The Role of Ranolazine for the Treatment of Residual Angina beyond the Percutaneous Coronary Revascularization

 ,
,
Abstract
:1. Introduction
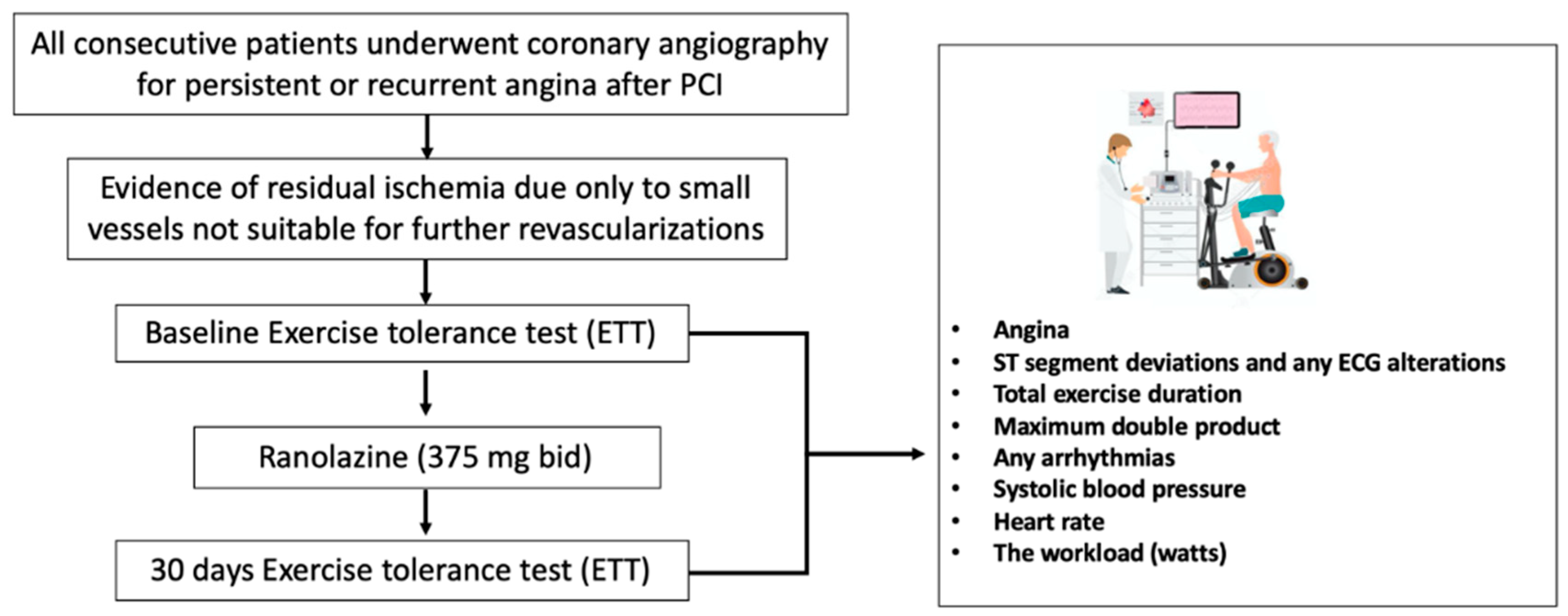
2. Study Population
2.1. Study Design
2.2. Exercise ECG Test (EET)
2.3. Endpoint
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Montalescot, G.; Sechtem, U.; Achenbach, S.; Andreotti, F.; Arden, C.; Budaj, A.; Bugiardini, R.; Crea, F.; Cuisset, T.; Di Mario, C.; et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur. Heart J. 2013, 34, 2949–3003. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Sardella, G.; Stefanini, G.G.; Briguori, C.; Tamburino, C.; Fabbiocchi, F.; Rotolo, F.; Tomai, F.; Paggi, A.; Lombardi, M.; Gioffrè, G.; et al. Safety and efficacy of polymer-free biolimus-eluting stents in all-comer patients: The RUDI-FREE study. EuroIntervention J. Eur. Collab. Work Group Interv. Cardiol. Eur. Soc. Cardiol. 2018, 14, 772–779. [Google Scholar] [CrossRef] [PubMed]
- Chiarito, M.; Sardella, G.; Colombo, A.; Briguori, C.; Testa, L.; Bedogni, F.; Fabbiocchi, F.; Paggi, A.; Palloshi, A.; Tamburino, C.; et al. Safety and Efficacy of Polymer-Free Drug-Eluting Stents. Circ. Cardiovasc Interv. 2019, 12, e007311. [Google Scholar] [CrossRef]
- Gaglia, M.A.; Torguson, R.; Lipinski, M.J.; Gai, J.; Koifman, E.; Kiramijyan, S.; Negi, S.; Rogers, T.; Steinvil, A.; Suddath, W.O.; et al. Frequency of Angina Pectoris After Percutaneous Coronary Intervention and the Effect of Metallic Stent Type. Am. J. Cardiol. 2016, 117, 526–531. [Google Scholar] [CrossRef]
