
Not Just a One-Way: Mahaim Accessory Pathway Concomitantly Supporting Orthodromic Atrioventricular Re-Entrant Tachycardia

1
Faculty of Medicine, Carol Davila University of Medicine and Pharmacy, 050474 Bucharest, Romania
2
Cardiology Department, Clinical Emergency Hospital, 014461 Bucharest, Romania
3
Department of Medical Electronics and Informatics, Polytechnic University of Bucharest, 060042 Bucharest, Romania
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2023, 12(1), 159; https://doi.org/10.3390/jcm12010159
Submission received: 28 November 2022
/
Revised: 18 December 2022
/
Accepted: 23 December 2022
/
Published: 25 December 2022
(This article belongs to the Special Issue Catheter Ablation of Cardiac Arrhythmias: Current Updates and Perspectives)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Introduction: We report the case of a 41-year-old female with documented narrow QRS tachycardia. During electrophysiological study, both orthodromic and antidromic atrioventricular reentry tachycardia (AVRT) were demonstrated as well as short episodes of pre-excited atrial fibrillation. Programmed atrial stimulation resulted in decremental anterograde conduction on the AP, thus confirming an unexpected Mahaim accessory pathway (AP) diagnosis. Discussion: Limited 3D activation maps of the right atrium during orthoAVRT, respectively, and the right ventricle (RV) during antiAVRT were constructed and helped accurately describe the atrial and ventricular insertion points, which were superposed on the tricuspid ring, confirming the existence of a single short atrio-ventricular right free wall AP. Short atrioventricular APs with anterograde Mahaim-type conduction concomitantly sustaining orthodromic AVRT are extremely rare. Conclusions: Electroanatomical 3D mapping may help both to clarify the diagnosis and increase the success rate by accurately describing the insertion points of complex accessory pathways.
1. Introduction
