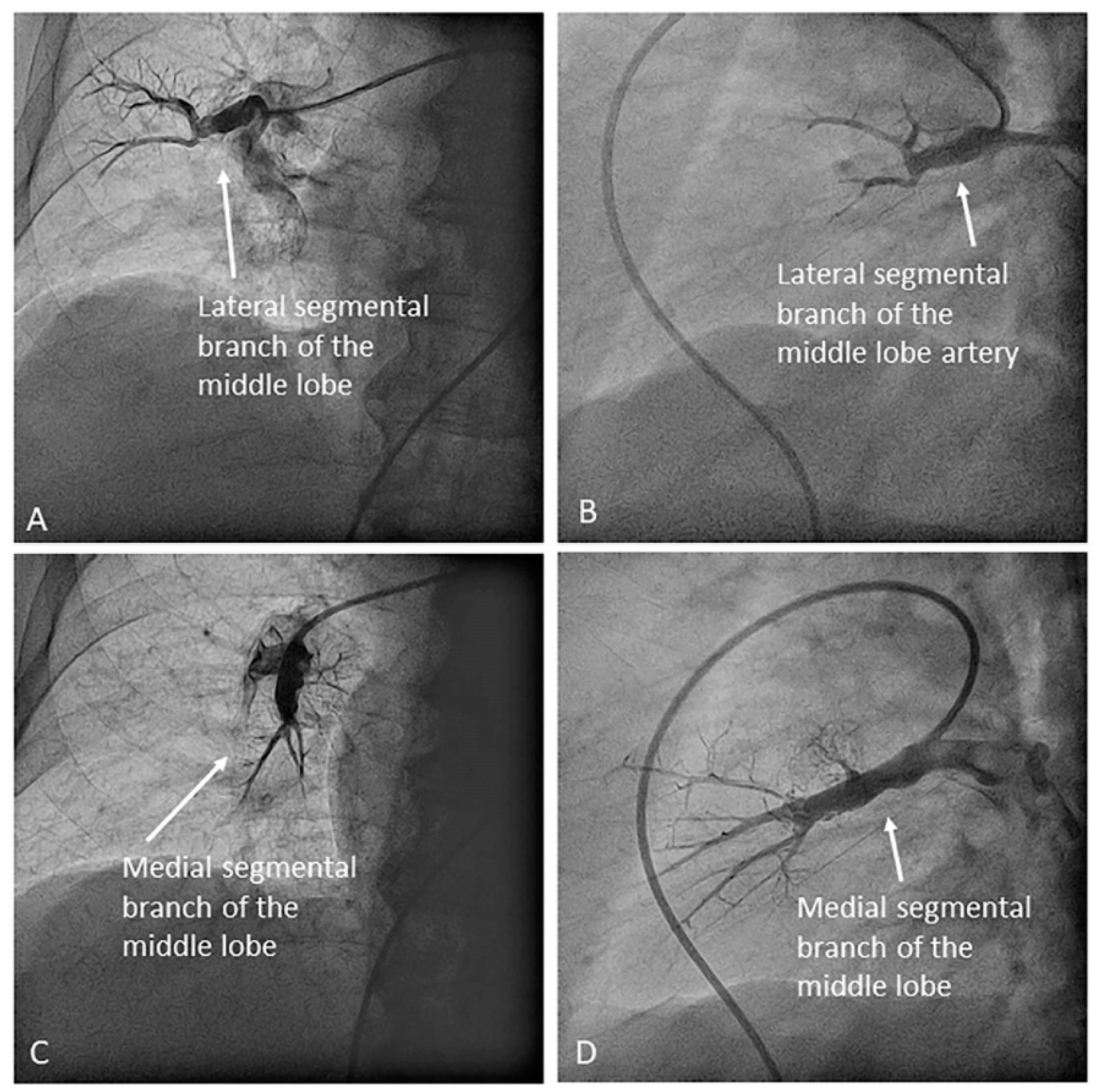
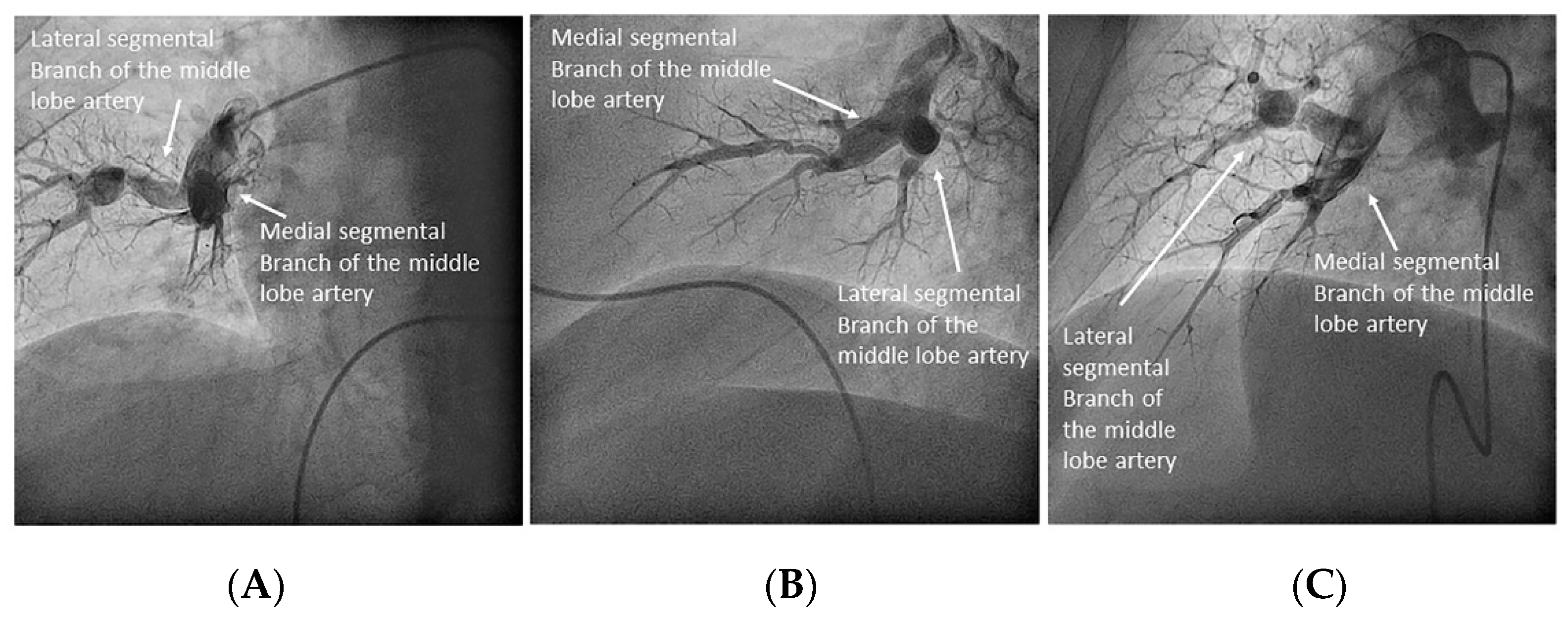
- Middle lobe. The middle lobe artery originates in front of the superior segmental artery of the RLL (A6), with an anterior direction, as does the lingula in the left lung (Figure 14). It is canalized with the MP, in the lateral view. The distal angulated segment of the MP should be bent, pressing against the bifurcation of the RLL, and rotated counterclockwise, with the tip of the catheter pointing towards the sternum (Figure 30). The JR 4 is also a good alternative. This artery bifurcates early in two segmental branches: lateral (A4) and medial (A5). The lateral and cranial LAO views display both branches. If these segmental branches have an independent origin in the RPA, they should be cannulated and filmed independently (Figure 31).
