
Laparoscopic Vaginoplasty Procedure Using a Modified Peritoneal Pull-Down Technique with Uterine Strand Incision in Patients with Mayer–Rokitansky–Küster–Hauser Syndrome: Kisu Modification

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
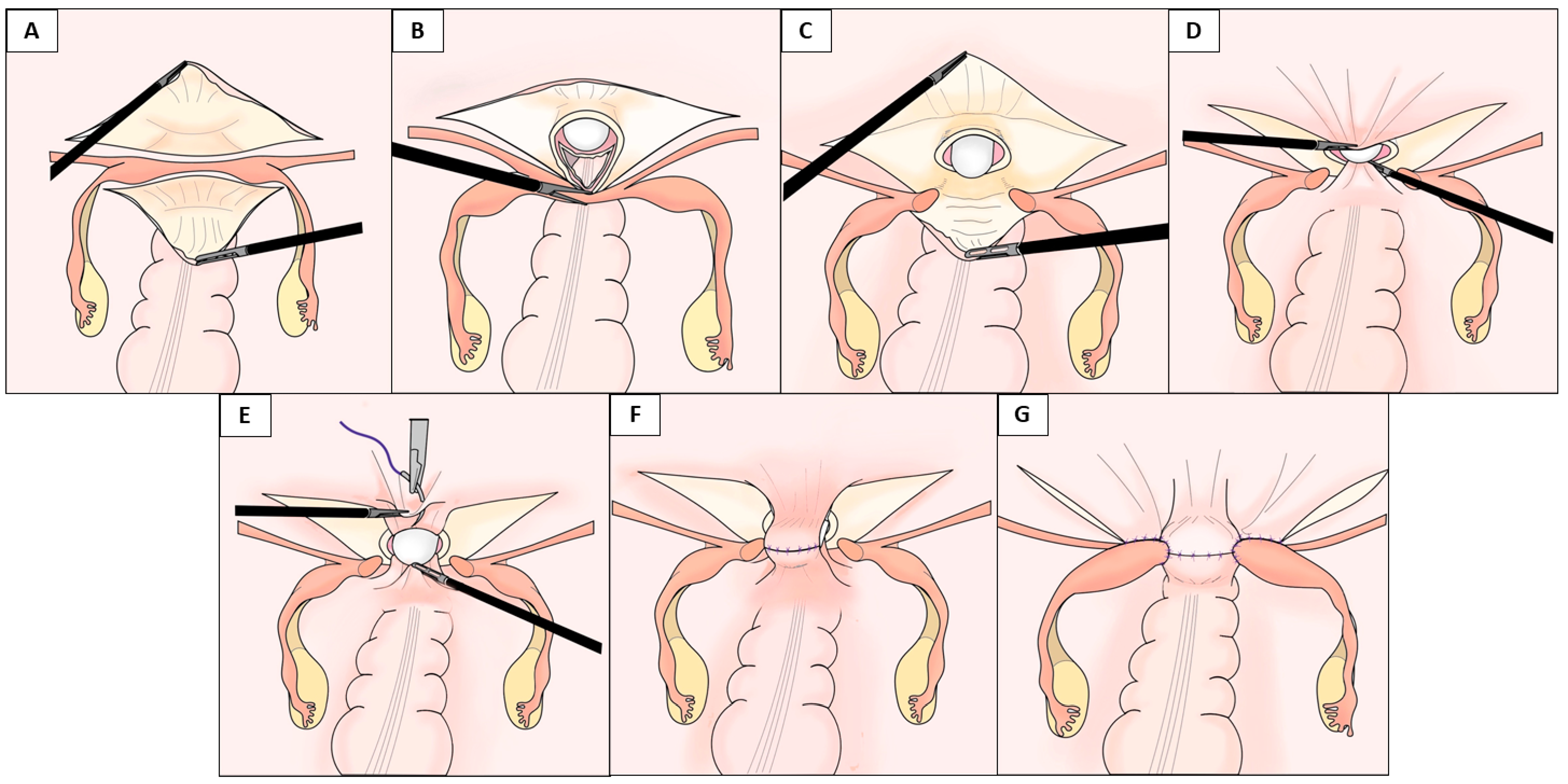
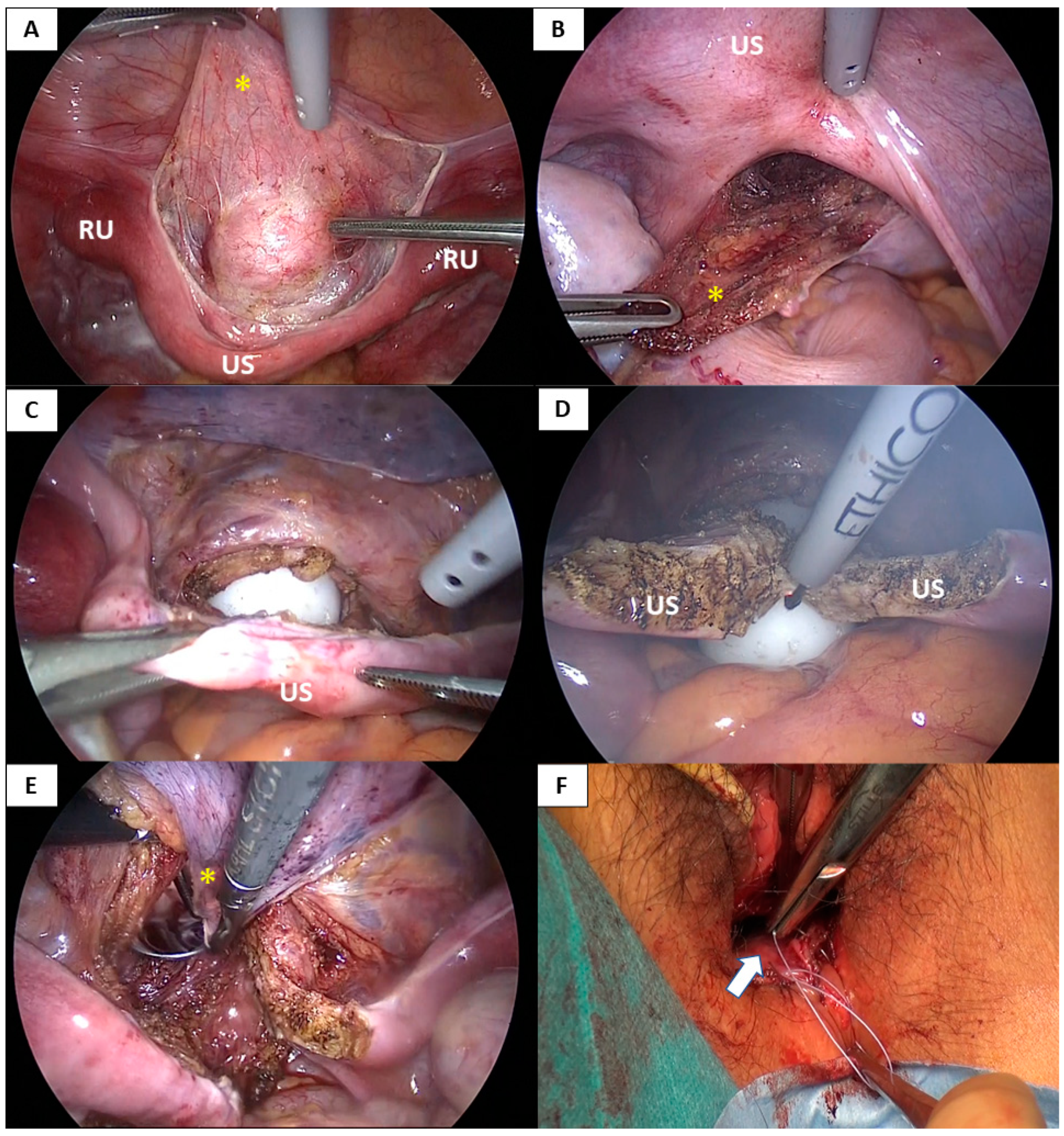
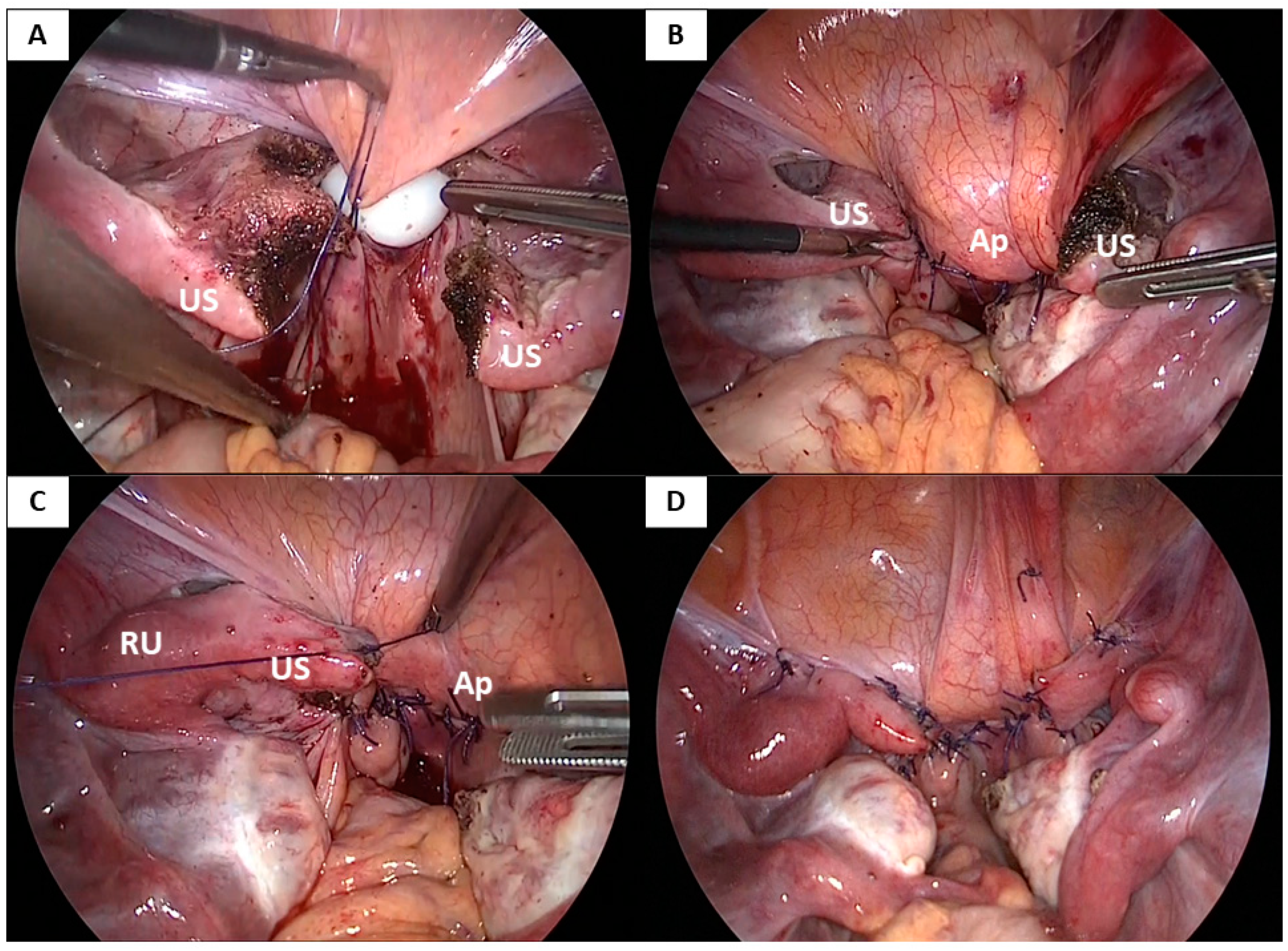
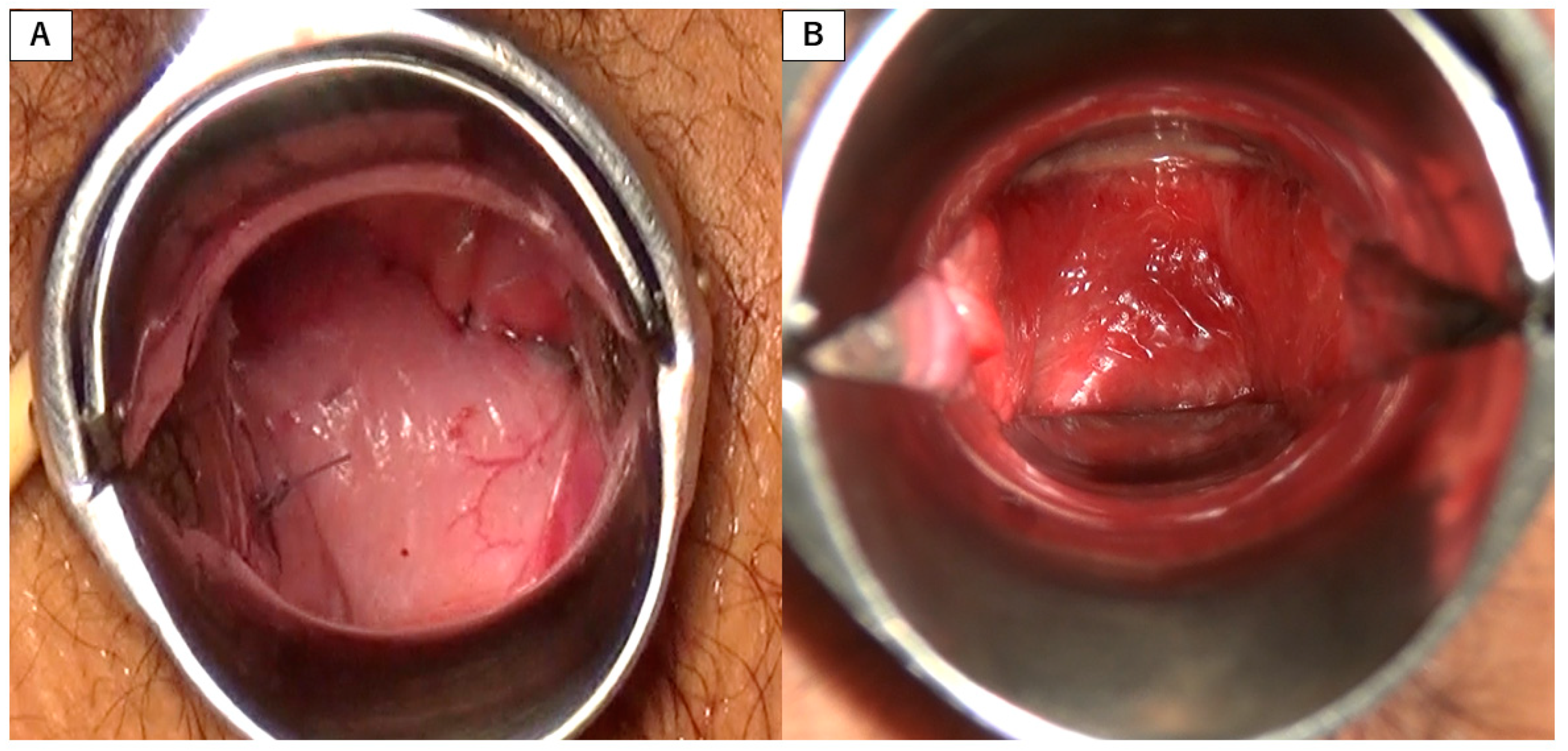
2.2. Surgical Procedure
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brännström, M.; Johannesson, L.; Bokström, H.; Kvarnström, N.; Mölne, J.; Dahm-Kähler, P.; Enskog, A.; Milenkovic, M.; Ekberg, J.; Diaz-Garcia, C.; et al. Livebirth after uterus transplantation. Lancet 2015, 385, 607–616. [Google Scholar] [CrossRef] [Green Version]
- Callens, N.; De Cuypere, G.; De Sutter, P.; Monstrey, S.; Weyers, S.; Hoebeke, P.; Cools, M. An update on surgical and non-surgical treatments for vaginal hypoplasia. Hum. Reprod. Update 2014, 20, 775–801. [Google Scholar] [CrossRef]
- Cheikhelard, A.; Bidet, M.; Baptiste, A.; Viaud, M.; Fagot, C.; Khen-Dunlop, N.; Louis-Sylvestre, C.; Sarnacki, S.; Touraine, P.; Elie, C.; et al. Surgery is not superior to dilation for the management of vaginal agenesis in Mayer-Rokitansky-Küster-Hauser syndrome: A multicenter comparative observational study in 131 patients. Am. J. Obstet. Gynecol. 2018, 219, 281.e1–281.e9. [Google Scholar] [CrossRef]
