
The Analysis of Facio-Dental Proportions to Determine the Width of Maxillary Anterior Teeth: A Clinical Study

 , , , ,
, , , ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Estimation of Sample Size
2.2. Participant Enrollment and Ethical Consideration
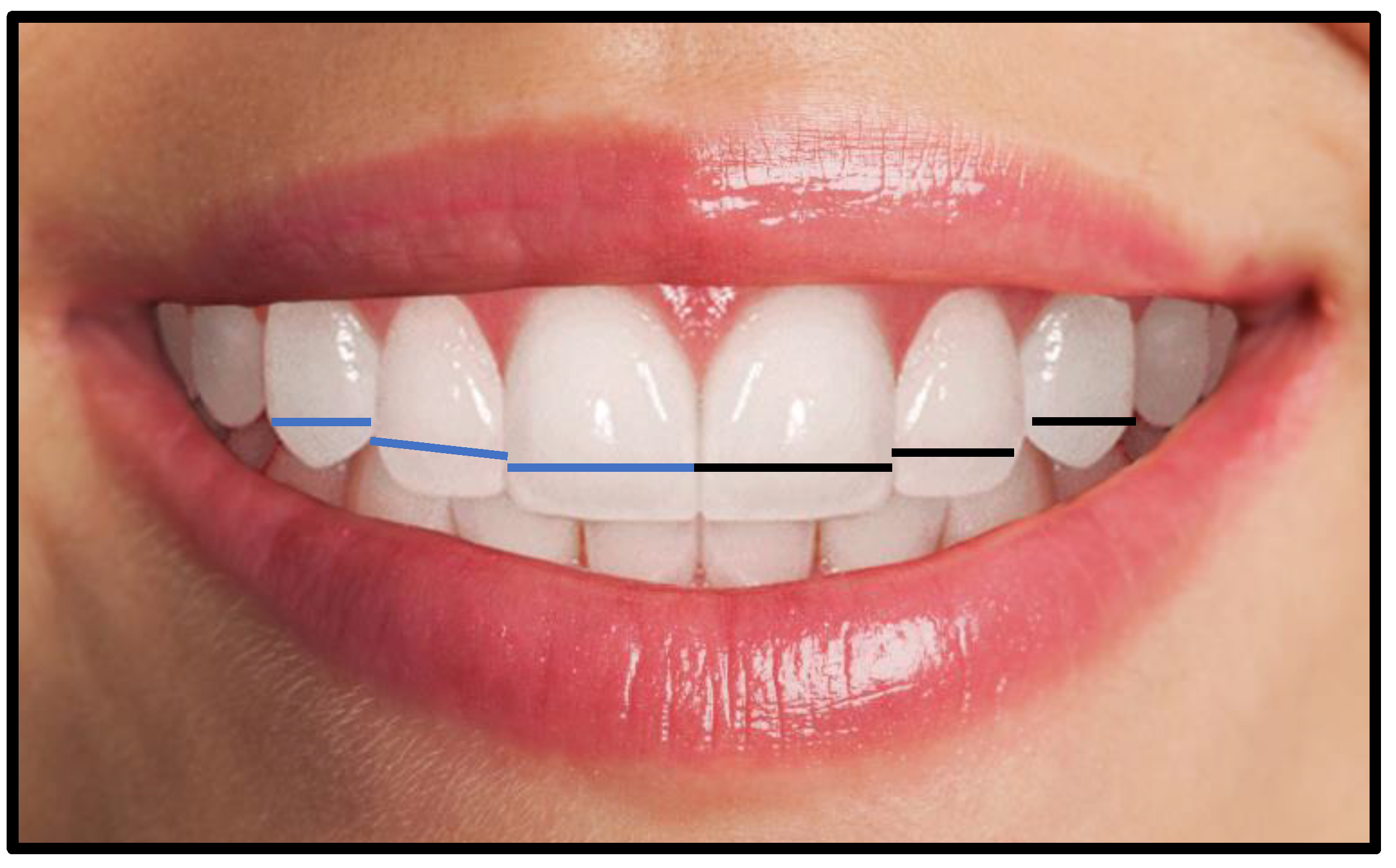
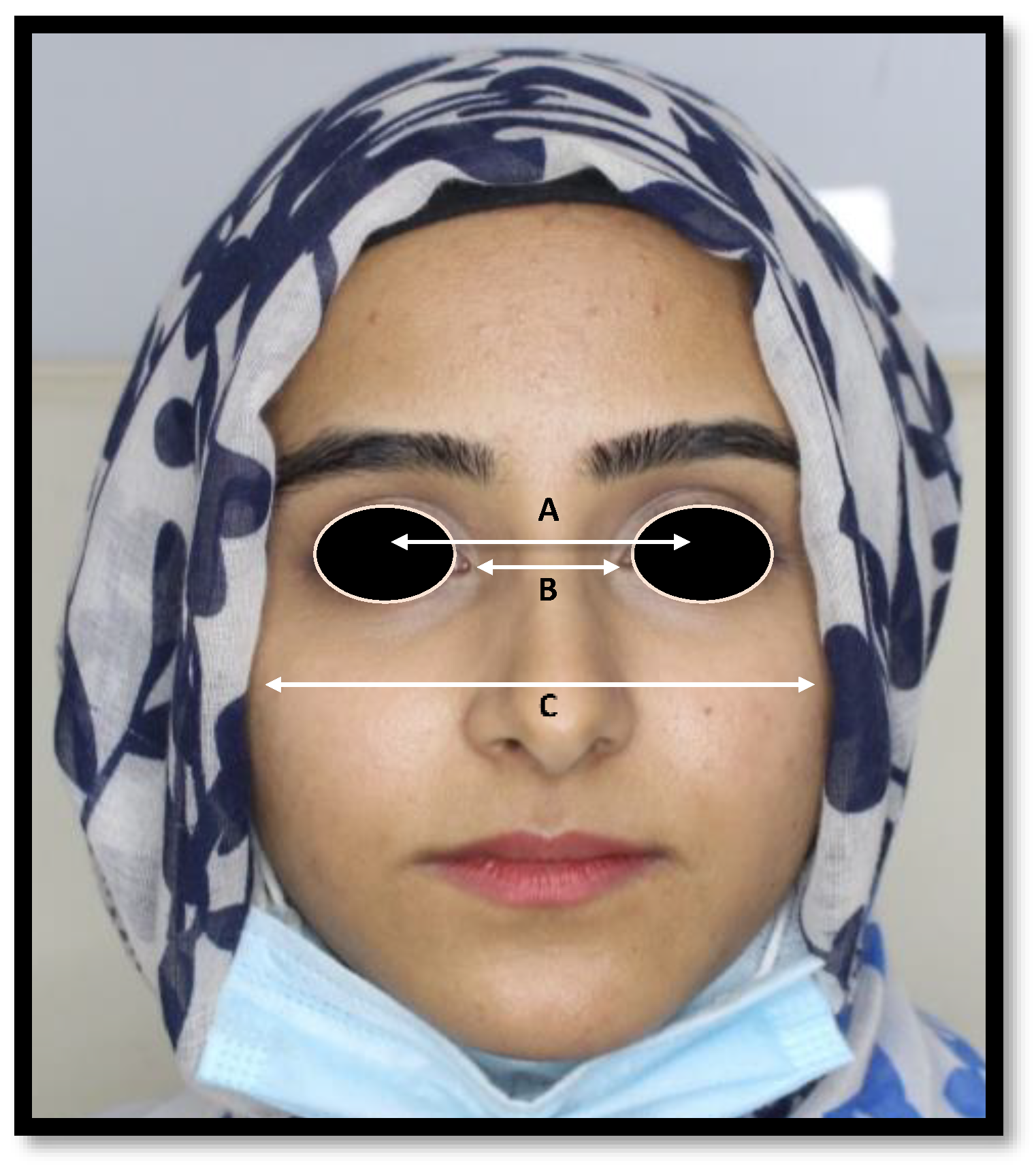
2.3. Capturing Dental and Full Face Frontal Photographs
2.4. Registration of Dental Impression and Fabrication of Dental Stone Cast
2.5. Dental Stone Cast and 3D Model Analysis
2.6. Horizontal Facial Third Proportion Calculation
2.7. Data Validity, Reliability, and Photographic Error Assessment
2.8. Statistical Analysis
2.9. Predicting ITCD and CIW from MHFP Modification by Dental Proportions
3. Results
4. Discussion
5. Conclusions
- The IPD, ICD, and BZD could not directly help in determining the central incisor’s width and intercanine distance.
- The inner-canthal distance modified by the golden percentage can be used to determine CIW.
- The inter-pupillary distance modified by the golden proportion can reliably determine CIW in females.
