
Dysfunctional Beliefs and Cognitive Performance across Symptom Dimensions in Childhood and Adolescent OCD
 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Procedure
2.3. Data Analysis
3. Results
3.1. Demographic and Clinical Characteristics
3.2. OCD Symptoms, Dysfunctional Beliefs and General Functioning
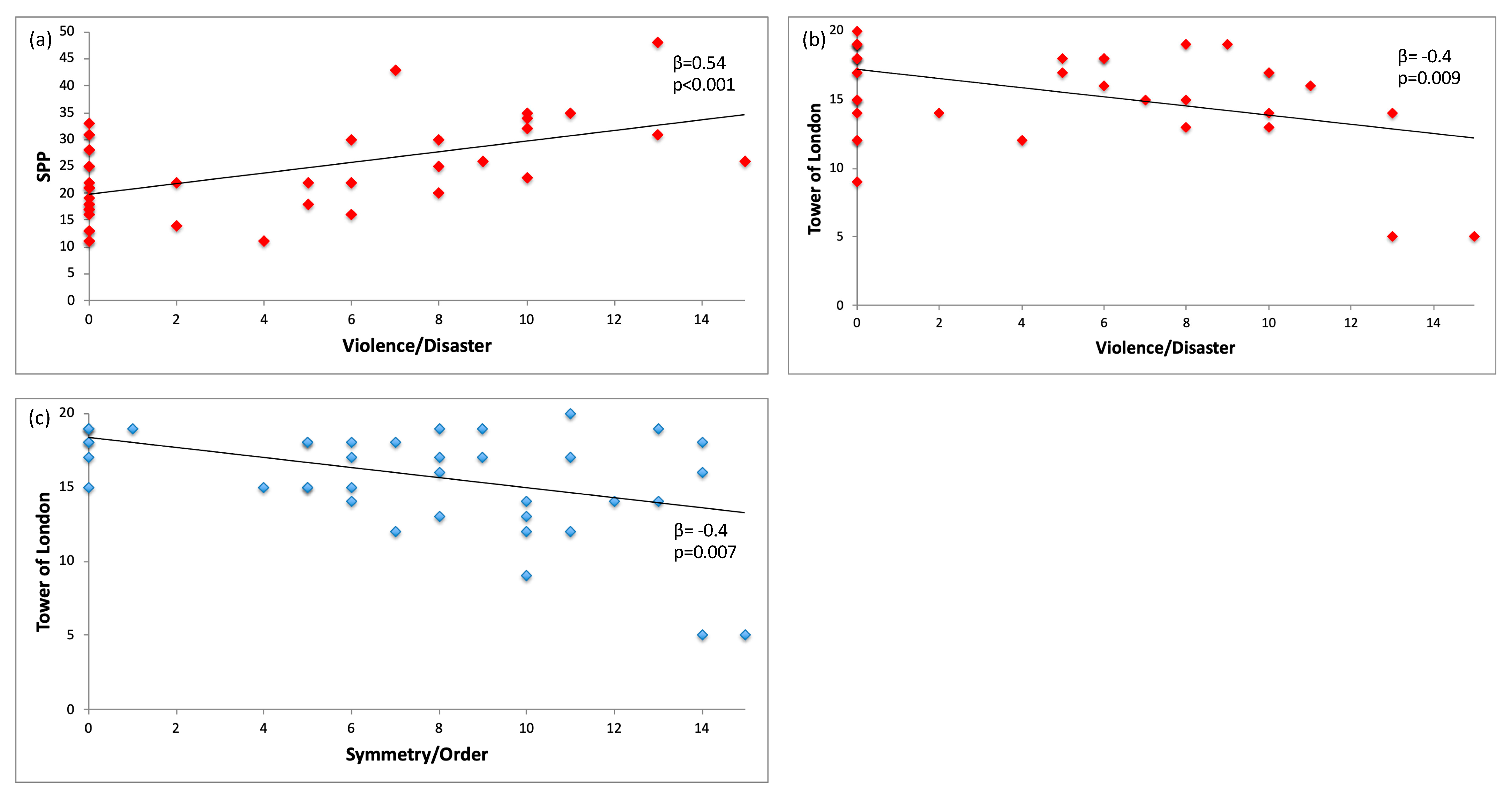
3.3. OCD Symptom Dimensions, Dysfunctional Beliefs and Cognitive Profile
4. Discussion
4.1. Relationship between OCD Symptom Dimensions and Dysfunctional Beliefs
4.2. OCD Symptom Dimensions and Cognitive Profile
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mataix-Cols, D.; Rauch, S.L.; Baer, L.; Eisen, J.L.; Shera, D.M.; Goodman, W.K.; Rasmussen, S.A.; Jenike, M.A. Symptom Stability in Adult Obsessive-Compulsive Disorder: Data from a Naturalistic Two-Year Follow-up Study. Am. J. Psychiatry 2002, 159, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Van Grootheest, D.S.; Boomsma, D.I.; Hettema, J.M.; Kendler, K.S. Heritability of Obsessive-Compulsive Symptom Dimensions. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2008, 147, 473–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iervolino, A.C.; Rijsdijk, F.V.; Cherkas, L.; Fullana, M.A.; Mataix-Cols, D. A Multivariate Twin Study of Obsessive-Compulsive Symptom Dimensions. Arch. Gen. Psychiatry 2011, 68, 637–644. [Google Scholar] [CrossRef] [Green Version]
- Van Den Heuvel, O.A.; Remijnse, P.L.; Mataix-Cols, D.; Vrenken, H.; Groenewegen, H.J.; Uylings, H.B.M.; Van Balkom, A.J.L.M.; Veltman, D.J. The Major Symptom Dimensions of Obsessive-Compulsive Disorder Are Mediated by Partially Distinct Neural Systems. Brain 2009, 132, 853–868. [Google Scholar] [CrossRef] [PubMed]
- Mataix-Cols, D.; Wooderson, S.; Lawrence, N.; Brammer, M.J.; Speckens, A.; Phillips, M.L. Distinct Neural Correlates of Washing, Checking, and Hoarding Symptom Dimensions in Obsessive-Compulsive Disorder. Arch. Gen. Psychiatry 2004. [Google Scholar] [CrossRef] [Green Version]
- Cherian, A.V.; Math, S.B.; Kandavel, T.; Reddy, Y.C.J. A 5-Year Prospective Follow-up Study of Patients with Obsessive-Compulsive Disorder Treated with Serotonin Reuptake Inhibitors. J. Affect. Disord. 2014, 152–154, 387–394. [Google Scholar] [CrossRef]
- Williams, M.T.; Mugno, B.; Franklin, M.; Faber, S. Symptom Dimensions in Obsessive-Compulsive Disorder: Phenomenology and Treatment Outcomes with Exposure and Ritual Prevention. Psychopathology 2013, 46, 365–376. [Google Scholar] [CrossRef] [Green Version]
- Landeros-Weisenberger, A.; Bloch, M.H.; Kelmendi, B.; Wegner, R.; Nudel, J.; Dombrowski, P.; Pittenger, C.; Krystal, J.H.; Goodman, W.K.; Leckman, J.F.; et al. Dimensional Predictors of Response to SRI Pharmacotherapy in Obsessive-Compulsive Disorder. J. Affect. Disord. 2010, 121, 175–179. [Google Scholar] [CrossRef] [Green Version]
- Cifter, A.; Erdogdu, A. Are the Symptom Dimensions a Predictor of Short-Term Response to Pharmacotherapy in Pediatric Obsessive-Compulsive Disorder? A Retrospective Cohort Study. Indian J. Psychiatry 2022, 64, 395–400. [Google Scholar] [CrossRef]
- Liu, X.; Yang, X.; Wang, P.; Li, Z. Validation of Symptom Dimensions and Sub-Type Responses in Cognitive Behavioral Therapy in Obsessive Compulsive Disorder: A Systemic Review and Meta-Analysis. Int. J. Ment. Health Promot. 2022, 24, 843–854. [Google Scholar] [CrossRef]
- Rachman, S. A Cognitive Theory of Obsessions. In Behavior and Cognitive Therapy Today; Università di Padova: Padova, Italy, 1998; pp. 209–222. [Google Scholar]
- Salkovskis, P.M. Understanding and Treating Obsessive-Compulsive Disorder. Behav. Res. Ther. 1999, 37, S29–S52. [Google Scholar] [CrossRef] [PubMed]
