
Redefining Unilateral Pulmonary Edema after Mitral Valve Surgery on Chest X-ray Imaging Using the RALE Scoring System
 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
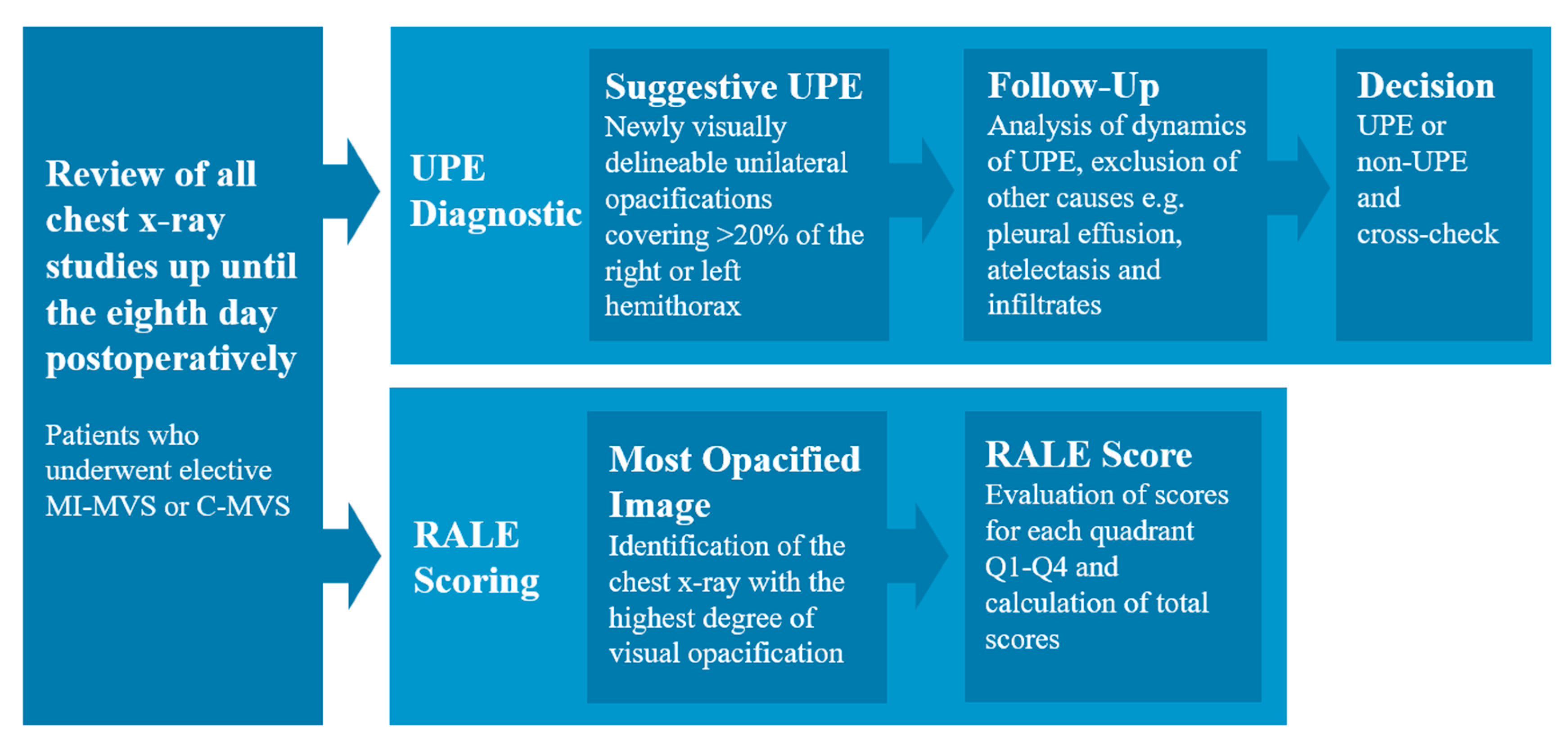
2.2. Chest X-ray Analysis and Diagnosis of UPE
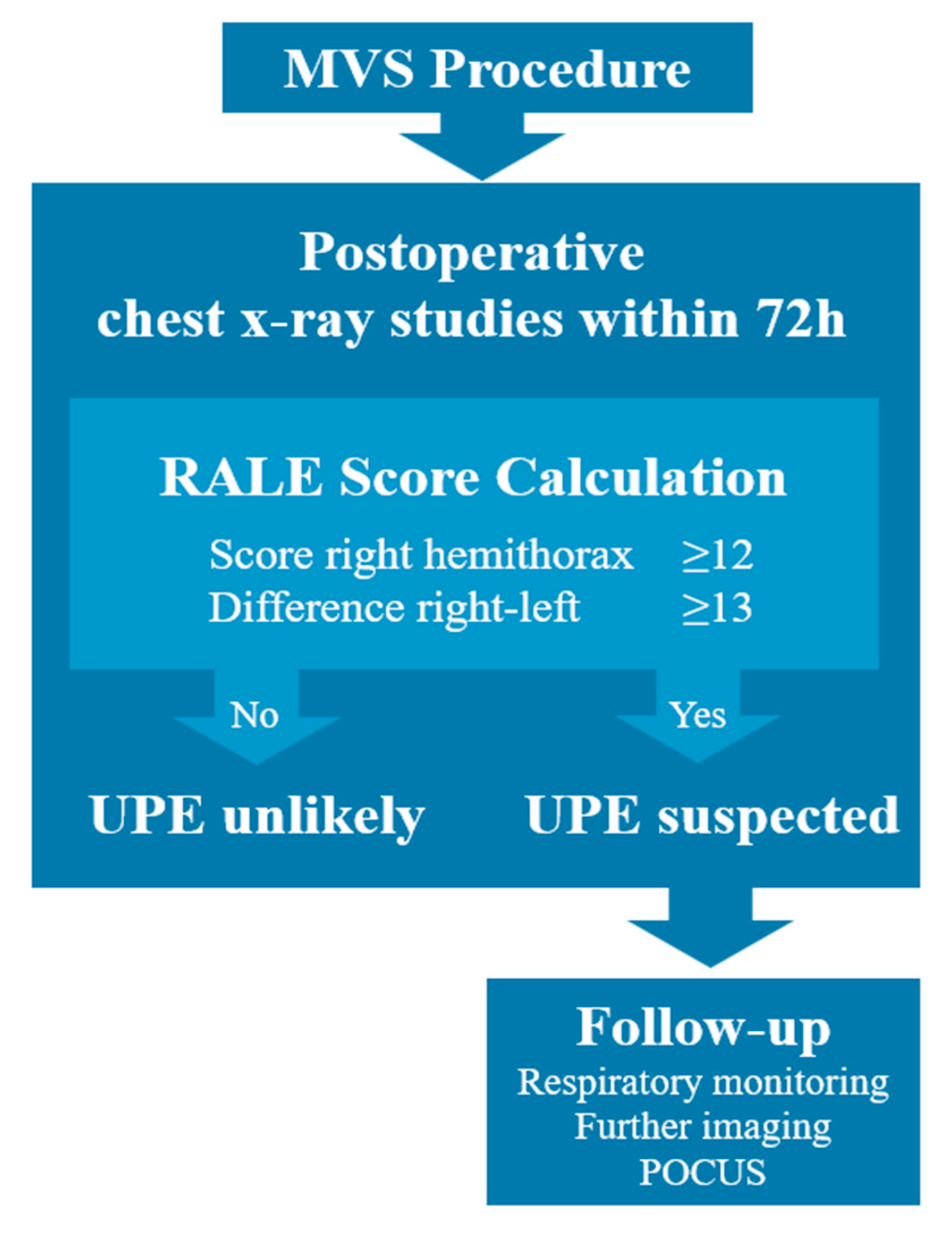
2.3. Rale Score Evaluation for Diagnosis of UPE
2.4. Statistical Analysis
3. Results
3.1. Study Population
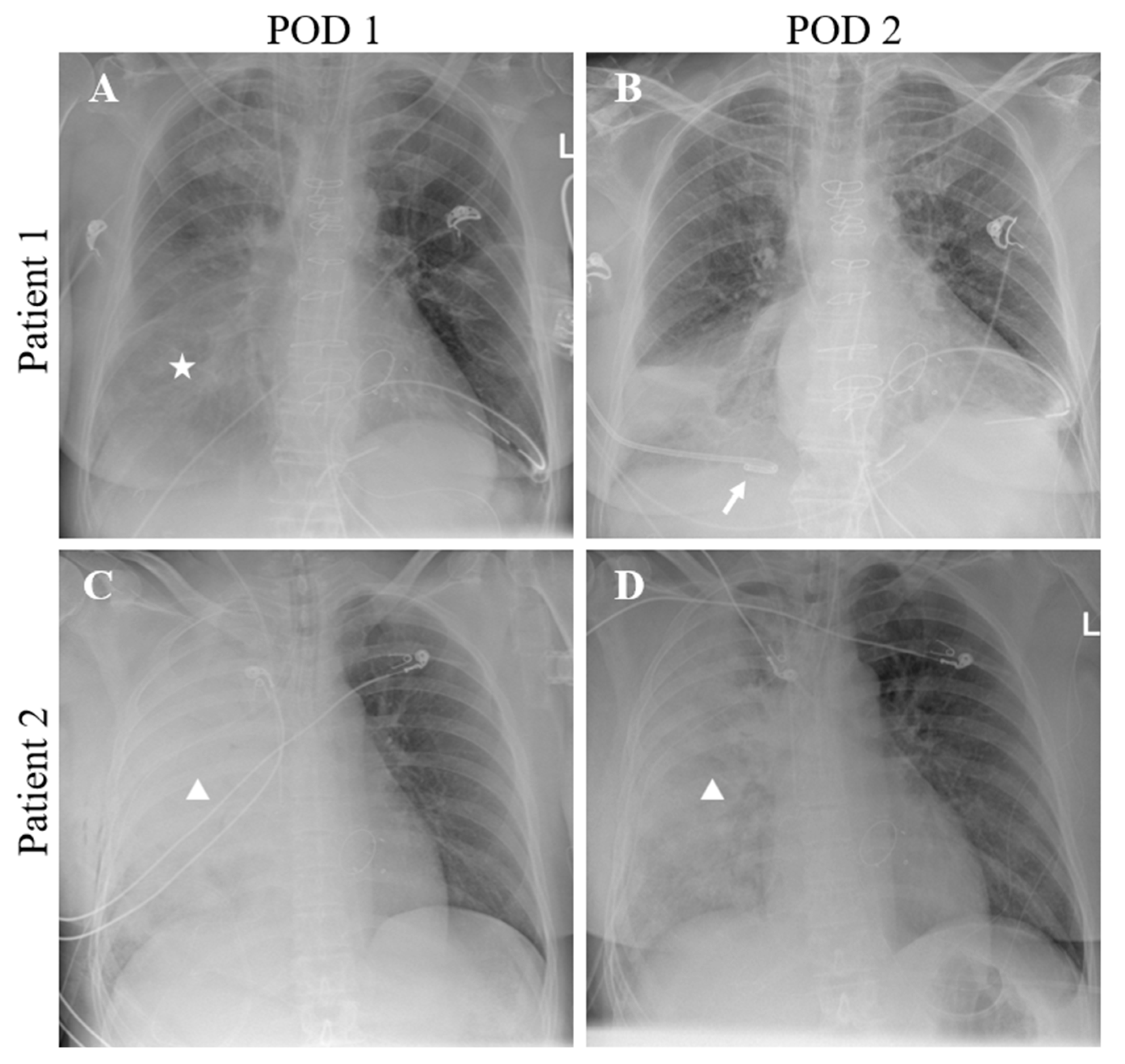
3.2. Chest X-ray Analysis and Diagnosis of UPE
3.3. RALE Scoring of Chest X-ray and ROC Analysis Results
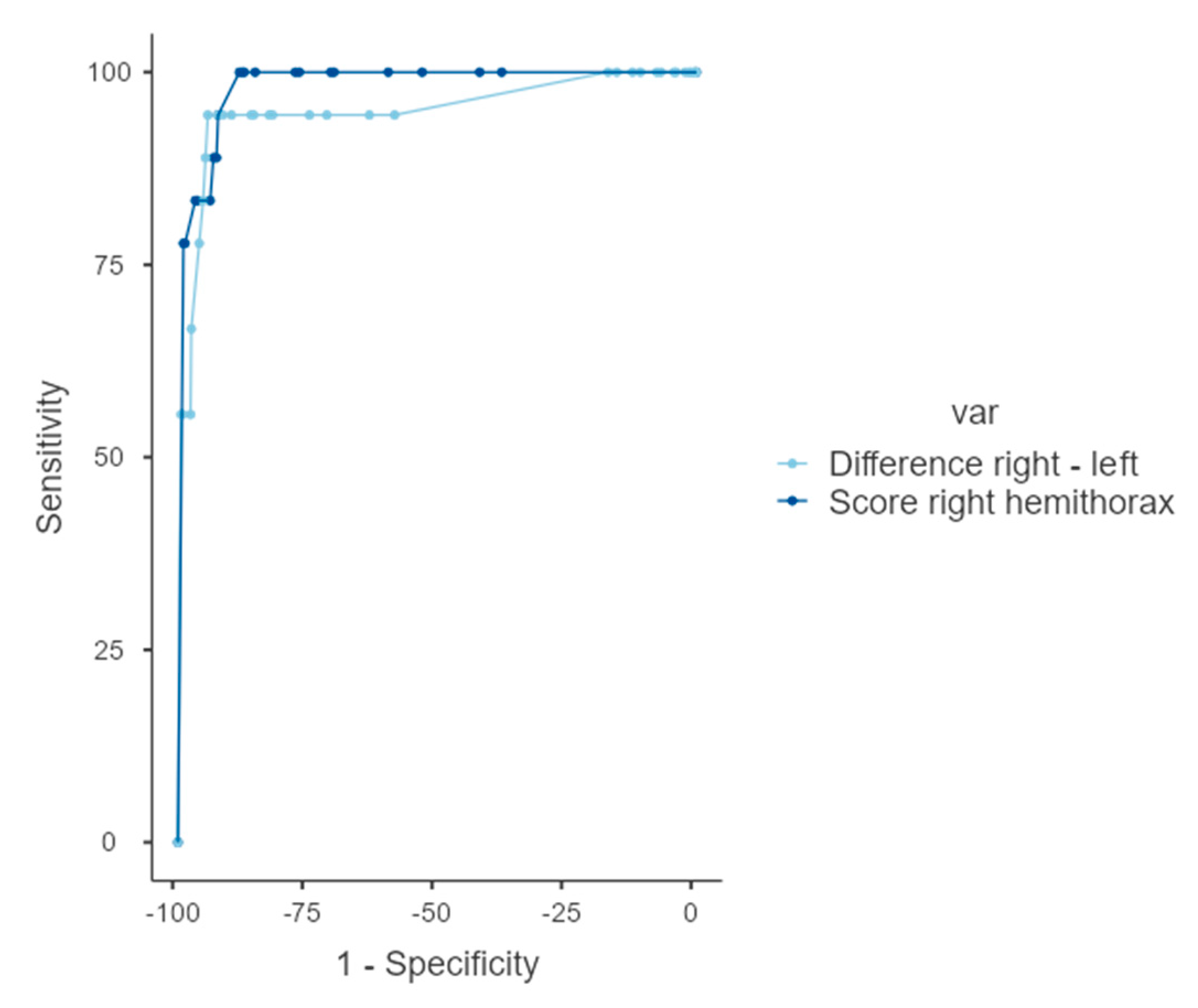
3.4. ROC Analysis
4. Discussion
4.1. Diagnosis and Incidence of UPE
4.2. RALE Scoring for UPE Assessment
4.3. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ARDS | Acute respiratory distress syndrome |
| AUC | Area under the curve |
| BMI | Body mass index |
| C-MVS | Conventional mitral valve surgery (median sternotomy) |
| ICU | Intensive care unit |
| MIS | Minimally invasive surgery |
| MVS | Mitral valve surgery |
| MI-MVS | Minimally invasive mitral valve surgery |
| POCUS | Point-of-care ultrasound |
| POD | Postoperative day |
| RALE | Radiographic assessment of lung edema |
| ROC | Receiver operating characteristic |
| UPE | Unilateral pulmonary edema |
References
