
Procollagen I and III as Prognostic Markers in Patients Treated with Extracorporeal Membrane Oxygenation: A Prospective Observational Study


Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Ethics
2.2. Participants
2.3. Standard Therapy
2.4. Data Collection
2.5. Statistical Analysis
3. Results
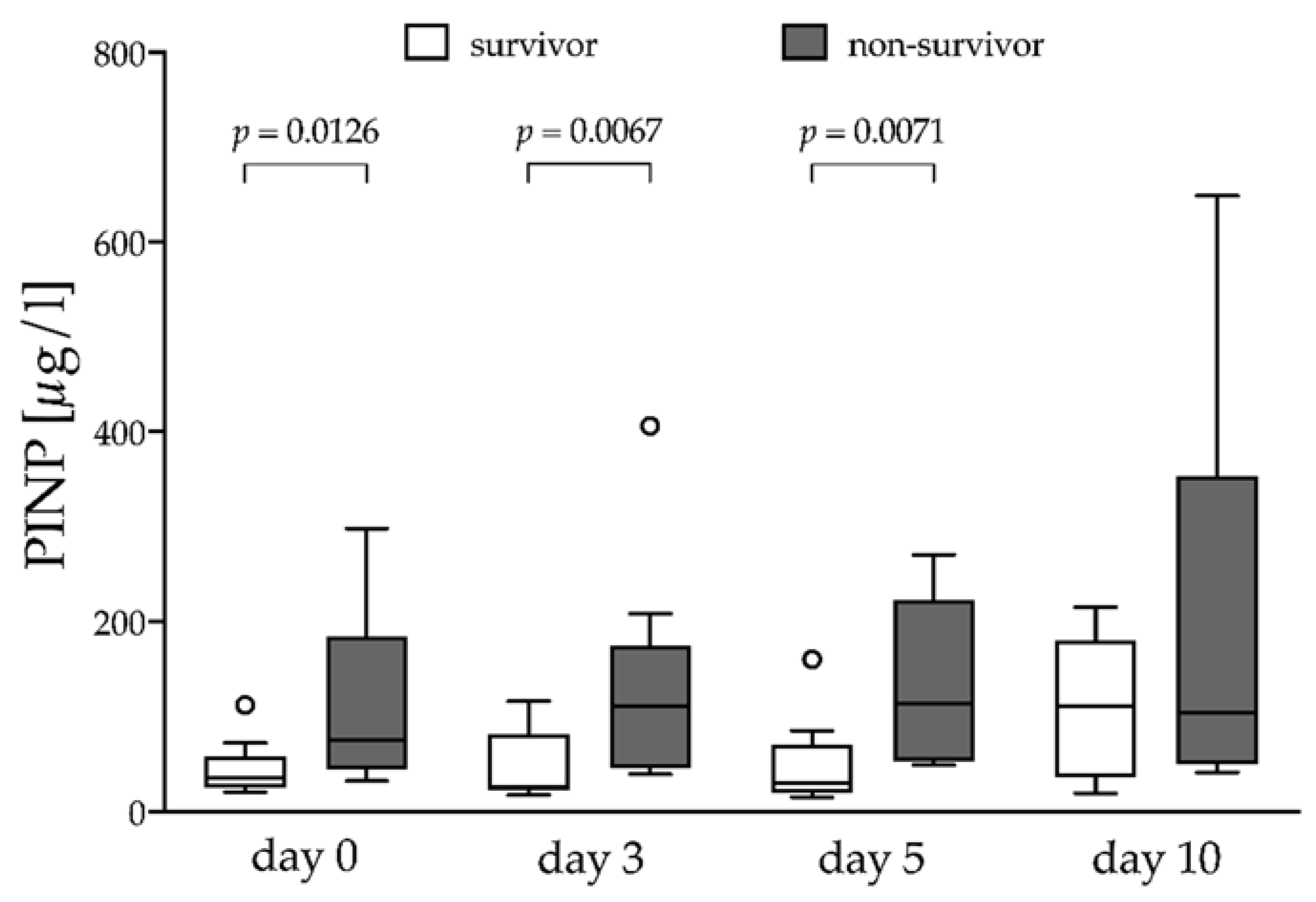
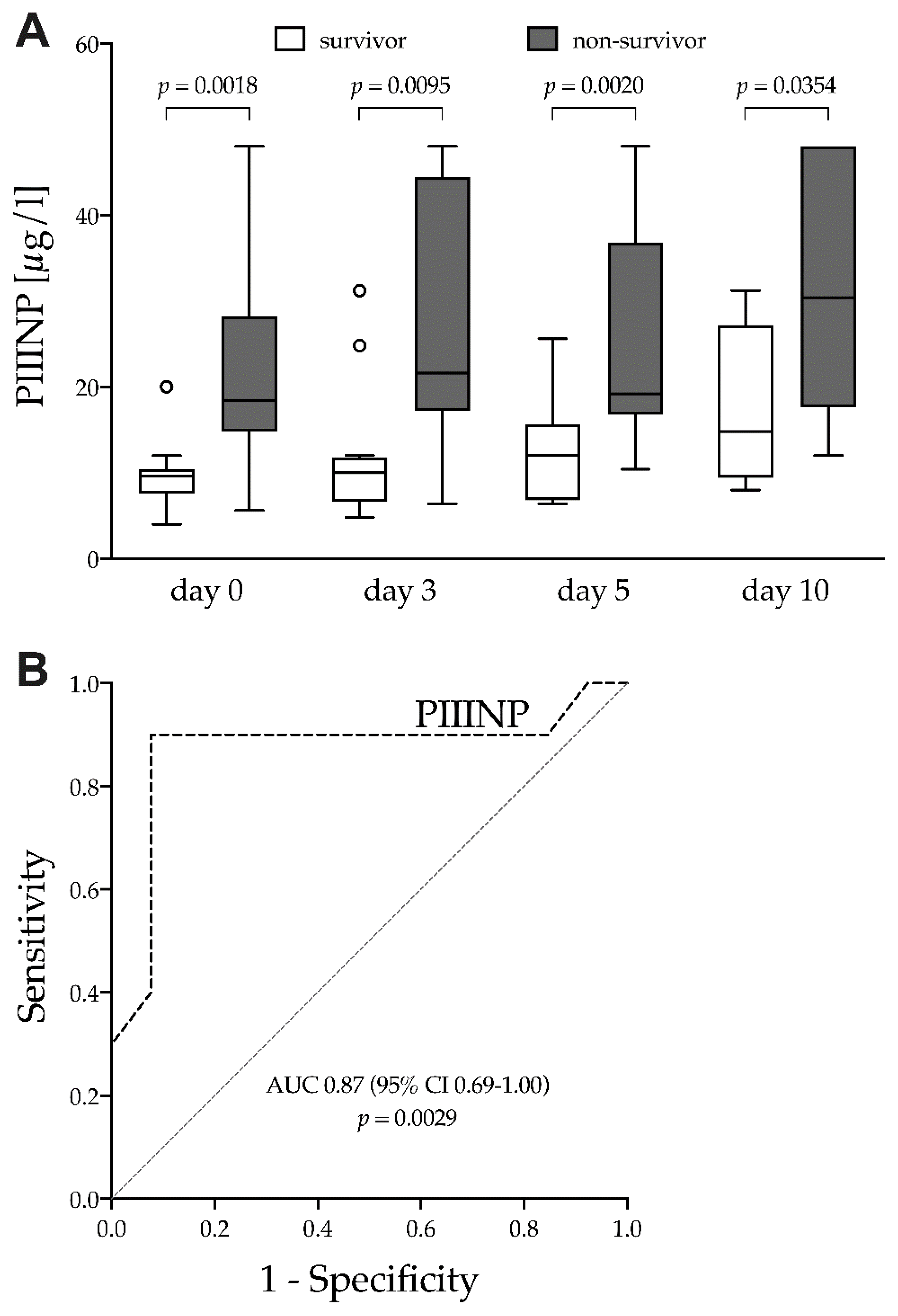
Procollagen I and III
4. Discussion
4.1. Procollagen I and III in ARDS
4.2. ECMO Support and Respiratory Mechanics
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| APACHE II | Acute Physiology and Chronic Health Evaluation II |
| ARDS | acute respiratory distress syndrome |
| AUC | area under the ROC curve |
| BAL | bronchoalveolar lavage fluid |
| CI | confidence interval |
| CRP | C-reactive protein |
| Crs | static compliance of the respiratory system |
| DOR | diagnostic odds ratio |
| ECMO | extracorporeal membrane oxygenation |
| IBW | idealized body weight |
| ICU | intensive care unit |
| LR | likelihood ratio |
| LRT | likelihood ratio test |
| MVNPV | mechanical ventilationnegative predictive value |
| OR | odds ratio |
| PIIINP | N-terminal procollagen III-peptide |
| PINP | N-terminal procollagen I-peptide |
| PaCO2 | arterial partial pressure of carbon dioxide |
| PaO2 | arterial partial pressure of oxygen |
| PCT | procalcitonin |
| PEEP | positive end-expiratory pressure |
| Pplat | end-inspiratory plateau pressure |
| PPV | positive predictive value |
| PRESERVE | Predicting Death for Severe ARDS on vv-ECMO |
| RESP | Respiratory ECMO Survival Prediction |
| ROC | Receiver operating characteristics |
| RR | respiratory rate |
| SaO2 | arterial oxygen saturation |
| SAPS II | Simplified Acute Physiology Score |
| Se | sensitivity |
| Sp | specificity |
| SOFA | Sequential Organ Failure Assessment |
| VT | tidal volume |
| WBC | white blood cell count |
References
- Wilson, J.G.; Calfee, C.S. ARDS Subphenotypes: Understanding a Heterogeneous Syndrome. Crit. Care (Lond. Engl.) 2020, 24, 102. [Google Scholar] [CrossRef] [Green Version]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients with Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef]
- Phua, J.; Badia, J.R.; Adhikari, N.K.; Friedrich, J.O.; Fowler, R.A.; Singh, J.M.; Scales, D.C.; Stather, D.R.; Li, A.; Jones, A.; et al. Has mortality from acute respiratory distress syndrome decreased over time? A systematic review. Am. J. Respir. Crit. Care Med. 2009, 179, 220–227. [Google Scholar] [CrossRef] [Green Version]
- Villar, J.; Blanco, J.; Kacmarek, R.M. Current incidence and outcome of the acute respiratory distress syndrome. Curr. Opin. Crit. Care 2016, 22, 1–6. [Google Scholar] [CrossRef]
- Thompson, B.T.; Chambers, R.C.; Liu, K.D. Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2017, 377, 562–572. [Google Scholar] [CrossRef] [PubMed]