- Soong, Y.K.; Chang, F.H.; Lai, Y.M.; Lee, C.L.; Chou, H.H. Results of modified laparoscopically assisted neovaginoplasty in 18 patients with congenital absence of vagina. Hum. Reprod. 1996, 11, 200–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willemsen, W.N.; Kluivers, K.B. Long-term results of vaginal construction with the use of Frank dilation and a peritoneal graft (Davydov procedure) in patients with Mayer-Rokitansky-Küster syndrome. Fertil Steril. 2015, 103, 220–227.e1. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Wang, R.; Wang, Y.; Li, L.; Zhang, H.; Kang, S. Comparison of two laparoscopic peritoneal vaginoplasty techniques in patients with Mayer-Rokitansky-Küster-Hauser syndrome. Int. Urogynecol. J. 2015, 26, 1201–1207. [Google Scholar] [CrossRef] [PubMed]
- Uncu, G.; Özerkan, K.; Ata, B.; Kasapoğlu, I.; Atalay, M.A.; Orhan, A.; Aslan, K. Anatomic and Functional Outcomes of Paramesonephric Remnant-Supported Laparoscopic Double-Layer Peritoneal Pull-Down Vaginoplasty Technique in Patients with Mayer-Rokitansky-Küster-Hauser Syndrome: Uncu Modification. J. Minim. Invasive Gynecol. 