
Implementation of a Real-Time Medication Intake Monitoring Technology Intervention in Community Pharmacy Settings: A Mixed-Method Pilot Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
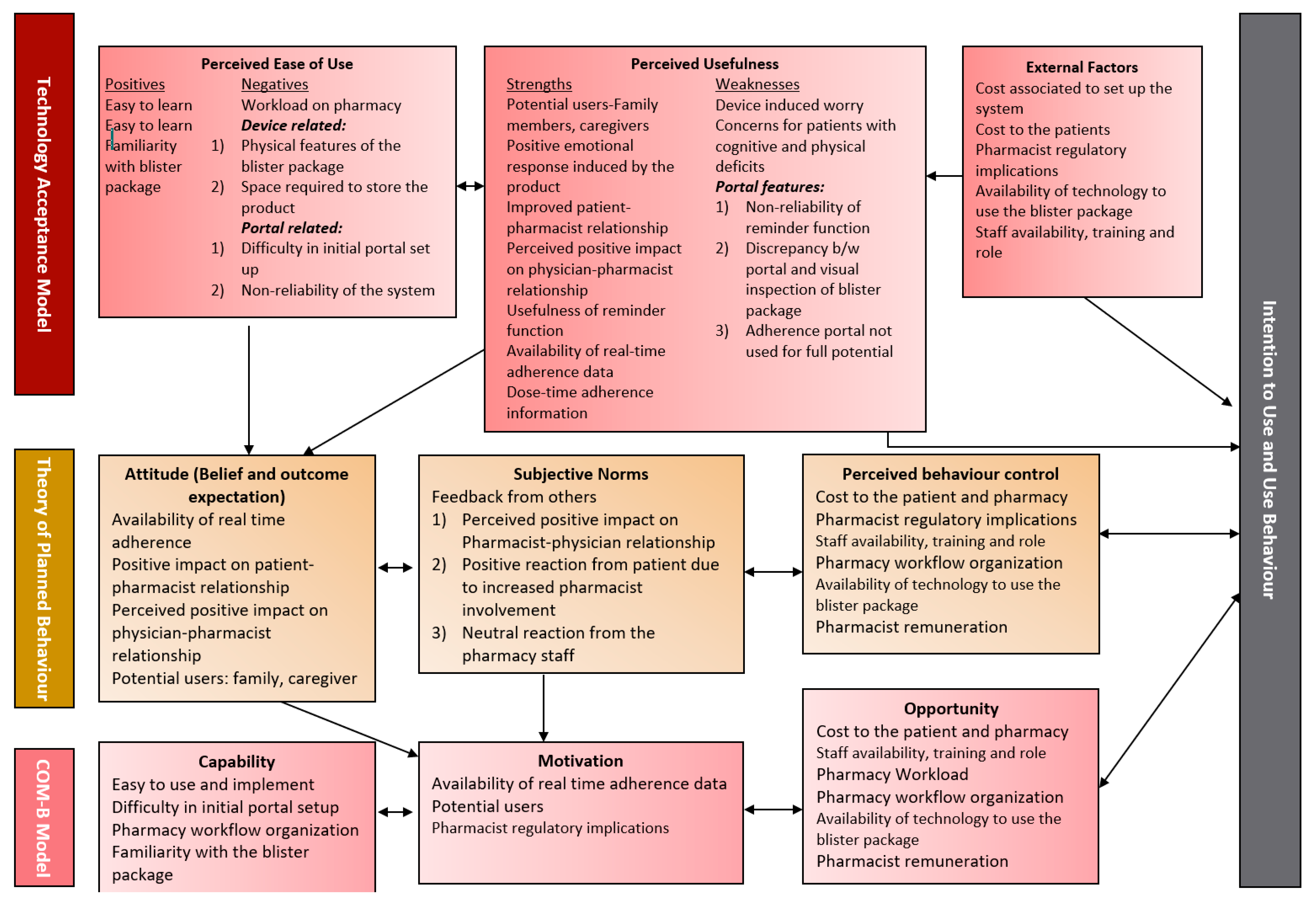
2.1. Theoretical Framework
2.2. System Usability Scale
2.3. Study Design
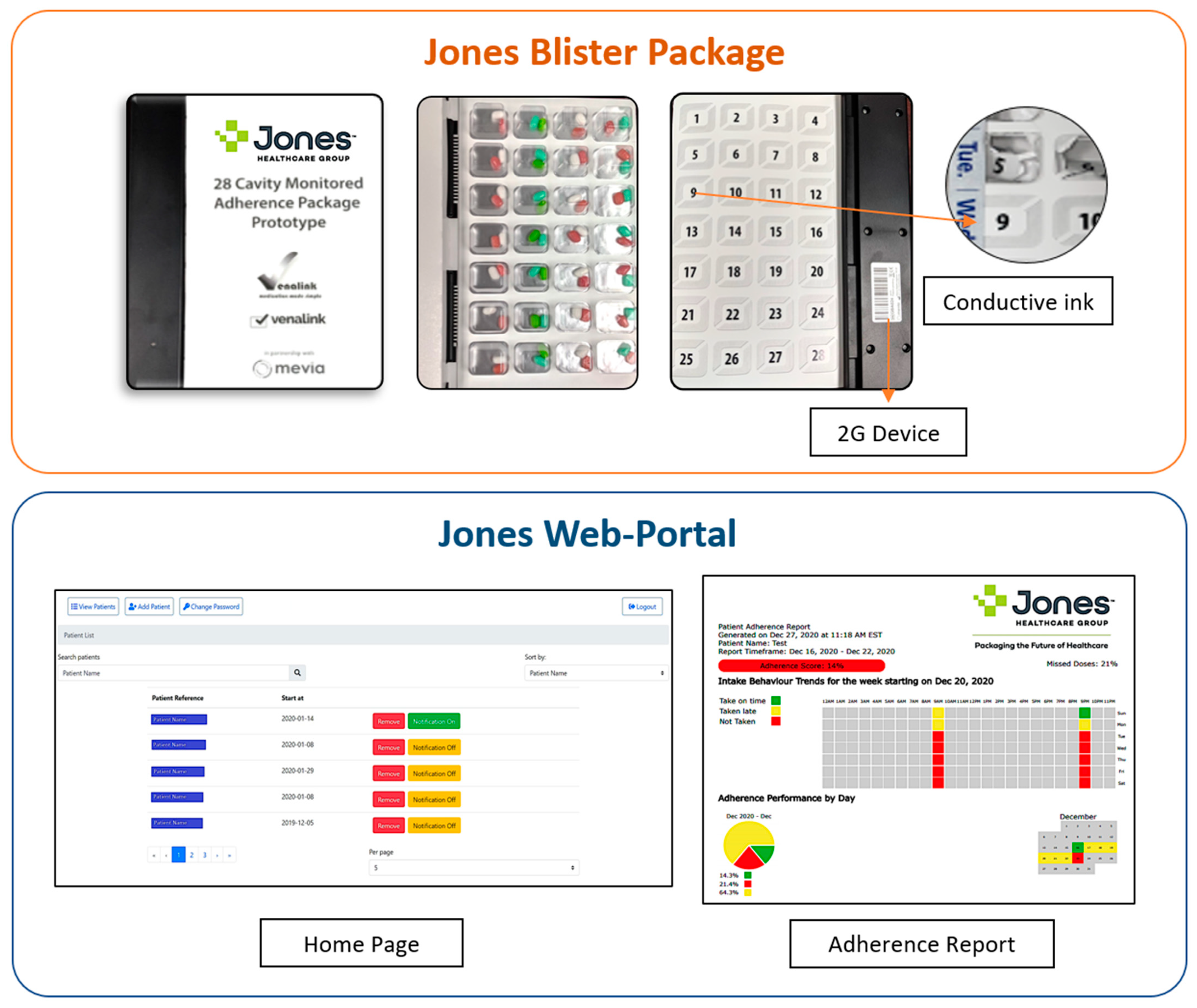
2.4. Study Material
Smart Adherence Technology System
- (a)
- Smart multidose blister package
- (b)
- Cloud-based Software Portal
2.5. Ethical Consideration
2.6. Study Participants
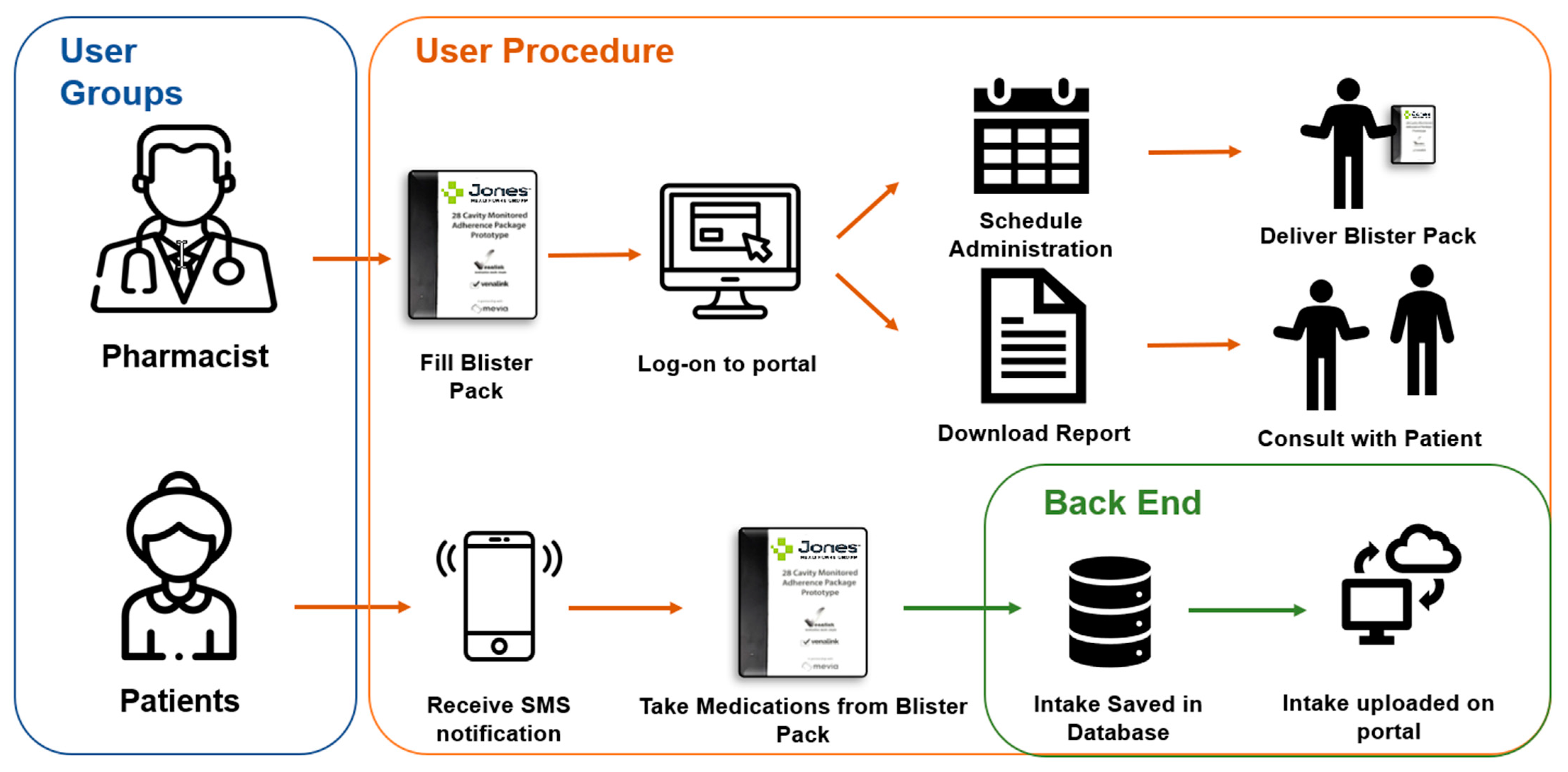
2.7. Study Procedures
2.8. Data Collection
2.8.1. Qualitative: Semi-structured Interviews
2.8.2. Quantitative: System Usability Scale
2.9. Data Analysis
3. Results
3.1. Demographic Characteristics
3.2. Themes and Sub-Themes
3.2.1. Theme 1: Pharmacy Workflow Related Factors
Sub-Theme 1.1: Pharmacy Workload
Sub-Theme 1.2: Staff Availability, Training and Role
Sub-Theme 1.3: Pharmacy Workflow Organization
Sub-Theme 1.4: Cost Associated to Set up the System
