
Hypercalcemia Associated with Calcium Supplement Use: Prevalence and Characteristics in Hospitalized Patients

Abstract
:1. Introduction
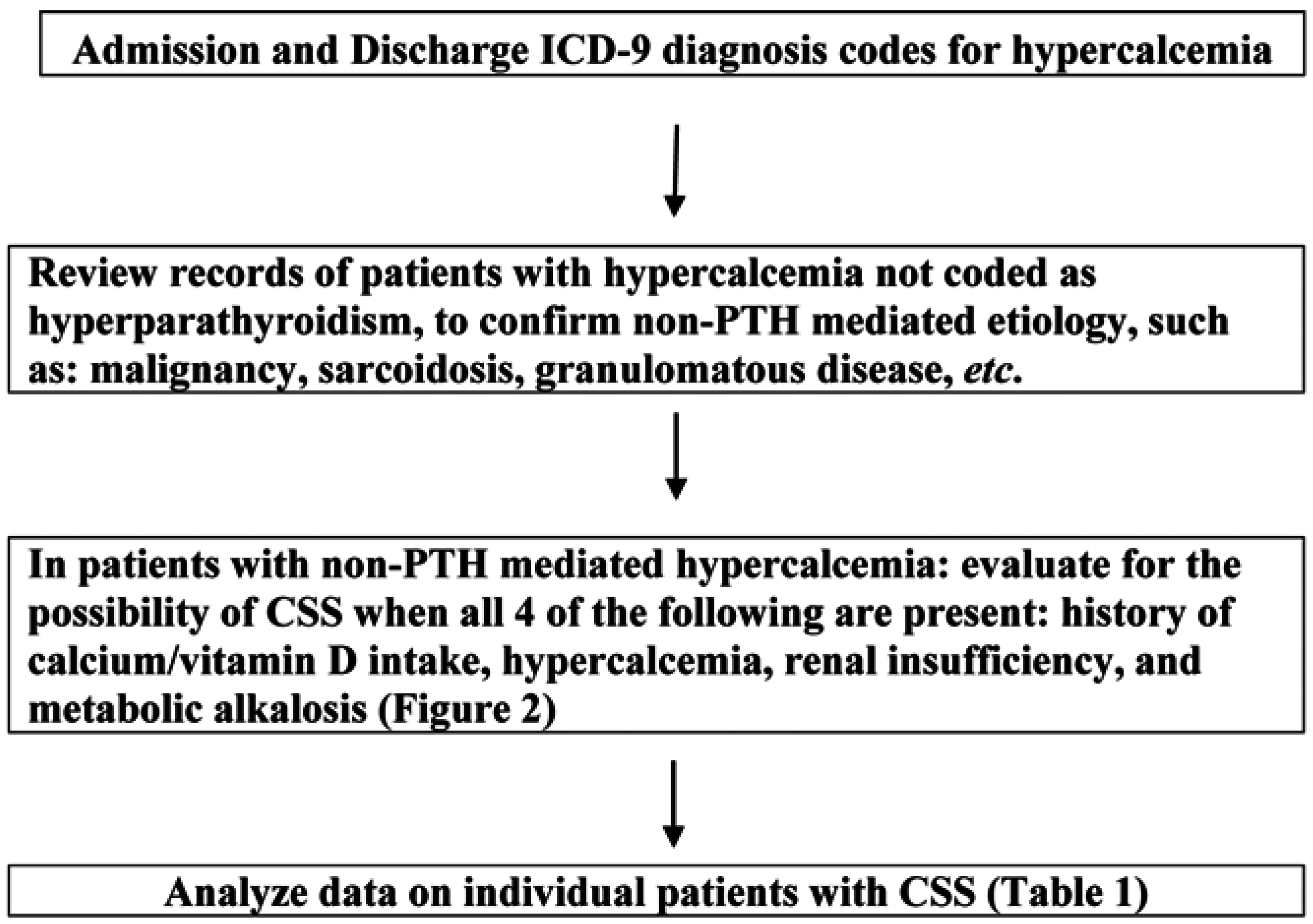
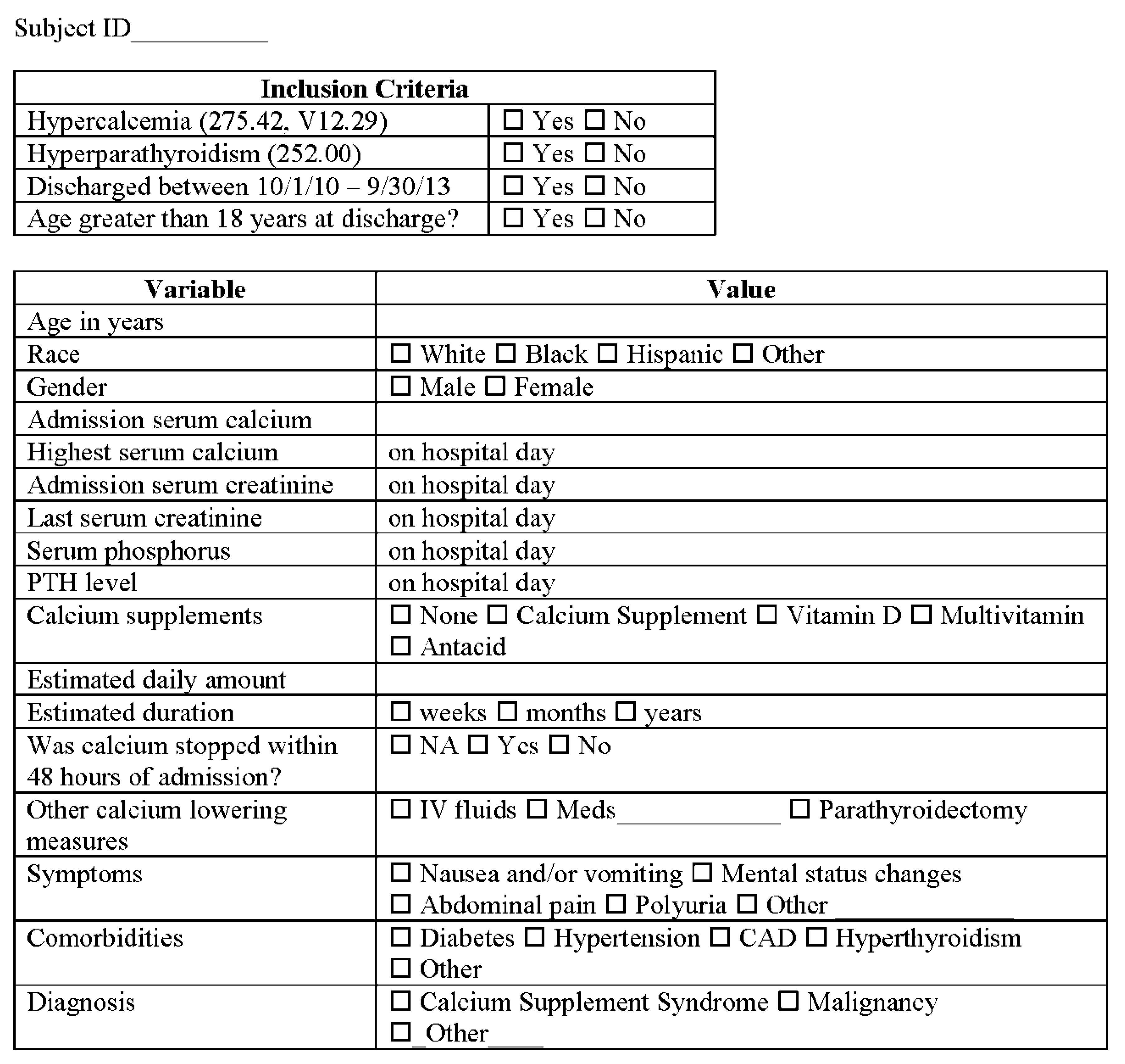
2. Aims and Methods
3. Data Analysis
4. Results



{kind=link}
{kind=link}
| No. | Age | Sex | Race | Medical Problems | Presenting Features | Meds | Supplements | Adm. Ca mg/dL | Last Ca mg/dL | PTH mg/mL | Ser. Cr mg/dL | Last Cr mg/dL | Bic mg/dL | Last Bic mg/dL | Ph mg/dL | Treatment |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 67 | M | B | hypertension | abdominal pain | Simvastatin aspirin | Calcium Vit D3 | 12.4 | 10.1 | 2.8 | 1.6 | 0.7 | 37 | 29 | 3.8 | IV fluids |
| 2 | 75 | F | W | Osteoporosis, hypertension | polyuria, weakness, bone pain | Lisinopril Metoprolol | Calcium 2 mg daily ibandronate | 16.2 | 8.8 | 12.5 | 2.2 | 0.9 | 37 | 23 | 2.8 | IV fluids, calcitonin |
| 3 | 74 | M | W | diabetes, hypertension, CAD renal insufficiency | mental status change, CVA | Metoprolol Lisinopril glipizide | calcium supplement multivitamin with mineral Vit D 1000 IU | 10.9 | 10.3 | 12.4 | 2.4 | 2.4 | 33 | 29 | 4.6 | IV fluids |
| 4 | 60 | M | B | hypertension | abdominal pain, abdominal swelling | Hydralazine testosterone | Calcium vitamin D 2000 IU per day | 10.7 | 10.3 | 21.7 | 3.9 | 1.9 | 37 | 17 | 3.3 | IV fluids |
| 5 | 86 | M | W | hypertension | abdominal pain, dehydration, weakness, back pain | Amlodipine Labetalol aspirin | Calcium multivitaminvit D | 11.3 | 10.1 | 4.1 | 2.1 | 1.6 | 32 | 27 | 2.1 | IV fluids |
| 6 | 73 | F | W | diabetes, hyperthyroidism | nausea and/or vomiting, cough, SOB | Methimazole metformin | calcium supplement Vit D multivitamin | 11.6 | 9.0 | <2.5 | 0.9 | 0.8 | 33 | 33 | 2.7 | IV fluids |
