
Lung Involvement in Inflammatory Bowel Diseases: Shared Pathways and Unwanted Connections

 ,
,
Abstract
:1. Introduction
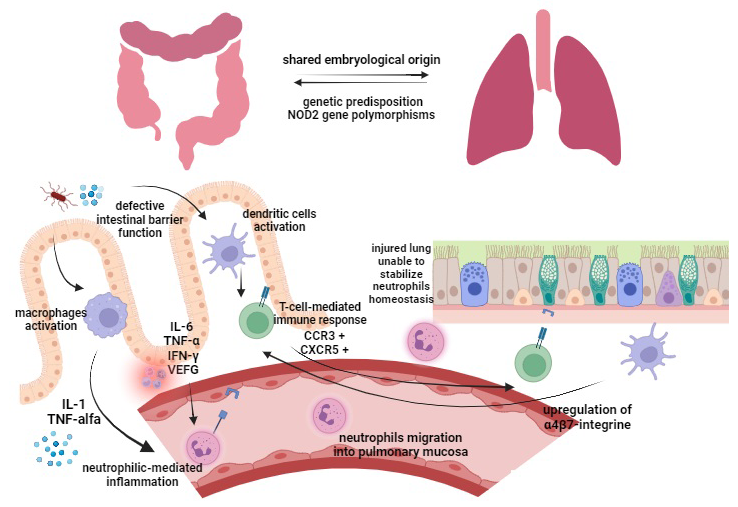
2. Pathogenesis
3. Respiratory Tract Involvement Specifically Related to IBD
3.1. IBD-Associated Airway Diseases
3.2. IBD-Associated Interstitial Lung Diseases
3.3. IBD-Associated Pulmonary Embolism
3.4. IBD-Associated Vasculitis
3.5. Subclinical Pulmonary Dysfunction in IBD
3.6. IBD-Associated Lung Cancer
3.7. Respiratory Infections in IBD Patients
4. Drug-Induced Pulmonary Manifestations
4.1. Salicylates (Sulfasalazine, Mesalazine)
4.2. Azathioprine and 6-Mercaptopurine
4.3. Methotrexate
4.4. Biological Therapy
4.4.1. Anti-TNF Agents
4.4.2. Ustekinumab
4.4.3. Vedolizumab
4.5. Small Molecules
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Roda, G.; Chien Ng, S.; Kotze, P.G.; Argollo, M.; Panaccione, R.; Spinelli, A.; Kaser, A.; Peyrin-Biroulet, L.; Danese, S. Crohn’s Disease. Nat. Rev. Dis. Primers 2020, 6, 22. [Google Scholar] [CrossRef]
- Kobayashi, T.; Siegmund, B.; Le Berre, C.; Wei, S.C.; Ferrante, M.; Shen, B.; Bernstein, C.N.; Danese, S.; Peyrin-Biroulet, L.; Hibi, T. Ulcerative Colitis. Nat. Rev. Dis. Primers 2020, 6, 74. [Google Scholar] [CrossRef]
- Ananthakrishnan, A.N.; Bernstein, C.N.; Iliopoulos, D.; Macpherson, A.; Neurath, M.F.; Ali, R.A.R.; Vavricka, S.R.; Fiocchi, C. Environmental Triggers in IBD: A Review of Progress and Evidence. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Guan, Q. A Comprehensive Review and Update on the Pathogenesis of Inflammatory Bowel Disease. J. Immunol. Res. 2019, 2019, 7247238. [Google Scholar] [CrossRef] [PubMed]
- Harbord, M.; Annese, V.; Vavricka, S.R.; Allez, M.; Barreiro-de Acosta, M.; Boberg, K.M.; Burisch, J.; De Vos, M.; De Vries, A.-M.; Dick, A.D.; et al. The First European Evidence-Based Consensus on Extra-Intestinal Manifestations in Inflammatory Bowel Disease. J. Crohn’s Colitis 2016, 10, 239–254. [Google Scholar] [CrossRef]
- Gordon, H.; Burisch, J.; Ellul, P.; Karmiris, K.; Katsanos, K.; Allocca, M.; Bamias, G.; Barreiro-de Acosta, M.; Braithwaite, T.; Greuter, T.; et al. ECCO Guidelines on Extraintestinal Manifestations in Inflammatory Bowel Disease. J. Crohn’s Colitis 2023. [Google Scholar] [CrossRef]
- Storch, I.; Sachar, D.; Katz, S. Pulmonary Manifestations of Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2003, 9, 104–115. [Google Scholar] [CrossRef]
- Vavricka, S.R.; Schoepfer, A.; Scharl, M.; Lakatos, P.L.; Navarini, A.; Rogler, G. Extraintestinal Manifestations of Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2015, 21, 1982–1992. [Google Scholar] [CrossRef]
- Pemmasani, G.; Loftus, E.V.; Tremaine, W.J. Prevalence of Pulmonary Diseases in Association with Inflammatory Bowel Disease. Dig. Dis. Sci. 2022, 67, 5187–5194. [Google Scholar] [CrossRef]
- Keely, S.; Talley, N.J.; Hansbro, P.M. Pulmonary-Intestinal Cross-Talk in Mucosal Inflammatory Disease. Mucosal Immunol. 2012, 5, 7–18. [Google Scholar] [CrossRef]
- Schmid, F.; Chao, C.-M.; Däbritz, J. Pathophysiological Concepts and Management of Pulmonary Manifestation of Pediatric Inflammatory Bowel Disease. Int. J. Mol. Sci. 2022, 23, 7287. [Google Scholar] [CrossRef] [PubMed]
- Soderholm, J.D. Augmented Increase in Tight Junction Permeability by Luminal Stimuli in the Non-Inflamed Ileum of Crohn’s Disease. Gut 2002, 50, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Johansson, M.E.V.; Gustafsson, J.K.; Holmén-Larsson, J.; Jabbar, K.S.; Xia, L.; Xu, H.; Ghishan, F.K.; Carvalho, F.A.; Gewirtz, A.T.; Sjövall, H.; et al. Bacteria Penetrate the Normally Impenetrable Inner Colon Mucus Layer in Both Murine Colitis Models and Patients with Ulcerative Colitis. Gut 2014, 63, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Bernardo, D.; Chaparro, M.; Gisbert, J.P. Human Intestinal Dendritic Cells in Inflammatory Bowel Diseases. Mol. Nutr. Food Res. 2018, 62, 1700931. [Google Scholar] [CrossRef] [PubMed]
- Charo, I.F.; Ransohoff, R.M. The Many Roles of Chemokines and Chemokine Receptors in Inflammation. N. Engl. J. Med. 2006, 354, 610–621. [Google Scholar] [CrossRef] [PubMed]
- Funderburg, N.T.; Stubblefield Park, S.R.; Sung, H.C.; Hardy, G.; Clagett, B.; Ignatz-Hoover, J.; Harding, C.V.; Fu, P.; Katz, J.A.; Lederman, M.M.; et al. Circulating CD4+ and CD8+ T Cells Are Activated in Inflammatory Bowel Disease and Are Associated with Plasma Markers of Inflammation. Immunology 2013, 140, 87–97. [Google Scholar] [CrossRef]
- Scaldaferri, F.; Vetrano, S.; Sans, M.; Arena, V.; Straface, G.; Stigliano, E.; Repici, A.; Sturm, A.; Malesci, A.; Panes, J.; et al. VEGF-A Links Angiogenesis and Inflammation in Inflammatory Bowel Disease Pathogenesis. Gastroenterology 2009, 136, 585–595.e5. [Google Scholar] [CrossRef]
- Raddatz, D.; Bockemühl, M.; Ramadori, G. Quantitative Measurement of Cytokine MRNA in Inflammatory Bowel Disease: Relation to Clinical and Endoscopic Activity and Outcome. Eur. J. Gastroenterol. Hepatol. 2005, 17, 547–557. [Google Scholar] [CrossRef]
- Mateer, S.W.; Maltby, S.; Marks, E.; Foster, P.S.; Horvat, J.C.; Hansbro, P.M.; Keely, S. Potential Mechanisms Regulating Pulmonary Pathology in Inflammatory Bowel Disease. J. Leukoc. Biol. 2015, 98, 727–737. [Google Scholar] [CrossRef]