- The Preston proportion and 70% RED proportion did not serve as reliable predictors of CIW and ITCD.
- A significant difference was found in both sexes when IPD, ICD, and BZD values were modified with GP, PRP, and 70% RED proportion. However, the ICD by golden percentage values were found to be similar in both sexes.
- The IPD was significantly correlated with gender in this study, while the BZD values varied significantly with the weight of participants.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Passia, N.; Blatz, M.; Strub, J.R. Is the smile line a valid parameter for esthetic evaluation? A systematic literature review. Eur. J. Esthet. Dent. 2011, 6, 314–327. [Google Scholar] [PubMed]
- Suhasini, J.; Suresh, V. Comparing the Anthropometric Measurements as a Tool for Anterior Teeth Selection. Indian J. Public Health 2020, 11, 131–135. [Google Scholar]
- Shahid, F.; Alam, M.K.; Khamis, M.F. Maxillary and mandibular anterior crown width/height ratio and its relation to various arch perimeters, arch length, and arch width groups. Eur. J. Dent. 2015, 9, 490–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kern, B.E. Anthropometric parameters of tooth selection. J. Prosthet. Dent. 1967, 17, 431–437. [Google Scholar] [CrossRef]
- Shuchita, S.; Archana, N.; Verma, P. Correlation between facial measurements and the mesiodistal width of the maxillary anterior teeth. Indian J. Dent. Sci. 2012, 4, 20–24. [Google Scholar]
- Ellakwa, A.; McNamara, K.; Sandhu, J.; James, K.; Arora, A.; Klineberg, I.; El-Sheikh, A.; Martin, F.E. Quantifying the selection of maxillary anterior teeth using intraoral and extraoral anatomical landmarks. J. Contemp. Dent. Pract. 2011, 12, 414–421. [Google Scholar] [CrossRef]
- Singh, K.D.; Rao, J.; Kumar, L.; Singh, S. Comparative evaluation of facial landmarks and their correlation in the natural teeth of North Indian and northeast Indian people—A cohort study. J. Oralfacial Health Sci. 2012, 3, 1–11. [Google Scholar]
- Varjao, F.M.; Nogueira, S.S. Nasal width as a guide for the selection of maxillary complete denture anterior teeth in four racial groups. J. Prosthodont. 2006, 15, 353–358. [Google Scholar] [CrossRef]
- Ward, D.H. Proportional smile design using the recurring esthetic dental (RED) proportion. Dent. Clin. N. Am. 2001, 45, 143–154. [Google Scholar] [CrossRef]
- Ward, D.H. Using the RED proportion to engineer the perfect smile. Dent. Today 2008, 27, 112–117. [Google Scholar]
- Levin, E.I. Dental esthetics and the golden proportion. J. Prosthet. Dent. 1978, 40, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Snow, S.R. Esthetic smile analysis of maxillary anterior tooth width: The golden percentage. J. Esthet. Dent. 1999, 11, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Preston, J.D. The golden proportion revisited. J. Esthet. Restor. Dent. 1993, 5, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Liao, P.; Fan, Y.; Nathanson, D. Evaluation of maxillary anterior teeth width: A systematic review. J. Prosthet. Dent. 2019, 122, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Calçada, D.; Correia, A.; Araújo, F. Anthropometric analysis of anterior maxillary teeth with digital photography-a study in a Portuguese sample. Int. J. Esthet. Dent. 2014, 9, 370–380. [Google Scholar] [PubMed]