- Sardella, G.; Stella, P.; Chiarito, M.; Leone, A.M.; Balian, V.; Prosperi, F.; Sorropago, G.; Mancone, M.; Calcagno, S.; Briguori, C.; et al. Clinical outcomes with reservoir-based polymer-free amphilimus-eluting stents in real-world patients according to diabetes mellitus and complexity: The INVESTIG8 registry. Catheter. Cardiovasc. Interv. Off. J. Soc. Cardiovasc. Angiogr. Interv. 2018, 91, 884–891. [Google Scholar] [CrossRef]
- Sardella, G.; Mancone, M.; Stio, R.E.; Cavallo, E.; Di Roma, A.; Colantonio, R.; Calcagno., S. Prasugrel or Ticagrelor in ST-Segment-Elevation Myocardial Infarction Patients with Diabetes Mellitus. Circulation 2017, 136, 602–604. [Google Scholar] [CrossRef]
- Codolosa, J.N.; Acharjee, S.; Figueredo, V.M. Update on ranolazine in the management of angina. Vasc. Health Risk Manag. 2014, 10, 353–362. [Google Scholar] [CrossRef] [Green Version]
- Cattaneo, M.; Porretta, A.P.; Gallino, A. Ranolazine: Drug overview and possible role in primary microvascular angina management. Int. J. Cardiol. 2015, 181, 376–381. [Google Scholar] [CrossRef]
- Wenger, N.K.; Chaitman, B.; Vetrovec, G.W. Gender comparison of efficacy and safety of ranolazine for chronic angina pectoris in four randomized clinical trials. Am. J. Cardiol. 2007, 99, 11–18. [Google Scholar] [CrossRef]
- Savarese, G.; Rosano, G.; D’Amore, C.; Musella, F.; Della Ratta, G.L.; Pellegrino, A.M.; Formisano, T.; Vitagliano, A.; Cirillo, A.; Cice, G.; et al. Effects of ranolazine in symptomatic patients with stable coronary artery disease. A systematic review and meta-analysis. Int J. Cardiol. 2013, 169, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Calcagno, S.; Infusino, F.; Dettori, O.; Taccheri, T.; Bruno, P.; Maestrini, V.; Sardella, G.; Mancone, M.; Fedele, F. Effects of Ivabradine on Residual Myocardial Ischemia after PCI Evaluated by Stress Echocardiography. Cardiol. Res. Pract. 