- Le Cras, T.D.; Spitzmiller, R.E.; Albertine, K.H.; Greenberg, J.M.; Whitsett, J.A.; Akeson, A.L. VEGF Causes Pulmonary Hemorrhage, Hemosiderosis, and Air Space Enlargement in Neonatal Mice. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2004, 287, L134–L142. [Google Scholar] [CrossRef]
- Haslett, C.; Worthen, G.S.; Giclas, P.C.; Morrison, D.C.; Henson, J.E.; Henson, P.M. The Pulmonary Vascular Sequestration of Neutrophils in Endotoxemia Is Initiated by an Effect of Endotoxin on Neutrophil in the Rabbit. Am. Rev. Respir. Dis. 1987, 136, 9–18. [Google Scholar] [CrossRef]
- Nahum, A.; Chamberlin, W.; Sznajder, J.I. Differential Activation of Mixed Venous and Arterial Neutrophils in Patients with Sepsis Syndrome and Acute Lung Injury. Am. Rev. Respir. Dis. 1991, 143, 1083–1087. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.-H.; ten Hove, T.; The, F.O.; Slors, J.F.M.; van Deventer, S.J.H.; te Velde, A.A. Chemokine Receptor CXCR3 Expression in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2001, 7, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Agace, W.W.; Roberts, A.I.; Wu, L.; Greineder, C.; Ebert, E.C.; Parker, C.M. Human Intestinal Lamina Propria and Intraepithelial Lymphocytes Express Receptors Specific for Chemokines Induced by Inflammation. Eur. J. Immunol. 2000, 30, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Ruane, D.; Brane, L.; Reis, B.S.; Cheong, C.; Poles, J.; Do, Y.; Zhu, H.; Velinzon, K.; Choi, J.-H.; Studt, N.; et al. Lung Dendritic Cells Induce Migration of Protective T Cells to the Gastrointestinal Tract. J. Exp. Med. 2013, 210, 1871–1888. [Google Scholar] [CrossRef] [PubMed]
- Koelink, P.J.; Overbeek, S.A.; Braber, S.; Morgan, M.E.; Henricks, P.A.J.; Roda, M.A.; Verspaget, H.W.; Wolfkamp, S.C.; te Velde, A.A.; Jones, C.W.; et al. Collagen Degradation and Neutrophilic Infiltration: A Vicious Circle in Inflammatory Bowel Disease. Gut 2014, 63, 578–587. [Google Scholar] [CrossRef]
- Vutcovici, M.; Brassard, P.; Bitton, A. Inflammatory Bowel Disease and Airway Diseases. World J. Gastroenterol. 2016, 22, 7735. [Google Scholar] [CrossRef]
- Adler, J.; Rangwalla, S.C.; Dwamena, B.A.; Higgins, P.D. The Prognostic Power of the NOD2 Genotype for Complicated Crohn’s Disease: A Meta-Analysis. Am. J. Gastroenterol. 2011, 106, 699–712. [Google Scholar] [CrossRef]
- Kinose, D.; Ogawa, E.; Hirota, T.; Ito, I.; Kudo, M.; Haruna, A.; Marumo, S.; Hoshino, Y.; Muro, S.; Hirai, T.; et al. A NOD2 Gene Polymorphism Is Associated with the Prevalence and Severity of Chronic Obstructive Pulmonary Disease in a Japanese Population. Respirology 2012, 17, 164–171. [Google Scholar] [CrossRef]
- Salem, M.; Seidelin, J.B.; Rogler, G.; Nielsen, O.H. Muramyl Dipeptide Responsive Pathways in Crohn’s Disease: From NOD2 and Beyond. Cell. Mol. Life Sci. 2013, 70, 3391–3404. [Google Scholar] [CrossRef]
- Fritz, T.; Niederreiter, L.; Adolph, T.; Blumberg, R.S.; Kaser, A. Crohn’s Disease: NOD2, Autophagy and ER Stress Converge. Gut 2011, 60, 1580–1588. [Google Scholar] [CrossRef] [PubMed]
- Wehkamp, J. NOD2 (CARD15) Mutations in Crohn’s Disease Are Associated with Diminished Mucosal -Defensin Expression. Gut 2004, 53, 1658–1664. [Google Scholar] [CrossRef] [PubMed]
- Lees, C.W.; Barrett, J.C.; Parkes, M.; Satsangi, J. New IBD Genetics: Common Pathways with Other Diseases. Gut 2011, 60, 1739–1753. [Google Scholar] [CrossRef] [PubMed]
- Camus, P.; Piard, F.; Ashcroft, T.; Gal, A.A.; Colby, T.V. The Lung in Inflammatory Bowel Disease. Medicine 1993, 72, 151–183. [Google Scholar] [CrossRef] [PubMed]
- Betancourt, S.L.; Palacio, D.; Jimenez, C.A.; Martinez, S.; Marom, E.M. Thoracic Manifestations of Inflammatory Bowel Disease. Am. J. Roentgenol. 2011, 197, W452–W456. [Google Scholar] [CrossRef] [PubMed]
- Higenbottam, T.; Cochrane, G.M.; Clark, T.J.; Turner, D.; Millis, R.; Seymour, W. Bronchial Disease in Ulcerative Colitis. Thorax 1980, 35, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Papanikolaou, I. Patterns of Airway Involvement in Inflammatory Bowel Diseases. World J. Gastrointest. Pathophysiol. 2014, 5, 560. [Google Scholar] [CrossRef]
- Cozzi, D.; Moroni, C.; Addeo, G.; Danti, G.; Lanzetta, M.M.; Cavigli, E.; Falchini, M.; Marra, F.; Piccolo, C.L.; Brunese, L.; et al. Radiological Patterns of Lung Involvement in Inflammatory Bowel Disease. Gastroenterol. Res. Pract. 2018, 2018, 5697846. [Google Scholar] [CrossRef]
- Lu, D.-G. Tracheobronchial Nodules and Pulmonary Infiltrates in a Patient with Crohn’s Disease. World J. Gastroenterol. 2012, 18, 5653. [Google Scholar] [CrossRef]
- Plataki, M.; Tzortzaki, E.; Lambiri, I.; Giannikaki, E.; Ernst, A.; Siafakas, N.M. Severe Airway Stenosis Associated with Crohn’s Disease: Case Report. BMC Pulm. Med. 2006, 6, 7. [Google Scholar] [CrossRef]
- Aliberti, S.; Goeminne, P.C.; O’Donnell, A.E.; Aksamit, T.R.; Al-Jahdali, H.; Barker, A.F.; Blasi, F.; Boersma, W.G.; Crichton, M.L.; De Soyza, A.; et al. Criteria and Definitions for the Radiological and Clinical Diagnosis of Bronchiectasis in Adults for Use in Clinical Trials: International Consensus Recommendations. Lancet Respir. Med. 2022, 10, 298–306. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Polverino, E.; Crichton, M.L.; Ringshausen, F.C.; De Soyza, A.; Vendrell, M.; Burgel, P.R.; Haworth, C.S.; Loebinger, M.R.; Dimakou, K.; et al. Bronchiectasis in Europe: Data on Disease Characteristics from the European Bronchiectasis Registry (EMBARC). Lancet Respir. Med. 2023, 11, 637–649. [Google Scholar] [CrossRef] [PubMed]