- Valleni-Basile, L.A.; Garrison, C.Z.; Waller, J.L.; Addy, C.L.; McKeown, R.E.; Jackson, K.L.; Cuffe, S.P. Incidence of Obsessive-Compulsive Disorder in a Community Sample of Young Adolescents. J. Am. Acad. Child Adolesc. Psychiatry 1996, 35, 898–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steketee, G.; Frost, R.; Bhar, S.; Bouvard, M.; Calamari, J.; Carmin, C.; Clark, D.A.; Cottraux, J.; Emmelkamp, P.; Forrester, E.; et al. Psychometric Validation of the Obsessive Belief Questionnaire and Interpretation of Intrusions Inventory—Part 2: Factor Analyses and Testing of a Brief Version. Behav. Res. Ther. 2005, 43, 1527–1542. [Google Scholar] [CrossRef]
- Rachman, S. A Cognitive Theory of Compulsive Checking. Behav. Res. Ther. 2002, 40, 625–639. [Google Scholar] [CrossRef] [PubMed]
- Rachman, S. Fear of Contamination. Behav. Res. Ther. 2004, 42, 1227–1255. [Google Scholar] [CrossRef] [PubMed]
- Summerfeldt, L.J. Ordering, Incompleteness, and Arranging. In Clinical Handbook of Obsessive-Compulsive Disorder and Related Problems; Johns Hopkins University Press: Baltimore, MD, USA, 2008; ISBN1 0-8018-8697-X (Hardcover). ISBN2 978-0-8018-8697-3 (Hardcover). [Google Scholar]
- Wheaton, M.G.; Abramowitz, J.S.; Berman, N.C.; Riemann, B.C.; Hale, L.R. The Relationship between Obsessive Beliefs and Symptom Dimensions in Obsessive-Compulsive Disorder. Behav. Res. Ther. 2010, 48, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Tolin, D.F.; Brady, R.E.; Hannan, S. Obsessional Beliefs and Symptoms of Obsessive-Compulsive Disorder in a Clinical Sample. J. Psychopathol. Behav. Assess. 2008, 30, 31–42. [Google Scholar] [CrossRef]
- Cordeiro, T.; Sharma, M.; Thennarasu, K.; Janardhan Reddy, Y. Symptom Dimensions in Obsessive-Compulsive Disorder and Obsessive Beliefs. Indian J. Psychol. Med. 2015, 37, 403–408. [Google Scholar] [CrossRef] [Green Version]
- Soreni, N.; Streiner, D.; McCabe, R.; Bullard, C.; Swinson, R.; Greco, A.; Pires, P.; Szatmari, P. Dimensions of Perfectionism in Children and Adolescents with Obsessive-Compulsive Disorder. J. Can. Acad. Child Adolesc. Psychiatry 2014, 23, 136–141. [Google Scholar]
- Pozza, A.; Albert, U.; Dèttore, D. Perfectionism and Intolerance of Uncertainty Are Predictors of OCD Symptoms in Children and Early Adolescents: A Prospective, Cohort, One-Year, Follow-up Study. Clin. Neuropsychiatry 2019, 16, 53–61. [Google Scholar]
- Schultz, R.T.; Evans, D.W.; Wolff, M. Neuropsychological Models of Childhood Obsessive-Compulsive Disorder. Child Adolesc. Psychiatr. Clin. N. Am. 1999, 8, 513–531. [Google Scholar] [CrossRef] [PubMed]
- Grisham, J.R.; Anderson, T.M.; Poulton, R.; Moffitt, T.E.; Andrews, G. Childhood Neuropsychological Deficits Associated with Adult Obsessive-Compulsive Disorder. Br. J. Psychiatry 2009, 195, 138–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakao, T.; Okada, K.; Kanba, S. Neurobiological Model of Obsessive-Compulsive Disorder: Evidence from Recent Neuropsychological and Neuroimaging Findings. Psychiatry Clin. Neurosci. 2014, 68, 587–605. [Google Scholar] [CrossRef]
- Abramovitch, A.; Abramowitz, J.S.; Mittelman, A. The Neuropsychology of Adult Obsessive-Compulsive Disorder: A Meta-Analysis. Clin. Psychol. Rev. 2013, 33, 1163–1171. [Google Scholar] [CrossRef]
