Application of Anti-Inflammatory Agents in Prostate Cancer


1
Department of Urology, Osaka University Graduate School of Medicine, Suita, Osaka 565-0871, Japan
2
Department of Urology, Kindai University Faculty of Medicine, Osakasayama, Osaka 589-8511, Japan
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2020, 9(8), 2680; https://doi.org/10.3390/jcm9082680
Submission received: 29 June 2020
/
Revised: 14 August 2020
/
Accepted: 17 August 2020
/
Published: 18 August 2020
(This article belongs to the Special Issue The Application of Anti-inflammatory Agents in Prostate Cancer)
Abstract
:Chronic inflammation is a major cause of human cancers. The environmental factors, such as microbiome, dietary components, and obesity, provoke chronic inflammation in the prostate, which promotes cancer development and progression. Crosstalk between immune cells and cancer cells enhances the secretion of intercellular signaling molecules, such as cytokines and chemokines, thereby orchestrating the generation of inflammatory microenvironment. Tumor-associated macrophages (TAMs) and myeloid-derived suppressor cells (MDSCs) play pivotal roles in inflammation-associated cancer by inhibiting effective anti-tumor immunity. Anti-inflammatory agents, such as aspirin, metformin, and statins, have potential application in chemoprevention of prostate cancer. Furthermore, pro-inflammatory immunity-targeted therapies may provide novel strategies to treat patients with cancer. Thus, anti-inflammatory agents are expected to suppress the “vicious cycle” created by immune and cancer cells and inhibit cancer progression. This review has explored the immune cells that facilitate prostate cancer development and progression, with particular focus on the application of anti-inflammatory agents for both chemoprevention and therapeutic approach in prostate cancer.
1. Introduction
Chronic inflammation plays a major role in the etiology and development of various types of malignant tumors, including hepatocellular carcinoma, gastric cancer, lung cancer, colorectal cancer, and prostate cancer [1,2,3,4,5]. Although inherited germline mutations are involved in prostate cancer development [6,7], immigration studies indicate the importance of environmental factors; for instance, it was found that immigrants from Asian countries in Western countries acquired higher prostate cancer risks within one generation [8,9]. The exposure to environmental factors, such as microbiome, cellular trauma, hormonal imbalances, dietary carcinogens, and obesity, leads to prostate epithelium injury and causes chronic inflammation [3,10,11,12]. In the adult prostate, chronic inflammation is prevalent and associated with putative precursor lesions that can provoke prostate cancer development [13,14,15,16].
A meta-analysis revealed an increased risk of prostate cancer among men with a history of prostatitis, syphilis, and gonorrhea [17]. Although a number of studies supported the idea of a connection between prostatitis and prostate cancer risk [18,19,20,21,22], subsequence studies revealed conflicting results [23,24,25,26,27]. The inconsistent results could be attributed to differences in the study population and potential selection bias, as acute and chronic prostatitis is associated with increased serum prostate-specific antigen (PSA) levels [28]. Previous epidemiological studies focused on the relationship between inflammation and prostate cancer development [29,30,31]. The first prospective study in men without biopsy indication revealed that benign tissue inflammation was positively associated with prostate cancer development [32]. Furthermore, the progression and aggressiveness of prostate cancer was reportedly associated with systemic inflammation markers in the serum, such as C-reactive protein levels, as well as differential blood cell count (neutrophils, lymphocytes, monocytes, and platelets) [33,34,35,36,37].
The pathogenesis of inflammation-associated cancer is complex as both the innate and adaptive immune systems are involved in the process [38,39,40]. Chronic inflammation in the prostate microenvironment causes chronic increase in reactive oxygen species, which is associated with oxidative DNA damage in prostate epithelium [41]. Accumulated DNA damage can cause somatic mutations in key tumor suppressor genes and induce genome instability resulting in genomic changes in oncogenes, thus facilitating the development and progress of prostate cancer [3,42,43]. In fact, in patients with castration-resistant prostate cancer (CRPC), aberrations of AR (androgen receptor), E26 transformation-specific genes, TP53 (tumor protein p53), and PTEN (phosphatase and tensin homolog) were frequently observed (40–60% of cases), whereas only few (8%) cases had pathogenic germline alterations [44]. Additionally, inflammatory cells also secrete cytokines and chemokines that stimulate prostate cancer growth, angiogenesis, invasion, and metastasis [45,46,47]. Thus, anti-inflammatory agents are expected to suppress inflammation in the tumor microenvironment and inhibit prostate cancer progression (Figure 1). In this article, we have reviewed the immune cells that facilitate prostate cancer development and progression, and especially focused on the application of anti-inflammatory agents for both chemoprevention and therapeutic approach in prostate cancer.
2. Immune Cells Involved in Inflammation and Prostate Cancer Progression
Cancer development and its response to therapy are strongly affected by innate and adaptive immunity, which either promote or attenuate tumorigenesis and can have opposing effects on therapeutic outcome [48]. A large number of studies have focused on immune cells in prostate cancer, including innate immune cells: Macrophages, neutrophils, and mast cells; adaptive immune cells: T cells and B cells; and immune-suppressive cells: regulatory T cells (Treg cells) and myeloid-derived suppressor cells (MDSCs) [49]. In the prostate microenvironment, these immune cells act as either friends or foes [50]. Growing evidence suggests that both macrophages and MDSCs play pivotal roles in inflammation-associated prostate cancer development and progression via down-regulation of effective anti-tumor immunity (Figure 2). Although the precise molecular mechanisms involved are still unclear, animal models of prostate cancer, which mimic the human disease, have contributed to the determination of specific pathways and helped develop novel therapeutic agents.
2.1. Macrophages
Tumor-associated macrophages (TAMs) are crucial drivers of tumor promoting inflammation and are generally associated with poor prognosis in solid tumors [51], including prostate cancer [52,53,54,55,56,57,58]. TAMs contribute to tumor progression at different levels by promoting genetic instability, cell proliferation, angiogenesis, and metastasis, as well as suppressing protective adaptive immunity [59,60,61,62,63]. Historically, macrophages are divided into classically activated macrophages (M1) and alternatively activated macrophages (M2), exhibiting anti-tumoral and pro-tumoral properties, respectively. Although interleukin (IL)-4 and IL-13 are the acknowledged signals that regulate M2 polarization of macrophages, recently other subtypes of the M2 class have been identified [64,65,66,67]. Thus, TAM population is referred to as “M2-like” when they include diverse phenotypes that share the functional outputs of tumor promotion and adaptive immunity suppression; these typically express characteristic surface molecules, such as CD163, CD204, and CD206 [62].
Furthermore, elements within the tumor microenvironment, such as hypoxia, fibrosis, cellular stress, and inflammation, dramatically shift the macrophage polarity towards M2-like phenotypes [68,69,70] (Figure 2). Many studies have shed light on the complex signaling network that drives myeloid cells toward M2-like TAMs, which involves various cytokines, chemokines, and signals within the tumor microenvironment [71], including prostaglandin E2 (PGE2) [72], chemokine (C–C motif) ligand (CCL)2 [73], colony stimulating factor (CSF)-1 [74], C–X–C motif chemokine (CXCL)12, and IL-6 [75,76]. Thus, tumor microenvironment can influence TAM polarization by releasing various factors that give rise to a large spectrum of pro-tumoral TAMs [77]. TAMs inhibit effector T cells by secreting IL-10, transforming growth factor (TGF)-β, and arginase (ARG)1 as well as via direct cell to cell contact. They also induce Treg cells via IL-10 and TGF-β [78,79] (Figure 2). Therefore, TAMs can be potential therapeutic targets, and re-education of pro-tumoral M2-like TAMs toward anti-tumorigenic phenotype may be a potent strategy to treat prostate cancer [80,81].
2.2. MDSCs
MDSCs are a tolerogenic and immune-suppressive population of myeloid cells that are significantly expanded in patients with various types of cancers. High MDSC number negatively correlates with disease progression and overall survival, thus suggesting these to be a possible target for cancer immunotherapy [82,83]. MDSCs have distinct phenotypic surface markers as well as functional characteristics, particularly T cell activity inhibition. MDSCs were originally identified in mice as Gr-1+ CD11b+ cells [84,85]. The Gr-1 marker is not a singular molecule, but a combination of Ly6C and Ly6G markers. Currently, MDSCs include two major subsets based on their phenotypic and morphological features: Polymorphonuclear (PMN)-MDSCs, including CD11b+ Ly6Clo Ly6G+ cells, and monocytic (M)-MDSCs, including CD11b+ Ly6Chi Ly6G− cells. In humans, PMN-MDSC equivalent cells are defined as CD11b+ CD14− CD15+ or CD11b+ CD14− CD66b+ and M-MDSCs as CD11b+ CD14+ HLA-DRlow/− CD15− [86]. Growing evidence suggests that MDSCs play an important role in cancer development and progression via suppression of anti-tumoral T cell function in patients with prostate cancer [87,88,89,90,91,92]. However, the MDSC subsets that have clinical relevance during disease progression remain to be identified.
To date, various signaling pathways, including PGE2 [93], CCL2 [94,95], CSF-1 [96], TGF-β [97], CXCL5, CXCL12 [98], IL-1β [99,100], and IL-6 [101], have been identified to be involved in the infiltration and activation of MDSCs in tumor microenvironment [102,103,104,105,106]. MDSCs suppress anti-tumor immunity through a variety of diverse mechanisms, including ARG1, inducible nitric oxide synthase (iNOS), TGF-β, and IL-10, and PMN-MDSCs and M-MDSCs exhibit different mechanisms of immune suppression [107,108,109,110,111,112]. Ultimately, MDSCs inhibit the activation and clonal expansion of tumor-specific T cells, as well as induce Treg cell development (Figure 2). Furthermore, MDSCs secrete various factors that promote prostate cancer progression, such as IL-1 receptor antagonist (IL-1RA) that antagonizes senescence of prostate cancer in a paracrine manner [113], and IL-23 that acts as a driver of CRPC [114]. Thus, targeting MDSCs may provide novel opportunities for cancer therapy.
2.3. Crosstalk between Immune Cells, Stromal Cells, and Cancer Cells in Prostate Microenvironment
In the inflammatory prostate microenvironment, crosstalk between immune, stromal, and cancer cells potentially facilitates further tumor progression [115,116,117]. An ex vivo prostate tumor model, derived from patients with prostate cancer, demonstrated that prostate tumors showed low levels of cytotoxic T lymphocytes and T-helper (Th)1 cells-recruiting chemokines, such as CCL5, CXCL9, and CXCL10, but expressed high levels of chemokines implicated in attracting TAMs, MDSCs, and Treg cells, such as CCL2, CCL22, and CXCL12 [118]. CCL22, secreted by tumor cells and TAMs, activates trafficking of Treg cells within the tumor as well as promotes tumor migration and invasion [119,120,121]. Human prostate carcinoma-associated fibroblasts and prostate cancer cells orchestrate and enhance TAM and MDSC recruitment to prostate tumors as well as M2-like TAM differentiation by the chemokines CCL2, CXCL12, and IL-6 during cancer progression [76,122]. Sexually transmitted disease-associated inflammation facilitates IL-6 production by prostate epithelial cells, which induces M2-like TAM polarization [123]. Furthermore, MDSC and tumor cell cross-talk enhances IL-6 production within tumor microenvironment [124], while IL-10, produced by MDSCs, increases M2-like TAMs [125,126,127]. The MDSCs derived from patients with prostate cancer inhibit CD8+ T cells through ARG1, a downstream signal transducer and activator of transcription (STAT)3 target gene [91]. Moreover, the phenotypic analysis of prostate infiltrating lymphocytes, derived from patients with prostate cancer, revealed them to be skewed towards a regulatory Treg and Th17 phenotypes [128]. Tregs are associated with poor prognosis and were found to be highly infiltrated in the prostate tissue of patients with prostate cancer [129,130]. Th17 cells, the key mediators in a number of autoimmune diseases, play a role in inflammation-associated prostate cancer [131,132]. Their development depends on the pleiotropic cytokine TGF-β, which is also linked to Treg cell development and function [133]. In Hi-Myc mouse model of prostate cancer, retrograde urethral instillation of CP1, a human prostatic isolate of Escherichia coli, was reported to induce chronic inflammation characterized by an influx of TAMs and Th17 lymphocytes with distinct cytokine profiles and thus accelerate cancer progression [134].
Crosstalk between MDSCs and mast cells was found to further suppress effective anti-tumor immunity in a transgenic adenocarcinoma of the mouse prostate (TRAMP) model [135]. PhIP (2-amino-1-methyl-6-phenylimidazo[4,5-b]pyridine), one of the most abundant heterocyclic amines in cooked meat, induced rat prostate cancer with elevated DNA mutation frequencies in the prostate as well as infiltration of TAMs and mast cells, suggesting a potential mechanism involving inflammation promotion by which dietary compounds can increase cancer risk [136]. Furthermore, bacterial prostatitis accelerates PhIP-induced prostate carcinogenesis by increasing the level of circulating IL-6 in the rat prostate [137]. Another factor that facilitates chronic inflammation is obesity, wherein adipose derived proinflammatory molecules activate TAMs and MDSCs, subsequently promoting cancer progression [138,139,140,141,142,143,144,145]. CCL2 produced by adipocytes enhances the growth and invasion of prostate cancer cells [146]. Upregulation of serum CCL2 levels enhanced the tumor growth of prostate cancer LNCaP xenografts in high-fat diet fed mice [147]. In obese mice, expanded MDSCs suppress CD8+ T cells via iNOS and interferon-γ, and also induce M2 TAM polarization via IL-10 [148,149]. The loss of Pten in the prostate epithelium causes local MDSC expansion via inflammatory cytokines, such as CSF-1 and IL-1β. [96]. In a mouse prostate cancer model driven by loss of Pten and Smad4, MDSCs play a critical role in cancer progression, as CXCR2-expressing MDSCs infiltrate in the prostate due to CXCL5 up-regulation in tumors [150]. In Pten-deficient model mice for prostate cancer, a high-fat diet mediated inflammation-induced M2 TAM differentiation and expansion of MDSCs, accelerated IL-6 secretion, and facilitated tumor growth via IL-6/STAT3 signaling pathway [151]. Thus, the inflammation-associated prostate cancer progression is potentially mediated by diverse mechanisms, such as microbiome, dietary carcinogens, obesity, cellular stress, hypoxia, and fibrosis, which consequently inhibit effective anti-tumor immunity (Figure 2). These pathways may be promising targets for chemoprevention and cancer therapy.
3. Chemoprevention of Prostate Cancer
Exposure to various environmental factors can cause chronic inflammation in the prostate and stimulate cancer development and progression. The presence of pathogens in the urogenital organ and gut [152,153] as well as sexual activity [154,155] are associated with chronic inflammation and prostate cancer (Figure 2). The DNA adduct of PhIP, a type of DNA damage, was identified in prostate cancer tissues of patients who frequently consumed cooked red meat [156]. In a cohort of health professionals in the U.S. (n = 26,030), intake of PhIP from red meat was significantly associated with prostate cancer risk (HR 1.18, 95% CI 1.03–1.35), especially in high-grade (Gleason score 7 with pattern 4 + 3, and Gleason score 8–10) cancers (HR 1.44, 95% CI 1.04–1.98). [157]. Higher dietary inflammatory index score is associated with a higher risk of incidence and mortality of all cancer types, including prostate cancer [158,159,160]. Consumption of diets rich in anti-inflammatory food components, such as omega-3 fatty acids and green tea, should help prevent prostate cancer [161]. Interestingly, in a mouse prostate cancer MycCaP model, dietary omega-3 fatty acids decreased M2 TAM polarization and inhibited prostate cancer progression [162,163]. Obesity is associated with chronic inflammation and mortality due to various types of malignancies, including prostate cancer [164]. A high-fat diet induced lipid accumulation in prostate tumors, which led to metastatic progression in a nonmetastatic Pten-null mouse model [165]. Moreover, epidemiological evidence suggests that metabolic disease, food, and dietary factors are associated with the risk of prostate cancer [166,167,168]. Thus, lifestyle changes are beneficial for prevention of prostate cancer. In addition, anti-inflammatory agents, such as aspirin, non-steroidal anti-inflammatory drugs (NSAIDs), metformin, and statins, may be useful for chemoprevention of prostate cancer (Table 1).
3.1. Aspirin and NSAIDs
Aspirin (acetylsalicylic acid), an NSAID, was developed in the late 19th century. As an anti-inflammatory and anti-thrombotic agent, aspirin is widely administrated in order to prevent and treat cardiovascular diseases. Over the last several decades, a number of epidemiological studies demonstrated the association between aspirin use and decreased risk of human carcinogenesis, especially in inflammation-related cancers such as colorectal cancer, gastric cancer, liver cancer, and prostate cancer [169,170,188].
In the Physicians’ Health Study, where healthy male physicians (n = 22,071) were randomized to aspirin, β-carotene, both, or placebo, current and past regular aspirin use was associated with a lower risk of lethal prostate cancer (current: HR 0.68, 95% CI 0.52–0.89; past: HR 0.54, 95% CI 0.40–0.74) compared to never users [170]. Similarly, in the REDUCE Study, where all men (n = 6729) were biopsied independent of PSA levels and had a negative baseline biopsy, the use of aspirin and/or other NSAIDs was significantly associated with decreased total (OR = 0.87, 95% CI 0.76–0.99, p = 0.03) and high-grade (OR = 0.80, 95% CI 0.64–0.99, p = 0.04) prostate cancer risk [171]. In the Health Professionals Follow-Up Study cohort (n = 51,529), long-term higher dose of aspirin (≥ 6 tablets/week) was associated with the reduction of high-grade (HR 0.72, 95% CI 0.54–0.96) and lethal (HR 0.71, 95% CI 0.50–1.00) prostate cancer [172]. In PLCO study (n = 29,450) intake of at least one aspirin/day was associated with a lower risk of prostate cancer (HR 0.92, 95% CI 0.85–0.99) compared with never use [173]. In a Finnish Prostate Cancer Screening Trial, an elevated risk of prostate cancer was reported in current NSAID users, but not in previous users, due to protopathic bias as NSAIDs were used to treat symptoms of undiagnosed metastatic prostate cancer as mentioned by the authors [189]. Thus, accumulating evidence indicates the potential inhibitory effect of aspirin on prostate cancer incidence and progression.
