
Biological Approach in the Treatment of External Popliteal Sciatic Nerve (Epsn) Neurological Injury: Review

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
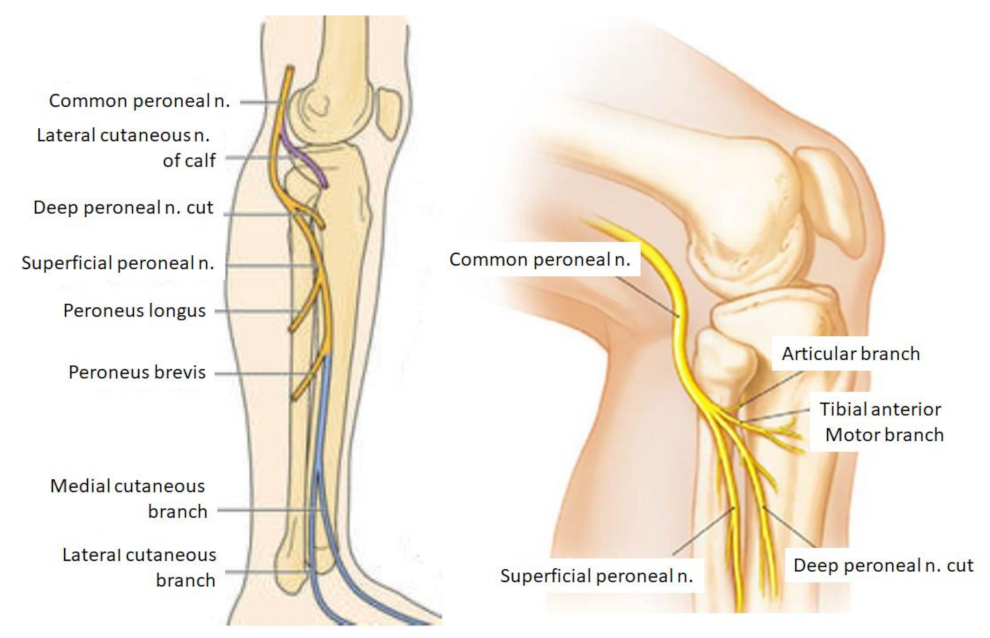
2. Anatomy of the EPSN
3. Compression of the EPSN
4. Clinical
5. Diagnosis
6. Treatment
6.1. Surgical Treatment
6.2. Biological Treatment
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kurze, T. Microtechniques in neurological surgery. Neurosurgery 1964, 11, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Huckhagel, T.; Nüchtern, J.; Regelsberger, J.; Gelderblom, M.; Lefering, R.; TraumaRegister DGU®. Nerve trauma of the lower extremity: Evaluation of 60,422 leg injured patients from the TraumaRegister DGU® between 2002 and 2015. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grinsell, D.; Keating, C.P. Peripheral nerve reconstruction after injury: A review of clinical and experimental therapies. BioMed Res. Int. 2014, 2014, 698256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marciniak, C. Fibular (peroneal) neuropathy: Electrodiagnostic features and clinical correlates. Phys. Med. Rehabil. Clin. N. Am. 2013, 24, 121–137. [Google Scholar] [CrossRef] [PubMed]
- Moatshe, G.; Dornan, G.J.; Løken, S.; Ludvigsen, T.C.; Laprade, R.F.; Engebretsen, L. Demographics and injuries associated with knee dislocation: A prospective review of 303 patients. Orthop. J. Sports Med. 2017, 5, 2325967117706521. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.L.; Rivlin, M.; Graham, J.G.; Beredjiklian, P.K. Peripheral nerve injury, scarring, and recovery. Connect. Tissue Res. 2019, 60, 3–9. [Google Scholar] [CrossRef]
- Mathot, F.; Shin, A.Y.; Van Wijnen, A.J. Targeted stimulation of MSCs in peripheral nerve repair. Gene 2019, 710, 17–23. [Google Scholar] [CrossRef]
- Sumner, A.J. Aberrant reinnervation. Muscle Nerve 1990, 13, 801–803. [Google Scholar] [CrossRef]
- Piton, C.; Fabre, T.; Lasseur, E.; André, D.; Geneste, M.; Durandeau, A. Les lésions du nerf fibulaire commun: Approche étiologique et thérapeutique. A propos de 146 cas traités chirurgicalement [Common fibular nerve lesions. Etiology and treatment. Apropos of 146 cases with surgical treatment]. Rev. Chir. Orthop. Reparatrice Appar. Mot. 1997, 83, 515–521. [Google Scholar]
- Beccari, S.; Turki, M.; Zinelabidine, M.; Ennouri, K.H.; Tarhouni, L.; Bahri, H. Une étiologie rare de paralysie du nerf sciatique poplité externe: L’entorse de la cheville. À propos de 6 cas. J. Traumatol Sport 2000, 17, 208–212. [Google Scholar]
- Sunderland, S. Nerves and Nerves Injuries, 2nd ed.; Churchill Livinstone: Edinburg, UK, 1978. [Google Scholar]
- Menorca, R.M.; Fussell, T.S.; Elfar, J.C. Nerve physiology: Mechanisms of injury and recovery. Hand Clin. 2013, 29, 317–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kendall, J.P.; Stokes, I.A.; O’Hara, J.P.; Dickson, R.A. Tension and creep phenomena in peripheral nerve. Acta Orthop. Scand. 1979, 50, 721–725. [Google Scholar] [CrossRef] [PubMed]
- Pham, K.; Gupta, R. Understanding the mechanisms of entrapment neuropathies. Review article. Neurosurg. Focus 2009, 26, E7. [Google Scholar] [CrossRef] [PubMed]
