
A Review: Integrative Perspectives on the Features and Clinical Management of Psychotic Episodes in Pregnancy
 , , , , , ,
, , , , , ,  , , , ,
, , , ,  and
and
Abstract
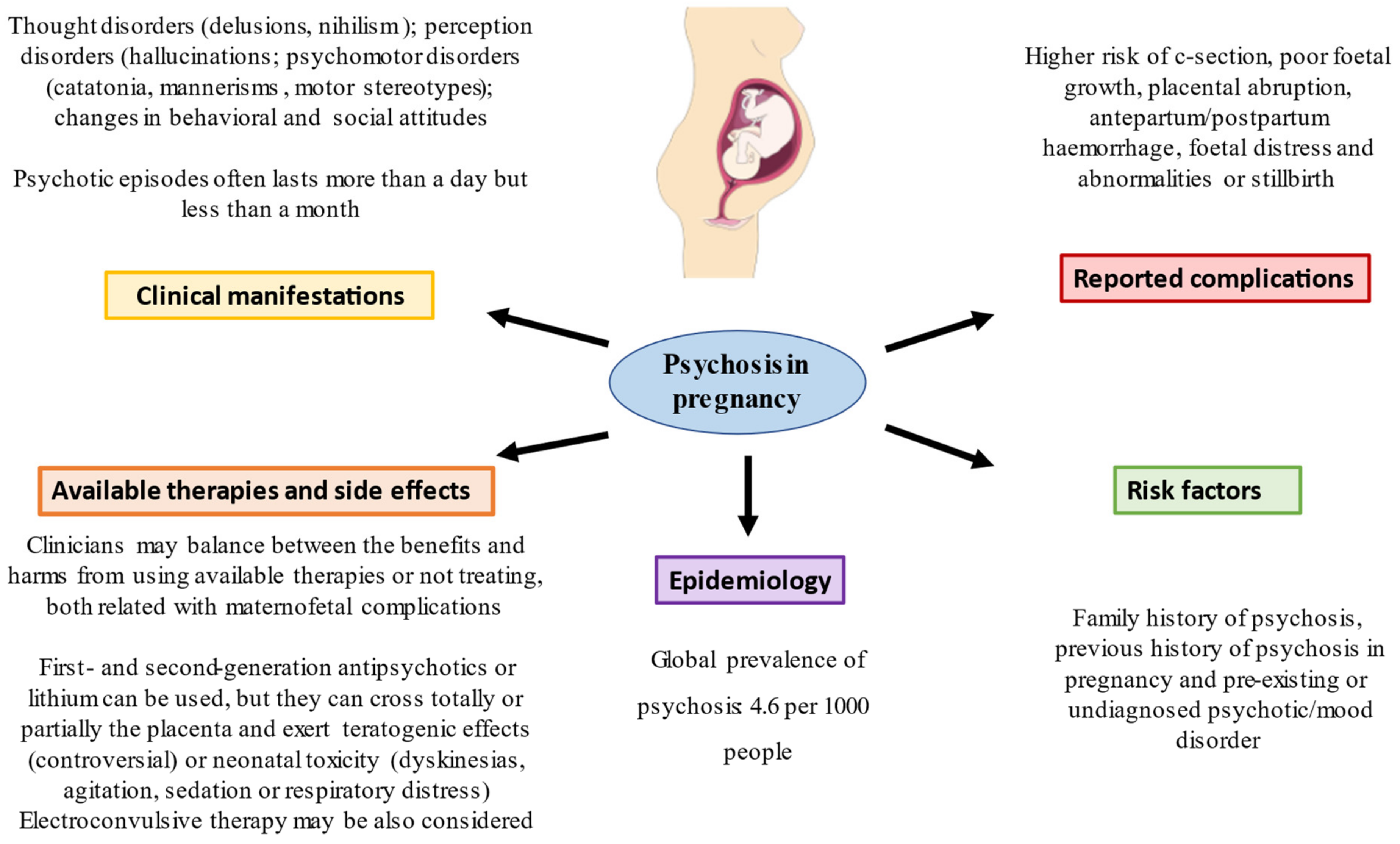
:1. Introduction and Psychosis during Pregnancy
2. Treatment of Psychotic Episodes during Pregnancy
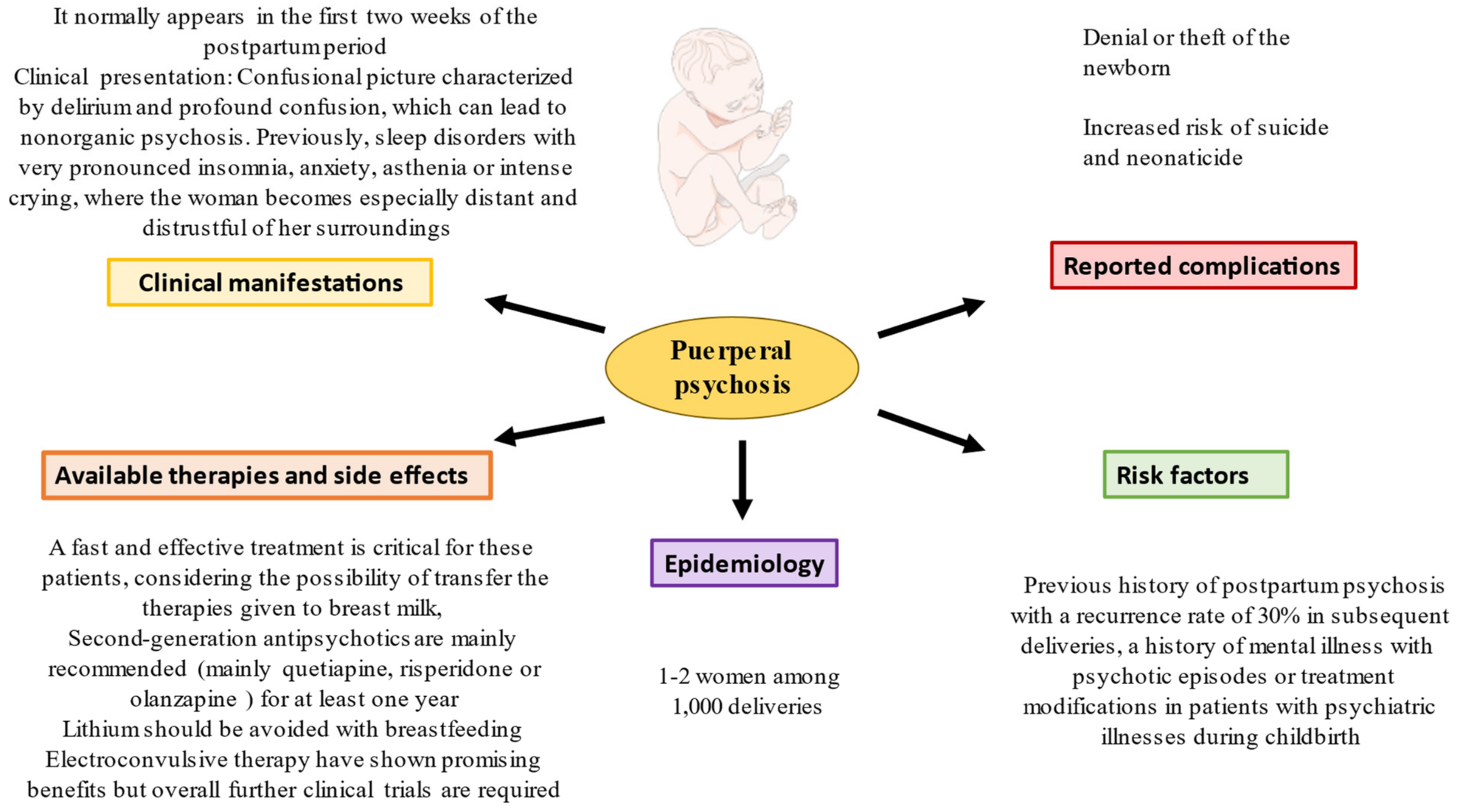
3. Puerperal Psychosis
4. Puerperal Psychosis Treatment
5. Prevention
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heckers, S.; Barch, D.M.; Bustillo, J.; Gaebel, W.; Gur, R.; Malaspina, D.; Owen, M.J.; Schultz, S.; Tandon, R.; Tsuang, M.; et al. Structure of the psychotic disorders classification in DSM-5. Schizophr. Res. 2013, 150, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Küstner, B.; Martín, C.; Pastor, L. Prevalence of psychotic disorders and its association with methodological issues. A systematic review and meta-analyses. PLoS ONE 2018, 13, e0195687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salud_Mental_Datos. Available online: https://www.sanidad.gob.es/estadEstudios/estadisticas/estadisticas/estMinisterio/SIAP/Salud_mental_datos.pdf (accessed on 5 December 2022).