Furthermore, in the Physicians’ Health Study, post-diagnostic aspirin use was associated with lower risk of lethal prostate cancer (HR 0.68, 95% CI 0.52–0.90) and overall mortality (HR 0.72, 95% CI 0.61–0.9) [170]. According to the Cancer of the Prostate Strategic Urologic Research Endeavor (CaPSURE) database, aspirin use was associated with a lower risk of prostate cancer-specific mortality (adjusted HR 0.43, 95% CI 0.21–0.87, p = 0.02) among patients (n = 5955) with localized prostate cancer treated with radical prostatectomy or radiotherapy [174]. Similarly, in the Cancer Prevention Study-II Nutrition Cohort, among men diagnosed with high-risk cancers (≥ T3 and/or Gleason score ≥ 8), post-diagnosis daily aspirin use was also associated with lower prostate cancer-specific mortality (HR 0.60, 95% CI 0.37–0.97) [175]. In a Nationwide Cohort Study (n = 29,136), the post-diagnostic use of low-dose aspirin (75–150 mg) slightly reduced prostate cancer mortality over 5-year (HR 0.91, 95% CI 0.83–1.01) and 7.5-year (HR 0.84, 95% CI 0.72–0.97) post-diagnosis exposure periods [176]. An ongoing randomized Add-Aspirin trial (NCT02804815), that began in 2015, aims to determine if post-diagnosis aspirin use improves cancer outcome among men with non-metastatic prostate cancer as well as other types of cancers [190].
Aspirin inhibits cyclooxygenases, COX1 and COX2, which catalyze the production of prostaglandins that trigger pain, fever, blood clotting, or inflammation. Aspirin controls the activity of platelets via COX1 inhibition, which blocks the interaction between platelets and cancer cells [191,192]. In addition, COX2 is frequently expressed in various types of cancers and plays multiple roles in inflammation and cancer progression [193,194]. The histopathological analysis of prostatic tissue derived from patients with prostate cancer revealed that COX2 expression was associated with local chronic inflammation [195]. In a TRAMP model, a COX2 selective inhibitor, celecoxib, inhibited prostate tumor growth and improved survival [196]. COX2 inhibitors suppress prostate cancer growth via a variety of pathways [197,198,199,200,201], including androgen receptor signaling pathway [202,203]. In various types of tumor microenvironment, COX2-mediated PGE2 inhibition suppresses MDSC expansion and provokes a shift in the tumor inflammatory profiles toward anti-cancer immune pathways [204,205,206]. In the prostate tumor microenvironment, PGE2 induces CXCL12 expression in prostate stromal cells [207]. Further, in an ex vivo prostate tumor model, celecoxib suppressed intra-tumoral production of the Treg/MDSC-attractant CXCL12 and Treg-attractant CCL22, while increasing the production of the cytotoxic T lymphocyte (CTL) attractant CXCL10. These changes in local chemokine production were accompanied by the reduced ability of celecoxib-treated tumors to attract Treg cells, and strongly enhanced the attraction of CTLs [118]. As COX2 inhibition also blocks M2 TAM differentiation [208,209], celecoxib suppressed M2 TAMs and local MDSCs, and subsequently inhibited high-fat diet-mediate inflammation, resulting in tumor regression in Pten-deficient model mice for prostate cancer [151]. Thus, NSAIDs potentially modulate the immune system, enhance anti-cancer immunity, and inhibit prostate cancer progression.
Long-term administration of COX-2 selective inhibitor is limited for the use of cancer chemoprevention because of the potential cardiovascular risks involved, particularly in older men who are likely to have cardiovascular comorbidities [177,178]. Moreover, neoadjuvant use of short-term celecoxib for 4–6 weeks did not greatly influence COX-related biologic markers in patients with localized prostate cancer who underwent radical prostatectomy [210,211,212]. In the STAMPEDE trial as well, celecoxib daily use for up to one year was insufficient to improve overall survival in patients with advanced hormone naïve prostate cancer who underwent androgen deprivation therapy (ADT), although the preplanned subgroup analyses revealed that celecoxib in combination with zoledronic acid improved overall survival in patients with metastatic disease (HR 0.78, 95% CI 0.62–0.98) [179,180]. Thus, future studies are needed to identify feasible COX2 inhibitor candidates for preventing disease progression in patients with prostate cancer.
3.2. Metformin
Metabolic syndrome prevalence was reported to be 55% in men who underwent long-term ADT compared to 22% in those who did not receive ADT [213]. Abdominal obesity and hyperglycemia are responsible for this higher prevalence, predisposing them to higher cardiovascular risk [214]. Thus, metformin, a first-line medication for type 2 diabetes, is beneficial for patients with advanced prostate cancer as it prevents ADT-induced metabolic syndrome [181] and has potential antineoplastic activity in prostate cancer [215]. A recent meta-analysis, which included 30 cohort studies (n = 1,660,795), demonstrated that metformin improved both overall survival (HR 0.72, 95% CI 0.59–0.88) and cancer-specific survival (HR 0.78, 95% CI 0.64–0.94) in patients with prostate cancer compared with those not treated with metformin, although the incidence of prostate cancer was not associated with metformin [182]. Importantly, a dose-dependent inverse association between metformin and serum PSA levels was observed, which potentially affects the indication of prostate biopsy as well as detection of prostate cancer [216]. Metformin exerts its anti-cancer effect directly by acting on the tumor via inhibition of the mitochondrial electron transport chain and consequent activation of adenosine monophosphate-activated protein kinase, as well as indirectly by lowering systemic insulin levels [217]. Metformin is also capable of repressing prostate cancer progression by inhibiting infiltration of TAMs, especially those induced by ADT, by inhibiting the COX2/PGE2 axis as observed in the TRAMP model [218]. It also inhibited prostate cancer growth induced by a high-fat diet via inhibition of MDSCs in Pten-deficient model mice [219]. Based on its anti-cancer effects and to help prevent the adverse metabolic effects of long-term ADT, metformin is included in the STAMPEDE (Arm K), a randomized controlled phase 3 trial (NCT00268476). Another ongoing randomized phase 3 study aims to determine if metformin can delay the time to progression in men with low risk prostate cancer who underwent active surveillance (NCT01864096).
3.3. Statins
Statins are the most commonly used cholesterol-lowering drugs that act by inhibiting HMG-CoA (3-hydroxy-3-methylglutaryl-coenzyme A) reductase activity and are widely used in prevention of coronary artery disease [183]. Emerging evidence suggests that statins may also reduce the risk of cancers. A meta-analysis including 27 studies (n = 1,893,571) indicated that statin use reduced the risk of total (RR 0.93, 95% CI 0.87–0.99) and particularly advanced (RR 0.80, 95% CI 0.70–0.90) prostate cancer [184]. In a cohort from Danish registries (statin use n = 18,721, no-statin n = 277,204), statin use in patients with cancer reduced death due to any cause (HR 0.85, 95% CI 0.83–0.87) as well as due to cancer (HR 0.85, 95% CI 0.82–0.87) [185]. In another cohort from nationwide Danish registries (n = 31,790), post-diagnosis statin use was associated with reduced all-cause mortality (HR 0.81, 95% CI 0.76–0.85) and prostate cancer mortality (HR 0.83, 95% CI 0.77–0.89) [186]. A meta-analysis of 13 studies (n = 100,536) also showed that post-diagnostic statin use was correlated with reductions in both all-cause mortality (HR 0.77, 95% CI 0.69–0.87) and prostate cancer-specific mortality (HR 0.64, 95% CI 0.52–0.79) [187]. However, statin intake is inversely related to serum PSA levels, which can influence the indication of prostate biopsy [220,221,222,223]. The antineoplastic effect of statins arises from a number of cholesterol-mediated mechanisms, as cholesterol is a key component of lipid rafts, which facilitate intracellular signaling processes such as epidermal growth factor and IL-6 [224]. Importantly, statins inhibit chemokine production, such as CCL2 and CCL5, and act as anti-inflammation agents [225,226]. Therefore, the beneficial effects of statins on the reduction of cardiovascular events as well as cancer-related mortality are attributed to their anti-inflammatory properties. Further studies are needed to identify the mechanism of statin action on chemoprevention of prostate cancer. A phase 3 clinical trial to evaluate impact of atorvastatin on prostate cancer progression during ADT is ongoing (NCT04026230). Another 2 × 2 factorial randomized phase 3 trial was recently launched to evaluate the benefit of aspirin and atorvastatin on overall survival in patients with CRPC (NCT03819101).
4. Future Directions: Direct Targeting of Pro-Inflammatory Immunity
There have been substantial advances in the therapeutics of prostate cancer over the past decade. Understanding the mechanism of tumor-promoting chronic inflammation provides novel therapeutic targets for advanced and refractory prostate cancer. Therapeutic strategies against cancer-associated chronic inflammation include: (1) inhibition of pro-tumoral inflammation, (2) boost of anti-cancer pathways, and (3) reprogramming and/or depleting immune cells [227]. TAMs and MDSCs play a vital role in the development of prostate tumor inflammatory microenvironment, which cooperatively inhibits effective anti-tumoral immunity and induces Treg cells. As a result, prostate tumor microenvironment usually becomes immunologically “cold” (Figure 2). Thus, therapeutic strategies that directly target TAMs [228,229,230,231,232,233] as well as MDSCs [109,234,235,236,237,238,239,240] are promising for improved cancer outcomes. Several clinical trials that potentially target TAMs and/or MDSCs have been designed and launched to treat patients with prostate cancer (Table 2).
The IL-6/Janus kinase (JAK)/STAT3 pathway is aberrantly hyperactivated in many types of cancer, including prostate cancer, and such hyperactivation is generally associated with a poor prognosis [241,242,243]. In addition to direct effects on tumor cells, IL-6/JAK/STAT3 signaling has a fundamental effect on tumor-infiltrating immune cells [244,245]. STAT3 negatively regulates dendritic cells, effector T cells, natural killer cells, and neutrophils, suggesting that STAT3 activation in immune cells likely leads to the down-regulation of anti-tumor immunity [246]. At the same time, STAT3 positively regulates TAMs, MDSCs, Treg cells, and Th17 cells [247,248]. Thus, collectively, IL-6/JAK/STAT3 pathway contributes to the development of a highly immunosuppressive tumor microenvironment. In Pten-deficient murine model for prostate cancer, inhibition of IL-6 suppressed high-fat diet-mediated prostatic inflammation and subsequent cancer progression [151]. Siltuximab (CNTO 328), an anti-IL-6 monoclonal antibody, was approved by the FDA for treatment in patients with multicentric Castleman’s disease [249]. Inhibition of IL-6 with siltuximab suppressed castration-resistant progression in androgen-dependent prostate cancer xenograft model mice [250]. However, phase 2 clinical trials (NCT00433446, NCT00385827) revealed that siltuximab had no significant clinical benefit in patients with metastatic CRPC who showed a dramatic increase in plasma IL-6 after treatment and confirmed the poor prognosis associated with elevated IL-6 at baseline [251,252]. As analyses of radical prostatectomy specimens from a phase 1 study revealed a decrease in phosphorylated STAT3 and mitogen-activated protein kinases by siltuximab treatment, IL-6 blockade may be effective early during disease progression [253]. Another FDA-approved drug called niclosamide, an oral antihelminthic drug, exerts its effects via Wnt/β-catenin, mammalian target of rapamycin complex 1, STAT3, NF-κB, and Notch signaling pathways. Therefore, it potentially has broad clinical applications for the treatment of diseases other than those caused by parasites, including metabolic diseases, infection, and cancer [254]. Niclosamide suppresses macrophage-induced inflammation via STAT3 and/or NF-κB signaling [255]. In addition, niclosamide was identified as a potent androgen receptor splice variant 7 (AR-V7) inhibitor in prostate cancer cells [256]. Clinical trials to evaluate impact of niclosamide combined with enzalutamide or abiraterone in patients with metastatic CRPC are ongoing (NCT03123978, NCT02807805). Antisense oligonucleotides provide another distinctly different approach to inhibit cellular STAT3, inhibiting immunosuppressive MDSCs and enhancing anti-tumor immunity, which could effectively eradicate prostate tumors in a mouse model [257].
CSF-1 is a major survival factor for TAMs, as CSF-1 receptor inhibition strongly reduces TAMs and increases cytotoxic CD8+ T cells in animal models [258]. CSF-1 is reportedly increased in irradiated prostate tumors, which enhances tumor-infiltrating TAMs and MDSCs that can limit the efficacy of radiotherapy in prostate tumor murine model [259]. ADT-induced prostate cancer cells express CSF-1 and other cytokines that significantly increase M2 TAM infiltration and potentially cause castration-resistant cancer progression [260]. Pexidartinib (PLX3397), an FDA-approved CSF-1 receptor inhibitor, shows a robust tumor response in tenosynovial giant cell tumor [261]. The addition of pexidartinib to docetaxel improved therapeutic efficacy in CRPC by reducing the pro-tumorigenic influences of TAMs in mouse xenograft models [262]. A clinical trial to evaluate the impact of pexidartinib combined with radiation therapy and ADT in patients with localized prostate cancer is ongoing (NCT02472275).
CCL2, also known as monocyte chemoattractant protein (MCP)-1, is a potent monocyte-attracting chemokine and greatly contributes to the recruitment of peripheral blood monocytes into sites of inflammatory responses and tumors [263,264]. In prostate cancer, CCL2 is particularly up-regulated in bone metastasis, and promotes tumor growth and progression [265,266,267,268,269]. Systemic administration of CCL2 monoclonal antibody, carlumab (CNTO 888), in VCaP xenograft model mice attenuated TAM infiltration and retarded tumor growth. Thus, CCL2 acts as a mediator of prostate cancer growth through the regulation of TAMs [270]. Moreover, inhibition of CCL2 by carlumab combined with docetaxel significantly reduced tumor burden compared with docetaxel alone in prostate cancer xenograft model mice [271]. However, carlumab could not effectively block serum CCL2 levels and showed no anti-tumor activity as a single agent in metastatic CRPC in the clinical trial (NCT00992186) [272].
CXCL12, also known as stromal cell-derived factor (SDF)-1, is a strong chemotactic for lymphocytes as well as myeloid cells, including TAMs and MDSCs [273,274,275]. CXCL12 and its receptor, CXCR4, play pivotal roles in tumor development, progression, angiogenesis, and metastasis in various types of cancers [276]. The expression of CXCR4 protein is significantly associated with the presence of bone metastasis in prostate cancer [277]. Inhibition of CXCR4 by plerixafor (AMD3100) or CTE9908 significantly reduced bone metastasis in prostate cancer model mice [278], as the tumorigenic potential is largely regulated by the CXCR4 signaling pathway in prostate cancer cells [279]. Obesity causes inflammation-mediated tumor progression via CXCL12–CXCR4/CXCR7 signaling axis which was attenuated by plerixafor in Myc-induced prostate tumor model mice [280]. Plerixafor inhibits tumor–stroma interactions through CXCL12/CXCR4 pathway, enhancing efficacy of docetaxel in prostate cancer [281]. Although plerixafor is approved by the FDA for autologous transplantation in patients with Non-Hodgkin’s lymphoma or multiple myeloma, it can also be used in various other malignancies and immunological disorders [282].
Tasquinimod (ABR-215050), an oral immunomodulatory compound, reportedly affects the accumulation and function of tumor-suppressive myeloid cells, MDSCs, and M2-like TAMs via targeting the inflammatory protein S100A9 [283,284,285]. In a randomized phase 3 trial (NCT01234311), chemotherapy-naive men with metastatic CRPC (n = 1245) were randomly assigned either tasquinimod or placebo. Tasquinimod significantly improved radiographic progression-free survival compared with placebo (HR 0.64, 95% CI 0.54–0.75), although no overall survival benefit was observed [286]. Bruton tyrosine kinase (BTK) plays a crucial role in B cell development as well as T2 TAM polarization. Inhibition of BTK with an FDA-approved inhibitor, ibrutinib, restores T cell-dependent anti-tumor immune responses, and potentially inhibits the progression of solid tumors. [287,288]. A clinical trial to evaluate the efficacy of ibrutinib on localized prostate cancer is ongoing (NCT02643667). Recently, a substantial number of studies focused on immunometabolism, particularly the changes in intracellular metabolic pathways in immune cells that alter their function [289]. Among these, tryptophan metabolism catalyzed by the enzyme indoleamine 2,3-dioxygenase (IDO) was reported to be crucial for anti-tumor immunity [290]. IDO is widely overexpressed in various types of cancers and inhibits CD8+ effector T cells and natural killer cells, while activating Treg cells and MDSCs [291,292]. Accordingly, inhibitors of the enzymatic activity and effector functions of IDO have been developed as tools for novel cancer therapy [293,294]. Indoximod, an IDO1 pathway inhibitor, was used to treat patients with metastatic CRPC in combination with Sipuleucel-T in a phase 2 clinical trial (NCT01560923).
Immune checkpoint inhibitors which target cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) and the programmed cell death protein 1 pathway (PD-1/PD-L1) have presented substantial benefits for many types of cancers, but only a marginal benefit for prostate cancer, because of the immunosuppressive tumor microenvironment and low mutation burden [295,296]. However, novel strategies are emerging to modulate the prostate immune-suppressive microenvironment. The preclinical studies demonstrated that the combination therapy with immune checkpoint inhibitors and agents targeted at pro-inflammatory immunity could effectively eradicate prostate cancer [297,298,299,300]. Thus, recent advances may shed new light on immunotherapy for prostate cancer.
5. Conclusions
Chronic inflammation plays a major role in the etiology, development, and progression of prostate cancer. A number of studies demonstrated that aspirin is a potent chemopreventive agent for prostate cancer, concurrently preventing cardiovascular diseases. Metformin and statins may also have potential benefit for chemoprevention of prostate cancer. Crosstalk between immune cells and cancer cells orchestrates the generation of prostatic inflammatory microenvironment via a variety of cytokines and chemokines. Importantly, TAMs and MDSCs are significantly expanded in patients with prostate cancer, causing effector T cell inhibition and Treg cell induction, thus providing possible targets for cancer immunotherapy. Recent years have seen emergence of novel strategies that target pro-inflammatory immunity to treat patients with prostate cancer.
Author Contributions
Conceptualization, K.H., K.F., and N.N.; methodology, K.H. and K.F.; formal analysis, K.H.; investigation, K.H.; resources, K.F.; data curation, K.H.; writing—original draft preparation, K.H. and K.F.; writing—review and editing, K.F. and N.N.; visualization, K.H. and K.F.; supervision, N.N.; project administration, K.F.; funding acquisition, K.H., K.F., and N.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Japan Society for the Promotion of Science KAKENHI, grant numbers, 20K18090, T18K091320 and T19K096890.