2019, 2019, 9185876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexander, K.; Weisz, G.; Prather, K.; James, S.; Mark, D.B.; Anstrom, K.J.; Davidson-Ray, L.; Witkowski, A.; Mulkay, A.J.; Osmukhina, A.; et al. Effects of Ranolazine on Angina and Quality of Life after Percutaneous Coronary Intervention With Incomplete Revascularization: Results From the Ranolazine for Incomplete Vessel Revascularization (RIVER-PCI) Trial. Circulation 2016, 133, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Weisz, G.; Généreux, P.; Iñiguez, A.; Zurakowski, A.; Shechter, M.; Alexander, K.; Dressler, O.; Osmukhina, A.; James, S.; Ohman, E.M.; et al. Ranolazine in patients with incomplete revascularisation after percutaneous coronary intervention (RIVER-PCI): A multicentre, randomised, double-blind, placebo-controlled trial. Lancet Lond. Engl. 2016, 387, 136–145. [Google Scholar] [CrossRef]
- Belsey1, J.; Savelieva, I.; Mugelli, A.; Camm, A.J. Relative efficacy of antianginal drugs used as add-on therapy in patients with stable angina: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2015, 22, 837–848. [Google Scholar] [CrossRef]
- Briguori, C.; Donahue, M.; Visconti, G.; Focaccio, A.; Pennacchi, M.; Lucisano, L.; Stio, R.; Mancone, M.; Calcagno, S.; Di Palma, V.; et al. Coronary artery bifurcation narrowing treated by Axxess stent implantation: The CARINAX registry. Catheter. Cardiovasc. Interv Off. J. Soc. Cardiovasc. Angiogr. Interv. 2017, 89, 112–123. [Google Scholar] [CrossRef]
- Lucisano, L.; Pennacchi, M.; Stio, R.E.; Calcagno, S.; Mancone, M.; Sardella, G. Do angle and anatomy influence outcomes in bifurcation stenting? Minerva Cardioangiol. 2013, 61, 61–70. [Google Scholar]