- Flume, P.A.; Chalmers, J.D.; Olivier, K.N. Advances in Bronchiectasis: Endotyping, Genetics, Microbiome, and Disease Heterogeneity. Lancet 2018, 392, 880–890. [Google Scholar] [CrossRef] [PubMed]
- Shoemark, A.; Shteinberg, M.; De Soyza, A.; Haworth, C.S.; Richardson, H.; Gao, Y.; Perea, L.; Dicker, A.J.; Goeminne, P.C.; Cant, E.; et al. Characterization of Eosinophilic Bronchiectasis: A European Multicohort Study. Am. J. Respir. Crit. Care Med. 2022, 205, 894–902. [Google Scholar] [CrossRef]
- Gramegna, A.; Aliberti, S.; Sibila, O.; Di Francesco, C.; Sotgiu, G.; Perea, L.; Terranova, L.; Oriano, M.; Pilocane, T.; Saderi, L.; et al. Sputum Neutrophil Elastase in Bronchiectasis: A Southern European Cohort Study. Eur. Respir. J. 2020, 56, 2001702. [Google Scholar] [CrossRef] [PubMed]
- Oriano, M.; Gramegna, A.; Amati, F.; D’Adda, A.; Gaffuri, M.; Contoli, M.; Bindo, F.; Simonetta, E.; Di Francesco, C.; Santambrogio, M.; et al. T2-High Endotype and Response to Biological Treatments in Patients with Bronchiectasis. Biomedicines 2021, 9, 772. [Google Scholar] [CrossRef]
- Keir, H.R.; Shoemark, A.; Dicker, A.J.; Perea, L.; Pollock, J.; Giam, Y.H.; Suarez-Cuartin, G.; Crichton, M.L.; Lonergan, M.; Oriano, M.; et al. Neutrophil Extracellular Traps, Disease Severity, and Antibiotic Response in Bronchiectasis: An International, Observational, Multicohort Study. Lancet Respir. Med. 2021, 9, 873–884. [Google Scholar] [CrossRef] [PubMed]
- Shoemark, A.; Cant, E.; Carreto, L.; Smith, A.; Oriano, M.; Keir, H.R.; Perea, L.; Canto, E.; Terranova, L.; Vidal, S.; et al. A Point-of-Care Neutrophil Elastase Activity Assay Identifies Bronchiectasis Severity, Airway Infection and Risk of Exacerbation. Eur. Respir. J. 2019, 53, 1900303. [Google Scholar] [CrossRef]
- Kelly, M.G.; Frizelle, F.A.; Thornley, P.T.; Beckert, L.; Epton, M.; Lynch, A.C. Inflammatory Bowel Disease and the Lung: Is There a Link between Surgery and Bronchiectasis? Int. J. Color. Dis. 2006, 21, 754–757. [Google Scholar] [CrossRef]
- Kuenzig, M.E.; Bishay, K.; Leigh, R.; Kaplan, G.G.; Benchimol, E.I. Co-Occurrence of Asthma and the Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis. Clin. Transl. Gastroenterol. 2018, 9, e188. [Google Scholar] [CrossRef]
- Frolkis, A.; Dieleman, L.A.; Barkema, H.W.; Panaccione, R.; Ghosh, S.; Fedorak, R.N.; Madsen, K.; Kaplan, G.G.; Alberta IBD Consortium. Environment and the Inflammatory Bowel Diseases. Can. J. Gastroenterol. 2013, 27, e18–e24. [Google Scholar] [CrossRef] [PubMed]
- Aujnarain, A.; Mack, D.R.; Benchimol, E.I. The Role of the Environment in the Development of Pediatric Inflammatory Bowel Disease. Curr. Gastroenterol. Rep. 2013, 15, 326. [Google Scholar] [CrossRef] [PubMed]
- Dogaru, C.M.; Nyffenegger, D.; Pescatore, A.M.; Spycher, B.D.; Kuehni, C.E. Breastfeeding and Childhood Asthma: Systematic Review and Meta-Analysis. Am. J. Epidemiol. 2014, 179, 1153–1167. [Google Scholar] [CrossRef] [PubMed]
- Daley, D. The Evolution of the Hygiene Hypothesis: The Role of Early-Life Exposures to Viruses and Microbes and Their Relationship to Asthma and Allergic Diseases. Curr. Opin. Allergy Clin. Immunol. 2014, 14, 390–396. [Google Scholar] [CrossRef]
- Stiemsma, L.T.; Reynolds, L.A.; Turvey, S.E.; Finlay, B.B. The Hygiene Hypothesis: Current Perspectives and Future Therapies. Immunotargets Ther. 2015, 4, 143–157. [Google Scholar] [CrossRef]
- Persson, P.; Bernell, O.; Leijonmarck, C.; Farahmand, B.; Hellers, G.; Ahlbom, A. Survival and Cause-Specific Mortality in Inflammatory Bowel Disease: A Population-Based Cohort Study. Gastroenterology 1996, 110, 1339–1345. [Google Scholar] [CrossRef]
- Raftery, A.L.; Tsantikos, E.; Harris, N.L.; Hibbs, M.L. Links between Inflammatory Bowel Disease and Chronic Obstructive Pulmonary Disease. Front. Immunol. 2020, 11, 2144. [Google Scholar] [CrossRef]
- Basseri, B.; Enayati, P.; Marchevsky, A.; Papadakis, K.A. Pulmonary Manifestations of Inflammatory Bowel Disease: Case Presentations and Review. J. Crohn’s Colitis 2010, 4, 390–397. [Google Scholar] [CrossRef]
- Koutroumpakis, E.; Tsiolakidou, G.; Koutroubakis, I. Risk of Venous Thromboembolism in Patients with Inflammatory Bowel Disease. Semin. Thromb. Hemost. 2013, 39, 461–468. [Google Scholar] [CrossRef]
- Nguyen, G.C.; Sam, J. Rising Prevalence of Venous Thromboembolism and Its Impact on Mortality Among Hospitalized Inflammatory Bowel Disease Patients. Am. J. Gastroenterol. 2008, 103, 2272–2280. [Google Scholar] [CrossRef]
- Johannesdottir, S.A.; Horváth-Puhó, E.; Dekkers, O.M.; Cannegieter, S.C.; Jørgensen, J.O.L.; Ehrenstein, V.; Vandenbroucke, J.P.; Pedersen, L.; Sørensen, H.T. Use of Glucocorticoids and Risk of Venous Thromboembolism. JAMA Intern. Med. 2013, 173, 743. [Google Scholar] [CrossRef] [PubMed]
- Cheng, K.; Faye, A.S. Venous Thromboembolism in Inflammatory Bowel Disease. World J. Gastroenterol. 2020, 26, 1231–1241. [Google Scholar] [CrossRef]
- Higgins, P.D.R.; Skup, M.; Mulani, P.M.; Lin, J.; Chao, J. Increased Risk of Venous Thromboembolic Events with Corticosteroid vs Biologic Therapy for Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2015, 13, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Detrez, I.; Thomas, D.; Van Steen, K.; Ballet, V.; Peeters, M.; Hoylaerts, M.F.; Van Assche, G.; Vermeire, S.; Ferrante, M.; Gils, A. Successful Infliximab Treatment Is Associated with Reversal of Clotting Abnormalities in Inflammatory Bowel Disease Patients. J. Clin. Gastroenterol. 2020, 54, 819–825. [Google Scholar] [CrossRef] [PubMed]