- Abrams, D.; Brodie, D. Extracorporeal Membrane Oxygenation for Adult Respiratory Failure: 2017 Update. Chest 2017, 152, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoué, S.; Guervilly, C.; Da Silva, D.; Zafrani, L.; Tirot, P.; Veber, B.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2018, 378, 1965–1975. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Brodie, D.; Strassmann, S.; Stoelben, E.; Philipp, A.; Bein, T.; Müller, T.; Windisch, W. Extracorporeal membrane oxygenation: Evolving epidemiology and mortality. Intensive Care Med. 2016, 42, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Fessler, J.H.; Fessler, L.I. Biosynthesis of procollagen. Annu. Rev. Biochem. 1978, 47, 129–162. [Google Scholar] [CrossRef]
- Rocco, P.R.M.; Negri, E.M.; Kurtz, P.M.; Vasconcellos, F.P.; Silva, G.H.; Capelozzi, V.L.; Romero, P.V.; Zin, W.A. Lung tissue mechanics and extracellular matrix remodeling in acute lung injury. Am. J. Respir. Crit. Care Med. 2001, 164, 1067–1071. [Google Scholar] [CrossRef]
- Pelosi, P.; Rocco, P.R. Effects of mechanical ventilation on the extracellular matrix. Intensive Care Med. 2008, 34, 631–639. [Google Scholar] [CrossRef]
- Kivirikko, K.I.; Myllyla, R. Post-translational processing of procollagens. Ann. N. Y. Acad. Sci. 1985, 460, 187–201. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Lopez, A.; García-Prieto, E.; Batalla-Solís, E.; Amado-Rodríguez, L.; Avello, N.; Blanch, L.; Albaiceta, G.M. Lung strain and biological response in mechanically ventilated patients. Intensive Care Med. 2012, 38, 240–247. [Google Scholar] [CrossRef]
- Horslev-Petersen, K. Circulating extracellular matrix components as markers for connective tissue response to inflammation. A clinical and experimental study with special emphasis on serum aminoterminal type III procollagen peptide in rheumatic diseases. Dan. Med. Bull. 1990, 37, 308–329. [Google Scholar]
- Kirk, J.M.; Bateman, E.D.; Haslam, P.L.; Laurent, G.J.; Turner-Warwick, M. Serum type III procollagen peptide concentration in cryptogenic fibrosing alveolitis and its clinical relevance. Thorax 1984, 39, 726–732. [Google Scholar] [CrossRef] [Green Version]
- Rocco, P.R.M.; Souza, A.B.; Faffe, D.S.; Pássaro, C.P.; Santos, F.B.; Negri, E.M.; Lima, J.G.M.; Contador, R.S.; Capelozzi, V.L.; Zin, W.A. Effect of corticosteroid on lung parenchyma remodeling at an early phase of acute lung injury. Am. J. Respir. Crit. Care Med. 2003, 168, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Santos, F.B.; Nagato, L.K.S.; Boechem, N.M.; Negri, E.M.; Guimaraes, A.; Capelozzi, V.L.; Faffe, D.S.; Zin, W.A.; Rocco, P.R.M. Time course of lung parenchyma remodeling in pulmonary and extrapulmonary acute lung injury. J. Appl. Physiol. 2006, 100, 98–106. [Google Scholar] [CrossRef]