- Jetté, M.; Sidney, K.; Blümchen, G. Metabolic equivalents (METS) in exercise testing, exercise prescription, and evaluation of functional capacity. Clin. Cardiol. 1990, 13, 555–565. [Google Scholar] [CrossRef]
- Niccoli, G.; Montone, R.A.; Lanza, G.A.; Crea, F. Angina after percutaneous coronary intervention: The need for precision medicine. Int. J. Cardiol. 2017, 248, 14–19. [Google Scholar] [CrossRef]
- Rayner-Hartley, E.; Parvand, M.; Humphries, K.H.; Starovoytov, A.; Park, J.E.; Sedlak, T. Ranolazine for Symptomatic Management of Microvascular Angina. Am. J. Ther. 2018. [Google Scholar] [CrossRef]
- Zhu, H.; Xu, X.; Fang, X.; Zheng, J.; Zhao, Q.; Chen, T.; Huang, J. Effects of the Antianginal Drugs Ranolazine, Nicorandil, and Ivabradine on Coronary Microvascular Function in Patients with Nonobstructive Coronary Artery Disease: A Meta-analysis of Randomized Controlled Trials. Clin. Ther. 2019, 41, 2137–2152. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, B.; Mondragon, J.; Sheldon, M.; Clegg, S. Impact of ranolazine on coronary microvascular dysfunction (MICRO) study. Cardiovasc. Revascularization Med. Mol. Interv. 2017, 18, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Safdar, B.; D’Onofrio, G.; Dziura, J.; Russell, R.R.; Johnson, C.; Sinusas, A.J. Ranolazine and Microvascular Angina by PET in the Emergency Department: Results from a Pilot Randomized Controlled Trial. Clin. Ther. 2017, 39, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Population (N = 49) | |
|---|---|
| Age (years) ± SD | 62.6 ± 11.2 |
| Gender (male) | 44 (89.8%) |
| Height (cm) ± SD | 172.2 ± 7.02 |