- Agarwal, B.; Kumar, M.; Alvi, H.A.; Arora, V.; Agarwal, S. Relating central incisor to inner canthal distance-a flexible approach adaptable to different population groups. Int. J. Contemp. Med. 2013, 1, 8–11. [Google Scholar] [CrossRef]
- Ward, D.H. A study of dentists’ preferred maxillary anterior tooth width proportions: Comparing the recurring esthetic dental proportion to other mathematical and naturally occurring proportions. J. Esthet. Restor. Dent. 2007, 19, 324–337. [Google Scholar] [CrossRef]
- Bali, P.; Singh, S.; Singh, A.P.; Goyal, R.R. Biometric relationship between inner canthal distance and geometric progression for the prediction of maxillary central incisor width. Indian. J. Dent. Sci. 2013, 5, 53–56. [Google Scholar]
- Bidra, A.S.; Uribe, F.; Taylor, T.D.; Agar, J.R.; Rungruanganunt, P.; Neace, W.P. The relationship of facial anatomic landmarks with midlines of the face and mouth. J. Esthet. Dent. 2009, 102, 94–103. [Google Scholar] [CrossRef]
- Godinho, J.; Gonçalves, R.P.; Jardim, L. Contribution of facial components to the attractiveness of the smiling face in male and female patients: A cross-sectional correlation study. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 98–104. [Google Scholar] [CrossRef]
- Kolte, R.A.; Kolte, A.P.; Kharkar, V.V.; Bawankar, P. Influence of facial index, facial profile, lip size, and angulations of teeth on gingival characteristics of anterior teeth: A gender-based evaluation. J. Esthet. Restor. Dent. 2020, 32, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Melo, M.; Ata-Ali, J.; Ata-Ali, F.; Bulsei, M.; Grella, P.; Cobo, T.; Martínez-González, J.M. Evaluation of the maxillary midline, curve of the upper lip, smile line and tooth shape: A prospective study of 140 Caucasian patients. BMC Oral Health 2020, 20, 42. [Google Scholar] [CrossRef] [PubMed]
- Ionaş, M. Photographic evaluation of golden proportion, recurring aesthetic dental red proportion and golden percentage. Int. J. Med. Dent. 2020, 24, 243–246. [Google Scholar]
- Ahmed, N.; Abbas, M.; Maqsood, A. Evaluation of recurring esthetic dental proportion in natural smile of Pakistani sample. Pak. Oral Dent. J. 2014, 34, 739–744. [Google Scholar]
- Shah, D.S.; Vaishnav, K.; Duseja, S.; Sheth, R.S. Evaluation of Recurring Esthetic Dental Proportion in Natural Mandibular Anterior Dentition. Adv. Hum. Biol. 2015, 5, 1–4. [Google Scholar]
- Aziz, M.; Hossain, M. Validity of mathematical proportions in maxillary anterior teeth among Bangladeshi population. APOS Trends Orthod. 2017, 7, 41. [Google Scholar] [CrossRef]
- Kalia, R. An analysis of the aesthetic proportions of anterior maxillary teeth in a UK population. Br. Dent. J. 2020, 228, 449–455. [Google Scholar] [CrossRef]
- Al-Marzok, M.I.; Majeed, K.R.; Ibrahim, I.K. Evaluation of maxillary anterior teeth and their relation to the golden proportion in Malaysian population. BMC Oral Health 2013, 13, 9. [Google Scholar] [CrossRef]
- Maharjan, A.; Joshi, S. Clinical evaluation of maxillary anterior teeth in relation to golden proportion, RED proportion and golden percentage. J. Nepal Health Res. Counc. 2018, 16, 11–15. [Google Scholar] [CrossRef] [Green Version]
- Ramirez, L.M.; Ospina, J.D.; Ballesteros, L.E. Proporciones de los Dientes Anteriores en una Población Mestiza. Int. J. Morphol. 2016, 34, 223–231. [Google Scholar] [CrossRef] [Green Version]