- Noble, J.; Munro, C.A.; Prasad, V.S.S.V.; Midha, R. Analysis of upper and lower extremity peripheral nerve injuries in a population of patients with multiple injuries. J. Trauma Inj. Infect. Crit. Care 1998, 45, 116–122. [Google Scholar] [CrossRef]
- Atkins, S.; Smith, K.G.; Loescher, A.R.; Boissonade, F.M.; O’Kane, S.; Ferguson, M.W.; Robinson, P.P. Scarring impedes regeneration at sites of peripheral nerve repair. NeuroReport 2006, 17, 1245–1249. [Google Scholar] [CrossRef]
- Piñeiro, L.; Rey, R.R.; Sabina, A.G.; Secades, R.M.; Pais, M.J.G. Paralysis of the external popliteal sciatic nerve associated with daptomycin administration. J. Clin. Pharm. Ther. 2018, 43, 578–580. [Google Scholar] [CrossRef]
- Pérez, L.M.; Vived, Á.M.; Gil, D.R. Manual y Atlas Fotográfico de Anatomía del Aparato Locomotor; Panamericana: Madrid, Spain, 2010. [Google Scholar]
- Sánchez-Martín, M.M. Traumatología y Ortopedia; Universidad de Valladolid: Valladolid, Spain, 2002. [Google Scholar]
- Cortet, B.; Bourgeois, P. Causes et mécanismes des souffrances sciatiques [Causes and mechanisms of sciatic pains]. Rev. Prat. 1992, 42, 539–543. [Google Scholar]
- Poage, C.; Roth, C.; Scott, B. Peroneal Nerve Palsy: Evaluation and Management. J. Am. Acad. Orthop. Surg. 2016, 24, 1–10. [Google Scholar] [CrossRef]
- Chow, A.L.; Levidy, M.F.; Luthringer, M.; Vasoya, D.; Ignatiuk, A. Clinical Outcomes After Neurolysis for the Treatment of Peroneal Nerve Palsy: A Systematic Review and Meta-Analysis. Ann. Plast. Surg. 2021, 87, 316–323. [Google Scholar] [CrossRef]
- Waldman, S.D. Waldman’s Comprehensive Atlas of Diagnostic Ultrasound of Painful Conditions, 1st ed.; Wolters Kluwer: Philadelphia, PA, USA, 2016. [Google Scholar]
- Martyn, C.N.; Hughes, R.A. Epidemiology of peripheral neuropathy. J. Neurol. Neurosurg. Psychiatry 1997, 62, 310–318. [Google Scholar] [CrossRef] [Green Version]
- Kitamura, T.; Kim, K.; Morimoto, D.; Kokubo, R.; Iwamoto, N.; Isu, T.; Morita, A. Dynamic factors involved in common peroneal nerve entrapment neuropathy. Acta Neurochir. 2017, 159, 1777–1781. [Google Scholar] [CrossRef] [PubMed]
- Dahlin, L.B.; Lundborg, G. The neurone and its response to peripheral nerve compression. J. Hand Surg. Br. Eur. Vol. 1990, 15, 5–10. [Google Scholar] [CrossRef]
- Gutiérrez-Mendoza, I. Generalidades y fisiopatología de la compresión nerviosa. Orthotips AMOT 2014, 10, 9–14. [Google Scholar]
- Eversmann, W.W., Jr. Compression and entrapment neuropathies of the upper extremity. J. Hand Surg. Am. 1983, 8 Pt 2, 759–766. [Google Scholar] [CrossRef]
- Rydevik, B.L. The effects of compression on the physiology of nerve roots. J. Manip. Physiol. Ther. 1992, 15, 62–66. [Google Scholar]
- Artico, M.; Pastore, F.S.; Nucci, F.; Giuffre, R. 290 surgical procedures for ulnar nerve entrapment at the elbow: Physiopathology, clinical experience and results. Acta Neurochir. 2000, 142, 303–308. [Google Scholar] [CrossRef] [Green Version]
- Radosevich, J. (Ed.) Apoptosis and Beyond: The Many Ways Cells Die; Wiley Blackwell: Hoboken, NJ, USA, 2018. [Google Scholar]
- Dy, C.J.; Brogan, D.M.; Wagner, E.R. Peripheral Nerve Issues after Orthopedic Surgery: A Multidisciplinary Approach to Prevention, Evaluation and Treatment, 1st ed; Springer: Berlin/Heidelberg, Germany, 2021. [Google Scholar]