- Sündermann, S.H.; Czerny, M.; Falk, V. Open vs. Minimally Invasive Mitral Valve Surgery: Surgical Technique, Indications and Results. Cardiovasc. Eng. Technol. 2015, 6, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Svensson, L.G.; Atik, F.A.; Cosgrove, D.M.; Blackstone, E.H.; Rajeswaran, J.; Krishnaswamy, G.; Jin, U.; Gillinov, A.M.; Griffin, B.; Navia, J.L.; et al. Minimally invasive versus conventional mitral valve surgery: A propensity-matched comparison. J. Thorac. Cardiovasc. Surg. 2010, 139, 926–932.e2. [Google Scholar] [CrossRef] [PubMed]
- Sündermann, S.H.; Sromicki, J.; Biefer, H.R.C.; Seifert, B.; Holubec, T.; Falk, V.; Jacobs, S. Mitral valve surgery: Right lateral minithoracotomy or sternotomy? A systematic review and meta-analysis. J. Thorac. Cardiovasc. Surg. 2014, 148, 1989–1995.e4. [Google Scholar] [CrossRef] [PubMed]
- López-Baamonde, M.; Eulufi, S.; Ascaso, M.; Arguis, M.; Navarro-Ripoll, R.; Rovira, I. Unilateral pulmonary edema associated factors after minimally invasive mitral valve surgery. Rev. Esp. Anestesiol. Reanim. 2022, 69, 134–142. [Google Scholar] [CrossRef]
- Kesävuori, R.I.; Vento, A.E.; Lundbom, N.M.; Iivonen, M.R.; Huuskonen, A.S.; Raivio, P.M. Unilateral pulmonary oedema after minimally invasive and robotically assisted mitral valve surgery. Eur. J. Cardio-Thorac. Surg. 2020, 57, 504–511. [Google Scholar] [CrossRef]
- Renner, J.; Lorenzen, U.; Borzikowsky, C.; Schoeneich, F.; Cremer, J.; Haneya, A.; Hensler, J.; Panholzer, B.; Huenges, K.; Broch, O. Unilateral pulmonary oedema after minimally invasive mitral valve surgery: A single-centre experience. Eur. J. Cardio-Thoracic Surg. 2017, 53, 764–770. [Google Scholar] [CrossRef] [PubMed]
