
Spontaneous Bacterial Peritonitis among Cirrhotic Patients: Prevalence, Clinical Characteristics, and Outcomes

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Patients
3.2. Positive vs. Negative Ascitic Fluid Culture
3.3. Microbial Growth in Ascitic Fluid Culture
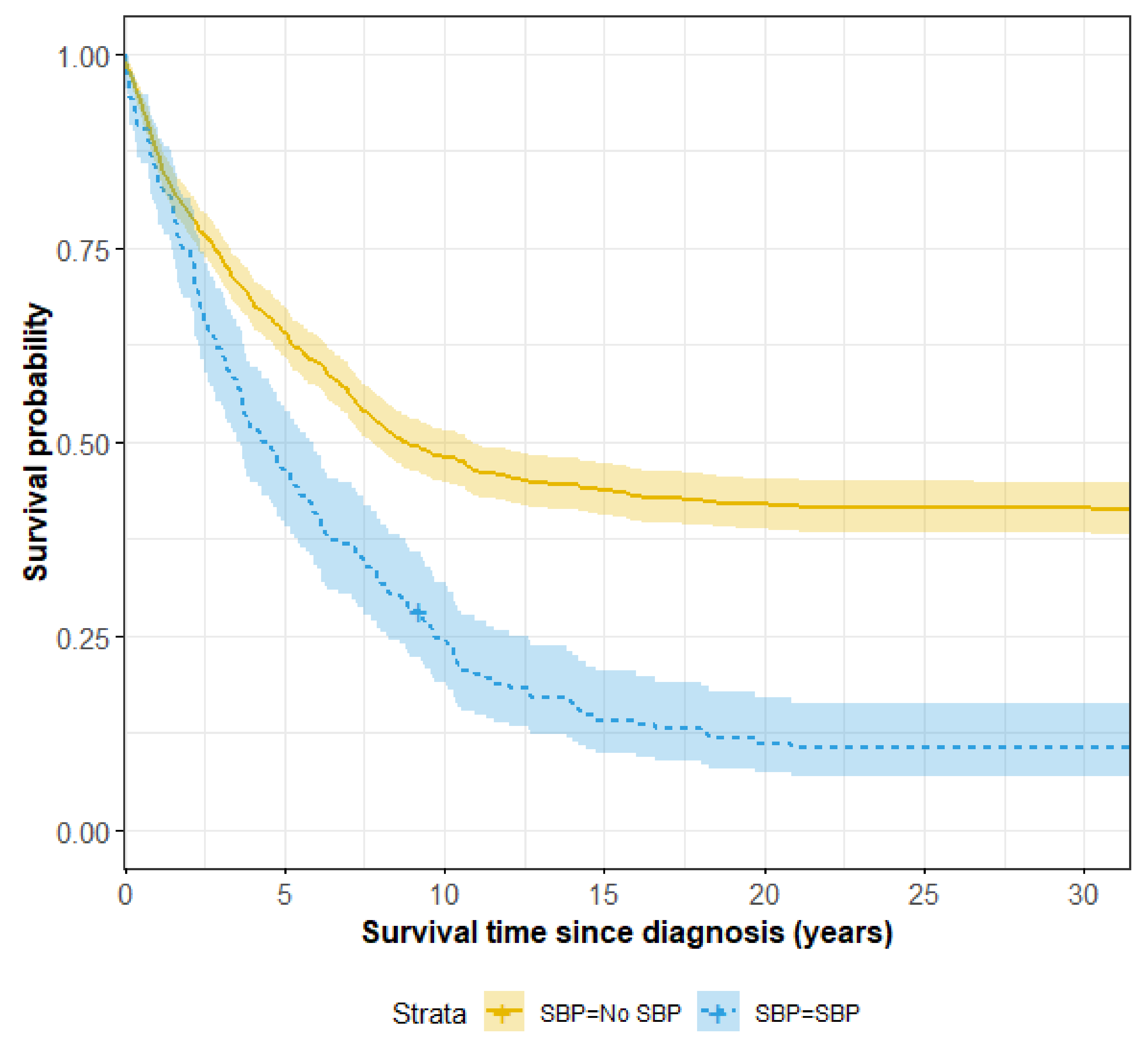
3.4. Survival and Risk Factors for Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Strauss, E. The impact of bacterial infections on survival of patients with decompensated cirrhosis. Ann. Hepatol. 2014, 13, 7–19. [Google Scholar] [CrossRef]
- Ariza, X.; Castellote, J.; Lora-Tamayo, J.; Girbau, A.; Salord, S.; Rota, R.; Xiol, X. Risk factors for resistance to ceftriaxone and its impact on mortality in community, healthcare and nosocomial spontaneous bacterial peritonitis. J. Hepatol. 2012, 56, 825–832. [Google Scholar] [CrossRef]
- Fernandez, J.; Acevedo, J.; Castroetal, M. Prevalence and risk factors of infections by multiresistant bacteria in cirrhosis: A prospectivestudy. Hepatology 2012, 55, 1551–1561. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.M.; Branco, J.C.; Barosa, R.; Rodrigues, J.A.; Ramos, L.; Martins, A.; Karvellas, C.J.; Cardoso, F.S. Clinical and microbiological characteristics associated with mortality in spontaneous bacterial peritonitis: A multicenter cohort study. Eur. J. Gastroenterol. Hepatol. 2016, 28, 1216–1222. [Google Scholar] [CrossRef] [PubMed]
- Costabeber, A.M.; De Mattos, A.A.; Sukiennik, T.C.T. Prevalence of bacterial resistance in hospitalized cirrhotic patients in Southern Brazil: A new challenge. Rev. Inst. Med. Trop. São Paulo 2016, 58, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salerno, F.; Borzio, M.; Pedicino, C.; Simonetti, R.; Rossini, A.; Boccia, S.; Cacciola, I.; Burroughs, A.K.; Manini, M.A.; LA Mura, V.; et al. The impact of infection by multidrug-resistant agents in patients with cirrhosis. A multicenter prospective study. Liver Int. 2016, 37, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Oey, R.C.; de Man, R.A.; Erler, N.S.; Verbon, A.; van Buuren, H.R. Microbiology and antibiotic susceptibility patterns in spontaneous bacterial peritonitis: A study of two Dutch cohorts ata10-year interval. United Eur. Gastroenterol. J. 2018, 6, 614–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almeida, P.R.L.D.; Leão, G.S.; Gonçalves, C.D.G.; Picon, R.V.; Tovo, C.V. Impact of microbiological changes on spontaneous bacterial peritonitis in three different periods over 17 years. Arq. Gastroenterol. 