- Rita, M.E.; Kinga, J.; Carmen, B.; Diana, C.; Horga, C.; Bögözi, B.; Alina, I. Aesthetic Principles of the Upper Front Teeth: Application of Golden Proportion (Levin) and Golden Percentage (Snow). Acta Med. Marisiensis 2013, 59, 25–27. [Google Scholar]
- Ahmed, N.; Halim, M.S.; Ab Ghani, Z.; Khan, Z.A.; Abbasi, M.S.; Jamayet, N.B.; Alam, M.K. A 2D Photographic and 3D Digital Dental Model Analysis of Golden Percentage in Maxillary Anterior Teeth. BioMed Res. Int. 2021, 2021, 6674400. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-López, S.; Martínez, M.F.; Velasco, J.P.; Junquera, L.; García-Pola, M. Analysis of dental esthetic proportions in a Spanish population sample. J. Oral Sci. 2021, 29, 257–262. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Dental Proportions (DP) | Horizontal Facial Third Proportion Modification Metrics |
|---|---|
| 70% Recurring esthetic dental proportion (RED) | IPD or ICD or BZD × 0.70 |
| Golden proportion (GP) | IPD or ICD or BZD × 0.62 or 1.618 |
| Preston proportion (PRP) | IPD or ICD or BZD × 0.662 (1.32) and 0.842 (1.68). |
| Golden percentage (GM) | IPD or ICD or BZD × 0.5 or 0.3 or 0.2 |
| Maxillary Teeth | 2D Photographic Width | 3D Digital Model Width | Dental Stone Cast Width | |||
|---|---|---|---|---|---|---|
| Mean (mm) | Standard Deviation | Mean (mm) | Standard Deviation | Mean (mm) | Standard Deviation | |
| Right central incisor | 16.114 | 2.366 | 8.397 | 0.540 | 8.627 | 0.453 |
| Right lateral incisor | 13.888 | 5.156 | 7.735 | 0.554 | 7.371 | 0.539 |
| Right Canine | 11.079 | 3.093 | 8.042 | 0.390 | 7.864 | 0.457 |
| Left Central incisor | 16.366 | 5.655 | 8.788 | 0.426 | 8.723 | 0.479 |
| Left lateral incisor | 13.308 | 1.318 | 7.847 | 0.620 | 7.623 | 0.637 |
| Left canine | 10.937 | 0.803 | 8.157 | 0.464 | 7.959 | 0.482 |
| Combine six teeth width (ITCD) | 81.722 | 9.924 | 48.969 | 1.508 | 48.170 | 1.551 |
| Maxillary Anterior Teeth | 2D Photographic Width | Clean Width | p-Value | ||
|---|---|---|---|---|---|
| Mean (mm) | Standard Deviation | Mean (mm) | Standard Deviation | ||
| Right central incisor | 16.114 | 2.366 | 8.130 | 0.717 | 0.001 |
| Right lateral incisor | 13.888 | 5.156 | 6.241 | 0.903 | 0.001 |
| Right Canine | 11.079 | 3.093 | 6.619 | 1.319 | 0.001 |
| Left central incisor | 16.366 | 5.655 | 7.965 | 0.848 | 0.001 |
| Left lateral incisor | 13.308 | 1.318 | 5.983 | 0.937 | 0.014 |
| Left canine | 10.937 | 0.803 | 6.384 | 1.320 | 0.027 |
| Intercanine distance | 81.722 | 9.924 | 40.788 | 4.090 | 0.001 |
| Maxillary Anterior Teeth | Gender | Mean (mm) | St. Deviation | p-Value | t-Value | Mean Difference | Std. Error Difference |
|---|---|---|---|---|---|---|---|
| Right central incisor | Male | 8.342 | 0.616 | 0.138 | −1.490 | −0.105 | 0.071 |
| Female | 8.448 | 0.454 | |||||
| Right lateral Incisor | Male | 7.650 | 0.526 | 0.022 | −2.305 | −0.166 | 0.072 |
| Female | 7.816 | 0.569 | |||||
| Right Canine | Male | 8.060 | 0.408 | 0.502 | 0.672 | 0.034 | 0.051 |
| Female | 8.025 | 0.373 | |||||
| Left central incisor | Male | 8.801 | 0.433 | 0.651 | 0.453 | 0.025 | 0.056 |
| Female | 8.776 | 0.421 | |||||
| Left lateral incisor | Male | 7.863 | 0.554 | 0.700 | 0.386 | 0.031 | 0.081 |
| Female | 7.831 | 0.678 | |||||
| Left canine | Male | 8.186 | 0.477 | 0.361 | 0.915 | 0.056 | 0.061 |
| Female | 8.130 | 0.452 | |||||