- Forel, J.-M.; Guervilly, C.; Hraiech, S.; Voillet, F.; Thomas, G.; Somma, C.; Secq, V.; Farnarier, C.; Payan, M.-J.; Donati, S.-Y.; et al. Type III procollagen is a reliable marker of ARDS-associated lung fibroproliferation. Intensive Care Med. 2015, 41, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kropf, J.; Grobe, E.; Knoch, M.; Lammers, M.; Gressner, A.M.; Lennartz, H. The prognostic value of extracellular matrix component concentrations in serum during treatment of adult respiratory distress syndrome with extracorporeal CO2 removal. Eur. J. Clin. Chem. Clin. Biochem. 1991, 29, 805–812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Entzian, P.; Huckstadt, A.; Kreipe, H.; Barth, J. Determination of serum concentrations of type III procollagen peptide in mechanically ventilated patients. Pronounced augmented concentrations in the adult respiratory distress syndrome. Am. Rev. Respir. Dis. 1990, 142, 1079–1082. [Google Scholar] [CrossRef]
- Waydhas, C.; Nast-Kolb, D.; Trupka, A.; Lenk, S.; Duswald, K.H.; Schweiberer, L.; Jochum, M. Increased serum concentrations of procollagen type III peptide in severely injured patients: An indicator of fibrosing activity? Crit. Care Med. 1993, 21, 240–247. [Google Scholar] [CrossRef] [Green Version]
- Marshall, R.P.; Bellingan, G.; Webb, S.; Puddicombe, A.; Goldsack, N.; McAnulty, R.; Laurent, G.J. Fibroproliferation occurs early in the acute respiratory distress syndrome and impacts on outcome. Am. J. Respir. Crit. Care Med. 2000, 162, 1783–1788. [Google Scholar] [CrossRef] [Green Version]
- Clark, J.G.; Milberg, J.A.; Steinberg, K.P.; Hudson, L.D. Type III procollagen peptide in the adult respiratory distress syndrome. Association of increased peptide levels in bronchoalveolar lavage fluid with increased risk for death. Ann. Intern. Med. 1995, 122, 17–23. [Google Scholar] [CrossRef]
- Meduri, G.U.; Tolley, E.A.; Chinn, A.; Stentz, F.; Postlethwaite, A. Procollagen types I and III aminoterminal propeptide levels during acute respiratory distress syndrome and in response to methylprednisolone treatment. Am. J. Respir. Crit. Care Med. 1998, 158 Pt 1, 1432–1441. [Google Scholar] [CrossRef]
- Chesnutt, A.N.; Matthay, M.A.; Tibayan, F.A.; Clark, J.G. Early detection of type III procollagen peptide in acute lung injury. Pathogenetic and prognostic significance. Am. J. Respir. Crit. Care Med. 1997, 156 Pt 1, 840–845. [Google Scholar] [CrossRef] [Green Version]
- Farjanel, J.; Hartmann, D.J.; Guidet, B.; Luquel, L.; Offenstadt, G. Four markers of collagen metabolism as possible indicators of disease in the adult respiratory distress syndrome. Am. Rev. Respir. Dis. 1993, 147, 1091–1099. [Google Scholar] [CrossRef] [PubMed]
- Meduri, G.U.; Annane, D.; Chrousos, G.P.; Marik, P.E.; Sinclair, S.E. Activation and regulation of systemic inflammation in ARDS: Rationale for prolonged glucocorticoid therapy. Chest 2009, 136, 1631–1643. [Google Scholar] [CrossRef] [PubMed]
- Meduri, G.U.; Siemieniuk, R.A.C.; Ness, R.A.; Seyler, S.J. Prolonged low-dose methylprednisolone treatment is highly effective in reducing duration of mechanical ventilation and mortality in patients with ARDS. J. Intensive Care 2018, 6, 53. [Google Scholar] [CrossRef]