Sub-Theme 1.5: Regulatory Implication
Sub-Theme 1.6: Feedback from Others
Sub-Theme 1.7: Improved Patient Interaction
3.2.2. Theme 2: Integration Related Factors
Sub-Theme 2.1: Product Design Factors
Sub-Theme 2.2: Portal Factors
3.2.3. Theme 3: Pharmacist Perceived Patient Related Factors
Sub-Theme 3.1: Potential Users
Sub-Theme 3.2: Concerns for Users
Sub-Theme 3.3: Cost to the End-Users
Sub-Theme 3.4: Technology Access for the End-User
3.3. Themes and Sub-Themes Mapped to Theoretical Frameworks
3.4. System Usability Scale
4. Discussion
4.1. Principal Findings
4.2. System Usability Scale
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action; Sabate, D.G., Ed.; World Health Organization: Geneva, Switzerland, 2003; Available online: https://www.who.int/chp/knowledge/publications/adherence_full_report.pdf?ua=1 (accessed on 20 January 2021).
- Lee, H.J.; Jang, S.-I.; Park, E.-C. Effect of adherence to antihypertensive medication on stroke incidence in patients with hypertension: A population-based retrospective cohort study. BMJ Open 2017, 7, e014486. [Google Scholar] [CrossRef] [Green Version]
- Egede, L.E.; Gebregziabher, M.; Dismuke, C.E.; Lynch, C.P.; Axon, R.N.; Zhao, Y.; Mauldin, P.D. Medication nonadherence in diabetes: Longitudinal effects on costs and potential cost savings from improvement. Diabetes Care 2012, 35, 2533–2539. [Google Scholar] [CrossRef] [Green Version]
- Marengoni, A.; Monaco, A.; Costa, E.; Cherubini, A.; Prados-Torres, A.; Muth, C.; Melis, R.J.F.; Pasina, L.; Van Der Cammen, T.J.M.; Palmer, K.; et al. Strategies to Improve Medication Adherence in Older Persons: Consensus Statement from the Senior Italia Federanziani Advisory Board. Drugs Aging 2016, 33, 629–637. [Google Scholar] [CrossRef]
- Anghel, L.A.; Farcas, A.M.; Oprean, R.N. An overview of the common methods used to measure treatment adherence. Med. Pharm. Rep. 2019, 92, 117–122. [Google Scholar] [CrossRef]
- Van Heuckelum, M.; van den Ende, C.H.; Houterman, A.E.; Heemskerk, C.P.; van Dulmen, S.; van den Bemt, B.J. The effect of electronic monitoring feedback on medication adherence and clinical outcomes: A systematic review. PLoS ONE 2017, 12, e0185453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, L.G.; Howie-Esquivel, J.; Dracup, K. Electronic Measurement of Medication Adherence. West. J. Nurs. Res. 2015, 37, 28–49. [Google Scholar] [CrossRef]
- Morton, R.W.; Elphick, H.E.; Rigby, A.S.; Daw, W.J.; King, D.A.; Smith, L.J.; Everard, M.L. STAAR: A randomised controlled trial of electronic adherence monitoring with reminder alarms and feedback to improve clinical outcomes for children with asthma. Thorax 2017, 72, 347–354. [Google Scholar] [CrossRef]
- Abacus Data conducted for Canadian Pharmacists Association. Pharmacists in Canada—A National Survey of Canadians on Their Perceptions and Attitudes towards Pharmacists. 2018. Available online: http://www.pharmacists.ca/cpha-ca/assets/File/news-events/PAM2015-Poll.pdf (accessed on 27 January 2021).