2018, 25, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Kisu, I.; Ito, M.; Nakamura, K.; Shiraishi, T.; Iijima, T.; Senba, H.; Matsuda, K.; Hirao, N. New Laparoscopic Vaginoplasty Procedure With a Modified Peritoneal Pull-Down Technique in Four Patients with Mayer-Rokitansky-Küster-Hauser Syndrome. J. Pediatr. Adolesc. Gynecol. 2021, 34, 569–572. [Google Scholar] [CrossRef] [PubMed]
- Fedele, L.; Frontino, G.; Restelli, E.; Ciappina, N.; Motta, F.; Bianchi, S. Creation of a neovagina by Davydov’s laparoscopic modified technique in patients with Rokitansky syndrome. Am. J. Obstet. Gynecol. 2010, 202, 33.e1–33.e6. [Google Scholar] [CrossRef] [PubMed]
- Committee on Adolescent Health Care. ACOG Committee Opinion No. 728: Mullerian Agenesis: Diagnosis, Management, And Treatment. Obstet. Gynecol. 2018, 131, e35–e42. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, D.K.; Rose, G.L.; Lipton, M.G.; Quek, J. Mayer-Rokitansky-Kuster-Hauser syndrome: A review of 245 consecutive cases managed by a multidisciplinary approach with vaginal dilators. Fertil. Steril. 2012, 97, 686–690. [Google Scholar] [CrossRef] [PubMed]
- McQuillan, S.K.; Grover, S.R. Dilation and surgical management in vaginal agenesis: A systematic review. Int. Urogynecol. J. 2014, 25, 299–311. [Google Scholar] [CrossRef] [PubMed]