- Snyder, H.R.; Kaiser, R.H.; Warren, S.L.; Heller, W. Obsessive-Compulsive Disorder Is Associated With Broad Impairments in Executive Function: A Meta-Analysis. Clin. Psychol. Sci. 2015, 3, 301–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geller, D.A.; Abramovitch, A.; Mittelman, A.; Stark, A.; Ramsey, K.; Cooperman, A.; Baer, L.; Stewart, S.E. Neurocognitive Function in Paediatric Obsessive-Compulsive Disorder. World J. Biol. Psychiatry Off. J. World Fed. Soc. Biol. Psychiatry 2018, 19, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Ornstein, T.J.; Arnold, P.; Manassis, K.; Mendlowitz, S.; Schachar, R. Neuropsychological Performance in Childhood OCD: A Preliminary Study. Depress. Anxiety 2010, 27, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Shin, M.-S.; Choi, H.; Kim, H.; Hwang, J.-W.; Kim, B.-N.; Cho, S.-C. A Study of Neuropsychological Deficit in Children with Obsessive-Compulsive Disorder. Eur. Psychiatry 2008, 23, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Isik Taner, Y.; Erdogan Bakar, E.; Oner, O. Impaired Executive Functions in Paediatric Obsessive-Compulsive Disorder Patients. Acta Neuropsychiatr. 2011, 23, 272–281. [Google Scholar] [CrossRef]
- Abramovitch, A.; Abramowitz, J.S.; Mittelman, A.; Stark, A.; Ramsey, K.; Geller, D.A. Research Review: Neuropsychological Test Performance in Pediatric Obsessive-Compulsive Disorder—A Meta-Analysis. J. Child Psychol. Psychiatry Allied Discip. 2015, 56, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Abramovitch, A.; De Nadai, A.S.; Geller, D.A. Neurocognitive Endophenotypes in Pediatric OCD Probands, Their Unaffected Parents and Siblings. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 110, 110283. [Google Scholar] [CrossRef]
- Rosenberg, D.R.; Keshavan, M.S. Toward a Neurodevelopmental Model of Obsessive-Compulsive Disorder. Biol. Psychiatry 1998, 43, 623–640. [Google Scholar] [CrossRef]
- Geller, D.A.; Homayoun, S.; Johnson, G. Developmental Considerations in Obsessive Compulsive Disorder: Comparing Pediatric and Adult-Onset Cases. Front. Psychiatry 2021, 12, 678538. [Google Scholar] [CrossRef]
- Boedhoe, P.S.W.; Schmaal, L.; Abe, Y.; Ameis, S.H.; Arnold, P.D.; Batistuzzo, M.C.; Benedetti, F.; Beucke, J.C.; Bollettini, I.; Bose, A.; et al. Distinct Subcortical Volume Alterations in Pediatric and Adult OCD: A Worldwide Meta- and Mega-Analysis. Am. J. Psychiatry 2017, 174, 60–69. [Google Scholar] [CrossRef]
- Piras, F.; Piras, F.; Abe, Y.; Agarwal, S.M.; Anticevic, A.; Ameis, S.; Arnold, P.; Banaj, N.; Bargalló, N.; Batistuzzo, M.C.; et al. White Matter Microstructure and Its Relation to Clinical Features of Obsessive–Compulsive Disorder: Findings from the ENIGMA OCD Working Group. Transl. Psychiatry 2021, 11, 1–11. [Google Scholar] [CrossRef]
- Lawrence, N.S.; Wooderson, S.; Mataix-Cols, D.; David, R.; Speckens, A.; Phillips, M.L. Decision Making and Set Shifting Impairments Are Associated with Distinct Symptom Dimensions in Obsessive-Compulsive Disorder. Neuropsychology 2006, 20, 409–419. [Google Scholar] [CrossRef]
- Suhas, S.; Rao, N. Neurocognitive Deficits in Obsessive-Compulsive Disorder: A Selective Review. Indian J. Psychiatry 2019, 61 (Suppl. S1). [Google Scholar]
- Hashimoto, N.; Nakaaki, S.; Omori, I.M.; Fujioi, J.; Noguchi, Y.; Murata, Y.; Sato, J.; Tatsumi, H.; Torii, K.; Mimura, M.; et al. Distinct Neuropsychological Profiles of Three Major Symptom Dimensions in Obsessive-Compulsive Disorder. Psychiatry Res. 2011, 187, 166–173. [Google Scholar] [CrossRef]
- Saremi, A.A.; Shariat, S.V.; Nazari, M.A.; Dolatshahi, B. Neuropsychological Functioning in Obsessive-Compulsive Washers: Drug-Naive without Depressive Symptoms. Basic Clin. Neurosci. 2017, 8, 233–248. [Google Scholar] [CrossRef] [Green Version]