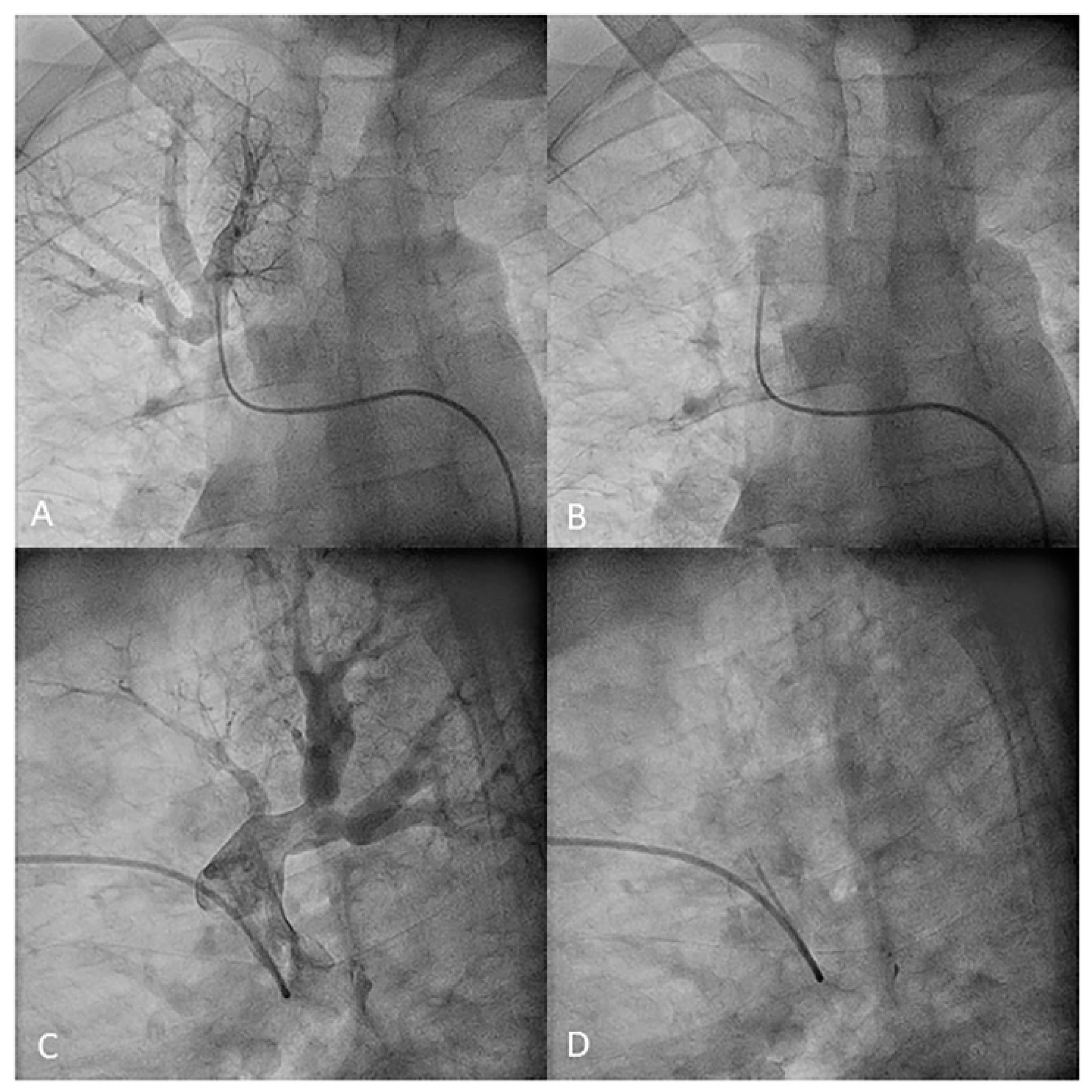
- Right lower lobe. The lateral projection and the MP are the best choices to canalize the two trunks of the basal pyramid and the superior segmental artery (A6). Use the AP and lateral views to assess the four segmental basal branches (Figure 32) and the lateral projection to display the superior segmental artery (A6) (Figure 16 and Figure 17).