- Fageeh, W.; Raffa, H.; Jabbad, H.; Marzouki, A. Transplantation of the human uterus. Int. J. Gynaecol. Obstet. 2002, 76, 245–251. [Google Scholar] [CrossRef]
- Brännström, M.; Johannesson, L.; Dahm-Kähler, P.; Enskog, A.; Mölne, J.; Kvarnström, N.; Diaz-Garcia, C.; Hanafy, A.; Lundmark, C.; Marcickiewicz, J.; et al. First clinical uterus transplantation trial: A six-month report. Fertil Steril. 2014, 101, 1228–1236. [Google Scholar] [CrossRef] [PubMed]
- Kölle, A.; Taran, F.A.; Rall, K.; Schöller, D.; Wallwiener, D.; Brucker, S.Y. Neovagina creation methods and their potential impact on subsequent uterus transplantation: A review. BJOG 2019, 126, 1328–1335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chmel, R.; Novackova, M.; Janousek, L.; Matecha, J.; Pastor, Z.; Maluskova, J.; Cekal, M.; Kristek, J.; Olausson, M.; Fronek, J. Revaluation and lessons learned from the first 9 cases of a Czech uterus transplantation trial: Four deceased donor and 5 living donor uterus transplantations. Am. J. Transplant. 2019, 19, 855–864. [Google Scholar] [CrossRef] [PubMed]