- Tutschka, M.P.; Bainbridge, D.; Chu, M.W.; Kiaii, B.; Jones, P.M. Unilateral Postoperative Pulmonary Edema After Minimally Invasive Cardiac Surgical Procedures: A Case-Control Study. Ann. Thorac. Surg. 2015, 99, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Khalil, N.H.; Anders, R.; Forner, A.F.; Gutberlet, M.; Ender, J. Radiological Incidence of Unilateral Pulmonary Edema After Minimally Invasive Cardiac Surgery. J. Cardiothorac. Vasc. Anesthesia 2020, 34, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Inotani, S.; Kubokawa, S.-I.; Nakaoka, Y.; Kotani, T.; Matsuda, H.; Yamamoto, S.; Seki, S.-I.; Kawai, K.; Hamashige, N.; Doi, Y. Unilateral cardiogenic pulmonary edema. J. Cardiol. Cases 2017, 17, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Handagala, R.; Ralapanawa, U.; Jayalath, T. Unilateral pulmonary edema: A case report and review of the literature. J. Med. Case Rep. 2018, 12, 219. [Google Scholar] [CrossRef] [PubMed]
- Warren, M.A.; Zhao, Z.; Koyama, T.; Bastarache, J.A.; Shaver, C.M.; Semler, M.W.; Rice, T.W.; Matthay, M.A.; Calfee, C.S.; Ware, L.B. Severity scoring of lung oedema on the chest radiograph is associated with clinical outcomes in ARDS. Thorax 2018, 73, 840–846. [Google Scholar] [CrossRef] [PubMed]