Mahaim and Winston first described in 1941 the histology of anomalous connections that arise from the atrioventricular (AV) node and insert into the right ventricle (RV) [1]. Later, it was demonstrated that decrementally conducting connections can be between the right atrium (RA) or the AV node and the RV in or close to the right bundle branch (RBB) [2,3]. Although Mahaim accessory pathways (APs) are anatomically distinct from the nodoventricular pathway, they present similar electrocardiographic and electrophysiological characteristics [4], because of the slow rate of recovery of excitability, and they are adenosine-sensitive [5]. Typically, Mahaim APs sustain antidromic atrioventricular re-entrant tachycardia (AVRT) with a left bundle branch (LBBB) morphology [4]. We will discuss the rare case of a short atrio-ventricular AP with anterograde Mahaim-type conduction which is concomitantly sustaining orthodromic AVRT.
2. Case Presentation
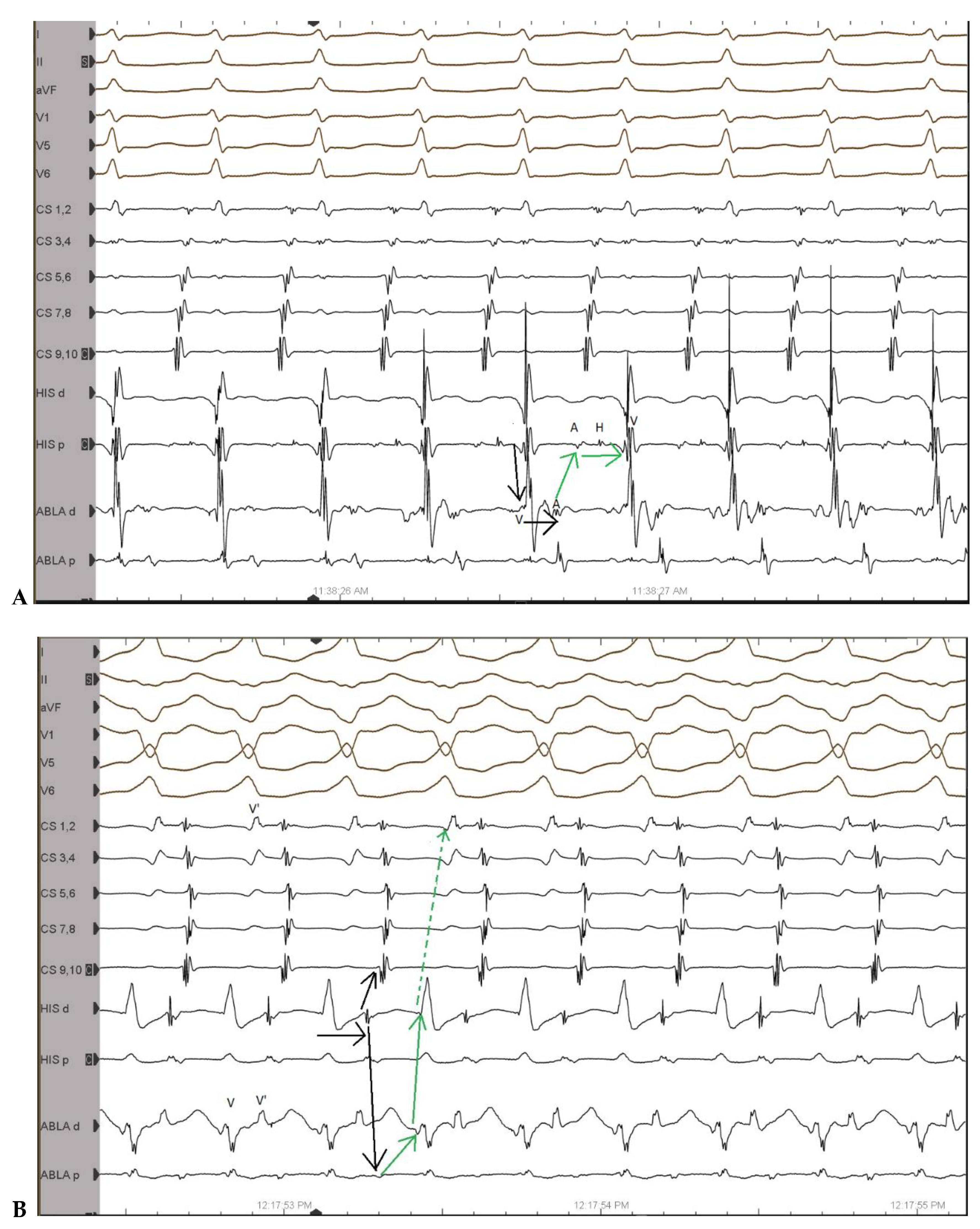