| Intercanine distance | Male | 48.905 | 1.511 | 0.531 | −0.627 | −0.125 | 0.199 |
| Female | 49.030 | 1.510 |
| Maxillary Anterior Teeth | Gender | Mean (mm) | St. Deviation | p-Value | t-Value | Mean Difference | Std. Error Difference |
|---|---|---|---|---|---|---|---|
| Right central incisor | Male | 8.075 | 0.743 | 0.261 | −1.125 | −0.106 | 0.094 |
| Female | 8.182 | 0.691 | |||||
| Right lateral Incisor | Male | 6.117 | 0.913 | 0.043 | −2.033 | −0.240 | 0.118 |
| Female | 6.358 | 0.880 | |||||
| Right Canine | Male | 6.367 | 1.404 | 0.004 | −2.872 | −0.492 | 0.171 |
| Female | 6.859 | 1.190 | |||||
| Left central incisor | Male | 7.854 | 0.931 | 0.053 | −1.945 | −0.216 | 0.111 |
| Female | 8.071 | 0.748 | |||||
| Left lateral incisor | Male | 5.885 | 0.960 | 0.124 | −1.545 | −0.190 | 0.123 |
| Female | 6.076 | 0.909 | |||||
| Left canine | Male | 6.072 | 1.337 | 0.001 | −3.582 | −0.608 | 0.169 |
| Female | 6.680 | 1.239 | |||||
| Intercanine distance | Male | 39.912 | 4.057 | 0.001 | −3.228 | −1.706 | 0.528 |
| Female | 41.619 | 3.961 |
| Facial Proportions | Mean (mm) | Standard Deviation |
|---|---|---|
| Interpupillary distance (IPD) | 69.233 | 13.319 |
| Inner intercanthal distance | 33.947 | 4.470 |
| Bi-zygomatic distance | 103.512 | 9.673 |
| Intercanine distance * | 45.976 | 1.784 |
| Central incisor width * | 16.909 | 0.697 |
| Maxillary Anterior Teeth | Gender | Mean | St. Deviation | p-Value | t-Value | Mean Difference | Std. Error Difference |
|---|---|---|---|---|---|---|---|
| Interpupillary distance | Male | 66.615 | 15.532 | 0.003 | −2.953 | −5.102 | 1.728 |
| Female | 71.717 | 10.273 | |||||
| Inner-intercanthal distance | Male | 33.631 | 4.393 | 0.296 | −1.047 | −0.617 | 0.589 |
| Female | 34.248 | 4.540 | |||||
| Bi-zygomatic distance | Male | 103.313 | 11.768 | 0.762 | −0.303 | −0.387 | 1.278 |
| Female | 103.700 | 7.188 |
| Variables | 70% Recurring Aesthetic Dental Proportion | Golden Proportion | Preston Proportion | Golden Percentage | ||
|---|---|---|---|---|---|---|
| Modified Values | ||||||
| Mean and SD | Mean and SD | Mean and SD | Mean and SD | |||
| CIW | ITCD | CIW | ITCD | |||
| Interpupillary distance | 48.463 ± 9.323 | 42.924 ± 8.257 | 45.693 ± 8.790 | 74.771 ± 4.384 | 34.616 ± 6.659 | 60.001 ± 11.543 |
| Inner-intercanthal distance | 23.763 ± 3.129 | 21.047 ± 2.771 | 22.405 ± 2.950 | 36.663 ±4.828 | 16.973 ± 2.235 a | 29.421 ± 3.874 |
| Bi-zygomatic distance | 72.458 ± 6.771 | 64.177 ± 5.997 | 68.317 ± 6.384 | 111.793 ± 10.447 | 51.756 ± 4.836 | 89.710 ± 8.383 |
| Measured Values | ||||||
| Central incisor width | 16.909 ± 0.697 a | |||||
| Intercanine distance | 45.976 ± 1.784 | |||||
| Variables | 70% Recurring Aesthetic Dental Proportion | Golden Proportion | Preston Proportion | Golden Percentage | ||
|---|---|---|---|---|---|---|
| Modified Values | ||||||
| Mean (mm) and SD | Mean (mm) and SD | Mean (mm) and SD | Mean (mm) and SD | |||
| CIW | ITCD | CIW | ITCD | |||
| Interpupillary distance | 46.630 ± 10.872 | 41.301 ± 9.630 | 43.966 ± 10.251 | 71.94 ± 16.775 | 33.307 ± 7.766 | 57.733 ± 13.461 |
| Inner-intercanthal distance | 23.541 ± 3.075 | 20.851 ± 2.723 | 22.196 ± 2.899 | 36.321 ± 4.744 | 16.815 ± 2.196 f | 29.147 ± 3.807 |
| Bi-zygomatic distance | 72.319 ± 8.237 | 64.054 ± 7.296 | 68.186 ± 7.767 | 111.578 ± 12.710 | 51.656 ± 5.884 | 89.538 ± 10.199 |