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ames, B.N.; Gold, L.S.; Willett, W.C. The causes and prevention of cancer. Proc. Natl. Acad. Sci. USA 1995, 92, 5258–5265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuper, H.; Adami, H.O.; Trichopoulos, D. Infections as a major preventable cause of human cancer. J. Intern. Med. 2000, 248, 171–183. [Google Scholar] [CrossRef] [PubMed]
- De Marzo, A.M.; Platz, E.A.; Sutcliffe, S.; Xu, J.; Grönberg, H.; Drake, C.G.; Nakai, Y.; Isaacs, W.B.; Nelson, W.G. Inflammation in prostate carcinogenesis. Nat. Rev. Cancer 2007, 7, 256–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elinav, E.; Nowarski, R.; Thaiss, C.A.; Hu, B.; Jin, C.; Flavell, R.A. Inflammation-induced cancer: Crosstalk between tumours, immune cells and microorganisms. Nat. Rev. Cancer 2013, 13, 759–771. [Google Scholar] [CrossRef] [PubMed]
- Cai, T.; Santi, R.; Tamanini, I.; Galli, I.C.; Perletti, G.; Bjerklund Johansen, T.E.; Nesi, G. Current Knowledge of the Potential Links between Inflammation and Prostate Cancer. Int. J. Mol. Sci. 2019, 20, 3833. [Google Scholar] [CrossRef] [Green Version]
- Leongamornlert, D.; Saunders, E.; Dadaev, T.; Tymrakiewicz, M.; Goh, C.; Jugurnauth-Little, S.; Kozarewa, I.; Fenwick, K.; Assiotis, I.; Barrowdale, D.; et al. Frequent germline deleterious mutations in DNA repair genes in familial prostate cancer cases are associated with advanced disease. Br. J. Cancer 2014, 110, 1663–1672. [Google Scholar] [CrossRef]
- Pritchard, C.C.; Mateo, J.; Walsh, M.F.; De Sarkar, N.; Abida, W.; Beltran, H.; Garofalo, A.; Gulati, R.; Carreira, S.; Eeles, R.; et al. Inherited DNA-Repair Gene Mutations in Men with Metastatic Prostate Cancer. N. Engl. J. Med. 2016, 375, 443–453. [Google Scholar] [CrossRef]
- Cook, L.S.; Goldoft, M.; Schwartz, S.M.; Weiss, N.S. Incidence of adenocarcinoma of the prostate in Asian immigrants to the United States and their descendants. J. Urol. 1999, 161, 152–155. [Google Scholar] [CrossRef]
- Peto, J. Cancer epidemiology in the last century and the next decade. Nature 2001, 411, 390–395. [Google Scholar] [CrossRef]
- Porter, C.M.; Shrestha, E.; Peiffer, L.B.; Sfanos, K.S. The microbiome in prostate inflammation and prostate cancer. Prostate Cancer Prostatic Dis. 2018, 21, 345–354. [Google Scholar] [CrossRef]
- Fujita, K.; Hayashi, T.; Matsushita, M.; Uemura, M.; Nonomura, N. Obesity, Inflammation, and Prostate Cancer. J. Clin. Med. 2019, 8, 201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsushita, M.; Fujita, K.; Nonomura, N. Influence of Diet and Nutrition on Prostate Cancer. Int. J. Mol. Sci. 2020, 21, 1447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidsson, S.; Fiorentino, M.; Andrén, O.; Fang, F.; Mucci, L.A.; Varenhorst, E.; Fall, K.; Rider, J.R. Inflammation, focal atrophic lesions, and prostatic intraepithelial neoplasia with respect to risk of lethal prostate cancer. Cancer Epidemiol. Biomark. Prev. 2011, 20, 2280–2287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vral, A.; Magri, V.; Montanari, E.; Gazzano, G.; Gourvas, V.; Marras, E.; Perletti, G. Topographic and quantitative relationship between prostate inflammation, proliferative inflammatory atrophy and low-grade prostate intraepithelial neoplasia: A biopsy study in chronic prostatitis patients. Int. J. Oncol. 2012, 41, 1950–1958. [Google Scholar] [CrossRef] [PubMed]
- Sfanos, K.S.; De Marzo, A.M. Prostate cancer and inflammation: The evidence. Histopathology 2012, 60, 199–215. [Google Scholar] [CrossRef] [Green Version]
- Sfanos, K.S.; Yegnasubramanian, S.; Nelson, W.G.; De Marzo, A.M. The inflammatory microenvironment and microbiome in prostate cancer development. Nat. Rev. Urol. 2018, 15, 11–24. [Google Scholar] [CrossRef]
- Dennis, L.K.; Lynch, C.F.; Torner, J.C. Epidemiologic association between prostatitis and prostate cancer. Urology 2002, 60, 78–83. [Google Scholar] [CrossRef]
- Irani, J.; Goujon, J.M.; Ragni, E.; Peyrat, L.; Hubert, J.; Saint, F.; Mottet, N. High-grade inflammation in prostate cancer as a prognostic factor for biochemical recurrence after radical prostatectomy. Pathologist Multi Center Study Group. Urology 1999, 54, 467–472. [Google Scholar] [CrossRef]
- Roberts, R.O.; Bergstralh, E.J.; Bass, S.E.; Lieber, M.M.; Jacobsen, S.J. Prostatitis as a risk factor for prostate cancer. Epidemiology 2004, 15, 93–99. [Google Scholar] [CrossRef]
- MacLennan, G.T.; Eisenberg, R.; Fleshman, R.L.; Taylor, J.M.; Fu, P.; Resnick, M.I.; Gupta, S. The influence of chronic inflammation in prostatic carcinogenesis: A 5-year followup study. J. Urol. 2006, 176, 1012–1016. [Google Scholar] [CrossRef]
- Jiang, J.; Li, J.; Yunxia, Z.; Zhu, H.; Liu, J.; Pumill, C. The role of prostatitis in prostate cancer: Meta-analysis. PLoS ONE 2013, 8, e85179. [Google Scholar] [CrossRef] [PubMed]
- Gurel, B.; Lucia, M.S.; Thompson, I.M.; Goodman, P.J.; Tangen, C.M.; Kristal, A.R.; Parnes, H.L.; Hoque, A.; Lippman, S.M.; Sutcliffe, S.; et al. Chronic inflammation in benign prostate tissue is associated with high-grade prostate cancer in the placebo arm of the prostate cancer prevention trial. Cancer Epidemiol. Biomark. Prev. 2014, 23, 847–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujita, K.; Hosomi, M.; Tanigawa, G.; Okumi, M.; Fushimi, H.; Yamaguchi, S. Prostatic inflammation detected in initial biopsy specimens and urinary pyuria are predictors of negative repeat prostate biopsy. J. Urol. 2011, 185, 1722–1727. [Google Scholar] [CrossRef] [PubMed]
- Fujita, K.; Imamura, R.; Tanigawa, G.; Nakagawa, M.; Hayashi, T.; Kishimoto, N.; Hosomi, M.; Yamaguchi, S. Low serum neutrophil count predicts a positive prostate biopsy. Prostate Cancer Prostatic Dis. 2012, 15, 386–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yli-Hemminki, T.H.; Laurila, M.; Auvinen, A.; Määttänen, L.; Huhtala, H.; Tammela, T.L.J.; Kujala, P.M. Histological inflammation and risk of subsequent prostate cancer among men with initially elevated serum prostate-specific antigen (PSA) concentration in the Finnish prostate cancer screening trial. BJU Int. 2013, 112, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Moreira, D.M.; Nickel, J.C.; Gerber, L.; Muller, R.L.; Andriole, G.L.; Castro-Santamaria, R.; Freedland, S.J. Baseline prostate inflammation is associated with a reduced risk of prostate cancer in men undergoing repeat prostate biopsy: Results from the REDUCE study. Cancer 2014, 120, 190–196. [Google Scholar] [CrossRef]
- Vasavada, S.R.; Dobbs, R.W.; Kajdacsy-Balla, A.A.; Abern, M.R.; Moreira, D.M. Inflammation on Prostate Needle Biopsy is Associated with Lower Prostate Cancer Risk: A Meta-Analysis. J. Urol. 2018, 199, 1174–1181. [Google Scholar] [CrossRef]
- Umbehr, M.H.; Gurel, B.; Murtola, T.J.; Sutcliffe, S.; Peskoe, S.B.; Tangen, C.M.; Goodman, P.J.; Thompson, I.M.; Lippman, S.M.; Lucia, M.S.; et al. Intraprostatic inflammation is positively associated with serum PSA in men with PSA. Prostate Cancer Prostatic Dis. 2015, 18, 264–269. [Google Scholar] [CrossRef]
- Nakai, Y.; Nonomura, N. Inflammation and prostate carcinogenesis. Int. J. Urol. 2013, 20, 150–160. [Google Scholar] [CrossRef]
- Sfanos, K.S.; Isaacs, W.B.; De Marzo, A.M. Infections and inflammation in prostate cancer. Am. J. Clin. Exp. Urol. 2013, 1, 3–11. [Google Scholar]
- Gandaglia, G.; Zaffuto, E.; Fossati, N.; Cucchiara, V.; Mirone, V.; Montorsi, F.; Briganti, A. The role of prostatic inflammation in the development and progression of benign and malignant diseases. Curr. Opin. Urol. 2017, 27, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Platz, E.A.; Kulac, I.; Barber, J.R.; Drake, C.G.; Joshu, C.E.; Nelson, W.G.; Lucia, M.S.; Klein, E.A.; Lippman, S.M.; Parnes, H.L.; et al. A Prospective Study of Chronic Inflammation in Benign Prostate Tissue and Risk of Prostate Cancer: Linked PCPT and SELECT Cohorts. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1549–1557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, X.; Gao, X.; Li, X.; Qi, X.; Ma, M.; Qin, S.; Yu, H.; Sun, S.; Zhou, D.; Wang, W. Prognostic significance of neutrophil-to-lymphocyte ratio in prostate cancer: Evidence from 16,266 patients. Sci. Rep. 2016, 6, 22089. [Google Scholar] [CrossRef]
- Sciarra, A.; Gentilucci, A.; Salciccia, S.; Pierella, F.; Del Bianco, F.; Gentile, V.; Silvestri, I.; Cattarino, S. Prognostic value of inflammation in prostate cancer progression and response to therapeutic: A critical review. J. Inflamm. 2016, 13, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, T.; Fujita, K.; Tanigawa, G.; Kawashima, A.; Nagahara, A.; Ujike, T.; Uemura, M.; Takao, T.; Yamaguchi, S.; Nonomura, N. Serum monocyte fraction of white blood cells is increased in patients with high Gleason score prostate cancer. Oncotarget 2017, 8, 35255–35261. [Google Scholar] [CrossRef]
- Hayashi, T.; Fujita, K.; Nojima, S.; Hayashi, Y.; Nakano, K.; Ishizuya, Y.; Wang, C.; Yamamoto, Y.; Kinouchi, T.; Matsuzaki, K.; et al. Peripheral blood monocyte count reflecting tumor-infiltrating macrophages is a predictive factor of adverse pathology in radical prostatectomy specimens. Prostate 2017, 77, 1383–1388. [Google Scholar] [CrossRef]
- Ohno, Y. Role of systemic inflammatory response markers in urological malignancy. Int. J. Urol. 2019, 26, 31–47. [Google Scholar] [CrossRef] [Green Version]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef]
- De Visser, K.E.; Eichten, A.; Coussens, L.M. Paradoxical roles of the immune system during cancer development. Nat. Rev. Cancer 2006, 6, 24–37. [Google Scholar] [CrossRef]
- Hayashi, T.; Fujita, K.; Matsushita, M.; Nonomura, N. Main Inflammatory Cells and Potentials of Anti-Inflammatory Agents in Prostate Cancer. Cancers 2019, 11, 1153. [Google Scholar] [CrossRef] [Green Version]
- Khandrika, L.; Kumar, B.; Koul, S.; Maroni, P.; Koul, H.K. Oxidative stress in prostate cancer. Cancer Lett. 2009, 282, 125–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colotta, F.; Allavena, P.; Sica, A.; Garlanda, C.; Mantovani, A. Cancer-related inflammation, the seventh hallmark of cancer: Links to genetic instability. Carcinogenesis 2009, 30, 1073–1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbieri, C.E.; Rubin, M.A. Genomic rearrangements in prostate cancer. Curr. Opin. Urol. 2015, 25, 71–76. [Google Scholar] [CrossRef] [Green Version]
- Robinson, D.; Van Allen, E.M.; Wu, Y.-M.; Schultz, N.; Lonigro, R.J.; Mosquera, J.-M.; Montgomery, B.; Taplin, M.-E.; Pritchard, C.C.; Attard, G.; et al. Integrative clinical genomics of advanced prostate cancer. Cell 2015, 161, 1215–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujita, K.; Ewing, C.M.; Sokoll, L.J.; Elliott, D.J.; Cunningham, M.; De Marzo, A.M.; Isaacs, W.B.; Pavlovich, C.P. Cytokine profiling of prostatic fluid from cancerous prostate glands identifies cytokines associated with extent of tumor and inflammation. Prostate 2008, 68, 872–882. [Google Scholar] [CrossRef] [Green Version]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [Green Version]
- Rani, A.; Dasgupta, P.; Murphy, J.J. Prostate Cancer: The Role of Inflammation and Chemokines. Am. J. Pathol. 2019, 189, 2119–2137. [Google Scholar] [CrossRef] [Green Version]
- Shalapour, S.; Karin, M. Immunity, inflammation, and cancer: An eternal fight between good and evil. J. Clin. Investig. 2015, 125, 3347–3355. [Google Scholar] [CrossRef] [Green Version]
- Strasner, A.; Karin, M. Immune Infiltration and Prostate Cancer. Front. Oncol. 2015, 5, 128. [Google Scholar] [CrossRef]
- Taverna, G.; Pedretti, E.; Di Caro, G.; Borroni, E.M.; Marchesi, F.; Grizzi, F. Inflammation and prostate cancer: Friends or foe? Inflamm. Res. 2015, 64, 275–286. [Google Scholar] [CrossRef]
- Komohara, Y.; Jinushi, M.; Takeya, M. Clinical significance of macrophage heterogeneity in human malignant tumors. Cancer Sci. 2014, 105, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gannon, P.O.; Poisson, A.O.; Delvoye, N.; Lapointe, R.; Mes-Masson, A.-M.; Saad, F. Characterization of the intra-prostatic immune cell infiltration in androgen-deprived prostate cancer patients. J. Immunol. Methods 2009, 348, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Nonomura, N.; Takayama, H.; Nakayama, M.; Nakai, Y.; Kawashima, A.; Mukai, M.; Nagahara, A.; Aozasa, K.; Tsujimura, A. Infiltration of tumour-associated macrophages in prostate biopsy specimens is predictive of disease progression after hormonal therapy for prostate cancer. BJU Int. 2011, 107, 1918–1922. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T.; Shimada, K.; Asai, O.; Tanaka, N.; Fujimoto, K.; Hirao, K.; Konishi, N. Immunohistochemical analysis of inflammatory cells in benign and precancerous lesions and carcinoma of the prostate. Pathobiology 2013, 80, 119–126. [Google Scholar] [CrossRef]
- Lanciotti, M.; Masieri, L.; Raspollini, M.R.; Minervini, A.; Mari, A.; Comito, G.; Giannoni, E.; Carini, M.; Chiarugi, P.; Serni, S. The role of M1 and M2 macrophages in prostate cancer in relation to extracapsular tumor extension and biochemical recurrence after radical prostatectomy. Biomed Res. Int. 2014, 2014, 486798. [Google Scholar] [CrossRef]
- Hu, W.; Qian, Y.; Yu, F.; Liu, W.; Wu, Y.; Fang, X.; Hao, W. Alternatively activated macrophages are associated with metastasis and poor prognosis in prostate adenocarcinoma. Oncol. Lett. 2015, 10, 1390–1396. [Google Scholar] [CrossRef] [Green Version]
- Cao, J.; Liu, J.; Xu, R.; Zhu, X.; Zhao, X.; Qian, B.-Z. Prognostic role of tumour-associated macrophages and macrophage scavenger receptor 1 in prostate cancer: A systematic review and meta-analysis. Oncotarget 2017, 8, 83261–83269. [Google Scholar] [CrossRef]
- Erlandsson, A.; Carlsson, J.; Lundholm, M.; Fält, A.; Andersson, S.-O.; Andrén, O.; Davidsson, S. M2 macrophages and regulatory T cells in lethal prostate cancer. Prostate 2019, 79, 363–369. [Google Scholar] [CrossRef]
- Ruffell, B.; Affara, N.I.; Coussens, L.M. Differential macrophage programming in the tumor microenvironment. Trends Immunol. 2012, 33, 119–126. [Google Scholar] [CrossRef] [Green Version]
- Fang, L.-Y.; Izumi, K.; Lai, K.-P.; Liang, L.; Li, L.; Miyamoto, H.; Lin, W.-J.; Chang, C. Infiltrating macrophages promote prostate tumorigenesis via modulating androgen receptor-mediated CCL4-STAT3 signaling. Cancer Res. 2013, 73, 5633–5646. [Google Scholar] [CrossRef] [Green Version]
- Sousa, S.; Määttä, J. The role of tumour-associated macrophages in bone metastasis. J. Bone Oncol. 2016, 5, 135–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantovani, A.; Marchesi, F.; Malesci, A.; Laghi, L.; Allavena, P. Tumour-associated macrophages as treatment targets in oncology. Nat. Rev. Clin. Oncol. 2017, 14, 399–416. [Google Scholar] [CrossRef] [PubMed]
- Roca, H.; Jones, J.D.; Purica, M.C.; Weidner, S.; Koh, A.J.; Kuo, R.; Wilkinson, J.E.; Wang, Y.; Daignault-Newton, S.; Pienta, K.J.; et al. Apoptosis-induced CXCL5 accelerates inflammation and growth of prostate tumor metastases in bone. J. Clin. Investig. 2018, 128, 248–266. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Sozzani, S.; Locati, M.; Allavena, P.; Sica, A. Macrophage polarization: Tumor-associated macrophages as a paradigm for polarized M2 mononuclear phagocytes. Trends Immunol. 2002, 23, 549–555. [Google Scholar] [CrossRef]
- Mantovani, A.; Sica, A.; Sozzani, S.; Allavena, P.; Vecchi, A.; Locati, M. The chemokine system in diverse forms of macrophage activation and polarization. Trends Immunol. 2004, 25, 677–686. [Google Scholar] [CrossRef]
- Sica, A.; Porta, C.; Morlacchi, S.; Banfi, S.; Strauss, L.; Rimoldi, M.; Totaro, M.G.; Riboldi, E. Origin and Functions of Tumor-Associated Myeloid Cells (TAMCs). Cancer Microenviron. 2012, 5, 133–149. [Google Scholar] [CrossRef] [Green Version]