- Raiche, T.; Pammett, R.; Dattani, S.; Dolovich, L.; Hamilton, K.; Kennie-Kaulbach, N.; McCarthy, L.; Jorgenson, D. Community pharmacists’ evolving role in Canadian primary health care: A vision of harmonization in a patchwork system. Pharm. Pract. (Granada) 2020, 18, 2171. [Google Scholar] [CrossRef] [PubMed]
- Labrie, Y. The Other Health Care System: Four Areas Where the Private Sector Answers Patients’ Needs; Montreal Economic Institute: Montreal, QC, Canada, 2015; Available online: https://www.iedm.org/sites/default/files/pub_files/cahier0115_en.pdf (accessed on 31 January 2021).
- Van Eikenhorst, L.; Taxis, K.; van Dijk, L.; de Gier, H. Pharmacist-led self-management interventions to improve diabetes outcomes. A systematic literature review and meta-analysis. Front. Pharmacol. 2017, 8, 891. [Google Scholar] [CrossRef] [Green Version]
- Williams, A.F.; Manias, E.; Gaskin, C.J.; Crawford, K. Medicine non-adherence in kidney transplantation. J. Ren. Care 2014, 40, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Marcum, Z.A.; Hanlon, J.T.; Murray, M.D. Improving Medication Adherence and Health Outcomes in Older Adults: An Evidence-Based Review of Randomized Controlled Trials. Drugs Aging 2017, 34, 191–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osterberg, L.; Blaschke, T. Adherence to Medication. N. Engl. J. Med. 2005, 353, 487–497. [Google Scholar] [CrossRef] [Green Version]
- Milosavljevic, A.; Aspden, T.; Harrison, J. Community pharmacist-led interventions and their impact on patients’ medication adherence and other health outcomes: A systematic review. Int. J. Pharm. Pract. 2018, 26, 387–397. [Google Scholar] [CrossRef]
- Akinbosoye, O.E.; Taitel, M.S.; Grana, J.; Hill, J.; Wade, R.L. Improving Medication Adherence and Health Care Outcomes in a Commercial Population through a Community Pharmacy. Popul. Health Manag. 2016, 19, 454–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, M.; Young, J.; Hoke, S.; Tu, W.; Weiner, M.; Morrow, D.; Stroupe, K.T.; Wu, J.; Clark, D.; Smith, F.; et al. Medicine Improving Patient Care Pharmacist Intervention to Improve Medication Adherence in Heart Failure. Ann. Intern. Med. 2007, 146, 714–725. [Google Scholar] [CrossRef]
- Aldeer, M.; Javanmard, M.; Martin, R.P. A Review of Medication Adherence Monitoring Technologies. Appl. Syst. Innov. 2018, 1, 14. [Google Scholar] [CrossRef] [Green Version]
- Faisal, S.; Ivo, J.; Patel, T. Smart Electronic Medication Adherence Products: A Comparison of Features. In Proceedings of the ACCP Virtual Poster Symposium, 26–27 May 2020; American College of Clinical Pharmacy: Lenexa, KS, USA, 2020. [Google Scholar]
- Spencer: In-home Medication Dispenser. Available online: https://catalystrms.com/products/spencer/ (accessed on 24 November 2019).
- RxPense. Available online: https://medipense.com/en/wp-content/uploads/2020/02/RxPense-Product-Brief-2020-EN.pdf (accessed on 30 November 2019).