- Tallis, F.; Pratt, P.; Jamani, N. Obsessive Compulsive Disorder, Checking, and Non-Verbal Memory: A Neuropsychological Investigation. Behav. Res. Ther. 1999, 37, 161–166. [Google Scholar] [CrossRef]
- Salkovskis, P.M. Obsessional-Compulsive Problems: A Cognitive-Behavioural Analysis. Behav. Res. Ther. 1985, 23, 571–583. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- American Psychiatric Association. The Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; DSM 5; American Psychiatric Publishing, Inc.: Washington, DC, USA, 2013; ISBN 9780890425541. [Google Scholar]
- First, M.B. SCID-5-CV: Structured Clinical Interview for DSM-5 Disorders, Clinician Version; American Psychiatric Association: Washington, DC, USA, 2016; ISBN 9781585624614. [Google Scholar]
- Wechsler, D. Wechsler Adult Intelligence Scale, 4th ed.; Edizione Italiana; Arturo Orsini e Lina Pezzuti, Giunti Psychometrics: Firenze, Italy, 2014. [Google Scholar]
- Vaughn-Blount, K.; Watson, S.T.; Kokol, A.L.; Grizzle, R.; Carney, R.N.; Rich, S.S.; LeClere, S.; Stylianou, M.; Anastassiou-Hadjicharalambous, X.; Joann Lang, M.; et al. Wechsler Intelligence Scale for Children, Fourth Edition. In Encyclopedia of Child Behavior and Development; Springer: Berlin/Heidelberg, Germany, 2011; pp. 1553–1555. [Google Scholar]
- Iorio, M.; Spalletta, G.; Chiapponi, C.; Luccichenti, G.; Cacciari, C.; Orfei, M.D.; Caltagirone, C.; Piras, F. White Matter Hyperintensities Segmentation: A New Semi-Automated Method. Front. Aging Neurosci. 2013, 5, 76. [Google Scholar] [CrossRef]
- Scahill, L.; Riddle, M.A.; McSwiggin-Hardin, M.; Ort, S.I.; King, R.A.; Goodman, W.K.; Cicchetti, D.; Leckman, J.F. Children’s Yale-Brown Obsessive Compulsive Scale: Reliability and Validity. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 844–852. [Google Scholar] [CrossRef]
- Rosario-Campos, M.C.; Miguel, E.C.; Quatrano, S.; Chacon, P.; Ferrao, Y.; Findley, D.; Katsovich, L.; Scahill, L.; King, R.A.; Woody, S.R.; et al. The Dimensional Yale–Brown Obsessive–Compulsive Scale (DY-BOCS): An Instrument for Assessing Obsessive–Compulsive Symptom Dimensions. Mol. Psychiatry 2006, 11, 495–504. [Google Scholar] [CrossRef] [Green Version]
- Flett, G.L.; Hewitt, P.L.; Besser, A.; Su, C.; Vaillancourt, T.; Boucher, D.; Munro, Y.; Davidson, L.A.; Gale, O. The Child–Adolescent Perfectionism Scale. J. Psychoeduc. Assess. 2016, 34, 634–652. [Google Scholar] [CrossRef]
- Comer, J.S.; Roy, A.K.; Furr, J.M.; Gotimer, K.; Beidas, R.S.; Dugas, M.J.; Kendall, P.C. The Intolerance of Uncertainty Scale for Children: A Psychometric Evaluation. Psychol Assess 2009, 21, 402–411. [Google Scholar] [CrossRef] [Green Version]
- Chorpita, B.F.; Tracey, S.A.; Brown, T.A.; Collica, T.J.; Barlow, D.H. Assessment of Worry in Children and Adolescents: An Adaptation of the Penn State Worry Questionnaire. Behav. Res. Ther. 1997, 35, 569–581. [Google Scholar] [CrossRef]
- Kovacs, M. The Children’s Depression Inventory (CDI). Psychopharmacol. Bull. 1985, 21, 995–998. [Google Scholar]
- Shaffer, D. A Children’s Global Assessment Scale (CGAS). Arch. Gen. Psychiatry 1983, 40, 1228. [Google Scholar] [CrossRef]
- Raven, J. Raven Progressive Matrices. In Handbook of Nonverbal Assessment; Springer: Berlin/Heidelberg, Germany, 2003; pp. 223–237. [Google Scholar]
- Caffarra, P.; Vezzadini, G.; Dieci, F.; Zonato, F.; Venneri, A. A Short Version of the Stroop Test: Normative Data in an Italian Population Sample. Nuova Riv. Neurol. 2002, 12, 111–115. [Google Scholar]
- Scarpina, F.; Tagini, S. The Stroop Color and Word Test. Front. Psychol. 2017, 8, 557. [Google Scholar] [CrossRef] [Green Version]