- Murray, P.J.; Allen, J.E.; Biswas, S.K.; Fisher, E.A.; Gilroy, D.W.; Goerdt, S.; Gordon, S.; Hamilton, J.A.; Ivashkiv, L.B.; Lawrence, T.; et al. Macrophage activation and polarization: Nomenclature and experimental guidelines. Immunity 2014, 41, 14–20. [Google Scholar] [CrossRef] [Green Version]
- Solinas, G.; Germano, G.; Mantovani, A.; Allavena, P. Tumor-associated macrophages (TAM) as major players of the cancer-related inflammation. J. Leukoc. Biol. 2009, 86, 1065–1073. [Google Scholar] [CrossRef] [Green Version]
- Colegio, O.R.; Chu, N.-Q.; Szabo, A.L.; Chu, T.; Rhebergen, A.M.; Jairam, V.; Cyrus, N.; Brokowski, C.E.; Eisenbarth, S.C.; Phillips, G.M.; et al. Functional polarization of tumour-associated macrophages by tumour-derived lactic acid. Nature 2014, 513, 559–563. [Google Scholar] [CrossRef]
- DeNardo, D.G.; Ruffell, B. Macrophages as regulators of tumour immunity and immunotherapy. Nat. Rev. Immunol. 2019, 19, 369–382. [Google Scholar] [CrossRef]
- Hagemann, T.; Wilson, J.; Burke, F.; Kulbe, H.; Li, N.F.; Plüddemann, A.; Charles, K.; Gordon, S.; Balkwill, F.R. Ovarian cancer cells polarize macrophages toward a tumor-associated phenotype. J. Immunol. 2006, 176, 5023–5032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luan, B.; Yoon, Y.-S.; Le Lay, J.; Kaestner, K.H.; Hedrick, S.; Montminy, M. CREB pathway links PGE2 signaling with macrophage polarization. Proc. Natl. Acad. Sci. USA 2015, 112, 15642–15647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arendt, L.M.; McCready, J.; Keller, P.J.; Baker, D.D.; Naber, S.P.; Seewaldt, V.; Kuperwasser, C. Obesity promotes breast cancer by CCL2-mediated macrophage recruitment and angiogenesis. Cancer Res. 2013, 73, 6080–6093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pyonteck, S.M.; Akkari, L.; Schuhmacher, A.J.; Bowman, R.L.; Sevenich, L.; Quail, D.F.; Olson, O.C.; Quick, M.L.; Huse, J.T.; Teijeiro, V.; et al. CSF-1R inhibition alters macrophage polarization and blocks glioma progression. Nat. Med. 2013, 19, 1264–1272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roca, H.; Varsos, Z.S.; Sud, S.; Craig, M.J.; Ying, C.; Pienta, K.J. CCL2 and interleukin-6 promote survival of human CD11b+ peripheral blood mononuclear cells and induce M2-type macrophage polarization. J. Biol. Chem. 2009, 284, 34342–34354. [Google Scholar] [CrossRef] [Green Version]
- Comito, G.; Giannoni, E.; Segura, C.P.; Barcellos-de-Souza, P.; Raspollini, M.R.; Baroni, G.; Lanciotti, M.; Serni, S.; Chiarugi, P. Cancer-associated fibroblasts and M2-polarized macrophages synergize during prostate carcinoma progression. Oncogene 2014, 33, 2423–2431. [Google Scholar] [CrossRef] [Green Version]
- Cassetta, L.; Fragkogianni, S.; Sims, A.H.; Swierczak, A.; Forrester, L.M.; Zhang, H.; Soong, D.Y.H.; Cotechini, T.; Anur, P.; Lin, E.Y.; et al. Human Tumor-Associated Macrophage and Monocyte Transcriptional Landscapes Reveal Cancer-Specific Reprogramming, Biomarkers, and Therapeutic Targets. Cancer Cell 2019, 35, 588–602.e10. [Google Scholar] [CrossRef] [Green Version]
- Noy, R.; Pollard, J.W. Tumor-associated macrophages: From mechanisms to therapy. Immunity 2014, 41, 49–61. [Google Scholar] [CrossRef] [Green Version]
- Ruffell, B.; Chang-Strachan, D.; Chan, V.; Rosenbusch, A.; Ho, C.M.T.; Pryer, N.; Daniel, D.; Hwang, E.S.; Rugo, H.S.; Coussens, L.M. Macrophage IL-10 blocks CD8+ T cell-dependent responses to chemotherapy by suppressing IL-12 expression in intratumoral dendritic cells. Cancer Cell 2014, 26, 623–637. [Google Scholar] [CrossRef] [Green Version]
- Sawa-Wejksza, K.; Kandefer-Szerszeń, M. Tumor-Associated Macrophages as Target for Antitumor Therapy. Arch. Immunol. Ther. Exp. 2018, 66, 97–111. [Google Scholar] [CrossRef] [Green Version]
- Di Mitri, D.; Mirenda, M.; Vasilevska, J.; Calcinotto, A.; Delaleu, N.; Revandkar, A.; Gil, V.; Boysen, G.; Losa, M.; Mosole, S.; et al. Re-education of Tumor-Associated Macrophages by CXCR2 Blockade Drives Senescence and Tumor Inhibition in Advanced Prostate Cancer. Cell Rep. 2019, 28, 2156–2168.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solito, S.; Marigo, I.; Pinton, L.; Damuzzo, V.; Mandruzzato, S.; Bronte, V. Myeloid-derived suppressor cell heterogeneity in human cancers. Ann. N. Y. Acad. Sci. 2014, 1319, 47–65. [Google Scholar] [CrossRef] [PubMed]
- Stromnes, I.M.; Greenberg, P.D.; Hingorani, S.R. Molecular pathways: Myeloid complicity in cancer. Clin. Cancer Res. 2014, 20, 5157–5170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabrilovich, D.I.; Bronte, V.; Chen, S.-H.; Colombo, M.P.; Ochoa, A.; Ostrand-Rosenberg, S.; Schreiber, H. The terminology issue for myeloid-derived suppressor cells. Cancer Res. 2007, 67, 425, author reply 426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talmadge, J.E.; Gabrilovich, D.I. History of myeloid-derived suppressor cells. Nat. Rev. Cancer 2013, 13, 739–752. [Google Scholar] [CrossRef]
- Bronte, V.; Brandau, S.; Chen, S.-H.; Colombo, M.P.; Frey, A.B.; Greten, T.F.; Mandruzzato, S.; Murray, P.J.; Ochoa, A.; Ostrand-Rosenberg, S.; et al. Recommendations for myeloid-derived suppressor cell nomenclature and characterization standards. Nat. Commun. 2016, 7, 12150. [Google Scholar] [CrossRef] [Green Version]
- Vuk-Pavlović, S.; Bulur, P.A.; Lin, Y.; Qin, R.; Szumlanski, C.L.; Zhao, X.; Dietz, A.B. Immunosuppressive CD14+HLA-DRlow/- monocytes in prostate cancer. Prostate 2010, 70, 443–455. [Google Scholar] [CrossRef] [Green Version]
- Brusa, D.; Simone, M.; Gontero, P.; Spadi, R.; Racca, P.; Micari, J.; Degiuli, M.; Carletto, S.; Tizzani, A.; Matera, L. Circulating immunosuppressive cells of prostate cancer patients before and after radical prostatectomy: Profile comparison. Int. J. Urol. 2013, 20, 971–978. [Google Scholar] [CrossRef]
- Chi, N.; Tan, Z.; Ma, K.; Bao, L.; Yun, Z. Increased circulating myeloid-derived suppressor cells correlate with cancer stages, interleukin-8 and -6 in prostate cancer. Int. J. Clin. Exp. Med. 2014, 7, 3181–3192. [Google Scholar]
- Idorn, M.; Køllgaard, T.; Kongsted, P.; Sengeløv, L.; Thor Straten, P. Correlation between frequencies of blood monocytic myeloid-derived suppressor cells, regulatory T cells and negative prognostic markers in patients with castration-resistant metastatic prostate cancer. Cancer Immunol. Immunother. 2014, 63, 1177–1187. [Google Scholar] [CrossRef]
- Hossain, D.M.S.; Pal, S.K.; Moreira, D.; Duttagupta, P.; Zhang, Q.; Won, H.; Jones, J.; D’Apuzzo, M.; Forman, S.; Kortylewski, M. TLR9-Targeted STAT3 Silencing Abrogates Immunosuppressive Activity of Myeloid-Derived Suppressor Cells from Prostate Cancer Patients. Clin. Cancer Res. 2015, 21, 3771–3782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, J.; Huang, G.; Liu, S.; Wan, J.; Wang, X.; Zhu, Y.; Kaliney, W.; Zhang, C.; Cheng, L.; Wen, X.; et al. Polymorphonuclear MDSCs are enriched in the stroma and expanded in metastases of prostate cancer. J. Pathol. Clin. Res. 2020. [Google Scholar] [CrossRef]
- Sinha, P.; Clements, V.K.; Fulton, A.M.; Ostrand-Rosenberg, S. Prostaglandin E2 promotes tumor progression by inducing myeloid-derived suppressor cells. Cancer Res. 2007, 67, 4507–4513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, B.; Lei, Z.; Zhao, J.; Gong, W.; Liu, J.; Chen, Z.; Liu, Y.; Li, D.; Yuan, Y.; Zhang, G.-M.; et al. CCL2/CCR2 pathway mediates recruitment of myeloid suppressor cells to cancers. Cancer Lett. 2007, 252, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Chun, E.; Lavoie, S.; Michaud, M.; Gallini, C.A.; Kim, J.; Soucy, G.; Odze, R.; Glickman, J.N.; Garrett, W.S. CCL2 Promotes Colorectal Carcinogenesis by Enhancing Polymorphonuclear Myeloid-Derived Suppressor Cell Population and Function. Cell Rep. 2015, 12, 244–257. [Google Scholar] [CrossRef] [Green Version]
- Garcia, A.J.; Ruscetti, M.; Arenzana, T.L.; Tran, L.M.; Bianci-Frias, D.; Sybert, E.; Priceman, S.J.; Wu, L.; Nelson, P.S.; Smale, S.T.; et al. Pten null prostate epithelium promotes localized myeloid-derived suppressor cell expansion and immune suppression during tumor initiation and progression. Mol. Cell. Biol. 2014, 34, 2017–2028. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.-R.; Lee, W.; Cho, S.K.; Park, S.-G. Characterization of Multiple Cytokine Combinations and TGF-β on Differentiation and Functions of Myeloid-Derived Suppressor Cells. Int. J. Mol. Sci. 2018, 19, 869. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.; Huang, J.; Ren, X.; Gorska, A.E.; Chytil, A.; Aakre, M.; Carbone, D.P.; Matrisian, L.M.; Richmond, A.; Lin, P.C.; et al. Abrogation of TGF beta signaling in mammary carcinomas recruits Gr-1+CD11b+ myeloid cells that promote metastasis. Cancer Cell 2008, 13, 23–35. [Google Scholar] [CrossRef] [Green Version]
- Song, X.; Krelin, Y.; Dvorkin, T.; Bjorkdahl, O.; Segal, S.; Dinarello, C.A.; Voronov, E.; Apte, R.N. CD11b+/Gr-1+ immature myeloid cells mediate suppression of T cells in mice bearing tumors of IL-1beta-secreting cells. J. Immunol. 2005, 175, 8200–8208. [Google Scholar] [CrossRef] [Green Version]
- Bunt, S.K.; Sinha, P.; Clements, V.K.; Leips, J.; Ostrand-Rosenberg, S. Inflammation induces myeloid-derived suppressor cells that facilitate tumor progression. J. Immunol. 2006, 176, 284–290. [Google Scholar] [CrossRef] [Green Version]
- Bunt, S.K.; Yang, L.; Sinha, P.; Clements, V.K.; Leips, J.; Ostrand-Rosenberg, S. Reduced inflammation in the tumor microenvironment delays the accumulation of myeloid-derived suppressor cells and limits tumor progression. Cancer Res. 2007, 67, 10019–10026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.; Wu, T.; Shao, S.; Shi, B.; Zhao, Y. Phenotype, development, and biological function of myeloid-derived suppressor cells. Oncoimmunology 2016, 5, e1004983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostrand-Rosenberg, S.; Fenselau, C. Myeloid-Derived Suppressor Cells: Immune-Suppressive Cells That Impair Antitumor Immunity and Are Sculpted by Their Environment. J. Immunol. 2018, 200, 422–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Safarzadeh, E.; Orangi, M.; Mohammadi, H.; Babaie, F.; Baradaran, B. Myeloid-derived suppressor cells: Important contributors to tumor progression and metastasis. J. Cell. Physiol. 2018, 233, 3024–3036. [Google Scholar] [CrossRef] [PubMed]
- Groth, C.; Hu, X.; Weber, R.; Fleming, V.; Altevogt, P.; Utikal, J.; Umansky, V. Immunosuppression mediated by myeloid-derived suppressor cells (MDSCs) during tumour progression. Br. J. Cancer 2019, 120, 16–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanaei, M.-J.; Salimzadeh, L.; Bagheri, N. Crosstalk between myeloid-derived suppressor cells and the immune system in prostate cancer: MDSCs and immune system in Prostate cancer. J. Leukoc. Biol. 2020, 107, 43–56. [Google Scholar] [CrossRef]
- Huang, B.; Pan, P.-Y.; Li, Q.; Sato, A.I.; Levy, D.E.; Bromberg, J.; Divino, C.M.; Chen, S.-H. Gr-1+CD115+ immature myeloid suppressor cells mediate the development of tumor-induced T regulatory cells and T-cell anergy in tumor-bearing host. Cancer Res. 2006, 66, 1123–1131. [Google Scholar] [CrossRef] [Green Version]
- Ostrand-Rosenberg, S.; Sinha, P. Myeloid-derived suppressor cells: Linking inflammation and cancer. J. Immunol. 2009, 182, 4499–4506. [Google Scholar] [CrossRef]
- Gabrilovich, D.I.; Ostrand-Rosenberg, S.; Bronte, V. Coordinated regulation of myeloid cells by tumours. Nat. Rev. Immunol. 2012, 12, 253–268. [Google Scholar] [CrossRef] [Green Version]
- Marvel, D.; Gabrilovich, D.I. Myeloid-derived suppressor cells in the tumor microenvironment: Expect the unexpected. J. Clin. Investig. 2015, 125, 3356–3364. [Google Scholar] [CrossRef]
- Kumar, V.; Patel, S.; Tcyganov, E.; Gabrilovich, D.I. The Nature of Myeloid-Derived Suppressor Cells in the Tumor Microenvironment. Trends Immunol. 2016, 37, 208–220. [Google Scholar] [CrossRef] [PubMed]
- Lerman, I.; Garcia-Hernandez, M.d.l.L.; Rangel-Moreno, J.; Chiriboga, L.; Pan, C.; Nastiuk, K.L.; Krolewski, J.J.; Sen, A.; Hammes, S.R. Infiltrating Myeloid Cells Exert Protumorigenic Actions via Neutrophil Elastase. Mol. Cancer Res. 2017, 15, 1138–1152. [Google Scholar] [CrossRef] [Green Version]
- Di Mitri, D.; Toso, A.; Chen, J.J.; Sarti, M.; Pinton, S.; Jost, T.R.; D’Antuono, R.; Montani, E.; Garcia-Escudero, R.; Guccini, I.; et al. Tumour-infiltrating Gr-1+ myeloid cells antagonize senescence in cancer. Nature 2014, 515, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Calcinotto, A.; Spataro, C.; Zagato, E.; Di Mitri, D.; Gil, V.; Crespo, M.; De Bernardis, G.; Losa, M.; Mirenda, M.; Pasquini, E.; et al. IL-23 secreted by myeloid cells drives castration-resistant prostate cancer. Nature 2018, 559, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Fujita, K.; Ewing, C.M.; Isaacs, W.B.; Pavlovich, C.P. Immunomodulatory IL-18 binding protein is produced by prostate cancer cells and its levels in urine and serum correlate with tumor status. Int. J. Cancer 2011, 129, 424–432. [Google Scholar] [CrossRef] [Green Version]
- Sottnik, J.L.; Zhang, J.; Macoska, J.A.; Keller, E.T. The PCa Tumor Microenvironment. Cancer Microenviron. 2011, 4, 283–297. [Google Scholar] [CrossRef] [Green Version]
- Shiao, S.L.; Chu, G.C.-Y.; Chung, L.W.K. Regulation of prostate cancer progression by the tumor microenvironment. Cancer Lett. 2016, 380, 340–348. [Google Scholar] [CrossRef] [Green Version]
- Muthuswamy, R.; Corman, J.M.; Dahl, K.; Chatta, G.S.; Kalinski, P. Functional reprogramming of human prostate cancer to promote local attraction of effector CD8(+) T cells. Prostate 2016, 76, 1095–1105. [Google Scholar] [CrossRef]
- Curiel, T.J.; Coukos, G.; Zou, L.; Alvarez, X.; Cheng, P.; Mottram, P.; Evdemon-Hogan, M.; Conejo-Garcia, J.R.; Zhang, L.; Burow, M.; et al. Specific recruitment of regulatory T cells in ovarian carcinoma fosters immune privilege and predicts reduced survival. Nat. Med. 2004, 10, 942–949. [Google Scholar] [CrossRef]
- Miller, A.M.; Lundberg, K.; Ozenci, V.; Banham, A.H.; Hellström, M.; Egevad, L.; Pisa, P. CD4+CD25high T cells are enriched in the tumor and peripheral blood of prostate cancer patients. J. Immunol. 2006, 177, 7398–7405. [Google Scholar] [CrossRef] [Green Version]
- Maolake, A.; Izumi, K.; Shigehara, K.; Natsagdorj, A.; Iwamoto, H.; Kadomoto, S.; Takezawa, Y.; Machioka, K.; Narimoto, K.; Namiki, M.; et al. Tumor-associated macrophages promote prostate cancer migration through activation of the CCL22-CCR4 axis. Oncotarget 2017, 8, 9739–9751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vickman, R.E.; Broman, M.M.; Lanman, N.A.; Franco, O.E.; Sudyanti, P.A.G.; Ni, Y.; Ji, Y.; Helfand, B.T.; Petkewicz, J.; Paterakos, M.C.; et al. Heterogeneity of human prostate carcinoma-associated fibroblasts implicates a role for subpopulations in myeloid cell recruitment. Prostate 2020, 80, 173–185. [Google Scholar] [CrossRef] [PubMed]
- Han, I.-H.; Song, H.-O.; Ryu, J.-S. IL-6 produced by prostate epithelial cells stimulated with Trichomonas vaginalis promotes proliferation of prostate cancer cells by inducing M2 polarization of THP-1-derived macrophages. PLoS Negl. Trop. Dis. 2020, 14, e0008126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, K.; Lee, O.-Y.; Shon, S.Y.; Nam, O.; Ryu, P.M.; Seo, M.W.; Lee, D.-S. A mutual activation loop between breast cancer cells and myeloid-derived suppressor cells facilitates spontaneous metastasis through IL-6 trans-signaling in a murine model. Breast Cancer Res. 2013, 15, R79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunt, S.K.; Clements, V.K.; Hanson, E.M.; Sinha, P.; Ostrand-Rosenberg, S. Inflammation enhances myeloid-derived suppressor cell cross-talk by signaling through Toll-like receptor 4. J. Leukoc. Biol. 2009, 85, 996–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beury, D.W.; Parker, K.H.; Nyandjo, M.; Sinha, P.; Carter, K.A.; Ostrand-Rosenberg, S. Cross-talk among myeloid-derived suppressor cells, macrophages, and tumor cells impacts the inflammatory milieu of solid tumors. J. Leukoc. Biol. 2014, 96, 1109–1118. [Google Scholar] [CrossRef]