- Philips Medication Dispenser. Available online: https://www.lifeline.philips.com/pill-dispenser/health-mdp.html (accessed on 15 November 2019).
- MacCallum, L.; Mathers, A.; Kellar, J.; Rousse-Grossman, J.; Moore, J.; Lewis, G.F.; Dolovich, L. Pharmacists report lack of reinforcement and the work environment as the biggest barriers to routine monitoring and follow-up for people with diabetes: A survey of community pharmacists. Res. Soc. Adm. Pharm. 2021, 17, 332–343. [Google Scholar] [CrossRef] [PubMed]
- Hossain, L.N.; Fernandez-Llimos, F.; Luckett, T.; Moullin, J.C.; Durks, D.; Franco-Trigo, L.; I Benrimoj, S.; Sabater-Hernández, D. Qualitative meta-synthesis of barriers and facilitators that influence the implementation of community pharmacy services: Perspectives of patients, nurses and general medical practitioners. BMJ Open 2017, 7. [Google Scholar] [CrossRef]
- Newman, T.V.; Hernandez, I.; Keyser, D.; San-Juan-Rodriguez, A.; Swart, E.C.; Shrank, W.H.; Parekh, N. Optimizing the Role of Community Pharmacists in Managing the Health of Populations: Barriers, Facilitators, and Policy Recommendations. J. Manag. Care Spec. Pharm. 2019, 25, 995–1000. [Google Scholar] [CrossRef]
- Lott, B.E.; Anderson, E.J.; Zapata, L.V.; Cooley, J.; Forbes, S.; Taylor, A.M.; Manygoats, T.; Warholak, T. Expanding pharmacists’ roles: Pharmacists’ perspectives on barriers and facilitators to collaborative practice. J. Am. Pharm. Assoc. 2021, 61, 213–220.e1. [Google Scholar] [CrossRef]
- Nielsen, J. Usability 101: Introduction to Usability. 2012. Available online: https://www.nngroup.com/articles/usability-101-introduction-to-usability/ (accessed on 1 February 2021).
- Holden, R.J.; Karsh, B.T. The Technology Acceptance Model: Its past and its future in health care. J. Biomed. Inform. 2010, 43, 159–172. [Google Scholar] [CrossRef] [Green Version]
- Lai, P. the Literature Review of Technology Adoption Models and Theories for the Novelty Technology. J. Inf. Syst. Technol. Manag. 2017, 14, 21–38. [Google Scholar] [CrossRef] [Green Version]
- Darby, A.B.; Su, Y.; Reynolds, R.B.; Madlock-Brown, C. A Survey-based Study of Pharmacist Acceptance and Resistance to Health Information Technology. Perspect. Health Inf. Manag. 2019, 16, 1a. [Google Scholar] [PubMed]
- Oyetunde, O.O.; Ogidan, O.; Akinyemi, M.I.; Ogunbameru, A.A.; Asaolu, O.F. Mobile authentication service in Nigeria: An assessment of community pharmacists’ acceptance and providers’ views of successes and challenges of deployment. Pharm. Pract. (Granada) 2019, 17, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tai, B.-W.B.; Hata, M.; Wu, S.; Frausto, S.; Law, A.V. Prediction of pharmacist intention to provide medication disposal education using the theory of planned behaviour. J. Eval. Clin. Pract. 2016, 22, 653–661. [Google Scholar] [CrossRef]
- Walker, A.; Watson, M.; Grimshaw, J.; Bond, C. Applying the theory of planned behaviour to pharmacists’ beliefs and intentions about the treatment of vaginal candidiasis with non-prescription medicines. Fam. Pract. 2004, 21, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Varisco, T.J.; Downs, C.G.; Rathburn, K.R.; Fleming, M.L.; Thornton, J.D. Applying the capability, opportunity, motivation, and behavior model to identify opportunities to increase pharmacist comfort dispensing naloxone in Texas: A structural equation modeling approach. Int. J. Drug Policy 2020, 83, 102827. [Google Scholar] [CrossRef]