- Force, A.D.T.; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Ferguson, N.D.; Fan, E.; Camporota, L.; Antonelli, M.; Anzueto, A.; Beale, R.; Brochard, L.; Brower, R.; Esteban, A.; Gattinoni, L.; et al. The Berlin definition of ARDS: An expanded rationale, justification, and supplementary material. Intensive Care Med. 2012, 38, 1573–1582. [Google Scholar] [CrossRef] [PubMed]
- ELSO. Guidelines for Adult Respiratory Failure; ELSO: Ann Arbor, MI, USA, 2017. [Google Scholar]
- Mauri, T.; Grasselli, G.; Suriano, G.; Eronia, N.; Spadaro, S.; Turrini, C.; Patroniti, N.; Bellani, G.; Pesenti, A. Control of Respiratory Drive and Effort in Extracorporeal Membrane Oxygenation Patients Recovering from Severe Acute Respiratory Distress Syndrome. Anesthesiology 2016, 125, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.; Thijs, L.G.; On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Bailey, M.; Sheldrake, J.; Hodgson, C.; Aubron, C.; Rycus, P.T.; Scheinkestel, C.; Cooper, D.J.; Brodie, D.; Pellegrino, V.; et al. Predicting survival after extracorporeal membrane oxygenation for severe acute respiratory failure. The Respiratory Extracorporeal Membrane Oxygenation Survival Prediction (RESP) score. Am. J. Respir. Crit. Care Med. 2014, 189, 1374–1382. [Google Scholar] [CrossRef]
- Schmidt, M.; Zogheib, E.; Rozé, H.; Repesse, X.; Lebreton, G.; Luyt, C.-E.; Trouillet, J.-L.; Bréchot, N.; Nieszkowska, A.; Dupont, H.; et al. The PRESERVE mortality risk score and analysis of long-term outcomes after extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. Intensive Care Med. 2013, 39, 1704–1713. [Google Scholar] [CrossRef]
- Mandrekar, J.N. Receiver operating characteristic curve in diagnostic test assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef] [Green Version]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models: A framework for traditional and novel measures. Epidemiology 2010, 21, 128–138. [Google Scholar] [CrossRef] [Green Version]
- Glas, A.S.; Lijmer, J.G.; Prins, M.H.; Bonsel, G.J.; Bossuyt, P.M. The diagnostic odds ratio: A single indicator of test performance. J. Clin. Epidemiol. 2003, 56, 1129–1135. [Google Scholar] [CrossRef]
- Altman, D.G.; Machin, D.; Bryant, T.N.; Gardner, M.J. Statistics with Confidence; BMJ Books; Wiley: Hoboken, NJ, USA, 2000; p. 109. [Google Scholar]
- Hsin, C.H.; Wu, M.Y.; Huang, C.C.; Kao, K.C.; Lin, P.J. Venovenous extracorporeal membrane oxygenation in adult respiratory failure: Scores for mortality prediction. Medicine 2016, 95, e3989. [Google Scholar] [CrossRef]
- Brunet, J.; Valette, X.; Buklas, D.; Lehoux, P.; Verrier, P.; Sauneuf, B.; Ivascau, C.; Dalibert, Y.; Seguin, A.; Terzi, N.; et al. Predicting Survival after Extracorporeal Membrane Oxygenation for ARDS: An External Validation of RESP and PRESERVE Scores. Respir. Care 2017, 62, 912–919. [Google Scholar] [CrossRef] [Green Version]