- Ostrand-Rosenberg, S.; Sinha, P.; Beury, D.W.; Clements, V.K. Cross-talk between myeloid-derived suppressor cells (MDSC), macrophages, and dendritic cells enhances tumor-induced immune suppression. Semin. Cancer Biol. 2012, 22, 275–281. [Google Scholar] [CrossRef] [Green Version]
- Sfanos, K.S.; Bruno, T.C.; Maris, C.H.; Xu, L.; Thoburn, C.J.; DeMarzo, A.M.; Meeker, A.K.; Isaacs, W.B.; Drake, C.G. Phenotypic analysis of prostate-infiltrating lymphocytes reveals TH17 and Treg skewing. Clin. Cancer Res. 2008, 14, 3254–3261. [Google Scholar] [CrossRef] [Green Version]
- Kiniwa, Y.; Miyahara, Y.; Wang, H.Y.; Peng, W.; Peng, G.; Wheeler, T.M.; Thompson, T.C.; Old, L.J.; Wang, R.-F. CD8+ Foxp3+ regulatory T cells mediate immunosuppression in prostate cancer. Clin. Cancer Res. 2007, 13, 6947–6958. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, M.; Kanao, K.; Suzuki, S.; Muramatsu, H.; Morinaga, S.; Kajikawa, K.; Kobayashi, I.; Nishikawa, G.; Kato, Y.; Zennami, K.; et al. Increased infiltration of CCR4-positive regulatory T cells in prostate cancer tissue is associated with a poor prognosis. Prostate 2019, 79, 1658–1665. [Google Scholar] [CrossRef]
- Zhang, Q.; Liu, S.; Ge, D.; Cunningham, D.M.; Huang, F.; Ma, L.; Burris, T.P.; You, Z. Targeting Th17-IL-17 Pathway in Prevention of Micro-Invasive Prostate Cancer in a Mouse Model. Prostate 2017, 77, 888–899. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Liu, F.; Zhang, B.; Yan, P.; Rowan, B.G.; Abdel-Mageed, A.B.; Steele, C.; Jazwinski, S.M.; Moroz, K.; Norton, E.B.; et al. CD4+ T helper 17 cell response of aged mice promotes prostate cancer cell migration and invasion. Prostate 2020, 80, 764–776. [Google Scholar] [CrossRef] [PubMed]
- Weaver, C.T.; Harrington, L.E.; Mangan, P.R.; Gavrieli, M.; Murphy, K.M. Th17: An effector CD4 T cell lineage with regulatory T cell ties. Immunity 2006, 24, 677–688. [Google Scholar] [CrossRef] [Green Version]
- Simons, B.W.; Durham, N.M.; Bruno, T.C.; Grosso, J.F.; Schaeffer, A.J.; Ross, A.E.; Hurley, P.J.; Berman, D.M.; Drake, C.G.; Thumbikat, P.; et al. A human prostatic bacterial isolate alters the prostatic microenvironment and accelerates prostate cancer progression. J. Pathol. 2015, 235, 478–489. [Google Scholar] [CrossRef]
- Jachetti, E.; Cancila, V.; Rigoni, A.; Bongiovanni, L.; Cappetti, B.; Belmonte, B.; Enriquez, C.; Casalini, P.; Ostano, P.; Frossi, B.; et al. Cross-Talk between Myeloid-Derived Suppressor Cells and Mast Cells Mediates Tumor-Specific Immunosuppression in Prostate Cancer. Cancer Immunol. Res. 2018, 6, 552–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakai, Y.; Nelson, W.G.; De Marzo, A.M. The dietary charred meat carcinogen 2-amino-1-methyl-6-phenylimidazo[4,5-b]pyridine acts as both a tumor initiator and promoter in the rat ventral prostate. Cancer Res. 2007, 67, 1378–1384. [Google Scholar] [CrossRef] [Green Version]
- Sfanos, K.S.; Canene-Adams, K.; Hempel, H.; Yu, S.-H.; Simons, B.W.; Schaeffer, A.J.; Schaeffer, E.M.; Nelson, W.G.; De Marzo, A.M. Bacterial Prostatitis Enhances 2-Amino-1-Methyl-6-Phenylimidazo[4,5-b]Pyridine (PhIP)-Induced Cancer at Multiple Sites. Cancer Prev. Res. 2015, 8, 683–692. [Google Scholar] [CrossRef] [Green Version]
- Weisberg, S.P.; McCann, D.; Desai, M.; Rosenbaum, M.; Leibel, R.L.; Ferrante, A.W. Obesity is associated with macrophage accumulation in adipose tissue. J. Clin. Investig. 2003, 112, 1796–1808. [Google Scholar] [CrossRef]
- Laurent, V.; Guérard, A.; Mazerolles, C.; Le Gonidec, S.; Toulet, A.; Nieto, L.; Zaidi, F.; Majed, B.; Garandeau, D.; Socrier, Y.; et al. Periprostatic adipocytes act as a driving force for prostate cancer progression in obesity. Nat. Commun. 2016, 7, 10230. [Google Scholar] [CrossRef]
- Divella, R.; De Luca, R.; Abbate, I.; Naglieri, E.; Daniele, A. Obesity and cancer: The role of adipose tissue and adipo-cytokines-induced chronic inflammation. J. Cancer 2016, 7, 2346–2359. [Google Scholar] [CrossRef] [Green Version]
- Corrêa, L.H.; Corrêa, R.; Farinasso, C.M.; de Sant’Ana Dourado, L.P.; Magalhães, K.G. Adipocytes and Macrophages Interplay in the Orchestration of Tumor Microenvironment: New Implications in Cancer Progression. Front. Immunol. 2017, 8, 1129. [Google Scholar] [CrossRef] [PubMed]
- Ostrand-Rosenberg, S. Myeloid derived-suppressor cells: Their role in cancer and obesity. Curr. Opin. Immunol. 2018, 51, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Nassar, Z.D.; Aref, A.T.; Miladinovic, D.; Mah, C.Y.; Raj, G.V.; Hoy, A.J.; Butler, L.M. Peri-prostatic adipose tissue: The metabolic microenvironment of prostate cancer. BJU Int. 2018, 121, 9–21. [Google Scholar] [CrossRef] [Green Version]
- Quail, D.F.; Dannenberg, A.J. The obese adipose tissue microenvironment in cancer development and progression. Nat. Rev. Endocrinol. 2019, 15, 139–154. [Google Scholar] [CrossRef] [PubMed]
- Narita, S.; Nara, T.; Sato, H.; Koizumi, A.; Huang, M.; Inoue, T.; Habuchi, T. Research Evidence on High-Fat Diet-Induced Prostate Cancer Development and Progression. J. Clin. Med. 2019, 8, 597. [Google Scholar] [CrossRef] [Green Version]
- Ito, Y.; Ishiguro, H.; Kobayashi, N.; Hasumi, H.; Watanabe, M.; Yao, M.; Uemura, H. Adipocyte-derived monocyte chemotactic protein-1 (MCP-1) promotes prostate cancer progression through the induction of MMP-2 activity. Prostate 2015, 75, 1009–1019. [Google Scholar] [CrossRef]
- Huang, M.; Narita, S.; Numakura, K.; Tsuruta, H.; Saito, M.; Inoue, T.; Horikawa, Y.; Tsuchiya, N.; Habuchi, T. A high-fat diet enhances proliferation of prostate cancer cells and activates MCP-1/CCR2 signaling. Prostate 2012, 72, 1779–1788. [Google Scholar] [CrossRef]
- Xia, S.; Sha, H.; Yang, L.; Ji, Y.; Ostrand-Rosenberg, S.; Qi, L. Gr-1+ CD11b+ myeloid-derived suppressor cells suppress inflammation and promote insulin sensitivity in obesity. J. Biol. Chem. 2011, 286, 23591–23599. [Google Scholar] [CrossRef] [Green Version]
- Veglia, F.; Perego, M.; Gabrilovich, D. Myeloid-derived suppressor cells coming of age. Nat. Immunol. 2018, 19, 108–119. [Google Scholar] [CrossRef]
- Wang, G.; Lu, X.; Dey, P.; Deng, P.; Wu, C.C.; Jiang, S.; Fang, Z.; Zhao, K.; Konaparthi, R.; Hua, S.; et al. Targeting YAP-Dependent MDSC Infiltration Impairs Tumor Progression. Cancer Discov. 2016, 6, 80–95. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, T.; Fujita, K.; Nojima, S.; Hayashi, Y.; Nakano, K.; Ishizuya, Y.; Wang, C.; Yamamoto, Y.; Kinouchi, T.; Matsuzaki, K.; et al. High-Fat Diet-Induced Inflammation Accelerates Prostate Cancer Growth via IL6 Signaling. Clin. Cancer Res. 2018, 24, 4309–4318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Silva, A.P.B.; Alluri, L.S.C.; Bissada, N.F.; Gupta, S. Association between oral pathogens and prostate cancer: Building the relationship. Am. J. Clin. Exp. Urol. 2019, 7, 1–10. [Google Scholar] [PubMed]
- Wheeler, K.M.; Liss, M.A. The Microbiome and Prostate Cancer Risk. Curr. Urol. Rep. 2019, 20, 66. [Google Scholar] [CrossRef] [PubMed]
- Leitzmann, M.F.; Platz, E.A.; Stampfer, M.J.; Willett, W.C.; Giovannucci, E. Ejaculation frequency and subsequent risk of prostate cancer. JAMA 2004, 291, 1578–1586. [Google Scholar] [CrossRef] [PubMed]
- Rider, J.R.; Wilson, K.M.; Sinnott, J.A.; Kelly, R.S.; Mucci, L.A.; Giovannucci, E.L. Ejaculation Frequency and Risk of Prostate Cancer: Updated Results with an Additional Decade of Follow-up. Eur. Urol. 2016, 70, 974–982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, S.; Guo, J.; Yun, B.H.; Villalta, P.W.; Krishna, S.; Tejpaul, R.; Murugan, P.; Weight, C.J.; Turesky, R.J. Biomonitoring DNA Adducts of Cooked Meat Carcinogens in Human Prostate by Nano Liquid Chromatography-High Resolution Tandem Mass Spectrometry: Identification of 2-Amino-1-methyl-6-phenylimidazo[4,5-b]pyridine DNA Adduct. Anal. Chem. 2016, 88, 12508–12515. [Google Scholar] [CrossRef] [Green Version]
- Rohrmann, S.; Nimptsch, K.; Sinha, R.; Willett, W.C.; Giovannucci, E.L.; Platz, E.A.; Wu, K. Intake of Meat Mutagens and Risk of Prostate Cancer in a Cohort of U.S. Health Professionals. Cancer Epidemiol. Biomark. Prev. 2015, 24, 1557–1563. [Google Scholar] [CrossRef] [Green Version]
- Fowler, M.E.; Akinyemiju, T.F. Meta-analysis of the association between dietary inflammatory index (DII) and cancer outcomes. Int. J. Cancer 2017, 141, 2215–2227. [Google Scholar] [CrossRef] [Green Version]
- Moradi, S.; Issah, A.; Mohammadi, H.; Mirzaei, K. Associations between dietary inflammatory index and incidence of breast and prostate cancer: A systematic review and meta-analysis. Nutrition 2018, 55–56, 168–178. [Google Scholar] [CrossRef]
- Zahedi, H.; Djalalinia, S.; Asayesh, H.; Mansourian, M.; Esmaeili Abdar, Z.; Mahdavi Gorabi, A.; Ansari, H.; Noroozi, M.; Qorbani, M. A Higher Dietary Inflammatory Index Score is associated with a Higher Risk of Incidence and Mortality of Cancer: A Comprehensive Systematic Review and Meta-Analysis. Int. J. Prev. Med. 2020, 11, 15. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, P.; Henning, S.M.; Schokrpur, S.; Wu, L.; Doan, N.; Said, J.; Grogan, T.; Elashoff, D.; Cohen, P.; Aronson, W.J. Effect of Dietary Omega-3 Fatty Acids on Tumor-Associated Macrophages and Prostate Cancer Progression. Prostate 2016, 76, 1293–1302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, P.; Henning, S.M.; Guan, J.; Grogan, T.; Elashoff, D.; Cohen, P.; Aronson, W.J. Effect of dietary omega-3 fatty acids on castrate-resistant prostate cancer and tumor-associated macrophages. Prostate Cancer Prostatic Dis. 2020, 23, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Calle, E.E.; Rodriguez, C.; Walker-Thurmond, K.; Thun, M.J. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N. Engl. J. Med. 2003, 348, 1625–1638. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.; Zhang, J.; Sampieri, K.; Clohessy, J.G.; Mendez, L.; Gonzalez-Billalabeitia, E.; Liu, X.-S.; Lee, Y.-R.; Fung, J.; Katon, J.M.; et al. An aberrant SREBP-dependent lipogenic program promotes metastatic prostate cancer. Nat. Genet. 2018, 50, 206–218. [Google Scholar] [CrossRef] [Green Version]
- Thompson, I.M.; Cabang, A.B.; Wargovich, M.J. Future directions in the prevention of prostate cancer. Nat. Rev. Clin. Oncol. 2014, 11, 49–60. [Google Scholar] [CrossRef] [Green Version]
- Mohsenzadegan, M.; Seif, F.; Farajollahi, M.M.; Khoshmirsafa, M. Anti-Oxidants as Chemopreventive Agents in Prostate Cancer: A Gap Between Preclinical and Clinical Studies. Recent Pat. Anticancer Drug Discov. 2018, 13, 224–239. [Google Scholar] [CrossRef]
- Campi, R.; Brookman-May, S.D.; Subiela Henríquez, J.D.; Akdoğan, B.; Brausi, M.; Klatte, T.; Langenhuijsen, J.F.; Linares-Espinos, E.; Marszalek, M.; Roupret, M.; et al. Impact of Metabolic Diseases, Drugs, and Dietary Factors on Prostate Cancer Risk, Recurrence, and Survival: A Systematic Review by the European Association of Urology Section of Oncological Urology. Eur. Urol. Focus 2019, 5, 1029–1057. [Google Scholar] [CrossRef]
- Cao, Y.; Nishihara, R.; Wu, K.; Wang, M.; Ogino, S.; Willett, W.C.; Spiegelman, D.; Fuchs, C.S.; Giovannucci, E.L.; Chan, A.T. Population-wide Impact of Long-term Use of Aspirin and the Risk for Cancer. JAMA Oncol. 2016, 2, 762–769. [Google Scholar] [CrossRef] [Green Version]
- Downer, M.K.; Allard, C.B.; Preston, M.A.; Gaziano, J.M.; Stampfer, M.J.; Mucci, L.A.; Batista, J.L. Regular Aspirin Use and the Risk of Lethal Prostate Cancer in the Physicians’ Health Study. Eur. Urol. 2017, 72, 821–827. [Google Scholar] [CrossRef]
- Vidal, A.C.; Howard, L.E.; Moreira, D.M.; Castro-Santamaria, R.; Andriole, G.L.; Freedland, S.J. Aspirin, NSAIDs, and risk of prostate cancer: Results from the REDUCE study. Clin. Cancer Res. 2015, 21, 756–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhillon, P.K.; Kenfield, S.A.; Stampfer, M.J.; Giovannucci, E.L. Long-term aspirin use and the risk of total, high-grade, regionally advanced and lethal prostate cancer in a prospective cohort of health professionals, 1988–2006. Int. J. Cancer 2011, 128, 2444–2452. [Google Scholar] [CrossRef] [PubMed]
- Shebl, F.M.; Sakoda, L.C.; Black, A.; Koshiol, J.; Andriole, G.L.; Grubb, R.; Church, T.R.; Chia, D.; Zhou, C.; Chu, L.W.; et al. Aspirin but not ibuprofen use is associated with reduced risk of prostate cancer: A PLCO study. Br. J. Cancer 2012, 107, 207–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choe, K.S.; Cowan, J.E.; Chan, J.M.; Carroll, P.R.; D’Amico, A.V.; Liauw, S.L. Aspirin use and the risk of prostate cancer mortality in men treated with prostatectomy or radiotherapy. J. Clin. Oncol. 2012, 30, 3540–3544. [Google Scholar] [CrossRef]
- Jacobs, E.J.; Newton, C.C.; Stevens, V.L.; Campbell, P.T.; Freedland, S.J.; Gapstur, S.M. Daily aspirin use and prostate cancer-specific mortality in a large cohort of men with nonmetastatic prostate cancer. J. Clin. Oncol. 2014, 32, 3716–3722. [Google Scholar] [CrossRef] [PubMed]
- Skriver, C.; Dehlendorff, C.; Borre, M.; Brasso, K.; Larsen, S.B.; Dalton, S.O.; Nørgaard, M.; Pottegård, A.; Hallas, J.; Sørensen, H.T.; et al. Use of Low-Dose Aspirin and Mortality After Prostate Cancer Diagnosis: A Nationwide Cohort Study. Ann. Intern. Med. 2019, 170, 443–452. [Google Scholar] [CrossRef]
- Solomon, S.D.; Wittes, J.; Finn, P.V.; Fowler, R.; Viner, J.; Bertagnolli, M.M.; Arber, N.; Levin, B.; Meinert, C.L.; Martin, B.; et al. Cardiovascular risk of celecoxib in 6 randomized placebo-controlled trials: The cross trial safety analysis. Circulation 2008, 117, 2104–2113. [Google Scholar] [CrossRef]
- McGettigan, P.; Henry, D. Cardiovascular risk with non-steroidal anti-inflammatory drugs: Systematic review of population-based controlled observational studies. PLoS Med. 2011, 8, e1001098. [Google Scholar] [CrossRef]
- James, N.D.; Sydes, M.R.; Mason, M.D.; Clarke, N.W.; Anderson, J.; Dearnaley, D.P.; Dwyer, J.; Jovic, G.; Ritchie, A.W.S.; Russell, J.M.; et al. Celecoxib plus hormone therapy versus hormone therapy alone for hormone-sensitive prostate cancer: First results from the STAMPEDE multiarm, multistage, randomised controlled trial. Lancet Oncol. 2012, 13, 549–558. [Google Scholar] [CrossRef] [Green Version]
- Mason, M.D.; Clarke, N.W.; James, N.D.; Dearnaley, D.P.; Spears, M.R.; Ritchie, A.W.S.; Attard, G.; Cross, W.; Jones, R.J.; Parker, C.C.; et al. Adding Celecoxib With or Without Zoledronic Acid for Hormone-Naïve Prostate Cancer: Long-Term Survival Results from an Adaptive, Multiarm, Multistage, Platform, Randomized Controlled Trial. J. Clin. Oncol. 2017, 35, 1530–1541. [Google Scholar] [CrossRef] [Green Version]
- Nobes, J.P.; Langley, S.E.M.; Klopper, T.; Russell-Jones, D.; Laing, R.W. A prospective, randomized pilot study evaluating the effects of metformin and lifestyle intervention on patients with prostate cancer receiving androgen deprivation therapy. BJU Int. 2012, 109, 1495–1502. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Hu, H.; Ye, S.; Wang, H.; Cui, R.; Yi, L. The effect of metformin therapy on incidence and prognosis in prostate cancer: A systematic review and meta-analysis. Sci. Rep. 2019, 9, 2218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- 183. Scandinavian Simvastatin Survival Study Group. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: The Scandinavian Simvastatin Survival Study (4S). Lancet 1994, 344, 1383–1389.