2018, 55, 23–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández, J.; Navasa, M.; Gómez, J.; Colmenero, J.; Vila, J.; Arroyo, V.; Rodés, J. Bacterial infections in cirrhosis: Epidemiological changes with invasive procedures and norfloxacin prophylaxis. Hepatology 2002, 35, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Rimola, A.; García-Tsao, G.; Navasa, M.; Piddock, L.J.; Planas, R.; Bernard, B.; Inadomi, J. Diagnosis, treatment and prophylaxis of spontaneous bacterial peritonitis: A consensus document. J. Hepatol. 2000, 32, 142–153. [Google Scholar] [CrossRef]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piano, S.; Singh, V.; Caraceni, P.; Maiwall, R.; Alessandria, C.; Fernandez, J.; Soares, E.; Kim, D.; Kim, S.; Marino, M.; et al. Epidemiology, predictors and outcomes of multi drug resistant (MDR) bacterial infections in patients with cirrhosis across the world. Final results of the “Global study”. Dig. Liver Dis. 2018, 50, 2–3. [Google Scholar] [CrossRef]
- Oliveira, J.D.C.; Carrera, E.; Petry, R.C.; Deutschendorf, C.; Mantovani, A.; Barcelos, S.T.A.; Cassales, S.; Schacher, F.C.; Lopes, A.B.; Alvares-Da-Silva, M.R. High Prevalence of Multidrug Resistant Bacteria in Cirrhotic Patients with Spontaneous Bacterial Peritonitis: Is It Time to Change the Standard Antimicrobial Approach? Can. J. Gastroenterol. Hepatol. 2019, 2019, 6963910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marciano, S.; Díaz, J.M.; Dirchwolf, M.; Gadano, A. Spontaneous bacterial peritonitis in patients with cirrhosis: Incidence, outcomes, and treatment strategies. Hepatic Med. Évid. Res. 2019, 11, 13–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angeli, P.; Bernardi, M.; Villanueva, C.; Francoz, C.; Mookerjee, R.P.; Trebicka, J.; Krag, A.; Laleman, W.; Gines, P. EASL clinical practice guidelines for the management of patients with decompensated cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Runyon, B.A. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012. Hepatology 2013, 57, 1651–1653. [Google Scholar] [CrossRef] [PubMed]