- Şahin, M.D.; Aybek, E.C. Jamovi: An Easy to Use Statistical Software for the Social Scientists. Int. J. Assess. Tools Educ. 2020, 6, 670–692. [Google Scholar] [CrossRef]
- Moss, E.; Halkos, M.E.; Binongo, J.N.; Murphy, D.A. Prevention of Unilateral Pulmonary Edema Complicating Robotic Mitral Valve Operations. Ann. Thorac. Surg. 2016, 103, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Irisawa, Y.; Hiraoka, A.; Totsugawa, T.; Chikazawa, G.; Nakajima, K.; Tamura, K.; Yoshitaka, H.; Sakaguchi, T. Re-expansion pulmonary oedema after minimally invasive cardiac surgery with right mini-thoracotomy. Eur. J. Cardio-Thoracic Surg. 2015, 49, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Keyl, C.; Staier, K.; Pingpoh, C.; Pache, G.; Thoma, M.; Günkel, L.; Henschke, S.; Beyersdorf, F. Unilateral pulmonary oedema after minimally invasive cardiac surgery via right anterolateral minithoracotomy. Eur. J. Cardio-Thoracic Surg. 2014, 47, 1097–1102. [Google Scholar] [CrossRef] [PubMed]
- Puehler, T.; Friedrich, C.; Lutter, G.; Kornhuber, M.; Salem, M.; Schoettler, J.; Ernst, M.; Saad, M.; Seoudy, H.; Frank, D.; et al. Outcome of Unilateral Pulmonary Edema after Minimal-Invasive Mitral Valve Surgery: 10-Year Follow-Up. J. Clin. Med. 2021, 10, 2411. [Google Scholar] [CrossRef] [PubMed]
- Valk, C.M.; Zimatore, C.; Mazzinari, G.; Pierrakos, C.; Sivakorn, C.; Dechsanga, J.; Grasso, S.; Beenen, L.; Bos, L.D.J.; Paulus, F.; et al. The RALE Score Versus the CT Severity Score in Invasively Ventilated COVID-19 Patients—A Retrospective Study Comparing Their Prognostic Capacities. Diagnostics 2022, 12, 2072. [Google Scholar] [CrossRef] [PubMed]