- Bansal, D.; Undela, K.; D’Cruz, S.; Schifano, F. Statin use and risk of prostate cancer: A meta-analysis of observational studies. PLoS ONE 2012, 7, e46691. [Google Scholar] [CrossRef]
- Nielsen, S.F.; Nordestgaard, B.G.; Bojesen, S.E. Statin use and reduced cancer-related mortality. N. Engl. J. Med. 2012, 367, 1792–1802. [Google Scholar] [CrossRef] [Green Version]
- Larsen, S.B.; Dehlendorff, C.; Skriver, C.; Dalton, S.O.; Jespersen, C.G.; Borre, M.; Brasso, K.; Nørgaard, M.; Johansen, C.; Sørensen, H.T.; et al. Postdiagnosis Statin Use and Mortality in Danish Patients With Prostate Cancer. J. Clin. Oncol. 2017, 35, 3290–3297. [Google Scholar] [CrossRef]
- Meng, Y.; Liao, Y.-B.; Xu, P.; Wei, W.-R.; Wang, J. Statin use and mortality of patients with prostate cancer: A meta-analysis. Onco Targets Ther. 2016, 9, 1689–1696. [Google Scholar] [CrossRef] [Green Version]
- Bardia, A.; Platz, E.A.; Yegnasubramanian, S.; De Marzo, A.M.; Nelson, W.G. Anti-inflammatory drugs, antioxidants, and prostate cancer prevention. Curr. Opin. Pharm. 2009, 9, 419–426. [Google Scholar] [CrossRef] [Green Version]
- Veitonmäki, T.; Murtola, T.J.; Määttänen, L.; Taari, K.; Stenman, U.-H.; Tammela, T.L.J.; Auvinen, A. Prostate cancer risk and nonsteroidal antiinflammatory drug use in the Finnish prostate cancer screening trial. Br. J. Cancer 2014, 111, 1421–1431. [Google Scholar] [CrossRef]
- Coyle, C.; Cafferty, F.H.; Rowley, S.; MacKenzie, M.; Berkman, L.; Gupta, S.; Pramesh, C.S.; Gilbert, D.; Kynaston, H.; Cameron, D.; et al. ADD-ASPIRIN: A phase III, double-blind, placebo controlled, randomised trial assessing the effects of aspirin on disease recurrence and survival after primary therapy in common non-metastatic solid tumours. Contemp. Clin. Trials 2016, 51, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Lichtenberger, L.M.; Fang, D.; Bick, R.J.; Poindexter, B.J.; Phan, T.; Bergeron, A.L.; Pradhan, S.; Dial, E.J.; Vijayan, K.V. Unlocking Aspirin’s Chemopreventive Activity: Role of Irreversibly Inhibiting Platelet Cyclooxygenase-1. Cancer Prev. Res. 2017, 10, 142–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Z.; Chen, F.; Shang, L. Advances in antitumor effects of NSAIDs. Cancer Manag. Res. 2018, 10, 4631–4640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hua, H.; Zhang, H.; Kong, Q.; Wang, J.; Jiang, Y. Complex roles of the old drug aspirin in cancer chemoprevention and therapy. Med. Res. Rev. 2019, 39, 114–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashemi Goradel, N.; Najafi, M.; Salehi, E.; Farhood, B.; Mortezaee, K. Cyclooxygenase-2 in cancer: A review. J. Cell. Physiol. 2019, 234, 5683–5699. [Google Scholar] [CrossRef]
- Wang, W.; Bergh, A.; Damber, J.-E. Cyclooxygenase-2 expression correlates with local chronic inflammation and tumor neovascularization in human prostate cancer. Clin. Cancer Res. 2005, 11, 3250–3256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, S.; Adhami, V.M.; Subbarayan, M.; MacLennan, G.T.; Lewin, J.S.; Hafeli, U.O.; Fu, P.; Mukhtar, H. Suppression of prostate carcinogenesis by dietary supplementation of celecoxib in transgenic adenocarcinoma of the mouse prostate model. Cancer Res. 2004, 64, 3334–3343. [Google Scholar] [CrossRef] [Green Version]
- Jain, S.; Chakraborty, G.; Kundu, G.C. The crucial role of cyclooxygenase-2 in osteopontin-induced protein kinase C alpha/c-Src/IkappaB kinase alpha/beta-dependent prostate tumor progression and angiogenesis. Cancer Res. 2006, 66, 6638–6648. [Google Scholar] [CrossRef] [Green Version]
- Jain, S.; Chakraborty, G.; Raja, R.; Kale, S.; Kundu, G.C. Prostaglandin E2 regulates tumor angiogenesis in prostate cancer. Cancer Res. 2008, 68, 7750–7759. [Google Scholar] [CrossRef] [Green Version]
- Abedinpour, P.; Baron, V.T.; Welsh, J.; Borgström, P. Regression of prostate tumors upon combination of hormone ablation therapy and celecoxib in vivo. Prostate 2011, 71, 813–823. [Google Scholar] [CrossRef] [Green Version]
- Bieniek, J.; Childress, C.; Swatski, M.D.; Yang, W. COX-2 inhibitors arrest prostate cancer cell cycle progression by down-regulation of kinetochore/centromere proteins. Prostate 2014, 74, 999–1011. [Google Scholar] [CrossRef]
- Garg, R.; Blando, J.M.; Perez, C.J.; Lal, P.; Feldman, M.D.; Smyth, E.M.; Ricciotti, E.; Grosser, T.; Benavides, F.; Kazanietz, M.G. COX-2 mediates pro-tumorigenic effects of PKCε in prostate cancer. Oncogene 2018, 37, 4735–4749. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, E.; Shiota, M.; Yokomizo, A.; Inokuchi, J.; Uchiumi, T.; Naito, S. EP2 signaling mediates suppressive effects of celecoxib on androgen receptor expression and cell proliferation in prostate cancer. Prostate Cancer Prostatic Dis. 2014, 17, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Benelli, R.; Barboro, P.; Costa, D.; Astigiano, S.; Barbieri, O.; Capaia, M.; Poggi, A.; Ferrari, N. Multifocal Signal Modulation Therapy by Celecoxib: A Strategy for Managing Castration-Resistant Prostate Cancer. Int. J. Mol. Sci. 2019, 20, 6091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, S.; Yang, S.-C.; Zhu, L.; Reckamp, K.; Gardner, B.; Baratelli, F.; Huang, M.; Batra, R.K.; Dubinett, S.M. Tumor cyclooxygenase-2/prostaglandin E2-dependent promotion of FOXP3 expression and CD4+ CD25+ T regulatory cell activities in lung cancer. Cancer Res. 2005, 65, 5211–5220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujita, M.; Kohanbash, G.; Fellows-Mayle, W.; Hamilton, R.L.; Komohara, Y.; Decker, S.A.; Ohlfest, J.R.; Okada, H. COX-2 blockade suppresses gliomagenesis by inhibiting myeloid-derived suppressor cells. Cancer Res. 2011, 71, 2664–2674. [Google Scholar] [CrossRef] [Green Version]
- Zelenay, S.; van der Veen, A.G.; Böttcher, J.P.; Snelgrove, K.J.; Rogers, N.; Acton, S.E.; Chakravarty, P.; Girotti, M.R.; Marais, R.; Quezada, S.A.; et al. Cyclooxygenase-Dependent Tumor Growth through Evasion of Immunity. Cell 2015, 162, 1257–1270. [Google Scholar] [CrossRef] [Green Version]
- Peng, Y.; Shi, J.; Du, X.; Wang, L.; Klocker, H.; Mo, L.; Mo, Z.; Zhang, J. Prostaglandin E2 induces stromal cell-derived factor-1 expression in prostate stromal cells by activating protein kinase A and transcription factor Sp1. Int. J. Biochem. Cell Biol. 2013, 45, 521–530. [Google Scholar] [CrossRef]
- Markosyan, N.; Chen, E.P.; Evans, R.A.; Ndong, V.; Vonderheide, R.H.; Smyth, E.M. Mammary carcinoma cell derived cyclooxygenase 2 suppresses tumor immune surveillance by enhancing intratumoral immune checkpoint activity. Breast Cancer Res. 2013, 15, R75. [Google Scholar] [CrossRef] [Green Version]
- Na, Y.-R.; Yoon, Y.-N.; Son, D.-I.; Seok, S.-H. Cyclooxygenase-2 inhibition blocks M2 macrophage differentiation and suppresses metastasis in murine breast cancer model. PLoS ONE 2013, 8, e63451. [Google Scholar] [CrossRef] [Green Version]
- Sooriakumaran, P.; Macanas-Pirard, P.; Bucca, G.; Henderson, A.; Langley, S.E.M.; Laing, R.W.; Smith, C.P.; Laing, E.E.; Coley, H.M. A gene expression profiling approach assessing celecoxib in a randomized controlled trial in prostate cancer. Cancer Genom. Proteom. 2009, 6, 93–99. [Google Scholar]
- Sooriakumaran, P.; Coley, H.M.; Fox, S.B.; Macanas-Pirard, P.; Lovell, D.P.; Henderson, A.; Eden, C.G.; Miller, P.D.; Langley, S.E.M.; Laing, R.W. A randomized controlled trial investigating the effects of celecoxib in patients with localized prostate cancer. Anticancer Res. 2009, 29, 1483–1488. [Google Scholar]
- Antonarakis, E.S.; Heath, E.I.; Walczak, J.R.; Nelson, W.G.; Fedor, H.; De Marzo, A.M.; Zahurak, M.L.; Piantadosi, S.; Dannenberg, A.J.; Gurganus, R.T.; et al. Phase II, randomized, placebo-controlled trial of neoadjuvant celecoxib in men with clinically localized prostate cancer: Evaluation of drug-specific biomarkers. J. Clin. Oncol. 2009, 27, 4986–4993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braga-Basaria, M.; Dobs, A.S.; Muller, D.C.; Carducci, M.A.; John, M.; Egan, J.; Basaria, S. Metabolic syndrome in men with prostate cancer undergoing long-term androgen-deprivation therapy. J. Clin. Oncol. 2006, 24, 3979–3983. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, H.; Daneshmand, S. Androgen deprivation therapy: Evidence-based management of side effects. BJU Int. 2013, 111, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Clements, A.; Gao, B.; Yeap, S.H.O.; Wong, M.K.Y.; Ali, S.S.; Gurney, H. Metformin in prostate cancer: Two for the price of one. Ann. Oncol. 2011, 22, 2556–2560. [Google Scholar] [CrossRef]
- Jayalath, V.H.; Ireland, C.; Fleshner, N.E.; Hamilton, R.J.; Jenkins, D.J.A. The Relationship between Metformin and Serum Prostate-Specific Antigen Levels. Prostate 2016, 76, 1445–1453. [Google Scholar] [CrossRef]
- Whitburn, J.; Edwards, C.M.; Sooriakumaran, P. Metformin and Prostate Cancer: A New Role for an Old Drug. Curr. Urol. Rep. 2017, 18, 46. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.; Tong, D.; Liu, G.; Gao, J.; Wang, L.-A.; Xu, J.; Yang, X.; Xie, Q.; Huang, Y.; Pang, J.; et al. Metformin Inhibits Prostate Cancer Progression by Targeting Tumor-Associated Inflammatory Infiltration. Clin. Cancer Res. 2018, 24, 5622–5634. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, T.; Fujita, K.; Matsushita, M.; Hayashi, Y.; Uemura, M.; Nonomura, N. Metformin inhibits prostate cancer growth induced by a high-fat diet in Pten-deficient model mice. Int. J. Urol. 2019, 26, 307–309. [Google Scholar] [CrossRef] [Green Version]
- Cyrus-David, M.S.; Weinberg, A.; Thompson, T.; Kadmon, D. The effect of statins on serum prostate specific antigen levels in a cohort of airline pilots: A preliminary report. J. Urol. 2005, 173, 1923–1925. [Google Scholar] [CrossRef]
- Hamilton, R.J.; Goldberg, K.C.; Platz, E.A.; Freedland, S.J. The influence of statin medications on prostate-specific antigen levels. J. Natl. Cancer Inst. 2008, 100, 1511–1518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, S.L.; Harshman, L.C.; Presti, J.C. Impact of common medications on serum total prostate-specific antigen levels: Analysis of the National Health and Nutrition Examination Survey. J. Clin. Oncol. 2010, 28, 3951–3957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Y.; Fung, K.Z.; Freedland, S.J.; Hoffman, R.M.; Tang, V.L.; Walter, L.C. Statin medications are associated with a lower probability of having an abnormal screening prostate-specific antigen result. Urology 2014, 84, 1058–1065. [Google Scholar] [CrossRef] [Green Version]
- Alfaqih, M.A.; Allott, E.H.; Hamilton, R.J.; Freeman, M.R.; Freedland, S.J. The current evidence on statin use and prostate cancer prevention: Are we there yet? Nat. Rev. Urol. 2017, 14, 107–119. [Google Scholar] [CrossRef] [Green Version]
- Romano, M.; Diomede, L.; Sironi, M.; Massimiliano, L.; Sottocorno, M.; Polentarutti, N.; Guglielmotti, A.; Albani, D.; Bruno, A.; Fruscella, P.; et al. Inhibition of monocyte chemotactic protein-1 synthesis by statins. Lab. Investig. 2000, 80, 1095–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimizu, K.; Aikawa, M.; Takayama, K.; Libby, P.; Mitchell, R.N. Direct anti-inflammatory mechanisms contribute to attenuation of experimental allograft arteriosclerosis by statins. Circulation 2003, 108, 2113–2120. [Google Scholar] [CrossRef] [Green Version]
- Coussens, L.M.; Zitvogel, L.; Palucka, A.K. Neutralizing tumor-promoting chronic inflammation: A magic bullet? Science 2013, 339, 286–291. [Google Scholar] [CrossRef] [Green Version]
- Ruffell, B.; Coussens, L.M. Macrophages and therapeutic resistance in cancer. Cancer Cell 2015, 27, 462–472. [Google Scholar] [CrossRef] [Green Version]
- Petty, A.J.; Yang, Y. Tumor-associated macrophages: Implications in cancer immunotherapy. Immunotherapy 2017, 9, 289–302. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.M.; Recht, L.; Strober, S. The Promise of Targeting Macrophages in Cancer Therapy. Clin. Cancer Res. 2017, 23, 3241–3250. [Google Scholar] [CrossRef] [Green Version]
- Cassetta, L.; Kitamura, T. Macrophage targeting: Opening new possibilities for cancer immunotherapy. Immunology 2018, 155, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Cassetta, L.; Pollard, J.W. Targeting macrophages: Therapeutic approaches in cancer. Nat. Rev. Drug Discov. 2018, 17, 887–904. [Google Scholar] [CrossRef] [PubMed]
- Pathria, P.; Louis, T.L.; Varner, J.A. Targeting Tumor-Associated Macrophages in Cancer. Trends Immunol. 2019, 40, 310–327. [Google Scholar] [CrossRef]
- Gabrilovich, D.I. Myeloid-Derived Suppressor Cells. Cancer Immunol. Res. 2017, 5, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Lopez-Bujanda, Z.; Drake, C.G. Myeloid-derived cells in prostate cancer progression: Phenotype and prospective therapies. J. Leukoc. Biol. 2017, 102, 393–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleming, V.; Hu, X.; Weber, R.; Nagibin, V.; Groth, C.; Altevogt, P.; Utikal, J.; Umansky, V. Targeting Myeloid-Derived Suppressor Cells to Bypass Tumor-Induced Immunosuppression. Front. Immunol. 2018, 9, 398. [Google Scholar] [CrossRef]
- Weber, R.; Fleming, V.; Hu, X.; Nagibin, V.; Groth, C.; Altevogt, P.; Utikal, J.; Umansky, V. Myeloid-Derived Suppressor Cells Hinder the Anti-Cancer Activity of Immune Checkpoint Inhibitors. Front. Immunol. 2018, 9, 1310. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Wei, G.; Cheng, W.A.; Dong, Z.; Sun, H.; Lee, V.Y.; Cha, S.-C.; Smith, D.L.; Kwak, L.W.; Qin, H. Targeting myeloid-derived suppressor cells for cancer immunotherapy. Cancer Immunol. Immunother. 2018, 67, 1181–1195. [Google Scholar] [CrossRef]
- Park, S.-M.; Youn, J.-I. Role of myeloid-derived suppressor cells in immune checkpoint inhibitor therapy in cancer. Arch. Pharm. Res. 2019, 42, 560–566. [Google Scholar] [CrossRef]
- Law, A.M.K.; Valdes-Mora, F.; Gallego-Ortega, D. Myeloid-Derived Suppressor Cells as a Therapeutic Target for Cancer. Cells 2020, 9, 561. [Google Scholar] [CrossRef] [Green Version]
- George, D.J.; Halabi, S.; Shepard, T.F.; Sanford, B.; Vogelzang, N.J.; Small, E.J.; Kantoff, P.W. The prognostic significance of plasma interleukin-6 levels in patients with metastatic hormone-refractory prostate cancer: Results from cancer and leukemia group B 9480. Clin. Cancer Res. 2005, 11, 1815–1820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, D.P.; Li, J.; Tewari, A.K. Inflammation and prostate cancer: The role of interleukin 6 (IL-6). BJU Int. 2014, 113, 986–992. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.E.; O′Keefe, R.A.; Grandis, J.R. Targeting the IL-6/JAK/STAT3 signalling axis in cancer. Nat. Rev. Clin. Oncol. 2018, 15, 234–248. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-T.; Hsieh, C.-C.; Lin, C.-C.; Chen, W.-C.; Hong, J.-H.; Chen, M.-F. Significance of IL-6 in the transition of hormone-resistant prostate cancer and the induction of myeloid-derived suppressor cells. J. Mol. Med. 2012, 90, 1343–1355. [Google Scholar] [CrossRef]
- Kitamura, H.; Ohno, Y.; Toyoshima, Y.; Ohtake, J.; Homma, S.; Kawamura, H.; Takahashi, N.; Taketomi, A. Interleukin-6/STAT3 signaling as a promising target to improve the efficacy of cancer immunotherapy. Cancer Sci. 2017, 108, 1947–1952. [Google Scholar] [CrossRef]