- Rostkowska, K.A.; Szymanek-Pasternak, A.; Simon, K.A. Spontaneous bacterial peritonitis—Therapeutic challenges in the era of increasing drug resistance of bacteria. Clin. Exp. Hepatol. 2018, 4, 224–231. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | SBP | without SBP | p Value |
|---|---|---|---|
| n = 173 (%) | n = 869 (%) | ||
| Sex—male (%) | (62) 108 | (61) 533 | 0.7 |
| Age—median (IQR) | 60 (58, 76) | 66 (55, 76) | 0.7 |
| Age at diagnosis cirrhosis median (IQR) | 60 (51, 70) | 59 (51, 72) | 0.9 |
| Ethnicity—Bedouin | 16 (9.2) | 78 (9) | 0.9 |
| Etiology of cirrhosis | |||
| Hepatitis B | 13 (7.5) | 89 (10) | 0.3 |
| Hepatitis C | 72 (42) | 314 (36) | 0.2 |
| Fatty liver | 32 (18) | 151 (17) | 0.5 |
| Wilson disease | 0 0 | 6 6 (0.7) | 0.6 |
| Alcoholic liver Disease | 16 (9.2) | 123 (14) | 0.08 |
| Autoimmune Hepatitis | 5 (2.9) | 19 (2.2) | 0.6 |
| PBC | 1 (0.6) | 15 (1.7) | 0.2 |
| PSC | 2 (1.2) | 2 (0.2) | 0.1 |
| Cryptogenic | 17 (9.8) | 83 (9.6) | >0.9 |
| HCV and alcoholic | 9 (5.2) | 32 (3.7) | 0.3 |
| HCV and HBV | 2 (1.2) | 11 (1.3) | >0.9 |
| HBV and alcoholic | 1 (0.6) | 11 (1.3) | 0.7 |
| Liver biopsy | 40 (23) | 221 (26) | 0.5 |
| Esophageal varices | 120 (71) | 452 (53) | <0.001 |
| Esophageal varices bleeding | 67 (41) | 209 (26) | <0.001 |
| Hepatocellular carcinoma (HCC) | 22 (13) | 128 (15) | 0.5 |
| Liver Transplantation | 13 (7.6) | 43 (5) | 0.2 |
| Death | 157 (91) | 515 (60) | <0.001 |
| Age at death, Median (IQR) | 66 (55, 76) | 68 (59, 78) | 0.2 |
| Hb (gr/dL) | 9.3 (8.3, 11) | 11.2 (9.2, 3.2) | <0.001 |
| WBC (103/uL) | 8 (5, 14) | 7 (5, 10) | 0.008 |
| PLT (103/uL) | 80 (48, 130) | 109 (72, 163) | <0.001 |
| ALT (U/L) | 30 (16, 58) | 27 (17, 50) | 0.5 |
| AST (U/L) | 64 (33, 109) | 43 (28, 84) | 0.001 |
| Alkaline Phosphatase (U/L) | 132 (85, 216) | 114 (84, 178) | 0.036 |
| GGT (U/L) | 56 (27, 121) | 66 (34, 148) | 0.015 |
| Bili total (mg/dL), Last value | 2.5 (1.5, 6.8) | 1.4 (0.8, 3.1) | <0.001 |
| Bili total (mg/dL), At diagnosis | 1.3 (0.9, 2.3) | 1.2 (0.7, 2) | 0.043 |
| Albumin (gr/dL), Last value | 2.5 (2.0, 3.0) | 2.9 (2.3, 3.8) | <0.001 |
| Albumin (gr/dL), At diagnosis | 3.2 (2.8, 3.6) | 3.4 (2.9, 4.0) | <0.001 |
| INR, Last value | 1.7 (1.3, 2.4) | 1.3 (1.1, 1.7) | <0.001 |
| INR, At diagnosis | 1.3 (1.1, 1.5) | 1.2 (1.0, 1.4) | <0.001 |