- Steinberg, K.P.; Hudson, L.D.; Goodman, R.B.; Hough, C.L.; Lanken, P.N.; Hyzy, R.; Thompson, B.T.; Ancukiewicz, M.; National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network. Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome. N. Engl. J. Med. 2006, 354, 1671–1684. [Google Scholar]
- Neto, A.S.; Schmidt, M.; Azevedo, L.C.; Bein, T.; Brochard, L.; Beutel, G.; Combes, A.; Costa, E.L.; Hodgson, C.; Lindskov, C.; et al. Associations between ventilator settings during extracorporeal membrane oxygenation for refractory hypoxemia and outcome in patients with acute respiratory distress syndrome: A pooled individual patient data analysis: Mechanical ventilation during ECMO. Intensive Care Med. 2016, 42, 1672–1684. [Google Scholar] [CrossRef]
- Schmidt, M.; Pham, T.; Arcadipane, A.; Agerstrand, C.; Ohshimo, S.; Pellegrino, V.; Vuylsteke, A.; Guervilly, C.; McGuinness, S.; Pierard, S.; et al. Mechanical Ventilation Management during Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome. An International Multicenter Prospective Cohort. Am. J. Respir. Crit. Care Med. 2019, 200, 1002–1012. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.; Papazian, L.; Payan, M.J.; Saux, P.; Gouin, F. Pulmonary fibrosis correlates with outcome in adult respiratory distress syndrome. A study in mechanically ventilated patients. Chest 1995, 107, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Papazian, L.; Doddoli, C.; Chetaille, B.; Gernez, Y.; Thirion, X.; Roch, A.; Donati, Y.; Bonnety, M.; Zandotti, C.; Thomas, P. A contributive result of open-lung biopsy improves survival in acute respiratory distress syndrome patients. Crit. Care Med. 2007, 35, 755–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dos Santos, C.C. Advances in mechanisms of repair and remodelling in acute lung injury. Intensive Care Med. 2008, 34, 619–630. [Google Scholar] [CrossRef]
- Meduri, G.U.; Eltorky, M.A. Understanding ARDS-associated fibroproliferation. Intensive Care Med. 2015, 41, 517–520. [Google Scholar] [CrossRef]
- Calfee, C.S.; Delucchi, K.; Parsons, P.E.; Thompson, B.T.; Ware, L.B.; Matthay, M.A. Subphenotypes in acute respiratory distress syndrome: Latent class analysis of data from two randomised controlled trials. Lancet Respir. Med. 2014, 2, 611–620. [Google Scholar] [CrossRef] [Green Version]
- Calfee, C.S.; Delucchi, K.L.; Sinha, P.; Matthay, M.A.; Hackett, J.; Shankar-Hari, M.; McDowell, C.; Laffey, J.; O’Kane, C.; McAuley, D.; et al. Acute respiratory distress syndrome subphenotypes and differential response to simvastatin: Secondary analysis of a randomised controlled trial. Lancet Respir. Med. 2018, 6, 691–698. [Google Scholar] [CrossRef] [Green Version]
- Famous, K.R.; Delucchi, K.; Ware, L.B.; Kangelaris, K.N.; Liu, K.; Thompson, B.T.; Calfee, C.S. Acute Respiratory Distress Syndrome Subphenotypes Respond Differently to Randomized Fluid Management Strategy. Am. J. Respir. Crit. Care Med. 2017, 195, 331–338. [Google Scholar] [CrossRef]