- Kortylewski, M.; Kujawski, M.; Wang, T.; Wei, S.; Zhang, S.; Pilon-Thomas, S.; Niu, G.; Kay, H.; Mulé, J.; Kerr, W.G.; et al. Inhibiting Stat3 signaling in the hematopoietic system elicits multicomponent antitumor immunity. Nat. Med. 2005, 11, 1314–1321. [Google Scholar] [CrossRef]
- Yu, H.; Pardoll, D.; Jove, R. STATs in cancer inflammation and immunity: A leading role for STAT3. Nat. Rev. Cancer 2009, 9, 798–809. [Google Scholar] [CrossRef]
- Hellsten, R.; Lilljebjörn, L.; Johansson, M.; Leandersson, K.; Bjartell, A. The STAT3 inhibitor galiellalactone inhibits the generation of MDSC-like monocytes by prostate cancer cells and decreases immunosuppressive and tumorigenic factors. Prostate 2019, 79, 1611–1621. [Google Scholar] [CrossRef] [Green Version]
- Van Rhee, F.; Wong, R.S.; Munshi, N.; Rossi, J.-F.; Ke, X.-Y.; Fosså, A.; Simpson, D.; Capra, M.; Liu, T.; Hsieh, R.K.; et al. Siltuximab for multicentric Castleman’s disease: A randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2014, 15, 966–974. [Google Scholar] [CrossRef]
- Wallner, L.; Dai, J.; Escara-Wilke, J.; Zhang, J.; Yao, Z.; Lu, Y.; Trikha, M.; Nemeth, J.A.; Zaki, M.H.; Keller, E.T. Inhibition of interleukin-6 with CNTO328, an anti-interleukin-6 monoclonal antibody, inhibits conversion of androgen-dependent prostate cancer to an androgen-independent phenotype in orchiectomized mice. Cancer Res. 2006, 66, 3087–3095. [Google Scholar] [CrossRef] [Green Version]
- Dorff, T.B.; Goldman, B.; Pinski, J.K.; Mack, P.C.; Lara, P.N.; Van Veldhuizen, P.J.; Quinn, D.I.; Vogelzang, N.J.; Thompson, I.M.; Hussain, M.H.A. Clinical and correlative results of SWOG S0354: A phase II trial of CNTO328 (siltuximab), a monoclonal antibody against interleukin-6, in chemotherapy-pretreated patients with castration-resistant prostate cancer. Clin. Cancer Res. 2010, 16, 3028–3034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fizazi, K.; De Bono, J.S.; Flechon, A.; Heidenreich, A.; Voog, E.; Davis, N.B.; Qi, M.; Bandekar, R.; Vermeulen, J.T.; Cornfeld, M.; et al. Randomised phase II study of siltuximab (CNTO 328), an anti-IL-6 monoclonal antibody, in combination with mitoxantrone/prednisone versus mitoxantrone/prednisone alone in metastatic castration-resistant prostate cancer. Eur. J. Cancer 2012, 48, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Karkera, J.; Steiner, H.; Li, W.; Skradski, V.; Moser, P.L.; Riethdorf, S.; Reddy, M.; Puchalski, T.; Safer, K.; Prabhakar, U.; et al. The anti-interleukin-6 antibody siltuximab down-regulates genes implicated in tumorigenesis in prostate cancer patients from a phase I study. Prostate 2011, 71, 1455–1465. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Mook, R.A.; Premont, R.T.; Wang, J. Niclosamide: Beyond an antihelminthic drug. Cell. Signal. 2018, 41, 89–96. [Google Scholar] [CrossRef]
- Sekulovski, N.; Whorton, A.E.; Tanaka, T.; Hirota, Y.; Shi, M.; MacLean, J.A.; de Mola, J.R.L.; Groesch, K.; Diaz-Sylvester, P.; Wilson, T.; et al. Niclosamide suppresses macrophage-induced inflammation in endometriosis. Biol. Reprod. 2020, 102, 1011–1019. [Google Scholar] [CrossRef]
- Liu, C.; Lou, W.; Zhu, Y.; Nadiminty, N.; Schwartz, C.T.; Evans, C.P.; Gao, A.C. Niclosamide inhibits androgen receptor variants expression and overcomes enzalutamide resistance in castration-resistant prostate cancer. Clin. Cancer Res. 2014, 20, 3198–3210. [Google Scholar] [CrossRef] [Green Version]
- Moreira, D.; Adamus, T.; Zhao, X.; Su, Y.-L.; Zhang, Z.; White, S.V.; Swiderski, P.; Lu, X.; DePinho, R.A.; Pal, S.K.; et al. STAT3 Inhibition Combined with CpG Immunostimulation Activates Antitumor Immunity to Eradicate Genetically Distinct Castration-Resistant Prostate Cancers. Clin. Cancer Res. 2018, 24, 5948–5962. [Google Scholar] [CrossRef] [Green Version]
- Ries, C.H.; Cannarile, M.A.; Hoves, S.; Benz, J.; Wartha, K.; Runza, V.; Rey-Giraud, F.; Pradel, L.P.; Feuerhake, F.; Klaman, I.; et al. Targeting tumor-associated macrophages with anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer Cell 2014, 25, 846–859. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Escamilla, J.; Mok, S.; David, J.; Priceman, S.; West, B.; Bollag, G.; McBride, W.; Wu, L. CSF1R signaling blockade stanches tumor-infiltrating myeloid cells and improves the efficacy of radiotherapy in prostate cancer. Cancer Res. 2013, 73, 2782–2794. [Google Scholar] [CrossRef] [Green Version]
- Escamilla, J.; Schokrpur, S.; Liu, C.; Priceman, S.J.; Moughon, D.; Jiang, Z.; Pouliot, F.; Magyar, C.; Sung, J.L.; Xu, J.; et al. CSF1 receptor targeting in prostate cancer reverses macrophage-mediated resistance to androgen blockade therapy. Cancer Res. 2015, 75, 950–962. [Google Scholar] [CrossRef] [Green Version]
- Tap, W.D.; Gelderblom, H.; Palmerini, E.; Desai, J.; Bauer, S.; Blay, J.-Y.; Alcindor, T.; Ganjoo, K.; Martín-Broto, J.; Ryan, C.W.; et al. Pexidartinib versus placebo for advanced tenosynovial giant cell tumour (ENLIVEN): a randomised phase 3 trial. Lancet 2019, 394, 478–487. [Google Scholar] [CrossRef]
- Guan, W.; Hu, J.; Yang, L.; Tan, P.; Tang, Z.; West, B.L.; Bollag, G.; Xu, H.; Wu, L. Inhibition of TAMs improves the response to docetaxel in castration-resistant prostate cancer. Endocr. Relat. Cancer 2019, 26, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, T. The production of monocyte chemoattractant protein-1 (MCP-1)/CCL2 in tumor microenvironments. Cytokine 2017, 98, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, T. The chemokine MCP-1 (CCL2) in the host interaction with cancer: a foe or ally? Cell. Mol. Immunol. 2018, 15, 335–345. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.; Cai, Z.; Galson, D.L.; Xiao, G.; Liu, Y.; George, D.E.; Melhem, M.F.; Yao, Z.; Zhang, J. Monocyte chemotactic protein-1 (MCP-1) acts as a paracrine and autocrine factor for prostate cancer growth and invasion. Prostate 2006, 66, 1311–1318. [Google Scholar] [CrossRef]
- Loberg, R.D.; Day, L.L.; Harwood, J.; Ying, C.; St John, L.N.; Giles, R.; Neeley, C.K.; Pienta, K.J. CCL2 is a potent regulator of prostate cancer cell migration and proliferation. Neoplasia 2006, 8, 578–586. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.; Cai, Z.; Xiao, G.; Liu, Y.; Keller, E.T.; Yao, Z.; Zhang, J. CCR2 expression correlates with prostate cancer progression. J. Cell. Biochem. 2007, 101, 676–685. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Patel, L.; Pienta, K.J. CC chemokine ligand 2 (CCL2) promotes prostate cancer tumorigenesis and metastasis. Cytokine Growth Factor Rev. 2010, 21, 41–48. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Lu, Y.; Pienta, K.J. Multiple roles of chemokine (C-C motif) ligand 2 in promoting prostate cancer growth. J. Natl. Cancer Inst. 2010, 102, 522–528. [Google Scholar] [CrossRef] [Green Version]
- Loberg, R.D.; Ying, C.; Craig, M.; Yan, L.; Snyder, L.A.; Pienta, K.J. CCL2 as an important mediator of prostate cancer growth in vivo through the regulation of macrophage infiltration. Neoplasia 2007, 9, 556–562. [Google Scholar] [CrossRef] [Green Version]
- Loberg, R.D.; Ying, C.; Craig, M.; Day, L.L.; Sargent, E.; Neeley, C.; Wojno, K.; Snyder, L.A.; Yan, L.; Pienta, K.J. Targeting CCL2 with systemic delivery of neutralizing antibodies induces prostate cancer tumor regression in vivo. Cancer Res. 2007, 67, 9417–9424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pienta, K.J.; Machiels, J.-P.; Schrijvers, D.; Alekseev, B.; Shkolnik, M.; Crabb, S.J.; Li, S.; Seetharam, S.; Puchalski, T.A.; Takimoto, C.; et al. Phase 2 study of carlumab (CNTO 888), a human monoclonal antibody against CC-chemokine ligand 2 (CCL2), in metastatic castration-resistant prostate cancer. Investig. New Drugs 2013, 31, 760–768. [Google Scholar] [CrossRef] [PubMed]
- Hughes, R.; Qian, B.-Z.; Rowan, C.; Muthana, M.; Keklikoglou, I.; Olson, O.C.; Tazzyman, S.; Danson, S.; Addison, C.; Clemons, M.; et al. Perivascular M2 Macrophages Stimulate Tumor Relapse after Chemotherapy. Cancer Res. 2015, 75, 3479–3491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, Y.; Cheng, J.; Fu, B.; Liu, W.; Chen, G.; Zhang, Q.; Yang, Y. Hepatic carcinoma-associated fibroblasts enhance immune suppression by facilitating the generation of myeloid-derived suppressor cells. Oncogene 2017, 36, 1090–1101. [Google Scholar] [CrossRef] [PubMed]
- Eckert, F.; Schilbach, K.; Klumpp, L.; Bardoscia, L.; Sezgin, E.C.; Schwab, M.; Zips, D.; Huber, S.M. Potential Role of CXCR4 Targeting in the Context of Radiotherapy and Immunotherapy of Cancer. Front. Immunol. 2018, 9, 3018. [Google Scholar] [CrossRef] [PubMed]
- Teicher, B.A.; Fricker, S.P. CXCL12 (SDF-1)/CXCR4 pathway in cancer. Clin. Cancer Res. 2010, 16, 2927–2931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; Zhong, T. The association of CXCR4 expression with clinicopathological significance and potential drug target in prostate cancer: a meta-analysis and literature review. Drug Des. Dev. Ther. 2015, 9, 5115–5122. [Google Scholar] [CrossRef] [Green Version]
- Gravina, G.L.; Mancini, A.; Muzi, P.; Ventura, L.; Biordi, L.; Ricevuto, E.; Pompili, S.; Mattei, C.; Di Cesare, E.; Jannini, E.A.; et al. CXCR4 pharmacogical inhibition reduces bone and soft tissue metastatic burden by affecting tumor growth and tumorigenic potential in prostate cancer preclinical models. Prostate 2015, 75, 1227–1246. [Google Scholar] [CrossRef]
- Hatano, K.; Yamaguchi, S.; Nimura, K.; Murakami, K.; Nagahara, A.; Fujita, K.; Uemura, M.; Nakai, Y.; Tsuchiya, M.; Nakayama, M.; et al. Residual prostate cancer cells after docetaxel therapy increase the tumorigenic potential via constitutive signaling of CXCR4, ERK1/2 and c-Myc. Mol. Cancer Res. 2013, 11, 1088–1100. [Google Scholar] [CrossRef] [Green Version]
- Saha, A.; Ahn, S.; Blando, J.; Su, F.; Kolonin, M.G.; DiGiovanni, J. Proinflammatory CXCL12-CXCR4/CXCR7 Signaling Axis Drives Myc-Induced Prostate Cancer in Obese Mice. Cancer Res. 2017, 77, 5158–5168. [Google Scholar] [CrossRef] [Green Version]
- Domanska, U.M.; Timmer-Bosscha, H.; Nagengast, W.B.; Oude Munnink, T.H.; Kruizinga, R.C.; Ananias, H.J.K.; Kliphuis, N.M.; Huls, G.; De Vries, E.G.E.; de Jong, I.J.; et al. CXCR4 inhibition with AMD3100 sensitizes prostate cancer to docetaxel chemotherapy. Neoplasia 2012, 14, 709–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Clercq, E. Mozobil® (Plerixafor, AMD3100), 10 years after its approval by the US Food and Drug Administration. Antivir. Chem. Chemother. 2019, 27, 2040206619829382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raymond, E.; Dalgleish, A.; Damber, J.-E.; Smith, M.; Pili, R. Mechanisms of action of tasquinimod on the tumour microenvironment. Cancer Chemother. Pharmacol. 2014, 73, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, N.; Al Ustwani, O.; Shen, L.; Pili, R. Mechanism of action and clinical activity of tasquinimod in castrate-resistant prostate cancer. Onco Targets Ther. 2014, 7, 223–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, L.; Sundstedt, A.; Ciesielski, M.; Miles, K.M.; Celander, M.; Adelaiye, R.; Orillion, A.; Ciamporcero, E.; Ramakrishnan, S.; Ellis, L.; et al. Tasquinimod modulates suppressive myeloid cells and enhances cancer immunotherapies in murine models. Cancer Immunol Res 2015, 3, 136–148. [Google Scholar] [CrossRef] [Green Version]
- Sternberg, C.; Armstrong, A.; Pili, R.; Ng, S.; Huddart, R.; Agarwal, N.; Khvorostenko, D.; Lyulko, O.; Brize, A.; Vogelzang, N.; et al. Randomized, Double-Blind, Placebo-Controlled Phase III Study of Tasquinimod in Men With Metastatic Castration-Resistant Prostate Cancer. J. Clin. Oncol. 2016, 34, 2636–2643. [Google Scholar] [CrossRef]
- Gunderson, A.J.; Kaneda, M.M.; Tsujikawa, T.; Nguyen, A.V.; Affara, N.I.; Ruffell, B.; Gorjestani, S.; Liudahl, S.M.; Truitt, M.; Olson, P.; et al. Bruton Tyrosine Kinase-Dependent Immune Cell Cross-talk Drives Pancreas Cancer. Cancer Discov. 2016, 6, 270–285. [Google Scholar] [CrossRef] [Green Version]
- Molina-Cerrillo, J.; Alonso-Gordoa, T.; Gajate, P.; Grande, E. Bruton’s tyrosine kinase (BTK) as a promising target in solid tumors. Cancer Treat. Rev. 2017, 58, 41–50. [Google Scholar] [CrossRef]
- O′Neill, L.A.J.; Kishton, R.J.; Rathmell, J. A guide to immunometabolism for immunologists. Nat. Rev. Immunol. 2016, 16, 553–565. [Google Scholar] [CrossRef] [Green Version]
- Uyttenhove, C.; Pilotte, L.; Théate, I.; Stroobant, V.; Colau, D.; Parmentier, N.; Boon, T.; Van den Eynde, B.J. Evidence for a tumoral immune resistance mechanism based on tryptophan degradation by indoleamine 2,3-dioxygenase. Nat. Med. 2003, 9, 1269–1274. [Google Scholar] [CrossRef]
- Godin-Ethier, J.; Hanafi, L.-A.; Piccirillo, C.A.; Lapointe, R. Indoleamine 2,3-dioxygenase expression in human cancers: clinical and immunologic perspectives. Clin. Cancer Res. 2011, 17, 6985–6991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prendergast, G.C.; Smith, C.; Thomas, S.; Mandik-Nayak, L.; Laury-Kleintop, L.; Metz, R.; Muller, A.J. Indoleamine 2,3-dioxygenase pathways of pathogenic inflammation and immune escape in cancer. Cancer Immunol. Immunother. 2014, 63, 721–735. [Google Scholar] [CrossRef] [PubMed]
- Prendergast, G.C.; Malachowski, W.P.; DuHadaway, J.B.; Muller, A.J. Discovery of IDO1 Inhibitors: From Bench to Bedside. Cancer Res. 2017, 77, 6795–6811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, E.; Oliver, T.; Rowe, M.; Thomas, S.; Zakharia, Y.; Gilman, P.B.; Muller, A.J.; Prendergast, G.C. Indoximod: An Immunometabolic Adjuvant That Empowers T Cell Activity in Cancer. Front. Oncol. 2018, 8, 370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Velasco, M.A.; Uemura, H. Prostate cancer immunotherapy: where are we and where are we going? Curr. Opin. Urol. 2018, 28, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Boettcher, A.N.; Usman, A.; Morgans, A.; VanderWeele, D.J.; Sosman, J.; Wu, J.D. Past, Current, and Future of Immunotherapies for Prostate Cancer. Front. Oncol. 2019, 9, 884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, X.; Horner, J.W.; Paul, E.; Shang, X.; Troncoso, P.; Deng, P.; Jiang, S.; Chang, Q.; Spring, D.J.; Sharma, P.; et al. Effective combinatorial immunotherapy for castration-resistant prostate cancer. Nature 2017, 543, 728–732. [Google Scholar] [CrossRef] [Green Version]
- Jayaprakash, P.; Ai, M.; Liu, A.; Budhani, P.; Bartkowiak, T.; Sheng, J.; Ager, C.; Nicholas, C.; Jaiswal, A.R.; Sun, Y.; et al. Targeted hypoxia reduction restores T cell infiltration and sensitizes prostate cancer to immunotherapy. J. Clin. Investig. 2018, 128, 5137–5149. [Google Scholar] [CrossRef]
- Feng, S.; Cheng, X.; Zhang, L.; Lu, X.; Chaudhary, S.; Teng, R.; Frederickson, C.; Champion, M.M.; Zhao, R.; Cheng, L.; et al. Myeloid-derived suppressor cells inhibit T cell activation through nitrating LCK in mouse cancers. Proc. Natl. Acad. Sci. USA 2018, 115, 10094–10099. [Google Scholar] [CrossRef] [Green Version]
- Anker, J.F.; Naseem, A.F.; Mok, H.; Schaeffer, A.J.; Abdulkadir, S.A.; Thumbikat, P. Multi-faceted immunomodulatory and tissue-tropic clinical bacterial isolate potentiates prostate cancer immunotherapy. Nat. Commun. 2018, 9, 1591. [Google Scholar] [CrossRef]
Figure 1.