A 41-year-old female with documented narrow QRS tachycardia which was termed orthodromic AVRT presented for ablation of the AP. During electrophysiological (EP) study, both orthodromic as well as antidromic AVRT were demonstrated (Figure 1A,B).
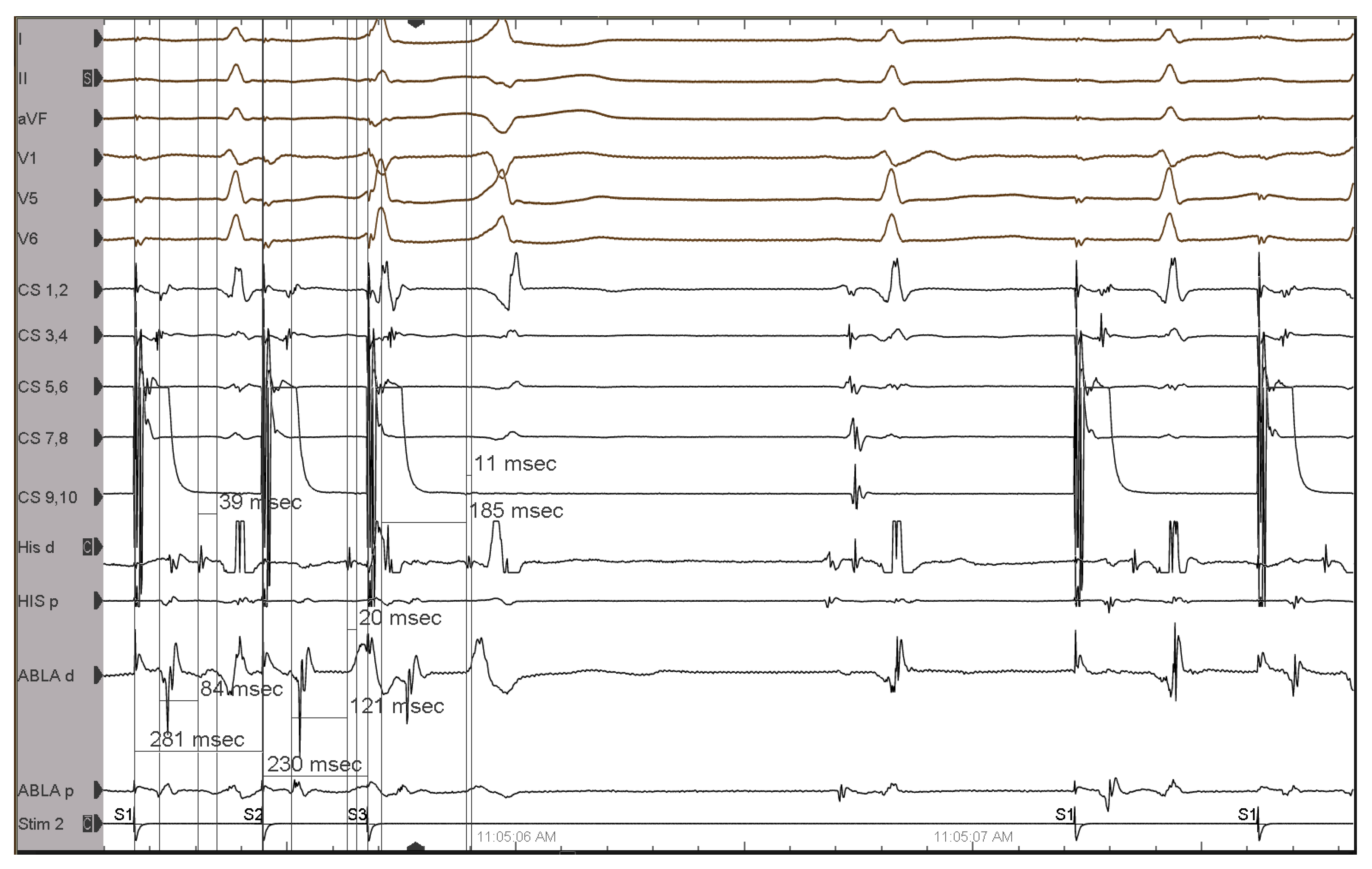
Programmed atrial stimulation resulted in decremental conduction over the AP. During the programmed atrial stimulation with two premature stimuli, the HV interval shortened while the AH interval increased (Figure 2), thus confirming the Mahaim AP diagnosis.
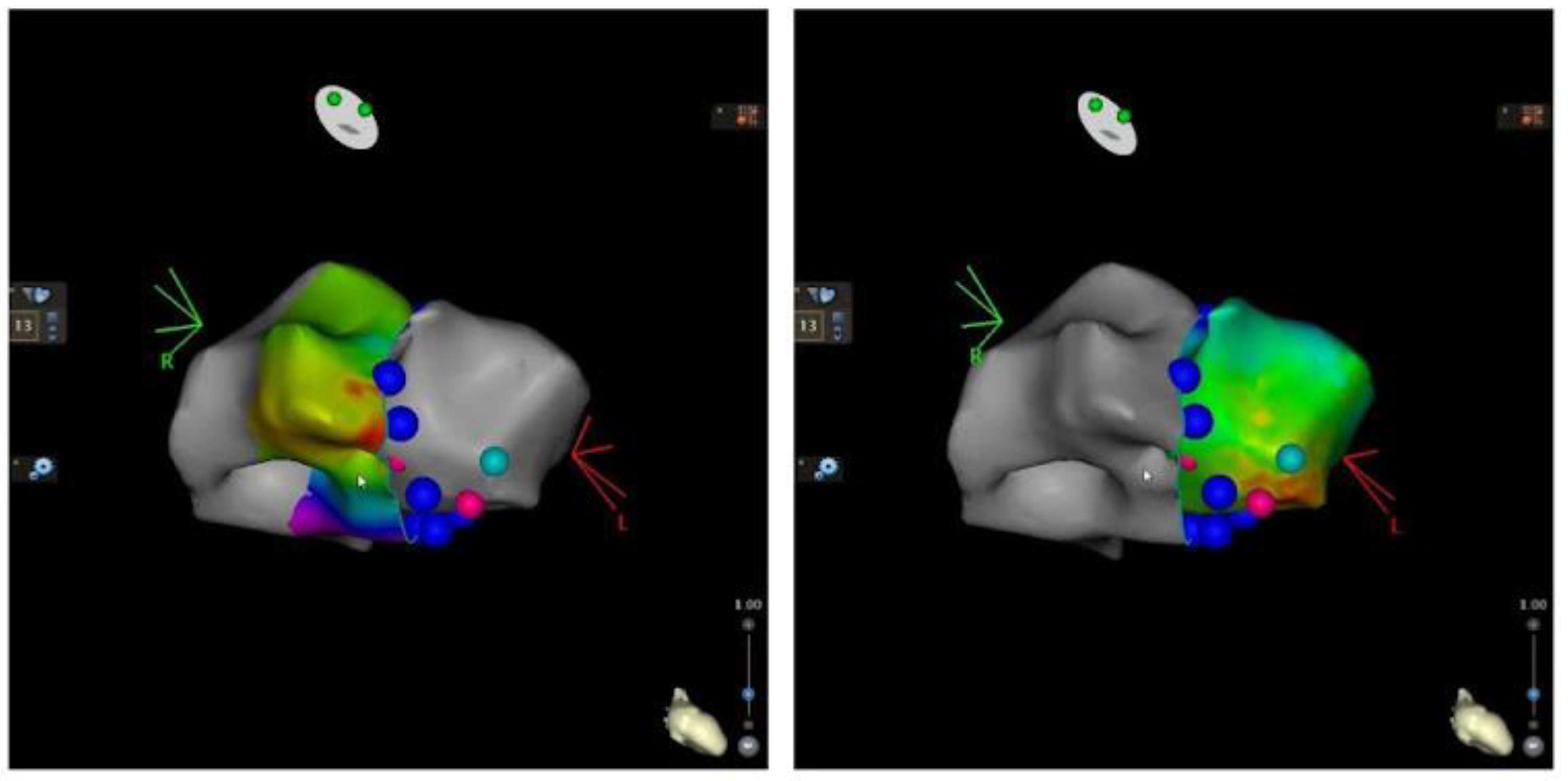
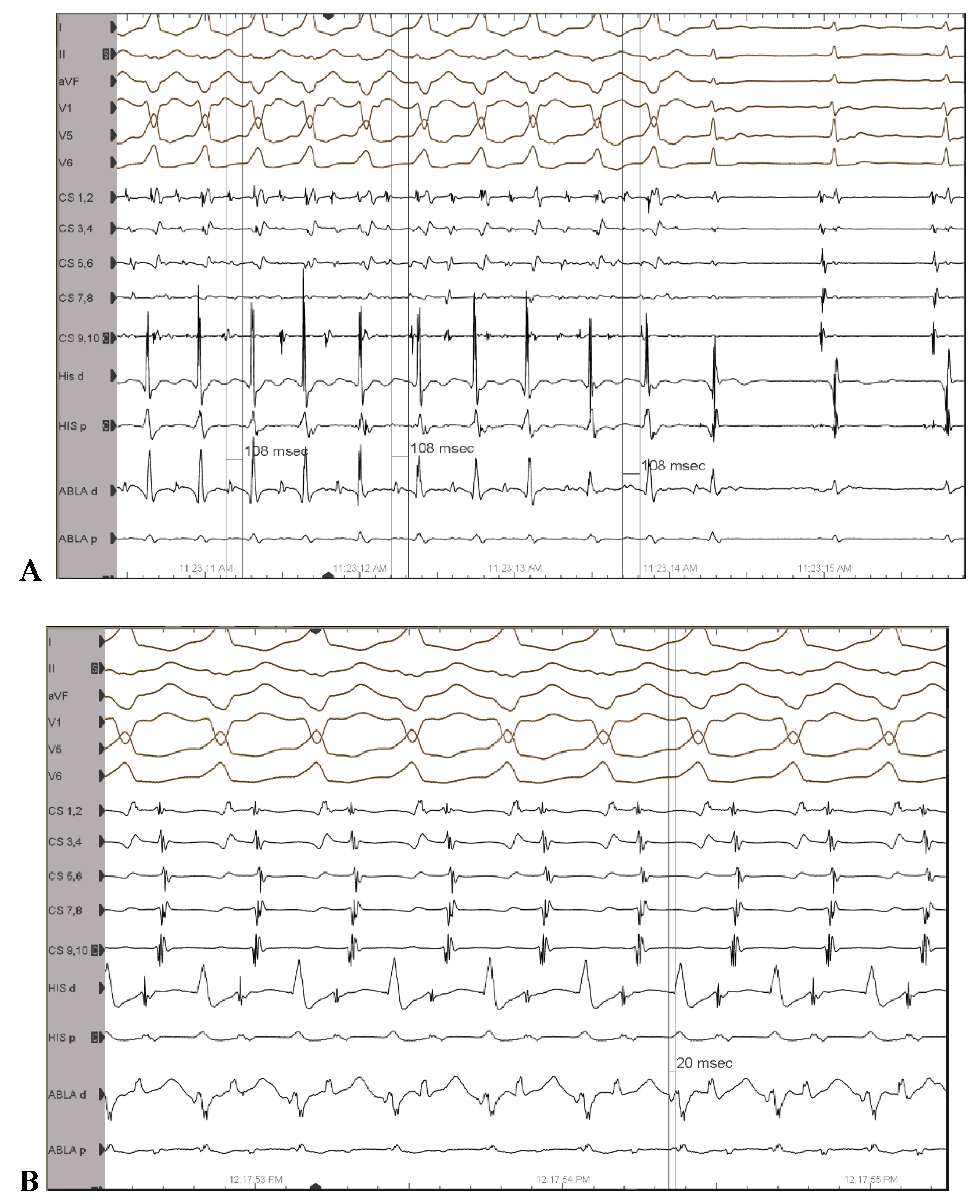
3D activation maps were constructed as follows: an atrial activation map during or-thodromic AVRT and a ventricular activation map during antidromic AVRT in order to accurately describe the insertion points of the Mahaim AP (Figure 3). This resulted in an unusual anatomy of the AP, as it proved to be a short AP, situated at 7 o’clock in LAO projection and close to the tricuspid annulus. AP potentials were also recorded on the ventricular side of the tricuspid ring (Figure 4).