- Sinha, P.; Network, F.T.N.A.; Delucchi, K.L.; Thompson, B.T.; McAuley, D.; Matthay, M.A.; Calfee, C.S. Latent class analysis of ARDS subphenotypes: A secondary analysis of the statins for acutely injured lungs from sepsis (SAILS) study. Intensive Care Med. 2018, 44, 1859–1869. [Google Scholar] [CrossRef] [Green Version]
- Sinha, P.; Delucchi, K.L.; McAuley, D.F.; O’Kane, C.M.; Matthay, M.A.; Calfee, C.S. Development and validation of parsimonious algorithms to classify acute respiratory distress syndrome phenotypes: A secondary analysis of randomised controlled trials. Lancet Respir. Med. 2020, 8, 247–257. [Google Scholar] [CrossRef]
- Pinto, E.; Santos, R.S.; Antunes, M.A.; Maia, L.A.; Padilha, G.A.; Machado, J.D.A.; Carvalho, A.C.F.; Fernandes, M.V.S.; Capelozzi, V.L.; de Abreu, M.G.; et al. Static and Dynamic Transpulmonary Driving Pressures Affect Lung and Diaphragm Injury during Pressure-controlled versus Pressure-support Ventilation in Experimental Mild Lung Injury in Rats. Anesthesiology 2020, 132, 307–320. [Google Scholar] [CrossRef] [PubMed]
- Santos, C.L.; Moraes, L.; Santos, R.S.; Samary, C.D.S.; Silva, J.D.; Morales, M.M.; Capelozzi, V.L.; De Abreu, M.G.; Schanaider, A.; Silva, P.L.; et al. The biological effects of higher and lower positive end-expiratory pressure in pulmonary and extrapulmonary acute lung injury with intra-abdominal hypertension. Crit. Care 2014, 18, R121. [Google Scholar] [CrossRef] [Green Version]
- Santos, C.L.; Moraes, L.; Santos, R.S.; Oliveira, M.G.; Silva, J.D.; Maron-Gutierrez, T.; Ornellas, D.S.; Morales, M.M.; Capelozzi, V.L.; Jamel, N.; et al. Effects of different tidal volumes in pulmonary and extrapulmonary lung injury with or without intraabdominal hypertension. Intensive Care Med. 2012, 38, 499–508. [Google Scholar] [CrossRef]
- Marhong, J.D.; Munshi, L.; Detsky, M.; Telesnicki, T.; Fan, E. Mechanical ventilation during extracorporeal life support (ECLS): A systematic review. Intensive Care Med. 2015, 41, 994–1003. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.B.P.; Meade, M.O.; Slutsky, A.S.; Brochard, L.; Costa, E.L.V.; Schoenfeld, D.A.; Stewart, T.E.; Briel, M.; Talmor, D.S.; Mercat, A.; et al. Driving pressure and survival in the acute respiratory distress syndrome. N. Engl. J. Med. 2015, 372, 747–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demoule, A.; Decailliot, F.; Jonson, B.; Christov, C.; Maitre, B.; Touqui, L.; Brochard, L.; Delclaux, C. Relationship between pressure-volume curve and markers for collagen turn-over in early acute respiratory distress syndrome. Intensive Care Med. 2006, 32, 413–420. [Google Scholar] [CrossRef]
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network. Comparison of two fluid-management strategies in acute lung injury. N. Engl. J. Med. 2006, 354, 2564–2575. [Google Scholar] [CrossRef] [PubMed]