- Barbarotto, R.; Laiacona, M.; Frosio, R.; Vecchio, M.; Farinato, A.; Capitani, E. A Normative Study on Visual Reaction Times and Two Stroop Colour-Word Tests. Ital. J. Neurol. Sci. 1998, 19, 161–170. [Google Scholar] [CrossRef]
- Osterrieth, P.A. Le Test de Copie d’une Figure Complexe; Contribution à l’étude de La Perception et de La Mémoire. Arch. Psychol. 1944, 30, 206–356. [Google Scholar]
- Habeck, C.; Rakitin, B.; Steffener, J.; Stern, Y. Contrasting Visual Working Memory for Verbal and Non-Verbal Material with Multivariate Analysis of FMRI. Brain Res. 2012, 1467, 27–41. [Google Scholar] [CrossRef] [Green Version]
- Keefe, R.S.E.; Goldberg, T.E.; Harvey, P.D.; Gold, J.M.; Poe, M.P.; Coughenour, L. The Brief Assessment of Cognition in Schizophrenia: Reliability, Sensitivity, and Comparison with a Standard Neurocognitive Battery. Schizophr. Res. 2004, 68, 283–297. [Google Scholar] [CrossRef]
- Marquaridt, D.W. Generalized Inverses, Ridge Regression, Biased Linear Estimation, and Nonlinear Estimation. Technometrics 1970, 12, 591–612. [Google Scholar] [CrossRef]
- Sharma, E.; Tripathi, A.; Grover, S.; Avasthi, A.; Dan, A.; Srivastava, C.; Goyal, N.; Manohari, S.M.; Reddy, J. Clinical Profile of Obsessive-Compulsive Disorder in Children and Adolescents: A Multicentric Study from India. Indian J. Psychiatry 2019, 61, 564–571. [Google Scholar] [CrossRef]
- Weidle, B.; Ivarsson, T.; Thomsen, P.H.; Lydersen, S.; Jozefiak, T. Quality of Life in Children with OCD before and after Treatment. Eur. Child Adolesc. Psychiatry 2015, 24, 1061–1074. [Google Scholar] [CrossRef] [Green Version]
- Krebs, G.; Heyman, I. Obsessive-Compulsive Disorder in Children and Adolescents. Arch. Dis. Child. 2015, 100, 495–499. [Google Scholar] [CrossRef] [Green Version]
- Brakoulias, V.; Perkes, I.E.; Tsalamanios, E. A Call for Prevention and Early Intervention in Obsessive-Compulsive Disorder. Early Interv. Psychiatry 2018, 12, 572–577. [Google Scholar] [CrossRef]
- Steketee, G.; Frost, R.; Bhar, S.; Bouvard, M.; Calamari, J.; Carmin, C.; Clark, D.A.; Cottraux, J.; Emmelkamp, P.; Forrester, E.; et al. Psychometric Validation of the Obsessive Beliefs Questionnaire and the Interpretation of Intrusions Inventory: Part I. Behav. Res. Ther. 2003, 41, 863–878. [Google Scholar] [CrossRef]
- Salkovskis, P.; Shafran, R.; Rachman, S.; Freeston, M.H. Multiple Pathways to Inflated Responsibility Beliefs in Obsessional Problems: Possible Origins and Implications for Therapy and Research. Behav. Res. Ther. 1999, 37, 1055–1072. [Google Scholar] [CrossRef]
- Frost, R.O.; Novara, C.; Rhéaume, J. Perfectionism in Obsessive Compulsive Disorder. In Cognitive Approaches to Obsessions and Compulsions; Elsevier: Amsterdam, The Netherlands, 2002; pp. 91–105. [Google Scholar]
- Mataix-Cols, D.; Do Rosario-Campos, M.C.; Leckman, J.F. A Multidimensional Model of Obsessive-Compulsive Disorder. Am. J. Psychiatry 2005, 162, 228–238. [Google Scholar] [CrossRef] [Green Version]
- Summerfeldt, L.J. Understanding and Treating Incompleteness in Obsessive-Compulsive Disorder. J. Clin. Psychol. 2004, 60, 1155–1168. [Google Scholar] [CrossRef]
- Mataix-Cols, D.; Nakatani, E.; Micali, N.; Heyman, I. Structure of Obsessive-Compulsive Symptoms in Pediatric OCD. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 773–778. [Google Scholar] [CrossRef]
- Evans, D.W.; Leckman, J.F.; Carter, A.; Reznick, J.S.; Henshaw, D.; King, R.A.; Pauls, D. Ritual, Habit, and Perfectionism: The Prevalence and Development of Compulsive-like Behavior in Normal Young Children. Child Dev. 1997, 68, 58–68. [Google Scholar] [CrossRef]