- Seddon, H.J. Three Types of Nerve Injury. Brain 1943, 66, 237–288. [Google Scholar] [CrossRef]
- Tubbs, R.S.; Rizk, E.; Shoja, M.M.; Loukas, M.; Barbaro, N.; Spinner, R.J. Nerves and Nerve Injuries; Academic Press (Elsevier): Waltham, MA, USA, 2015. [Google Scholar]
- Distad, B.J.; Weiss, M.D. Clinical and Electrodiagnostic Features of Sciatic Neuropathies. Phys. Med. Rehabil. Clin. N. Am. 2013, 24, 107–120. [Google Scholar] [CrossRef]
- Anderson, J.C. Common Fibular Nerve Compression: Anatomy, Symptoms, Clinical Evaluation, and Surgical Decompression. Clin. Podiatr. Med. Surg. 2016, 33, 283–291. [Google Scholar] [CrossRef]
- Garg, B.; Poage, C. Peroneal Nerve Palsy: Evaluation and Management. J. Am. Acad. Orthop. Surg. 2016, 24, e49. [Google Scholar] [CrossRef]
- Tzika, M.; Paraskevas, G.; Natsis, K. Entrapment of the superficial peroneal nerve: An anatomical insight. J. Am. Podiatr. Med. Assoc. 2015, 105, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Fortier, L.M.; Markel, M.; Thomas, B.G.; Sherman, W.F.; Thomas, B.H.; Kaye, A.D. An Update on Peroneal Nerve Entrapment and Neuropathy. Orthop. Rev. 2021, 13, 24937. [Google Scholar] [CrossRef] [PubMed]
- Riccio, M.; Marchesini, A.; Pugliese, P.; De Francesco, F. Nerve repair and regeneration: Biological tubulization limits and future perspectives. J. Cell. Physiol. 2019, 234, 3362–3375. [Google Scholar] [CrossRef] [PubMed]
- Hobson-Webb, L.D.; Juel, V.C. Common Entrapment Neuropathies. Contin. Lifelong Learn. Neurol. 2017, 23, 487–511. [Google Scholar] [CrossRef]
- Karakis, I.; Khoshnoodi, M.; Liew, W.; Nguyen, E.S.; Jones, H.R.; Darras, B.T.; Kang, P.B. Electrophysiologic features of fibular neuropathy in childhood and adolescence. Muscle Nerve 2017, 55, 693–697. [Google Scholar] [CrossRef]
- Roy, P.C. Electrodiagnostic evaluation of lower extremity neurogenic problems. Foot Ankle Clin. 2011, 16, 225–242. [Google Scholar] [CrossRef]
- Bendszus, M.; Stoll, G. Technology insight: Visualizing peripheral nerve injury using MRI. Nat. Clin. Pract. Neurol. 2005, 1, 45–53. [Google Scholar] [CrossRef]
- Grant, G.A.; Britz, G.W.; Goodkin, R.; Jarvik, J.G.; Maravilla, K.; Kliot, M. The utility of magnetic resonance imaging in evaluating peripheral nerve disorders. Muscle Nerve 2002, 25, 314–331. [Google Scholar] [CrossRef]
- Stoll, G.; Bendszus, M.; Perez, J.; Pham, M. Magnetic resonance imaging of the peripheral nervous system. J. Neurol. 2009, 256, 1043–1051. [Google Scholar] [CrossRef]
- Tsukamoto, H.; Granata, G.; Coraci, D.; Paolasso, I.; Padua, L. Ultrasound and neurophysiological correlation in common fibular nerve conduction block at fibular head. Clin. Neurophysiol. 2014, 125, 1491–1495. [Google Scholar] [CrossRef]
- Pabari, A.; Yang, S.Y.; Seifalian, A.M.; Mosahebi, A. Modern surgical management of peripheral nerve gap. J. Plast. Reconstr. Aesthetic Surg. 2010, 63, 1941–1948. [Google Scholar] [CrossRef] [PubMed]