7. Contrast Injection Settings
8. Differential Characteristics between Diagnostic Selective Segmental Pulmonary Angiography Technique and Central Pulmonary Angiography with Digital Subtraction
9. Selective Segmental Pulmonary Angiography Complications
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galiè, N.; Humbert, M.; Vachiery, J.-L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Noordegraaf, A.V.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [PubMed]
- Ang, L.; McDivit Mizzell, A.; Daniels, L.B.; Ben-Yehuda, O.; Mahmud, E. Optimal Technique for Performing Invasive Pulmonary Angiography for Chronic Thromboembolic Pulmonary Disease. J. Invasive Cardiol. 2019, 31, E211–E219. [Google Scholar]
- Mehta, S.; Helmersen, D.; Provencher, S.; Hirani, N.; Rubens, F.D.; De Perrot, M.; Blostein, M.; Boutet, K.; Chandy, G.; Dennie, C.; et al. Diagnostic evaluation and management of chronic thromboembolic pulmonary hypertension: A clinical practice guideline. Can. Respir. J. 2010, 17, 301–334. [Google Scholar] [CrossRef]
- Hinrichs, J.B.; Marquardt, S.; Von Falck, C.; Hoeper, M.M.; Olsson, K.M.; Wacker, F.K.; Meyer, B.C. Comparison of C-arm Computed Tomography and Digital Subtraction Angiography in Patients with Chronic Thromboembolic Pulmonary Hypertension. Cardiovasc. Interv. Radiol. 2016, 39, 53–63. [Google Scholar]
- Kim, N.H.; Delcroix, M.; Jais, X.; Madani, M.M.; Matsubara, H.; Mayer, E.; Ogo, T.; Tapson, V.F.; Ghofrani, H.-A.; Jenkins, D.P. Chronic thromboembolic pulmonary hypertension. Eur. Respir. J. 2019, 53, 1801915. [Google Scholar] [CrossRef]
- Guillinta, P.; Peterson, K.L.; Ben-Yehuda, O. Cardiac catheterization techniques in pulmonary hypertension. Cardiol. Clin. 2004, 22, 401–415. [Google Scholar] [CrossRef] [PubMed]
- Kandathil, A.; Chamarthy, M. Pulmonary vascular anatomy & anatomical variants. Cardiovasc. Diagn. Ther. 2018, 8, 201–207. [Google Scholar] [PubMed]
- Helmersen, D.; Provencher, S.; Hirsch, A.M.; Van Dam, A.; Dennie, C.; De Perrot, M.; Mielniczuk, L.; Hirani, N.; Chandy, G.; Swiston, J.; et al. Diagnosis of chronic thromboembolic pulmonary hypertension: A Canadian Thoracic Society clinical practice guideline update. Can. J. Respir. Crit. Care Sleep Med. 2019, 3, 177–198. [Google Scholar] [CrossRef]
- Gopalan, D.; Delcroix, M.; Held, M. Diagnosis of chronic thromboembolic pulmonary hypertension. Eur. Respir. Rev. 2017, 26, 160108. [Google Scholar] [CrossRef] [PubMed]
- Ley, S.; Ley-Zaporozhan, J.; Pitton, M.; Schneider, J.; Wirth, G.M.; Mayer, E.; Düber, C.; Kreitner, K.-F. Diagnostic performance of state-of-the-art imaging techniques for morphological assessment of vascular abnormalities in patients with chronic thromboembolic pulmonary hypertension (CTEPH). Eur. Radiol. 2012, 22, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Hinrichs, J.B.; Renne, J.; Hoeper, M.M.; Olsson, K.M.; Wacker, F.K.; Meyer, B.C. Balloon pulmonary angioplasty: Applicability of C-Arm CT for procedure guidance. Eur. Radiol. 2016, 26, 4064–4071. [Google Scholar] [CrossRef] [PubMed]
- Hoeper, M.M.; Lee, S.H.; Voswinckel, R.; Palazzini, M.; Jais, X.; Marinelli, A.; Barst, R.J.; Ghofrani, H.A.; Jing, Z.-C.; Opitz, C.; et al. Complications of right heart catheterization procedures in patients with pulmonary hypertension in experienced centers. J. Am. Coll. Cardiol. 2006, 48, 2546–2552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofmann, L.V.; Lee, D.S.; Gupta, A.; Arepally, A.; Sood, S.; Girgis, R.; Eng, J. Safety and hemodynamic effects of pulmonary angiography in patients with pulmonary hypertension: 10-year single-center experience. AJR Am. J. Roentgenol. 2004, 183, 779–786. [Google Scholar] [CrossRef] [PubMed]