- Brännström, M.; Dahm-Kähler, P.; Ekberg, J.; Akouri, R.; Growth, K.; Enskog, A.; Broecker, V.; Mölne, J.; Ayoubi, J.-M.; Kvarnström, N. Outcome of Recipient Surgery and 6-Month Follow-Up of the Swedish Live Donor Robotic Uterus Transplantation Trial. J. Clin. Med. 2020, 9, 2338. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age at Surgery | Postoperative Follow-Up Length (Months) | Vaginal Length at Initial Examination (cm) | Neovaginal Length (cm) | Intraoperative Complications | Sexual Activity | |||
|---|---|---|---|---|---|---|---|---|---|
| at Discharge | Three Months Postoperatively | 6 Months Postoperatively | 12 Months Postoperatively | ||||||
| 1 | 26 | 24 | 1 | 9 | 8 | 8 | 8 | No | Satisfactory |
| 2 | 21 | 23 | Absent | 10.5 | 10.5 | 10.5 | 9.5 | No | Satisfactory |
| 3 | 19 | 15 | Absent | 10.5 | 10.5 | 10 | 9 | No | Satisfactory |
| 4 | 23 | 16 | Absent | 10.5 | 10.5 | 10.5 | 10.5 | No | Not attempted |
| 5 | 34 | 14 | 4 * | 10.5 | 11 | 11.0 | 10.5 | No | Not attempted |
| 6 | 18 | 15 | Absent | 10.5 | 10 | 9 | 9.5 | No | Satisfactory |
| 7 | 16 | 19 | 2.5 | 10.5 | 11 | 11 | 11 | No | Not attempted |
| 8 | 19 | 19 | 2 | 10.5 | 11 | 11 | 11 | No | Not attempted |
| 9 | 36 | 16 | Absent | 10.5 | 10.5 | 11 | 11 | No | Not attempted |
| 10 | 27 | 12 | 2 | 10.5 | 11 | 11 | 11 | No | Satisfactory |