| Characteristics | Negative Culture Neutrocytic Ascites n = 91 (%) | Positive Culture n = 82 (%) | p-Value |
|---|---|---|---|
| S–male | 50 (55) | 59 (72) | 0.018 |
| Age | 68 (58, 77) | 64 (54, 75) | 0.066 |
| Age at diagnosis | 62 (53, 74) | 58 (48, 67) | 0.033 |
| Ethnicity | 7 (7.8) | 8 (9.8) | 0.8 |
| Etiology of Cirrhosis | |||
| Hepatitis B | 9 (9.9%) | 4 (4.9%) | 0.2 |
| Hepatitis C | 44 (48.3%) | 28 (34%) | 0.05 |
| Fatty Liver | 14 (15%) | 19 (23%) | 0.2 |
| Alcoholic Liver Cirrhosis | 7 (7.8%) | 9 (11%) | 0.5 |
| Cryptogenic | 10 (11%) | 6 (7.7%) | |
| Liver Biopsy | 17 (18.7%) | 23 (28%) | 0.14 |
| Esophageal Varices | 58 (63.7%) | 61 (74%) | 0.3 |
| Esophageal Varices Bleeding | 27 (29.7%) | 39 (49%) | 0.034 |
| HCC | 12 (13%) | 10 (12%) | 0.8 |
| Acute renal failure | 35 (38.5) | 46 (56) | 0.023 |
| Death | 81 (89%) | 74 (90%) | >0.9 |
| HB | 10.00 (8.8, 11.17) | 9.00 (7.90, 10.47) | 0.001 |
| WBC | 9 (5, 13) | 7 (4, 14) | 0.2 |
| PLT | 94 (55, 143) | 66 (44, 117) | 0.011 |
| INR last Value | 1.55 (1.30, 2.08) | 1.7 (1.40, 2.58) | 0.029 |
| INR at diagnosis | 1.30 (1.2, 1.50) | 1.30 (1.10, 1.50) | 0.4 |
| Child-Pugh Score last value | 10 (9, 12) | 11 (9, 12) | 0.020 |
| Child-Pugh Stage last | 0.091 | ||
| A | 10 (11%) | 4 (4.9%) | |
| B | 30 (33%) | 20 (24%) | |
| C | 52 (57%) | 58 (71%) |
| Antibiotics Resistance | E. coli n = 31 | Klebsiella n = 4 | Pseudomonas n = 1 | Strep. pneum n = 4 | Staph. areus n = 7 | CONS, n = 13 | Citrobacter n = 2 | Acinetobacter n = 3 | Enterobacter n = 2 | Enterococcus n = 6 | Strepviridans n = 4 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ampicillin | 22 (71%) | 4 (100%) | 0 | 2 (18%) | 2 (100%) | 2 (67%) | 1 (100%) | 3 (50) | 0 | ||
| Cefuroxime | 16 (52%) | 2 (50%) | 0 | 1 (25%) | 2 (18%) | 1 (50%) | 2 (100%) | 2 (100%) | 0 | ||
| Rocephin | 16 (52%) | 2 (50%) | 0 | 1 (20%) | 2 (18%) | 1 (50%) | 2 (100%) | 1 (50%) | 0 | ||
| Ceftazidime | 16 (52%) | 2 (50%) | 0 | 0 | 1 (25%) | 2 (18%) | 0 (0%) | 3 (100%) | 2 (100%) | 0 | |
| Gentamicin | 7 (23%) | 0 | 0 | 0 | 1 (14%) | 2 (17%) | 0 (0%) | 3 (100%) | 2 (100%) | 2 (40) | 0 |
| Cotrimoxazole | 15 (48%) | 2 (50%) | 0 (0%) | 0 | 2 (17%) | 0 (0%) | 3 (100%) | 1 (50%) | 0 | ||