- Zimatore, C.; Pisani, L.; Lippolis, V.; Warren, M.A.; Calfee, C.S.; Ware, L.B.; Algera, A.G.; Smit, M.R.; Grasso, S.; Schultz, M.J. Accuracy of the Radiographic Assessment of Lung Edema Score for the Diagnosis of ARDS. Front. Physiol. 2021, 12, 672823. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall MVS (n = 676) | MI-MVS (n = 434) | C-MVS (n = 242) | p-Value | |
|---|---|---|---|---|
| Demographic data | ||||
| Female gender, n (%) | 275 (40.7) | 175 (40.3) | 100 (41.3) | 0.800 |
| Age (years) | 65 [56, 74] | 64 [54, 73] | 68.5 [59, 75] | <0.001 |
| Weight (kg) | 77 [67, 89.3] | 75.5 [66, 89] | 78 [67, 89.8] | 0.308 |
| Height (cm) | 174 [167, 181] | 174 [167, 182] | 172 [166, 180] | 0.328 |
| Duration of procedure (minutes) | 280 [243, 320] | 287 [257, 322] | 261 [214, 313] | <0.001 |
| Overall MVS (n = 676) | MI-MVS (n = 434) | C-MVS (n = 242) | p-Value | |
|---|---|---|---|---|
| UPE, n (%) | 18 (2.6) | 15 (3.5) | 3 (1.2) | 0.043 |
| Non-UPE (n = 658) | UPE (n = 18) | p-Value | |
|---|---|---|---|
| Scores | |||
| Q1 | 0 [0, 0] | 12 [12, 12] | <0.001 |
| Q2 | 2 [0, 4] | 12 [12, 12] | <0.001 |
| Q3 | 0 [0, 0] | 0 [0, 0] | 0.543 |
| Q4 | 0 [0, 3] | 0 [0, 3.5] | 0.937 |
| Right hemithorax (Q1 + Q2) | 2 [0, 6] | 24 [24, 24] | 0.001 |
| Left hemithorax (Q3 + Q4) | 0 [0, 4] | 0 [0, 5] | 0.952 |