| Previous AMI | 25 (51.1%) |
| Previous CABG | 18 (36.7%) |
| Hypertension | 29 (59.2%) |
| Smoker | 32 (65.3%) |
| Familiarity | 22 (44.8%) |
| Dyslipidaemia | 32 (65.3%) |
| Diabetes Mellitus II | 9 (18.3%) |
| Stroke/TIA | 4 (8.1%) |
| Chronic Renal failure | 3 (6.1%) |
| Ejection Fraction (%) ± SD | 48.3 ± 5.7 |
| WMSI ± dS | 1.3 ± 0.39 |
| End-diastolic diameter (mm) ± SD | 51.7 ± 5.2 |
| End-systolic diameter (mm) ± SD | 37 ± 3.6 |
| Population (N = 49) | |
|---|---|
| Acetylsalicylic acid (ASA) | 47 (95.9%) |
| Clopidogrel | 29 (59.2%) |
| Prasugrel | 13 (26.5%) |
| Ticagrelor | 4 (8.1%) |
| Beta-blockers | 41 (83.7%) |
| Nitrates | 33 (67.3%) |
| Calcium channel blockers | 4 (8.1%) |
| ACE inhibitors | 41 (83.7%) |
| Angiotensin receptor Antagonists | 9 (18.3%) |
| Statins | 44 (89.8%) |
| BL (N = 49) | T1 (N = 49) | Mean Difference (CI 95%) | p | |
|---|---|---|---|---|
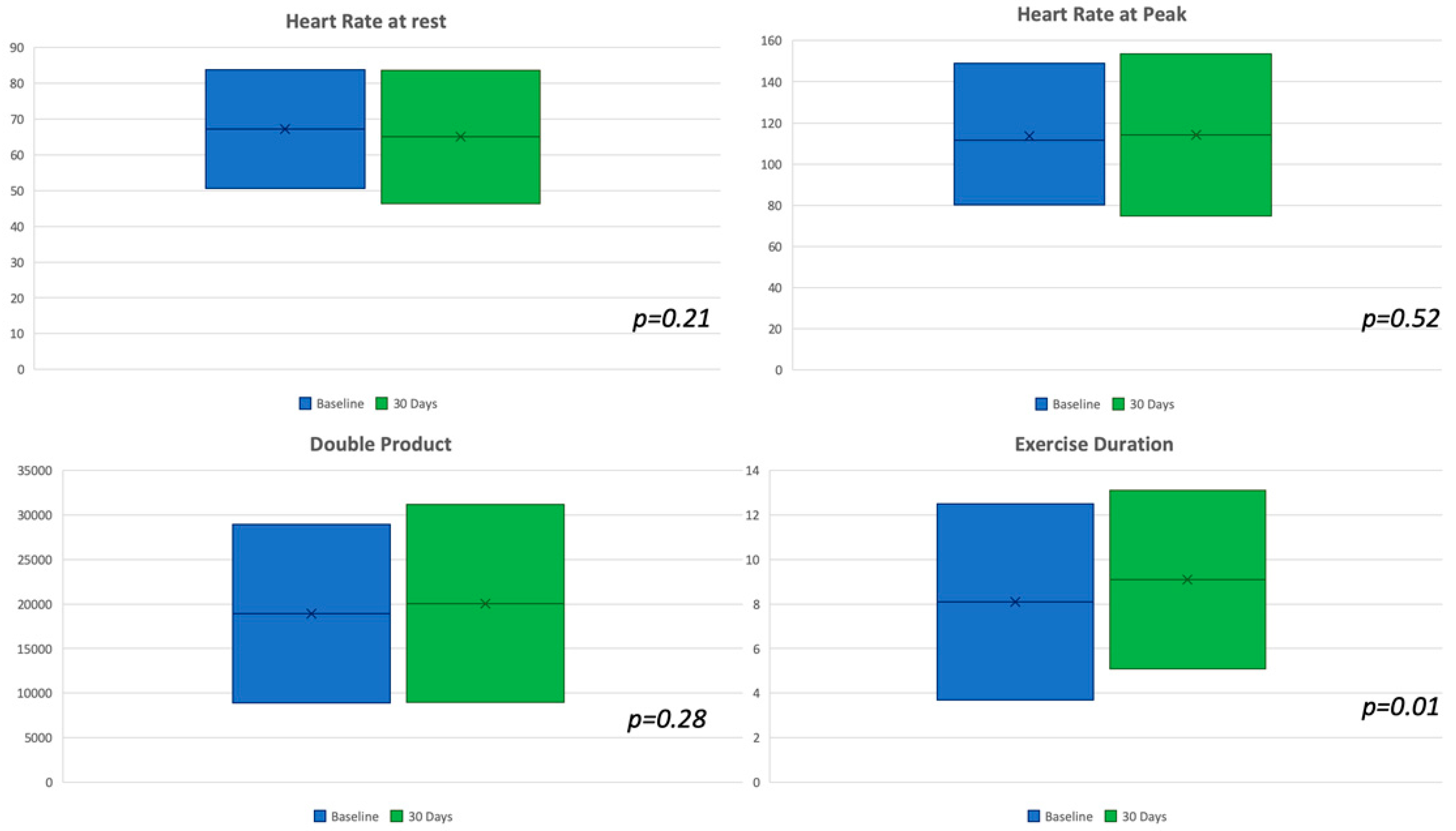
| Heart rate at rest (bpm) ± SD | 67.2 ± 8.3 | 65.0 ± 9.3 | 2.2 (CI: −1.33 to 5.73) | 0.21 |
| Heart rate at peak (bpm) ± SD | 111.7 ± 18.7 | 114.2 ± 19.7 | −2.5 (CI −10.20 to 5.20) | 0.52 |
| Systolic blood pressure at rest (mmHg) ± SD | 119.5 ± 15.2 | 125.9 ± 14.9 | −6.4 (CI: −12.44 to −0.36) | 0.03 |
| Diastolic blood pressure at rest (mmHg) ± SD | 78.5 ± 14.2 | 75.6 ± 8.9 | 2.9 (CI: −1.85 to 7.65) | 0.22 |
| Systolic blood pressure at peak (mmHg) ± SD | 167.9 ± 23.9 | 176.4 ± 22.7 | −8.5 (CI: −56.54 to 39.54) | 0.07 |
| Diastolic blood pressure at peak (mmHg) ± SD | 94.3 ± 21.6 | 90.4 ± 22.7 | 3.9 (CI: −4.98 to 12.78) | 0.38 |
| Double product (SBP x HR at peak) | 18,913 ± 5008.4 | 20,066 ± 5548.9 | −1153 (CI: −3272.6 to 966.6) | 0.28 |