| Mean (±SD) | 23.9 ± 6.5 | 17.3 ± 3.7 | 1.2 ± 1.3 | 10.3 ± 0.5 | 10.4 ± 0.9 | 10.3 ± 1.0 | 10.1 ± 1.0 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kisu, I.; Iida, M.; Nakamura, K.; Banno, K.; Shiraishi, T.; Tokuoka, A.; Yamaguchi, K.; Tanaka, K.; Iijima, M.; Senba, H.; et al. Laparoscopic Vaginoplasty Procedure Using a Modified Peritoneal Pull-Down Technique with Uterine Strand Incision in Patients with Mayer–Rokitansky–Küster–Hauser Syndrome: Kisu Modification. J. Clin. Med. 2021, 10, 5510. https://doi.org/10.3390/jcm10235510
Kisu I, Iida M, Nakamura K, Banno K, Shiraishi T, Tokuoka A, Yamaguchi K, Tanaka K, Iijima M, Senba H, et al. Laparoscopic Vaginoplasty Procedure Using a Modified Peritoneal Pull-Down Technique with Uterine Strand Incision in Patients with Mayer–Rokitansky–Küster–Hauser Syndrome: Kisu Modification. Journal of Clinical Medicine. 2021; 10(23):5510. https://doi.org/10.3390/jcm10235510
Chicago/Turabian StyleKisu, Iori, Miho Iida, Kanako Nakamura, Kouji Banno, Tetsuro Shiraishi, Asahi Tokuoka, Keigo Yamaguchi, Kunio Tanaka, Moito Iijima, Hiroshi Senba, and et al. 2021. "Laparoscopic Vaginoplasty Procedure Using a Modified Peritoneal Pull-Down Technique with Uterine Strand Incision in Patients with Mayer–Rokitansky–Küster–Hauser Syndrome: Kisu Modification" Journal of Clinical Medicine 10, no. 23: 5510. https://doi.org/10.3390/jcm10235510