- De Fonseka, A.M.; Tuskey, A.; Conaway, M.R.; Behm, B.W. Antitumor Necrosis Factor-α Therapy Is Associated with Reduced Risk of Thromboembolic Events in Hospitalized Patients with Inflammatory Bowel Disease. J. Clin. Gastroenterol. 2016, 50, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Sy, A.; Khalidi, N.; Dehghan, N.; Barra, L.; Carette, S.; Cuthbertson, D.; Hoffman, G.S.; Koening, C.L.; Langford, C.A.; McAlear, C.; et al. Vasculitis in Patients with Inflammatory Bowel Diseases: A Study of 32 Patients and Systematic Review of the Literature. Semin. Arthritis Rheum. 2016, 45, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Stebbing, J.; Askin, F.; Fishman, E.; Stone, J. Pulmonary Manifestations of Ulcerative Colitis Mimicking Wegener’s Granulomatosis. J. Rheumatol. 1999, 26, 1617–1621. [Google Scholar]
- Godet, P.G.; Cowie, R.; Woodman, R.C.; Sutherland, L.R. Pulmonary Function Abnormalities in Patients with Ulcerative Colitis. Am. J. Gastroenterol. 1997, 92, 1154–1156. [Google Scholar]
- Heatley, R.V.; Thomas, P.; Prokipchuk, E.J.; Gauldie, J.; Sieniewicz, D.J.; Bienenstock, J. Pulmonary Function Abnormalities in Patients with Inflammatory Bowel Disease. Q. J. Med. 1982, 51, 241–250. [Google Scholar]
- Herrlinger, K.R.; Noftz, M.K.; Dalhoff, K.; Ludwig, D.; Stange, E.F.; Fellermann, K. Alterations in Pulmonary Function in Inflammatory Bowel Disease Are Frequent and Persist during Remission. Am. J. Gastroenterol. 2002, 97, 377–381. [Google Scholar] [CrossRef]
- Dierkes-Globisch, A.; Mohr, H.-H. Pulmonary Function Abnormalities in Respiratory Asymptomatic Patients with Inflammatory Bowel Disease. Eur. J. Intern. Med. 2002, 13, 385–388. [Google Scholar] [CrossRef] [PubMed]
- Ellrichmann, M.; Bethge, J.; Boesenkoetter, J.; Conrad, C.; Noth, R.; Bahmer, T.; Nikolaus, S.; Aden, K.; Zeissig, S.; Schreiber, S. Subclinical Pulmonary Involvement in Active IBD Responds to Biologic Therapy. J. Crohn’s Colitis 2021, 15, 1339–1345. [Google Scholar] [CrossRef]
- Georgakopoulou, V.E.; Tarantinos, K.; Papalexis, P.; Spandidos, D.A.; Damaskos, C.; Gkoufa, A.; Chlapoutakis, S.; Sklapani, P.; Trakas, N.; Mermigkis, D. Role of Pulmonary Function Testing in Inflammatory Bowel Diseases (Review). Med. Int. 2022, 2, 25. [Google Scholar] [CrossRef] [PubMed]
- Ji, X.-Q.; Wang, L.-X.; Lu, D.-G. Pulmonary Manifestations of Inflammatory Bowel Disease. World J. Gastroenterol. 2014, 20, 13501–13511. [Google Scholar] [CrossRef]
- Songür, N.; Songür, Y.; Tüzün, M.; Doğan, I.; Tüzün, D.; Ensari, A.; Hekimoglu, B. Pulmonary Function Tests and High-Resolution CT in the Detection of Pulmonary Involvement in Inflammatory Bowel Disease. J. Clin. Gastroenterol. 2003, 37, 292–298. [Google Scholar] [CrossRef]
- Marvisi, M.; Fornasari, G. Is the Lung a Target Organ in Inflammatory Bowel Disease? Recent. Prog. Med. 2001, 92, 774–777. [Google Scholar]
- Neilly, J.B.; Main, A.N.; McSharry, C.; Murray, J.; Russell, R.I.; Moran, F. Pulmonary Abnormalities in Crohn’s Disease. Respir. Med. 1989, 83, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, A. Pulmonary Involvement in Inflammatory Bowel Disease. World J. Gastroenterol. 2010, 16, 4952. [Google Scholar] [CrossRef]
- Tzanakis, N.; Bouros, D.; Samiou, M.; Panagou, P.; Mouzas, J.; Manousos, O.; Siafakas, N. Lung Function in Patients with Inflammatory Bowel Disease. Respir. Med. 1998, 92, 516–522. [Google Scholar] [CrossRef]
- Douglas, J.G.; McDonald, C.F.; Leslie, M.J.; Gillon, J.; Crompton, G.K.; McHardy, G.J. Respiratory Impairment in Inflammatory Bowel Disease: Does It Vary with Disease Activity? Respir. Med. 1989, 83, 389–394. [Google Scholar] [CrossRef]
- Sethy, P.K.; Dutta, U.; Aggrawal, A.N.; Das, R.; Gulati, M.; Sinha, S.K.; Singh, K. Pulmonary and Hematological Alterations in Idiopathic Ulcerative Colitis. Indian J. Gastroenterol. 2003, 22, 176–179. [Google Scholar] [PubMed]
- Ateş, F.; Karincaoğlu, M.; Hacievlıyagıl, S.S.; Yalniz, M.; Seçkın, Y. Alterations in the Pulmonary Function Tests of Inflammatory Bowel Diseases. Turk. J. Gastroenterol. 2011, 22, 293–299. [Google Scholar] [CrossRef]
- Tunc, B.; Filik, L.; Bilgic, F.; Arda, K.; Ulker, A. Pulmonary Function Tests, High-Resolution Computed Tomography Findings and Inflammatory Bowel Disease. Acta Gastroenterol. Belg. 2006, 69, 255–260. [Google Scholar]
- Louis, E.; Louis, R.; Drion, V.; Bonnet, V.; Lamproye, A.; Radermecker, M.; Belaiche, J. Increased Frequency of Bronchial Hyperresponsiveness in Patients with Inflammatory Bowel Disease. Allergy 1995, 50, 729–733. [Google Scholar] [CrossRef] [PubMed]
- Bartholo, R.M.; Zaltman, C.; Elia, C.; Cardoso, A.P.; Flores, V.; Lago, P.; Cassabian, L.; Dorileo, F.C.; Lapa-e-Silva, J.R. Bronchial Hyperresponsiveness and Analysis of Induced Sputum Cells in Crohn’s Disease. Braz. J. Med. Biol. Res. 2005, 38, 197–203. [Google Scholar] [CrossRef]
- Ceyhan, B.B.; Karakurt, S.; Cevik, H.; Sungur, M. Bronchial Hyperreactivity and Allergic Status in Inflammatory Bowel Disease. Respiration 2003, 70, 60–66. [Google Scholar] [CrossRef]
- Koek, G.H.; Verleden, G.M.; Evenepoel, P.; Rutgeerts, P. Activity Related Increase of Exhaled Nitric Oxide in Crohn’s Disease and Ulcerative Colitis: A Manifestation of Systemic Involvement? Respir. Med. 2002, 96, 530–535. [Google Scholar] [CrossRef]