- Sharma, I.; Rai, S.; Pathak, A. Postpartum psychiatric disorders: Early diagnosis and management. Indian J. Psychiatry 2015, 57, S216. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Q.-Y.; Gelaye, B.; Fricchione, G.L.; Avillach, P.; Karlson, E.W.; Williams, M.A. Adverse obstetric and neonatal outcomes complicated by psychosis among pregnant women in the United States. BMC Pregnancy Childbirth 2018, 18, 120. [Google Scholar] [CrossRef] [PubMed]
- Watkins, M.E.; Newport, D.J. Psychosis in pregnancy. Obstet. Gynecol. 2009, 113, 1349–1353. [Google Scholar] [CrossRef]
- MacCabe, J.H.; Martinsson, L.; Lichtenstein, P.; Nilsson, E.; Cnattingius, S.; Murray, R.; Hultman, C.M. Adverse pregnancy outcomes in mothers with affective psychosis. Bipolar Disord. 2007, 9, 305–309. [Google Scholar] [CrossRef]
- Calabrese, J.; Al Khalili, Y. Psychosis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK546579/ (accessed on 5 December 2022).
- Grace, A.A. Pathophysiology of psychosis and novel approaches to treatment. Int. Clin. Psychopharmacol. 2012, 28, e12. [Google Scholar] [CrossRef]
- Guillén, J.M.B.; Company, E.S. Uso de antipsicóticos durante el embarazo y la lactancia. Rev. Psiquiatr. Salud Ment. 2009, 2, 138–145. [Google Scholar] [CrossRef]
- Forde, R.; Peters, S.; Wittkowski, A. Recovery from postpartum psychosis: A systematic review and metasynthesis of women’s and families’ experiences. Arch. Women’s Ment. Health 2020, 23, 597–612. [Google Scholar] [CrossRef] [Green Version]
- Viguera, A.C.; Tondo, L.; Koukopoulos, A.E.; Reginaldi, D.; Lepri, B.; Baldessarini, R.J. Episodes of Mood Disorders in 2252 Pregnancies and Postpartum Periods. Am. J. Psychiatry 2011, 168, 1179–1185. [Google Scholar] [CrossRef]
- Khalifeh, H.; Hunt, I.M.; Appleby, L.; Howard, L.M. Suicide in perinatal and non-perinatal women in contact with psychiatric services: 15 year findings from a UK national inquiry. Lancet Psychiatry 2016, 3, 233–242. [Google Scholar] [CrossRef]
- Grof, P.; Robbins, W.; Alda, M.; Berghoefer, A.; Vojtechovsky, M.; Nilsson, A.; Robertson, C. Protective effect of pregnancy in women with lithium-responsive bipolar disorder. J. Affect. Disord. 2000, 61, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Fabre, C.; Pauly, V.; Baumstarck, K.; Etchecopar-Etchart, D.; Orleans, V.; Llorca, P.-M.; Blanc, J.; Lancon, C.; Auquier, P.; Boyer, L.; et al. Pregnancy, delivery and neonatal complications in women with schizophrenia: A national population-based cohort study. Lancet Reg. Health—Eur. 2021, 10, 100209. [Google Scholar] [CrossRef]
- Simoila, L.; Isometsä, E.; Gissler, M.; Suvisaari, J.; Halmesmäki, E.; Lindberg, N. Schizophrenia and pregnancy: A national register-based follow-up study among Finnish women born between 1965 and 1980. Arch. Women’s Ment. Health 2019, 23, 91–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantwell, R.; Cox, J. Psychiatric disorders in pregnancy and the puerperium. Curr. Obstet. Gynaecol. 2003, 13, 7–13. [Google Scholar] [CrossRef]