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Age (years) | 58.5 ± 15.7 |
| Sex (women) | 56.4 (255) |
| Weight (Kg) | 76.9 ± 16.8 |
| Height (cm) | 164.5 ± 10.8 |
| Body surface (m2) | 1.82 ± 0.2 |
| Heart rate (beats per minute) | 75.5 ± 13.7 |
| Oxygen saturation (%) | 94.1 ± 3.7 |
| Pulmonary artery oxygen saturation (%) | 62.5 ± 7.9 |
| Right atrial pressure (mmHg) | 8.8 ± 4.6 |
| Systolic pulmonary artery pressure (mmHg) | 74.9 ± 22.8 |
| Diastolic pulmonary artery pressure(mmHg) | 26.7 ± 13.2 |
| Mean pulmonary artery pressure (mmHg) | 43.9 ± 12.8 |
| Wedge pressure (mmHg) | 10.8 ± 4.1 |
| Cardiac output (L/min) | 3.2 ± 1.5 |
| Cardiac index (L/min/m2) | 1.8 ± 0.8 |
| Pulmonary vascular resistance (WU) | 10.4 ± 4.0 |
| Venous access | |
| ● Femoral | 92.0 (416) |
| ● Jugular | 5.5 (25) |
| ● Basilica/cephalic/humeral vein | 2.4 (11) |
| Scopia time (min) | 19.1 ± 10.6 |
| PDA (Gycm2) | 102.3 ± 65.2 |
| Procedure time (min) | 81.3 ± 17.9 |
| Contrast dose (mL) | 300.8 ± 85.5 |
| Complication | % (Absolute Value) |
|---|---|
| Any complication | 4.9 (22) |
| Bleeding | 2.2 (10) |
| Puncture site | 1.8 (8) |
| Hemoptysis | 0.2 (1) |
| Other bleeding | 0.2 (1) |
| Bleeding type (BARC criteria) | |
| 2 | 1.8 (8) |
| 3 | 0.4 (2) |
| Arteriovenous fistula | 0 (0) |
| Pseudoaneurysm | 0.7 (3) |
| Puncture site ischemia | 0 (0) |
| Acute renal failure (AKIN criteria) | 1.1 (5) |
| Needing dialysis | 0 (0) |
| Arrhythmias | 0.7 (3) |
| Atrial fibrillation | 0.4 (2) |
| Paroxysmal Complete AV block | 0.2 (1) |
| Allergic reaction | 0.4 (2) |
| ● Cutaneous | 0.4 (2) |
| ● Anaphylaxis | 0 (0) |
| ● Cardiac tamponade | 0 (0) |
| Respiratory insufficiency requiring ventilatory support | 0.2 (1) |
| Hemodynamic instability requiring pharmacological or mechanical support | 0.4 (2) |
| Death | 0.2 (1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velázquez, M.; Maneiro, N.; Lareo, A.; Albarrán, A.; Huertas, S.; Olazábal, A.P.; Delgado, J.F.; Alonso, S.; Sarnago, F.; García Tejada, J.; et al. Selective Segmental Pulmonary Angiography: Anatomical, Technical and Safety Aspects of a Must-Learn Technique in Times of Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension. J. Clin. Med. 2021, 10, 3358. https://doi.org/10.3390/jcm10153358
Velázquez M, Maneiro N, Lareo A, Albarrán A, Huertas S, Olazábal AP, Delgado JF, Alonso S, Sarnago F, García Tejada J, et al. Selective Segmental Pulmonary Angiography: Anatomical, Technical and Safety Aspects of a Must-Learn Technique in Times of Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension. Journal of Clinical Medicine. 2021; 10(15):3358. https://doi.org/10.3390/jcm10153358
Chicago/Turabian StyleVelázquez, Maite, Nicolás Maneiro, Ana Lareo, Agustín Albarrán, Sergio Huertas, Allende P. Olazábal, Juan F. Delgado, Sergio Alonso, Fernando Sarnago, Julio García Tejada, and et al. 2021. "Selective Segmental Pulmonary Angiography: Anatomical, Technical and Safety Aspects of a Must-Learn Technique in Times of Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension" Journal of Clinical Medicine 10, no. 15: 3358. https://doi.org/10.3390/jcm10153358