| 7 | 72 | F | W | diabetes, hypertension, CAD | generalized edema, chronic pain | Simvastatin furosemide | Calcium supplement | 13.8 | 10.4 | <2.5 | 2.6 | 1.5 | 38 | 26 | 2.7 | IV fluids, zoledronic acid |
| 8 | 54 | F | W | diabetes, hypertension, CAD renal insufficiency | abdominal pain, urinary retention, constipation | Nitroglycerin Amiodarone furosemide | TUMS antacid 4–6 mg per day | 14.1 | 8.8 | 2.8 | 2.1 | 2.1 | 37 | 25 | 4.1 | IV fluids, calcitonin |
| 9 | 77 | F | W | diabetes, hypertension | weakness | Insulin Losartan aspirin | Calcium multivitamin | 14.5 | 9.0 | 3.6 | 2.2 | 1.5 | 33 | 25 | 2.6 | IV fluids, calcitonin |
| 10 | 65 | M | W | diabetes, hypertension, CAD | nausea and/or vomiting, chest pain | Metformin glipizide Metoprolol mag ox | Multivitamin “large amount” of TUMS | 15.0 | 7.6 | 8.0 | 1.6 | 1.0 | 35 | 28 | 4.2 | IV fluids |
| 11 | 55 | F | W | diabetes, hypertension, renal insufficiency | nausea and/or vomiting, chills, dizziness | Insulin Enalapril Furosemide aspirin | Multivitamin Vit D antacid | 14.6 | 8.7 | 53.1 | 3.9 | 2.6 | 32 | 20 | 2.6 | IV fluids, calcitonin |
| 12 | 83 | F | W | hypertension | dyspnea, hypoxia | Atorvastatin Metoprolol Furosemide Hctz aspirin | calcium supplementmultivitamin Vit D | 13.7 | 7.7 | <2.5 | 1.4 | 1.0 | 43 | 30 | 2.7 | IV fluids |
| 13 | 60 | F | B | diabetes, hypertension | pain from wounds | Insulin Valproic acid | Calcium Vit D 50000 IU weekly | 13.8 | 9.1 | 7.8 | 2.7 | 1.1 | 33 | 24 | 4.1 | IV fluids, zoledronic acid |
| 14 | 68 | M | B | diabetes, hypertension renal insufficiency | hypercalcemia | Hydralazine Levothyroxine Lisinopril amlodipine | calcium supplement TUMS antacid Vit D | 12.7 | 9.3 | <2.5 | 3.6 | 3.2 | 33 | 23 | 3.5 | IV fluids |
| 15 | 87 | F | W | Hypertension Arthritis GERD Venous thromosis | encephalopathy, weakness, fatigue | Furosemide Amlodipine Warfarin albuterol | calcium supplemen Vit D 1000 IU multivitamin | 13.8 | 9.7 | <2.5 | 2.6 | 1.0 | 32 | 25 | 4.0 | IV fluids |