- Julien, D.; O’Connor, K.P.; Aardema, F.; Todorov, C. The Specificity of Belief Domains in Obsessive-Compulsive Symptom Subtypes. Pers. Individ. Dif. 2006, 41, 1205–1216. [Google Scholar] [CrossRef]
- Cervin, M.; McNeel, M.M.; Wilhelm, S.; McGuire, J.F.; Murphy, T.K.; Small, B.J.; Geller, D.A.; Storch, E.A. Cognitive Beliefs Across the Symptom Dimensions of Pediatric Obsessive-Compulsive Disorder: Type of Symptom Matters. Behav. Ther. 2022, 53, 240–254. [Google Scholar] [CrossRef]
- Foa, E.B.; Coles, M.; Huppert, J.D.; Pasupuleti, R.V.; Franklin, M.E.; March, J. Development and Validation of a Child Version of the Obsessive Compulsive Inventory. Behav. Ther. 2010, 41, 121–132. [Google Scholar] [CrossRef]
- Coles, M.E.; Wolters, L.H.; Sochting, I.; De Haan, E.; Pietrefesa, A.S.; Whiteside, S.P. Development and Initial Validation of the Obsessive Belief Questionnaire-Child Version (OBQ-CV). Depress. Anxiety 2010, 27, 982–991. [Google Scholar] [CrossRef]
- Tolin, D.F.; Woods, C.M.; Abramowitz, J.S. Relationship between Obsessive Beliefs and Obsessive-Compulsive Symptoms. Cognit. Ther. Res. 2003, 27, 657–669. [Google Scholar] [CrossRef]
- Chamberlain, S.R.; Blackwell, A.D.; Fineberg, N.A.; Robbins, T.W.; Sahakian, B.J. The Neuropsychology of Obsessive Compulsive Disorder: The Importance of Failures in Cognitive and Behavioural Inhibition as Candidate Endophenotypic Markers. Neurosci. Biobehav. Rev. 2005, 29, 399–419. [Google Scholar] [CrossRef]
- Omori, I.M.; Murata, Y.; Yamanishi, T.; Nakaaki, S.; Akechi, T.; Mikuni, M.; Furukawa, T.A. The Differential Impact of Executive Attention Dysfunction on Episodic Memory in Obsessive-Compulsive Disorder Patients with Checking Symptoms vs. Those with Washing Symptoms. J. Psychiatr. Res. 2007, 41, 776–784. [Google Scholar] [CrossRef]
- McGuire, J.F.; Crawford, E.A.; Park, J.M.; Storch, E.A.; Murphy, T.K.; Larson, M.J.; Lewin, A.B. Neuropsychological Performance across Symptom Dimensions in Pediatric Obsessive Compulsive Disorder. Depress. Anxiety 2014, 31, 988–996. [Google Scholar] [CrossRef]
- Garcia-Delgar, B.; de la Serna, E.; Lera, S.; Varela, E.; Andrés-Perpiñá, S.; Lázaro, L. Neuropsychological Functioning in Pediatric Obsessive-Compulsive Disorder: One Size Does Not Fit All. J. Obs. Compuls. Relat. Disord. 2018, 16, 36–42. [Google Scholar] [CrossRef]
- Kashyap, H.; Kumar, J.K.; Kandavel, T.; Reddy, Y.C.J. Relationships between Neuropsychological Variables and Factor-Analysed Symptom Dimensions in Obsessive Compulsive Disorder. Psychiatry Res. 2017, 249, 58–64. [Google Scholar] [CrossRef]
- Egan, S.J.; Wade, T.D.; Shafran, R. The Transdiagnostic Process of Perfectionism. Rev. Psicopatol. Psicol. Clin. 2012, 17, 279–294. [Google Scholar] [CrossRef] [Green Version]
- Flamarique, I.; Plana, M.T.; Castro-Fornieles, J.; Borràs, R.; Moreno, E.; Lázaro, L. Comparison of Perfectionism Dimensions in Adolescents with Anorexia Nervosa or Obsessive-Compulsive Disorder. J. Can. Acad. Child Adolesc. Psychiatry 2019, 28, 45–54. [Google Scholar]
- Caspi, A.; Houts, R.M.; Ambler, A.; Danese, A.; Elliott, M.L.; Hariri, A.; Harrington, H.L.; Hogan, S.; Poulton, R.; Ramrakha, S.; et al. Longitudinal Assessment of Mental Health Disorders and Comorbidities Across 4 Decades Among Participants in the Dunedin Birth Cohort Study. JAMA Netw. Open 2020, 3, e203221. [Google Scholar] [CrossRef]
- WMA. WMA Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects—WMA—The World Medical Association; World Medical Association: Ferney-Voltaire, France, 2018. [Google Scholar]


{kind=link}
| OCD (N = 41) Mean (SD) | |
|---|---|
| Age | 14 (2.2) |
| Education | 7.8 (2) |
| Gender (males) | N = 30 (73%) |