Consequently, efficient ablation of the AP was facilitated by a Agilis NxT steerable introducer (St. Jude Medical, St. Paul, MN, USA) and performed successfully by targeting the distal ventricular insertion (Figure 5). An automatic rhythm with similar morphology to that of the clinical tachycardia occurred during radiofrequency delivery at the point of successful ablation. The tachycardia was rendered non-inducible, and there was no evidence of the persistence of the AP.
3. Discussion
Mahaim APs represent an atypical form of APs that are rare in clinical practice. The term Mahaim APs is commonly used to report decrementally conducting connections between the right atrium or the atrioventricular (AV) node and the right ventricle in or close to the right bundle branch [4], or its distal Purkinje network [5]. Consequently, pathways with Mahaim characteristics can be atriofascicular, atrioventricular, nodofascicular, or nodoventricular, depending on their variable proximal and distal insertions, and the term Mahaim is widely used as an umbrella term for pathways with characteristic electrophysiological properties, long conduction times, and rate-dependent conduction. During ventricular activation through the Mahaim AP, it results in antidromic re-entrant tachycardia, with a left bundle branch block morphology [5]. The baseline ECG of patients with Mahaim APs generally shows minimal or no pre-excitation (as in our patient) because of conduction through the atrioventricular node, due to the long conduction time over the AP [5].
Mahaim APs are typically decremental and conduct only anterogradely [4]. Rarely, retrogradely conducting nodoventricular pathways has been described [6,7]. Whether such pathways are classified as ‘true’ Mahaims is a matter of terminology rather than essence [4]. Moreover, patients with Mahaim APs often have accompanying APs or dual-node physiology with AV nodal re-entrant tachycardia [8]. In one large study, 9 patients out of 55 patients with Mahaim AP were found to have other types of supraventricular tachyarrhythmias in addition to MAP during the electrophysiological study: 6 patients with AV re-entrant tachycardia, 2 with AV nodal re-entrant tachycardia, and 1 with atrial tachycardia [9]. Additionally, this study found that 43 out of 55 cases were ablated at the free wall tricuspid anulus. In our case, an associated concealed AV pathway which would explain the orthodromic AVRT was excluded by electroanatomical 3D mapping. The mapping of atrial insertion of the AP during orthodromic AVRT and the mapping of the ventricular insertion of the AP during programmed atrial stimulation with pre-excitation were performed and the two insertions correspond over the tricuspid valve ring. To the best of our knowledge, this is the first report in which 3D electroanatomical atrial and ventricular mapping confirmed that a single short right free wall atrioventricular AP with anterograde Mahaim properties can sustain both antidromic as well as orthodromic AVRT. In a complex AP, 3D electroanatomical mapping helps to identify the insertion points of the AP, reduce the fluoroscopy times, and accurately perform ablation at the insertion sites. Additionally, 3D-guided ablation allows the operator to return to the target zone and apply consolidating radiofrequency lesions in cases with catheter instability even after temporary loss of accessory pathway conduction.
In Mahaim APs, catheter ablation is performed by identifying the proximal and distal insertions [4]. Furthermore, recording of a proximal pathway potential at the tricuspid annulus or a distal one on the right ventricular free wall would be ideal [4]. Atrial pacing may facilitate pathway potential recording [4]. In 80% of cases, successful ablation is from the atrial side, while in the remaining cases. Ablation needs to be performed at the ventricular insertion [10]. In our case, we decided to perform ablation at the ventricular insertion since the accessory pathway potential was recorded at this site. Ablation at the ventricular insertion site should be carried out proximal to the pathway’s first connection with the ventricle or right bundle to avoid prolonging the VA conduction time and escalating episodes of AVRT [11].
4. Conclusions
In rare cases of complex and/or atypical accessory pathways, electroanatomical 3D mapping should be used both to clarify the diagnosis and increase the success rate by accurately describing the insertion points of the pathway.