- Quenon, L.; Hindryckx, P.; De Vos, M.; De Looze, D.; Joos, G.; Brusselle, G.; Peeters, H. Hand-Held Fractional Exhaled Nitric Oxide Measurements as a Non-Invasive Indicator of Systemic Inflammation in Crohn’s Disease. J. Crohn’s Colitis 2013, 7, 644–648. [Google Scholar] [CrossRef] [PubMed]
- Ozyilmaz, E.; Yildirim, B.; Erbas, G.; Akten, S.; Oguzulgen, I.K.; Tunc, B.; Tuncer, C.; Turktas, H. Value of Fractional Exhaled Nitric Oxide (FE NO) for the Diagnosis of Pulmonary Involvement Due to Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2010, 16, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Protopapas, A.A.; Vradelis, S.; Karampitsakos, T.; Steiropoulos, P.; Chatzimichael, A.; Paraskakis, E. Elevated Levels of Alveolar Nitric Oxide May Indicate Presence of Small Airway Inflammation in Patients with Inflammatory Bowel Disease. Lung 2019, 197, 663–670. [Google Scholar] [CrossRef]
- Aydin, B.; Songur, Y.; Songur, N.; Aksu, O.; Senol, A.; Ciris, I.M.; Sutcu, R. Investigation of Pulmonary Involvement in Inflammatory Bowel Disease in an Experimental Model of Colitis. Korean J. Intern. Med. 2016, 31, 853–859. [Google Scholar] [CrossRef]
- Biancone, L.; Armuzzi, A.; Scribano, M.L.; Castiglione, F.; D’Incà, R.; Orlando, A.; Papi, C.; Daperno, M.; Vecchi, M.; Riegler, G.; et al. Cancer Risk in Inflammatory Bowel Disease: A 6-Year Prospective Multicenter Nested Case-Control IG-IBD Study. Inflamm. Bowel Dis. 2020, 26, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Lo, B.; Zhao, M.; Vind, I.; Burisch, J. The Risk of Extraintestinal Cancer in Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis of Population-Based Cohort Studies. Clin. Gastroenterol. Hepatol. 2021, 19, 1117–1138.e19. [Google Scholar] [CrossRef] [PubMed]
- Jess, T.; Horváth-Puhó, E.; Fallingborg, J.; Rasmussen, H.H.; Jacobsen, B.A. Cancer Risk in Inflammatory Bowel Disease According to Patient Phenotype and Treatment: A Danish Population-Based Cohort Study. Am. J. Gastroenterol. 2013, 108, 1869–1876. [Google Scholar] [CrossRef]
- Kappelman, M.D.; Farkas, D.K.; Long, M.D.; Erichsen, R.; Sandler, R.S.; Sørensen, H.T.; Baron, J.A. Risk of Cancer in Patients with Inflammatory Bowel Diseases: A Nationwide Population-Based Cohort Study with 30 Years of Follow-up Evaluation. Clin. Gastroenterol. Hepatol. 2014, 12, 265–273.e1. [Google Scholar] [CrossRef]
- Karlén, P.; Löfberg, R.; Broström, O.; Leijonmarck, C.-E.; Hellers, G.; Persson, P.-G. Increased Risk of Cancer in Ulcerative Colitis: A Population-Based Cohort Study. Am. J. Gastroenterol. 1999, 94, 1047–1052. [Google Scholar] [CrossRef]
- Palli, D.; Trallori, G.; Bagnoli, S.; Saieva, C.; Tarantino, O.; Ceroti, M.; D’Albasio, G.; Pacini, F.; Amorosi, A.; Masala, G. Hodgkin’s Disease Risk Is Increased in Patients with Ulcerative Colitis. Gastroenterology 2000, 119, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Deng, Y.; Tin, M.S.; Lok, V.; Ngai, C.H.; Zhang, L.; Lucero-Prisno, D.E.; Xu, W.; Zheng, Z.-J.; Elcarte, E.; et al. Distribution, Risk Factors, and Temporal Trends for Lung Cancer Incidence and Mortality. Chest 2022, 161, 1101–1111. [Google Scholar] [CrossRef]
- Kucharzik, T.; Ellul, P.; Greuter, T.; Rahier, J.F.; Verstockt, B.; Abreu, C.; Albuquerque, A.; Allocca, M.; Esteve, M.; Farraye, F.A.; et al. ECCO Guidelines on the Prevention, Diagnosis, and Management of Infections in Inflammatory Bowel Disease. J. Crohn’s Colitis 2021, 15, 879–913. [Google Scholar] [CrossRef]
- Kantsø, B.; Simonsen, J.; Hoffmann, S.; Valentiner-Branth, P.; Petersen, A.M.; Jess, T. Inflammatory Bowel Disease Patients Are at Increased Risk of Invasive Pneumococcal Disease: A Nationwide Danish Cohort Study 1977–2013. Am. J. Gastroenterol. 2015, 110, 1582–1587. [Google Scholar] [CrossRef]
- Case, D.J.; Copeland, L.A.; Stock, E.M.; Herrera, H.R.; Pfanner, T.P. Pneumococcal Vaccination Rates in VHA Patients with Inflammatory Bowel Disease. Medicine 2015, 94, e417. [Google Scholar] [CrossRef] [PubMed]
- Fernández Llamas, T.; Sánchez Torres, A.; Egea Valenzuela, J. Community-Acquired Pneumonia by Legionella Pneumophila. Do We Need to Include New Recommendations for Inflammatory Bowel Disease Patients under Immunomodulators? Rev. Española Enfermedades Dig. 2016, 108, 524. [Google Scholar] [CrossRef] [PubMed]
- Bonovas, S.; Fiorino, G.; Allocca, M.; Lytras, T.; Nikolopoulos, G.K.; Peyrin-Biroulet, L.; Danese, S. Biologic Therapies and Risk of Infection and Malignancy in Patients with Inflammatory Bowel Disease: A Systematic Review and Network Meta-Analysis. Clin. Gastroenterol. Hepatol. 2016, 14, 1385–1397.e10. [Google Scholar] [CrossRef] [PubMed]
- Cagatay, T.; Bingol, Z.; Kıyan, E.; Yegin, Z.; Okumus, G.; Arseven, O.; Erkan, F.; Gulbaran, Z.; Erelel, M.; Ece, T.; et al. Follow-up of 1887 Patients Receiving Tumor Necrosis-alpha Antagonists: Tuberculin Skin Test Conversion and Tuberculosis Risk. Clin. Respir. J. 2018, 12, 1668–1675. [Google Scholar] [CrossRef]
- Abitbol, Y.; Laharie, D.; Cosnes, J.; Allez, M.; Nancey, S.; Amiot, A.; Aubourg, A.; Fumery, M.; Altwegg, R.; Michetti, P.; et al. Negative Screening Does Not Rule Out the Risk of Tuberculosis in Patients with Inflammatory Bowel Disease Undergoing Anti-TNF Treatment: A Descriptive Study on the GETAID Cohort. J. Crohn’s Colitis 2016, 10, 1179–1185. [Google Scholar] [CrossRef]