- Guimaraes, F.J.; Santos, F.J.D.S.; Leite, A.F.B.; de Holanda, V.R.; De Sousa, G.S.; Perrelli, J.G.A. Preferencias Enfermedad mental en mujeres embarazadas. Enferm. Glob. 2018, 18, 499–534. [Google Scholar] [CrossRef]
- Toh, S.; Li, Q.; Cheetham, T.C.; Cooper, W.O.; Davis, R.L.; Dublin, S.; Hammad, T.A.; Li, D.-K.; Pawloski, P.; Pinheiro, S.P.; et al. Prevalence and trends in the use of antipsychotic medications during pregnancy in the U.S.; 2001–2007: A population-based study of 585,615 deliveries. Arch. Women’s Ment. Health 2013, 16, 149–157. [Google Scholar] [CrossRef] [Green Version]
- Altshuler, L.L.; Cohen, L.; Szuba, M.P.; Burt, V.K.; Gitlin, M.; Mintz, J. Pharmacologic management of psychiatric illness during pregnancy: Dilemmas and guidelines. Am. J. Psychiatry 1996, 153, 592–606. [Google Scholar] [CrossRef] [PubMed]
- McKenna, K.; Koren, G.; Tetelbaum, M.; Wilton, L.; Shakir, S.; Diav-Citrin, O.; Levinson, A.; Zipursky, R.B.; Einarson, A. Pregnancy Outcome of Women Using Atypical Antipsychotic Drugs. J. Clin. Psychiatry 2005, 66, 444–449. [Google Scholar] [CrossRef]
- Huybrechts, K.F.; Hernández-Díaz, S.; Patorno, E.; Desai, R.J.; Mogun, H.; Dejene, S.Z.; Cohen, J.; Panchaud, A.; Cohen, L.; Bateman, B.T. Antipsychotic Use in Pregnancy and the Risk for Congenital Malformations. JAMA Psychiatry 2016, 73, 938–946. [Google Scholar] [CrossRef] [PubMed]
- Newport, D.J.; Calamaras, M.R.; DeVane, C.L.; Donovan, J.; Beach, A.J.; Winn, S.; Knight, B.T.; Gibson, B.B.; Viguera, A.C.; Owens, M.J.; et al. Atypical Antipsychotic Administration During Late Pregnancy: Placental Passage and Obstetrical Outcomes. Am. J. Psychiatry 2007, 164, 1214–1220. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, M.R.; Goldfield, M. Cardiovascular malformations with lithium use during pregnancy. Am. J. Psychiatry 1975, 132, 529–531. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.T.T.; Sharma, V.; McIntyre, R.S. Teratogenesis associated with antibipolar agents. Adv. Ther. 2009, 26, 281–294. [Google Scholar] [CrossRef] [PubMed]
- Menon, S.J. Psychotropic medication during pregnancy and lactation. Arch. Gynecol. Obstet. 2007, 277, 1–13. [Google Scholar] [CrossRef]
- Cipriani, A.; Barbui, C.; Salanti, G.; Rendell, J.; Brown, R.; Stockton, S.; Purgato, M.; Spineli, L.M.; Goodwin, G.M.; Geddes, J.R. Comparative efficacy and acceptability of antimanic drugs in acute mania: A multiple-treatments meta-analysis. Lancet 2011, 378, 1306–1315. [Google Scholar] [CrossRef]
- Ortega, M.A.; Fraile-Martinez, O.; García-Montero, C.; Rodriguez-Martín, S.; Funes Moñux, R.M.; Bravo, C.; De Leon-Luis, J.A.; Saz, J.V.; Saez, M.A.; Guijarro, L.G.; et al. Evidence of Increased Oxidative Stress in the Placental Tissue of Women Who Suffered an Episode of Psychosis during Pregnancy. Antioxidants 2023, 12, 179. [Google Scholar] [CrossRef]
- Overview|Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance|Guidance|NICE. NICE|The National Institute for Health and Care Excellence. Available online: https://www.nice.org.uk/guidance/cg192 (accessed on 5 December 2022).