- Bamba, R.; Loewenstein, S.N.; Adkinson, J.M. Donor site morbidity after sural nerve grafting: A systematic review. J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 3055–3060. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Meng, D.; Yin, G.; Hou, C.; Lin, H. Translocation of the soleus muscular branch of the tibial nerve to repair high common peroneal nerve injury. Acta Neurochir. 2019, 161, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Nath, R.K.; Lyons, A.B.; Paizi, M. Successful management of foot drop by nerve transfers to the deep peroneal nerve. J. Reconstr. Microsurg. 2008, 24, 419–427. [Google Scholar] [CrossRef] [PubMed]
- El-Taher, M.; Sallam, A.; Saleh, M.; Metwally, A. Foot Reanimation Using Double Nerve Transfer to Deep Peroneal Nerve: A Novel Technique for Treatment of Neurologic Foot Drop. Foot Ankle Int. 2021, 42, 1011–1021. [Google Scholar] [CrossRef]
- Siemionow, M.; Brzezicki, G. Chapter 8: Current techniques and concepts in peripheral nerve repair. Int. Rev. Neurobiol. 2009, 87, 141–172. [Google Scholar] [CrossRef]
- Lapuente, J.P.; Dos-Anjos, S.; Blázquez-Martínez, A. Intra-articular infiltration of adipose-derived stromal vascular fraction cells slows the clinical progression of moderate-severe knee osteoarthritis: Hypothesis on the regulatory role of intra-articular adipose tissue. J. Orthop. Surg. Res. 2020, 15, 137. [Google Scholar] [CrossRef] [Green Version]
- Jessen, K.R.; Mirsky, R. The repair Schwann cell and its function in regenerating nerves. J. Physiol. 2016, 594, 3521–3531. [Google Scholar] [CrossRef] [Green Version]
- Mirsky, R.; Jessen, K.R.; Brennan, A.; Parkinson, D.; Dong, Z.; Meier, C.; Parmantier, E.; Lawson, D. Schwann cells as regulators of nerve development. J. Physiol. 2002, 96, 17–24. [Google Scholar] [CrossRef]
- Woodhoo, A.; Alonso, M.B.; Droggiti, A.; Turmaine, M.; D’Antonio, M.; Parkinson, D.B.; Wilton, D.K.; Al-Shawi, R.; Simons, P.; Shen, J.; et al. Notch controls embryonic Schwann cell differentiation, postnatal myelination and adult plasticity. Nat. Neurosci. 2009, 12, 839–847. [Google Scholar] [CrossRef] [Green Version]
- Monk, K.R.; Feltri, M.L.; Taveggia, C. New insights on Schwann cell development. Glia 2015, 63, 1376–1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salzer, J.L. Schwann cell myelination. Cold Spring Harb. Perspect. Biol. 2015, 7, a020529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, M.; Hall, S.; Follows, R.; Rees, L.; Gregson, N.; Sievers, J. Response of axons and glia at the site of anastomosis between the optic nerve and cellular or acellular sciatic nerve grafts. J. Neurocytol. 1988, 17, 727–744. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.; Hu, D.; Chen, J.; Wang, Q.; Zhang, Y.; Qi, C.; Yu, T. Repair of the Injured Spinal Cord by Schwann Cell Transplantation. Front. Neurosci. 2022, 16, 800513. [Google Scholar] [CrossRef]
- Lee, S.K.; Wolfe, S.W. Peripheral nerve injury and repair. J. Am. Acad. Orthop. Surg. 2000, 8, 243–252. [Google Scholar] [CrossRef] [Green Version]
- Noriega, D.C.; Ardura, F.; Hernández-Ramajo, R.; Martín-Ferrero, M.Á.; Sánchez-Lite, I.; Toribio, B.; Alberca, M.; García, V.; Moraleda, J.M.; González-Vallinas, M.; et al. Treatment of Degenerative Disc Disease with Allogeneic Mesenchymal Stem Cells: Long-term Follow-up Results. Transplantation 2021, 105, e25–e27. [Google Scholar] [CrossRef]