- Winthrop, K.L.; Park, S.-H.; Gul, A.; Cardiel, M.H.; Gomez-Reino, J.J.; Tanaka, Y.; Kwok, K.; Lukic, T.; Mortensen, E.; Ponce de Leon, D.; et al. Tuberculosis and Other Opportunistic Infections in Tofacitinib-Treated Patients with Rheumatoid Arthritis. Ann. Rheum. Dis. 2016, 75, 1133–1138. [Google Scholar] [CrossRef]
- Tinsley, A.; Navabi, S.; Williams, E.D.; Liu, G.; Kong, L.; Coates, M.D.; Clarke, K. Increased Risk of Influenza and Influenza-Related Complications Among 140,480 Patients with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2019, 25, 369–376. [Google Scholar] [CrossRef]
- Ungaro, R.C.; Brenner, E.J.; Gearry, R.B.; Kaplan, G.G.; Kissous-Hunt, M.; Lewis, J.D.; Ng, S.C.; Rahier, J.-F.; Reinisch, W.; Steinwurz, F.; et al. Effect of IBD Medications on COVID-19 Outcomes: Results from an International Registry. Gut 2021, 70, 725–732. [Google Scholar] [CrossRef]
- Le Gros, V.; Saveuse, H.; Lesur, G.; Brion, N. Lung and Skin Hypersensitivity to 5-Aminosalicylic Acid. BMJ 1991, 302, 970. [Google Scholar] [CrossRef]
- Foster, R.A.; Zander, D.S.; Mergo, P.J.; Valentine, J.F. Mesalamine-Related Lung Disease: Clinical, Radiographic, and Pathologic Manifestations. Inflamm. Bowel Dis. 2003, 9, 308–315. [Google Scholar] [CrossRef]
- Matsuno, O. Drug-Induced Interstitial Lung Disease: Mechanisms and Best Diagnostic Approaches. Respir. Res. 2012, 13, 39. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Lee, J.-H.; Koh, E.-S.; Park, S.W.; Jang, A.-S.; Kim, D.; Park, C.-S. Acute Eosinophilic Pneumonia Related to a Mesalazine Suppository. Asia Pac. Allergy 2013, 3, 136–139. [Google Scholar] [CrossRef]
- Abraham, A.; Karakurum, A. Acute Respiratory Failure Secondary to Mesalamine-Induced Interstitial Pneumonitis. Case Rep. 2013, 2013, bcr2013009834. [Google Scholar] [CrossRef]
- Oi, H.; Suzuki, A.; Yamano, Y.; Yokoyama, T.; Matsuda, T.; Kataoka, K.; Suzuki, Y.; Kimura, T.; Kondoh, Y. Mesalazine-Induced Lung Injury with Severe Respiratory Failure Successfully Treated with Steroids and Non-Invasive Positive Pressure Ventilation. Respir. Med. Case Rep. 2020, 31, 101157. [Google Scholar] [CrossRef]
- Das, K.M.; Dubin, R. Clinical Pharmacokinetics of Sulphasalazine. Clin. Pharmacokinet. 1976, 1, 406–425. [Google Scholar] [CrossRef] [PubMed]
- Parry, S.D.; Barbatzas, C.; Peel, E.T.; Barton, J.R. Sulphasalazine and Lung Toxicity. Eur. Respir. J. 2002, 19, 756–764. [Google Scholar] [CrossRef] [PubMed]
- Nagy, F. A Case of Interstitial Pneumonitis in a Patient with Ulcerative Colitis Treated with Azathioprine. World J. Gastroenterol. 2007, 13, 316. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, A.N.; Attila, T.; Otterson, M.F.; Lipchik, R.J.; Massey, B.T.; Komorowski, R.A.; Binion, D.G. Severe Pulmonary Toxicity After Azathioprine/6-Mercaptopurine Initiation for the Treatment of Inflammatory Bowel Disease. J. Clin. Gastroenterol. 2007, 41, 682–688. [Google Scholar] [CrossRef]
- Atzeni, F.; Boiardi, L.; Sallì, S.; Benucci, M.; Sarzi-Puttini, P. Lung Involvement and Drug-Induced Lung Disease in Patients with Rheumatoid Arthritis. Expert. Rev. Clin. Immunol. 2013, 9, 649–657. [Google Scholar] [CrossRef]
- Fragoulis, G.E.; Conway, R.; Nikiphorou, E. Methotrexate and Interstitial Lung Disease: Controversies and Questions. A Narrative Review of the Literature. Rheumatology 2019, 58, 1900–1906. [Google Scholar] [CrossRef]
- Jakubovic, B.D.; Donovan, A.; Webster, P.M.; Shear, N.H. Methotrexate-Induced Pulmonary Toxicity. Can. Respir. J. 2013, 20, 153–155. [Google Scholar] [CrossRef] [PubMed]
- Imokawa, S.; Colby, T.V.; Leslie, K.O.; Helmers, R.A. Methotrexate Pneumonitis: Review of the Literature and Histopathological Findings in Nine Patients. Eur. Respir. J. 2000, 15, 373. [Google Scholar] [CrossRef] [PubMed]
- Bedrossian, C.W.M.; Miller, W.C.; Luna, M.A. Methotrexate-Induced Diffuse Interstitial Pulmonary Fibrosis. S. Med. J. 1979, 72, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, R.L.; Waite, D.H. Progressive Interstitial Lung Disease from Prolonged Methotrexate Therapy. Arch. Dermatol. 1978, 114, 1800–1802. [Google Scholar] [CrossRef] [PubMed]
- Phillips, T.J.; Jones, D.H.; Baker, H. Pulmonary Complications Following Methotrexate Therapy. J. Am. Acad. Dermatol. 1987, 16, 373–375. [Google Scholar] [CrossRef]
- Quah, E.; Amoasii, C.; Mudawi, T.; Dawson, J. Systematic Literature Review Investigating Whether Methotrexate Causes Chronic Pulmonary Fibrosis. Future Healthc. J. 2019, 6, 4. [Google Scholar] [CrossRef]
- Raine, T.; Bonovas, S.; Burisch, J.; Kucharzik, T.; Adamina, M.; Annese, V.; Bachmann, O.; Bettenworth, D.; Chaparro, M.; Czuber-Dochan, W.; et al. ECCO Guidelines on Therapeutics in Ulcerative Colitis: Medical Treatment. J. Crohn’s Colitis 2022, 16, 2–17. [Google Scholar] [CrossRef]
- Torres, J.; Bonovas, S.; Doherty, G.; Kucharzik, T.; Gisbert, J.P.; Raine, T.; Adamina, M.; Armuzzi, A.; Bachmann, O.; Bager, P.; et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Medical Treatment. J. Crohn’s Colitis 2020, 14, 4–22. [Google Scholar] [CrossRef]
- Aqsa, A.; Sharma, D.; Chalhoub, M. Adalimumab Induced Interstitial Lung Disease. Respir. Med. Case Rep. 2020, 29, 101012. [Google Scholar] [CrossRef]
- Thavarajah, K.; Wu, P.; Rhew, E.J.; Yeldandi, A.K.; Kamp, D.W. Pulmonary Complications of Tumor Necrosis Factor-Targeted Therapy. Respir. Med. 2009, 103, 661–669. [Google Scholar] [CrossRef]