| Amoxicillin/Clavulanic acid | 13 (42%) | 0 | 0 | 1 (25%) | 2 (18%) | 1 (50%) | 2 (100%) | 1 (50%) | 0 | 0 | |
| Piperacillin | 15 (54%) | 1 (25%) | 0 | 0 | 1 (25%) | 2 (18%) | 0 (0%) | 3 (100%) | 1 (50%) | 0 | 0 |
| Amikacin | 0 | 0 | 0 | 0 | 1 (25%) | 2 (18%) | 0 (0%) | 1 (50%) | 0 | 0 | 0 |
| Ciprofloxacin | 15 (48%) | 0 | 0 | 0 (0%) | 3 (100%) | 1 (50%) | |||||
| Meropenem | 0 | 0 | 0 | 0 | 1 (25%) | 2 (18%) | 0 (0%) | 3 (100%) | 0 | 0 | |
| Piperacillin-Tazobactam | 1 (3.2%) | 0 | 0 | 0 | 2 (18%) | 0 (0%) | 3 (100%) | 1 (50%) | 0 | 0 | |
| Tobramycin | 7 (25%) | 0 | 0 | 0 | 1 (25%) | 2 (18%) | 0 (0%) | 2 (100%) | 0 | 0 | 0 |
| Vancomycin | 0 | 0 | 0 | 0 | 0 |
| Characteristic | HR | 95% CI | p-Value |
|---|---|---|---|
| SBP | 1.62 | (1.47, 1.78) | <0.001 |
| Sex—Male | 1.20 | (1.11, 1.31) | 0.03 |
| Age | 1.01 | (1.00, 1.01) | <0.001 |
| Ethnicity—Bedouin | 0.67 | (0.57, 0.8) | 0.02 |
| Anemia (Hemoglobin < 12) | 2.71 | (2.44, 3) | <0.001 |
| Platelets | 1.00 | (1, 1) | 0.67 |
| Albumin < 3.5 at diagnosis | 1.73 | (0.57, 0.73) | <0.001 |
| INR > 1 at diagnosis | 1.40 | (1.32, 1.63) | <0.001 |
| Hepatitis B | 0.68 | (0.58, 0.8) | 0.02 |
| Hepatitis C | 0.85 | (0.76, 0.95) | 0.14 |
| Fatty liver | 0.80 | (0.7, 0.91) | 0.09 |
| Alcoholic liver disease | 1.08 | (0.94, 1.23) | 0.59 |
| Esophageal Varices | 0.94 | (0.87, 1.03) | 0.50 |
| HCC | 1.54 | (1.39, 1.72) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu-Freha, N.; Michael, T.; Poupko, L.; Estis-Deaton, A.; Aasla, M.; Abu-Freha, O.; Etzion, O.; Nesher, L. Spontaneous Bacterial Peritonitis among Cirrhotic Patients: Prevalence, Clinical Characteristics, and Outcomes. J. Clin. Med. 2022, 11, 227. https://doi.org/10.3390/jcm11010227
Abu-Freha N, Michael T, Poupko L, Estis-Deaton A, Aasla M, Abu-Freha O, Etzion O, Nesher L. Spontaneous Bacterial Peritonitis among Cirrhotic Patients: Prevalence, Clinical Characteristics, and Outcomes. Journal of Clinical Medicine. 2022; 11(1):227. https://doi.org/10.3390/jcm11010227
Chicago/Turabian StyleAbu-Freha, Naim, Tal Michael, Liat Poupko, Asia Estis-Deaton, Muhammad Aasla, Omar Abu-Freha, Ohad Etzion, and Lior Nesher. 2022. "Spontaneous Bacterial Peritonitis among Cirrhotic Patients: Prevalence, Clinical Characteristics, and Outcomes" Journal of Clinical Medicine 11, no. 1: 227. https://doi.org/10.3390/jcm11010227