Chronic inflammation is associated with prostate cancer. Pro-inflammatory factors, such as microbiome and dietary components, are the potential cause of prostatic inflammation. Immune cells secrete reactive oxygen and nitrogen species, induce DNA damage and genome instability in prostate epithelium and cause prostate cancer development. Both immune cells and prostate cancer cells secrete intercellular signaling molecules, such as cytokines and chemokines, and contribute to the generation of inflammatory microenvironment, which facilitates cancer progression. Anti-inflammatory agents suppress the “vicious cycle” and inhibit prostate cancer development and progression. NSAIDs, non-steroidal anti-inflammatory drugs; MDSC, myeloid-derived suppressor cell; Treg, regulatory T cell.
Figure 1.
Chronic inflammation is associated with prostate cancer. Pro-inflammatory factors, such as microbiome and dietary components, are the potential cause of prostatic inflammation. Immune cells secrete reactive oxygen and nitrogen species, induce DNA damage and genome instability in prostate epithelium and cause prostate cancer development. Both immune cells and prostate cancer cells secrete intercellular signaling molecules, such as cytokines and chemokines, and contribute to the generation of inflammatory microenvironment, which facilitates cancer progression. Anti-inflammatory agents suppress the “vicious cycle” and inhibit prostate cancer development and progression. NSAIDs, non-steroidal anti-inflammatory drugs; MDSC, myeloid-derived suppressor cell; Treg, regulatory T cell.

Figure 2.
Inflammatory microenvironment in prostate cancer. Diverse mechanisms, such as microbiome, dietary carcinogens, obesity, cellular stress, hypoxia and fibrosis, can be a potential cause of inflammation in prostate cancer. Crosstalk between cancer cells, stromal cells, and immune cells promotes chronic inflammation and facilitates prostate cancer progression via a variety of intercellular signaling molecules. Prostate tumor microenvironment is generally considered to be immunologically “cold” as M2-like TAMs and MDSCs cooperatively inhibit effector T cells and activate regulatory T cells. PhIP, 2-amino-1-methyl-6-phenylimidazo [4,5-b]pyridine; PGE2, prostaglandin E2; CSF-1, colony stimulating factor-1; TGF-β, transforming growth factor-β; ARG1, arginase 1; iNOS, inducible nitric oxide synthase; TAM, tumor-associated macrophage; MDSC, myeloid-derived suppressor cell; Treg, regulatory T cell.
Figure 2.
Inflammatory microenvironment in prostate cancer. Diverse mechanisms, such as microbiome, dietary carcinogens, obesity, cellular stress, hypoxia and fibrosis, can be a potential cause of inflammation in prostate cancer. Crosstalk between cancer cells, stromal cells, and immune cells promotes chronic inflammation and facilitates prostate cancer progression via a variety of intercellular signaling molecules. Prostate tumor microenvironment is generally considered to be immunologically “cold” as M2-like TAMs and MDSCs cooperatively inhibit effector T cells and activate regulatory T cells. PhIP, 2-amino-1-methyl-6-phenylimidazo [4,5-b]pyridine; PGE2, prostaglandin E2; CSF-1, colony stimulating factor-1; TGF-β, transforming growth factor-β; ARG1, arginase 1; iNOS, inducible nitric oxide synthase; TAM, tumor-associated macrophage; MDSC, myeloid-derived suppressor cell; Treg, regulatory T cell.


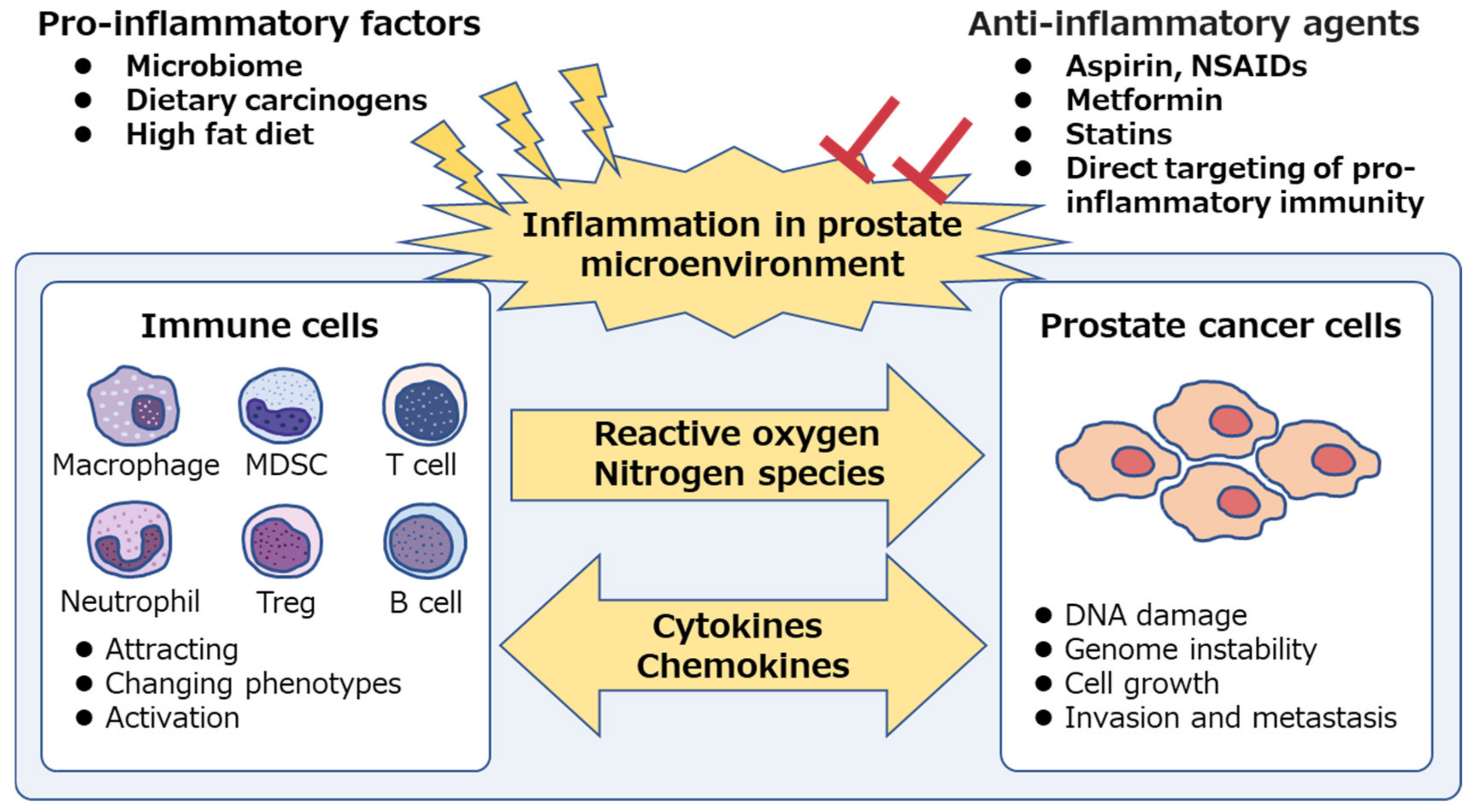{kind=link}
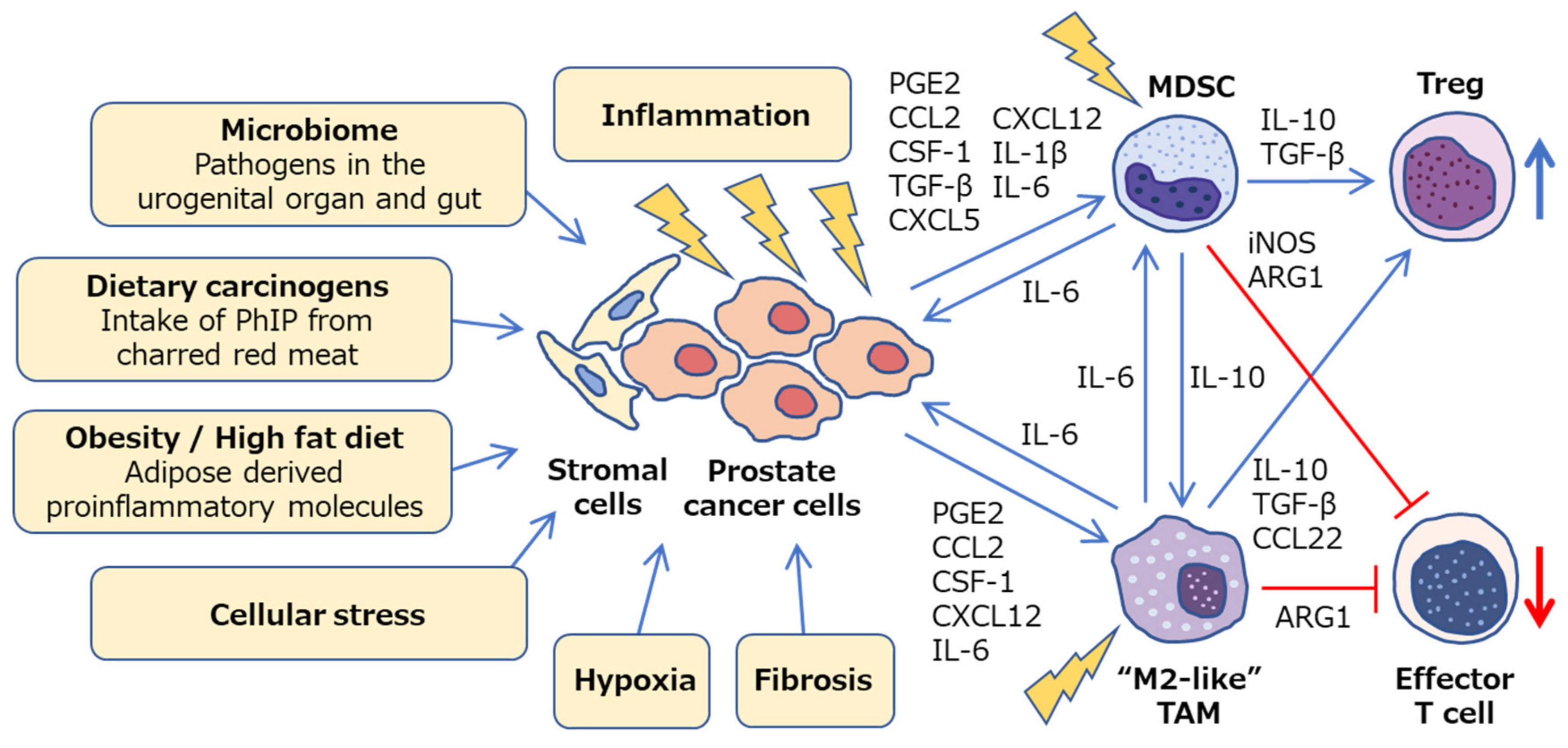{kind=link}
Table 1.
Overview of potential applications of anti-inflammatory agents in chemoprevention of PCa.
| Agents | Summary of Findings | References |
|---|---|---|
| Aspirin | 1. Aspirin, which is widely administrated in order to prevent and treat cardiovascular diseases, potentially reduces a risk of human carcinogenesis. | [169] |
| 2. Current and past regular aspirin use is likely to be associated with a lower risk of PCa. | [170,171,172,173] | |
| 3. Post-diagnosis aspirin use is likely to be associated with lower PCa-specific mortality. | [170,174,175,176] | |
| COX-2 inhibitors | 1. Long-term use of COX-2 selective inhibitor is associated with the potential cardiovascular risks. | [177,178] |
| 2. Feasible COX2 inhibitor candidates are still unclear for preventing PCa progression. | [179,180] | |
| Metformin | 1. Metformin is beneficial for patients with PCa, preventing ADT-induced metabolic syndrome. | [181] |
| 2. Metformin may improve PCa-specific survival, although the incidence of PCa is not associated with metformin. | [182] | |
| Statins | 1. Statins are widely used in the prevention of coronary artery disease. | [183] |
| 2. Statin use may reduce the risk of PCa. | [184] | |
| 3. Post-diagnostic statin use may correlate with reductions in PCa-specific mortality. | [185,186,187] |
PCa, prostate cancer; ADT, androgen deprivation therapy.
Table 2.
Clinical trials of agents targeted at TAMs and/or MDSCs in prostate cancer.
| Drug Name | Target | Inhibitor Type | Phase | Indication | Combination | ClinicalTrials.gov Reference |
|---|---|---|---|---|---|---|
| CNTO328 (siltuximab) | IL-6 | mAb | 1 | mCRPC | DOC | NCT00401765 b |
| CNTO328 (siltuximab) | IL-6 | mAb | 2 | mCRPC | NA | NCT00433446 b |
| CNTO328 (siltuximab) | IL-6 | mAb | 2 | mCRPC | MIT + Pred | NCT00385827 b |
| Ruxolitinib | JAK1/2 | SM | 2 | mCRPC | NA | NCT00638378 b |
| Niclosamide | STAT3 | SM | 1 | mCRPC | ENZ | NCT02532114 b |
| Niclosamide | STAT3 | SM | 1 | mCRPC | ENZ | NCT03123978 a |
| Niclosamide | STAT3 | SM | 2 | mCRPC | ABI + Pred | NCT02807805 a |
| PLX3397 (Pexidartinib) | CSF1R | SM | 1 | Intermediate or high risk PCa | RT + ADT | NCT02472275 a |
| PLX3397 (Pexidartinib) | CSF1R | SM | 2 | mCRPC | NA | NCT01499043 b |
| JNJ-40346527 | CSF1R | SM | 1 | High risk localized PCa | RP | NCT03177460 a |
| LY3022855 (IMC-CS4) | CSF1R | mAb | 1 | Advanced PCa and BCa | NA | NCT02265536 b |
| CNTO 888 (Carlumab) | CCL2 | mAb | 2 | mCRPC | NA | NCT00992186 b |
| Burixafor hydrobromide | CXCR4 | SM | 1 | mCRPC | ± G-CSF ± DOC | NCT02478125 b |
| Tasquinimod | S100A9 | SM | 3 | mCRPC | NA | NCT01234311 b |
| Ibrutinib | BTK | SM | 1, 2 | Localized PCa | RP | NCT02643667 a |
| Indoximod | IDO | SM | 2 | mCRPC | Sipuleucel-T | NCT01560923 b |
mAb, monoclonal antibody; SM, small molecule; mCRPC, metastatic castration resistant prostate cancer; PCa, prostate cancer; BCa, breast cancer; DOC, docetaxel; NA, not applicable; MIT, mitoxantrone; Pred, Prednisone; ENZ, enzalutamide; ABI, Abiraterone; RT, radiation therapy; ADT, androgen deprivation therapy; RP, Radical Prostatectomy. a Trial currently ongoing. b Trial completed.
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Hatano, K.; Fujita, K.; Nonomura, N. Application of Anti-Inflammatory Agents in Prostate Cancer. J. Clin. Med. 2020, 9, 2680. https://doi.org/10.3390/jcm9082680
AMA Style
Hatano K, Fujita K, Nonomura N. Application of Anti-Inflammatory Agents in Prostate Cancer. Journal of Clinical Medicine. 2020; 9(8):2680. https://doi.org/10.3390/jcm9082680
Chicago/Turabian StyleHatano, Koji, Kazutoshi Fujita, and Norio Nonomura. 2020. "Application of Anti-Inflammatory Agents in Prostate Cancer" Journal of Clinical Medicine 9, no. 8: 2680. https://doi.org/10.3390/jcm9082680
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.