- Sen, S.; Jordan, K.; Boes, T.J.; Peltz, C. Infliximab-Induced Nonspecific Interstitial Pneumonia. Am. J. Med. Sci. 2012, 344, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Perez-Alvarez, R.; Perez-de-Lis, M.; Diaz-Lagares, C.; Pego-Reigosa, J.M.; Retamozo, S.; Bove, A.; Brito-Zeron, P.; Bosch, X.; Ramos-Casals, M. Interstitial Lung Disease Induced or Exacerbated by TNF-Targeted Therapies: Analysis of 122 Cases. Semin. Arthritis Rheum. 2011, 41, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Komiya, K.; Ishii, H.; Fujita, N.; Oka, H.; Iwata, A.; Sonoda, H.; Kadota, J. Adalimumab-Induced Interstitial Pneumonia with an Improvement of Pre-Existing Rheumatoid Arthritis-Associated Lung Involvement. Intern. Med. 2011, 50, 749–751. [Google Scholar] [CrossRef]
- Dias, O.M.; Pereira, D.A.S.; Baldi, B.G.; Costa, A.N.; Athanazio, R.A.; Kairalla, R.A.; Carvalho, C.R.R. Adalimumab-Induced Acute Interstitial Lung Disease in a Patient with Rheumatoid Arthritis. J. Bras. Pneumol. 2014, 40, 77–81. [Google Scholar] [CrossRef]
- Alaee, S.; Jones, Q. Case of Drug-Induced Interstitial Lung Disease Secondary to Adalimumab. BMJ Case Rep. 2018, 2018, bcr-2018-224375. [Google Scholar] [CrossRef]
- Casanova, M.J.; Chaparro, M.; Valenzuela, C.; Cisneros, C.; Gisbert, J.P. Adalimumab-Induced Interstitial Pneumonia in a Patient with Crohn’s Disease. World J. Gastroenterol. 2015, 21, 2260–2262. [Google Scholar] [CrossRef]
- Yamazaki, H.; Isogai, S.; Sakurai, T.; Nagasaka, K. A Case of Adalimumab-Associated Interstitial Pneumonia with Rheumatoid Arthritis. Mod. Rheumatol. 2010, 20, 518–521. [Google Scholar] [CrossRef]
- Reid, J.D.; Bressler, B.; English, J. A Case of Adalimumab-Induced Pneumonitis in a 45-Year-Old Man with Crohn’s Disease. Can. Respir. J. 2011, 18, 262–264. [Google Scholar] [CrossRef]
- Phang, K.F.; Teng, G.G.; Teo, L.L.S.; Seet, J.E.; Teoh, C.M.; Teo, F.S.W. A 67-Year-Old Man with Psoriatic Arthritis and New-Onset Dyspnea. Chest 2018, 154, e127–e134. [Google Scholar] [CrossRef]
- Valesini, G.; Iannuccelli, C.; Marocchi, E.; Pascoli, L.; Scalzi, V.; Di Franco, M. Biological and Clinical Effects of Anti-TNFα Treatment. Autoimmun. Rev. 2007, 7, 35–41. [Google Scholar] [CrossRef]
- Ramos-Casals, M.; Brito-Zerón, P.; Muñoz, S.; Soria, N.; Galiana, D.; Bertolaccini, L.; Cuadrado, M.-J.; Khamashta, M.A. Autoimmune Diseases Induced by TNF-Targeted Therapies. Medicine 2007, 86, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Nugent, K.; Diri, E.; Tello, W.; Ratnoff, W.D. Letter to the Editor: Infliximab-Induced SLE-like Syndrome Involving the Lung and Pleura. Lupus 2007, 16, 764–766. [Google Scholar] [CrossRef] [PubMed]
- Abreu, M.T.; Rowbotham, D.S.; Danese, S.; Sandborn, W.J.; Miao, Y.; Zhang, H.; Tikhonov, I.; Panaccione, R.; Hisamatsu, T.; Scherl, E.J.; et al. Efficacy and Safety of Maintenance Ustekinumab for Ulcerative Colitis Through 3 Years: UNIFI Long-Term Extension. J. Crohn’s Colitis 2022, 16, 1222–1234. [Google Scholar] [CrossRef]
- Brinker, A.; Cheng, C.; Chan, V. Association of Noninfectious Pneumonia with Ustekinumab Use. JAMA Dermatol. 2019, 155, 221. [Google Scholar] [CrossRef]
- Kalra, S.S.; Chizinga, M.; Trillo-Alvarez, C.; Papierniak, E.S. Ustekinumab Associated Chronic Eosinophilic Pneumonia. J. Asthma 2021, 58, 1670–1674. [Google Scholar] [CrossRef]
- Despotes, K.A.; Vigeland, C.L. Stelara Struck: A Case of Noninfectious Pneumonitis Secondary to Ustekinumab. BMC Pulm. Med. 2022, 22, 280. [Google Scholar] [CrossRef] [PubMed]
- De la Bretèque, M.A.; Appere-De Vecchi, C.; Zeboulon, C.; Zaien, I.; Sigal, M.-L.; Mahé, E. Pneumopathie à Éosinophiles Chez Un Patient Atteint de Psoriasis En Plaques Traité Par Ustékinumab. Ann. Dermatol. Venereol. 2015, 142, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Chertoff, J.; Harden, C.; Wakefield, D.; Wynne, J. Stop Being So Sensitive: An Exceptionally Rare Report of Ustekinumab-Induced Sub-Acute Hypersensitivity Pneumonitis. Turk. J. Anesth. Reanim. 2017, 45, 313–317. [Google Scholar] [CrossRef]
- Schwaiblmair, M. Drug Induced Interstitial Lung Disease. Open Respir. Med. J. 2012, 6, 63–74. [Google Scholar] [CrossRef]
- Yashiro, M.; Maejima, H.; Taniguchi, T.; Katsuoka, K.; Kimura, M.; Wada, M. Psoriasis Vulgaris Complicated by Eosinophilic Pneumonia during Ustekinumab Treatment. Eur. J. Dermatol. 2013, 23, 396–397. [Google Scholar] [CrossRef]
- Fischer, A.; Zundler, S.; Atreya, R.; Rath, T.; Voskens, C.; Hirschmann, S.; López-Posadas, R.; Watson, A.; Becker, C.; Schuler, G.; et al. Differential Effects of A4β7 and GPR15 on Homing of Effector and Regulatory T Cells from Patients with UC to the Inflamed Gut in Vivo. Gut 2016, 65, 1642–1664. [Google Scholar] [CrossRef] [PubMed]
- Feagan, B.G.; Bhayat, F.; Khalid, M.; Blake, A.; Travis, S.P.L. Respiratory Tract Infections in Patients with Inflammatory Bowel Disease: Safety Analyses from Vedolizumab Clinical Trials. J. Crohn’s Colitis 2018, 12, 905–919. [Google Scholar] [CrossRef] [PubMed]
- Marafini, I.; Troncone, E.; Rocchetti, I.; Monteleone, G. Respiratory Tract Infections in Inflammatory Bowel Disease Patients Taking Vedolizumab: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Pharmacol. 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Prados, A.; Muñoz-Fernández, R.; Fernandez-Rubio, P.; Olivares, E.G. Characterization of Mesenchymal Stem/Stromal Cells with Lymphoid Tissue Organizer Cell Potential in Tonsils from Children. Eur. J. Immunol. 2018, 48, 829–843. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, D.; Privitera, G.; Schepis, T.; Larosa, L.; Onali, S.; Scaldaferri, F.; Gasbarrini, A.; Caprioli, F.; Armuzzi, A. Drug-Related Pneumonitis in Patients Receiving Vedolizumab Therapy for Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2022, 20, e1483–e1487. [Google Scholar] [CrossRef]