- Terragni, P.; Rosboch, G.; Tealdi, A.; Corno, E.; Menaldo, E.; Davini, O.; Gandini, G.; Herrmann, P.; Mascia, L.; Quintel, M.; et al. Tidal hyperinflation during low tidal volume ventilation in acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2007, 175, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Rozencwajg, S.; Guihot, A.; Franchineau, G.; Lescroat, M.; Bréchot, N.; Hékimian, G.; Lebreton, G.; Autran, B.; Luyt, C.-E.; Combes, A.; et al. Ultra-Protective Ventilation Reduces Biotrauma in Patients on Venovenous Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. Crit. Care Med. 2019, 47, 1505–1512. [Google Scholar] [CrossRef] [PubMed]
- Krebs, J.; Kolz, A.; Tsagogiorgas, C.; Pelosi, P.; Rocco, P.R.; Luecke, T. Effects of lipopolysaccharide-induced inflammation on initial lung fibrosis during open-lung mechanical ventilation in rats. Respir. Physiol. Neurobiol. 2015, 212–214, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Domenici, L.; Pieri, L.; Galle, M.B.; Romagnoli, P.; Adembri, C. Evolution of endotoxin-induced lung injury in the rat beyond the acute phase. Pathobiology 2004, 71, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Keshari, R.S.; Silasi-Mansat, R.; Zhu, H.; Popescu, N.I.; Peer, G.; Chaaban, H.; Lambris, J.D.; Polf, H.; Lupu, C.; Kinasewitz, G.; et al. Acute lung injury and fibrosis in a baboon model of Escherichia coli sepsis. Am. J. Respir. Cell Mol. Biol. 2014, 50, 439–450. [Google Scholar]
- Madtes, D.K.; Rubenfeld, G.; Klima, L.D.; Milberg, J.A.; Steinberg, K.P.; Martin, T.R.; Raghu, G.; Hudson, L.D.; Clark, J.G. Elevated transforming growth factor-alpha levels in bronchoalveolar lavage fluid of patients with acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 1998, 158, 424–430. [Google Scholar] [CrossRef] [Green Version]
- Coalson, J.J.; Winter, V.T.; Siler-Khodr, T.; Yoder, B.A. Neonatal chronic lung disease in extremely immature baboons. Am. J. Respir. Crit. Care Med. 1999, 160, 1333–1346. [Google Scholar] [CrossRef] [Green Version]
- Yoder, B.A.; Siler-Khodr, T.; Winter, V.T.; Coalson, J.J. High-frequency oscillatory ventilation: Effects on lung function, mechanics, and airway cytokines in the immature baboon model for neonatal chronic lung disease. Am. J. Respir. Crit. Care Med. 2000, 162, 1867–1876. [Google Scholar] [CrossRef] [Green Version]
- Krebs, J.; Pelosi, P.; Tsagogiorgas, C.; Haas, J.; Yard, B.; Rocco, P.R.; Luecke, T. Time course of lung inflammatory and fibrogenic responses during protective mechanical ventilation in healthy rats. Respir. Physiol. Neurobiol. 2011, 178, 323–328. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| ICU Survivor (n = 13) | ICU Non-Survivor (n = 10) | p-Value | |
|---|---|---|---|
| Sex (male) | 11 (85%) | 4 (40%) | 0.0393 |
| Age (years) | 54.2 ± 9.2 | 59.7 ± 9.4 | 0.1695 |
| Height (cm) | 177.7 ± 9.6 | 171.8 ± 8.9 | 0.1477 |
| Body weight (kg) | 104.5 ± 17.6 | 95.4 ± 19.6 | 0.2569 |
| Body mass index (kg/m2) | 33.5 ± 7.6 | 32.7 ± 8.5 | 0.8262 |
| Main cause of ARDS (n (%)) | |||
| Pneumonia | 12 (92) | 7 (70) | 0.5596 |