| Exercise duration (min) ± SD | 8’1” ± 2’2” | 9’1” ± 2’0” | 1’ (CI: −1.84 to −0.15) | 0.01 |
| Odds Ratio (CI 95%) | ||||
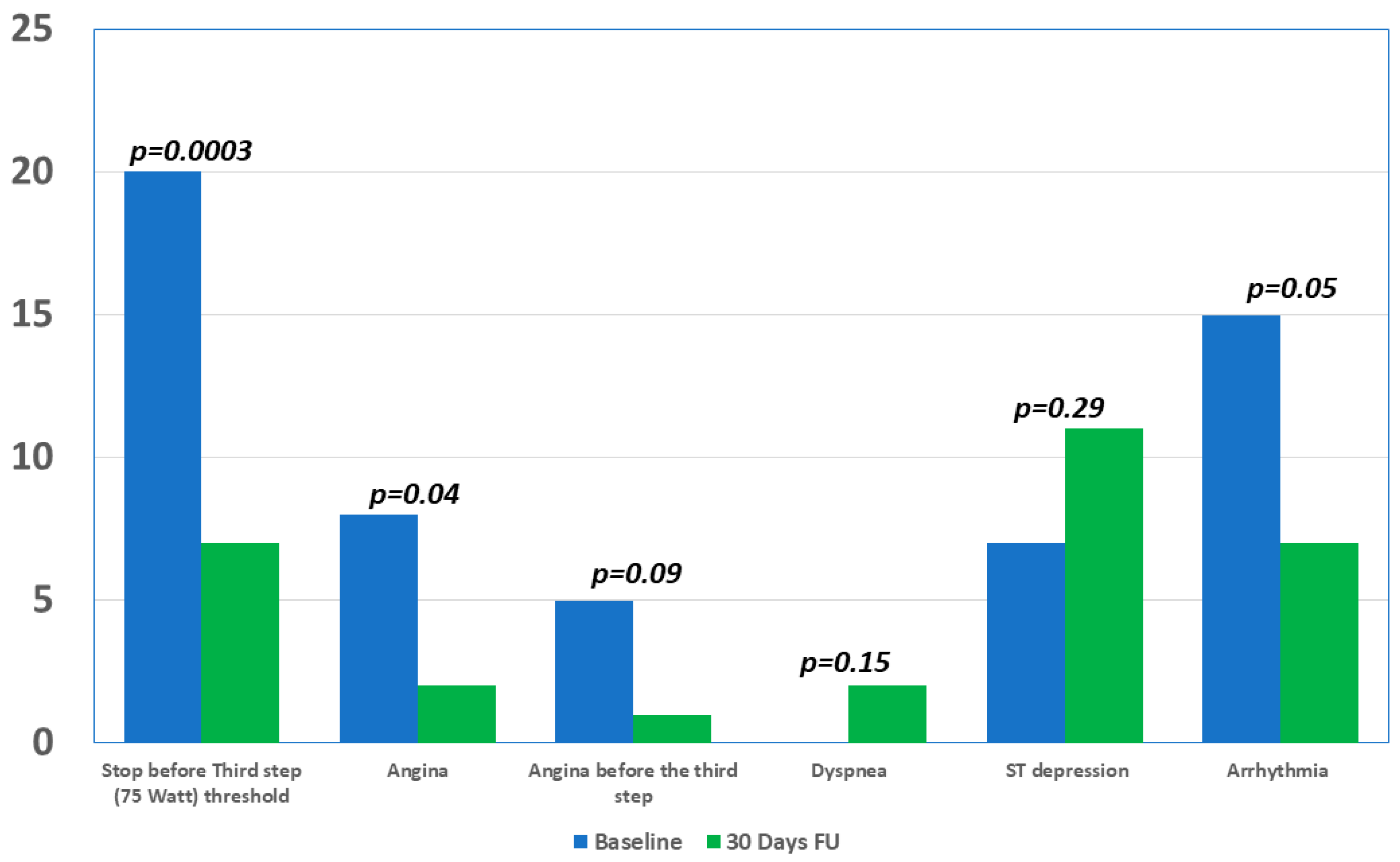
| Stop before third step (75 Watt)threshold | 20 (40.8%) | 7 (14.3%) | 0.24 (CI: 0.09 to 0.64) | 0.0003 |
| Angina | 8 (16.3 %) | 2 (4.1%) | 0.21 (CI: 0.043 to 1.08) | 0.04 |
| Angina before the third step | 5 (10.2%) | 1 (2.0%) | 0.18 (CI: 0.0206 to 1.63) | 0.09 |
| Dyspnea | 0 (0.0%) | 2 (4.1%) | 0.15 | |
| ST depression | 7 (14.3%) | 11 (22.4%) | 1.73 (CI: 0.6113 to 4.93) | 0.29 |
| Arrhythmia | 15 (30.6%) | 7 (14.3%) | 0.37 (CI: 0.1383 to 1.03) | 0.05 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calcagno, S.; Infusino, F.; Salvi, N.; Taccheri, T.; Colantonio, R.; Bruno, E.; Birtolo, L.I.; Severino, P.; Lavalle, C.; Pucci, M.; et al. The Role of Ranolazine for the Treatment of Residual Angina beyond the Percutaneous Coronary Revascularization. J. Clin. Med. 2020, 9, 2110. https://doi.org/10.3390/jcm9072110
Calcagno S, Infusino F, Salvi N, Taccheri T, Colantonio R, Bruno E, Birtolo LI, Severino P, Lavalle C, Pucci M, et al. The Role of Ranolazine for the Treatment of Residual Angina beyond the Percutaneous Coronary Revascularization. Journal of Clinical Medicine. 2020; 9(7):2110. https://doi.org/10.3390/jcm9072110
Chicago/Turabian StyleCalcagno, Simone, Fabio Infusino, Nicolò Salvi, Temistocle Taccheri, Riccardo Colantonio, Emanuele Bruno, Lucia Ilaria Birtolo, Paolo Severino, Carlo Lavalle, Mariateresa Pucci, and et al. 2020. "The Role of Ranolazine for the Treatment of Residual Angina beyond the Percutaneous Coronary Revascularization" Journal of Clinical Medicine 9, no. 7: 2110. https://doi.org/10.3390/jcm9072110