- Perugi, G.; Medda, P.; Toni, C.; Mariani, M.G.; Socci, C.; Mauri, M. The Role of Electroconvulsive Therapy (ECT) in Bipolar Disorder: Effectiveness in 522 Patients with Bipolar Depression, Mixed-state, Mania and Catatonic Features. Curr. Neuropharmacol. 2017, 15, 359–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wesseloo, R.; Kamperman, A.M.; Munk-Olsen, T.; Pop, V.J.; Kushner, S.A.; Bergink, V. Risk of Postpartum Relapse in Bipolar Disorder and Postpartum Psychosis: A Systematic Review and Meta-Analysis. Am. J. Psychiatry 2016, 173, 117–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blackmore, E.R.; Rubinow, D.R.; O’Connor, T.G.; Liu, X.; Tang, W.; Craddock, N.; Jones, I. Reproductive outcomes and risk of subsequent illness in women diagnosed with postpartum psychosis. Bipolar Disord. 2013, 15, 394–404. [Google Scholar] [CrossRef] [Green Version]
- Ortega, M.A.; Fraile-Martinez, O.; García-Montero, C.; Moñux, R.M.F.; Rodriguez-Martín, S.; Bravo, C.; De Leon-Luis, J.A.; Saz, J.V.; Saez, M.A.; Guijarro, L.G.; et al. The Placentas of Women Who Suffer an Episode of Psychosis during Pregnancy Have Increased Lipid Peroxidation with Evidence of Ferroptosis. Biomolecules 2023, 13, 120. [Google Scholar] [CrossRef]
- Kendell, R.E.; Chalmers, J.C.; Platz, C. Epidemiology of Puerperal Psychoses. Br. J. Psychiatry 1987, 150, 662–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spinelli, M.G. Postpartum Psychosis: Detection of Risk and Management. Am. J. Psychiatry 2009, 166, 405–408. [Google Scholar] [CrossRef] [PubMed]
- Chandra, P.S.; Bhargavaraman, R.P.; Raghunandan, V.N.G.P.; Shaligram, D. Delusions related to infant and their association with mother–infant interactions in postpartum psychotic disorders. Arch. Women’s Ment. Health 2006, 9, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Gilden, J.; Kamperman, A.M.; Munk-Olsen, T.; Hoogendijk, W.J.G.; Kushner, S.A.; Bergink, V. Long-Term Outcomes of Postpartum Psychosis. J. Clin. Psychiatry 2020, 81, 10750. [Google Scholar] [CrossRef] [PubMed]
- Jones, I.; Chandra, P.S.; Dazzan, P.; Howard, L.M. Bipolar disorder, affective psychosis, and schizophrenia in pregnancy and the post-partum period. Lancet 2014, 384, 1789–1799. [Google Scholar] [CrossRef] [PubMed]
- González-Castro, P.; Hulak, F.; Sigales-Ruiz, S.; Orozco-Guzmán, M. Psicosis puerperal. Panorama general sobre su diagnóstico, etiología e interpretación. Perinatol. Reprod. Hum. 2016, 30, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Bergink, V.; Burgerhout, K.M.; Koorengevel, K.M.; Kamperman, A.M.; Hoogendijk, W.J.; Berg, M.P.L.-V.D.; Kushner, S.A. Treatment of Psychosis and Mania in the Postpartum Period. Am. J. Psychiatry 2015, 172, 115–123. [Google Scholar] [CrossRef]
- Leucht, S.; Corves, C.; Arbter, D.; Engel, R.R.; Li, C.; Davis, J.M. Second-generation versus first-generation antipsychotic drugs for schizophrenia: A meta-analysis. Lancet 2009, 373, 31–41. [Google Scholar] [CrossRef]
- Carbon, M.; Hsieh, C.-H.; Kane, J.M.; Correll, C.U. Tardive Dyskinesia Prevalence in the Period of Second-Generation Antipsychotic Use. J. Clin. Psychiatry 2017, 78, e264–e278. [Google Scholar] [CrossRef] [PubMed]
- Eberhard-Gran, M.; Eskild, A.; Opjordsmoen, S. Use of Psychotropic Medications in Treating Mood Disorders during Lactation. CNS Drugs 2006, 20, 187–198. [Google Scholar] [CrossRef]
- Alvarez-Mon, M.A.; Gómez-Lahoz, A.M.; Orozco, A.; Lahera, G.; Diaz, D.; Ortega, M.A.; Albillos, A.; Quintero, J.; Aubá, E.; Monserrat, J.; et al. Expansion of CD4 T Lymphocytes Expressing Interleukin 17 and Tumor Necrosis Factor in Patients with Major Depressive Disorder. J. Pers. Med. 2021, 11, 220. [Google Scholar] [CrossRef] [PubMed]
- Birnbaum, C.S.; Cohen, L.S.; Bailey, J.W.; Grush, L.R.; Robertson, L.M.; Stowe, Z.N. Serum Concentrations of Antidepressants and Benzodiazepines in Nursing Infants: A Case Series. Pediatrics 1999, 104, e11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sani, G.; Perugi, G.; Tondo, L. Treatment of Bipolar Disorder in a Lifetime Perspective: Is Lithium Still the Best Choice? Clin. Drug Investig. 2017, 37, 713–727. [Google Scholar] [CrossRef] [PubMed]