| Variable | CSS (N = 15) n (%) | Non-CSS (N = 57) n (%) | p-Value |
|---|---|---|---|
| Gender (Female) | 9 (60.0) | 24 (42.1) | 0.216 |
| Calcium Intake | 12 (80.0) | 8 (14.0) | <0.0001 |
| Vitamin D Intake | 9 (60.0) | 15 (26.3) | 0.014 |
| Multivitamin Use | 7 (46.7) | 12 (21.1) | 0.045 |
| Hypertension | 14 (93.3) | 39 (68.4) | 0.051 |
| Diabetes | 9 (60.0) | 21 (36.84) | 0.106 |
| Renal insufficiency (serum creatinine above 1.3 mg/dL) | 14 (93.3) | 44 (77.2) | 0.160 |
5. Discussion
| Milk-Alkali Syndrome | Calcium Supplement Syndrome | |
|---|---|---|
| Patient population | Middle-aged men | Older women |
| Symptoms | Present | Asymptomatic |
| Presentation | Acute: nausea, vomiting, weakness, mental status changes | Hypercalcemia and renal insufficiency are incidental findings |
| Chronic: polyuria, polydipsia, muscle aches | ||
| Phosphorus level | Normal or high due to phosphate load from milk | Low from lack of milk load and the binding properties of calcium carbonate |
| Post-treatment hypocalcemia | Not usually seen | May develop |
| Prognosis | Variable | Complete recovery with treatment (insufficient data) |
6. Conclusions
Author Contributions
Conflicts of Interest
References
- Burnett, C.H.; Commons, R.R. Hypercalcemia without hypercalcuria or hypophosphatemia, calcinosis and renal insufficiency; a syndrome following prolonged intake of milk and alkali. N. Engl. J. Med. 1949, 240, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Orwoll, E.S. The milk-alkali syndrome: Current concepts. Ann. Intern. Med. 1982, 97, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, M.J. Hypercalcaemia. Br. Med. J. (Clin. Res. Ed.) 1985, 290, 378–382. [Google Scholar] [CrossRef]
- McGuinness, B.; Logan, J.I. Milk alkali syndrome. Ulster Med. J. 2002, 71, 132–135. [Google Scholar] [PubMed]