| Illness duration (years) | 4.2 (3.1) |
| CY-BOCS tot | 23.1 (8.6) |
| CY-BOCS obsessive | 11.7 (4.3) |
| CY-BOCS compulsive | 11.4 (4.5) |
| Symmetry/Order | 7.3 (4.5) |
| Contamination/Cleaning | 4.8 (5) |
| Violence/Disaster | 4.1 (4.7) |
| Hoarding/Collecting | 2.6 (3.4) |
| Miscellaneous | 2.6 (3.5) |
| Somatic | 2.5 (3.9) |
| Sex/Religious | 2.1 (3.7) |
| CDI tot | 13.9 (7.2) |
| CAPS tot | 58.7 (17.3) |
| SOP | 34.8 (10.8) |
| SPP | 23.9 (8.6) |
| IUSC | 67.2 (26.4) |
| PSWQ-C | 34.4 (8.7) |
| CGAS | 49.4 (9.2) |
| CY-BOCS Tot | CY-BOCS Obsessive | CY-BOCS Compulsive | Contam. Cleaning | Symmetry Order | Violence/ Disaster | IUSC | CAPS Tot | SOP | SPP | PSWQ-C | CDI | CGAS | SCWT Word | SCWT Colour | SCWT Interf. | Go/No Go Hit | Go/No Go Mean RTs | RCPM | ROCF Copy | ROCF Recall | Tower of London | DIR Hit | DIR Mean RTs | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CY-BOCS tot | 1.0 | 1.0 | 1.0 | 0.4 | 0.6 | 0.3 | 0.4 | 0.4 | 0.3 | 0.4 | 0.3 | 0.4 | −0.7 | 0.0 | 0.1 | 0.1 | 0.0 | −0.1 | −0.2 | 0.0 | 0.2 | −0.2 | 0.0 | −0.1 |
| CY-BOCS obsessive | 1.0 | 1.0 | 0.9 | 0.4 | 0.5 | 0.4 | 0.4 | 0.5 | 0.5 | 0.4 | 0.3 | 0.4 | −0.7 | 0.1 | 0.1 | 0.0 | 0.0 | −0.1 | −0.1 | 0.0 | 0.2 | −0.2 | 0.0 | −0.1 |
| CY-BOCS compulsive | 1.0 | 0.9 | 1.0 | 0.4 | 0.6 | 0.2 | 0.3 | 0.3 | 0.2 | 0.2 | 0.3 | 0.4 | −0.6 | −0.1 | 0.1 | 0.1 | −0.1 | −0.1 | −0.2 | 0.1 | 0.2 | −0.2 | 0.0 | 0.0 |
| Contam./ Cleaning | 0.4 | 0.4 | 0.4 | 1.0 | 0.0 | 0.1 | 0.0 | 0.2 | 0.1 | 0.3 | 0.1 | −0.2 | −0.3 | −0.1 | 0.0 | −0.2 | −0.2 | −0.1 | 0.0 | −0.2 | 0.1 | 0.0 | 0.1 | −0.1 |
| Symmetry Order | 0.6 | 0.5 | 0.6 | 0.0 | 1.0 | 0.3 | 0.3 | 0.4 | 0.4 | 0.3 | 0.4 | 0.2 | −0.5 | −0.1 | 0.0 | 0.1 | 0.2 | 0.2 | −0.2 | −0.1 | −0.1 | −0.4 | 0.2 | −0.1 |
| Violence/ Disaster | 0.3 | 0.4 | 0.2 | 0.1 | 0.3 | 1.0 | 0.4 | 0.4 | 0.3 | 0.5 | 0.4 | 0.2 | −0.3 | 0.2 | 0.4 | 0.2 | 0.1 | 0.2 | −0.2 | −0.2 | −0.1 | −0.4 | 0.0 | −0.3 |
| IUSC | 0.4 | 0.4 | 0.3 | 0.0 | 0.3 | 0.4 | 1.0 | 0.7 | 0.6 | 0.6 | 0.7 | 0.5 | −0.3 | 0.1 | −0.1 | −0.2 | 0.3 | 0.1 | 0.0 | 0.1 | 0.0 | −0.1 | 0.2 | −0.2 |
| CAPS tot | 0.4 | 0.5 | 0.3 | 0.2 | 0.4 | 0.4 | 0.7 | 1.0 | 0.9 | 0.9 | 0.5 | 0.2 | −0.4 | 0.2 | 0.1 | 0.0 | 0.2 | 0.0 | 0.0 | 0.1 | 0.1 | −0.1 | 0.4 | −0.4 |
| SOP | 0.3 | 0.5 | 0.2 | 0.1 | 0.4 | 0.3 | 0.6 | 0.9 | 1.0 | 0.6 | 0.5 | 0.2 | −0.3 | 0.3 | 0.1 | 0.0 | 0.2 | 0.1 | 0.0 | 0.1 | 0.1 | 0.0 | 0.3 | −0.3 |
| SPP | 0.4 | 0.4 | 0.2 | 0.3 | 0.3 | 0.5 | 0.6 | 0.9 | 0.6 | 1.0 | 0.4 | 0.1 | −0.3 | 0.1 | 0.0 | 0.1 | 0.2 | −0.1 | 0.0 | 0.0 | 0.2 | −0.2 | 0.3 | −0.4 |
| PSWQ-C | 0.3 | 0.3 | 0.3 | 0.1 | 0.4 | 0.4 | 0.7 | 0.5 | 0.5 | 0.4 | 1.0 | 0.5 | −0.3 | 0.2 | 0.2 | −0.2 | 0.1 | 0.4 | −0.2 | 0.0 | −0.1 | −0.1 | 0.3 | 0.0 |
| CDI | 0.4 | 0.4 | 0.4 | −0.2 | 0.2 | 0.2 | 0.5 | 0.2 | 0.2 | 0.1 | 0.5 | 1.0 | −0.2 | 0.0 | −0.1 | −0.1 | 0.2 | 0.1 | −0.1 | 0.0 | −0.1 | −0.1 | 0.1 | −0.1 |
| CGAS | −0.7 | −0.7 | −0.6 | −0.3 | −0.5 | −0.3 | −0.3 | −0.4 | −0.3 | −0.3 | −0.3 | −0.2 | 1.0 | −0.1 | −0.1 | −0.1 | 0.1 | −0.2 | 0.2 | 0.1 | 0.1 | 0.3 | 0.1 | 0.2 |
| SCWT word | 0.0 | 0.1 | −0.1 | −0.1 | −0.1 | 0.2 | 0.1 | 0.2 | 0.3 | 0.1 | 0.2 | 0.0 | −0.1 | 1.0 | 0.7 | 0.6 | -0.4 | 0.2 | -0.3 | −0.1 | −0.1 | 0.0 | -0.4 | 0.3 |
| SCWT colour | 0.1 | 0.1 | 0.1 | 0.0 | 0.0 | 0.4 | −0.1 | 0.1 | 0.1 | 0.0 | 0.2 | −0.1 | −0.1 | 0.7 | 1.0 | 0.6 | -0.3 | 0.2 | -0.5 | -0.2 | -0.2 | -0.2 | -0.4 | 0.3 |
| SCWT interf. | 0.1 | 0.0 | 0.1 | -0.2 | 0.1 | 0.2 | −0.2 | 0.0 | 0.0 | 0.1 | −0.2 | −0.1 | −0.1 | 0.6 | 0.6 | 1.0 | −0.1 | 0.2 | −0.4 | −0.3 | −0.2 | −0.4 | −0.4 | 0.2 |