- Fleming, M.L.; Barner, J.C.; Brown, C.M.; Shepherd, M.D.; Strassels, S.; Novak, S. Using the theory of planned behavior to examine pharmacists’ intention to utilize a prescription drug monitoring program database. Res. Soc. Adm. Pharm. 2014, 10, 285–296. [Google Scholar] [CrossRef]
- McDonagh, L.K.; Saunders, J.M.; Cassell, J.; Curtis, T.; Bastaki, H.; Hartney, T.; Rait, G. Application of the COM-B model to barriers and facilitators to chlamydia testing in general practice for young people and primary care practitioners: A systematic review. Implement. Sci. 2018, 13, 130. [Google Scholar] [CrossRef]
- Korenvain, C.; MacKeigan, L.D.; Dainty, K.N.; Guilcher, S.J.; McCarthy, L.M. Exploring deprescribing opportunities for community pharmacists using the Behaviour Change Wheel. Res. Soc. Adm. Pharm. 2020, 16, 1746–1753. [Google Scholar] [CrossRef]
- Brooke, J. SUS—A quick and dirty usability scale. Usability Eval. Ind. 1996, 189, 4–7. [Google Scholar]
- Kortum, P.T.; Bangor, A. Usability Ratings for Everyday Products Measured With the System Usability Scale. Int. J. Hum. Comput. Interact. 2013, 29, 67–76. [Google Scholar] [CrossRef]
- Bloom, B.M.; Pott, J.; Thomas, S.; Gaunt, D.R.; Hughes, T.C. Usability of electronic health record systems in UK EDs. Emerg. Med. J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Holden, R.J.; Campbell, N.L.; Abebe, E.; Clark, D.O.; Ferguson, D.; Bodke, K.; Boustani, M.A.; Callahan, C.M. Usability and feasibility of consumer-facing technology to reduce unsafe medication use by older adults. Res. Soc. Adm. Pharm. 2020, 16, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Gao, M.; Kortum, P. Measuring the Usability of Home Healthcare Devices Using Retrospective Measures. Proc. Hum. Factors Ergon. Soc. 2017, 61, 1281–1285. [Google Scholar] [CrossRef]
- Patel, T.; Ivo, J.; Faisal, S.; McDougall, A.; Carducci, J.; Pritchard, S.; Chang, F. A prospective study of usability and workload of electronic medication adherence products by older adults, caregivers, and health care providers. J. Med. Internet Res. 2020, 22, e18073. [Google Scholar] [CrossRef]
- Mol, M.; van Schaik, A.; Dozeman, E.; Ruwaard, J.; Vis, C.; Ebert, D.D.; Etzelmueller, A.; Mathiasen, K.; Moles, B.; Mora, T.; et al. Dimensionality of the system usability scale among professionals using internet-based interventions for depression: A confirmatory factor analysis. BMC Psychiatry 2020, 20, 218. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- McGrath, C.; Palmgren, P.J.; Liljedahl, M. Twelve tips for conducting qualitative research interviews. Med. Teach. 2019, 41, 1002–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latif, A.; Waring, J.; Watmough, D.; Barber, N.; Chuter, A.; Davies, J.; Salema, N.-E.; Boyd, M.J.; Elliott, R.A. Examination of England’s New Medicine Service (NMS) of complex health care interventions in community pharmacy. Res. Soc. Adm. Pharm. 2016, 12, 966–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quintana-Bárcena, P.; LaLonde, L.; Lauzier, S. Beliefs influencing community pharmacists’ interventions with chronic kidney disease patients: A theory-based qualitative study. Res. Soc. Adm. Pharm. 2019, 15, 145–153. [Google Scholar] [CrossRef]
- Witry, M.J.; Doucette, W.R. Community pharmacists, medication monitoring, and the routine nature of refills: A qualitative study. J. Am. Pharm. Assoc. 2014, 54, 594–603. [Google Scholar] [CrossRef]