Author Contributions
Conceptualization, A.D. and R.V.; methodology, R.V.; software, A.D.; validation, A.D. and R.V.; resources, V.G.; writing—original draft preparation, A.D.; writing—review and editing, A.D and R.V..; visualization, A.D. supervision, R.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data available on request due to restrictions eg privacy or ethical The data presented in this study are available on request from the corresponding author. The data are not publicly available due to General Data Protection Regulation.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mahaim, I.; Winston, M.R. Recherches d’Anatomie Comparée et de Pathologie Expérimentale Sur Les Connexions Hautes Du Faisceau de His-Tawara. Cardiology 1941, 5, 189–260. [Google Scholar] [CrossRef]
- Haïssaguerre, M.; Cauchemez, B.; Marcus, F.; Le Métayer, P.; Lauribe, P.; Poquet, F.; Gencel, L.; Clémenty, J. Characteristics of the Ventricular Insertion Sites of Accessory Pathways With Anterograde Decremental Conduction Properties. Circulation 1995, 91, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- Gandhavadi, M.; Sternick, E.B.; Jackman, W.M.; Wellens, H.J.J.; Josephson, M.E. Characterization of the Distal Insertion of Atriofascicular Accessory Pathways and Mechanisms of QRS Patterns in Atriofascicular Antidromic Tachycardia. Heart Rhythm 2013, 10, 1385–1392. [Google Scholar] [CrossRef] [PubMed]
- Katritsis, D.G.; Wellens, H.J.; Josephson, M.E. Mahaim Accessory Pathways. Arrhythmia Electrophysiol. Rev. 2017, 6, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Arias, M.A.; Pachón, M.; Martín-Sierra, C. Spontaneous Wide QRS Complex Rhythm in a Patient With Wide QRS Complex Tachycardia. Circulation 2020, 141, 1498–1503. [Google Scholar] [CrossRef] [PubMed]
- Hluchy, J.; Schlegelmilch, P.; Schickel, S.; Jörger, U.; Jurkovicova, O.; Sabin, G.V. Radiofrequency Ablation of a Concealed Nodoventricular Mahaim Fiber Guided by a Discrete Potential. J. Cardiovasc. Electrophysiol. 1999, 10, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Josephson, M.E. Electrophysiology at a Crossroads. Heart Rhythm 2007, 4, 658–661. [Google Scholar] [CrossRef] [PubMed]
- Sternick, E.B. Mahaim Fibre Tachycardia: Recognition and Management. Indian Pacing Electrophysiol. J. 2003, 3, 47–59. [Google Scholar] [PubMed]
- Gormel, S.; Yasar, S.; Yildirim, E.; Asil, S.; Baris, V.O.; Gokoglan, Y.; Celik, M.; Yuksel, U.C.; Vurgun, V.K.; Kabul, H.K.; et al. Comprehensive Assessment of Mahaim Accessory Pathways’ Anatomic Distribution. J. Int. Med. Res. 2022, 50, 03000605211069751. [Google Scholar] [CrossRef] [PubMed]
- Vali, Z.; Ng, G.A.; Aboulmaaty, M.; Ibrahim, M. Mahaim-Mediated Tachycardia Using at Times the Atrioventricular Node and Other Times a Left Lateral Accessory Pathway. Heart. Case Rep. 2021, 7, 641–649. [Google Scholar] [CrossRef] [PubMed]
- McClelland, J.H.; Wang, X.; Beckman, K.J.; Hazlitt, H.A.; Prior, M.I.; Nakagawa, H.; Lazzara, R.; Jackman, W.M. Radiofrequency Catheter Ablation of Right Atriofascicular (Mahaim) Accessory Pathways Guided by Accessory Pathway Activation Potentials. Circulation 1994, 89, 2655–2666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
(A): Orthodromic AVRT—Shortest VA interval on the ablation catheter without VA fusion; (B): antidromic AVRT; ECG leads from the top: DI, DII, aVF, V1, V5, V6. His d and His p indicate distal and proximal His bundle electrogram; CS 1-10, coronary sinus distal to proximal; Abla d and p, ablation catheter distal and proximal, respectively, placed in the RV; A = atrium, H = His, V = ventricle, V’ = far-field ventricle; black and green arrows indicate the sequence of activation.
Figure 1.
(A): Orthodromic AVRT—Shortest VA interval on the ablation catheter without VA fusion; (B): antidromic AVRT; ECG leads from the top: DI, DII, aVF, V1, V5, V6. His d and His p indicate distal and proximal His bundle electrogram; CS 1-10, coronary sinus distal to proximal; Abla d and p, ablation catheter distal and proximal, respectively, placed in the RV; A = atrium, H = His, V = ventricle, V’ = far-field ventricle; black and green arrows indicate the sequence of activation.

Figure 2.