- Noriega, D.C.; Ardura, F.; Hernández-Ramajo, R.; Martín-Ferrero, M.Á.; Sánchez-Lite, I.; Toribio, B.; Alberca, M.; García, V.; Moraleda, J.M.; Sánchez, A.; et al. Intervertebral Disc Repair by Allogeneic Mesenchymal Bone Marrow Cells: A Randomized Controlled Trial. Transplantation 2017, 101, 1945–1951. [Google Scholar] [CrossRef]
- Chen, Z.L.; Yu, W.M.; Strickland, S. Peripheral regeneration. Annu. Rev. Neurosci. 2007, 30, 209–233. [Google Scholar] [CrossRef]
- Kitada, M. Mesenchymal cell populations: Development of the induction systems for Schwann cells and neuronal cells and finding the unique stem cell population. Anat. Sci. Int. 2012, 87, 24–44. [Google Scholar] [CrossRef]
- Scuteri, A.; Miloso, M.; Foudah, D.; Orciani, M.; Cavaletti, G.; Tredici, G. Mesenchymal stem cells neuronal differentiation ability: A real perspective for nervous system repair? Curr. Stem Cell Res. Ther. 2011, 6, 82–92. [Google Scholar] [CrossRef]
- Cai, S.; Shea, G.K.; Tsui, A.Y.; Chan, Y.S.; Shum, D.K. Derivation of clinically applicable schwann cells from bone marrow stromal cells for neural repair and regeneration. CNS Neurol. Disord.-Drug Targets 2011, 10, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Wakao, S.; Matsuse, D.; Dezawa, M. Mesenchymal stem cells as a source of Schwann cells: Their anticipated use in peripheral nerve regeneration. Cells Tissues Organs 2014, 200, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Konofaos, P.; Ver Halen, J.P. Nerve repair by means of tubulization: Past, present, future. J. Reconstr. Microsurg. 2013, 29, 149–164. [Google Scholar] [CrossRef] [Green Version]
- Klimaschewski, L.; Claus, P. Fibroblast Growth Factor Signalling in the Diseased Nervous System. Mol. Neurobiol. 2021, 58, 3884–3902. [Google Scholar] [CrossRef] [PubMed]
- Grothe, C.; Nikkhah, G. The role of basic fibroblast growth factor in peripheral nerve regeneration. Anat. Embryol. 2001, 204, 171–177. [Google Scholar] [CrossRef]
- Boyd, J.G.; Gordon, T. Neurotrophic factors and their receptors in axonal regeneration and functional recovery after peripheral nerve injury. Mol. Neurobiol. 2003, 27, 277–324. [Google Scholar] [CrossRef]
- Scheib, J.; Höke, A. Advances in peripheral nerve regeneration. Nat. Rev. Neurol. 2013, 9, 668–676. [Google Scholar] [CrossRef]
- Wood, M.D.; Mackinnon, S.E. Pathways regulating modality-specific axonal regeneration in peripheral nerve. Exp. Neurol. 2015, 265, 171–175. [Google Scholar] [CrossRef] [Green Version]
- Spector, J.G.; Derby, A.; Lee, P.; Roufa, D.G. Comparison of Rabbit Facial Nerve Regeneration in Nerve Growth Factor-Containing Silicone Tubes to that in Autologous Neural Grafts. Ann. Otol. Rhinol. Laryngol. 1995, 104, 875–885. [Google Scholar] [CrossRef]
- De Francesco, F.; Ricci, G.; D’Andrea, F.; Nicoletti, G.F.; Ferraro, G.A. Human Adipose Stem Cells: From Bench to Bedside. Tissue Eng. Part B Rev. 2015, 21, 572–584. [Google Scholar] [CrossRef] [Green Version]