- Nambiar, S.; Karippot, A.; Oliver, T. Vedolizumab-Associated Acute Respiratory Distress Syndrome. Am. J. Ther. 2018, 25, e592–e593. [Google Scholar] [CrossRef]
- De Backer, E.; Bode, H.; Baert, F. New-Onset Diffuse Parenchymal Lung Disease in a 52-Year-Old Woman with Ulcerative Colitis. Gastroenterology 2020, 158, 478–479. [Google Scholar] [CrossRef]
- Rizos, E.D.; Antonogiannaki, E.-M.; Chatzidakis, A.; Kallieri, M.; Tsilogianni, Z.; Manali, E.D.; Economopoulos, N.; Triantafyllou, K.; Papiris, S.A.; Polymeros, D. Vedolizumab-Induced Acute Interstitial Lung Injury in a 39-Year-Old Male with Ulcerative Colitis. Eur. J. Gastroenterol. Hepatol. 2021, 33, e1057–e1059. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, M.-H.; Gao, X.; Dong, C.; Li, Y.-X. Vedolizumab-Associated Diffuse Interstitial Lung Disease in Patients with Ulcerative Colitis: A Case Report. World J. Clin. Cases 2022, 10, 1716–1722. [Google Scholar] [CrossRef]
- Lissner, D.; Glauben, R.; Allers, K.; Sonnenberg, E.; Loddenkemper, C.; Schneider, T.; Siegmund, B. Pulmonary Manifestation of Crohn’s Disease Developed Under Treatment with Vedolizumab. Am. J. Gastroenterol. 2018, 113, 146–148. [Google Scholar] [CrossRef]
- Abu Shtaya, A.; Cohen, S.; Kogan, Y.; Shteinberg, M.; Sagol, O. Crohn’s Disease with Atypical Extra-Intestinal Manifestations Developing Under Treatment with Vedolizumab. Eur. J. Case Rep. Intern. Med. 2021, 8, 002265. [Google Scholar] [CrossRef] [PubMed]
- Myc, L.A.; Girton, M.R.; Stoler, M.H.; Davis, E.M. Necrobiotic Pulmonary Nodules of Crohn’s Disease in a Patient Receiving Vedolizumab. Am. J. Respir. Crit. Care Med. 2019, 199, e1–e2. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Zhao, T.; Wei, J.; Chai, D.; Zhao, C.; Zhu, Y.; Deng, M. Case Report: Eosinophilic Pneumonia Associated with Vedolizumab Therapy in a Patient with Ulcerative Colitis. Front. Med. 2022, 9, 942237. [Google Scholar] [CrossRef] [PubMed]
- Dulaney, D.; Dave, P.; Walsh, S.; Mehandru, S.; Colombel, J.-F.; Agrawal, M. Noninfectious Pulmonary Complications Associated with Anti-Integrin Therapy: A Case Report and Systematic Review of the Literature. Inflamm. Bowel Dis. 2022, 28, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.R.; Khan, D.A. Non-IgE-Mediated Drug Hypersensitivity Reactions. Curr. Allergy Asthma Rep. 2021, 21, 41. [Google Scholar] [CrossRef] [PubMed]
- Khoo, J.K.; Barnes, H.; Key, S.; Glaspole, I.N.; Östör, A.J. Pulmonary Adverse Events of Small Molecule JAK Inhibitors in Autoimmune Disease: Systematic Review and Meta-Analysis. Rheumatology 2020, 59, 2217–2225. [Google Scholar] [CrossRef]
- Ytterberg, S.R.; Bhatt, D.L.; Mikuls, T.R.; Koch, G.G.; Fleischmann, R.; Rivas, J.L.; Germino, R.; Menon, S.; Sun, Y.; Wang, C.; et al. Cardiovascular and Cancer Risk with Tofacitinib in Rheumatoid Arthritis. N. Engl. J. Med. 2022, 386, 316–326. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Panés, J.; Sands, B.E.; Reinisch, W.; Su, C.; Lawendy, N.; Koram, N.; Fan, H.; Jones, T.V.; Modesto, I.; et al. Venous Thromboembolic Events in the Tofacitinib Ulcerative Colitis Clinical Development Programme. Aliment. Pharmacol. Ther. 2019, 50, 1068–1076. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Lawendy, N.; Danese, S.; Su, C.; Loftus, E.V.; Hart, A.; Dotan, I.; Damião, A.O.M.C.; Judd, D.T.; Guo, X.; et al. Safety and Efficacy of Tofacitinib for Treatment of Ulcerative Colitis: Final Analysis of OCTAVE Open, an Open-label, Long-term Extension Study with up to 7.0 Years of Treatment. Aliment. Pharmacol. Ther. 2022, 55, 464–478. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Anatomical Site | Pathology | Symptoms | Imaging and Additional Investigations |
| Airways diseases |
| Cough Phlegm Hoarseness Dyspnea Stridor Respiratory distress Sputum production Wheezing |
|
| Interstitium |
| Dyspnea Fever Acute respiratory failure Chest pain Dry cough |
|
| Pulmonary embolism |
| Cough Palpitations Chest pain Shortness of breath |
|
| Vasculitis |
| Cough Shortness of breath Constitutional symptom (fever, weight loss, or fatigue) |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavalli, C.A.M.; Gabbiadini, R.; Dal Buono, A.; Quadarella, A.; De Marco, A.; Repici, A.; Bezzio, C.; Simonetta, E.; Aliberti, S.; Armuzzi, A. Lung Involvement in Inflammatory Bowel Diseases: Shared Pathways and Unwanted Connections. J. Clin. Med. 2023, 12, 6419. https://doi.org/10.3390/jcm12196419
Cavalli CAM, Gabbiadini R, Dal Buono A, Quadarella A, De Marco A, Repici A, Bezzio C, Simonetta E, Aliberti S, Armuzzi A. Lung Involvement in Inflammatory Bowel Diseases: Shared Pathways and Unwanted Connections. Journal of Clinical Medicine. 2023; 12(19):6419. https://doi.org/10.3390/jcm12196419
Chicago/Turabian StyleCavalli, Carolina Aliai Micol, Roberto Gabbiadini, Arianna Dal Buono, Alessandro Quadarella, Alessandro De Marco, Alessandro Repici, Cristina Bezzio, Edoardo Simonetta, Stefano Aliberti, and Alessandro Armuzzi. 2023. "Lung Involvement in Inflammatory Bowel Diseases: Shared Pathways and Unwanted Connections" Journal of Clinical Medicine 12, no. 19: 6419. https://doi.org/10.3390/jcm12196419