Programmed atrial stimulation with two premature stimuli: An extrastimulus is introduced from the coronary sinus at 340 ms after the last pacing drive stimulus (cycle length of 600 ms). This results in minimal pre-excitation: wider QRS, with a delta wave better visible in DI predominately negative in aVF and V1 (positive during the pacing drive and sinus rhythm); a second extrastimulus is delivered 10 ms earlier than the first (330 ms) and results in an atrial-His bundle (A-H) interval of 125 ms, longer than the A-H interval during the pacing drive (84 ms), and a His-ventricular (H-V) interval of 11 ms, shorter than that observed during the pacing drive (39 ms) de-fining an even greater degree of pre-excitation, with a clearly wider QRS. That electrophysiological behavior is the so-called Mahaim physiology of the accessory pathway. ECG leads from the top: DI, DII, aVF, V1, V5, V6. His d and His p indicate distal and proximal His bundle electrogram; CS 1-10, coronary sinus distal to proximal; Abla d and p, ablation catheter distal and proximal, respectively, placed in the RV.
Figure 2.
Programmed atrial stimulation with two premature stimuli: An extrastimulus is introduced from the coronary sinus at 340 ms after the last pacing drive stimulus (cycle length of 600 ms). This results in minimal pre-excitation: wider QRS, with a delta wave better visible in DI predominately negative in aVF and V1 (positive during the pacing drive and sinus rhythm); a second extrastimulus is delivered 10 ms earlier than the first (330 ms) and results in an atrial-His bundle (A-H) interval of 125 ms, longer than the A-H interval during the pacing drive (84 ms), and a His-ventricular (H-V) interval of 11 ms, shorter than that observed during the pacing drive (39 ms) de-fining an even greater degree of pre-excitation, with a clearly wider QRS. That electrophysiological behavior is the so-called Mahaim physiology of the accessory pathway. ECG leads from the top: DI, DII, aVF, V1, V5, V6. His d and His p indicate distal and proximal His bundle electrogram; CS 1-10, coronary sinus distal to proximal; Abla d and p, ablation catheter distal and proximal, respectively, placed in the RV.

Figure 3.
Limited 3D atrial mapping during orthodromic AVRT (left) and limited 3D ventricular activation mapping during antidromic AVRT (right); pink dots: earliest atrial and ventricular signals, respectively; dark-blue dots: tricuspid annulus; light blue dots: mark the limit from which ventricular electrograms no longer precede the surface QRS.
Figure 3.
Limited 3D atrial mapping during orthodromic AVRT (left) and limited 3D ventricular activation mapping during antidromic AVRT (right); pink dots: earliest atrial and ventricular signals, respectively; dark-blue dots: tricuspid annulus; light blue dots: mark the limit from which ventricular electrograms no longer precede the surface QRS.

Figure 4.
(A): Accessory pathway potential recorded on the AV ring during pre-excited atrial fibrillation. (B): Accessory pathway potential during antidromic AVRT; ECG leads from the top: DI, DII, aVF, V1, V5, V6. His d and His p indicate distal and proximal His bundle electrogram; CS 1-10, coronary sinus distal to proximal; Abla d and p, ablation catheter distal and proximal, respectively, placed in the RV.
Figure 4.
(A): Accessory pathway potential recorded on the AV ring during pre-excited atrial fibrillation. (B): Accessory pathway potential during antidromic AVRT; ECG leads from the top: DI, DII, aVF, V1, V5, V6. His d and His p indicate distal and proximal His bundle electrogram; CS 1-10, coronary sinus distal to proximal; Abla d and p, ablation catheter distal and proximal, respectively, placed in the RV.

Figure 5.