| Go/No Go hit | 0.0 | 0.0 | −0.1 | −0.2 | 0.2 | 0.1 | 0.3 | 0.2 | 0.2 | 0.2 | 0.1 | 0.2 | 0.1 | −0.4 | −0.3 | −0.1 | 1.0 | 0.0 | 0.2 | 0.2 | 0.1 | 0.0 | 0.4 | −0.4 |
| Go/No Go mean RTs | −0.1 | −0.1 | −0.1 | −0.1 | 0.2 | 0.2 | 0.1 | 0.0 | 0.1 | −0.1 | 0.4 | 0.1 | −0.2 | 0.2 | 0.2 | 0.2 | 0.0 | 1.0 | 0.0 | −0.1 | −0.3 | −0.2 | 0.0 | 0.1 |
| RCPM | −0.2 | −0.1 | −0.2 | 0.0 | −0.2 | −0.2 | 0.0 | 0.0 | 0.0 | 0.0 | −0.2 | −0.1 | 0.2 | −0.3 | −0.5 | −0.4 | 0.2 | 0.0 | 1.0 | 0.3 | 0.2 | 0.5 | 0.4 | −0.2 |
| ROCF copy | 0.0 | 0.0 | 0.1 | −0.2 | −0.1 | −0.2 | 0.1 | 0.1 | 0.1 | 0.0 | 0.0 | 0.0 | 0.1 | −0.1 | −0.2 | −0.3 | 0.2 | −0.1 | 0.3 | 1.0 | 0.7 | 0.2 | 0.3 | −0.2 |
| ROCF recall | 0.2 | 0.2 | 0.2 | 0.1 | −0.1 | −0.1 | 0.0 | 0.1 | 0.1 | 0.2 | −0.1 | −0.1 | 0.1 | −0.1 | −0.2 | −0.2 | 0.1 | −0.3 | 0.2 | 0.7 | 1.0 | 0.2 | 0.3 | −0.4 |
| Tower of London | −0.2 | −0.2 | −0.2 | 0.0 | −0.4 | −0.4 | −0.1 | −0.1 | 0.0 | −0.2 | −0.1 | −0.1 | 0.3 | 0.0 | −0.2 | −0.4 | 0.0 | −0.2 | 0.5 | 0.2 | 0.2 | 1.0 | 0.1 | 0.0 |
| DIR hit | 0.0 | 0.0 | 0.0 | 0.1 | 0.2 | 0.0 | 0.2 | 0.4 | 0.3 | 0.3 | 0.3 | 0.1 | 0.1 | −0.4 | −0.4 | −0.4 | 0.4 | 0.0 | 0.4 | 0.3 | 0.3 | 0.1 | 1.0 | −0.2 |
| DIR mean RTs | −0.1 | −0.1 | 0.0 | −0.1 | −0.1 | −0.3 | −0.2 | −0.4 | −0.3 | −0.4 | 0.0 | −0.1 | 0.2 | 0.3 | 0.3 | 0.2 | −0.4 | 0.1 | −0.2 | −0.2 | −0.4 | 0.0 | −0.2 | 1.0 |
| Original p Value | Critical Value | Benjamini-Hochberg Adjusted p Value | |
|---|---|---|---|
| CY-BOCS tot, DY-BOCS Symmetry/Order | 0.0001 | 0.0007 | 0.0069 |
| CY-BOCS obsessive, DY-BOCS Symmetry/Order | 0.0002 | 0.0038 | 0.0026 |
| CY-BOCS compulsive, DY-BOCS Symmetry/Order | 0.0001 | 0.0016 | 0.0031 |
| CY-BOCS obsessive, CAPS tot | 0.0006 | 0.0042 | 0.0072 |
| CY-BOCS obsessive, SOP | 0.0023 | 0.0054 | 0.0212 |
| CY-BOCS obsessive, SPP | 0.0032 | 0.0056 | 0.0285 |
| CY-BOCS obsessive, IUSC | 0.0038 | 0.0062 | 0.0308 |
| CY-BOCS obsessive, CGAS | 0.0001 | 0.0009 | 0.0055 |
| CY-BOCS compulsive, CGAS | 0.0001 | 0.0024 | 0.0021 |
| DY-BOCS Violence/Disaster, SPP | 0.0002 | 0.0036 | 0.0028 |
| DY-BOCS Violence/Disaster, IUSC | 0.0037 | 0.0060 | 0.0309 |
| DY-BOCS Violence/Disaster, Tower of London | 0.0046 | 0.0067 | 0.0343 |
| DY-BOCS Symmetry/Order, CGAS | 0.001 | 0.0043 | 0.0115 |
| DY-BOCS Symmetry/Order, Tower of London | 0.0065 | 0.0074 | 0.0438 |
| OCD Symptoms | Dysfunctional Beliefs | Cognitive Traits |
|---|---|---|
| Higher obsessions severity |
| |
| Greater severity of obsessions and compulsions about harm due to aggression/injury/violence/natural disasters |
| Decreased accuracy in a problem-solving, non-verbal reasoning task |
| Greater severity of obsessions about symmetry, and compulsions to count or order/arrange |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piras, F.; Banaj, N.; Ciullo, V.; Piras, F.; Ducci, G.; Demaria, F.; Vicari, S.; Spalletta, G. Dysfunctional Beliefs and Cognitive Performance across Symptom Dimensions in Childhood and Adolescent OCD. J. Clin. Med. 2023, 12, 219. https://doi.org/10.3390/jcm12010219
Piras F, Banaj N, Ciullo V, Piras F, Ducci G, Demaria F, Vicari S, Spalletta G. Dysfunctional Beliefs and Cognitive Performance across Symptom Dimensions in Childhood and Adolescent OCD. Journal of Clinical Medicine. 2023; 12(1):219. https://doi.org/10.3390/jcm12010219
Chicago/Turabian StylePiras, Federica, Nerisa Banaj, Valentina Ciullo, Fabrizio Piras, Giuseppe Ducci, Francesco Demaria, Stefano Vicari, and Gianfranco Spalletta. 2023. "Dysfunctional Beliefs and Cognitive Performance across Symptom Dimensions in Childhood and Adolescent OCD" Journal of Clinical Medicine 12, no. 1: 219. https://doi.org/10.3390/jcm12010219