| Aspiration | 0 (0) | 1 (10) | 0.4348 |
| Extrapulmonary-sepsis | 1 (8) | 2 (20) | 0.5596 |
| SAPS II | 67.4 ± 14.0 | 72.4 ± 6.6 | 0.3096 |
| SOFA | 13.3 ± 3.6 | 15.5 ± 2.7 | 0.1265 |
| APACHE II | 28.7 ± 8.5 | 31.9 ± 4.1 | 0.2852 |
| RESP | −4.0 ± 4.3 | −5.9 ± 4.7 | 0.3256 |
| PRESERVE | 5.1 ± 2.2 | 5.6 ± 2.2 | 0.5773 |
| MV prior to inclusion (days) | 4.5 ± 2.7 | 6.9 ± 4.1 | 0.1415 |
| Transferred from external hospital | 5/13 | 6/10 | 0.8790 |
| Salvage ECMO | 2/13 | 3/10 | 0.7443 |
| Driving pressure before ECMO | 18.4 ± 5.3 | 17.7 ± 4.2 | 0.2891 |
| P/F-ratio prior to ECMO | 87.1 ± 23.6 | 79.1 ± 27.8 | 0.3564 |
| Prone positioning before ECMO | 6/13 | 6/10 | 0.1459 |
| Neuromuscular blocking agents before ECMO | 11/13 | 10/10 | 0.8995 |
| Dialysis/CRRT before ECMO | 3/13 | 2/10 | 0.4378 |
| Duration of ECMO support (days) | 11.2 ± 2.9 | 16.4 ± 8.1 | 0.0437 |
| ICU length of stay (days) | 37.0 (32–73) | 24.0 (15.8–33.5) | 0.0039 |
| Sensitivity (%) | Specificity (%) | Positive Predictive Value (%) | Negative Predictive Value (%) | Likelihood Ratio Positive | Likelihood Ratio Negative | Diagnostic Odds Ratio | |
|---|---|---|---|---|---|---|---|
| PIIINP >12.8 µg/L | 90.0 (59.6–99.5) | 92.3 (66.7–99.6) | 90.0 (59.6–99.5) | 92.3 (66.7–99.6) | 11.7 (1.7–77.8) | 0.1 (0.02–0.7) | 108 (5.9–1969.5) |
| Number of Patients | TP | TN | FP | FN | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Diagnostic Odds Ratio | |
|---|---|---|---|---|---|---|---|---|---|---|
| PIIINP >8.4 µg/L | 18 | 9 | 4 | 9 | 1 | 90.0 (59.6–99.5) | 30.7 (12.7–57.6) | 50.0 (39.7–60.3) | 34.4 (34.5–76.8) | 4.0 (0.4–43.1) |
| PIIINP >12.8 µg/L | 10 | 9 | 12 | 1 | 1 | 90.0 (59.6–99.5) | 92.3 (66.7–99.6) | 90.0 (59.6–99.5) | 92.3 (66.7–99.6) | 108 (5.9–1969.5) |
| PIIINP >14.4 µg/L | 9 | 8 | 12 | 1 | 2 | 80.0 (49.0–96.5) | 92.3 (66.7–99.6) | 88.9 (54.3–98.2) | 85.7 (63.2–95.4) | 48.0 (3.7–622.0) |
| PIIINP >19.2 µg/L | 5 | 4 | 12 | 1 | 6 | 40.0 (16.8–68.7) | 92.3 (66.7–99.6) | 80.0 (34.4–96.8) | 66.7 (54.1–77.3) | 8.0 (0.7–88.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boesing, C.; Graf, P.T.; Thiel, M.; Luecke, T.; Krebs, J. Procollagen I and III as Prognostic Markers in Patients Treated with Extracorporeal Membrane Oxygenation: A Prospective Observational Study. J. Clin. Med. 2021, 10, 3686. https://doi.org/10.3390/jcm10163686
Boesing C, Graf PT, Thiel M, Luecke T, Krebs J. Procollagen I and III as Prognostic Markers in Patients Treated with Extracorporeal Membrane Oxygenation: A Prospective Observational Study. Journal of Clinical Medicine. 2021; 10(16):3686. https://doi.org/10.3390/jcm10163686
Chicago/Turabian StyleBoesing, Christoph, Peter T. Graf, Manfred Thiel, Thomas Luecke, and Joerg Krebs. 2021. "Procollagen I and III as Prognostic Markers in Patients Treated with Extracorporeal Membrane Oxygenation: A Prospective Observational Study" Journal of Clinical Medicine 10, no. 16: 3686. https://doi.org/10.3390/jcm10163686