| Measured Values | ||||||
| Central incisors width | 16.909 ± 0.697 f | |||||
| Intercanine distance | 45.976 ± 1.784 | |||||
| Mid Horizontal Facial Proportion | 70% Recurring Aesthetic Dental Proportion | Golden Proportion | Preston Proportion | Golden Percentage | ||
|---|---|---|---|---|---|---|
| Modified Values | ||||||
| Mean (mm) and SD | Mean (mm) and SD | Mean (mm) and SD | Mean (mm) and SD | |||
| CIW | ITCD | CIW | ITCD | |||
| Interpupillary distance | 50.20 ± 7.191 | 45.465 ± 6.369 β | 47.333 ± 6.780 | 77.455 ± 11.095 | 35.858 ± 5.136 | 62.155 ± 8.903 |
| Inner intercanthal distance | 23.97 ± 3.178 | 21.233 ± 2.815 | 22.603 ± 2.996 | 36.988 ± 4.903 | 16.124 ± 2.270 b | 29.681 ± 3.935 |
| Bi-zygomatic distance | 72.59 ± 5.031 | 64.294 ± 4.456 | 68.442 ± 4.744 | 111.996 ± 7.763 | 51.850 ± 3.594 | 89.874 ± 6.229 |
| Measured Values | ||||||
| Combined central incisor width | 16.909 ± 0.697 b | |||||
| Intercanine distance | 45.976 ± 1.784 β | |||||
| Dependent Variables | Independent Variables | Unstandardized Coefficients | Standardized Coefficients Beta (B) | t | p-Value | 95% Confidence Interval for B | Collinearity | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Bo | Std. Error | Lower Bound | Upper Bound | Tolerance | VIF | |||||
| IPD | Age | −0.022 | 0.246 | −0.006 | −0.090 | 0.928 | −0.508 | 0.463 | 0.993 | 1.007 |
| Gender | 4.834 | 1.943 | 0.182 | 2.487 | 0.014 * | 1.004 | 8.663 | 0.798 | 1.253 | |
| Height | 0.045 | 0.060 | 0.050 | 0.749 | 0.454 | −0.073 | 0.162 | 0.963 | 1.038 | |
| Weight | −0.045 | 0.074 | −0.044 | −0.609 | 0.543 | −0.190 | 0.100 | 0.821 | 1.218 | |
| ICD | Age | −0.025 | 0.084 | −0.020 | −0.296 | 0.767 | −0.190 | 0.140 | 0.993 | 1.007 |
| Gender | 0.410 | 0.661 | 0.046 | 0.619 | 0.536 | −0.894 | 1.713 | 0.798 | 1.253 | |
| Height | −0.027 | 0.020 | −0.090 | −1.340 | 0.182 | −0.067 | 0.013 | 0.963 | 1.038 | |
| Weight | −0.006 | 0.025 | −0.017 | −0.239 | 0.811 | −0.055 | 0.043 | 0.821 | 1.218 | |
| BZD | Age | 0.141 | 0.181 | 0.051 | 0.778 | 0.437 | −0.215 | 0.496 | 0.993 | 1.007 |
| Gender | −0.973 | 1.424 | −0.050 | −0.683 | 0.495 | −3.780 | 1.834 | 0.798 | 1.253 | |
| Height | −0.025 | 0.044 | −0.038 | −0.564 | 0.573 | −0.111 | 0.062 | 0.963 | 1.038 | |
| Weight | −0.114 | 0.054 | −0.154 | −2.119 | 0.035 * | −0.220 | −0.008 | 0.821 | 1.218 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, N.; Halim, M.S.; Ab-Ghani, Z.; Abbasi, M.S.; Aslam, A.; Safdar, J.; Das, G.; Ahmed, A.R.; Jamayet, N.B. The Analysis of Facio-Dental Proportions to Determine the Width of Maxillary Anterior Teeth: A Clinical Study. J. Clin. Med. 2022, 11, 7340. https://doi.org/10.3390/jcm11247340
Ahmed N, Halim MS, Ab-Ghani Z, Abbasi MS, Aslam A, Safdar J, Das G, Ahmed AR, Jamayet NB. The Analysis of Facio-Dental Proportions to Determine the Width of Maxillary Anterior Teeth: A Clinical Study. Journal of Clinical Medicine. 2022; 11(24):7340. https://doi.org/10.3390/jcm11247340
Chicago/Turabian StyleAhmed, Naseer, Mohamad Syahrizal Halim, Zuryati Ab-Ghani, Maria Shakoor Abbasi, Ayesha Aslam, Jawad Safdar, Gotam Das, Abdul Razzaq Ahmed, and Nafij Bin Jamayet. 2022. "The Analysis of Facio-Dental Proportions to Determine the Width of Maxillary Anterior Teeth: A Clinical Study" Journal of Clinical Medicine 11, no. 24: 7340. https://doi.org/10.3390/jcm11247340