| RALE score total | 4 [0, 10] | 24 [24, 24] | <0.001 |
| Difference (Q1 + Q2) to (Q3 + Q4) | 0 [0, 4] | 24 [16, 24] | <0.001 |
| Threshold Value | Sensitivity (%) | Specificity (%) | Youden’s Index | AUC | |
|---|---|---|---|---|---|
| Scores | |||||
| Right hemithorax (Q1 + Q2) | 12 | 100 | 88.2 | 0.88 | 0.980 |
| Difference (Q1 + Q2) to (Q3 + Q4) | 13 | 94.44 | 94.22 | 0.887 | 0.949 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mostafa, K.; Wolf, C.; Seehafer, S.; Horr, A.; Pommert, N.; Haneya, A.; Lutter, G.; Pühler, T.; Both, M.; Jansen, O.; et al. Redefining Unilateral Pulmonary Edema after Mitral Valve Surgery on Chest X-ray Imaging Using the RALE Scoring System. J. Clin. Med. 2023, 12, 6043. https://doi.org/10.3390/jcm12186043
Mostafa K, Wolf C, Seehafer S, Horr A, Pommert N, Haneya A, Lutter G, Pühler T, Both M, Jansen O, et al. Redefining Unilateral Pulmonary Edema after Mitral Valve Surgery on Chest X-ray Imaging Using the RALE Scoring System. Journal of Clinical Medicine. 2023; 12(18):6043. https://doi.org/10.3390/jcm12186043
Chicago/Turabian StyleMostafa, Karim, Carmen Wolf, Svea Seehafer, Agreen Horr, Nina Pommert, Assad Haneya, Georg Lutter, Thomas Pühler, Marcus Both, Olav Jansen, and et al. 2023. "Redefining Unilateral Pulmonary Edema after Mitral Valve Surgery on Chest X-ray Imaging Using the RALE Scoring System" Journal of Clinical Medicine 12, no. 18: 6043. https://doi.org/10.3390/jcm12186043