- Beall, D.P.; Henslee, H.B.; Webb, H.R.; Scofield, R.H. Milk-alkali syndrome: A historical review and description of the modern version of the syndrome. Am. J. Med. Sci. 2006, 331, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.M.; Goldfarb, S. Got calcium? Welcome to the calcium-alkali syndrome. J. Am. Soc. Nephrol. 2010, 21, 1440–1443. [Google Scholar] [CrossRef] [PubMed]
- Beall, D.P.; Scofield, R.H. Milk-alkali syndrome associated with calcium carbonate consumption. Report of 7 patients with parathyroid hormone levels and an estimate of prevalence among patients hospitalized with hypercalcemia. Medicine (Baltimore) 1995, 74, 89–96. [Google Scholar] [CrossRef]
- Caruso, J.B.; Patel, R.M.; Julka, K.; Parish, D.C. Health-behavior induced disease: Return of the milk-alkali syndrome. J. Gen. Intern. Med. 2007, 22, 1053–1055. [Google Scholar] [CrossRef] [PubMed]
- Picolos, M.K.; Lavis, V.R.; Orlander, P.R. Milk-alkali syndrome is a major cause of hypercalcaemia among non-end-stage renal disease (non-ESRD) inpatients. Clin. Endocrinol. (Oxf.) 2005, 63, 566–576. [Google Scholar] [CrossRef]
- Abreo, K.1.; Adlakha, A.; Kilpatrick, S.; Flanagan, R.; Webb, R.; Shakamuri, S. The milk-alkali syndrome. A reversible form of acute renal failure. Arch. Intern. Med. 1993, 153, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Satoh, F.; Okado, T.; Iwamoto, M.; Akita, W.; Wakabayashi, M.; Ohta, A.; Sohara, E.; Noda, Y.; Rai, T.; Uchida, S.; Sasaki, S. Calcium-alkali syndrome-like symptoms manifested by daily alphacalcidol and thiazide. Intern. Med. 2010, 49, 837–840. [Google Scholar] [CrossRef] [PubMed]