- Dillon, P.; McDowell, R.; Smith, S.M.; Gallagher, P.; Cousins, G. Determinants of intentions to monitor antihypertensive medication adherence in Irish community pharmacy: A factorial survey. BMC Fam. Pract. 2019, 20, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houle, S.K.D.; Grindrod, K.A.; Chatterley, T.; Tsuyuki, R.T. Paying pharmacists for patient care: A systematic review of remunerated pharmacy clinical care services. Can. Pharm. J. 2014, 147, 209–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katangwe, T.; Family, H.; Sokhi, J.; Al-Jabr, H.; Kirkdale, C.L.; Twigg, M.J. The community pharmacy setting for diabetes prevention: Views and perceptions of stakeholders. PLoS ONE 2019, 14, e0219686. [Google Scholar] [CrossRef] [Green Version]
- Nakhla, N.; Killeen, R. Pharmacist-Led Smoking Cessation Care in Canada: Current Status & Strategies for Expansion; University of Waterloo School of Pharmacy: Kitchener, ON, Canada, 2019; pp. 1–32. Available online: https://uwaterloo.ca/pharmacy/sites/ca.pharmacy/files/uploads/files/whitepaper_final_nov_28_2019.pdf (accessed on 15 January 2021).
- Pullagura, G.R.; Violette, R.; Houle, S.K.; Waite, N.M. Shades of gray in vaccination decisions—Understanding community pharmacists’ perspectives of, and experiences with, influenza vaccine hesitancy in Ontario, Canada. Vaccine 2020, 38, 2551–2558. [Google Scholar] [CrossRef]
- Government of Canada. Canada’s Health Care System. 2011. Available online: https://www.canada.ca/en/health-canada/services/health-care-system/reports-publications/health-care-system/canada.html (accessed on 15 February 2021).
- Ministry of Health and Long-Term Care. Drugs and Device Divisons, Ontario Public Drug Progrms. Available online: https://www.health.gov.on.ca/en/public/programs/drugs/ (accessed on 15 February 2021).
- Ministry of Health and Long-Term Care. Health Care Professional Minsitry Prograns and Services. Available online: https://www.health.gov.on.ca/en/pro/programs/ (accessed on 20 February 2021).
- Pringle, J.; Coley, K. Improving medication adherence: A framework for community pharmacy-based interventions. Integr. Pharm. Res. Pract. 2015, 4, 175–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | (N = 4) |
|---|---|
| Gender (n, %) Male | 3 (75.00%) |
| Age (years) Mean ± SD/Range | 43 ± 7.9/30–50 |
| Years of Practice Mean ± SD/Range | 19 ± 9.7/5–3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faisal, S.; Ivo, J.; Tennant, R.; Prior, K.-A.; Grindrod, K.; McMillan, C.; Patel, T. Implementation of a Real-Time Medication Intake Monitoring Technology Intervention in Community Pharmacy Settings: A Mixed-Method Pilot Study. Pharmacy 2021, 9, 105. https://doi.org/10.3390/pharmacy9020105
Faisal S, Ivo J, Tennant R, Prior K-A, Grindrod K, McMillan C, Patel T. Implementation of a Real-Time Medication Intake Monitoring Technology Intervention in Community Pharmacy Settings: A Mixed-Method Pilot Study. Pharmacy. 2021; 9(2):105. https://doi.org/10.3390/pharmacy9020105
Chicago/Turabian StyleFaisal, Sadaf, Jessica Ivo, Ryan Tennant, Kelsey-Ann Prior, Kelly Grindrod, Colleen McMillan, and Tejal Patel. 2021. "Implementation of a Real-Time Medication Intake Monitoring Technology Intervention in Community Pharmacy Settings: A Mixed-Method Pilot Study" Pharmacy 9, no. 2: 105. https://doi.org/10.3390/pharmacy9020105