- Nicoletti, G.F.; De Francesco, F.; D’Andrea, F.; Ferraro, G.A. Methods and procedures in adipose stem cells: State of the art and perspective for translation medicine. J. Cell. Physiol. 2015, 230, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Allbright, K.O.; Bliley, J.M.; Havis, E.; Kim, D.Y.; Dibernardo, G.A.; Grybowski, D.; Waldner, M.; James, I.B.; Sivak, N.; Rubin, J.P.; et al. Delivery of adipose-derived stem cells in poloxamer hydrogel improves peripheral nerve regeneration. Muscle Nerve 2018, 58, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, M.; Valente, S.G.; Sabongi, R.G.; Gomes Dos Santos, J.B.G.; Leite, V.M.; Ulrich, H.; Nery, A.A.; da Silva Fernandes, M.J. Bone marrow-derived mesenchymal stem cells versus adipose-derived mesenchymal stem cells for peripheral nerve regeneration. Neural Regen. Res. 2018, 13, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Kingham, P.J.; Kalbermatten, D.F.; Mahay, D.; Armstrong, S.J.; Wiberg, M.; Terenghi, G. Adipose-derived stem cells differentiate into a Schwann cell phenotype and promote neurite outgrowth In Vitro. Exp. Neurol. 2007, 207, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Alsmadi, N.Z.; Bendale, G.S.; Kanneganti, A.; Shihabeddin, T.; Nguyen, A.H.; Hor, E.; Dash, S.; Johnston, B.; Granja-Vazquez, R.; Romero-Ortega, M.I. Glial-derived growth factor and pleiotrophin synergistically promote axonal regeneration in critical nerve injuries. Acta Biomater. 2018, 78, 165–177. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.A.; Ratner, N.; Roberts, T.M.; Stiles, C.D. Schwann cell proliferative responses to cAMP and Nf1 are mediated by cyclin D1. J. Neurosci. 2001, 21, 1110–1116. [Google Scholar] [CrossRef] [Green Version]
- Davis, J.B.; Stroobant, P. Platelet-derived growth factors and fibroblast growth factors are mitogens for rat Schwann cells. J. Cell Biol. 1990, 110, 1353–1360. [Google Scholar] [CrossRef] [Green Version]
- Nave, K.A.; Salzer, J.L. Axonal regulation of myelination by neuregulin 1. Curr. Opin. Neurobiol. 2006, 16, 492–500. [Google Scholar] [CrossRef]
- Garratt, A.N.; Britsch, S.; Birchmeier, C. Neuregulin, a factor with many functions in the life of a schwann cell. BioEssays 2000, 22, 987–996. [Google Scholar] [CrossRef]
- Faroni, A.; Terenghi, G.; Reid, A.J. Adipose-derived stem cells and nerve regeneration: Promises and pitfalls. Int. Rev. Neurobiol. 2013, 108, 121–136. [Google Scholar] [CrossRef]
- Walocko, F.M.; Khouri, R.K., Jr.; Urbanchek, M.G.; Levi, B.; Cederna, P.S. The potential roles for adipose tissue in peripheral nerve regeneration. Microsurgery 2016, 36, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
León-Andrino, A.; Noriega, D.C.; Lapuente, J.P.; Pérez-Valdecantos, D.; Caballero-García, A.; Herrero, A.J.; Córdova, A. Biological Approach in the Treatment of External Popliteal Sciatic Nerve (Epsn) Neurological Injury: Review. J. Clin. Med. 2022, 11, 2804. https://doi.org/10.3390/jcm11102804
León-Andrino A, Noriega DC, Lapuente JP, Pérez-Valdecantos D, Caballero-García A, Herrero AJ, Córdova A. Biological Approach in the Treatment of External Popliteal Sciatic Nerve (Epsn) Neurological Injury: Review. Journal of Clinical Medicine. 2022; 11(10):2804. https://doi.org/10.3390/jcm11102804
Chicago/Turabian StyleLeón-Andrino, Alejandro, David C. Noriega, Juan P. Lapuente, Daniel Pérez-Valdecantos, Alberto Caballero-García, Azael J. Herrero, and Alfredo Córdova. 2022. "Biological Approach in the Treatment of External Popliteal Sciatic Nerve (Epsn) Neurological Injury: Review" Journal of Clinical Medicine 11, no. 10: 2804. https://doi.org/10.3390/jcm11102804