- Picolos, M.K.; Orlander, P.R. Calcium carbonate toxicity: The updated milk-alkali syndrome; report of 3 cases and review of the literature. Endocr. Pract. 2005, 11, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Bailey, C.S.; Weiner, J.J.; Gibby, O.M.; Penney, M.D. Excessive calcium ingestion leading to milk-alkali syndrome. Ann. Clin. Biochem. 2008, 45, 527–529. [Google Scholar] [CrossRef] [PubMed]
- Felsenfeld, A.J.; Levine, B.S. Milk alkali syndrome and the dynamics of calcium homeostasis. Clin. J. Am. Soc. Nephrol. 2006, 1, 641–654. [Google Scholar] [CrossRef] [PubMed]
- Broadus, A.E.; Insogna, K.L.; Lang, R.; Ellison, A.F.; Dreyer, B.E. Evidence for disordered control of 1,25-dihydroxyvitamin D production in absorptive hypercalciuria. N. Engl. J. Med. 1984, 311, 73–80. [Google Scholar] [CrossRef] [PubMed]
- McMillan, D.E.; Freeman, R.B. The milk alkali syndrome: A study of the acute disorder with comments on the development of the chronic condition. Medicine (Baltimore) 1965, 44, 485–501. [Google Scholar] [CrossRef]
- Sutton, R.A.; Wong, N.L.; Dirks, J.H. Effects of metabolic acidosis and alkalosis on sodium and calcium transport in the dog kidney. Kidney Int. 1979, 15, 520–533. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machado, M.C.; Bruce-Mensah, A.; Whitmire, M.; Rizvi, A.A. Hypercalcemia Associated with Calcium Supplement Use: Prevalence and Characteristics in Hospitalized Patients. J. Clin. Med. 2015, 4, 414-424. https://doi.org/10.3390/jcm4030414
Machado MC, Bruce-Mensah A, Whitmire M, Rizvi AA. Hypercalcemia Associated with Calcium Supplement Use: Prevalence and Characteristics in Hospitalized Patients. Journal of Clinical Medicine. 2015; 4(3):414-424. https://doi.org/10.3390/jcm4030414
Chicago/Turabian StyleMachado, Maria C., Araba Bruce-Mensah, Melanie Whitmire, and Ali A. Rizvi. 2015. "Hypercalcemia Associated with Calcium Supplement Use: Prevalence and Characteristics in Hospitalized Patients" Journal of Clinical Medicine 4, no. 3: 414-424. https://doi.org/10.3390/jcm4030414