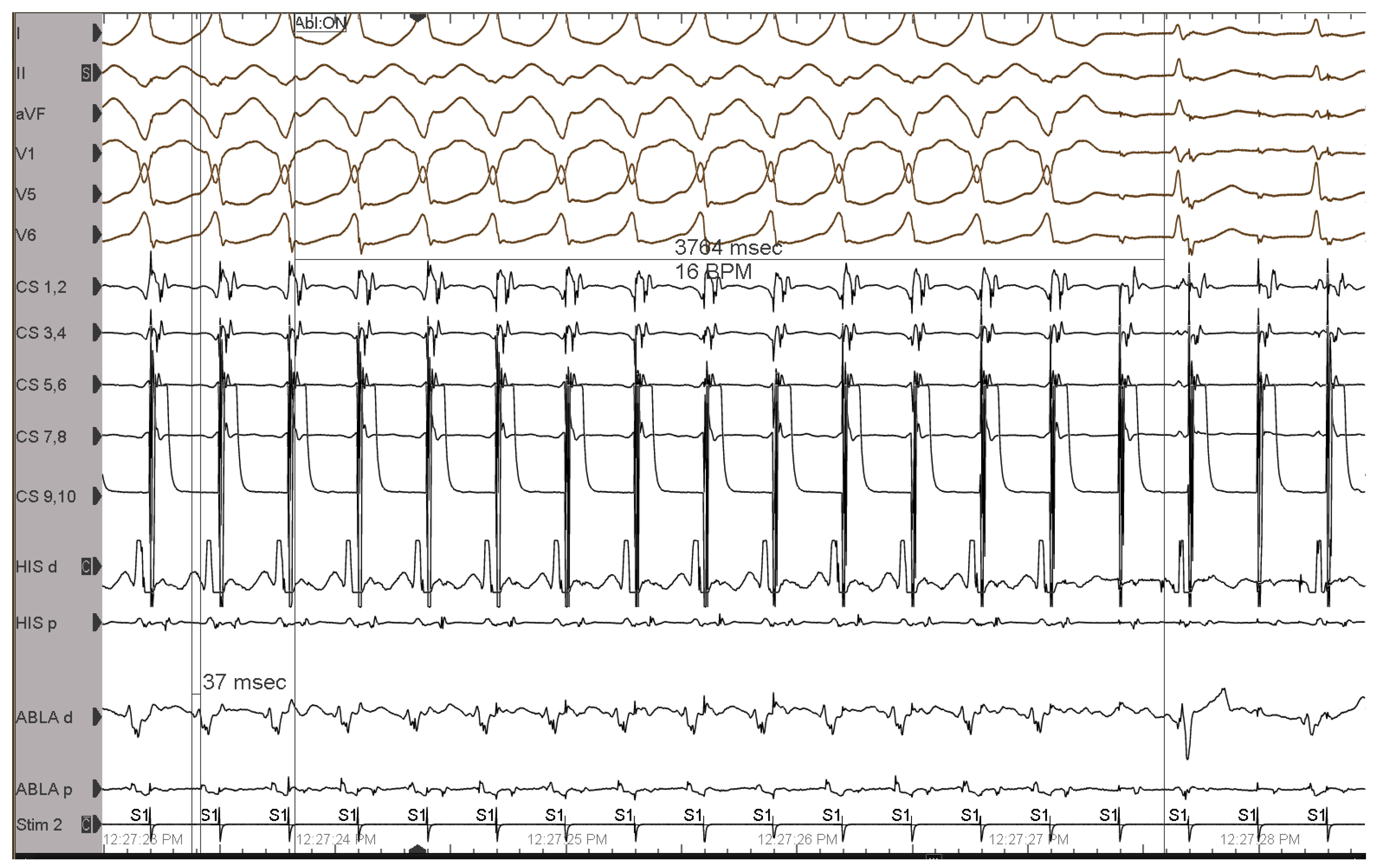
During full pre-excitation elicited by fast atrial pacing (CL 290 ms), radiofrequency application at the ventricular insertion of the accessory pathway induced a loss of pre-excitation in 3.5 s; ECG leads from the top: DI, DII, aVF, V1, V5, V6. His d and His p indicate distal and proximal His bundle electrogram; CS 1-10, coronary sinus distal to proximal; Abla d and p, ablation catheter distal and proximal, respectively, placed in the RV.
Figure 5.
During full pre-excitation elicited by fast atrial pacing (CL 290 ms), radiofrequency application at the ventricular insertion of the accessory pathway induced a loss of pre-excitation in 3.5 s; ECG leads from the top: DI, DII, aVF, V1, V5, V6. His d and His p indicate distal and proximal His bundle electrogram; CS 1-10, coronary sinus distal to proximal; Abla d and p, ablation catheter distal and proximal, respectively, placed in the RV.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Deaconu, A.; Gondos, V.; Vatasescu, R. Not Just a One-Way: Mahaim Accessory Pathway Concomitantly Supporting Orthodromic Atrioventricular Re-Entrant Tachycardia. J. Clin. Med. 2023, 12, 159. https://doi.org/10.3390/jcm12010159
AMA Style
Deaconu A, Gondos V, Vatasescu R. Not Just a One-Way: Mahaim Accessory Pathway Concomitantly Supporting Orthodromic Atrioventricular Re-Entrant Tachycardia. Journal of Clinical Medicine. 2023; 12(1):159. https://doi.org/10.3390/jcm12010159
Chicago/Turabian StyleDeaconu, Alexandru, Viviana Gondos, and Radu Vatasescu. 2023. "Not Just a One-Way: Mahaim Accessory Pathway Concomitantly Supporting Orthodromic Atrioventricular Re-Entrant Tachycardia" Journal of Clinical Medicine 12, no. 1: 159. https://doi.org/10.3390/jcm12010159
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.