- Bergink, V.; Rasgon, N.; Wisner, K.L. Postpartum Psychosis: Madness, Mania, and Melancholia in Motherhood. Am. J. Psychiatry 2016, 173, 1179–1188. [Google Scholar] [CrossRef] [PubMed]
- Reed, P.; Sermin, N.; Appleby, L.; Faragher, B. A comparison of clinical response to electroconvulsive therapy in puerperal and non-puerperal psychoses. J. Affect. Disord. 1999, 54, 226–255. [Google Scholar] [CrossRef] [PubMed]
- Rundgren, S.; Brus, O.; Båve, U.; Landén, M.; Lundberg, J.; Nordanskog, P.; Nordenskjöld, A. Improvement of postpartum depression and psychosis after electroconvulsive therapy: A population-based study with a matched comparison group. J. Affect. Disord. 2018, 235, 258–264. [Google Scholar] [CrossRef]
- Jones, I.; Smith, S. Puerperal psychosis: Identifying and caring for women at risk. Adv. Psychiatr. Treat. 2009, 15, 411–418. [Google Scholar] [CrossRef]
- Bezerra, H.D.S.; Alves, R.M.; Nunes, A.D.D.S.; Barbosa, I.R. Prevalence and Associated Factors of Common Mental Disorders in Women: A Systematic Review. Public Health Rev. 2021, 42, 16. [Google Scholar] [CrossRef] [PubMed]
- Lassi, Z.S.; Imam, A.M.; Dean, S.V.; Bhutta, Z.A. Preconception care: Screening and management of chronic disease and promoting psychological health. Reprod. Health 2014, 11, S5. [Google Scholar] [CrossRef] [Green Version]
- Atif, N.; Nazir, H.; Zafar, S.; Chaudhri, R.; Atiq, M.; Mullany, L.C.; Rowther, A.A.; Malik, A.; Surkan, P.J.; Rahman, A. Development of a Psychological Intervention to Address Anxiety During Pregnancy in a Low-Income Country. Front. Psychiatry 2020, 10, 927. [Google Scholar] [CrossRef]
- Arango, C.; Díaz-Caneja, C.M.; McGorry, P.D.; Rapoport, J.; Sommer, I.E.; Vorstman, J.A.; McDaid, D.; Marín, O.; Serrano-Drozdowskyj, E.; Freedman, R.; et al. Preventive strategies for mental health. Lancet Psychiatry 2018, 5, 591–604. [Google Scholar] [CrossRef] [PubMed]
- Dimidjian, S.; Goodman, S. Nonpharmacologic Intervention and Prevention Strategies for Depression During Pregnancy and the Postpartum. Clin. Obstet. Gynecol. 2009, 52, 498–515. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Antepartum Psychosis | Puerperal Psychosis | References | |
|---|---|---|---|
| Incidence | 0.89 out of 1000 pregnant women | 1–2 women per 1000 deliveries | [10,11,31] |
| Associated psychiatric diseases | Mainly bipolar disorder | In all, 50% have no history of previous psychiatric illnesses. | [12,32] |
| Treatment | Second-generation antipsychotics, lithium or electroconvulsive therapy in refractory cases | Second-generation antipsychotics, lithium or electroconvulsive therapy in refractory cases | [27,28,29,30,41,42,43,44,45,46,47] |
| Prognosis | ~52% recurrence in women with bipolar disorder | If they have presented puerperal psychosis, they have a ~30% risk of recurrence in other pregnancies. Suicide risk of ~11% | [13,14,34,37] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega, M.A.; Pekarek, T.; Fraile-Martinez, O.; García-Montero, C.; Pekarek, L.; Rodriguez-Martín, S.; Funes Moñux, R.M.; Bravo, C.; De León-Luis, J.A.; Lahera, G.; et al. A Review: Integrative Perspectives on the Features and Clinical Management of Psychotic Episodes in Pregnancy. J. Clin. Med. 2023, 12, 656. https://doi.org/10.3390/jcm12020656
Ortega MA, Pekarek T, Fraile-Martinez O, García-Montero C, Pekarek L, Rodriguez-Martín S, Funes Moñux RM, Bravo C, De León-Luis JA, Lahera G, et al. A Review: Integrative Perspectives on the Features and Clinical Management of Psychotic Episodes in Pregnancy. Journal of Clinical Medicine. 2023; 12(2):656. https://doi.org/10.3390/jcm12020656
Chicago/Turabian StyleOrtega, Miguel A., Tatiana Pekarek, Oscar Fraile-Martinez, Cielo García-Montero, Leonel Pekarek, Sonia Rodriguez-Martín, Rosa M. Funes Moñux, Coral Bravo, Juan A. De León-Luis, Guillermo Lahera, and et al. 2023. "A Review: Integrative Perspectives on the Features and Clinical Management of Psychotic Episodes in Pregnancy" Journal of Clinical Medicine 12, no. 2: 656. https://doi.org/10.3390/jcm12020656